damage control laparotomy - an evidence based approach
TRANSCRIPT
Dr. Yasser Abbas Department of General surgery
Concept of Damage control
History
Indications of Damage Control.
Damage Control Sequence.
Complications.
Summary.
Outlines
“ …keeping afloat a badly damaged ship by procedures to limit flooding , stabilize the vessel, isolate fires and explosions and avoid their spreading”
Surface ship survivability, Naval war publication
3-20.31, Washington, DC. Department of defense; 1996
Concept of Damage control
Definitive Surgery Approach?
“The operation was a success but the patient died anyway.”
– Anonymous
“He who fights and runs away, may live to fight another day.” – JA Aulls, 1876
Damage Control Approach ?
History
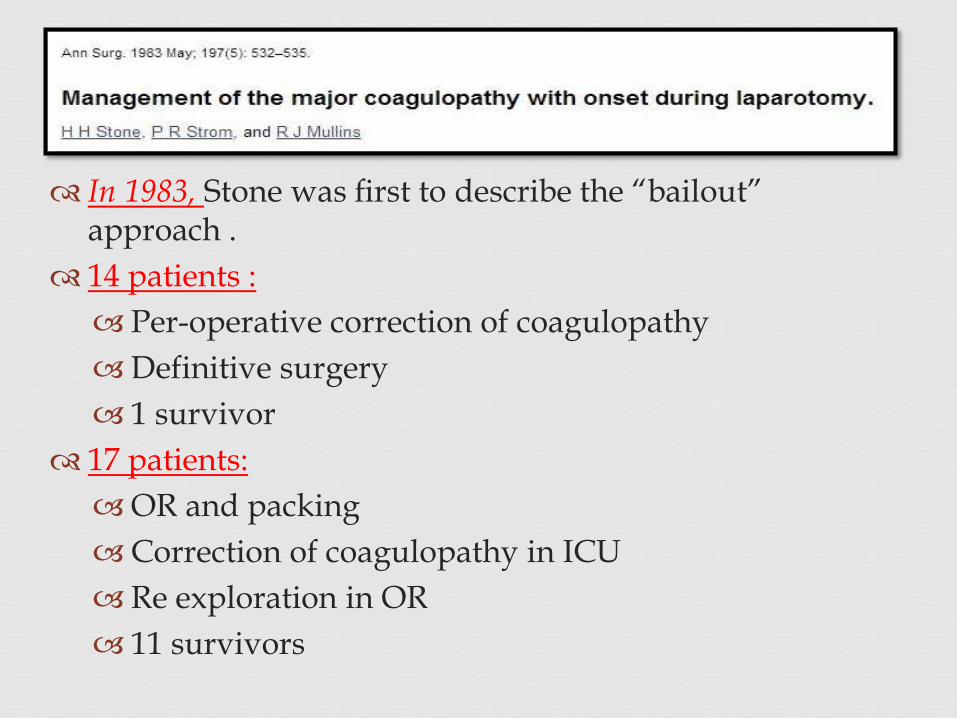
In 1983, Stone was first to describe the “bailout” approach .
14 patients :
Per-operative correction of coagulopathy
Definitive surgery
1 survivor
17 patients:
OR and packing
Correction of coagulopathy in ICU
Re exploration in OR
11 survivors
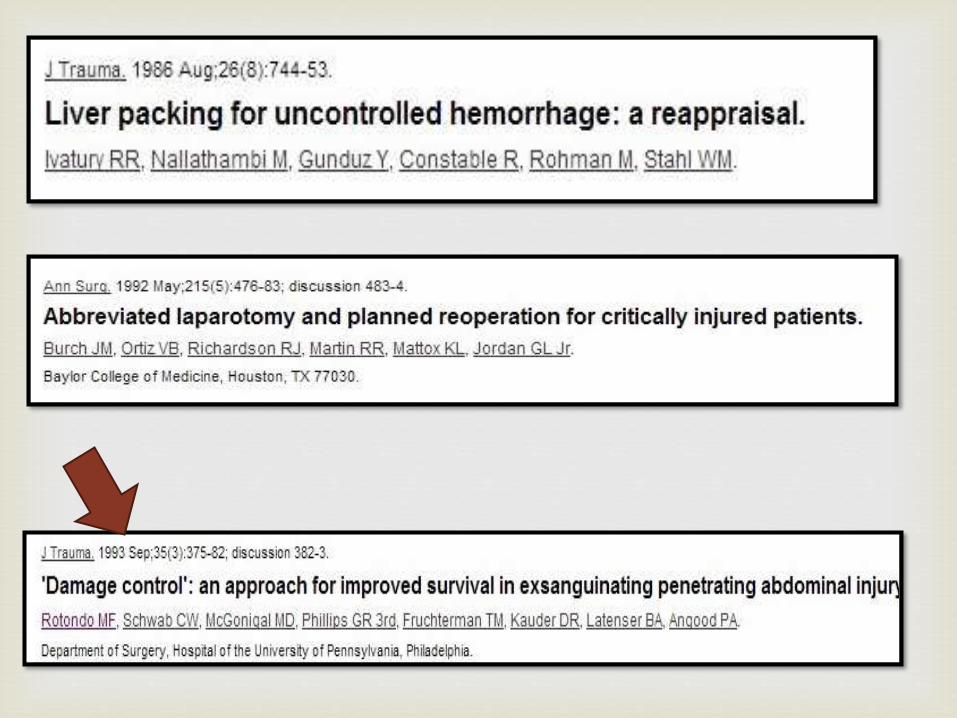
The concept of DC was initially described for intra-abdominal trauma, it has been expanded to :
Thoracic.
Extremity vascular.
Orthopedic injuries.
“Damage Control Resuscitation”. 1c
The Concept Expansion
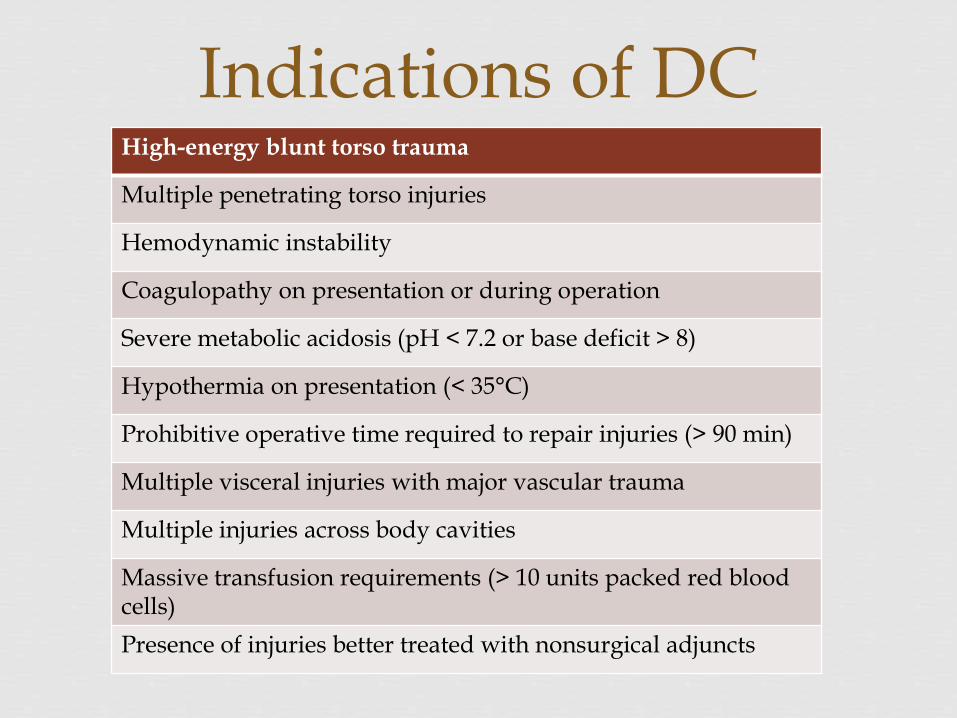
Indications of DCHigh-energy blunt torso trauma
Multiple penetrating torso injuries
Hemodynamic instability
Coagulopathy on presentation or during operation
Severe metabolic acidosis (pH < 7.2 or base deficit > 8)
Hypothermia on presentation (< 35°C)
Prohibitive operative time required to repair injuries (> 90 min)
Multiple visceral injuries with major vascular trauma
Multiple injuries across body cavities
Massive transfusion requirements (> 10 units packed red blood cells)
Presence of injuries better treated with nonsurgical adjuncts
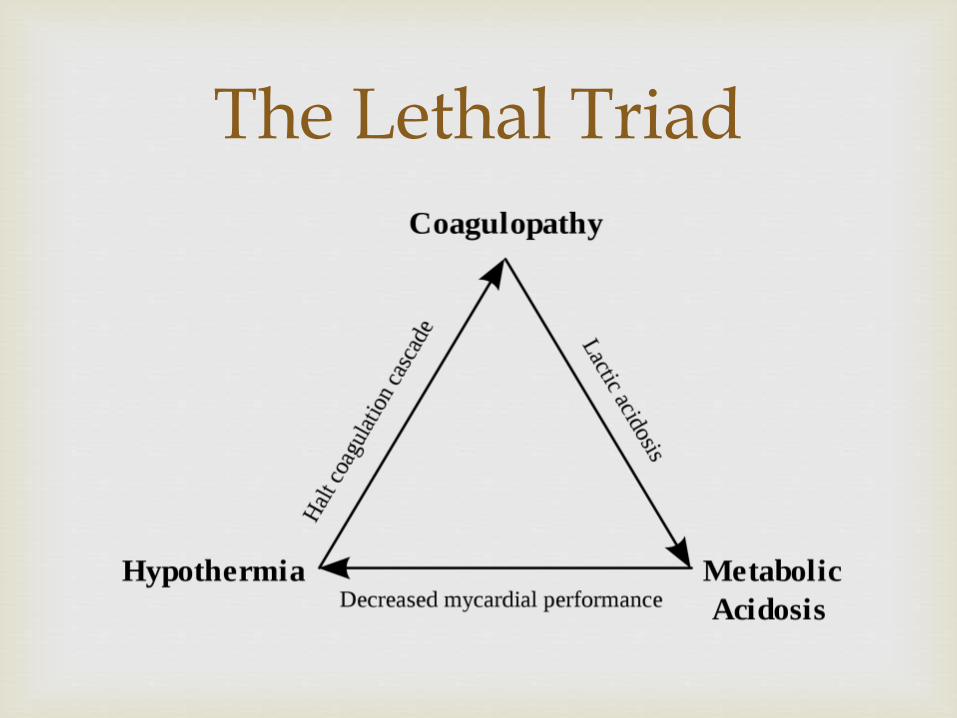
The Lethal Triad
It is Better to Cure in Phases rather than to Kill in one
- Anonymous
Prehospital care & Initial resuscitation:
Built on fundamentals of ATLS guidelines.
Rapid Transport to definitive care.
Rapid Evaluation.
FAST, Tube Thorocostomy , CXR, Pelvis X-ray, etc…
Damage Control Resuscitation to systolic 80-90 mmHg.
This phase should take 20-30 min.
DC SequenceGround 0
A DC approach should be taken with any patient in the
ED who has :
Revised Trauma Score ( RTS ) ≤ 5
Requires ≥ 2,000 ml of crystalloids for resuscitation in the ER.
Requires ≥ 2 units of PRBCs for resuscitation in the ER.
A pH of ≤ 7.2
Strength of evidence: C.
Asensio J, et al. Am J Surg 2001; 182: 743–51.
How do We Predict in ED ?
Control of Hemorrhage and Contamination:
Laparotomy
Evacuation of blood.
Four quadrant packing.
Full exposure of the injuries.
Kocher maneuver
Cattell-Braasch
Mattox
DC SequencePart 1(OR)
Solid organs: such as spleen and isolated kidney , are sacrificed in damage control if repair prolongs surgical times.
Bleeding vessel : Ligation /shunting.
Bowel injury: stapler/ ligation.
Intra-abdominal Packing
Temporary abdominal closure
This phase shouldn`t take more than 90 min.
DC SequencePart 1(OR)

Incisions in DC
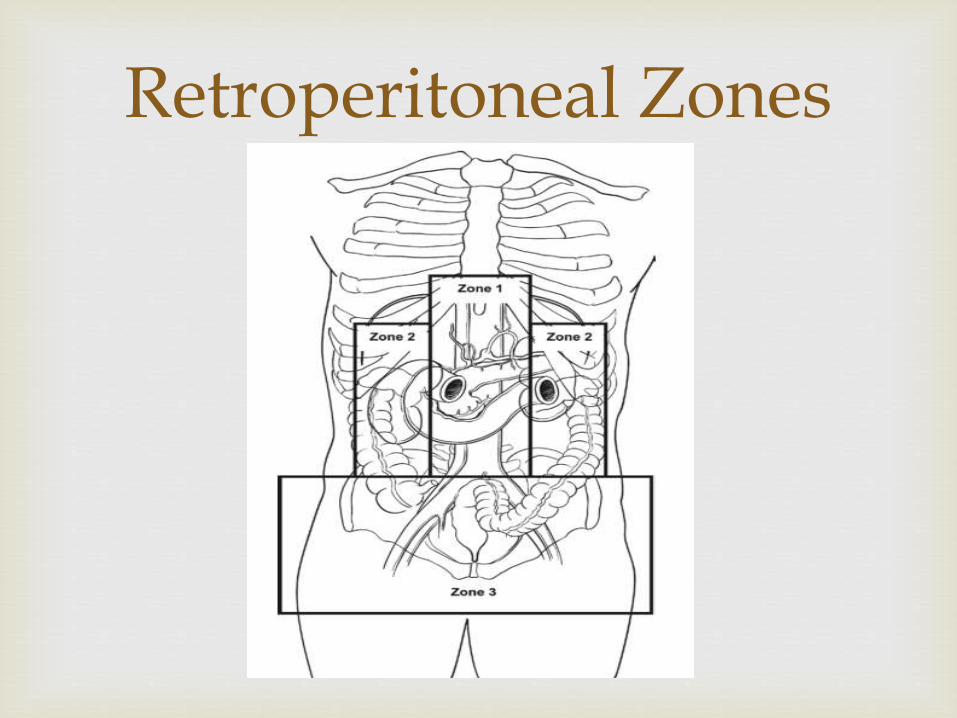
Retroperitoneal Zones
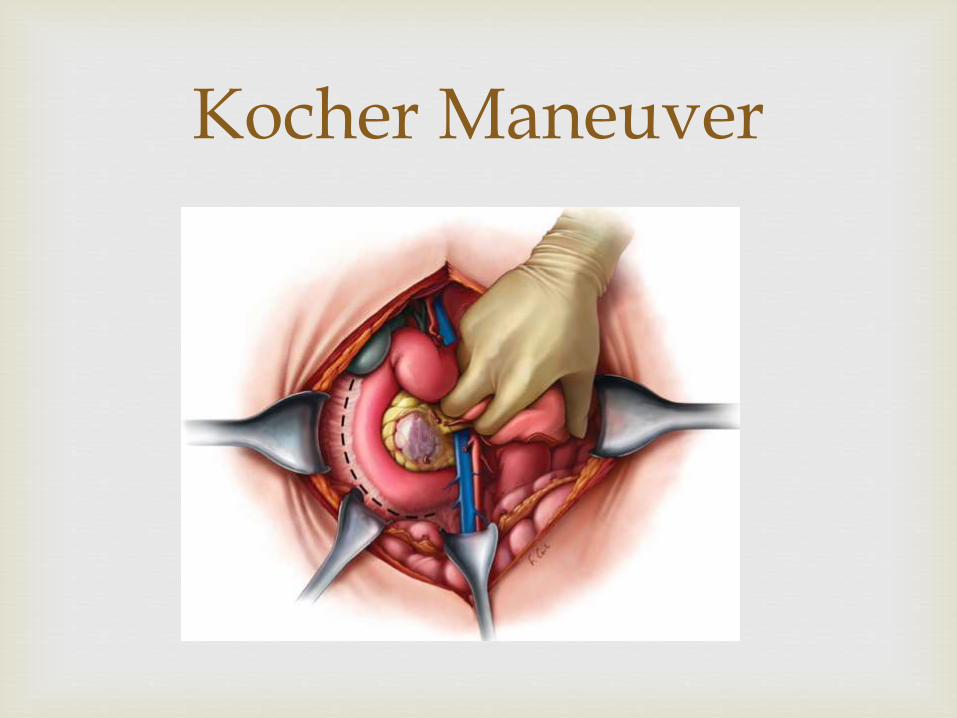
Kocher Maneuver
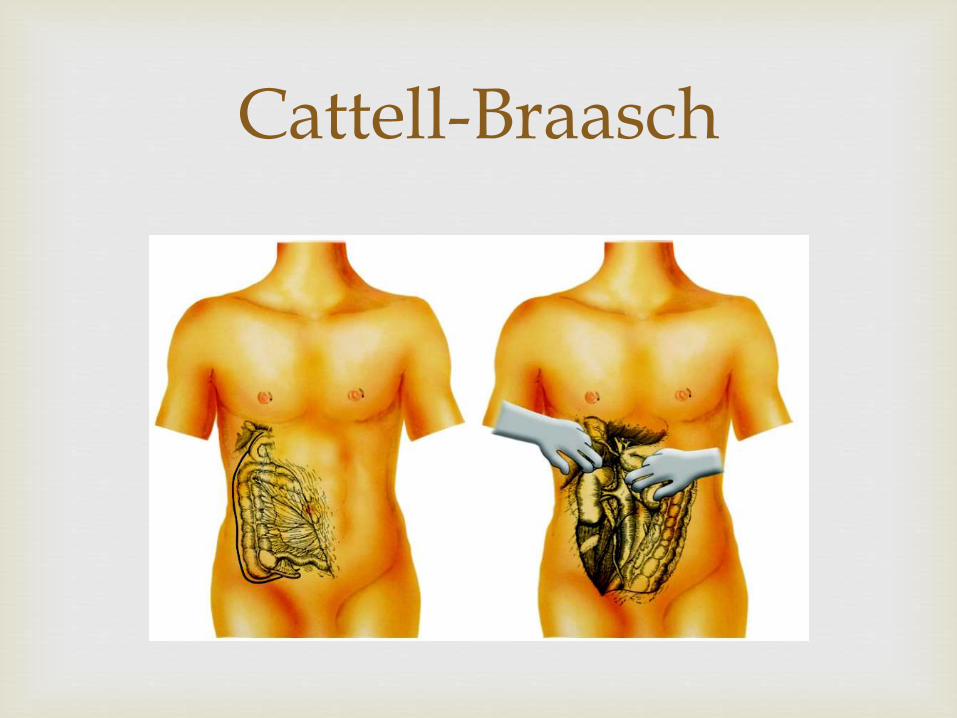
Cattell-Braasch
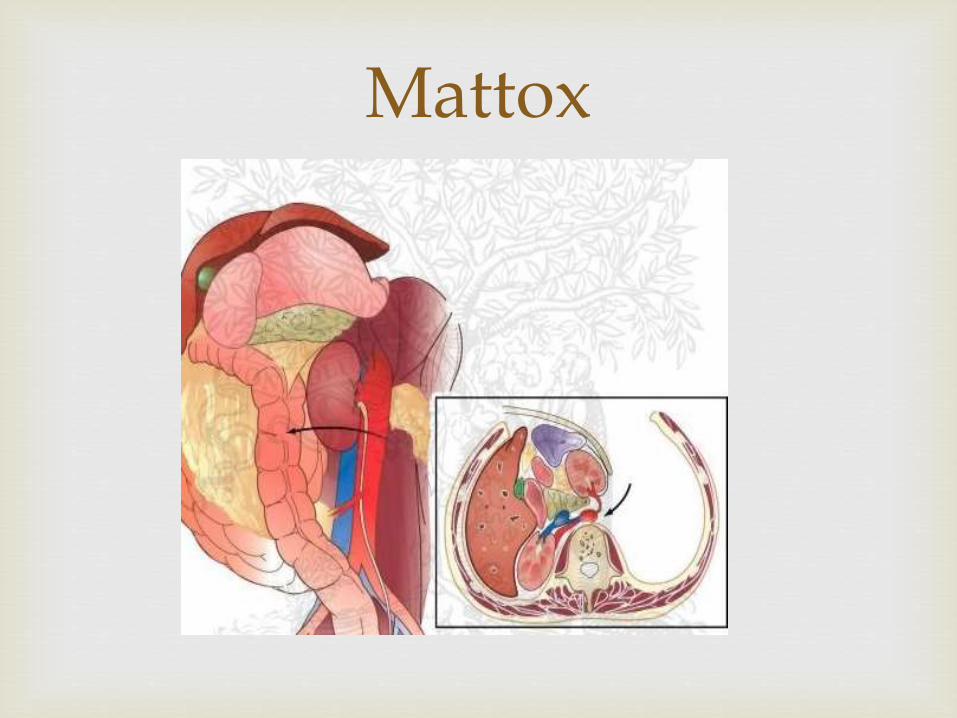
Mattox
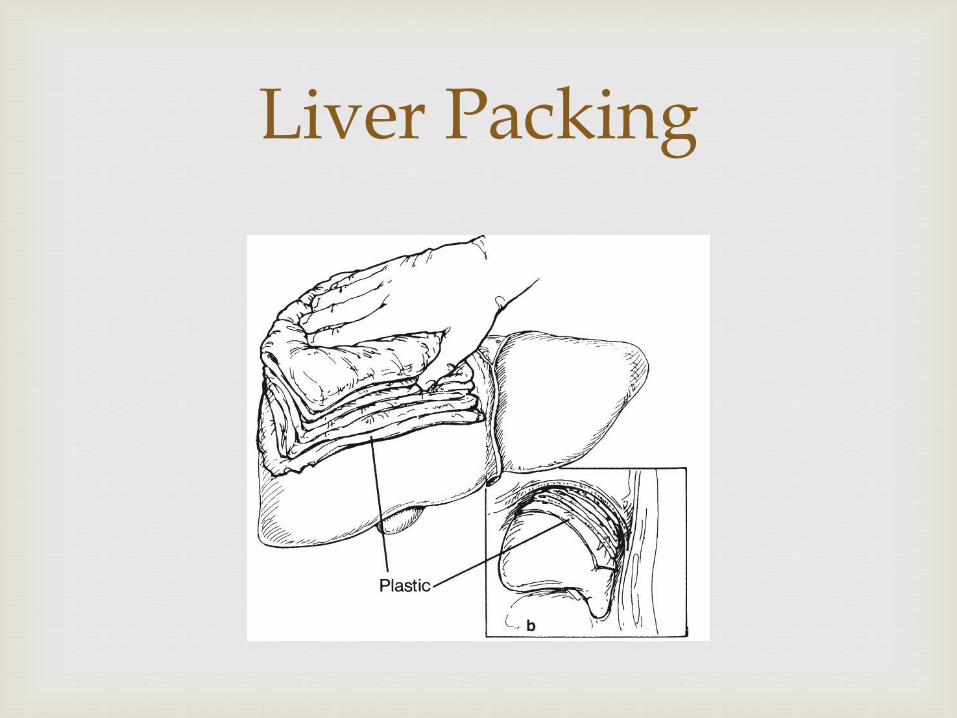
Liver Packing
Patients who require ≥ 4,000 ml PRBCs.
Patients who have had an ED or OR. thoracotomy.
pH ≤ 7.2
Temperature of ≤ 34°C
Inaccessible major venous injury
Intraoperative ; How to identify the patient for DC ?
If the surgeon cannot achieve hemostasis owing to coagulopathy
If the definitive operative repair is a time-consuming procedure in the patient with suboptimal response to resuscitation
If the patient requires the management of an extra-abdominal life-threatening injury
Intraoperative ; How to identify the patient for DC ?
If the patient will require a reassessment of intra-abdominal contents
If the surgeon cannot re-approximate the abdominal fascia due visceral edema.
Strength of recommendation: D.
Shapiro M, Jenkins D, Schwab C, et al. J Trauma 2000; 49: 969–78.
Rotondo M, Zonies D. Surg Clin N Am 1997; 77: 761–77.
Loveland J, Boffard K. Br J Surg 2004; 91: 1095–101
Intraoperative ; How to identify the patient for DC ?
Core temperature ≤ 34°C
pH ≤ 7.2
Prothromin time ≥ twice normal
Partial thromboplastin time ≥ twice normal
Strength of recommendation: B.
Ferrara A, MacArthur J, Wright H, et al. Am J Surg 1990; 160: 515–18.
Cosgriff N, Moore E, Sauaia A, et al. J Trauma 1997; 42: 857–61; discussion 861–2.
Garrison J, Richardson J, Hilakos A, et al. J Trauma 1996; 40: 923–7; discussion 927–9.
When We Terminate the Surgery?
Correct Acidosis and Coagulopathy
Rewarm the patient
Optimize oxygenation and ventilation
Measure Intra abdominal pressure. ( 1A)
Part 2: Resuscitation(ICU)
Careful removal of packs
Inspection of all injuries
Control of bleeding points
Definitive GIT repair
Thorough washout
Avoid stomas and tube entrostomies if possible
Temporary vs. definitive closure
Part 3: (OR 2)
Temporary closure of the open abdomen is best accomplished : VAC Dressing. and a fascial tensioning.
Abdominal closure is best accomplished by hospital day 8 to reduce morbidity.
Strength of recommendation: C.
Barker D, Green J, Maxwell R, et al. J Am Coll Surg 2007;204:784–92. Offner P, de Souza A, Moore E, et al. Arch Surg 2001; 136: 676–81.
Garner G, Ware D, Cocanour C, et al. Am J Surg 2001; 182:630–8.
Part 4: Open Abdominal Wounds
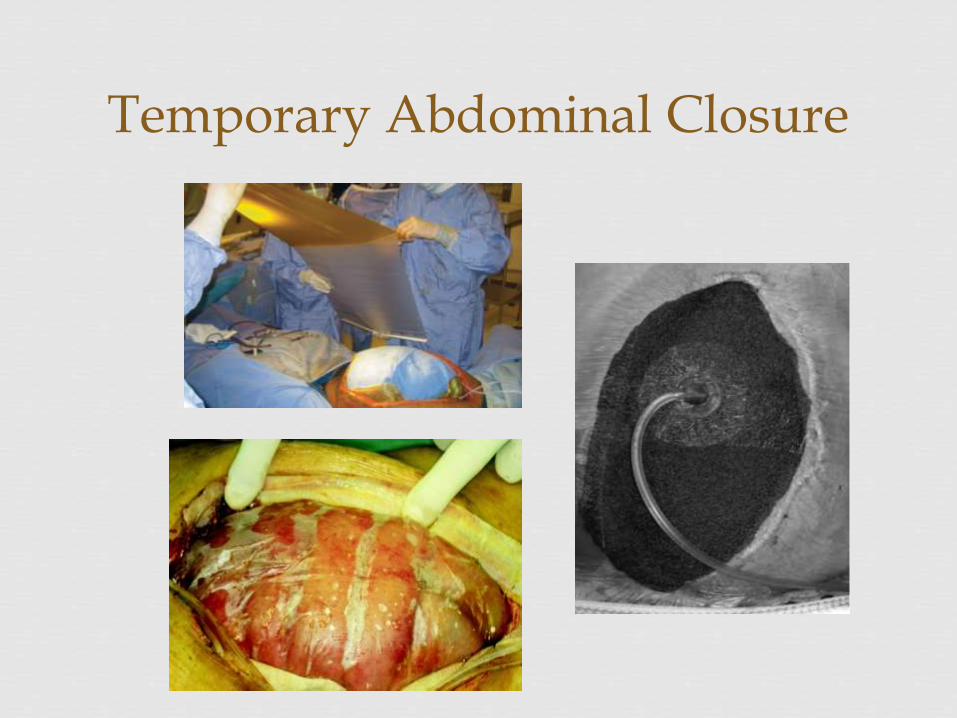
Temporary Abdominal Closure
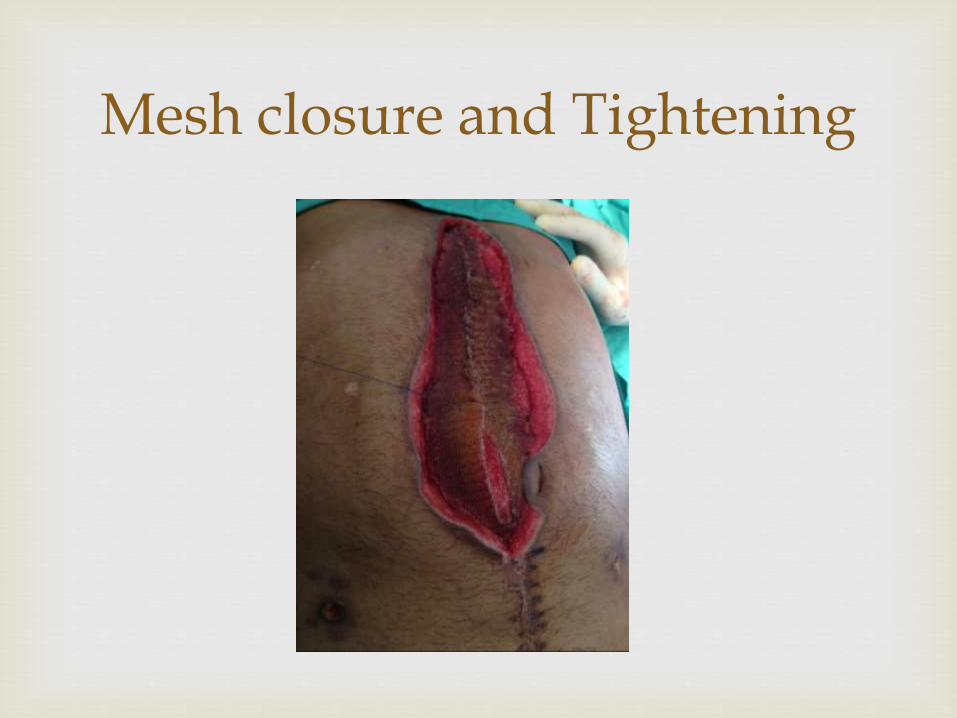
Mesh closure and Tightening

Definitive Repair

Outcome
Before After

Outcome
Before After

Outcome
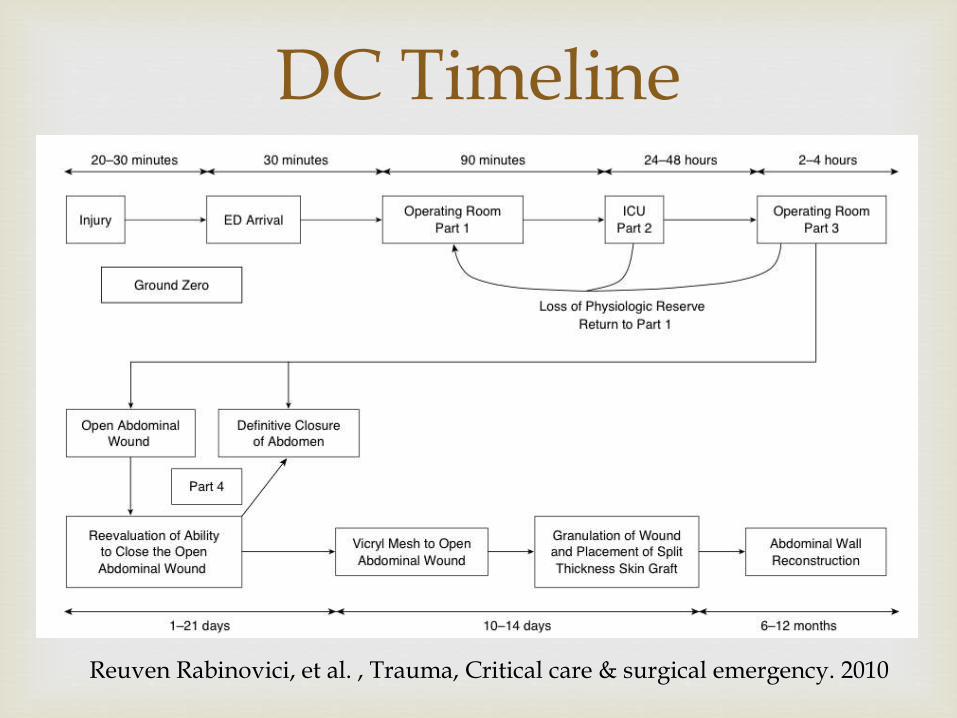
DC Timeline
Reuven Rabinovici, et al. , Trauma, Critical care & surgical emergency. 2010
Expected complication rate from damage control ranges from 25% to 40% .
The most common complications :
Intra-abdominal abscesses
Enterocutaneous fistulae.
Strength of recommendation: C.
Abikhaled J, Granchi T, Wall M, et al. Am Surg 1997; 63: 1109–12; discussion 1112–13.
Sharp K, Locicero R. Ann Surg 1992; 215: 467–74; discussion 474–5.
Complications of DC
The management of exsanguination requires leadership, prompt thinking and aggressive surgical intervention.
Delays in the decision to perform DC contribute to a higher morbidity and mortality.
DC is a vital part of the management of the multiply injured patient and should be performed before metabolic exhaustion.
Summary
