daniel - cfdna pe · t21 t18 t13 xo other sca ivf t21 t18 t13 xo other sca all pregnancies t21 t18...
TRANSCRIPT
23/02/20
1
Cell-free DNA testing for fetal aneuploidy&First trimester combined screening for preeclampsia
Daniel L RolnikMSc, MD, PhD
MFM Fellow – Monash UniversityDiploma in Fetal Medicine (FMF, UK)
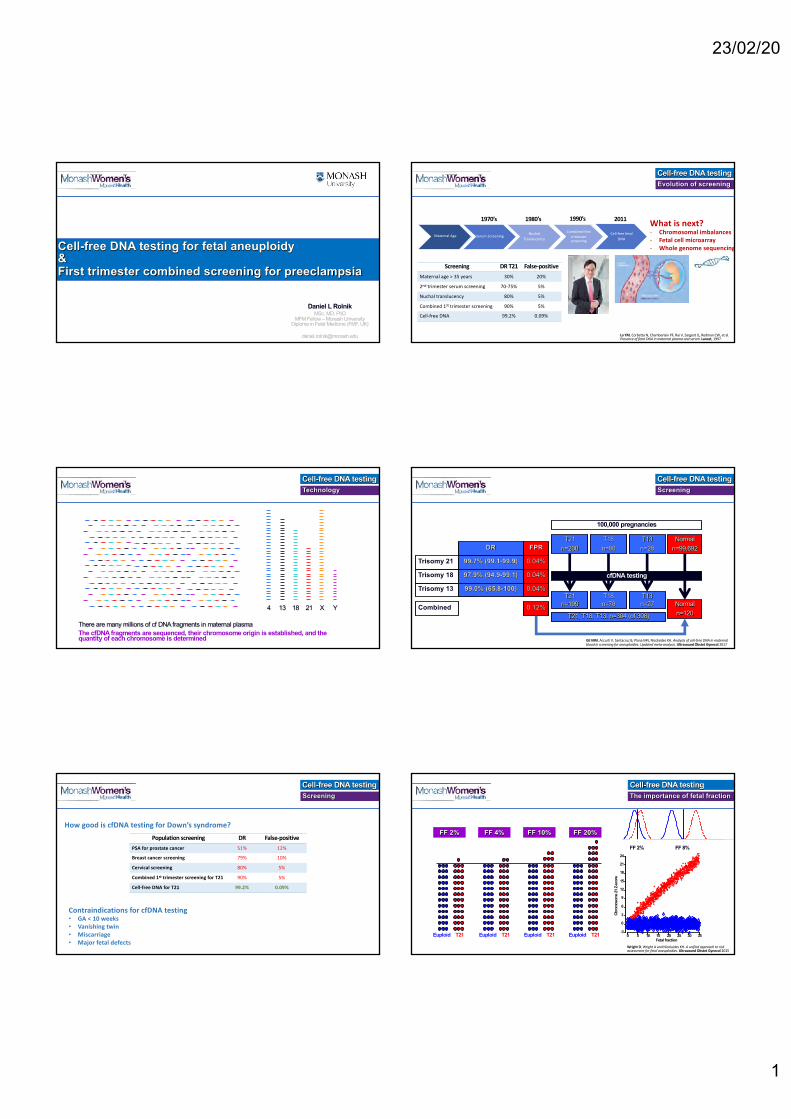
Evolution of screeningCell-free DNA testing
Serum ScreeningMaternal Age Nuchal Translucency
Combined first trimester screening
Cell-free fetal DNA
1970’s 1980’s 1990’s 2011 What is next?- Chromosomal imbalances- Fetal cell microarray- Whole genome sequencing
Screening DR T21 False-positiveMaternal age > 35 years 30% 20%
2nd trimester serum screening 70-75% 5%
Nuchal translucency 80% 5%
Combined 1st trimester screening 90% 5%
Cell-free DNA 99.2% 0.09%
Lo YM, Corbetta N, Chamberlain PF, Rai V, Sargent IL, Redman CW, et al. Presence of fetal DNA in maternal plasma and serum. Lancet, 1997.
TechnologyCell-free DNA testing
13 18 214 X Y
The cfDNA fragments are sequenced, their chromosome origin is established, and the quantity of each chromosome is determined
There are many millions of cf DNA fragments in maternal plasma
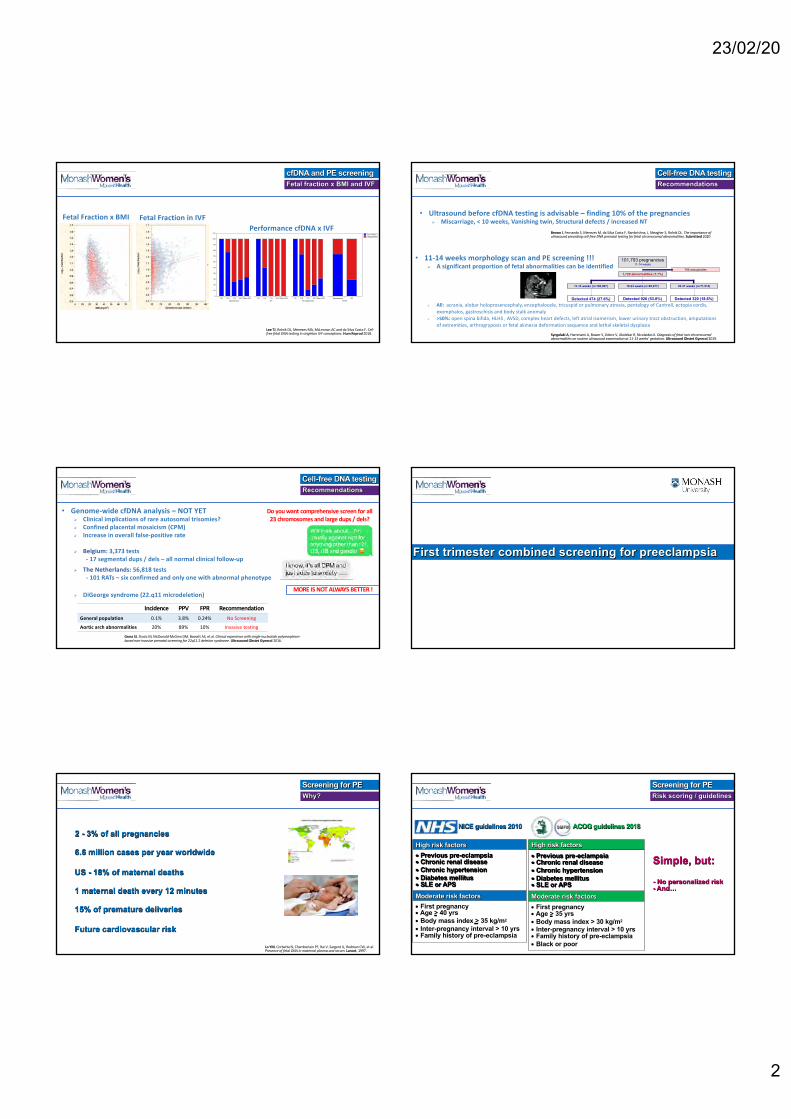
Screening
Cell-free DNA testing
Gil MM, Accurti V, Santacruz B, Plana MN, Nicolaides KH. Analysis of cell-free DNA in maternal blood in screening for aneuploidies: Updated meta-analysis. Ultrasound Obstet Gynecol 2017
0.04%
0.04%
FPRDR
Trisomy 21 99.7% (99.1-99.9)
Trisomy 18 97.9% (94.9-99.1)
0.04%Trisomy 13 99.0% (65.8-100)
100,000 pregnancies
T21n=200
Normaln=99,692
T18n=80
T13n=28
T21n=199 Normal
n=120
T18n=78
T13n=27
cfDNA testing
T21, T18, T13: n=304 (of 308) 0.12%Combined
ScreeningCell-free DNA testing
Population screening DR False-positive
PSA for prostate cancer 51% 12%
Breast cancer screening 79% 10%
Cervical screening 80% 5%
Combined 1st trimester screening for T21 90% 5%
Cell-free DNA for T21 99.2% 0.09%
How good is cfDNA testing for Down’s syndrome?
Contraindications for cfDNA testing• GA < 10 weeks• Vanishing twin• Miscarriage• Major fetal defects
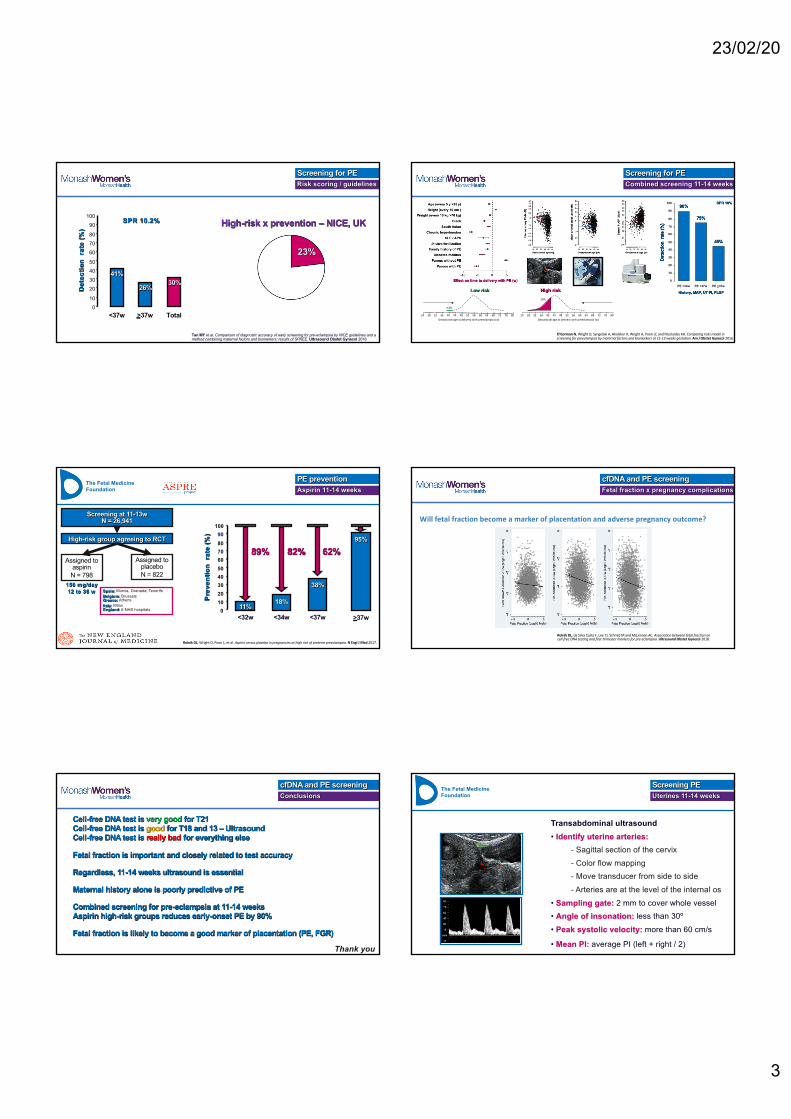
The importance of fetal fractionCell-free DNA testing
Wright D, Wright A and Nicolaides KH. A unified approach to risk assessment for fetal aneuploidies. Ultrasound Obstet Gynecol 2015
Fetal fraction
Chro
mos
ome 2
1 Z-sc
ore
-3
0
3
6
9
12
15
18
21
0 5 10 15 20 25 30 35
FF 8%FF 2%24
Euploid T21
FF 2%
Euploid T21
FF 4%
Euploid T21
FF 10%
Euploid T21
FF 20%
23/02/20
2
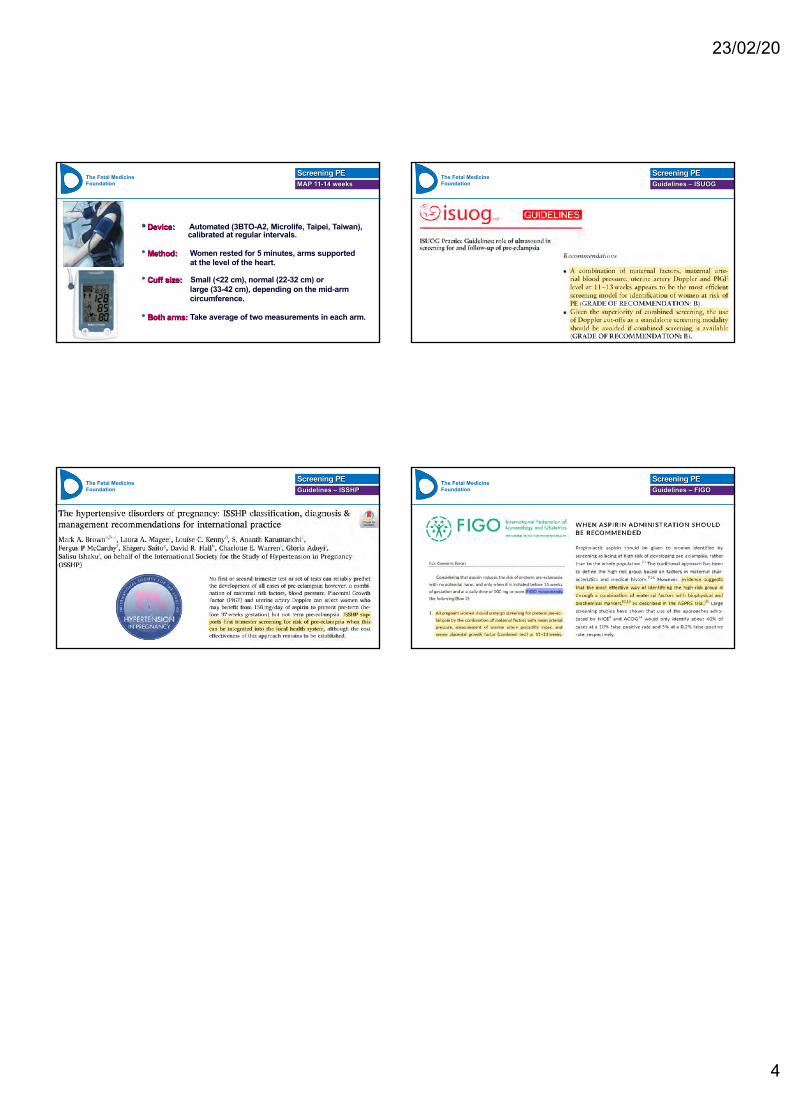
Lee TJ, Rolnik DL, Menezes MA, McLennan AC and da Silva Costa F. Cell-free fetal DNA testing in singleton IVF conceptions. Hum Reprod 2018.
Fetal fraction x BMI and IVFcfDNA and PE screening
Fetal Fraction in IVFFetal Fraction x BMI
True positiveFalse positive
%
0
10
20
30
40
50
60
70
80
90
100
110
SpontaneousT21 T18 T13 XO Other SCA
IVFT21 T18 T13 XO Other SCA
All pregnanciesT21 T18 T13 XO Other SCA
TOTALSpontaneous IVF
Performance cfDNA x IVF
RecommendationsCell-free DNA testing
• Ultrasound before cfDNA testing is advisable – finding 10% of the pregnanciesØ Miscarriage, < 10 weeks, Vanishing twin, Structural defects / increased NT
Brown I, Fernando S, Menezes M, da Silva Costa F, Ramkrishna, J, Meagher S, Rolnik DL. The importance of ultrasound preceding cell-free DNA prenatal testing for fetal chromosomal abnormalities. Submitted 2020
• 11-14 weeks morphology scan and PE screening !!!Ø A significant proportion of fetal abnormalities can be identified
Ø All: acrania, alobar holoprosencephaly, encephalocele, tricuspid or pulmonary atresia, pentalogy of Cantrell, ectopia cordis, exomphalos, gastroschisis and body stalk anomaly
Ø >50%: open spina bifida, HLHS , AVSD, complex heart defects, left atrial isomerism, lower urinary tract obstruction, amputations of extremities, arthrogryposis or fetal akinesia deformation sequence and lethal skeletal dysplasia
11-14 weeks (n=100,997) 18-24 weeks (n=99,677)
101,793 pregnancies11-14 weeks
30-37 weeks (n=71,514)
1,720 abnormalities (1.7%)796 aneuploidies
Detected 474 (27.6%) Detected 926 (53.8%) Detected 320 (18.6%)
Syngelaki A, Hammami A, Bower S, Zidere V, Akolekar R, Nicolaides K. Diagnosis of fetal non-chromosomal abnormalities on routine ultrasound examination at 11-13 weeks' gestation. Ultrasound Obstet Gynecol 2019.
RecommendationsCell-free DNA testing
• Genome-wide cfDNA analysis – NOT YETØ Clinical implications of rare autosomal trisomies?Ø Confined placental mosaicism (CPM)Ø Increase in overall false-positive rate
Ø Belgium: 3,373 tests- 17 segmental dups / dels – all normal clinical follow-up
Ø The Netherlands: 56,818 tests- 101 RATs – six confirmed and only one with abnormal phenotype
Ø DiGeorge syndrome (22.q11 microdeletion)
Do you want comprehensive screen for all 23 chromosomes and large dups / dels?
MORE IS NOT ALWAYS BETTER !
Incidence PPV FPR RecommendationGeneral population 0.1% 3.8% 0.24% No Screening
Aortic arch abnormalities 20% 89% 10% Invasive testing
Gross SJ, Stosic M, McDonald-McGinn DM, Bassett AS, et al. Clinical experience with single-nucleotide polymorphism-based non-invasive prenatal screening for 22q11.2 deletion syndrome. Ultrasound Obstet Gynecol 2016.
First trimester combined screening for preeclampsia
Why?Screening for PE
Lo YM, Corbetta N, Chamberlain PF, Rai V, Sargent IL, Redman CW, et al. Presence of fetal DNA in maternal plasma and serum. Lancet, 1997.
2 - 3% of all pregnancies
6.6 million cases per year worldwide
US - 18% of maternal deaths
1 maternal death every 12 minutes
15% of premature deliveries
Future cardiovascular risk
Risk scoring / guidelines
Screening for PE
High risk factors• Previous pre-eclampsia• Chronic renal disease• Chronic hypertension• Diabetes mellitus• SLE or APS
Moderate risk factors• First pregnancy•Age > 40 yrs• Body mass index > 35 kg/m2
• Inter-pregnancy interval > 10 yrs• Family history of pre-eclampsia
NICE guidelines 2010
High risk factors
• Previous pre-eclampsia• Chronic renal disease• Chronic hypertension• Diabetes mellitus• SLE or APS
Moderate risk factors
• First pregnancy•Age > 35 yrs• Body mass index > 30 kg/m2
• Inter-pregnancy interval > 10 yrs• Family history of pre-eclampsia• Black or poor
ACOG guidelines 2018SMFM
Simple, but:
- No personalized risk- And…
23/02/20
3
Risk scoring / guidelinesScreening for PE
Tan MY et al. Comparison of diagnostic accuracy of early screening for pre-eclampsia by NICE guidelines and a method combining maternal factors and biomarkers: results of SPREE. Ultrasound Obstet Gynecol 2018
23%
High-risk x prevention – NICE, UK
010
20304050
60
80
90100
70
Det
ectio
n ra
te (%
)
<37w >37w Total
SPR 10.2%
41%
26%30%
Combined screening 11-14 weeksScreening for PE
0
10
20
30
40
50
60
80
90
100
70
Det
ectio
n r
ate
(%)
History, MAP, UT PI, PLGF
PE <37w
75%
PE <34w
90%
PE >37w
45%
SPR 10%
Low risk
24 28 32 36 40 44 48 52 56 60 64 68 72 76 80Gestational age at delivery with preeclampsia (w)
0.5%
24 28 32 36 40 44 48 52 56 60 64 68 72 76 80Gestational age at delivery with preeclampsia (w)
High risk30%
O'Gorman N, Wright D, Syngelaki A, Akolekar R, Wright A, Poon LC and Nicolaides KH. Competing risks model in screening for preeclampsia by maternal factors and biomarkers at 11-13 weeks gestation. Am J Obstet Gynecol 2016.
The Fetal Medicine Foundation
Rolnik DL, Wright D, Poon L, et al. Aspirin versus placebo in pregnancies at high risk of preterm preeclampsia. N Engl J Med 2017.
0
10
20
30
40
50
60
80
90
100
70
Pre
ve
nti
on
ra
te (
%)
<34w
18%
38%
<37w
95%
>37w
82% 62%
<32w
11%
89%
High-risk group agreeing to RCT
Screening at 11-13wN = 26,941
Assigned to aspirinN = 798
Assigned to placeboN = 822
150 mg/day12 to 36 w Spain: Murcia, Granada, Tenerife
Belgium: Brussels Greece: AthensItaly: MilanEngland: 6 NHS hospitals
Aspirin 11-14 weeks
PE prevention
Rolnik DL, da Silva Costa F, Lee TJ, Schmid M and McLennan AC. Association between fetal fraction on cell-free DNA testing and first-trimester markers for pre-eclampsia. Ultrasound Obstet Gynecol 2018.
Fetal fraction x pregnancy complicationscfDNA and PE screening
Will fetal fraction become a marker of placentation and adverse pregnancy outcome?
Cell-free DNA test is very good for T21Cell-free DNA test is good for T18 and 13 – Ultrasound Cell-free DNA test is really bad for everything else
Fetal fraction is important and closely related to test accuracy
Regardless, 11-14 weeks ultrasound is essential
Maternal history alone is poorly predictive of PE
Combined screening for pre-eclampsia at 11-14 weeks Aspirin high-risk groups reduces early-onset PE by 90%
Fetal fraction is likely to become a good marker of placentation (PE, FGR)
ConclusionscfDNA and PE screening
Thank you
The Fetal Medicine Foundation
Transabdominal ultrasound• Identify uterine arteries:
- Sagittal section of the cervix- Color flow mapping- Move transducer from side to side- Arteries are at the level of the internal os
• Sampling gate: 2 mm to cover whole vessel• Angle of insonation: less than 30º• Peak systolic velocity: more than 60 cm/s
• Mean PI: average PI (left + right / 2)
Uterines 11-14 weeksScreening PE
23/02/20
4
The Fetal Medicine Foundation
• Device: Automated (3BTO-A2, Microlife, Taipei, Taiwan),calibrated at regular intervals.
•Method: Women rested for 5 minutes, arms supportedat the level of the heart.
• Cuff size: Small (<22 cm), normal (22-32 cm) orlarge (33-42 cm), depending on the mid-armcircumference.
• Both arms: Take average of two measurements in each arm.
MAP 11-14 weeks
Screening PE The Fetal Medicine Foundation Guidelines – ISUOG
Screening PE
The Fetal Medicine Foundation Guidelines – ISSHP
Screening PE The Fetal Medicine Foundation Guidelines – FIGO
Screening PE