department of emergency and organ transplantation · analisi multivariata cox covariate p-value si...
TRANSCRIPT


Department of Emergency and Organ TransplantationUrology, Andrology and Kidney Transplantation UnitU o ogy, d o ogy a d d ey a sp a tat o U t
University of Bari – Italy
La chirurgia conservativa nel carcinoma renale
Michele Battagliag

La rimozione chirurgica è il «gold standard» della
C i 2013 ll hi i d ll’RCC
terapia del tumore del rene
Controversie 2013 nella chirurgia dell’RCC
1 L bi i l Q d f l ?1. La biopsia renale. Quando e come farla? 2. Il problema della piccole masse renali: cosa fare ?
S h’ bi kill ?Sono anch’esse «big killer»? 3. Novità in tema di nefrectomia parziale ed i margini
hi i i i i i Q l è il bl ?chirurgici positivi. Qual è il vero «problema»?4. Il diabete e l’RCC5 L f t i di l i i ?5. La nefrectomia radicale in ogni caso?6. Sorveglianza attiva e trattamenti mininvasivi7 N ità i t di t i di t7. Novità in tema di terapia neoadiuvante8. Terapia adiuvante
SURGERYSURGERYSURGERYSURGERYPARTIAL NEPHRECTOMY: EXPANDED INDICATIONS
ABSOLUTE• Solitary kidney
ELECTIVE• Small lesions less than 4 cm (< 7 cm?)
• Bilateral renal mass• Severe renal failure
• Peripheral• Young health patients
RELATIVE• Controlateral kidney with pre-existing renal disease y p g(e.g. nephrolithiasis, recurrent pyelonephritis, ureteropelvic junction obstruction, reflux)
• Medical disease predisposing to renal failure (e.g. diabetes, hypertension)
• Known multifocality (e g genetic syndrome)• Known multifocality (e.g. genetic syndrome)

NEFRECTOMIA PARZIALE

NEFRECTOMIA PARZIALENEFRECTOMIA PARZIALE

NEFRECTOMIA PARZIALE

NEFRECTOMIA PARZIALE

Nefrectomia parziale laparoscopica

SOPRAVVIVENZA CANCRO SPECIFICASOPRAVVIVENZA CANCRO SPECIFICASOPRAVVIVENZA CANCRO SPECIFICASOPRAVVIVENZA CANCRO SPECIFICA
Sopravvivenza intero campione a 5 anni: 95,4% (95% CI 93,4-
97,4)
Sopravvivenza intero campione a 10 anni: 89% (95% CI 85-93)Sopravvivenza intero campione a 10 anni: 89% (95% CI 85 93)
8
1al
,4
,6
,8
Cum
. Sur
viva
NR
NP
0
,2
0 20 40 60 80 100 120 140Time
P-value: 0,1455
Time
NON SI OSSERVANO DIFFERENZE STATISTICAMENTE NON SI OSSERVANO DIFFERENZE STATISTICAMENTE
RILEVANTI TRA I GRUPPI NR E NPRILEVANTI TRA I GRUPPI NR E NPRILEVANTI TRA I GRUPPI NR E NPRILEVANTI TRA I GRUPPI NR E NP

SOPRAVVIVENZA CANCRO SPECIFICASOPRAVVIVENZA CANCRO SPECIFICA((stratificazionestratificazione per per gradogrado eded incidentalitàincidentalità))
GradoGrado IncidentalitàIncidentalità
4
,6
,8
1
m.S
urvi
val
Fuhrman 3-4
Fuhrman 1-2,6
,8
1
. Sur
viva
l.
Incidentale
Non incidentale
0
,2
,4
Cu
0 20 40 60 80 100 120 140Ti
P-value: 0,00440
,2
,4
Cum
0 20 40 60 80 100 120 140
Incidentale
P-value: 0,0082
Time 0 20 40 60 80 100 120 140Time
ANALISI MULTIVARIATA COX
1 -,128 ,982 -,131 ,017 ,8961 ,8801 -1,793 ,783 -2,291 5,249 ,0220 ,166
DF Coef Std. Error Coef/ES Chi-2 P-value Exp(Coef)
NP vs NRFhurman 1-2 vs 2-3 1 1,793 ,783 2,291 5,249 ,0220 ,166
1 1,277 ,739 1,729 2,989 ,0839 3,5871 -,031 ,017 -1,773 3,145 ,0762 ,9701 ,263 ,317 ,831 ,691 ,4059 1,301
Fhurman 1-2 vs 2-3Incidentalità:FGRDim.tumore
Likelihood Ratio 0,0025Significatività statistica P-value < 0,05
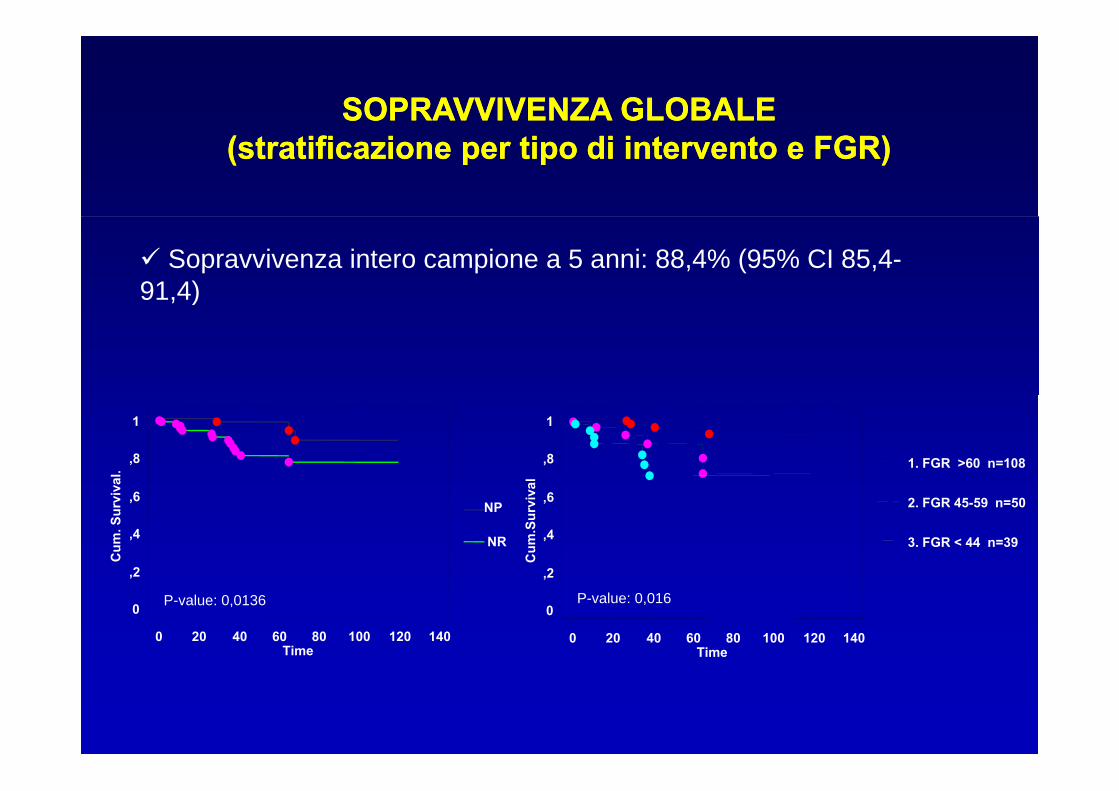
SOPRAVVIVENZA GLOBALESOPRAVVIVENZA GLOBALE((stratificazionestratificazione per per tipotipo di di interventointervento e FGR)e FGR)
Sopravvivenza intero campione a 5 anni: 88,4% (95% CI 85,4-91,4)
,8
1
val.
,8
1
al
1. FGR >60 n=108
,2
,4
,6
Cum
. Sur
viv
NR
NP
2
,4
,6
Cum
.Sur
viva
3. FGR < 44 n=39
2. FGR 45-59 n=50
0
,2
0 20 40 60 80 100 120 140Time
P-value: 0,01360
,2
0 20 40 60 80 100 120 140Time
P-value: 0,016

SOPRAVVIVENZA GLOBALESOPRAVVIVENZA GLOBALESOPRAVVIVENZA GLOBALESOPRAVVIVENZA GLOBALE((mortalitàmortalità da da tuttetutte le cause)le cause)
ANALISI MULTIVARIATA COXANALISI MULTIVARIATA COX
1 -,640 ,753 -,851 ,723 ,3950 ,527
1 917 506 1 813 3 286 0699 2 502
DF Coef Std. Error Coef/ES Chi-2 P-value Exp(Coef)
NP vs NR
Incidentalità 1 ,917 ,506 1,813 3,286 ,0699 2,502
1 -1,163 ,518 -2,243 5,029 ,0249 ,313
1 -,965 ,816 -1,183 1,400 ,2367 ,381
Incidentalità
Fuhrman 1-2 vs 3-4
Charlson Group 0-1 vs ≥2
1 ,248 ,207 1,200 1,439 ,2303 1,282
1 -,030 ,012 -2,567 6,590 ,0103 ,970
Dim.tumore
FGR
Significatività statistica P-value < 0,05
Likelihood Ratio <0,0001
N Engl J Med 2004;351:1296-305.

Confronto tra nefrectomia radicale e Nefrectomia parziale per tumori <4cm diametro
5616 Nefrectomia radicale Follow-up: 46 e 35 mesi2152 Nefrectomia parziale
R di l P i lRadicale ParzialeSopravvivenza globale 85.5% vs 88.9%
a 5 e 10 anni: 68.8% vs 70.9%a 5 e 10 anni: 68.8% vs 70.9%
Mortalità non cancro corr. 16.3% vs 11.7%a 5 e 10 anni: 31.6% vs 27.1%
P<0.001
Nefrectomia radicale determina una mortalità 1.23X maggiore della Nefrectomia parziale
Zini L, Cancer 2009

J Urol 2008;179:268

Thompson RH, J UROL 2008 ; 179:468
p 0.022
F 1 Overall survival in 327 patients younger than 65 years whoFIG 1. Overall survival in 327 patients younger than 65 years whounderwent PN or RN for solid renal mass 4 cm or less.
Ten-year overall survival rates were 82% and 93% for RN and PNTen-year overall survival rates were 82% and 93% for RN and PN, respectively (RR 2.16, 95% CI 1.12–4.19, p 0.022)
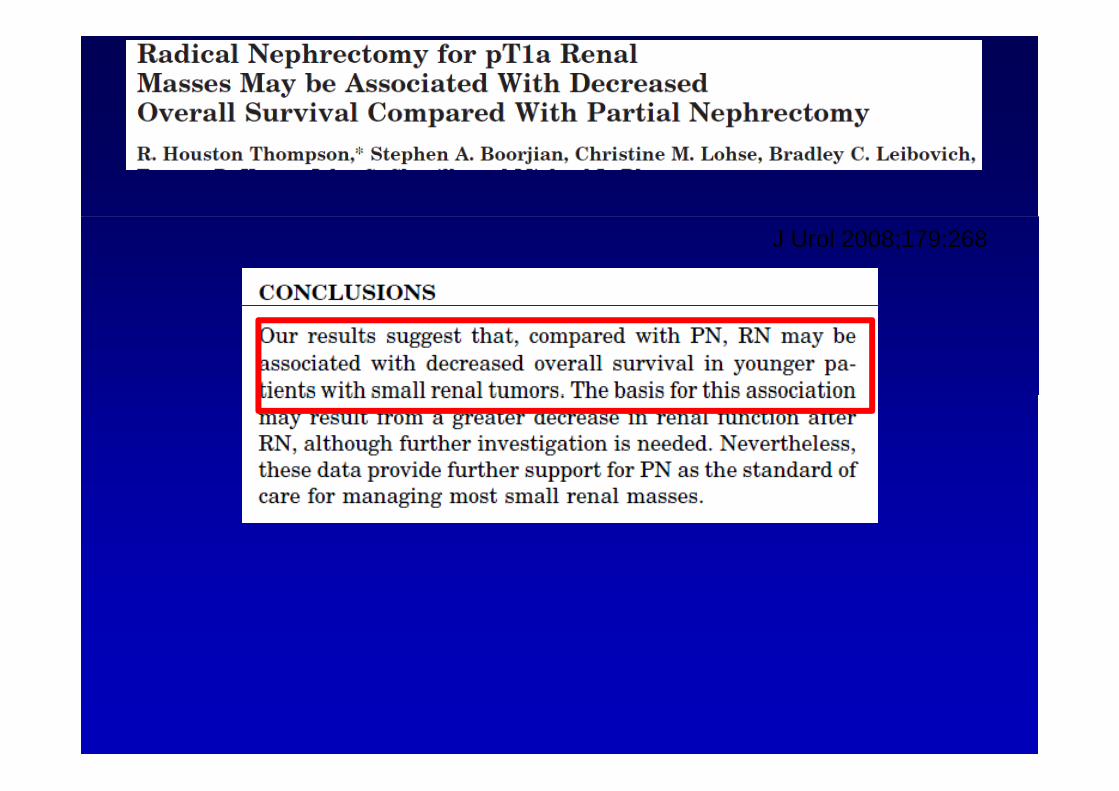
J Urol 2008;179:268

La nefrectomia radicale è un fattore di rischio significativo per lo sviluppo’i ffi idell’insufficienza renale…
No IRC (<45ml/min)
… e non … e non puòpuò essereessere considerataconsiderata piùpiù ilil trattamentotrattamento standard standard delledelle piccolepiccole lesionilesionirenalirenali
Huang WC, Lancet Oncol. 2006


UNIVERSITÀ DEGLI STUDI DI BARIÀFACOLTÀ DI MEDICINA E CHIRURGIA
DIPARTIMENTO DELL’EMERGENZA E DEI TRAPIANTI D’ORGANO (DETO)SEZIONE DI UROLOGIA I UNIVERSITARIA E TRAPIANTI DI RENE
Direttore: Prof. Michele Battaglia
L’IMPORTANZA DEL FILTRATO GLOMERULARE L’IMPORTANZA DEL FILTRATO GLOMERULARE
NELLA CHIRURGIA DEL CARCINOMA RENALE
STADIO pT1
Michele Battaglia

IL FILTRATO GLOMERULARE
Equazione abbreviata MDRD study:
GFR (ml/min/1.73 m2)= 186 x (sCr)-1,154 x (età)-0,203 x (0,742 nelle donne) x
(1,210 negli afroamericani)
Malattia renale cronica (CKD):Malattia renale cronica (CKD):
eGFR < 60 ml/min/1,73m^2 persistente da almeno 3 mesi con o senza un
danno renale documentabile.
un danno renale strutturale o funzionale dimostrabile attraverso:
- alterazioni degli esami di diagnostica per immagini- anomalie istologiche all’esame bioptico- alterazioni degli esami delle urine o del sangue
Queste modificazioni variabilmente associate fra loro devono essere
presenti per almeno 3 mesi con o senza una riduzione dell’ eGFRpresenti per almeno 3 mesi con o senza una riduzione dell eGFR.

IL FILTRATO GLOMERULARE

MATERIALI E METODI
U.O.C. Urologia 1 e Trapianto di Rene della AOU Policlinico – Università di Bari
• Dal 1997 al 2011 250 Nefrectomie per RCC stadio pT1:• Dal 1997 al 2011 250 Nefrectomie per RCC stadio pT1:
• Follow-up medio: 61,95 mesi (ultimo aggiornamento: Gennaio 2013)
• 134 NEFRECTOMIE PARZIALI
116ETÁ MEDIA: 61 (range 20-85)
• 116 NEFRECTOMIE RADICALI
Sottotipi
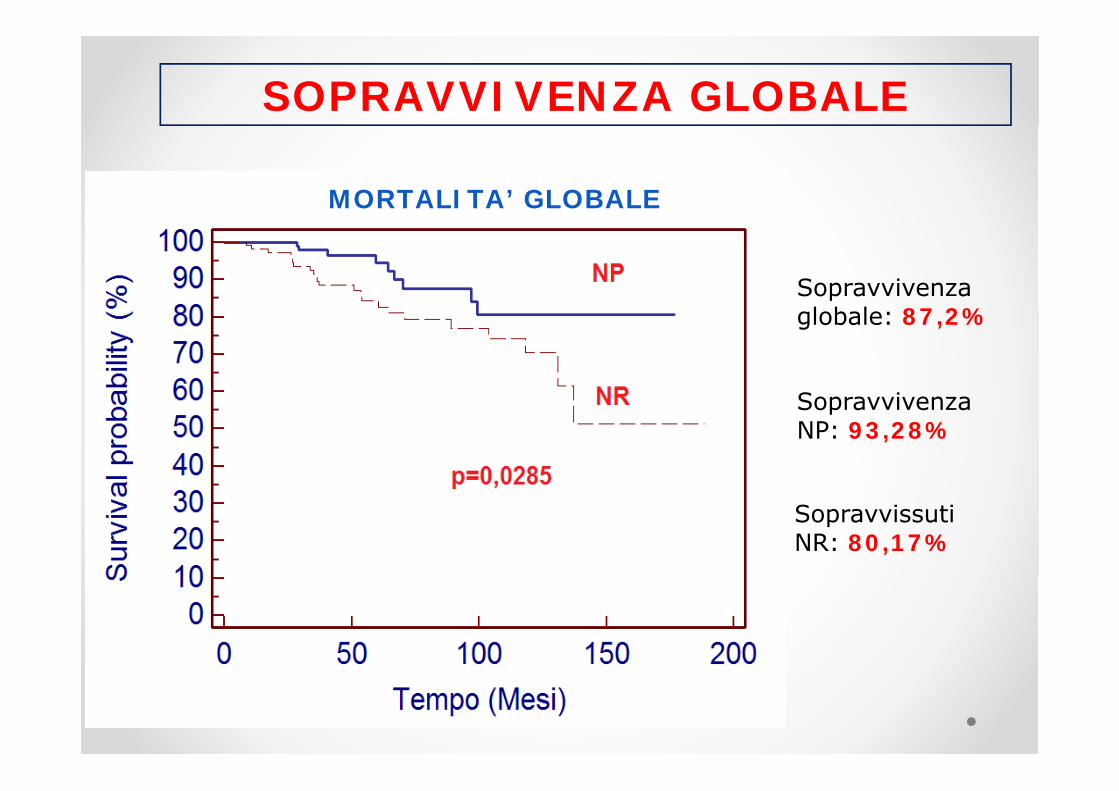
SOPRAVVIVENZA GLOBALE
MORTALITA’ GLOBALE
Sopravvivenza
S i
globale: 87,2%
Sopravvivenza NP: 93,28%
Sopravvissuti NR: 80,17%

SOPRAVVIVENZA CARDIOVASCOLARE
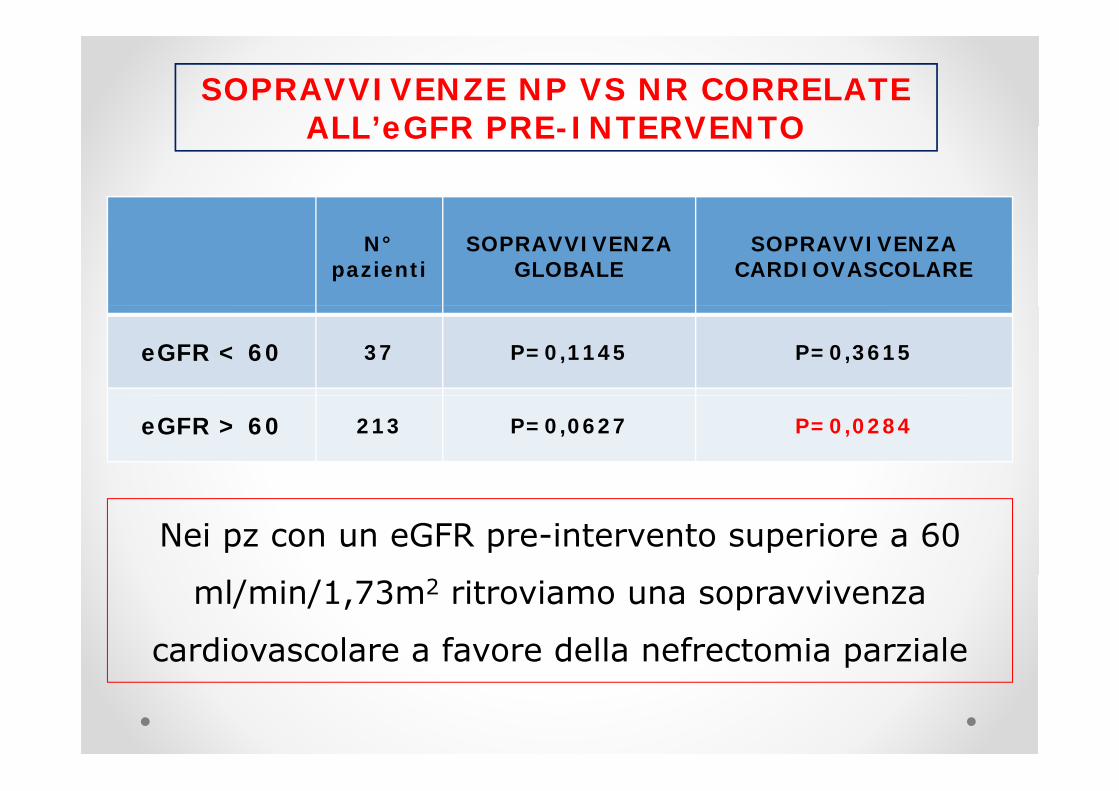
SOPRAVVIVENZE NP VS NR CORRELATE ALL’eGFR PRE-INTERVENTOALL eGFR PRE-INTERVENTO
N°pazienti
SOPRAVVIVENZA GLOBALE
SOPRAVVIVENZA CARDIOVASCOLARE
eGFR < 60 37 P=0,1145 P=0,3615
eGFR > 60 213 P=0,0627 P=0,0284
Nei pz con un eGFR pre-intervento superiore a 60
ml/min/1,73m2 ritroviamo una sopravvivenza
cardiovascolare a favore della nefrectomia parzialep

RIDUZIONE DEL FILTRATO GLOMERULARE A 12 MESI: Δ-eGFR (test t di student)A 12 MESI: Δ eGFR (test t di student)
∆= 8,3 ∆= 28,6
∆ 8,3
∆= 8,9 ∆= 4,6
p<0,0001 p<0,0001
p<0,0001 p<0,0663

Δ-eGFR a confronto(test t di student)
p=0 2254p<0 0001 p=0,2254p<0,0001
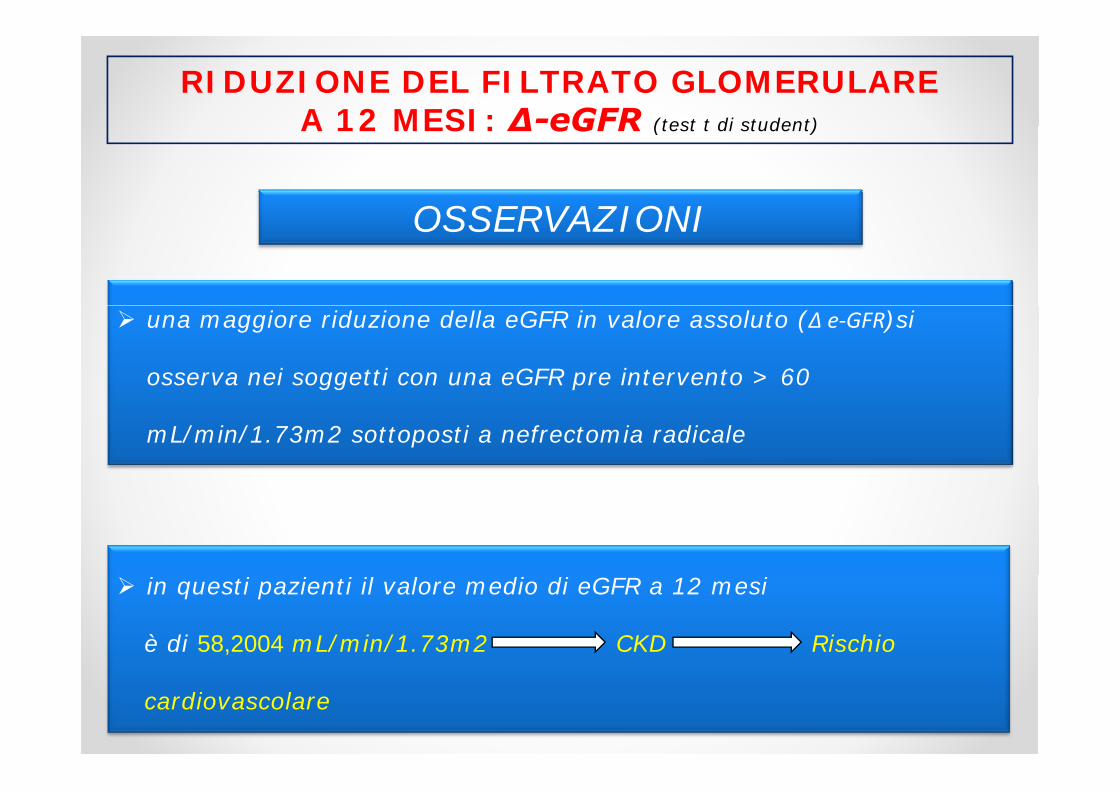
RIDUZIONE DEL FILTRATO GLOMERULARE A 12 MESI: Δ-eGFR (test t di student)A 12 MESI: Δ eGFR (test t di student)
OSSERVAZIONIOSSERVAZIONI
una maggiore riduzione della eGFR in valore assoluto (Δ e‐GFR)si
osserva nei soggetti con una eGFR pre intervento > 60
mL/min/1.73m2 sottoposti a nefrectomia radicale
in questi pazienti il valore medio di eGFR a 12 mesi
è di 58,2004 mL/min/1.73m2 CKD Rischio
cardiovascolare

SOPRAVVIVENZA GLOBALEANALISI MULTIVARIATA COX
COVARIATE P-VALUESignificance level: P = 0,0040
eGFRprechirurgico
0,0182
g ,
Grado 0,3470
Gruppi CharlsonRomano
0,0604 L’eGFR pre-chirurgico è f tt di i hi
Diabete 0,2111
un fattore di rischio indipendente per la mortalità globaleIpertensione 0,2721
Diametro MAX 0,8664
mortalità globale
Sesso 0,1514
Istotipo 0,9331
Nefrectomia Radicale
0,1085

SOPRAVVIVENZA CARDIOVASCOLARE SPECIFICAANALISI MULTIVARIATA COX
COVARIATE P-VALUE
Si ifi l l P 0 0141 eGFRprechirurgico
0,0389Significance level: P = 0,0141
Grado 0,8103
Gruppi CharlsonRomano
0,0237 L’eGFR pre-chirurgico è f tt di i hi
Diabete 0,8269
un fattore di rischio indipendente per la
mortalità Ipertensione 0,1459
Diametro MAX 0,5592
mortalità cardiovascolare
Sesso 0,4588
Istotipo 0,5632
Nefrectomia Radicale
0,1025

CONCLUSIONI
La nefrectomia parziale…
…GARANTISCE UNA MIGLIORE SOPRAVVIVENZA GLOBALE E
CARDIOVASCOLARE SPECIFICA RISPETTO ALLA NEFRECTOMIA RADICALE,
NEL TRATTAMENTO DEL RCC STADIO pT1
…RAPPRESENTA UN FATTORE PROTETTIVO NEI CONFRONTI DELLA
ÁMORTALITÁ CARDIOVASCOLARE E GLOBALE, SOPRATTUTTO NEI PAZIENTI
CON UNA BUONA FUNZIONALITÁ RENALE PRIMA DELL’INTERVENTO
…È IN GRADO DI RALLENTARE MA NON DI ARRESTARE IL DECORSO
DELLA MALATTIA RENALE CRONICA NEI PAZIENTI CON UNA DELLA MALATTIA RENALE CRONICA, NEI PAZIENTI CON UNA
FUNZIONALITÁ RENALE COMPROMESSA PRIMA DELL’INTERVENTO

CONCLUSIONI
L’e-GFR pre intervento…L e GFR pre intervento…
…PRE-INTERVENTO COSTITUISCE UN FATTORE DI RISCHIO
INDIPENDENTE PER LA MORTALITÁ CARDIOVASCOLARE PER LA
ÁMORTALITÁ GLOBALE
…DOVREBBE DIVENTARE UN PARAMETRO DI SCELTA PER IL
TRATTAMENTO CHIRURGICO DEI pT1 INDIPENDENTEMENTE DALLE TRATTAMENTO CHIRURGICO DEI pT1, INDIPENDENTEMENTE DALLE
DIMENSIONI DEL TUMORE
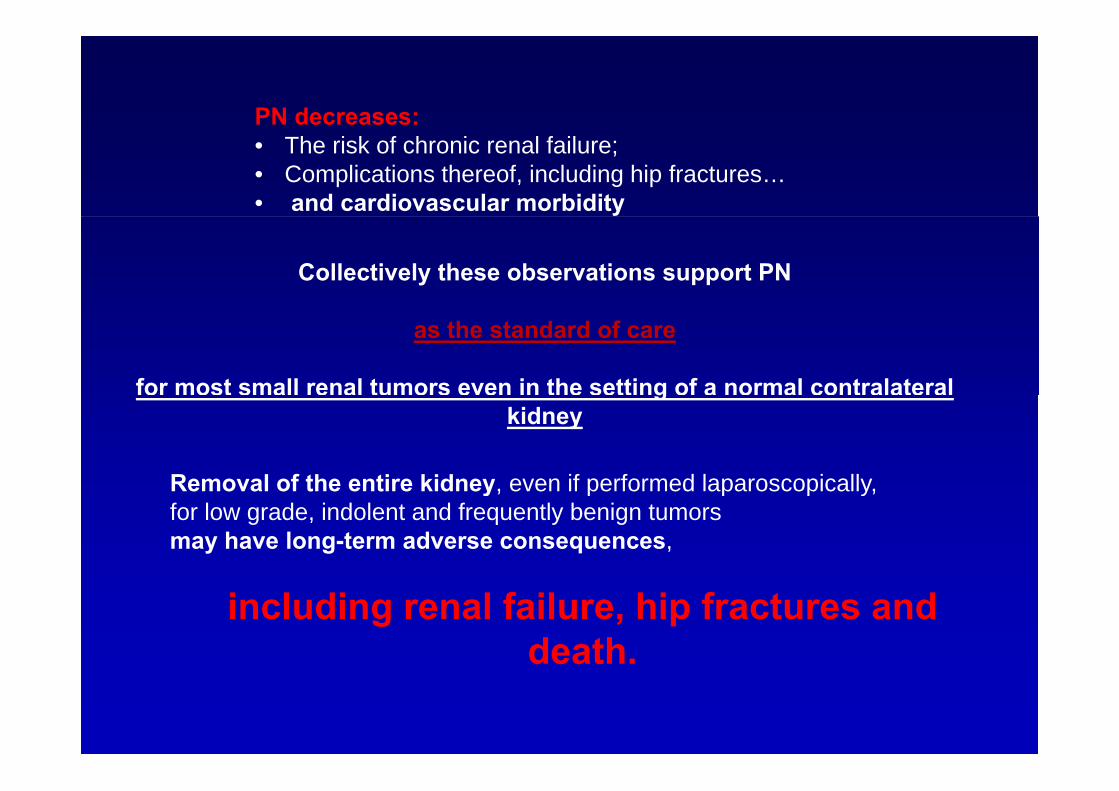
PN decreases:• The risk of chronic renal failure;• Complications thereof, including hip fractures…• and cardiovascular morbidity
Collectively these observations support PN
as the standard of care
for most small renal tumors even in the setting of a normal contralateral gkidney
Removal of the entire kidney even if performed laparoscopicallyRemoval of the entire kidney, even if performed laparoscopically, for low grade, indolent and frequently benign tumors may have long-term adverse consequences,
including renal failure, hip fractures and death.

La rimozione chirurgica è il «gold standard» della
C i 2013 ll hi i d ll’RCC
terapia del tumore del rene
Controversie 2013 nella chirurgia dell’RCC
1 L bi i l Q d f l ?1. La biopsia renale. Quando e come farla? 2. Il problema della piccole masse renali: cosa fare ?
S h’ bi kill ?Sono anch’esse «big killer»? 3. Novità in tema di nefrectomia parziale ed i margini
hi i i i i i Q l è il bl ?chirurgici positivi. Qual è il vero «problema»?4. Il diabete e l’RCC 5 L f t i di l i i ?5. La nefrectomia radicale in ogni caso?6. Sorveglianza attiva e trattamenti mininvasivi7 N ità i t di t i di t7. Novità in tema di terapia neoadiuvante8. Terapia adiuvante

n engl j med 364;9 march 3, 2011

DIABETES AND KIDNEY CANCER RISKDIABETES AND KIDNEY CANCER RISK
DOTTORATO DI RICERCA IN BIOTECNOLOGIE APPLICATE AI TRAPIANTI D’ORGANO E TESSUTI
Diabetes reduces survival in patients Diabetes reduces survival in patients ith l i l f th OGG1ith l i l f th OGG1with renal carcinoma: role of the OGG1 with renal carcinoma: role of the OGG1
andand tuberintuberinand and tuberintuberin
PhD Student:
Principal Investigators: Prof. Battaglia Michele e PhD Student:
Marica CarielloGiuseppe Grandaliano
CollaborationCollaboration:Prof. Giovanni PertosaDott. Antonia Loverre
Supervisor:Dott. Simona SimoneDott. Antonia Loverre
Dott. Monica Rutigliano

DIABETES AND CANCER RISKDIABETES AND CANCER RISK
Epidemiological studies have shown that patients with type Iand type II diabetes are at higher risk than the generalpopulation of developing cancer of the urinary tract liver
Adami HO et al. J Natl Cancer Inst, 1996
population of developing cancer of the urinary tract, liver,biliary tract, pancreas, colon, endometrium and kidney.
Adami HO et al. J Natl Cancer Inst, 1996Weiderpass E et al. Int J Cancer, 1997 Lindblad P et al. Diabetologia, 1999
Recently it has been demonstrated that diabetes is moderatelyi d i h d h f f h liassociated with death from cancers of the liver, pancreas, ovary,
colorectum, lung, bladder, and breast.Thompson A, et al. NEJM, 2011p , ,

CellularCellular and molecularand molecularCellularCellular and molecular and molecular mechanismsmechanisms byby whichwhichmechanisms mechanisms byby whichwhichdiabetesdiabetes associatesassociates totorenalrenal cellcell carcinoma carcinoma isis
kkunknownunknown..

DIABETESDIABETESHyperglycemia
Oxidative stress
Oxidative stressstressstress
PROTEIN DAMAGEPROTEIN DAMAGE LIPID ABNORMALITIESLIPID ABNORMALITIES DNA DAMAGEDNA DAMAGE
AGING STROKE
HEART DISEASE
CANCER
HEART DISEASE

DNA DAMAGE IN CARCINOGENESISDNA DAMAGE IN CARCINOGENESIS
Mutations in DNA repair genes are associated with cancer andMutations in DNA repair genes are associated with cancer andthe efficiency of DNA repair may determine the susceptibility tocarcinogens.
Loeb L. et al. Cancer Res., 1991
Wilson DM . et al. DNA Repair, 2007
8‐Oxo‐deoxyguanine (8‐Oxo‐dG) is a major form of oxidative DNAdamage and the ability of DNA adducts such as 8 oxo dG todamage and the ability of DNA adducts, such as 8‐oxo‐dG, tocause mutations is well documented.
Umemura T. et al. Carcinogenesis, 1990.Umemura T. et al. Carcinogenesis, 1990.
Wang D. et al. Mutat Res, 1998.

88‐‐oxoGoxoG‐‐DNA DNA glycosylaseglycosylase ((OGG1)OGG1)“DNA repair enzyme”“DNA repair enzyme”
Loss of heterozygosity (LOH) at the OGG1 allele was found in 85% of 99 human kidney clear
DNA repair enzymeDNA repair enzyme
cell carcinoma samples identifying loss of OGG1 function as a possible consequence of
multistep carcinogenesis in the kidney.
Audebert M. et al. Cancer Res., 2000.
Recent study shows that the Ser(326)Cys polymorphism of OGG1 is associated with Type 2
Diabetes in Mexican American families supporting a role for alterations of OGG1 in the
pathogenesis of Diabetes.
Thameem F. et al. Hum Hered., 2010

Mechanism of oxidative DNA damage in diabetes: Mechanism of oxidative DNA damage in diabetes: TuberinTuberininactivation and downregulation of DNA repair enzyme inactivation and downregulation of DNA repair enzyme
OGG1OGG1
GlGlucose PI3PI3--KK AktAktPP
ROSROSGlucoseHamartinHamartin
TuberinTuberinPP
Tuberin/mTOR pathway promotesapoptosis of tubular epithelial cellsin diabetes
OGG1OGG1
HamartinHamartin in diabetes.Velagapudi et al. JASN, 2011
88--OxodGOxodG
Tissue cell injury
DNA damageDNA damage
Tissue cell injury
S. Simone et al. Diabetes. 2008

PATIENTSPATIENTS462 patients treated with radical nephrectomy or nephron‐sparing surgery for
unilateral sporadic RCC between 1979 and 2009
CLINICAL FEATURESCLINICAL FEATURES PATHOLOGICAL FEATURES PATHOLOGICAL FEATURES
Age
(mean age 59.8 years)Histological subtype
Sex
(276 M 186 F)
TNM
Nuclear grade
ECOG performance status
Symptoms at presentation Coagulative necrosis
Sarcomatoid differentiationPresence of diabetes
76 pts (16.5%)
Sarcomatoid differentiation
11 type 1 DM 65 type 2 DM
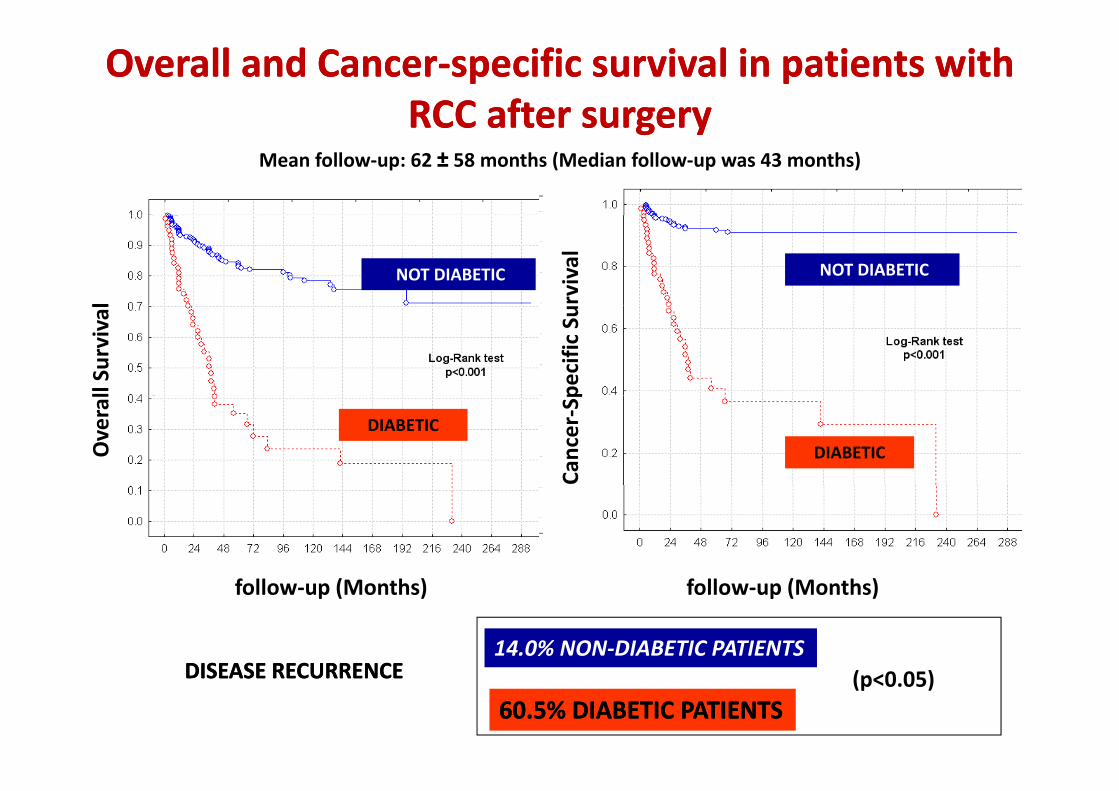
OverallOverall and and CancerCancer‐‐specificspecific survivalsurvival in patients in patients withwithRCCRCC afterafter surgerysurgery
Mean follow‐up: 62 ± 58 months (Median follow‐up was 43 months)
RCC RCC afterafter surgery surgery l rvivalNO DIABETES
NOT DIABETIC NOT DIABETIC
ll Survival
pecific
Su
Overal
Cancer‐Sp
DIABETESDIABETIC
DIABETIC
follow‐up (Months) follow‐up (Months)
DISEASE RECURRENCEDISEASE RECURRENCE14.0% NON‐DIABETIC PATIENTS
DISEASE RECURRENCEDISEASE RECURRENCE
60.5% DIABETIC PATIENTS60.5% DIABETIC PATIENTS(p<0.05)
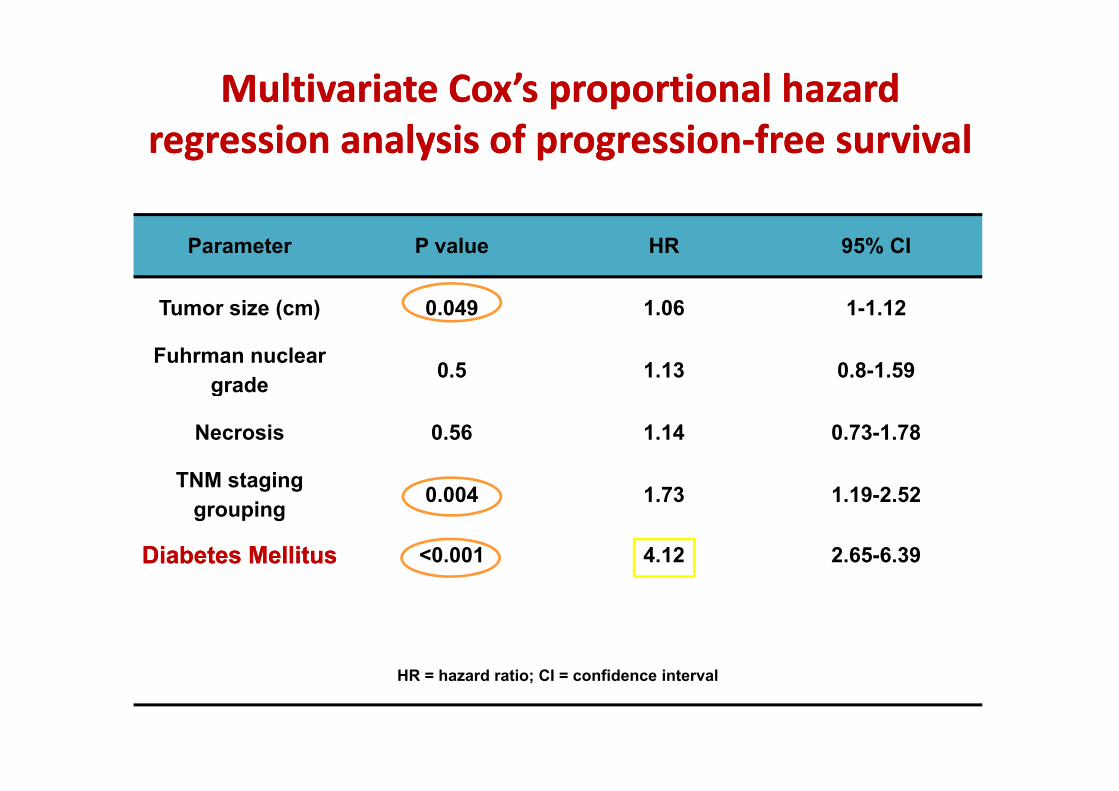
Multivariate Cox’s proportional hazard Multivariate Cox’s proportional hazard i l i f ii l i f i f i lf i lregression analysis of progressionregression analysis of progression‐‐free survivalfree survival
Parameter P value HR 95% CI
Tumor size (cm) 0 049 1 06 1 1 12Tumor size (cm) 0.049 1.06 1-1.12
Fuhrman nuclear grade 0.5 1.13 0.8-1.59g
Necrosis 0.56 1.14 0.73-1.78
TNM stagingTNM staging grouping 0.004 1.73 1.19-2.52
Diabetes MellitusDiabetes Mellitus <0.001 4.12 2.65-6.39
HR = hazard ratio; CI = confidence interval

Multivariate Cox’s proportional hazard Multivariate Cox’s proportional hazard regression analysis of cancerregression analysis of cancer specific survivalspecific survival
Parameter P value HR 95% CI
regression analysis of cancerregression analysis of cancer‐‐specific survivalspecific survival
a a ete a ue 95% C
Tumor size (cm) 0.028 1.09 1.01-1.18
Fuhrman nuclear grade 0.53 0.86 0.54-1.37
Necrosis 0 3 1 34 0 77 2 33Necrosis 0.3 1.34 0.77-2.33
TNM staging grouping 0.01 2.02 1.18-3.45g p g
Diabetes MellitusDiabetes Mellitus <0.001 4.9 2.8-8.58
HR = hazard ratio; CI = confidence interval

ConclusionsConclusionsDiabetes is associated with a higher rate of cancer‐relatedg
mortality and cancer recurrence in patients with of RCC
Tuberin phosphorylation and the loss of DNA repair enzyme
OGG1, observed in diabetic patients with RCC, may contribute to
progression of RCC in these patients.p g p

NEFRECTOMIA PARZIALE Stadio cT2E’ indicata?

J Urol 2010;183:983J Urol 2010;183:983
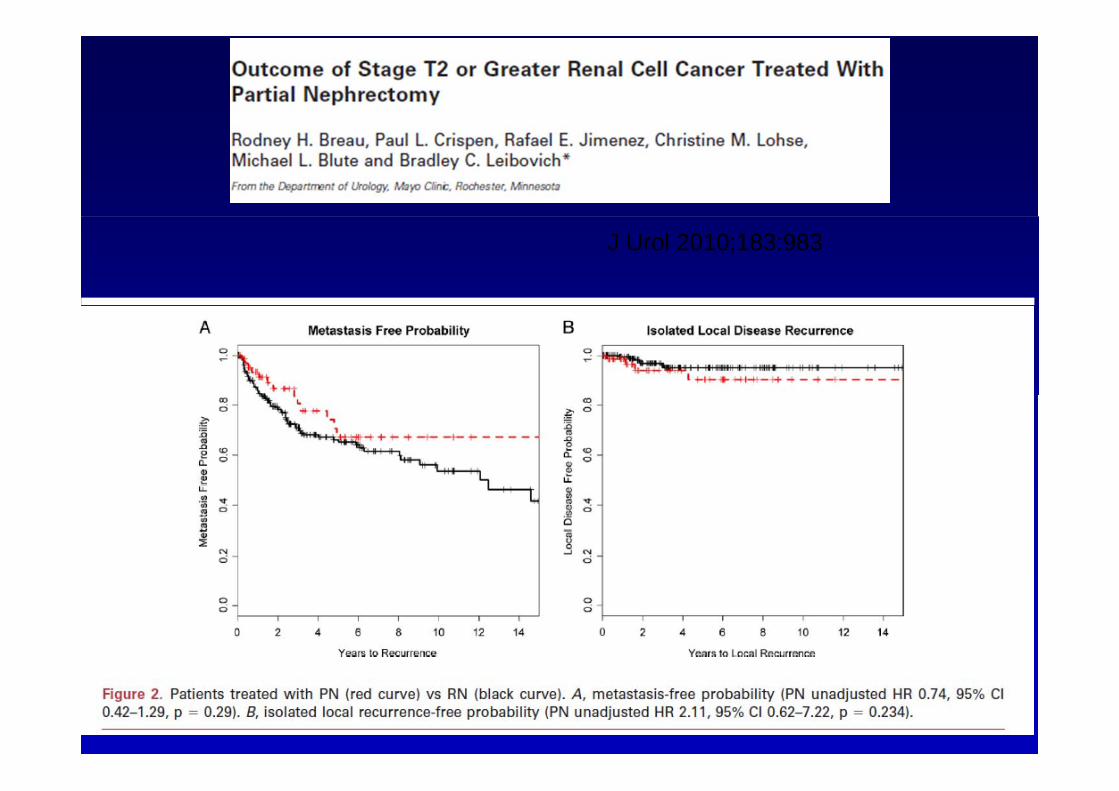
J Urol 2010;183:983

J Urol 2010;183:983

La rimozione chirurgica è il «gold standard» della
C i 2013 ll hi i d ll’RCC
terapia del tumore del rene
Controversie 2013 nella chirurgia dell’RCC
1 L bi i l Q d f l ?1. La biopsia renale. Quando e come farla? 2. Il problema della piccole masse renali: cosa fare ?
S h’ bi kill ?Sono anch’esse «big killer»? 3. Novità in tema di nefrectomia parziale ed i margini
hi i i i i i Q l è il bl ?chirurgici positivi. Qual è il vero «problema»?4. Il diabete e l’RCC5 L f t i di l i i ?5. La nefrectomia radicale in ogni caso?6. Sorveglianza attiva e trattamenti mininvasivi7 N ità i t di t i di t7. Novità in tema di terapia neoadiuvante8. Terapia adiuvante

Come si esegue?g

SURGERYSURGERY
PARTIAL NEPHRECTOMYFACTORS INFLUENCING OUTCOME:FACTORS INFLUENCING OUTCOME:
• TUMOR SIZE• MULTIFOCALITY• STAGE• POSITION• MARGINS
RISKS FACTORS FOR DISEASE RECURRENCEAFTER PARTIAL NEPHRECTOMY:
• TUMOR SIZE GREATER THAN 4 CM (> 7 CM?)• FUHRMAN NUCLEAR GRADE• MULTIFOCALITY• SYMPTOMATIC PRESENTATION• SYMPTOMATIC PRESENTATION
Nieder AM et al, 2003
[2] Novick AC, Campbell SC, Belldegrun A, et al. Guideline for managementof the clinical stage 1 renal mass (2009). American Urologicalo e c ca s age e a ass ( 009) e ca U o og caAssociation Web site. http://www.auanet.org/content/guidelinesand-quality-care/clinical-guidelines/main-reports/renalmass09.pdf.[3] Patard JJ, Shvarts O, Lam JS, et al. Safety and efficacy of partialnephrectomy for all T1 tumours based on an international multicenterexperience. J Urol 2004;171:2181–5.

THE standard of care for patients withlocalized renal malignancies is excision.In the last 2 decades nephronIn the last 2 decades nephronsparing surgery has emerged as an oncologicallyequivalent alternative to radicalnephrectomy in most cases of localizedp yRCC.1

Enucleazione vs EnucleoresezioneEnucleazione vs Enucleoresezione
Spessore margine peritumorale: 1 cm (Vermooten V., J Urol 1950; 64:200-8)
??
(Piper NY, Urology 2001;58:849-52)Non necessario (Piper NY, Urology 2001;58:849 52)
Nessuna differenza statisticamente sign. (Carini M, J Urol 2006;175:2022-6)
(with amedian follow-up of 51mo, the 5- and 8-yr CSS was(with amedian follow up of 51mo, the 5 and 8 yr CSS was85.1% and 81.6%, respectively. The local recurrence rate,however, was 4.5%)

SIA L’ENUCLEAZIONE CHE L’ENUCLEORESEZIONE POSSONO ESSERE ESEGUITI CON DIVERSE TECNICHE:
OPENLAPAROSCOPICAROBOT-ASSISTITA
Open vs laparoscopicaOpen vs laparoscopica
Nefrectomia radicale laparoscopica: p pnuovo standard of care?
D li USA 13 i d l i d i lDa un survey negli USA 13 anni dopo la sua introduzione, soloil 15% dei casi di tumore renale erano eseguiti con tecnicalaparoscopicalaparoscopica
In comparazione il 70% delle colecistectomie erano eseguiteper via laparoscopica solo dopo 4 anni l’introduzione dellatecnica
Rarità della procedura (10X meno frequente dellacolecistectomia) e maggior complessità rendono la curvacolecistectomia) e maggior complessità rendono la curvad’apprendimento una barriera alla sua diffusione
Miller DC, Cancer 2008 112:1708

La controversia più importante in tema di nefrectomia parziale, laddove possibile eseguirla, indipendentemente dalla via di accessoo delle altre modalità mininvasive di asportazione della neoplasia
è strettamente correlato alla persistenza dei
MARGINI CHIURGICI (PSM)
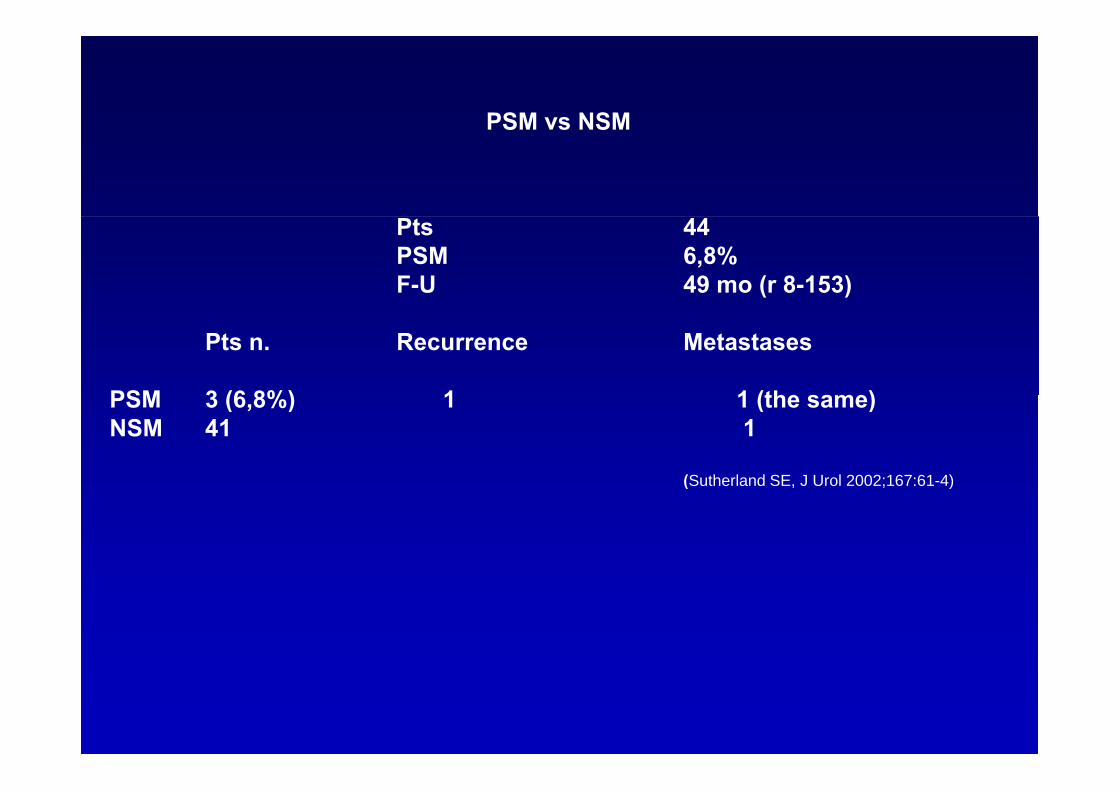
PSM vs NSMPSM vs NSM
Pts 44PSM 6,8%F-U 49 mo (r 8-153)
Pts n. Recurrence Metastases
PSM 3 (6 8%) 1 1 (the same)PSM 3 (6,8%) 1 1 (the same)NSM 41 1
(Sutherland SE, J Urol 2002;167:61-4)(Sutherland SE, J Urol 2002;167:61 4)

PSM vs NSMPSM vs NSM
Pts 777PSM 7%PSM 7%F-U 22 mo
RRecurrence
PSM 4%*
NSM 0,5%*
*Solo in soggetti con tumore ad alto potenziale di malignità (ccRCC,*Tumore del dotto di Bellini, presenza di elementi sarcomatoidi), p )
Know EO, BJU Int 2007;99:286-9)
(Khalifeh A, J Urol 2013;xxxxxx)
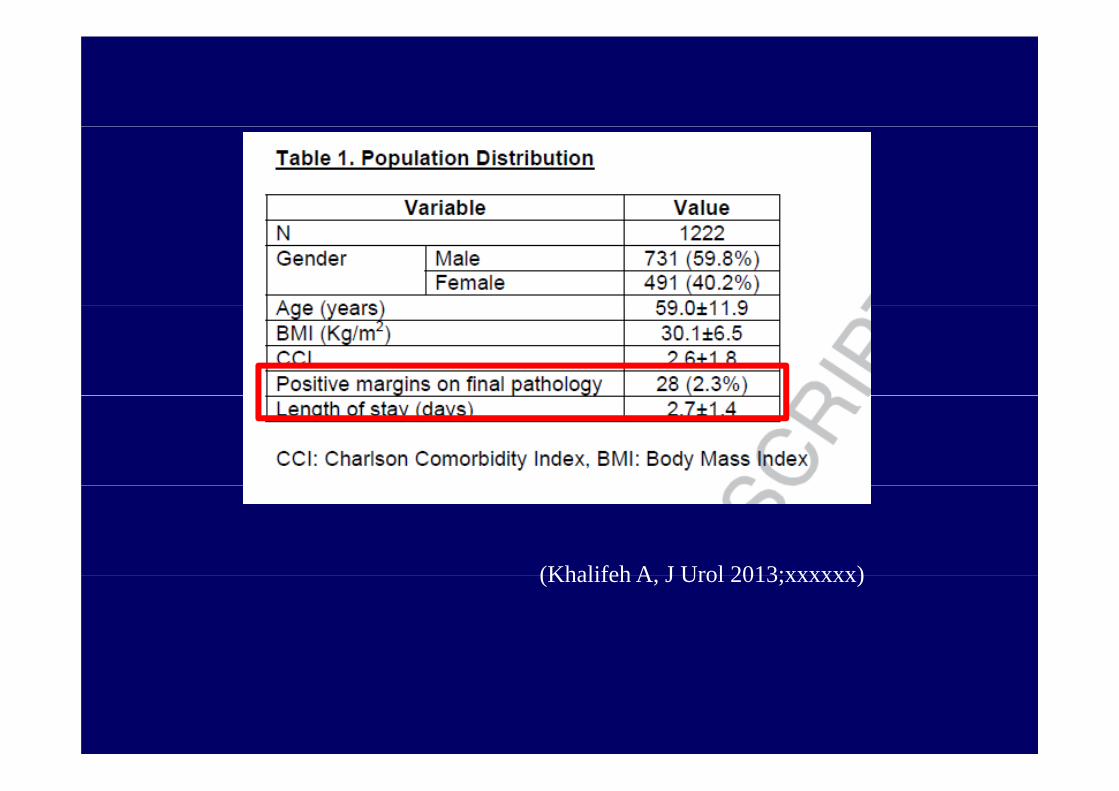
(Khalifeh A J Urol 2013;xxxxxx)(Khalifeh A, J Urol 2013;xxxxxx)

(Khalifeh A, J Urol 2013;xxxxxx)
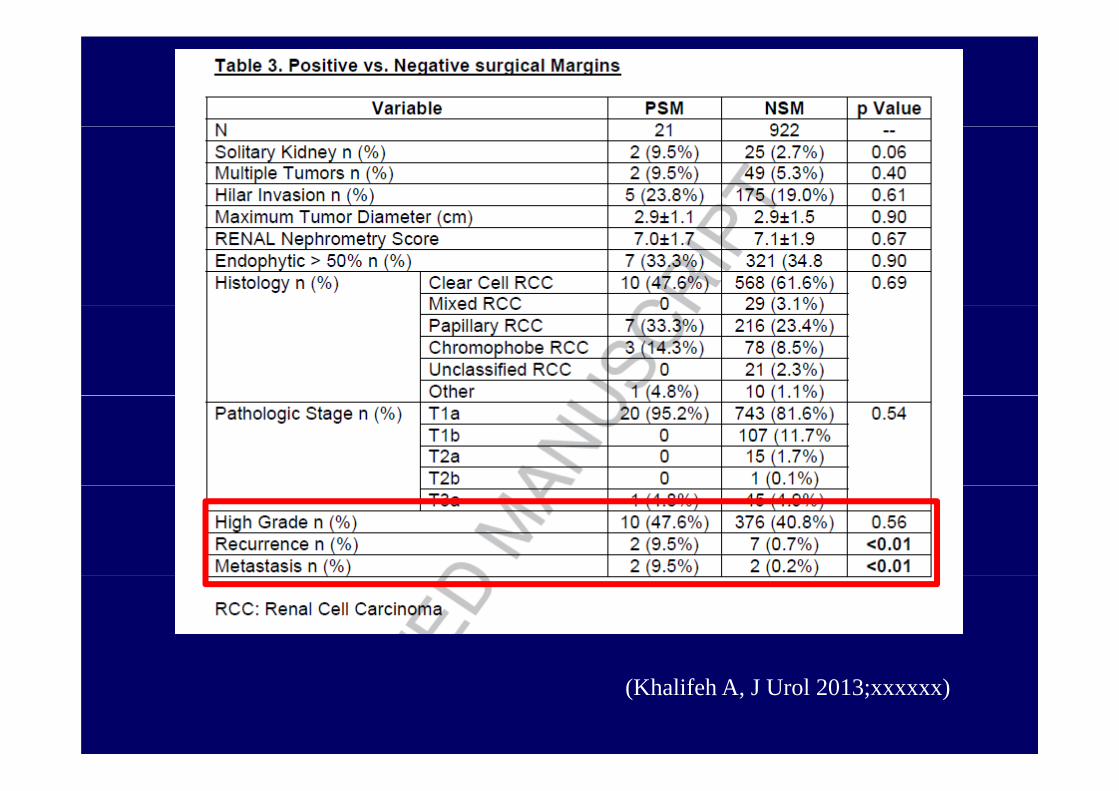
(Khalifeh A, J Urol 2013;xxxxxx)

J Urol 2008;179:2158–63.


CONCLUSIONI
• Non sempre è possibile garantire un margine di 1 cm• Alla luce delle evidenze riportate in letteratura, tale margine
non è necessario• Per tumori parailari, endofitici o centrali può essere sufficiente
la semplice enucleazione• I dati sul significato prognostico dei PSM sono controversi:a) In oncologia, è corretto avere NSMb) I margini intraoperatori ottenuti al congelatore, in genere, sono
random) I di PSM l’ i t t d ll l tt t è lc) In caso di PSM, l’orientamento della letteratura è la
=VIGILE ATTESA» ( nell’esperienza di tutti, la nefrectomia radicale successiva non trova tumore residuo!)

Novita’ in tema di nefrectomia parziale:
I DANNI DA ISCHEMIA RIPERFUSIONEI DANNI DA ISCHEMIA RIPERFUSIONE

Eur Urol 2010;58:340-345
…mandatorio minimizzare i tempidi ischemia calda durante la nefrectomia parziale!

Eur Urol 2011;59:128-134

D.E.T.ODipartimento dell’Emergenza e dei Trapianti d’Organo
Sezione di Urologia e Trapianto di Rene
Nefrectomia Nefrectomia segmentariasegmentariasegmentariasegmentaria
M. Battaglia
1. Imagingg g
• Anatomia• TAC con mdc• Ricostruzione 3D• Angio TAC / RM ?• Arteriografia tradizionale?Arteriografia tradizionale?
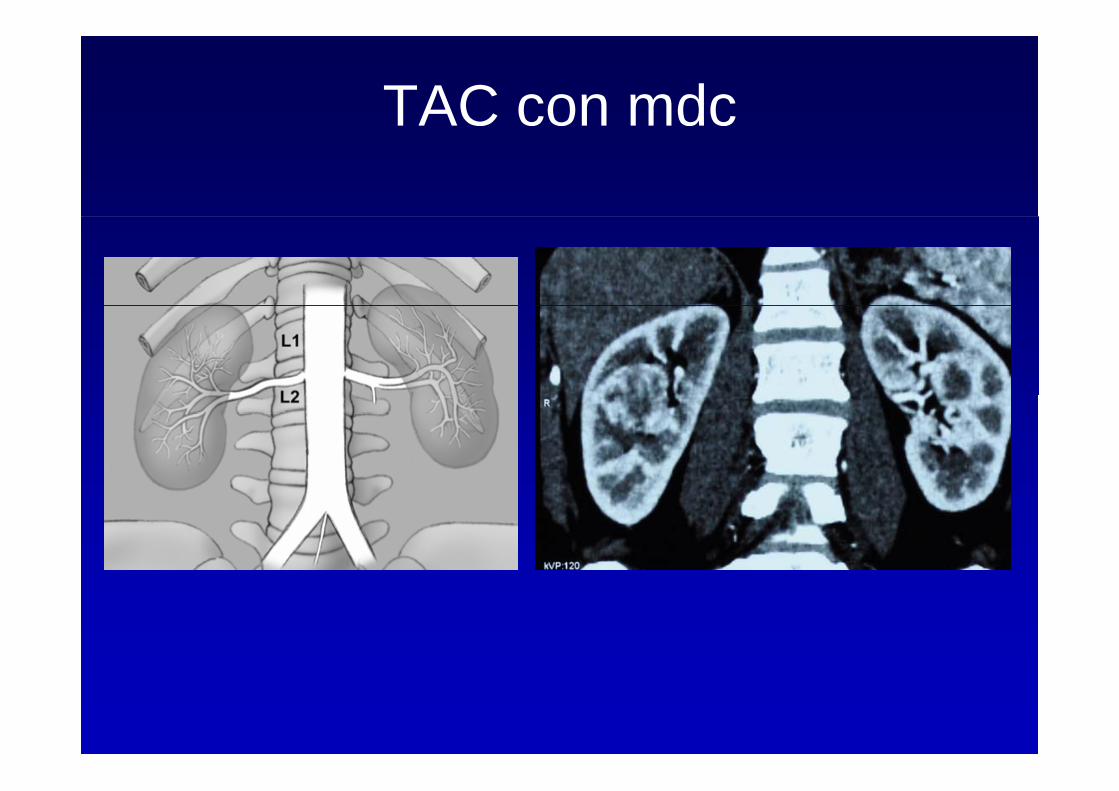
TAC con mdc


3 Segmento da cui origina3. Segmento da cui origina il tumoreil tumore
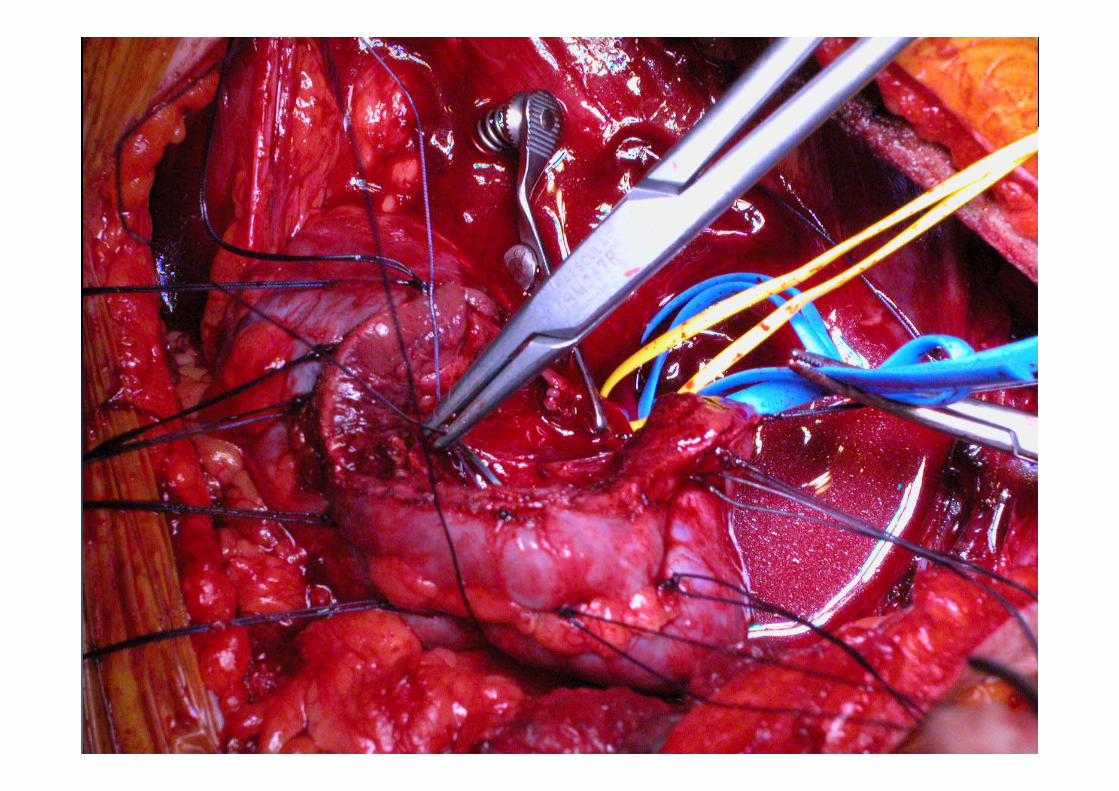
• Legatura del vaso con ischemia egatu a de aso co sc e asegmentaria
• Ischemia selettiva / super-selettivaIschemia selettiva / super selettiva


AsportazioneAsportazione neoformazioneneoformazione





Using a pig model, we found that a short period of warm ischemia followed by reperfusion led to myeloid cell infiltration of the kidney.
Conclusion: ischemia-reperfusion injury may cause an imbalance between i t ft l id d l t id DC hi h i ht b l t d t DGFintragraft myeloid and plasmacytoid DCs, which might be related to DGF and acute rejection.
Kidney International (2007) 72, 994–1003
Cosa è la “Zero Total Ischemia Time”Cosa è la Zero Total Ischemia Time
Chirurgia Nephron Chirurgia Nephron Sparing conChirurgia Nephron Sparing classica
Chirurgia Nephron Sparing con “Zero Total Ischemia Time”
Clamping completo dei Clamping selettivo deiClamping completo dei vasi ilari:
Evita il sanguinamento
Clamping selettivo dei vasi:
Evita il danno da Migliore escissione della massa eterologa
Complicanze:
ischemia/riperfusioneMigliore preservazione della funzionalità renalep
Danno da Ischemia/riperfusionePeggioramento della
della funzionalità renale soprattutto nei pazienti anziani
Peggioramento della funzionalità renale, progressiva nel tempo
MATERIALI E METODIMATERIALI E METODI
2010- Aprile 20122010 Aprile 201279 pazienti sottoposti a NP
40 NP tradizionale40 NP tradizionale39 NP “Zero Total Ischemia Time”
Età media: 60 anni (range: 20-83)Età media: 60 anni (range: 20 83)Follow up medio: 7,7 mese (range: 1-26)eFGR calcolato con l’EquazioneeFGR calcolato con l Equazione abbreviata MDRD study:
FGR(ml/min/1 73m2)=186 x (sCr)-1,154 x (età)-0,203 x (0 742 nelleFGR(ml/min/1,73m )=186 x (sCr) , x (età) , x (0,742 nelle donne) x (1,210 negli afroamericani)

NP tradizionale NP “Zero Total Ischemia time” P-Value
Di i i 3 14DimesioniTumore
3,14 cm(range 1,50-
6,50)
3,75 cm (range 1-7) 0,102
eFGR preintervento
98,97 ml/min(range 36,16-
177 33)
109,25 ml/min(range 49,03-
201 85)0,177
177,33) 201,85)eFGR postintervento
86,87 ml/min (range 29,60-
99,44 ml/min (range 36,89- 0,092
163,86) 207,94)eFGR Follow up 87,79 ml/min
(range 30 l53-102,85 ml/min(range 53 89- 0 106(range 30,l53-
179,08)(range 53,89-
157,81)0,106
Diff. eFGRpre/post
intervento13,1% 9,3% 0,372
Diff eFGR preDiff. eFGR preintervento/Follow
up12,2% 6,4% 0,570

CONCLUSIONICONCLUSIONI
La tecnica “Zero Total Ischemia Time” tt di l d l f i litàpermette di salvaguardare la funzionalità
renale meglio della tecnica classica poiché si evita di ischemizzare il parenchima renale in totoparenchima renale in toto
Questi primi risultati sono incoraggiantiQuesti primi risultati sono incoraggiantie necessitano di ulteriori studi diconfermaconferma.

5. Complicanzep
Emorragia• Emorragia• Stenosi ureterali alteStenosi ureterali alte• Esclusione rene• Insufficienza renale
Formazione di fistole• Formazione di fistole urinarieurinarie
Ematoma

Ematoma

Stenosi ureterale alta
Risk factors:• Tumour complexityp y• Imperative indications• Mid- or lower pole locationp• Postoperative urinary leak• HaemorrhageHaemorrhage
Necessità di posizionamento di
stentstent

ConclusioniConclusioni• Serve un’ ottima conoscenza dell’anatomia chirurgica e
vascolare del rene• L’imaging, nonostante i progressi, va opportunamente
applicata ed interpretata! • Necessità di esperti di riferimento• Bisogna sempre preservare quanto più possibile massaBisogna sempre preservare quanto più possibile massa
nefronica (riduce il rischio di mortalità non cancro correlata)
• Attenzione alle complicanze

NEFRECTOMIA PARZIALE

NEFRECTOMIA PARZIALE

Nefrectomia parziale laparoscopica

ConclusioniConclusioni• Serve un’ ottima conoscenza dell’anatomia chirurgica e
vascolare del rene• L’imaging, nonostante i progressi, va opportunamente
applicata ed interpretata! • Necessità di esperti di riferimento• Bisogna sempre preservare quanto più possibile massaBisogna sempre preservare quanto più possibile massa
nefronica (riduce il rischio di mortalità non cancro correlata)
• Attenzione alle complicanze

Grazie perGrazie per l’attenzion
e
Henry Gervex 1887 - Museo d'Orsay Parigi Il chirurgo Jules Louis Pean opera presso il San Louis Hopital Hanno Collaborato:
Dr. C. MiacolaDr. M. Tedeschi Made with a Mac

The study shows that:• small RCCs have an aggressive potential, resulting in lymph node and distal
metastases• even in a 1‐ to 2‐cm tumor
• 11% of 3‐ to 4‐cm tumors (T1a) had either lymph node or distant metastases.
• In total, 7%of all RCCs <4 cm had distant metastases
• Only in tumors <1 cm were neither lymph node nor distant metastases observed.