dra.casinello farmacos antiplaquetarios
TRANSCRIPT

AntiagregantesAntiagregantes y sangrado y sangrado perioperatorioperioperatorio
Dra. C. CassinelloHospital Universitario “Miguel Servet”
Zaragoza 2008
Antiagregantes y sangrado perioperatorio
• Sangrado asociado a AAP• Modelo celular de hemostasia• Aumento de trombosis perioperatoria• Del estudio clínico del sangrado perioperatorio al
NE – AAS– Clopidogrel– AAS + clopidogrel– I- GP IIb-IIIa– Flurbiprofeno-dexibuprofeno
• E. de cohortes prospectivo, Miguel Servet– Balance de riesgos hemorrágico y trombótico
• Antes y después de la implantación de un protocolo de sustitución por AAS 100mg

Sangrado mayor:Sangrado mayor:2 Meta2 Meta--ananáálisis: 467.532 pacienteslisis: 467.532 pacientes
NE: 1a NE: 1a
Serebruany VL. Risk of bleeding complications with antiplatelet agents: meta-analysis of 338.191 patients enrolled in 50 randomizedcontrolled trials. Am J Hematol 2004; 75: 40-47Serebruany VL. Bleeding risks of combination vs. single antiplatelet therapy: a meta-analysis of 18 randomized trials comprising129,314 patients. Fundam Clin Pharmacol 2008
6%6%
5%5%
4%4%
3%3%
2%2%
1%1%
AAS < 100mg13.337
AAS100-325mg
43.489
AAS>325mg
1.409
Dipiridamol
3.304
Clopidogrel
18574
AAS +Clopidogrel
49201
I-GP IIB/IIIaIV
22.501
1.47
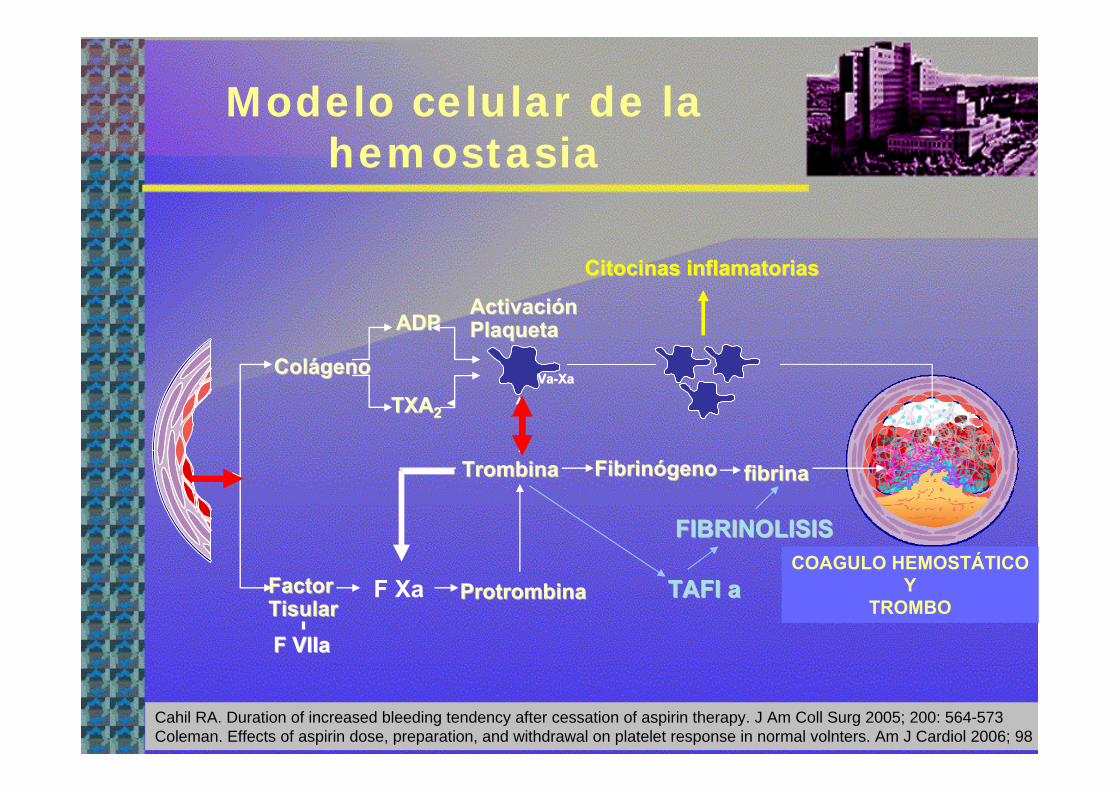
Modelo celular de la hemostasia
TAFI aTAFI a
FIBRINOLISISFIBRINOLISIS
ColColáágenogeno
FactorFactorTisularTisular
TrombinaTrombina
ActivaciActivacióónnPlaquetaPlaqueta
ProtrombinaProtrombina
ADPADP
TXATXA22
TROMBOTROMBO
FibrinFibrinóógenogeno fibrinafibrina
F XaCOAGULO HEMOSTÁTICO
YTROMBO
F F VIIaVIIa
VaVa--XaXa
CitocinasCitocinas inflamatoriasinflamatorias
Cahil RA. Duration of increased bleeding tendency after cessation of aspirin therapy. J Am Coll Surg 2005; 200: 564-573Coleman. Effects of aspirin dose, preparation, and withdrawal on platelet response in normal volnters. Am J Cardiol 2006; 98

Agregación y activación plaquetaria
GpGp IIbIIb--IIIaIIIa
ADPADP
AAAA
TXA TXA 22
TXA 2TXA 2ADPADP
AgregaciAgregacióón y activacin y activacióónn
TX ATX A22
ADPADP
ColagenoColagenoAdrenalinaAdrenalinaTrombinaTrombina


Hiperadhesividad plaquetariaAgregación plaquetaria
ADP
< Fibrinolisis> I-activador plasminógeno
S. Inflamatorio sistémico:*PCR*IL-6, IL-8 (Citocinas proinflamatorias) *Células: LPMN, monocitos
Alteraciones hemodinámicas*Cizallamiento sobre el vaso*E.hiperadrenérgico
VC, agregación plaquetaria
Samana Ch M. Perioperative activation of hemostasis in vascular surgerypatients Anesthesiology 2001; 94: 74-78

La decisión de mantener, suspender o sustituir un AAP
para cirugía
AAPPacienteCirugía
del sangradoy sus secuelas
del r trombóticoy sus secuelas

Burger et alAAS
• Metaanálisis cirugía no cardíaca:–49.590 pacientes
• 14.981: con AAS• 34.609: sin AAS
– AAS continuación conlleva 1.5 veces1.5 veces riesgo de sangrado perioperatorio (ic 95%: 1-2.5)
» Sin complicaciones por la severidad del sangrado
Burger W, Chennitus JM, Kneissl GD, Rucker GLow-dose aspirin For secondary cardiovascular prevention- cardiovascular risks after its Perioperative withdrawal versus bleeding risks with itscontinuation-review and meta-analysis. J Intern Med 2005; 257: 399-414.

Discontinuar AAS x > 3eventos trombóticos
3001003010520.50.20.1
1,82
2,4
SCA
By pass c
stent 89,78
Riesgo de SCAOR = 3,14,
IC 95% (1,75-5,61)
Biondi-Zoccai et al. A systematic review and meta-analysis on the hazards of Disconti-nuing or notadhering to aspirin among 50.279 patients at risk for coronary disease. Eur heart J 2006; 27: 2667-2674
9 meses stent FA
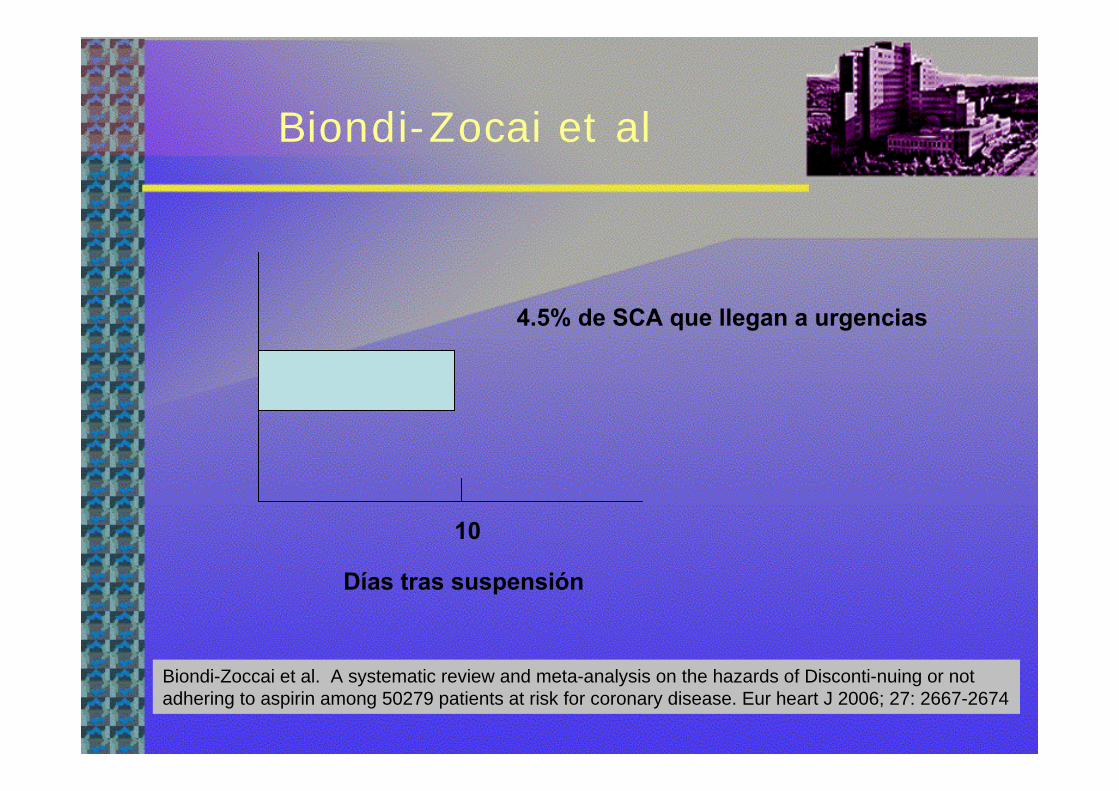
Biondi-Zocai et al
Días tras suspensión
10
4.5% de SCA que llegan a urgencias
Biondi-Zoccai et al. A systematic review and meta-analysis on the hazards of Disconti-nuing or notadhering to aspirin among 50279 patients at risk for coronary disease. Eur heart J 2006; 27: 2667-2674
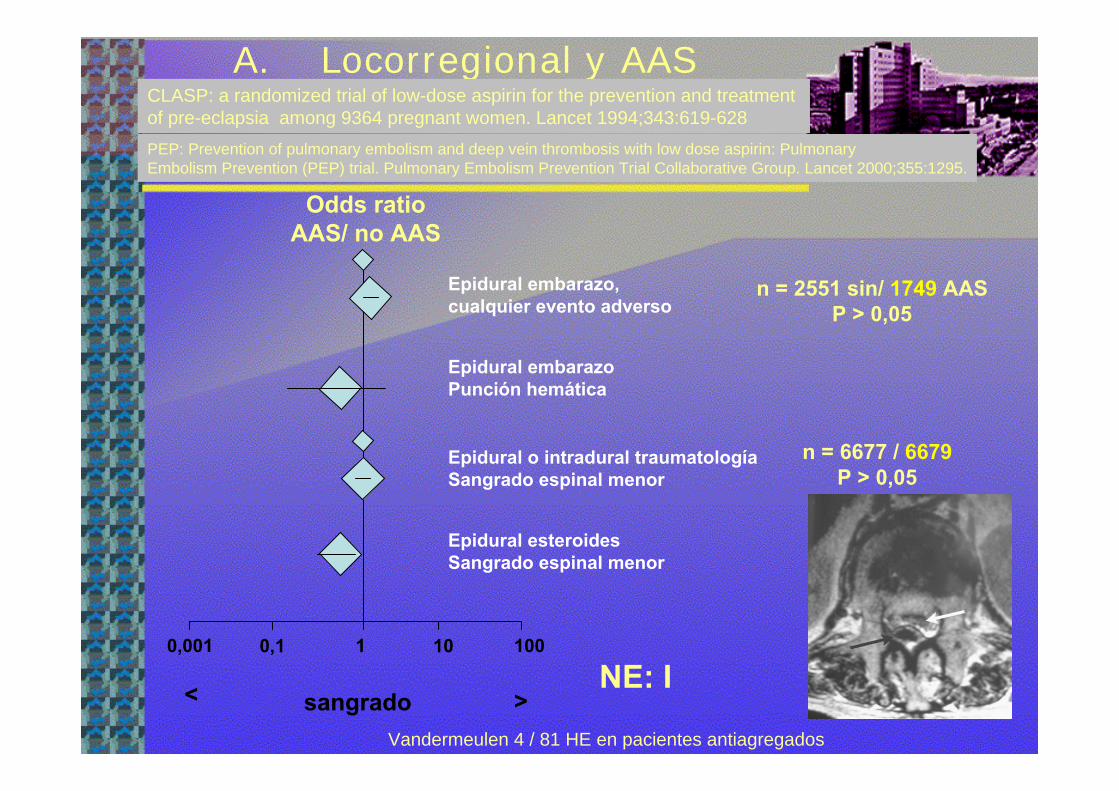
A. Locorregional y AAS
Odds ratioAAS/ no AAS
0,001 1001010,1
sangrado< >NE: I
Vandermeulen 4 / 81 HE en pacientes antiagregados
CLASP: a randomized trial of low-dose aspirin for the prevention and treatment of pre-eclapsia among 9364 pregnant women. Lancet 1994;343:619-628PEP: Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Pulmonary Embolism Prevention Trial Collaborative Group. Lancet 2000;355:1295.
Epidural embarazo, cualquier evento adverso
Epidural embarazoPunción hemática
Epidural o intradural traumatologíaSangrado espinal menor
Epidural esteroidesSangrado espinal menor
n = 2551 sin/ 1749 AASP > 0,05
n = 6677 / 6679P > 0,05
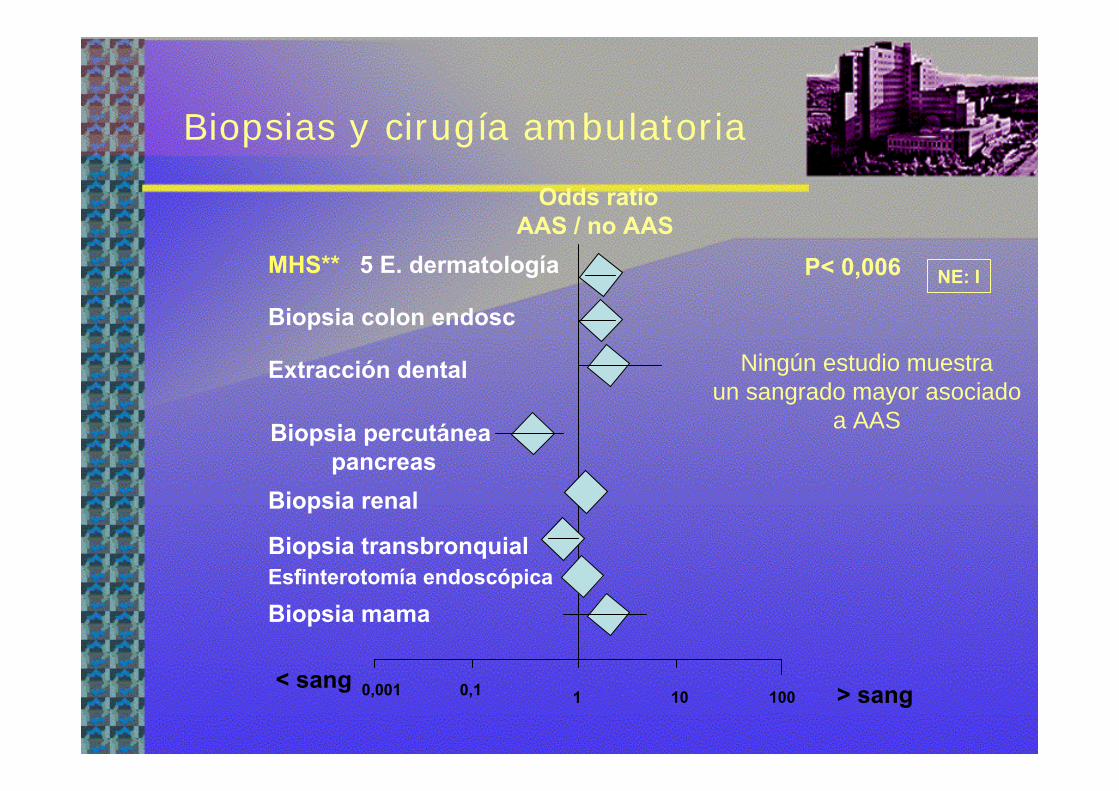
Biopsias y cirugía ambulatoria
< sang
MHS** 5 E. dermatología
Extracción dental
Biopsia percutáneapancreas
Biopsia transbronquial
Biopsia mama
Biopsia colon endosc
1 10 1000,10,001 > sang
Odds ratioAAS / no AAS
P< 0,006
Ningún estudio muestraun sangrado mayor asociado
a AAS
NE: I
Biopsia renal
Esfinterotomía endoscópica

Oftalmología
< sangrado > Sangrado1 100.1
Bloqueo retrobulbarperibulbar
Cirugía retina
MHS P = 0,86
Cataratas: Sangrado >
Cataratas ligera equímosis
0
ligera equímosis
Odds ratioAAS / no AAS
Trabeculectomía
CJ Cobb. The effect of aspirin and warfarin therapy in trabeculectoy. Eye 2007; 21: 598-603. Burger
NE: INE: I
AAP NE: IIINE: III
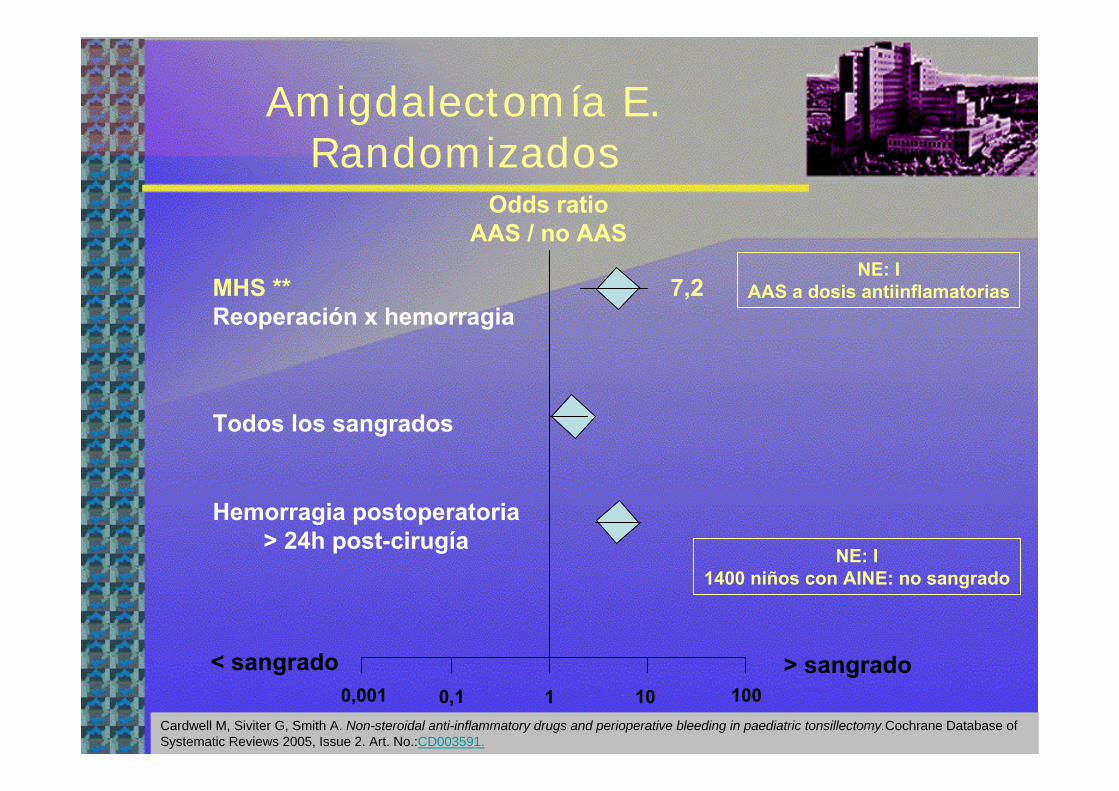
Amigdalectomía E. Randomizados
> sangrado< sangrado1 10 1000,10,001
MHS ** Reoperación x hemorragia
7,2
Todos los sangrados
Hemorragia postoperatoria> 24h post-cirugía
Odds ratioAAS / no AAS
NE: IAAS a dosis antiinflamatorias
Cardwell M, Siviter G, Smith A. Non-steroidal anti-inflammatory drugs and perioperative bleeding in paediatric tonsillectomy.Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No.:CD003591.
NE: I1400 niños con AINE: no sangrado
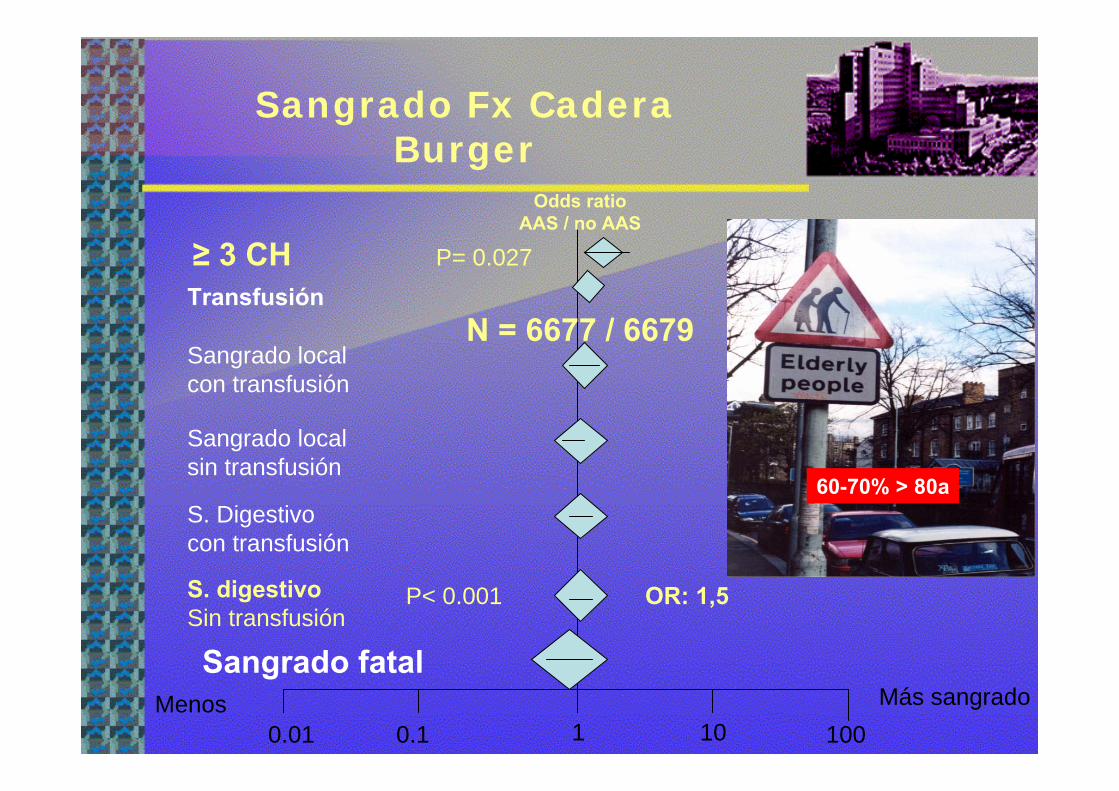
Sangrado Fx Cadera Burger
Menos Más sangrado0.01 0.1 1 10 100
P= 0.027≥ 3 CH
S. digestivoSin transfusión
P< 0.001
Sangrado local sin transfusión
S. Digestivo con transfusión
Sangrado fatal
Sangrado local con transfusión
N = 6677 / 6679Transfusión
OR: 1,5
Odds ratioAAS / no AAS
60-70% > 80a

C. Vascular
> sangrado< sangrado1 10 1000.10.001
C. Carótida
By pass femoro-poplíteoReoperación x sangrado
By pass femoro-poplíteoTodos sangrados
Odds ratioAAS / no AAS
Dorffler-Melly JAntiplatelet and anticoagulant drugs for prevention of restenosis /reoclusion following peripheral endovasculartreatment. Cochrane Database Syst Rev 2005; CD002071. Burger W. Journal Int Med 2005
Cochrane:ASA 50-300mg desde preoperatorio disminuye 60% la reestenosis al año, y disminuye mortalidad
NE: I
Cochrane CD001458:Disminuye ICTUS post endarterectomía
NE: IINE: II

Cirugía próstata
< sangrado10,001 0,01 10 100
MHS **Transfusión prostatectomía
2,7
P = 0,008
Sangrado biopsia transrectal próstata
Reoperación Prostatectomía transuretral
> sangrado
Hemorragia tardía sangrado
Odds ratioAAS / no AAS
NE: IINo hay sangrado mayor
75%

C. Cardíaca con CECmeta-analisis de cohortes
NE: Ib-IIa
> sangrado< sangrado 0,001 0,1 1 10 100
0,34
104
113
Randomizados (8 E, n = 805)
Observacionales (14 E, n = 4485)
> Sangrado mL
> Sangrado mL
Transfusión
Transfusión unidades
Reoperación
Reoperación
Odds ratioAAS / no AAS
No si AAS < 325 mg
The effect of preoperative aspirin on bleeding, transfusion, myocardial infarction, and mortality in coronary artery bypassSurgery: a systematic review of randomized and observational studies. Eur Hearth J 2008; 296: 1057-1071. Dunning Joel. Guidelineon antiplatelet and anticoagulation in cardiac surgery. Eur J Cardiothorac Surg (2008), doi: 10.1016/j.ejcts.2008.02.024
EACTS// GR: B
2-10d
Programada
URGENTE
6 h post-C75-325 mg GR: 1AGR: 1A

C. Cadera y rodillaC. Cadera y rodillaAAS, AINE, HBPMAAS, AINE, HBPM
N. EvidenciaN. EvidenciaCaderaCadera
RodillaRodilla
AAS + HBPM * 11
AAS + AINE * 33
AAS **
AINE + HBPM **
AINE
11
1
2
AINE + HBPM ** 1
AINE ** 2
Odss ratio
Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Can J Anesth 2006; 53: S103-112.
En cirugía no cardíaca:
• Burguer,• ACC / AHA 2007
Excepto:Próstata?
NeurocirugíaRetina?
Morbimortalidadisquémica
Morbimortalidadsangrado
Burger W, Chennitus JM, Kneissl GD, Rucker GLow-dose aspirin For secondary cardiovascular prevention-cardiovascular risks afterits Perioperative withdrawal versus bleeding risks with its continuation-review and meta-analysis. J Intern Med 2005; 257: 399-414.Anónimo. Drugs in the perioperative period: 4- cardiovscular drugs. Drug Ther Bull 1999; 37: 89-92ACC/AHA Guideline 2007 on perioperative cardiovascular evaluation and care for non cardiac surgery. Circulation 2007; 116:418-99
NE: I

Farmacología: AAP con clopidogrel
Harder S. Avoidance of bleedin during surgery in patients receiving anticoagulant and/or antiplatelet therapy:Pharmacokinetic and pharmacodynamic considerations. Clin Pharmcokinetics 2004; 43: 963-981Anónimo.Drugs in the perioperative period: 4- cardiovscular drugs. Drug Ther Bull 1999; 37: 89-92
ACC/AHA Guideline 2007 on perioperative cardiovascular evaluation and care for non cardiac surgery. Circulation 2007 e;
HarderNE: IV
ACC/AHANE: IV
?
CURE:Demora 5 días
1% IAM
Interacción ALR axial
Pocos estudios definen el sangrado

C. cataratas
Benzimra JD. The Cataract National Dataset electronic multicentre audit of 55 567 operations: antiplateletand anticoagulant medications. Eye 2008
Hemorragia subconjuntival
Sangrado grave
Sangre en aguja de bloqueo
OddsOdds ratioratioClopidogrelClopidogrel / no AAP/ no AAP
Clopidogrel, n = 928Sin AAP, n = 25359
2
2.5
><
2
N. EvidenciaN. Evidencia
2
OddsOdds ratio ratio ClopidogrelClopidogrel / AAS/ AAS
22
22
Clopidogrel, n = 928AAS, n = 13730
Hemorragia subconjuntival
22
Sangre en aguja de bloqueo222
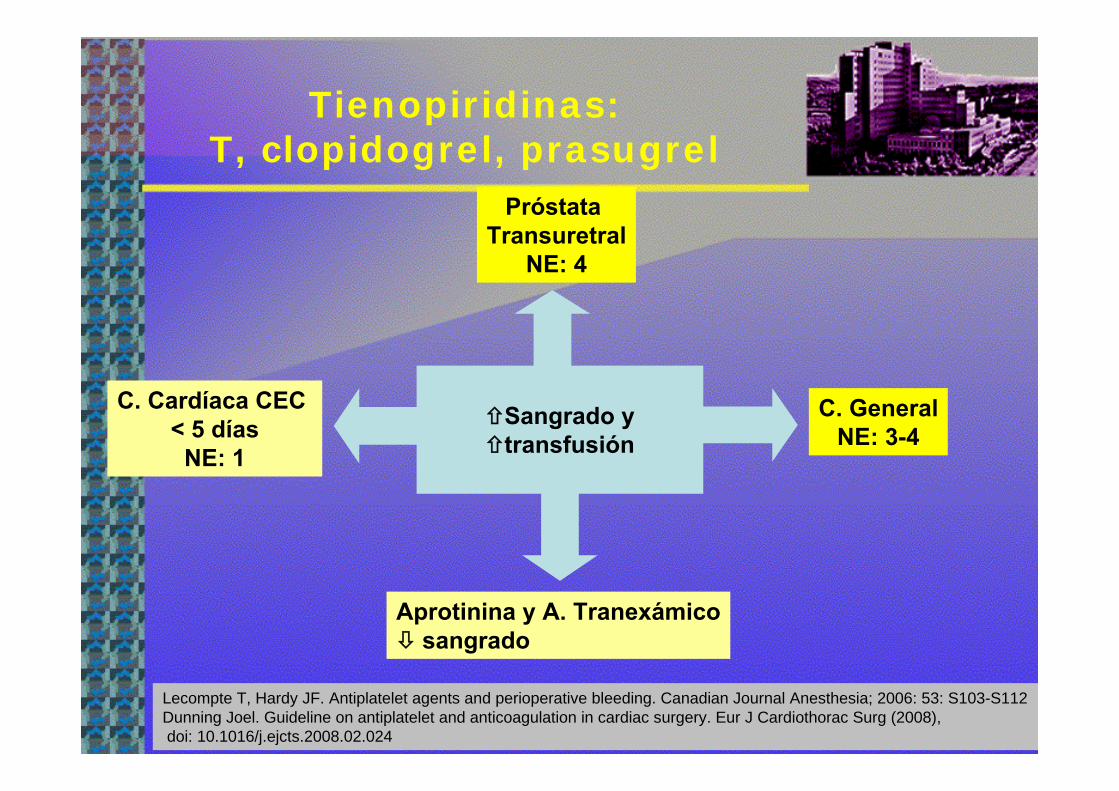
Tienopiridinas:T, clopidogrel, prasugrel
Sangrado ytransfusión
C. Cardíaca CEC < 5 días
NE: 1
Próstata Transuretral
NE: 4
C. GeneralNE: 3-4
Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Canadian Journal Anesthesia; 2006: 53: S103-S112 Dunning Joel. Guideline on antiplatelet and anticoagulation in cardiac surgery. Eur J Cardiothorac Surg (2008),doi: 10.1016/j.ejcts.2008.02.024
Aprotinina y A. Tranexámicosangrado
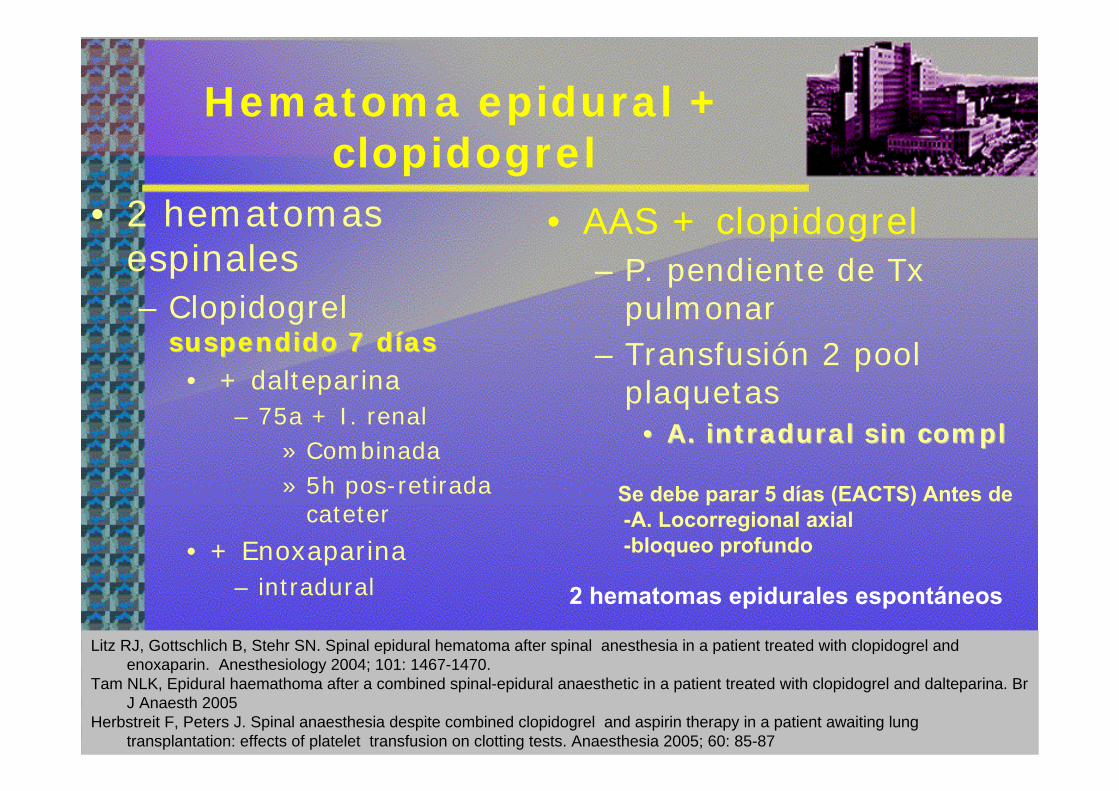
Hematoma epidural + clopidogrel
• 2 hematomas espinales– Clopidogrel
suspendido 7 dsuspendido 7 dííasas• + dalteparina
– 75a + I. renal» Combinada» 5h pos-retirada
cateter
• + Enoxaparina– intradural
• AAS + clopidogrel– P. pendiente de Tx
pulmonar– Transfusión 2 pool
plaquetas•• A. A. intraduralintradural sin sin complcompl
Litz RJ, Gottschlich B, Stehr SN. Spinal epidural hematoma after spinal anesthesia in a patient treated with clopidogrel and enoxaparin. Anesthesiology 2004; 101: 1467-1470.
Tam NLK, Epidural haemathoma after a combined spinal-epidural anaesthetic in a patient treated with clopidogrel and dalteparina. Br J Anaesth 2005
Herbstreit F, Peters J. Spinal anaesthesia despite combined clopidogrel and aspirin therapy in a patient awaiting lung transplantation: effects of platelet transfusion on clotting tests. Anaesthesia 2005; 60: 85-87
2 hematomas epidurales espontáneos
Se debe parar 5 días (EACTS) Antes de-A. Locorregional axial -bloqueo profundo

Clopidogrel preoperatorio C. Cardíaca con CEC
><
Odds ratioClopidogrel / no clopidogrel
Transfusión
Reexploración
Mortalidad
10 1000,10,01 1
6,9
4,9
Kapetakanis EI. Clopidogrel administration prior to coronary artery bypass grafting surgery: the Cardiologists panacea orthe surgeon´s headache? Eur Heart J 2005; 26: 576-594.Chu MWA. Does clopidogrel increase blood loss following coronary artery bypass surgery? Ann Thorac Surg 2004; 78: 1536-41Hongo RH. The effect of clopidogrel in combination with aspirin when given before coronary artery bypass grafting. J Am Coll Cardiol2002; 40: 231-7Yende S. Effect of clopidogrel on bleeding after coronary artery bypass surgery. Crit Care Med. 2001; 29: 2271-2275
NE: Ia -Ib
CURE 2359 pacientes +1 IAM / 90 demoras 5 días
1% IAM1% IAM
Demorar 5 d / no demorar
Drenaje tubo tórax 323 mL
6Reexploración
Transfusión
MHSMHS
CURECURE
EACTS
5 días
GR: BGR: B

¿Está justificado esperar 5 días sin clopidogrel para A.locorregional?
• Spah: NE: IV–En cirugía cardíaca: No–En cirugía no cardíaca: No
Epidural torácica:Protección hemodinámica
Riesgo trombótico
Locorregional lumbarNo tiene protección cardíaca
Chassot. British J Anesth 2007
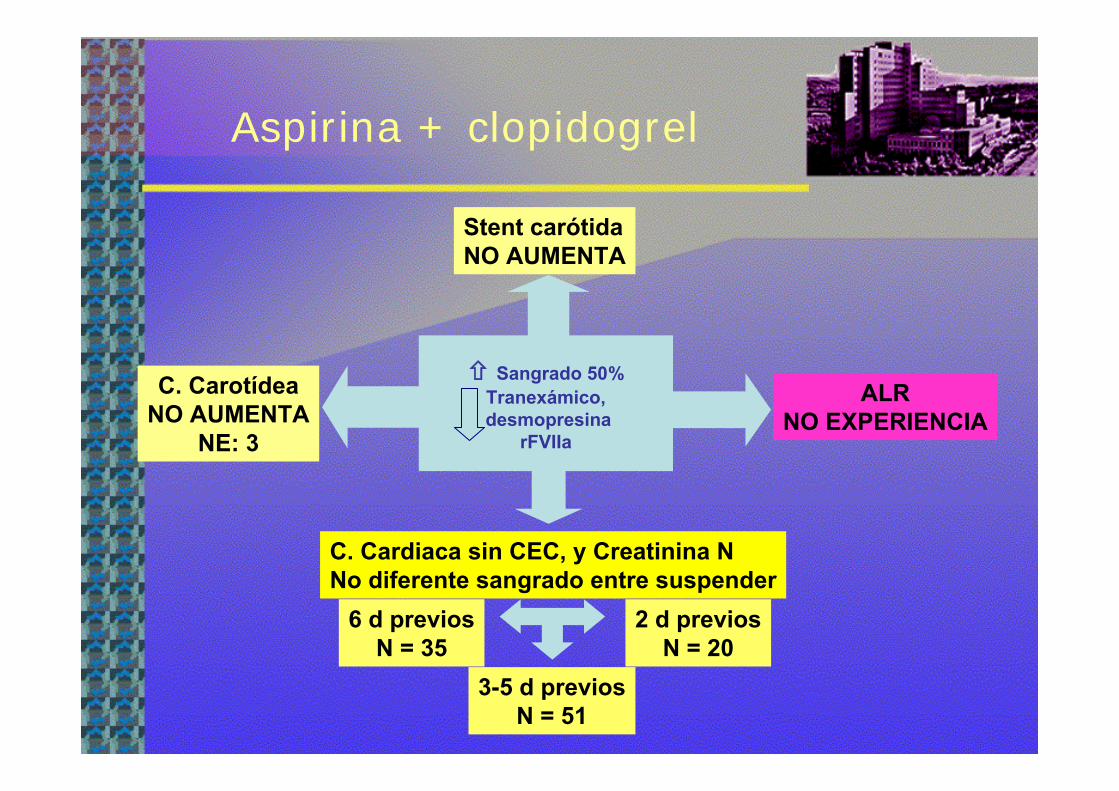
Aspirina + clopidogrel
C. CarotídeaNO AUMENTA
NE: 3
Stent carótidaNO AUMENTA
ALRNO EXPERIENCIA
C. Cardiaca sin CEC, y Creatinina NNo diferente sangrado entre suspender
6 d previosN = 35
3-5 d previosN = 51
2 d previosN = 20
Sangrado 50%Tranexámico,desmopresina
rFVIIa

Cirugía no cardíacaAAS + clopidogrel
Suspender 2 AAP en stent FA < 1 año20% de IAM
Mantener AAS + clopidogrelel sangrado microvascular
• 2 hematomas sofocantes – Bocio y carótida
• 1 aneurisma aorta
Con. Brief review: Coronary drug-eluting stents and anesthesia: [Article de synthese court :Les tuteurs coronariens actifs et l'anesthesie]. Can J Anesth 2006; 53: 1230-1243Perioperative
complications in patients with drug-eluting stents: a three-year audit at Geelong Hospital.

IdentificaciIdentificacióón de pacientes n de pacientes con > riesgo de transfusicon > riesgo de transfusióónn
• Factores modificables–– Anemia Anemia preoperatoriapreoperatoria NE: INE: I
• Relaciona con I renal, ICTUS y muerte
–– AAP y/o ACOAAP y/o ACO• AAS x 1.5
– No complicaciones x sangrado
• Clopidogrel?• AAS + clopidogrel > 50%
Ferraris VA. Society f Thoracic Surgeons blood conservation Guideline Task Force. Perioperative blood transfusion andblood conservation in cardiac surgery: the Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologistsclinical practice guideline. Ann Thorac Surg 2007; 83: S27-86
Kulier A. Impact of preoperative anemia on outcome in patients undergoing coronary artery bypass graft surgery.Circulation 2007; 116: 471-479
NE: MHS: INE: MHS: I
NE: IIINE: III
Búsqueda del AAP per-operatorio ideal
• Suspender el AAP: – 3 veces el riesgo isquémico
– 80 veces stent FA – Clopidogrel es esencial en defecto endotelial
• 1% IAM
• Características:– Protección eficaz de la trombosis – Permitir la hemostasia quirúrgica
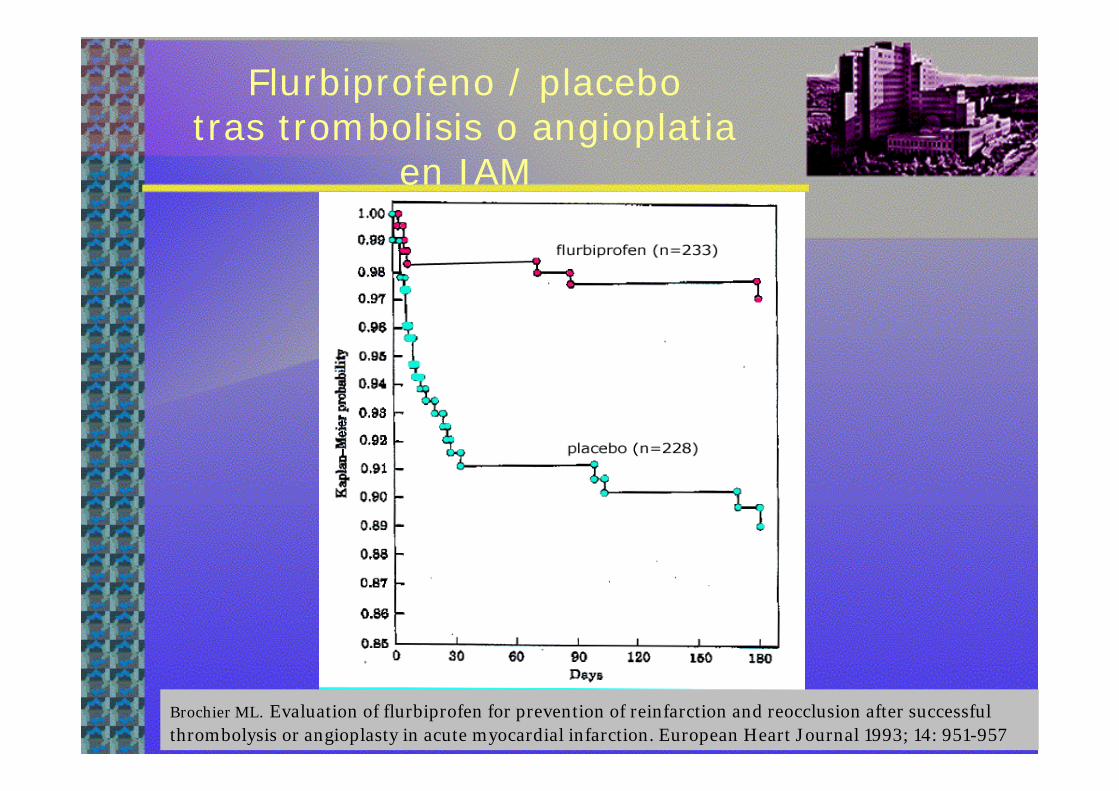
Brochier ML. Evaluation of flurbiprofen for prevention of reinfarction and reocclusion after successfulthrombolysis or angioplasty in acute myocardial infarction. European Heart Journal 1993; 14: 951-957
Flurbiprofeno / placebotras trombolisis o angioplatia
en IAM
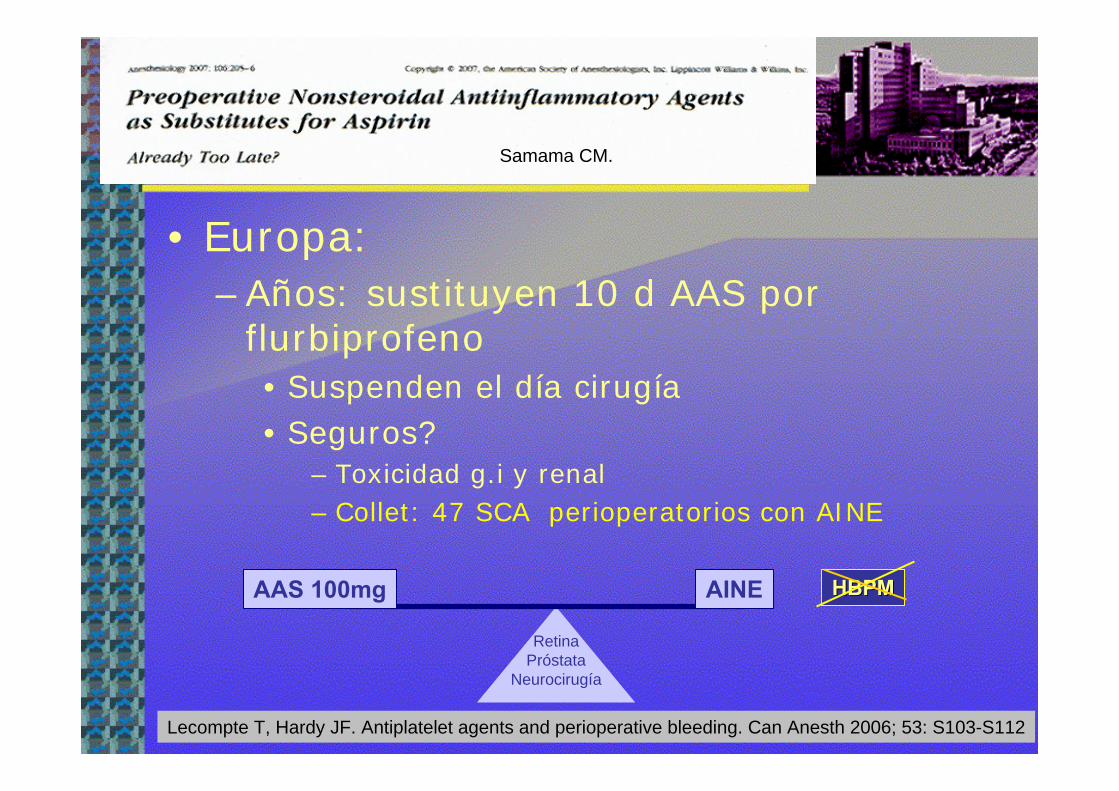
• Europa:–Años: sustituyen 10 d AAS por
flurbiprofeno• Suspenden el día cirugía• Seguros?
– Toxicidad g.i y renal– Collet: 47 SCA perioperatorios con AINE
RetinaPróstata
Neurocirugía
AAS 100mg AINE
Samama CM.
HBPMHBPM
Lecompte T, Hardy JF. Antiplatelet agents and perioperative bleeding. Can Anesth 2006; 53: S103-S112

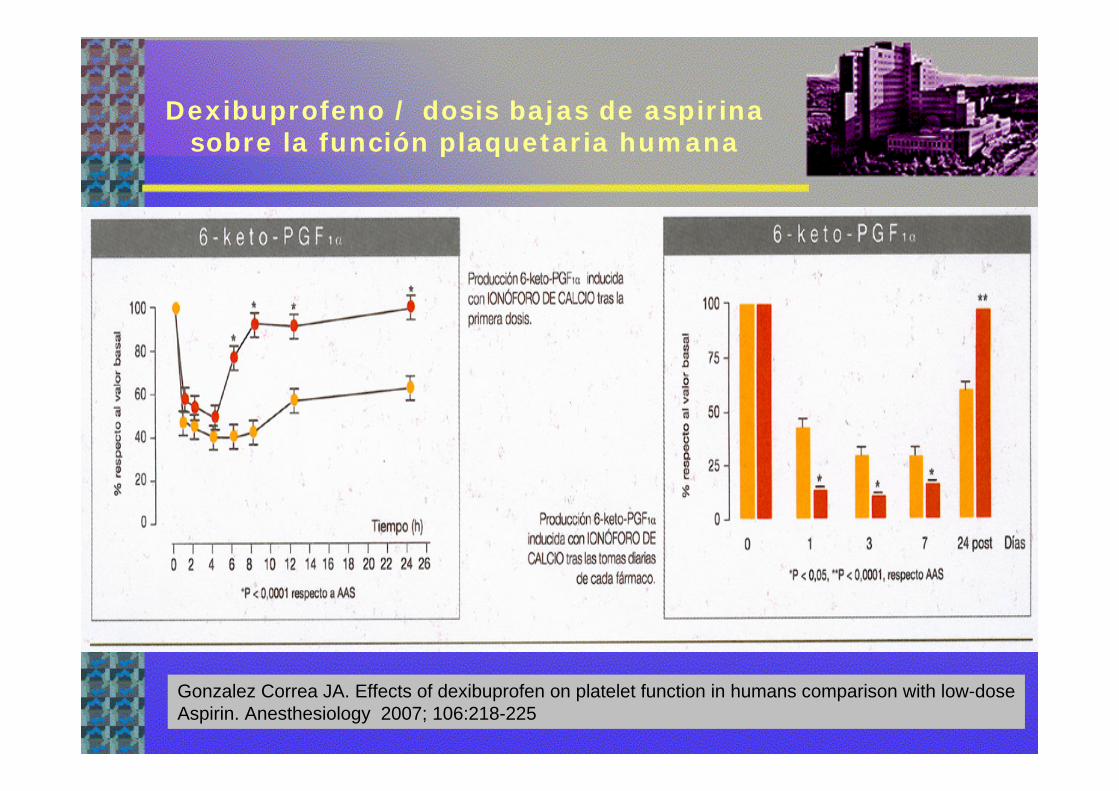
Dexibuprofeno / dosis bajas de aspirina sobre la función plaquetaria humana
Dexibuprofeno
Aspirina
24h1º dosis
1 semana
1 dosis
% AgregaciónPlaquetaria
- 11 sanos
% %
Gonzalez Correa JA. Effects of dexibuprofen on platelet function in humans comparison with low-doseAspirin. Anesthesiology 2007; 106:218-225
Dexibuprofeno / dosis bajas de aspirina sobre la función plaquetaria humana
Gonzalez Correa JA. Effects of dexibuprofen on platelet function in humans comparison with low-doseAspirin. Anesthesiology 2007; 106:218-225

Antiagregados con alto riesgo trombótico
Cirugía demorable?
Demorar 6m
Alto riesgo por el sangrado:Alto riesgo por el sangrado:NeurocirugíaCirugía retinaPolitraumatizadoProstatectomía?
Urgencia diferibleUrgencia no diferible
Riesgo intermedio por el sangrado:Riesgo intermedio por el sangrado:Otras C no cardiacasC Cardiaca sin CEC
Alto riesgo Alto riesgo trombtrombóóticotico::2 AARevascularización:
coronariacarotídeaEEII
SCA-IAMStent carotídeoACVA
2m ?

Sustitución de AAP porI-Glicoproteinas IIb-IIa
• Muy alto r trombótico y hemorrágico– Stent FA < 1 año– Stent < 2 m
AAS + clopidogrel
-5d Suspenderclopidogrel
-3dIngresar
I-Glicoproteinas IIb-IIIa+ Heparina o HBPM
Heparina-12h
I-Glicoproteinas-12h
Cirugía
75-300 mgclopi+1d
AASmantenido
Broad L. Succesful management of patients with a drug-eluting coronary stent presenting for elective, non cardiac surgery. Br J Anaesth 2007; 98: 19-22Chassot PG. Perioperative antiplatelet therapy: the case for continuing therapy in patients at risk of myocardialInfarction. Br J Anesth 2007; 99: 316-318
Indicación NE: III-IVCirugía vital o urgente + alto riesgo de sangradoPor ser una cavidad cerrada: neurocirugía intracraneal, Canal espinal y camara posterior del ojo

Farmacología I glicoproteinasIIb-IIIa
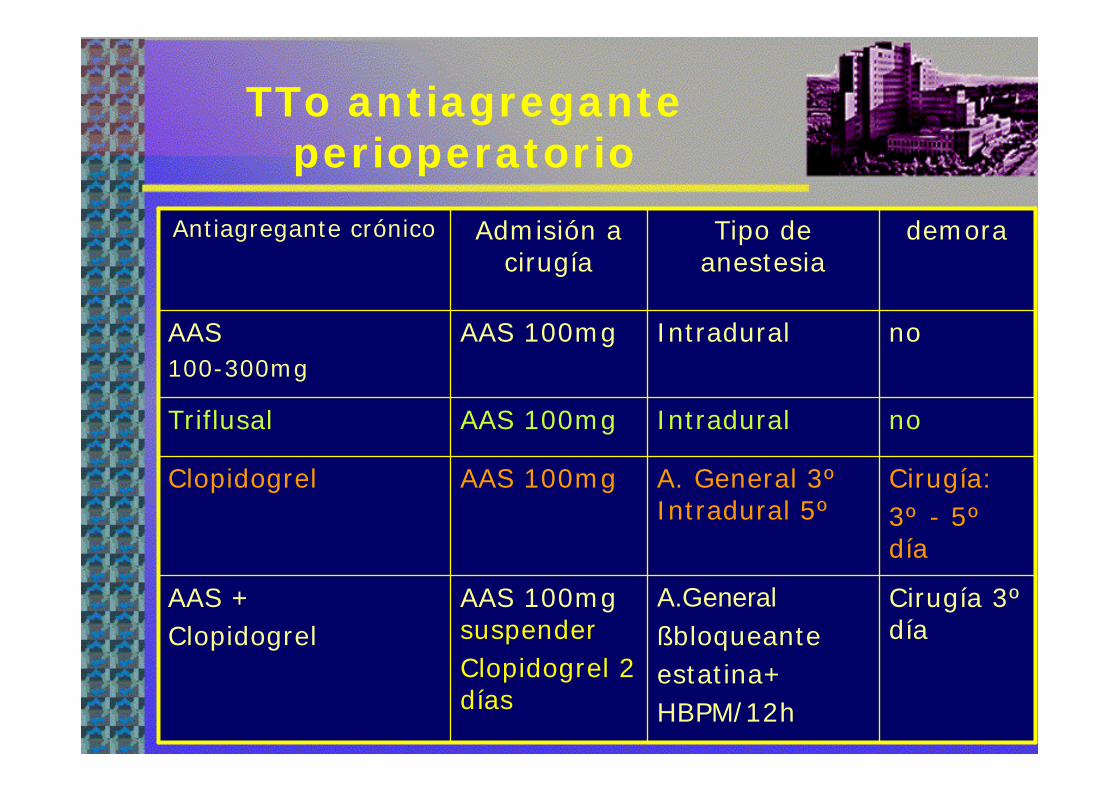
TTo antiagreganteperioperatorio
Cirugía 3ºdía
A.Generalßbloqueanteestatina+HBPM/12h
AAS 100mg suspenderClopidogrel 2 días
AAS + Clopidogrel
Cirugía:3º - 5ºdía
A. General 3ºIntradural 5º
AAS 100mgClopidogrel
noIntraduralAAS 100mgTriflusal
noIntraduralAAS 100mgAAS 100-300mg
demoraTipo de anestesia
Admisión a cirugía
Antiagregante crónico

Seguridad de A.locorregional y HBPM
6h
12h24h
Llau JV et al. Anticloting drugs and regional anaesthetic and analgesic techniques: Comparative update of the safety recomendations. Eur. J. Anaesthesiol 2007
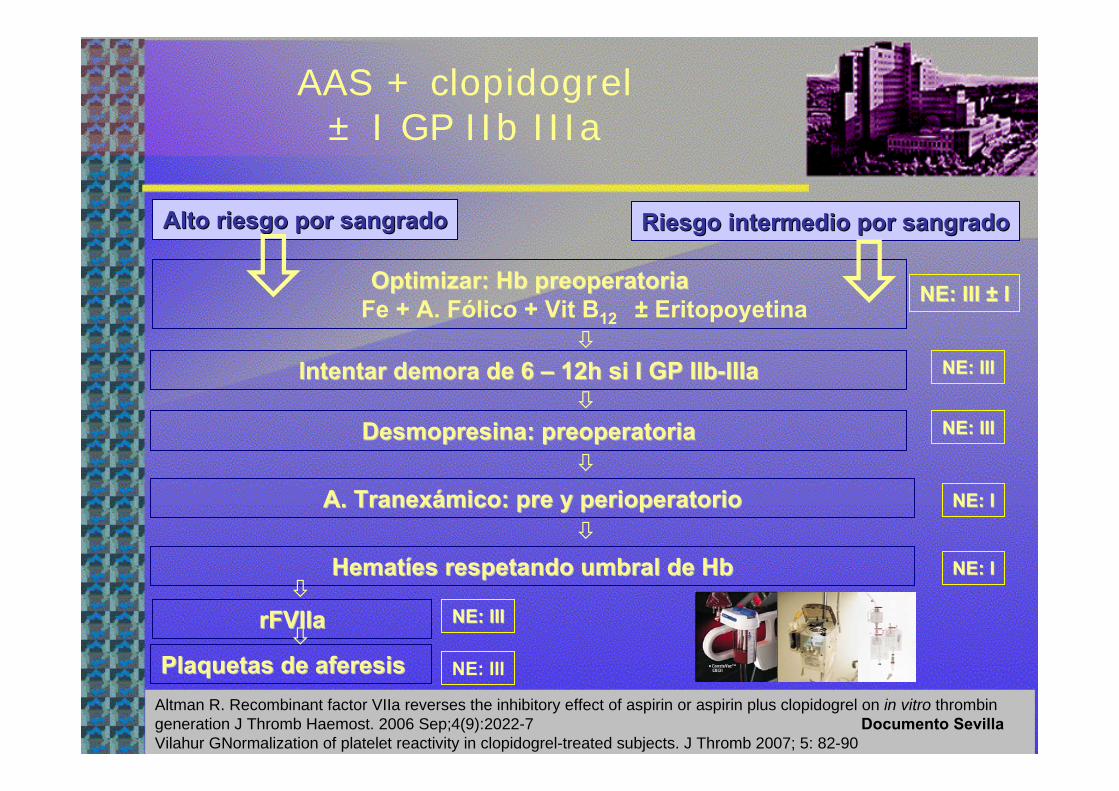
AAS + clopidogrel± I GP IIb IIIa
Altman R. Recombinant factor VIIa reverses the inhibitory effect of aspirin or aspirin plus clopidogrel on in vitro thrombingeneration J Thromb Haemost. 2006 Sep;4(9):2022-7 Documento SevillaVilahur GNormalization of platelet reactivity in clopidogrel-treated subjects. J Thromb 2007; 5: 82-90
Optimizar: Optimizar: HbHb preoperatoriapreoperatoriaFe + A. Fólico + Vit B12 ± Eritopoyetina NE: III NE: III ±± II
Intentar demora de 6 Intentar demora de 6 –– 12h si I GP IIb12h si I GP IIb--IIIaIIIa NE: IIINE: III
NE: IIINE: IIIDesmopresinaDesmopresina: : preoperatoriapreoperatoria
NE: INE: IA. A. TranexTranexáámicomico: : prepre y y perioperatorioperioperatorio
NE: INE: IHematHematííes respetando umbral de es respetando umbral de HbHb
rFVIIarFVIIa NE: IIINE: III
Plaquetas de Plaquetas de aferesisaferesis NE: III
Alto riesgo por sangradoAlto riesgo por sangrado Riesgo intermedio por sangradoRiesgo intermedio por sangrado
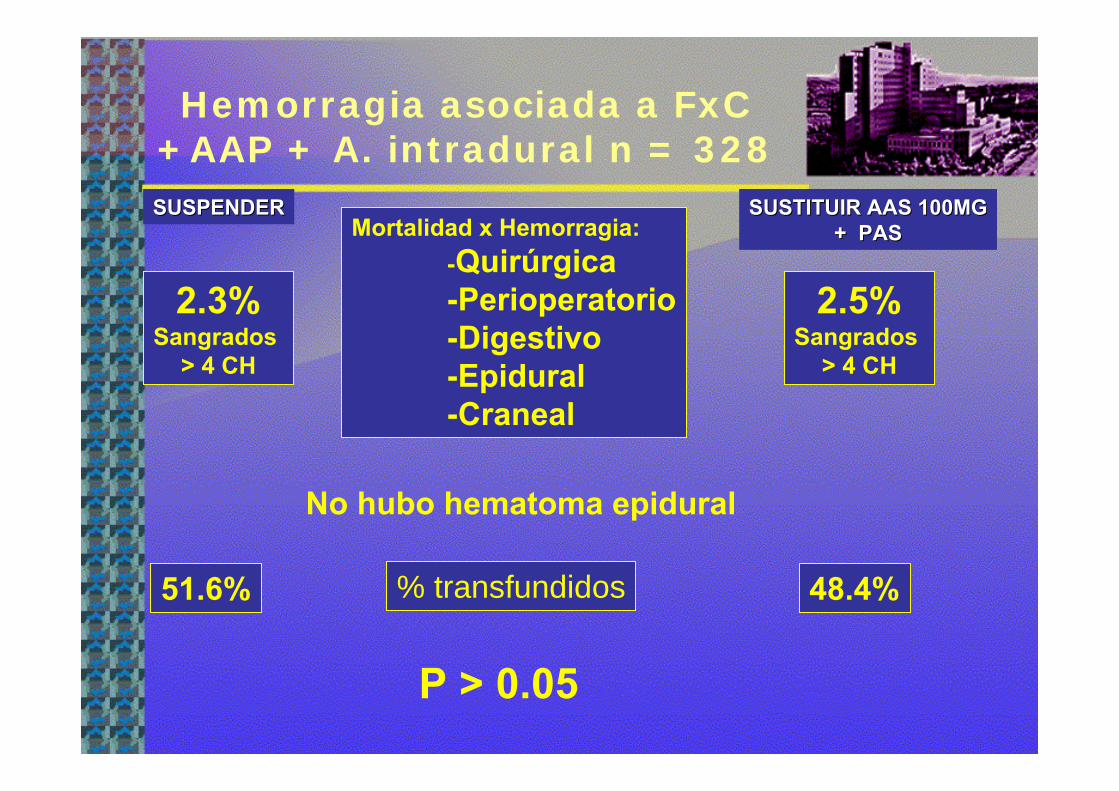
Hemorragia asociada a FxC+AAP + A. intradural n = 328
2.3%Sangrados
> 4 CH
2.5%Sangrados
> 4 CH
No hubo hematoma epidural
% transfundidos51.6% 48.4%
P > 0.05
Mortalidad x Hemorragia:-Quirúrgica-Perioperatorio-Digestivo-Epidural-Craneal
SUSPENDERSUSPENDER SUSTITUIR AAS 100MGSUSTITUIR AAS 100MG+ PAS+ PAS

Anciano + clopidogrel + fx de cadera y cirugía bajo anestesia intradural selectiva
0
10
20
30
40
50
60
% TRANSF COMPL. CV MORTALIDAD
ns0,69± 0,80,67± 0,80,89±0,9Transfusión
<0,0013,2± 0,53,4±0,53,1 ± 1ASA
<0,0011,7 ± 15,4 ± 0,6 7,1 ± 2Demora
0.00385,2 ±485,3 ±581,7 ±4Edad
pCBA
39 Clop. suspendido sin sustitución
74 74 ClopClop. sustituido por AAS 100mg. sustituido por AAS 100mg
91 AAS
nsns
P <0.001P <0.001 P < 0.001
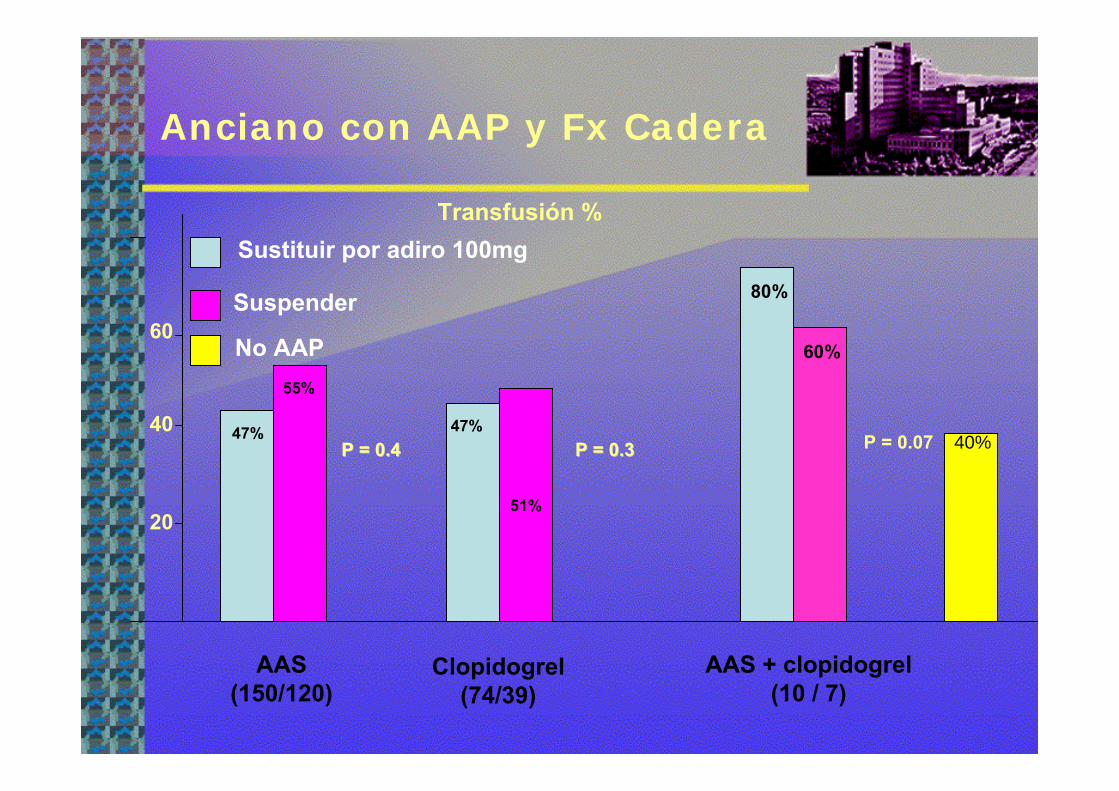
Anciano con AAP y Fx Cadera
AAS(150/120)
Clopidogrel(74/39)
AAS + clopidogrel(10 / 7)
Transfusión %
20
40
60
51%
Sustituir por adiro 100mg
Suspender
47%47%
55%
No AAP
80%
60%
40%P = 0.4P = 0.4 P = 0.3P = 0.3 P = 0.07

Anciano con AAP y FxCadera
CCV mortales o no 6 mI.Cardiaca + SCA + ICTUS
Sustituir por adiro 100mg + PAS
SuspenderNo AAP
AAS(150/120)
Clopidogrel(74/39)
AAS + clopidogrel(10 / 7)
10%
20%
30%
40%
50%
60%
10%
63%
4,5%
54%
10%
85%
6%
< 0.001< 0.001 < 0.001< 0.001 < 0.001< 0.001
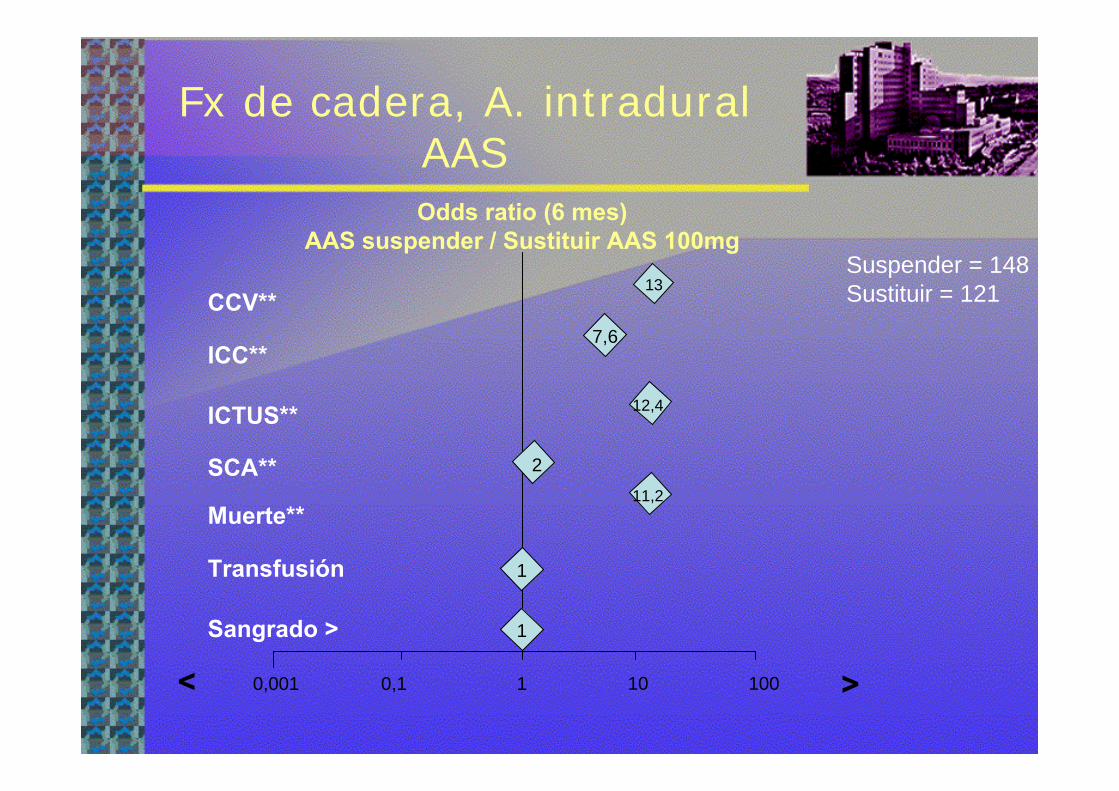
Fx de cadera, A. intraduralAAS
1 10 1000,10,001
Odds ratio (6 mes)AAS suspender / Sustituir AAS 100mg
><
ICC**
ICTUS**
CCV**
SCA**
Muerte**
Transfusión
Sangrado >
Suspender = 148Sustituir = 12113
7,6
12,4
11,2
2
1
1

Alto riesgo Alto riesgo trombtrombóóticoticoy fracturas HMSy fracturas HMS
AAS + clopidogrel
Riesgo intermedio por sangrado
n = 24
3 SCA 6 Stent FA 15 Stent c
Caída Hb 20% > no AAP
Transfusión hematíes 20% >No transfusion plaquetas
No rFVIIa
22, sobreviven a 6 meses sin eventos isquémicos, 1 exitus, 1 perdido
Mantener o sustituir antiagregación + precursores
hematínicos
BeneficioBeneficio< isquemia< isquemia
RiesgoRiesgoSangradoSangradoTransfusiTransfusióónn
Chasot PG. Antiplatelet drugs and intraoperative hemorrhage Rev Med Suise 2006;88: 2684-2687

Meningioma parasagital- 2d AAS 100mg -5d clopidogrel
+ HBPM + seractil
T ª, Hb preoperatoria 14 g/dLDesmopresina + A. Tranexámico
rFVIIa 20µg/Kg1 CH1 CH

ConclusionesConclusiones
• La cirugía incrementa el riesgo trombótico (NE: II)– La agregación plaquetaria es posible ante > estímulo pro-agregante
(ADP, TXA2)• Modelo celular de la hemostasia
• En cirugía no cardiaca, el riesgo de mantener los AAP es menor al de suspenderlos aunque implique mayor transfusión (NE: I)– Salvo: neurocirugía, retina y próstata (NE: III)– El AAS no asocia > Hematoma Espinal (NE: I)– ACC/AA G 2007 no suspender AAS en C no cardíaca, – no claro si suspender o no 5 d clopidogrel
• No hay evidencia de cuanto tiempo se necesita sustituir el clopidogrel– en cirugía no cardíaca– CC sin bomba– ALR
• 5 días está extraido del estudio CURE: cirugía cardiaca con CEC • La A. intradural tras 5 días sin clopidogrel sustituido por AAS 100mg y
reintroducido al día siguiente de la cirugía es segura (NE II)

Conclusiones
• En pacientes con stent FA suspender los AAP 80 el r trombótico (NE: III)
• El clopidogrel es fundamental en localizaciones con lesión endotelial
• Faltan estudios de seguimiento de las guías- En C. no cardiaca AAS + clopidogrel > 50% el sangrado NE:III
1 caso ALR con plaquetasAntifibrinolíticos disminuyen el exceso de sangrado
• No hay evidencia del beneficio de sustituir los AAP por AINE en el perioperatorio, una alternativa es sustituir por AAS 100mg
• La hemoglobina preoperatoria se correlaciona con la necesidad de transfusión
• Protocolizar consensuando facilita el cumplimiento, – Sólo el caso no habitual debería requerir un consenso entre especialistas– La suspensión preoperatoria de la AAP por el anestesista se sigue de la
no reintrodución postoperatoria por el cirujano

Muchas gracias por Muchas gracias por su atencisu atencióónn


Profilaxis 1ª: AAS 100-150mg/ placebo
Sangrado / disminución isquemia
Patrono C. Platelet active drugs: The relationships among dose, effectiveness and side effects. TheSeventh conference on antithrombotic and thrombolytic therapy. Chest 2004
Sangrado >producidoEn 1000 Tratados/1 año
CCVreducidapor 1000 tratados
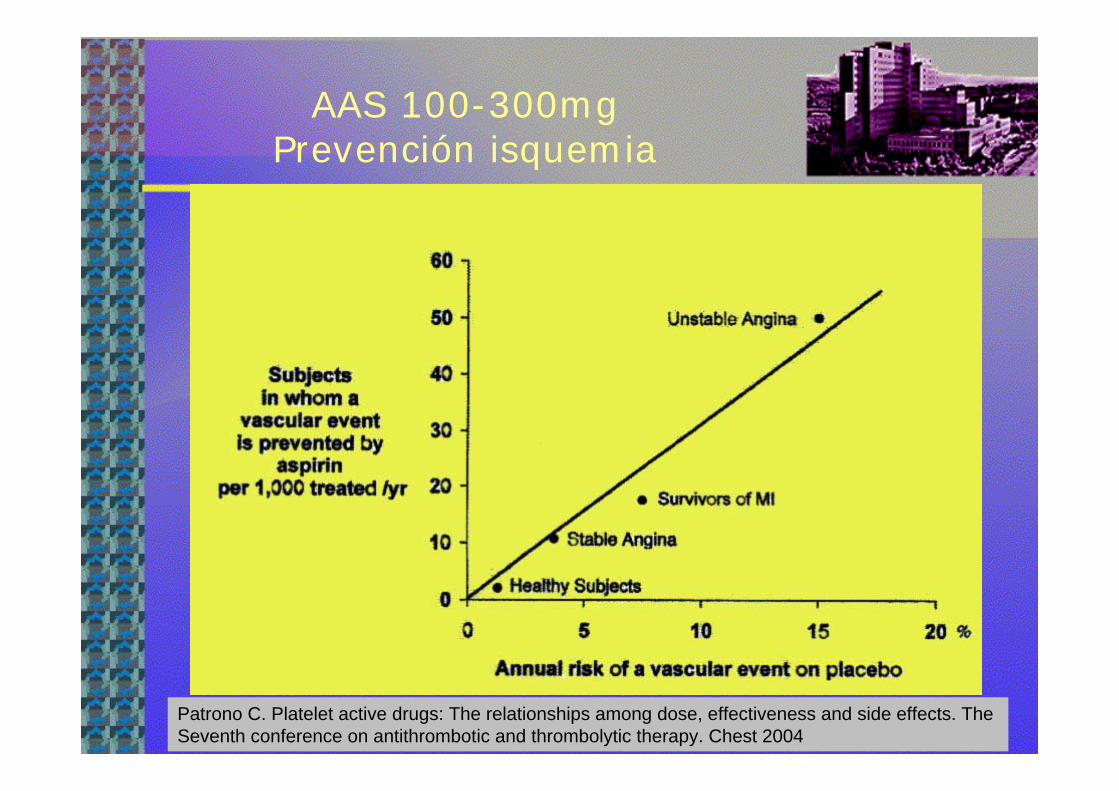
AAS 100-300mg Prevención isquemia
Patrono C. Platelet active drugs: The relationships among dose, effectiveness and side effects. TheSeventh conference on antithrombotic and thrombolytic therapy. Chest 2004

Mecanismos de AAP x la aspirina
López Farre A, Macaya C. Ácido acetil salicílico: farmacología y mecanismos de acción. Med Clin Monograf 2007; 8 (4): 3-7