electrodiagnostic findings and clinical symptoms of the...
TRANSCRIPT

1
Electrodiagnostic Findings and Clinical Symptoms of the Contralateral Side in Patients with Abnormal Distal Sensory
Latency of the Median Nerve
C. E. S. Hoogstins, student number 1568310 Faculty Supervisor: I.M. Nijholt, PhD Supervisor: D. Ring, MD, PhD Massachusetts General Hospital, Department of Orthopaedic Hand and Upper Extremity Surgery, Boston, U.S.A.

2
Abstract Purpose There is evidence that carpal tunnel syndrome is a genetic/structural, bilateral disease. The purpose of this study was to determine whether worsening of median nerve distal sensory latency conduction on patient’s worst side is associated with the occurrence of electrodiagnostic findings suggestive of carpal tunnel syndrome on the contralateral side. We also studied the occurrence of bilateral carpal tunnel syndrome-related symptoms and factors associated with electrodiagnostic evidence of carpal tunnel syndrome on the contralateral side. Methods We retrospectively reviewed 233 adult patients that had bilateral electrodiagnostic testing and a distal sensory latency greater than 3.6 ms on at least one side. Variables significantly associated with abnormal median nerve distal sensory latency on the contralateral side were analyzed in bivariate analysis and backwards stepwise logistic regression analysis. Results The contralateral side had electrodiagnostic abnormalities in 73% and clinical symptoms in 76% of patients. Age and median nerve distal sensory latency of the worst side were significantly associated with median nerve distal sensory latency on the contralateral side. Discussion Non-recordable distal sensory latency is strongly significantly associated with abnormal distal sensory latency on the contralateral side. These data suggest that as carpal tunnel syndrome advances, pathology appears on the contralateral side. Level of evidence: Prognostic II Introductie Er is bewijs dat carpaal tunnel syndroom een genetische/structurele, bilaterale ziekte is. Het doel van deze studie was om te bepalen of verergering van de “distal sensory latency” geleiding van de nervus medianus aan de meest aangedane kant van de patiënt geassocieerd is met het optreden van electrodiagnostische afwijkingen passend bij carpaal tunnel syndroom aan de contralaterale zijde. Ook hebben we het gekeken naar het voorkomen van de bilaterale carpaal tunnel syndroom-gerelateerde symptomen en naar welke factoren geassocieerd zijn met electrodiagnostisch bewezen carpaal tunnel syndroom aan de contralaterale zijde. Materiaal en methode We hebben de medische dossiers van 233 volwassenen, die bilateraal electrodiagnostisch getest waren en aan tenminste één zijde een “distal sensory latency” groter dan 3,6 ms vertoonden, retrospectief bekeken. Variabelen die significant geassocieerd waren met een abnormale “distal sensory latency” van de nervus medianus aan de contralaterale zijde werden geanalyseerd middels bivariate analyse en aan de hand van een stapsgewijze “backwards” logistische regressie-analyse. Resultaten Electrodiagnostische afwijkingen van de contralaterale zijde waren aanwezig in 73% van de patienten en de klinische symptomen aan de contralaterale zijde in 76%. Leeftijd en “distal sensory latency” van de nervus medianus aan de meest aangedane kant waren significant geassocieerd met “distal sensory latency” van de nervus medianus aan de contralaterale zijde. Conclusie Niet-meetbare “distal sensory latency” van de nervus medianus van de meest aangedane kant was zeer significant geassocieerd met een abnormale “distal sensory latency” van de nervus medianus aan de contralaterale zijde. Deze gegevens suggereren dat als carpaal tunnel syndroom verergert, pathologie ook tot uiting komt aan de contralaterale zijde. Mate van bewijs: Prognostisch II Keywords: Bilateral, Carpal tunnel syndrome, Electrodiagnostic testing, Electromyography, Etiology, Median nerve distal sensory latency

1
Table of Contents Introduction . . . . . . . . page 2 Research Question and Hypotheses . . . . . page 6 Material and Methods . . . . . . page 7 Results . . . . . . . . . page 9 Discussion . . . . . . . . page 12 Conclusion . . . . . . . . page 14 References . . . . . . . . page 15 Addendum . . . . . . . . page 17

2
Introduction Prevalence and Economical Implications Carpal tunnel syndrome, a compression neuropathy of the median nerve at the wrist, is the most common peripheral mononeuropathy, with a prevalence of clinically and electrophysiologically confirmed carpal tunnel syndrome of 2.7% in the general adult population (1).
A review of the long term earning losses of workers in Washington State, showed that carpal tunnel syndrome claimants recover to about half of their pre-injury earnings level relative to that of comparison groups with upper-extremity fractures and with medical-only dermatitis. In addition the cumulative excess loss of earnings of the carpal tunnel syndrome cohort is 45,000-89,000 dollars per claimant (2). The magnitude of these uncompensated losses causes a substantial economical and social burden on the workers, their households and society (2).
Since it is such a commonly seen disorder the way in which carpal tunnel syndrome is diagnosed and treated has enormous implications, including economically. Anatomy and Pathophysiology Carpal tunnel syndrome is caused by elevated pressure in the carpal tunnel, causing ischemia of the median nerve and subsequent impaired nerve conduction (3).
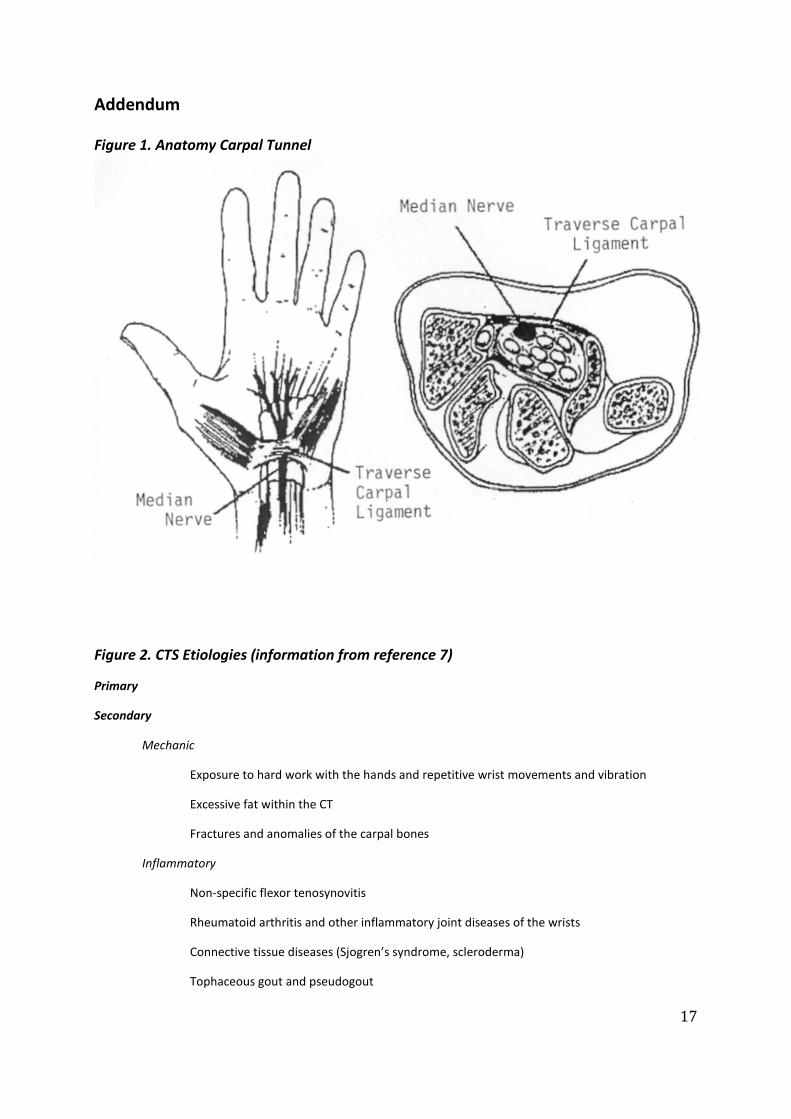
The flexor retinaculum (transverse carpal ligament), which extends from the hamate and triquetrum on the ulnar side to the scaphoid and trapezium on the radial side, forms the roof of the carpal canal. The median nerve lies just beneath the flexor retinaculum and passes through the carpal canal together with the flexor tendons (flexor pollicis longus, four flexor digitorum superficialis and four flexor digitorum profundus tendons) and their tendon sheets. The median nerve first gives off the recurrent motor branch that innervates the abductor pollicis brevis and the opponens pollicis muscles, it then splits into the digital nerves that provide sensation to the thumb, index, middle and radial half of the ring finger (Figure 1) (4).
The pressure in the carpal tunnel is around 13 mmHg in normal subjects, in patients with carpal tunnel syndrome the mean pressure is twice as high, i.e. 26 mmHg (5). As a result of this increased pressure the microneural circulation changes, causing the median nerve to be more prone to ischemia. When the compression persists it will induce localized demyelination, followed by diffuse demyelination and ultimately irreversible degeneration of the axons (4).
Etiology Anything that takes up space in the carpal tunnel, thereby causing an increased pressure, can cause carpal tunnel syndrome symptoms (6). A number of conditions that may be associated with carpal tunnel syndrome have been identified (Figure 2). It is described that about one third of carpal tunnel syndrome cases happen in association with one of these conditions (7). However the etiology of carpal tunnel syndrome remains unknown in the majority of cases.
The best available evidence suggests that carpal tunnel syndrome is a structural, genetically mediated disorder (8). The available evidence is also consistent with the theory

3
that carpal tunnel syndrome is inevitably bilateral and progressive (9, 10), although this is difficult to objectify.
Studies to date have shown that 38% (11) up to over 50% (9, 10) of patients with unilateral carpal tunnel syndrome symptoms have electrodiagnostic evidence of carpal tunnel syndrome on the contralateral side. In addition, there is a correlation between bilateral carpal tunnel syndrome -related symptoms and the duration of symptoms (9, 10). The occurrence of bilateral carpal tunnel syndrome symptoms is mostly found to be around 60% (9, 11-16), but higher percentages, of 87% (10), as well as lower percentages of 22% (17) have been reported also. The bilaterality of carpal tunnel syndrome is a logic consequence of the notion that carpal tunnel syndrome is a structural, genetically mediated disorder that inevitably progresses. Clinical Features The typical symptoms of carpal tunnel syndrome are parasthesias, numbness, pain or a combination of these symptoms in the distribution of the median nerve (thumb, index finger, middle finger and radial side of the ring finger). The presence of this classical pattern on a hand symptom diagram has a sensitivity of 64% for carpal tunnel syndrome. A history of nighttime pain and numbness has a sensitivity of 51 to 77% (18). Patients often report shacking their hands in attempt to alleviate discomfort, this is response is known as the flick sign. This sign is described to have a sensitivity of 93% (19).
Physical examination can demonstrate sensory loss in the median nerve distribution. A two-point discrimination test, in which the inability to discriminate two points less then 6 millimeter apart is considered to be abnormal, can be performed to evaluate for the presence of hypalgesia. However results of this two-point discrimination test remain normal until late in the course of carpal tunnel syndrome and the sensitivity is low (20). Thenar atrophy is also a late sign of carpal tunnel syndrome and is usually only seen in severe and chronic carpal tunnel syndrome. Thenar atrophy has a sensitivity of 16% (18). Weakness of the abductor pollicis brevis can be observed by asking the patient to raise the thumb at a 90 degree angle with the palm, while the physician applies downward pressure to the distal phalanx of the thumb. Several provocative tests can be used to elicit the patient’s symptoms, Phalen’s maneuver and Tinel’s sign are most commonly performed. These tests are deemed positive when flexion of the wrist for 60 seconds (Phalen’s maneuver) or percussion of the volar surface of the wrist (Tinel’s sign) causes parasthesias, numbness or pain in the median nerve distribution. However pain without numbness or parasthesias is not characteristic for carpal tunnel syndrome. Estimates of the sensitivity and specificity of these tests vary widely, causing the diagnostic value of these tests to be questionable (Figure 3) (18). Diagnosis The diagnosis of carpal tunnel syndrome is based on a combination of clinical symptoms and characteristic findings during physical examination. Subsequently electrodiagnostic studies can be done to confirm the diagnosis (21).
Electrodiagnostic studies include electromyography and nerve conduction studies, and can be used to document, inter alia, abnormalities of the median nerve fibers within the carpal tunnel. With the electromyography component of the electrodiagnostic studies the spontaneous or volitional electrical activity of the median-innervated thenar muscles is

4
recorded via recording electrodes inserted in the muscle. Electromyography is necessary to diagnose cervical radiculopathy, proximal median neuropathy, polyneuropathy and axonal loss. But it is not universally agreed upon in what situations an electromyography should or should not be performed as a part of electrodiagnostic studies (22).
Nerve conduction studies use surface electrodes to stimulate and record the nerve to study motor, sensory and mixed nerves. Amplitude, duration, latency, the area of the recorded response and conduction velocity can be recorded. These parameters give information about axon and myelin pathology, and can be used to grade the severity of carpal tunnel syndrome (4). Mild carpal tunnel syndrome is defined as prolonged (relative or absolute) median sensory latencies with normal motor studies and no evidence for axonal loss. Moderate carpal tunnel syndrome is defined as prolonged (relative or absolute) median sensory latencies with (relative or absolute) prolongation of median motor distal latency and no evidence for axonal loss. Severe carpal tunnel syndrome is defined as any of the above mentioned nerve conduction study abnormalities with evidence for axonal loss. Axonal loss is defined by either: an absent or low amplitude sensory or mixed nerve action potential; low amplitude or absent thenar compound muscle action potential; or a needle electromyography with fibrillation potentials or motor unit potential changes (22).
Even though these classification scales are commonly used to describe the extent of carpal tunnel syndrome, the correlation between electrodiagnostic findings and clinical symptoms is not well established (20, 23). Studies have shown a lack of correlation between carpal tunnel syndrome related symptoms of patients and the results of electrodiagnostic testing (23) and it is suggested that the process causing carpal tunnel syndrome related symptoms may not be the same as the process causing abnormalities on electrodiagnostic testing (20). There is also variability among physicians about how to interpret the findings of electrodiagnostic studies and how to distinguish between normal, borderline and abnormal results (22). For those reasons the use of these scales is not recommended, especially not when it comes to treatment decisions, those should be based on a multitude of factors, including symptoms and findings during physical examination (24).
Treatment Treatment options for carpal tunnel syndrome vary depending on a number of factors. When carpal tunnel syndrome is the result of an underlying condition such as rheumatoid arthritis, treatment of the underlying condition will usually reduce carpal tunnel syndrome symptoms. When carpal tunnel syndrome occurs together with an associated condition, such as diabetes mellitus, treatment of that condition is appropriate but whether it reduces the carpal tunnel syndrome symptoms is unknown (25).
Further management of carpal tunnel syndrome should be based on the severity of the disease. A number of non-operative treatments of carpal tunnel syndrome are available, of which wrist splinting is most frequently recommended (26, 27). With the wrist splinted in a neutral position, the pressure in the carpal canal is minimized. Symptoms are alleviated in 80% of patients using a wrist splint (28). However wrist splints do not treat the cause of carpal tunnel syndrome, they only control the symptoms. Therefore the use of splints will not completely resolve the symptoms of carpal tunnel syndrome.
Other non-operative treatment options include the use of oral medication and local corticosteroid injection. One small-short term (4 weeks) randomized controlled trial assessed the efficacy of a diuretic, a non-steroid anti-inflammatory drug (NSAID), and an oral

5
corticosteroid, compared to placebo. Only the oral corticosteroid produced a substantial reduction in carpal tunnel syndrome symptoms (29). Local corticosteroid injections have proven to be effective in reducing carpal tunnel syndrome symptoms and improving median nerve conduction, when compared to an injection with a placebo (12, 30-33).
After first being discussed by Paget in 1854 (34), Putnam described a group of 31 patients presenting to the Massachusetts General Hospital with a common complaint of periodically occurring numbness, but it was only in 1946 through the work of Brain and later Phalen that the diagnosis and treatment of carpal tunnel syndrome became popularized (35). The first to recommend decompression of the median nerve by surgically releasing the flexor retinaculum were Marie and Foix in 1913. Since then numerous techniques for carpal tunnel release, including the traditional open release, endoscopic release and small incision open release have been developed, but the basic principle: surgical decompression of the median nerve by releasing the flexor retinaculum, has remained the same. Relief of symptoms is comparable for the open and endoscopic procedure and over 70% of patients are completely or very satisfied after carpal tunnel release surgery, regardless of which technique was used (36-38). When it comes to bilateral carpal tunnel syndrome there are various treatment options, such as unilateral carpal tunnel release, bilateral staged carpal tunnel release and bilateral simultaneous carpal tunnel release. The opinions vary on which treatment is best for which patient. Some suggest that simultaneous carpal tunnel release increases morbidity (39, 40), while others have demonstrated higher patients satisfaction rates (40-43) and no increase in the number of complications (39, 41, 43, 44). Also the effect of unilateral carpal tunnel release on the nonoperated hand is not clear, worsening (45), improvement (46) and no change of symptoms (47) of the nonoperated hand have all been described. Summary Summarizing, carpal tunnel syndrome is caused by elevated pressure in the carpal canal which causes ischemia and impaired nerve conduction of the median nerve. It is the most common peripheral mononeuropathy and a frequent cause of parasthesias, numbness and pain in the upper extremity. The diagnosis of carpal tunnel syndrome is based on a combination of symptoms, findings on physical examination and electrodiagnostic testing. A number of conditions have been associated with carpal tunnel syndrome. The etiology of carpal tunnel syndrome often remains unknown, however the best available evidence suggests that carpal tunnel syndrome is for the most part a structural, genetic disorder that will inevitably progress and become bilateral. This conception is supported by the fact that the reported occurrence of bilateral carpal tunnel syndrome symptoms is mostly found to be around 60% but higher percentages, of 87% are also reported. Also 38% up to over 50% of patients with unilateral carpal tunnel syndrome symptoms have electrodiagnostic evidence of carpal tunnel syndrome on the contralateral side. And finally there is a correlation between bilateral carpal tunnel syndrome related symptoms and the duration of symptoms. There are various conservative as well as surgical treatment options for carpal tunnel syndrome. The choice of treatment is dependent on a number of factors, including the presence of bilateral carpal tunnel syndrome.

6
Research Question and Hypotheses Primary Research Question Is there a difference in impairment of median nerve distal sensory latency conduction of the contralateral side on electrodiagnostic testing between patients with a non-recordable median nerve distal sensory latency on electrodiagnostic testing of their worst side versus patients with a recordable, prolonged median nerve distal sensory latency on electrodiagnostic testing of their worst side? Primary Null Hypothesis Patients with a non-recordable median nerve distal sensory latency on electrodiagnostic testing of their worst side are equally likely to have impairment of median nerve distal sensory latency conduction on the contralateral side when compared to patients with a recordable prolonged distal sensory latency on electrodiagnostic testing. Secondary Research Questions What percentage of patients with prolonged recordable and non-recordable distal sensory latency on electrodiagnostic testing of their worst side has clinical symptoms of carpal tunnel syndrome on the contralateral side? What are the predictors of electrodiagnostic findings suggestive of carpal tunnel syndrome on the contralateral side?
Is there a correlation between distal sensory latency on the worst side and distal sensory latency on the contralateral side?
7
Material and Methods Study Design Using billing records we identified 509 electrodiagnostic test reports of 505 patients that were referred to our institution for electrodiagnostic testing to rule out carpal tunnel syndrome between November 2006 and June 2010. Patients were referred from several specialty clinics, mainly orthopedic surgery, neurology and plastic surgery, but also from primary care clinics.
Electrodiagnostic testing was conducted in clinical setting according to the technique described by Kimura (13). The TECA Synergy N2 EMG (Oxford Instruments Medical, Inc) was used for all electrodiagnostic studies. Sensory conduction of the median nerve was recorded using antidromic stimulation. The stimulation was performed at the wrist and recorded, using ring electrodes, from the index finger, 13 cm distally from the stimulation site. All studies were performed by experienced and certified electrodiagnostic technicians.
Patients who were 1) adult, defined as eighteen years or older; 2) who had electrodiagnostic testing of both hands (bilateral studies are done in the majority of patients; however, they are not conducted as standard care at our institution); and 3) who had median nerve distal sensory latency greater than 3.6 milliseconds on at least one side were included in our study.
Patients were excluded based on the following criteria: 1) systemic inflammatory illness (including systemic lupus erythematosus and rheumatoid arthritis); 2) trauma of the wrist less than two months ago; 3) history of median nerve surgery (including previous carpal tunnel release surgery); and 4) pregnancy.
An investigator not involved in patient care, retrospectively reviewed the electrodiagnostic test reports and medical records. Approval from our Human Research Committee was obtained. Chart Review and Definitions The following variables were recorded from patient’s medical records: sex (male, female), age at visit, symptomatic side (left, right, both sides left more than right, both sides right more than left, both sides equal), median nerve distal sensory latency, results of previous electrodiagnostic testing of the upper extremity (when applicable) and the presence of the following conditions at time of electrodiagnostic testing or conditions discovered during electrodiagnostic testing: cubital tunnel syndrome, polyneuropathy, cervical radiculopathy, myelopathy, cerebrovascular accident, diabetes mellitus, thyroid disease, depression, and wrist fracture of the worst side more than two months ago.
The worst affected side and the contralateral or least affected side were defined based on the median nerve distal sensory latency on electrodiagnostic testing. The worst affected side was defined as the side with the most prolonged or non-recordable median nerve distal sensory latency, and subsequently the contralateral side was defined as the side with the least affected median nerve distal sensory latency. In case of non-recordable median nerve distal sensory latency on both sides, the worst affected side was determined based on the side with the worst documented clinical symptoms. The following symptoms were regarded as clinical symptoms suggestive of carpal tunnel syndrome: (nocturnal) numbness, parasthesias or pain in the median nerve distribution.
8
Median nerve distal sensory latency was considered abnormal and suggestive of carpal tunnel syndrome if equal to or larger than 3.6 milliseconds; however, when it comes to differentiating between normal and abnormal median nerve sensory latency on electrodiagnostic studies, no consensus exists (22). Consequently, median nerve distal sensory latency was divided into the following categories: 1) a median nerve distal sensory latency smaller than 3.6 milliseconds was defined as a normal median nerve distal sensory latency; 2) a median nerve distal sensory latency equal to or larger than 3.6 milliseconds was defined as a prolonged median nerve distal sensory latency; and 3) an absent distal sensory latency was defined as a non-recordable median nerve distal sensory latency.
Moreover, median nerve distal sensory latency of the contralateral side was divided into two categories: 1) normal distal sensory latency; and 2) abnormal distal sensory latency by combining prolonged and non-recordable distal sensory latency.
All of following conditions: cubital tunnel syndrome, polyneuropathy, cervical radiculopathy, myelopathy, cerebrovascular accident, diabetes mellitus type 2, depression, and wrist fracture of the worst side more than two months ago, were dived in two categories 1) yes, if the condition was present at time of electrodiagnostic testing or discovered during electrodiagnostic testing; 2) no, if the condition was not present at time of electrodiagnostic testing or not discovered during electrodiagnostic testing. The only exception being thyroid disease which was divided into the following categories: 1) no thyroid disease; 2) hypothyroidism; 3) hyperthyroidism; and 4) other thyroid disease. None of the patients in the cohort had type 1 diabetes mellitus, therefore this was not one of the studies parameters.
Our primary outcome was the presence of normal median nerve distal sensory latency or abnormal median nerve distal sensory latency on the contralateral side. Statistical Analysis An a-priori sample size calculation was carried out using data known from previous research. Using these data in a Pearson Chi-square test, we calculated that a total sample of 82 patients achieves 90% power to detect a moderate effect size of 0.36 at a significance level of 0.05.
To determine differences between two categorical variables we used Pearson Chi-square test. When the cell frequency was less than five, we used Fisher’s exact test instead of Pearson Chi-square test. To determine differences between continuous and dichotomous variables we used Unpaired T-tests. Pearson Correlation was used to evaluate the relationship between two continuous variables.
In order to assess predictors of abnormal median nerve distal sensory latency on the contralateral side, we identified all variables with a p-value < 0.10 in the bivariate analysis. These variables were entered into a backwards stepwise logistic regression analysis. A p-value of < 0.05 was considered to be significant.

9
Results Two-hundred-and-seventy-six electrodiagnostic test reports were excluded based on the inclusion and exclusion criteria, leaving 233 tests. The cohort included 150 women (64%) and 83 men (36%). The mean age was 56 ± 13 years (range, 22 to 90). The median nerve distal sensory latency on the worst side was considered prolonged in 159 cases and non-recordable in 74 cases. There was a significant difference in the severity of median nerve distal sensory latency on the contralateral side between patients with a prolonged and non-recordable median nerve distal sensory latency on the worst side (p < 0.001; Table 1).
Number % Number % p value
DSL of contralateral side <0.001
Recordable, Normal 54 34.0 8 10.8
Recordable, Prolonged 105 66.0 39 52.7
Non-Recordable 0 0.0 27 36.5
DSL = Distal Sensory Latency; N = Number.
n = 159 n = 74
Table 1. Median Nerve DSL of Worst vs. Contralateral Side n = 233
DSL of Worst Side
Prolonged Non-Recordable
Clinical symptoms on the contralateral side occurred in 76% of patients with a non-recordable median nerve distal sensory latency on the worst side and in 77% of patients with a prolonged median nerve distal sensory latency (Table 2).
Number % Number %
Symptoms on contralateral side
Yes 122 76.7 56 75.7
No 37 23.3 18 24.3
CTS = Carpal Tunnel Syndrome; N = Number; DSL = Distal Sensory Latency.
n = 159 n = 74
n = 233Table 2. Clinical Symptoms of CTS on Contralateral Side
DSL of Worst Side
Prolonged Non-Recordable
In bivariate analysis median nerve distal sensory latency of the worst side was significantly associated with median nerve distal sensory latency on the contralateral side (p = <0.001;
10
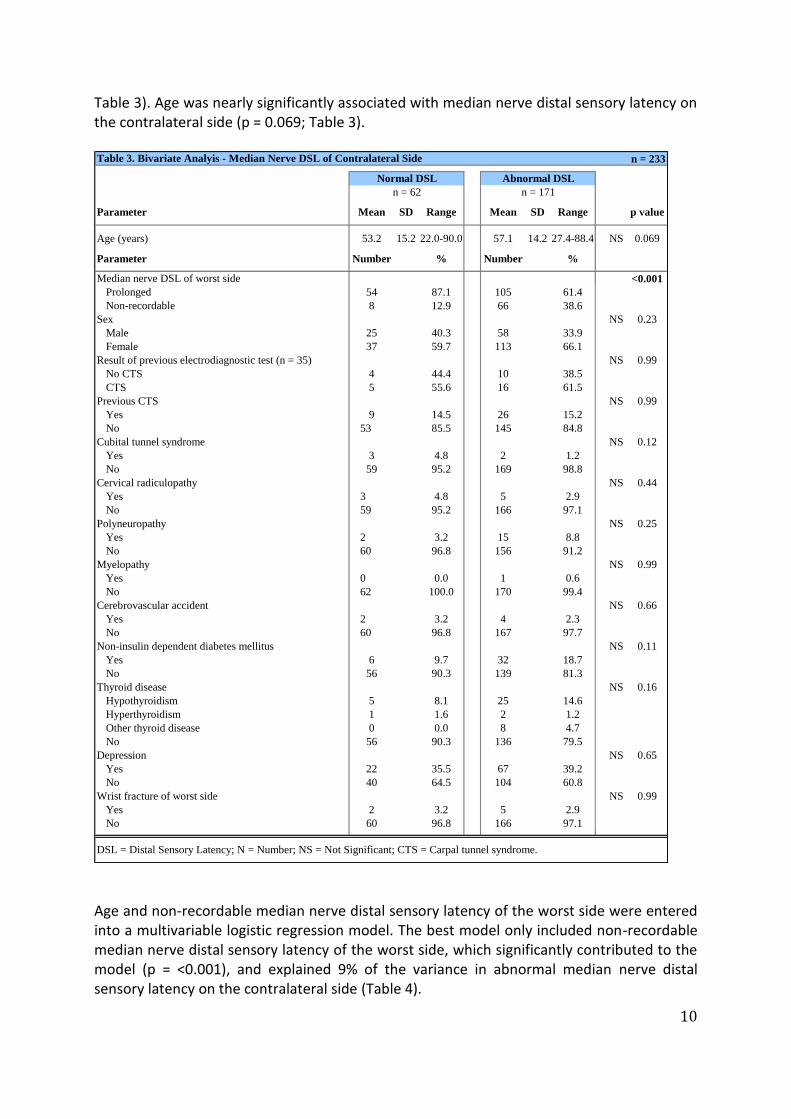
Table 3). Age was nearly significantly associated with median nerve distal sensory latency on the contralateral side (p = 0.069; Table 3).
n = 233
Parameter Mean SD Range Mean SD Range p value
Age (years) 53.2 15.2 22.0-90.0 57.1 14.2 27.4-88.4 NS 0.069
Parameter Number % Number %
Median nerve DSL of worst side <0.001
Prolonged 54 87.1 105 61.4
Non-recordable 8 12.9 66 38.6
Sex NS 0.23
Male 25 40.3 58 33.9
Female 37 59.7 113 66.1
Result of previous electrodiagnostic test (n = 35) NS 0.99
No CTS 4 44.4 10 38.5
CTS 5 55.6 16 61.5
Previous CTS NS 0.99
Yes 9 14.5 26 15.2
No 53 85.5 145 84.8
Cubital tunnel syndrome NS 0.12
Yes 3 4.8 2 1.2
No 59 95.2 169 98.8
Cervical radiculopathy NS 0.44
Yes 3 4.8 5 2.9
No 59 95.2 166 97.1
Polyneuropathy NS 0.25
Yes 2 3.2 15 8.8
No 60 96.8 156 91.2
Myelopathy NS 0.99
Yes 0 0.0 1 0.6
No 62 100.0 170 99.4
Cerebrovascular accident NS 0.66
Yes 2 3.2 4 2.3
No 60 96.8 167 97.7
Non-insulin dependent diabetes mellitus NS 0.11
Yes 6 9.7 32 18.7
No 56 90.3 139 81.3
Thyroid disease NS 0.16
Hypothyroidism 5 8.1 25 14.6
Hyperthyroidism 1 1.6 2 1.2
Other thyroid disease 0 0.0 8 4.7
No 56 90.3 136 79.5
Depression NS 0.65
Yes 22 35.5 67 39.2
No 40 64.5 104 60.8
Wrist fracture of worst side NS 0.99
Yes 2 3.2 5 2.9
No 60 96.8 166 97.1
DSL = Distal Sensory Latency; N = Number; NS = Not Significant; CTS = Carpal tunnel syndrome.
Table 3. Bivariate Analyis - Median Nerve DSL of Contralateral Side
Normal DSL Abnormal DSL
n = 62 n = 171
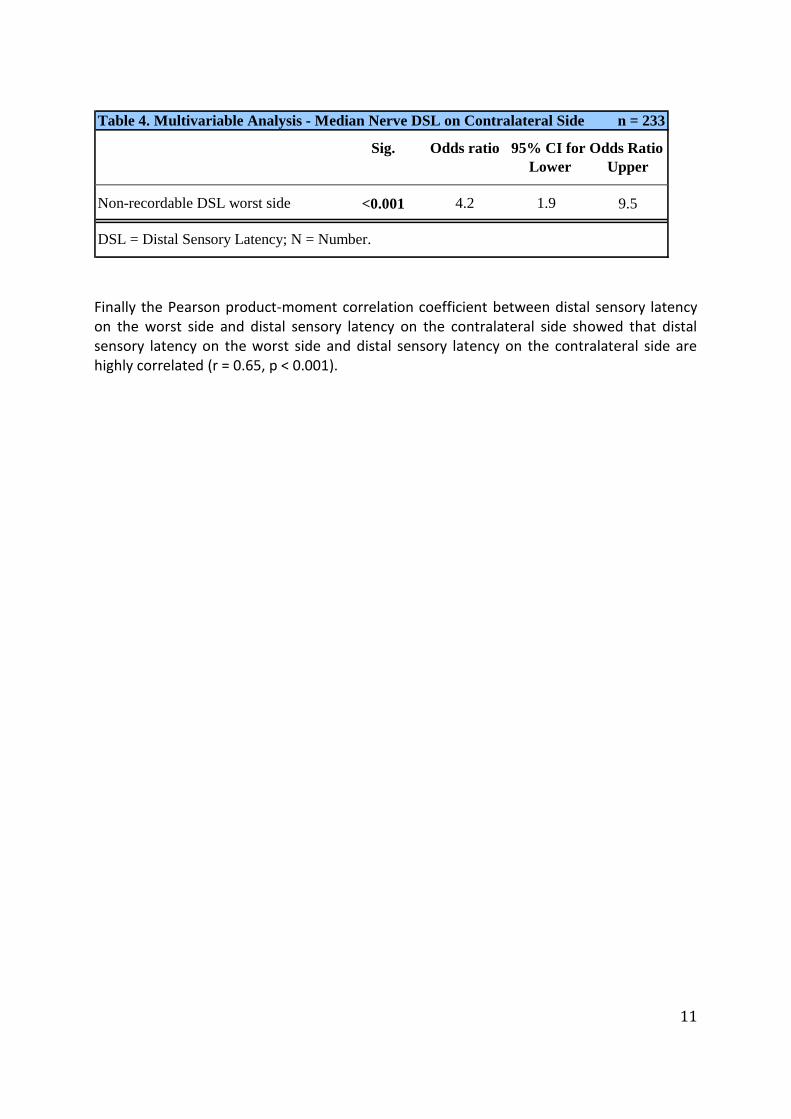
Age and non-recordable median nerve distal sensory latency of the worst side were entered into a multivariable logistic regression model. The best model only included non-recordable median nerve distal sensory latency of the worst side, which significantly contributed to the model (p = <0.001), and explained 9% of the variance in abnormal median nerve distal sensory latency on the contralateral side (Table 4).
11
n = 233
Sig. Odds ratio
Lower Upper
Non-recordable DSL worst side <0.001 4.2 1.9 9.5
Table 4. Multivariable Analysis - Median Nerve DSL on Contralateral Side
95% CI for Odds Ratio
DSL = Distal Sensory Latency; N = Number.
Finally the Pearson product-moment correlation coefficient between distal sensory latency on the worst side and distal sensory latency on the contralateral side showed that distal sensory latency on the worst side and distal sensory latency on the contralateral side are highly correlated (r = 0.65, p < 0.001).

12
Discussion To determine whether worsening of median nerve distal sensory latency conduction on patient’s worst side is associated with the occurrence of electrodiagnostic findings suggestive of carpal tunnel syndrome on the contralateral side 233 electrodiagnostic test reports were analyzed. This showed a significant difference in the severity of median nerve distal sensory latency on the contralateral side between patients with a prolonged and non-recordable median nerve distal sensory latency on the worst side; 1) patients with a non-recordable median nerve distal sensory latency on their worst side are less likely to have a normal median nerve distal sensory latency on their contralateral side when compared to patients with a recordable median nerve distal sensory latency; 2) patients with a non-recordable median nerve distal sensory latency on their worst side are more likely to have a non-recordable median nerve distal sensory latency on their contralateral side when compared with patients with a recordable median nerve distal sensory latency. Therefore our null hypothesis, that patients with a non-recordable median nerve distal sensory latency on electrodiagnostic testing of their worst side would be equally likely to have impairment of median nerve distal sensory latency conduction on the contralateral side when compared to patients with a recordable prolonged distal sensory latency on electrodiagnostic testing, was rejected.
Further statistical analysis showed that: 1) the occurrence of clinical symptoms on the contralateral side (76% in patients with a non-recordable median nerve distal sensory latency and 77% in patients with a prolonged median nerve distal sensory latency on the worst side) is about equal for the two groups; 2) median nerve distal sensory latency of the worst side was significantly associated with median nerve distal sensory latency on the contralateral side; 3) a multivariable logistic regression model including median nerve distal sensory latency of the worst side explains 9% of variance in abnormal median nerve distal sensory latency of the contralateral side; 4) median nerve distal sensory latency on the worst side and median nerve distal sensory latency on the contralateral side are highly correlated. This answers all of our secondary research questions. This study had several strenghts. First of all, all medical records and electrodiagnostic tests were reviewed by one research assistant who was not involved in patient care, thus minimizing intraobserver bias.
Secondly, all electrodiagnostic tests were conducted in one practice. And all the results of electrodiagnostic tests were reported in the same format, again minimizing bias.
Lastly this study had adequate power. Two-hundred-and-thirty-three patients were analyzed, almost three times as much as needed according to our power analysis. Potential shortcomings of this study include the reliance on medical records. As with all retrospective medical record review studies, the reliability of the information collected is dependent on how accurate the information was noted in the medical records. Reviewed records were from different doctors and from different departments with variation in the documentation of the visit.
Another limitation of this study is that we focused on the median nerve distal sensory latency rather than the overall electrodiagnostic findings. As a result we possibly excluded some patients from our study who would have been included if we had based our

13
electrodiagnostic test criteria on multiple outcomes, e.g., including mixed median median nerve and median distal motor latency. However there are number of arguments that justify the use of median nerve distal sensory latency. First of all, median nerve distal sensory latency is the most important factor with the highest predictive value (11). Secondly, it greatly simplified the analysis. Finally, we did not want to include patients based on the diagnosis of CTS made by different electrodiagnostic test specialists who all use individual cut off values for the different electrodiagnostic tests.
A third shortcoming is the absence of unilaterally tested patients, these patients may represent a group of patients who may be less likely to have abnormalities in electrodiagnostic testing on their contralateral side.
Also, this study’s percentages of bilateral symptoms and abnormal findings on electrodiagnostic testing of the contralateral should be interpreted in light of the fact that electrodiagnostic tests are typically obtained in patients considering surgery in our practice setting. This may have caused the spectrum to be towards more severe disease.
And lastly because of the retrospective nature of this study and the use of cross sectional data, prognostic and causal relationships should be drawn with caution. The reported occurrence of bilateral carpal tunnel syndrome related symptoms averages 60% (9, 11-16), although widely varying percentages of the occurrence have been reported, ranging from 22% to 87% (17, 10). In our study, the occurrence of bilateral carpal tunnel syndrome related symptoms was 76%, which was at the higher end of the earlier reported range.
The percentage of electrodiagnostic abnormalities of the contralateral side reported by other studies averages about 50% (range, 38% to 57%) (9-11). The three studies that looked at bilateral electrodiagnostic abnormalities defined the contralateral side as the asymptomatic or less severely affected hand based on clinical symptoms (9-11) while our study based the definition of the contralateral side on electrodiagnostic testing, and therefore a clear comparison cannot be made.
The main focus of our study was to determine whether the severity of median nerve distal sensory latency of the worst side was associated with abnormalities on electrodiagnostic testing suggestive of carpal tunnel syndrome of the contralateral side and to determine predictors of abnormal electrodiagnostic testing of the contralateral side. Our results suggest that the more severe carpal tunnel syndrome of the worst side on electrodiagnostic testing, the more likely electrodiagnostic abnormalities consistent with carpal tunnel syndrome will be present on the contralateral side and the more advanced it will be on the contralateral side. This is in line with the only three studies (9-11) that have specifically investigated bilateral carpal tunnel syndrome. They suggest in their conclusions that carpal tunnel syndrome is in almost all cases a bilateral disorder and that unilateral carpal tunnel syndrome cases will probably become bilateral. Because of the difference in research design between our study and these three studies further comparisons of results cannot be reliably made.

14
Conclusion Overall, 73% of patients have abnormal electrodiagnostic findings of their contralateral side compared to an even higher percentage of 89% of patients with a non-recordable median nerve distal sensory latency. These findings are in line with the notion that carpal tunnel syndrome is a structural, genetically mediated disorder that inevitably will become bilateral and inevitably progresses (9,10). Distal sensory latency on the worst side and distal sensory latency on the contralateral side are highly correlated. Patients with a non-recordable median nerve distal sensory latency on their worst side were significantly more likely to have abnormal electrodiagnostic testing on their contralateral side than patients with a prolonged median nerve distal sensory latency on their worst side. In short, the more severe the disease, the more likely it will be present on the contralateral side and the more advanced it will be on the contralateral side. Even though patients with non-recordable median nerve sensory latency on their worst side are more likely to have abnormalities on electrodiagnostic testing of their contralateral side compared to patients with prolonged median nerve sensory latency on their worst side, the occurrence of clinical symptoms on the contralateral side is about equal in patients with a non-recordable or prolonged median nerve distal sensory latency (76% versus 77%, respectively). Said in another way, 66 of 74 patients (89%) with a non-recordable median nerve distal sensory latency had electrodiagnostic evidence of contralateral carpal tunnel syndrome, but 10 of 66 patients (15%) had no symptoms.
This lack of correspondence between pathophysiology and symptoms means that we cannot rely on patient reports to gauge the presence or severity of disease. Other studies have also demonstrated the lack of correlation between electrodiagnostic findings and patients’ carpal tunnel syndrome related symptoms (12). This is particularly important for a disease that seems inevitably progressive and leads to permanent damage of a very important nerve. When a patient presents with unilateral symptoms and the median nerve distal sensory latency is non-recordable, the patient should be educated about the risk of carpal tunnel syndrome on the contralateral side, even if there are no symptoms. We advocate bilateral testing of patients being considered for surgery in order to make them aware of the disease on the other side. These steps could prevent patients from coming in later with severe, advanced median nerve damage for which surgery will likely not be beneficial.

15
References 1. Atroshi I, Gummesson C, Johnsson R, Ornstein E, Ranstam J, Rosen I. Prevalence of carpal tunnel
syndrome in a general population. JAMA. 1999 Jul 14;282(2):153-8.
2. Foley M, Silverstein B, Polissar N. The economic burden of carpal tunnel syndrome: long-term
earnings of CTS claimants in Washington State. Am J Ind Med. 2007 Mar;50(3):155-72.
3. Gelberman RH, Rydevik BL, Pess GM, Szabo RM, Lundborg G. Carpal tunnel syndrome. A scientific
basis for clinical care. Orthop Clin North Am. 1988 Jan;19(1):115-24.
4. Mackinnon SE. Novak CB. Compression Neuropathies. In: Wolfe SW, Hotchkiss RN, Pederson WC,
Kozin SH, eds. Green's operative hand surgery. Vol 2. Philadelphia: Elsevier; 2011: 977-1092.
5. Luchetti R, Schoenhuber R, De Cicco G, Alfarano M, Deluca S, Landi A. Carpal-tunnel pressure. Acta
Orthop Scand. 1989 Aug;60(4):397-9.
6. Cantatore FP, Dell'Accio F, Lapadula G. Carpal tunnel syndrome: a review. Clin Rheumatol. 1997
Nov;16(6):596-603.
7. Atcheson SG, Ward JR, Lowe W. Concurrent medical disease in work-related carpal tunnel syndrome.
Arch Intern Med. 1998 Jul 27;158(14):1506-12.
8. Lozano-Calderon S, Anthony S, Ring D. The quality and strength of evidence for etiology: example of
carpal tunnel syndrome. J Hand Surg Am. 2008 Apr;33(4):525-38.
9. Bagatur AE, Zorer G. The carpal tunnel syndrome is a bilateral disorder. J Bone Joint Surg Br. 2001
Jul;83(5):655-8.
10. Padua L, Padua R, Nazzaro M, Tonali P. Incidence of bilateral symptoms in carpal tunnel syndrome. J
Hand Surg Br. 1998 Oct;23(5):603-6.
11. Bendler EM, Greenspun B, Yu J, Erdman WJ, 2nd. The bilaterality of carpal tunnel syndrome. Arch
Phys Med Rehabil. 1977 Aug;58(8):362-4.
12. Girlanda P, Dattola R, Venuto C, Mangiapane R, Nicolosi C, Messina C. Local steroid treatment in
idiopathic carpal tunnel syndrome: short- and long-term efficacy. J Neurol. 1993;240(3):187-90.
13. Kimura J. The carpal tunnel syndrome: localization of conduction abnormalities within the distal
segment of the median nerve. Brain. 1979 Sep;102(3):619-35.
14. Macdonell RA, Schwartz MS, Swash M. Carpal tunnel syndrome: which finger should be tested? An
analysis of sensory conduction in digital branches of the median nerve. Muscle Nerve. 1990 Jul;13(7):601-6.
15. Stevens JC. AAEE minimonograph #26: The electrodiagnosis of carpal tunnel syndrome. Muscle
Nerve. 1987 Feb;10(2):99-113.
16. White JC, Hansen SR, Johnson RK. A comparison of EMG procedures in the carpal tunnel syndrome
with clinical-EMG correlations. Muscle Nerve. 1988 Nov;11(11):1177-82.
17. Silverstein BA, Fine LJ, Armstrong TJ. Occupational factors and carpal tunnel syndrome. Am J Ind
Med. 1987;11(3):343-58.
18. D'Arcy CA, McGee S. The rational clinical examination. Does this patient have carpal tunnel
syndrome? JAMA. 2000 Jun 21;283(23):3110-7.
19. Pryse-Phillips WE. Validation of a diagnostic sign in carpal tunnel syndrome. J Neurol Neurosurg
Psychiatry. 1984 Aug;47(8):870-2.
20. Katz JN, Larson MG, Sabra A, Krarup C, Stirrat CR, Sethi R, et al. The carpal tunnel syndrome:
diagnostic utility of the history and physical examination findings. Ann Intern Med. 1990 Mar 1;112(5):321-7.
21. Jablecki CK, Andary MT, So YT, Wilkins DE, Williams FH. Literature review of the usefulness of
nerve conduction studies and electromyography for the evaluation of patients with carpal tunnel syndrome.
AAEM Quality Assurance Committee. Muscle Nerve. 1993 Dec;16(12):1392-414.
22. Werner RA, Andary M. Electrodiagnostic evaluation of carpal tunnel syndrome. Muscle Nerve. 2011
Oct;44(4):597-607.
23. Chan L, Turner JA, Comstock BA, Levenson LM, Hollingworth W, Heagerty PJ, et al. The relationship
between electrodiagnostic findings and patient symptoms and function in carpal tunnel syndrome. Arch Phys
Med Rehabil. 2007 Jan;88(1):19-24.
24. Robinson L, Kliot M. Stop using arbitrary grading schemes in carpal tunnel syndrome. Muscle Nerve.
2008 Jun;37(6):804.
25. Katz JN, Simmons BP. Clinical practice. Carpal tunnel syndrome. N Engl J Med. 2002 Jun
6;346(23):1807-12.
26. Celiker R, Arslan S, Inanici F. Corticosteroid injection vs. nonsteroidal antiinflammatory drug and
splinting in carpal tunnel syndrome. Am J Phys Med Rehabil. 2002 Mar;81(3):182-6.
27. Weiss AP, Sachar K, Gendreau M. Conservative management of carpal tunnel syndrome: a
reexamination of steroid injection and splinting. J Hand Surg Am. 1994 May;19(3):410-5.

16
28. Burke DT, Burke MM, Stewart GW, Cambre A. Splinting for carpal tunnel syndrome: in search of the
optimal angle. Arch Phys Med Rehabil. 1994 Nov;75(11):1241-4.
29. Chang MH, Chiang HT, Lee SS, Ger LP, Lo YK. Oral drug of choice in carpal tunnel syndrome.
Neurology. 1998 Aug;51(2):390-3.
30. Ayhan-Ardic FF, Erdem HR. Long-term clinical and electrophysiological results of local steroid
injection in patients with carpal tunnel syndrome. Funct Neurol. 2000 Jul-Sep;15(3):157-65.
31. Dammers JW, Veering MM, Vermeulen M. Injection with methylprednisolone proximal to the carpal
tunnel: randomised double blind trial. BMJ. 1999 Oct 2;319(7214):884-6.
32. Gelberman RH, Aronson D, Weisman MH. Carpal-tunnel syndrome. Results of a prospective trial of
steroid injection and splinting. J Bone Joint Surg Am. 1980 Oct;62(7):1181-4.
33. Giannini F, Passero S, Cioni R, Paradiso C, Battistini N, Giordano N, et al. Electrophysiologic
evaluation of local steroid injection in carpal tunnel syndrome. Arch Phys Med Rehabil. 1991 Sep;72(10):738-
42.
34. Phalen GS. The carpal-tunnel syndrome. Seventeen years' experience in diagnosis and treatment of six
hundred fifty-four hands. J Bone Joint Surg Am. 1966 Mar;48(2):211-28.
35. Sternbach G. The carpal tunnel syndrome. J Emerg Med. 1999 May-Jun;17(3):519-23.
36. Agee JM, McCarroll HR, Jr., Tortosa RD, Berry DA, Szabo RM, Peimer CA. Endoscopic release of the
carpal tunnel: a randomized prospective multicenter study. J Hand Surg Am. 1992 Nov;17(6):987-95.
37. Brown RA, Gelberman RH, Seiler JG, 3rd, Abrahamsson SO, Weiland AJ, Urbaniak JR, et al. Carpal
tunnel release. A prospective, randomized assessment of open and endoscopic methods. J Bone Joint Surg Am.
1993 Sep;75(9):1265-75.
38. Katz JN, Keller RB, Simmons BP, Rogers WD, Bessette L, Fossel AH, et al. Maine Carpal Tunnel
Study: outcomes of operative and nonoperative therapy for carpal tunnel syndrome in a community-based
cohort. J Hand Surg Am. 1998 Jul;23(4):697-710.
39. Fehringer EV, Tiedeman JJ, Dobler K, McCarthy JA. Bilateral endoscopic carpal tunnel releases:
Simultaneous versus staged operative intervention. Arthroscopy. 2002 Mar;18(3):316-21.
40. Wang AA, Hutchinson DT, Vanderhooft JE. Bilateral simultaneous open carpal tunnel release: a
prospective study of postoperative activities of daily living and patient satisfaction. J Hand Surg Am. 2003
Sep;28(5):845-8.
41. Nesbitt KS, Innis PC, Dubin NH, Wilgis EF. Staged versus simultaneous bilateral endoscopic carpal
tunnel release: an outcome study. Plast Reconstr Surg. 2006 Jul;118(1):139-45; discussion 46-7.
42. Pagnanelli DM, Barrer SJ. Bilateral carpal tunnel release at one operation: report of 228 patients.
Neurosurgery. 1992 Dec;31(6):1030-3; discussion 3-4.
43. Weber RA, Boyer KM. Consecutive versus simultaneous bilateral carpal tunnel release. Ann Plast Surg.
2005 Jan;54(1):15-9.
44. Huracek J, Heising T, Wanner M, Troeger H. Recovery after carpal tunnel syndrome operation: the
influence of the opposite hand, if operated on in the same session. Arch Orthop Trauma Surg. 2001
Jul;121(7):368-70.
45. Stanek EJ, 3rd, Pransky G. Unilateral vs. bilateral carpal tunnel: challenges and approaches. Am J Ind
Med. 1996 Jun;29(6):669-78.
46. Yoon ES, Kwon HK, Lee HJ, Ahn DS. The outcome of the nonoperated contralateral hand in carpal
tunnel syndrome. Ann Plast Surg. 2001 Jul;47(1):20-4.
47. Afshar A, Yekta Z, Mirzatoluei F. Clinical course of the non-operated hand in patients with bilateral
idiopathic carpal tunnel syndrome. J Hand Surg Am. 2007 Oct;32(8):1166-70.
17
Addendum Figure 1. Anatomy Carpal Tunnel
Figure 2. CTS Etiologies (information from reference 7)
Primary
Secondary
Mechanic
Exposure to hard work with the hands and repetitive wrist movements and vibration
Excessive fat within the CT
Fractures and anomalies of the carpal bones
Inflammatory
Non-specific flexor tenosynovitis
Rheumatoid arthritis and other inflammatory joint diseases of the wrists
Connective tissue diseases (Sjogren’s syndrome, scleroderma)
Tophaceous gout and pseudogout

18
Infectious
Septic arthritis of the wrist or tenosynovitis
Mycobacterial infections
Lyme borreliosis
Metabolic
Diabetes
Hyper- and hypothyroidism
Acromegaly
Anatomic
Proximal origin of lumbrical muscles often associated with muscular hypertrophy
Aberrant muscles and other muscular alterations
Anomalous flexor tendons
Cysts and cyst like structures
Bifid median nerve
Persistence of the median artery and other vascular variants
Congenital
Congenital bone diseases (osteoporosis)
Thesaurimoses (Hunter’s syndrome, Hurler’s syndrome)
Pachydermoperiostosis
Vascular
Thromboses
Vasculitis
Aneurysms
Haemorrhages
Space occupying masses
Lipomas
Osteochondromas
Fibromas
Others
Pregnancy
Contraceptive pills
19
Menopause and after òophorectomy
Haemodialysis
Primary and secondary amyloidosis
Paraplegia
Idiopathic torsion dystonia
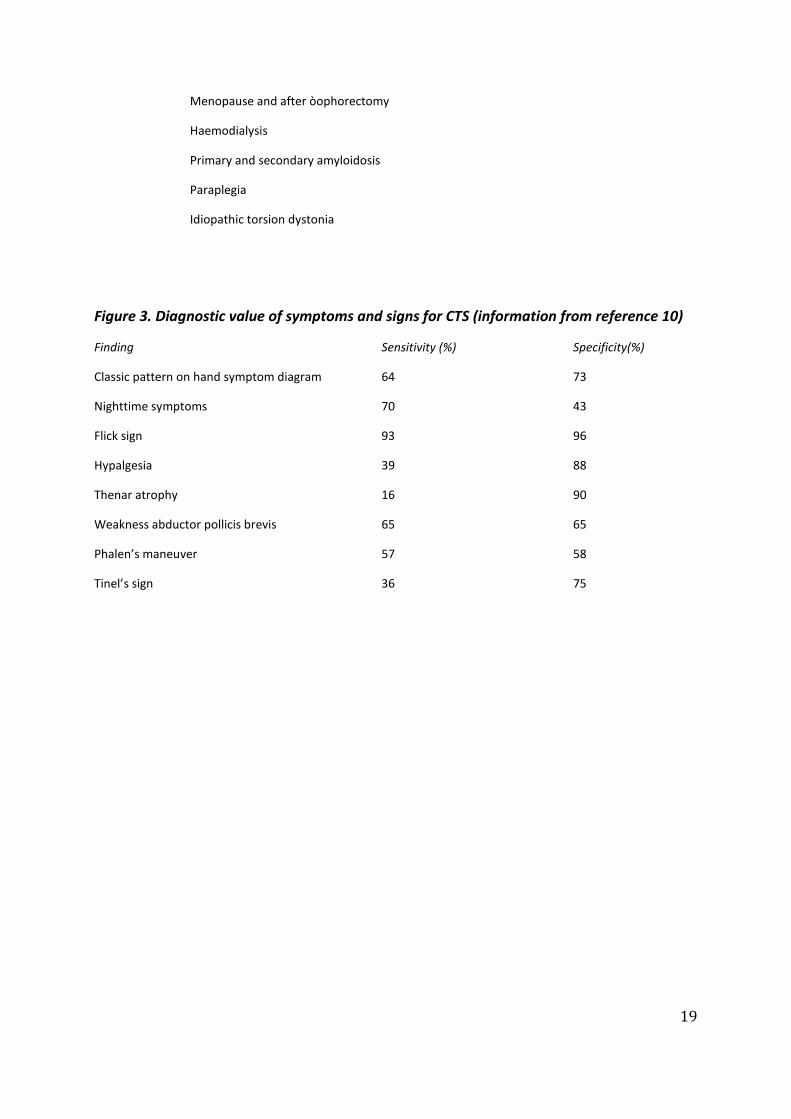
Figure 3. Diagnostic value of symptoms and signs for CTS (information from reference 10)
Finding Sensitivity (%) Specificity(%)
Classic pattern on hand symptom diagram 64 73
Nighttime symptoms 70 43
Flick sign 93 96
Hypalgesia 39 88
Thenar atrophy 16 90
Weakness abductor pollicis brevis 65 65
Phalen’s maneuver 57 58
Tinel’s sign 36 75