emergency care research in sheffield/file/mason-et-al... · ... school of health ... respiratory...
TRANSCRIPT

Emergency Care Research in Sheffield
Steve Goodacre: Professor of Emergency MedicineEmma Knowles: Research FellowSuzanne Mason: Professor of Emergency Medicine
Health Services Research, School of Health and Related Research

Why ScHARR?• Multi-disciplinary expertise in health services research which is providing an evidence base for healthcare delivery and organisation nationally and internationally
• Access to economists, modellers, statisticians, information technologists, trial managers, data experts, researchers and other healthcare professionals
• Stimulating, successful and creative environment to support this type of research


Collaboration
• Interdepartmental: IWP, Information Sciences, Clinical Psychology, Faculty of medicine
• Academic institutions: Swansea, Bristol, Manchester, Leicester, Leeds
• NHS organisations: Acute trusts, ambulance services and PCTs
• International: Ottawa, San Francisco, Melbourne, Hong Kong, Toronto

Training
• Medical undergraduates: BMedSci, SSC
• Medical Graduates: FY2, ACF and ACL posts, trainees in emergency medicine
• Postgraduate research: MD, MPhil, PhD
• Allied Health Professionals: MClinRes

Portfolio of Sheffield Research• Funding over last 5 years: >£6million
• Examples of impact…

10 acute trusts in England
NIAPP Project

112 acute trusts in England
UWAIT Study

Data from 83 Emergency
Departments in England
Impact of imposed targets

21 acute trusts;
3 ambulance services
England
Impact of Service Redesign

• 3Mg: Randomised trial of IV and nebulised magnesium sulphate in acute severe asthma (HTA, £1m)
• EDiT Study: Evaluation of junior doctor performance and competence in UK EDs (NIHR, £500K)
• DAVROS: Development and evaluation of risk-adjusted outcomes for emergency care (MRC, £900K)
• SAFETIME Project: Effect of four-hour emergency department target on patient care (BUPA, £52K)
Current research

• AHEAD Study: Outcomes following head injury in anticoagulated patients (RfPB, £250K)
• SAFER2 Trial: prehospital management of elderly fallers (HTA, £150K)
• PAINTED: Pandemic Influenza Triage in the ED (HTA, £150K)
• HITS-NS: Head Injury Transportation Straight to Neurosurgery (HITS-NS) trial - a feasibility study (HTA, £500K)
• Systematic Review of clinical outcome and cost effectiveness comparing a policy of triage and direct transfer to specialist centres with delivery to local hospital (SDO, £150K)
Current research

Bids in preparation / submission
• Decision making and safety in emergency care transitions (NIHR SDO - submitted)
• Ambulance calls for self-harm: exploring responses to people not transported to hospital (RfPB – in prep)
• Making patient handover safe – an electronic solution (SDO – in prep)
• Impact of the Electronic Patient Report Form (ePRF) on Ambulance Service Performance (SDO – in prep)

Bids in preparation / submission
• Developing outcome measures for pre-hospital care (NIHR £2m Programme- full proposal submitted)
• Cost-effectiveness of diagnostic strategies for ACS (HTA – funding agreed)
• RATPAC-CBE: Randomised Assessment of Treatment using Panel Assay of Cardiac markers –Contemporary Biomarker Evaluation (HTA – funding agreed)
• Ambulance-based lab-on-a-chip point-of-care cardiac marker testing (MRC – outline submitted)
• The ACUTE trial: Ambulance CPAP: Use, Treatment effect and Economics (HTA – outline submitted)
• ESETT: Established status epilepticus treatment trial(HTA – outline submitted)

A multicentre, randomised controlled trial of non invasive ventilation (CPAP or NIPPV)
versus standard therapy for acute cardiogenic pulmonary oedema (ACPO)
ISRCTN07448447
The 3CPO Trial

Acute Cardiogenic Pulmonary Oedema
• Common: 15-
20,000 hospital
admissions per
annum in UK
• Deadly: 10% in-
hospital mortality
• Costly: 6.5 million
hospital days per
annum in USA

Acute Cardiogenic Pulmonary Oedema
• Loop Diuretic Therapy
• Nitrate Therapy
• Oxygen Therapy
• (Opiates)
• Treat Underlying Cause

Non-invasive Ventilation in Acute Cardiogenic Pulmonary Oedema
“When the household vacuum cleaner is employed, the machine should be run for some minutes first of all to get
rid of dust”Poulton EP, Oxon DM: Left-sided heart failure with pulmonary oedema: Its treatment with the "pulmonary plus pressure machine." Lancet (1936);231:981-983.

Non-invasive VentilationIn Acute Cardiogenic Pulmonary Oedema
Non-invasive Ventilation:
• Continuous Positive Airway Pressure (CPAP) Ventilation
• Non-invasive Intermittent Positive Pressure Ventilation (NIPPV)

Mortality reducedfrom 22% to 11%
RR 0.53(95% CI 0.35-0.81)
(Individual GroupSizes of
n = 9 to 46)
Masip et al. JAMA 2005;294:3124-3130
Mortality Benefit of CPAP/NIPPV in Patients with ACPO

Aims and Hypothesis
In patients with acute cardiogenic Pulmonary oedema:
Aims
• Effectiveness of non-invasive ventilation• Comparative effectiveness of CPAP and NIPPV

Trial Design• Multicentre national randomised controlled trial
• Setting: Emergency Department
• Prospective non-blinded trial
• Three treatment interventions in a 1:1:1 randomisation: ‘standard’ oxygen therapy, CPAP or NIPPV

26 Emergency Departments

Results

Trial Treatment
Standard CPAP NIPPV P-value
Treatment allocated 367 346 356
Completed allocated treatment
298/363 (82.1%)
285/340 (83.8%)
267/352 (75.9%)
0.020
Reason not completed
Not tolerated 1 (0.3%) 18 (5.2%) 30 (8.4%) <0.001
Worsening ABGs 26 (7.1%) 10 (2.9%) 15 (4.2%) 0.027
Respiratory distress 31 (8.4%) 5 (1.4%) 12 (3.4%) <0.001
Other reason 18 (4.9%) 24 (6.9%) 25 (8.1%) 0.209
N (%)

Physiological Response to Intervention
One Hour Physiology
Standard therapy
CPAP or NIPPV
P Value
(t-test)
Decrease in pulse rate (/min) 13 16 0.004
Decrease in systolic BP (mmHg) 34 38 0.167
Decrease in diastolic BP (mmHg) 22 22 0.949
Decrease in respiratory rate (/min)
7.1 7.2 0.740
Increase in oxygen Saturation (%) 3.5 3.0 0.412
Increase in arterial pH 0.08 0.11 <0.001
Increase in arterial pO2 (kPa) 0.7 -0.6 0.068
Decrease in arterial pCO2 (kPa) 0.8 1.5 <0.001
Increase in bicarbonate (mmol/L) 1.7 1.8 0.767
Mean±SD

Breathlessness10cm VAS
• Baseline: 657 patients, mean score 8.9 (SD 1.6)
• One hour: 612 patients, mean score 4.6 (SD 3.0)
• Change: 535 patients, mean decrease 4.3 (SD 3.0)
• NIV =4.6; standard=3.9
• Difference=0.7; 95% CI 0.2 to 1.3; p=0.008
• CPAP=4.7; NIPPV=4.5
• Difference=0.2; 95% CI -0.4 to 0.8; p=0.520

Primary OutcomeAny NIV v standardMortality
• 7-day mortality: any NIV=9.5%, standard=9.8%
• OR for 7-day mortality, any NIV versus standard treatment = 0.97 (95% CI 0.63 to 1.48; p=0.869)
• 30-day mortality: any NIV=15.2%, standard=16.4%
• OR for 30-day mortality, any NIV versus standard
treatment = 0.92 (95% CI 0.64 to 1.31; p=0.637)

Primary OutcomeCPAP v NIPPV
Mortality
• 7-day mortality: CPAP=9.6%, NIPPV=9.4%
• OR for 7-day mortality, NIPPV versus CPAP = 0.97 (95% CI 0.58 to 1.61; p=0.912)
• 30-day mortality: CPAP=15.4%, NIPPV=15.1%
• OR for 30-day mortality, NIPPV versus CPAP = 0.98 (95% CI 0.64 to 1.49; p=0.923)

In patients with acute cardiogenic pulmonary oedema, non-invasive ventilation:
• Produces more rapid resolution of metabolic abnormalities and respiratory distress
• Has no major effect on 7-day or 30-day mortality
Conclusions




Why did 3CPO differ from previous studies?
• Patient selection
• Pragmatic trial
• Standard treatment included option of NIV if treatment failure
Optimal treatment for ACPO is probably oxygen, diuretics and nitrates followed by NIV if there is no response to treatment
Interpretation

A Randomised Controlled Trial to Evaluate the Effectiveness of Community Paramedic Practitioners Managing Older People Calling the Emergency Medical Services with Minor Acute Illness
ScHARR: Suzanne Mason, Emma Knowles, Brigitte Colwell, Jon Nicholl, Simon Dixon
Department of Emergency Medicine, Sheffield Teaching Hospitals: Suzanne Mason, Jim Wardrope, Julie Perrin
South Yorkshire Ambulance Service: Jim Wardrope, Rob Gorringe

• Increasing annual attendances at Emergency Departments
• 16% in 10 years
• Increasing use of ambulance service
• 50% last 10 years
• Increasing older population
• Maximising skills of workforce
Why Change?

The New Service
• Developed by South Yorkshire Ambulance Service (PPOPs)
• Provision of community-based clinical assessment for patients >60 years with minor acute conditions
• Operated by experienced paramedics with extended skills
• Between 0800-2000 each day
• 999 / GP urgent call with specific conditions activates response
• Modified cars to transport patients to ED
Practical Skills
• Local anaesthetic techniques, wound care, suturing & dressings
• Joint examination
• Neurological, ENT, cardiovascular, respiratory system examination
• Xray requests
• Protocol-led dispensing
• Mobility and social needs assessment
• Referral pathways: ED,GP, District Nurse, community social services.
Design
• Cluster randomised controlled trial
• Weeks randomised to the PP service being active or inactive
• Patients identified by PP in ambulance control room
• Patients included if condition could be assessed by PP
• Recruited by PP at initial consultation
• 3 and 28 day patient follow-up (postal survey, clinical notes, routine data)

Study Aims
• Differences in experiences and satisfaction with the management of acute minor conditions by community Paramedic Practitioners when compared to the existing standard service
• Assess clinical and cost effectiveness of community Paramedic Practitioners in the management of older people with acute minor conditions compared with existing standard service.
Main Outcome Measures
• ED attendance/hospital admission between 0 and 28 days
• Patient time from 999 call to completion of the initial care episode
• Patient satisfaction with service received
• Investigation/Treatment received
• Mortality at 28 days
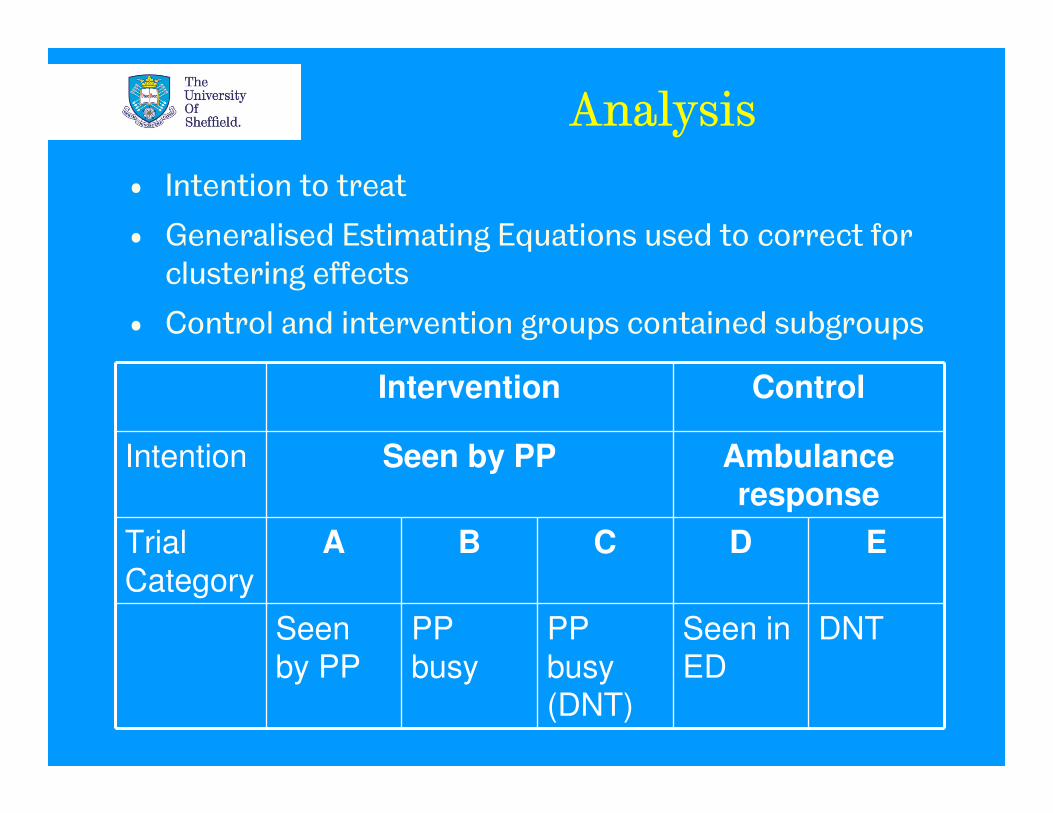
Analysis
• Intention to treat
• Generalised Estimating Equations used to correct for clustering effects
• Control and intervention groups contained subgroups
Intervention Control
Intention Seen by PP Ambulance response
Trial
Category
A B C D E
Seen
by PP
PP
busy
PP
busy (DNT)
Seen in
ED
DNT

Eligible patients (n=4175)
Identified post incident by
research team (n=179)
Randomised (n=3996) into 56 clusters
Intervention n=2087 (30 clusters)
Control n=1909(26 clusters)
Consented for study, n=1549
Lost to follow up n=440:Repeat patients (n=263)Died pre-consent (n=11)Refused (n=41)Other reason (n=125)
Lost to follow up n=538:Repeat patients (n=343)Died pre-consent (n=19)Refused (n=16)Other reason (n=160)
Consented for study, n=1469

Primary Outcomes
Intervention Control RR (95% CI’s) P value
ED attendance 0-28 days (n=3018)
970 (62.6) 1286 (87.5) 0.72 (0.68 to 0.75)
<0.001
Hospital admission 0-28 days (n=3018)
626 (40.4) 683 (46.5) 0.87 (0.81 to 0.94)
<0.001
Very satisfied with care (n=1482)
656 (85.5) 528 (73.8) 1.16 (1.09 to 1.23)
<0.001
Mean (SD) total episode time (min) (n=2968)
235.1 (183.3) 277.8 (182.6)
-42.2 (SE 8.8) (-59.5 to -
25.0)
<0.001
*ICC at 0.00

*ICC at 0.00
Intervention Control RR (95% CI’s) P value
Investigation at
initial episode
(n=2946)
754 (48.7) 971 (66.1) 0.73 (0.69 to 0.78)
<0.001
Treatment at
initial episode
(n=2946)
1233 (79.6) 1040 (70.8) 1.11 (1.06 to 1.17)
<0.001
Physical health ‘worse’ (n=1430)
166 (21.7) 170 (25.6) 0.85 (0.69 to 1.05)
0.13
Mortality at 28 days (n=3018)
68 (4.4) 74 (5.0) 0.87 (0.63 to 1.21)
0.41
Secondary Outcomes

Costs from Routine Data
Item Intervention
Mean*
n=1446
Control
Mean*
n=1408
Mean difference
(95% CI of difference)**
Paramedic practitioner 73 0 +73 (+70 to +76)
Other responders 155 232 -77 (-88 to -66)
ED/MIU attendance 46 78 -32 (-38 to -26)
Inpatient stay for same
day episodes
2696 3188 -490 (-1024 to +44)
Assessments 8 8 +0 (-2 to +3)
Subsequent secondary
care contacts
44 38 +6 (-1 to +12)
Subsequent inpatient
stays
944 572 +374 (+103 to +644)
Total cost 3966 4116 -140 (-694 to +415)
*Actual mean
** Adjusted estimates

Main Findings
• Reduced overall ED attendance and hospital admission
• Reduced rates of initial investigation, shorter episode times
• Patient satisfaction high
• Safe service: no differences in physical health or mortality
• Reduced costs

Publications
• Cost effectiveness: EMJ 2009
• Safety of the service: Academic Emergency Medicine 2008
• Impact on carers: EMJ (in press)

Impact
• National recognition: Health and Social Care Awards (emergency care). DHQuality and Safety in Health Care Award (community care). BMJDepartment of Health award for the Highest quality research. 999 EMS Forum
• International service development (Canada and New Zealand)
• Pre-cursor to the national ECP scheme
• Further research opportunities: NEECaP: clinical and cost effectiveness of ECPs
Safer2: new protocols for paramedics in assessment of fallers


Future Plans
PPI group
International
profile
