ent 00 march 22
TRANSCRIPT
Head & Neck PathologyHead & Neck PathologyOTOLARYNGOLOGYOTOLARYNGOLOGY
March. 29. 2015

Nasopharynx
Oropharynx
Laryngopharynx
Soft Palate
Epiglottis
Esophagus
ENT

Oropharynx
• Viral
• Bact. Infection (Pharyngitis).
- B H Strept.• Tonsillitis
- Peritonsilar abscess “Quinsy”
- GN, & RH H Dis.
• Laryngitis- TB- Diphtheritic pharyngitis.• Tumors of tonsilsTumors of tonsils

Pharyngitis

Tonsillitis & peritonsillar abscess “Quinsy”
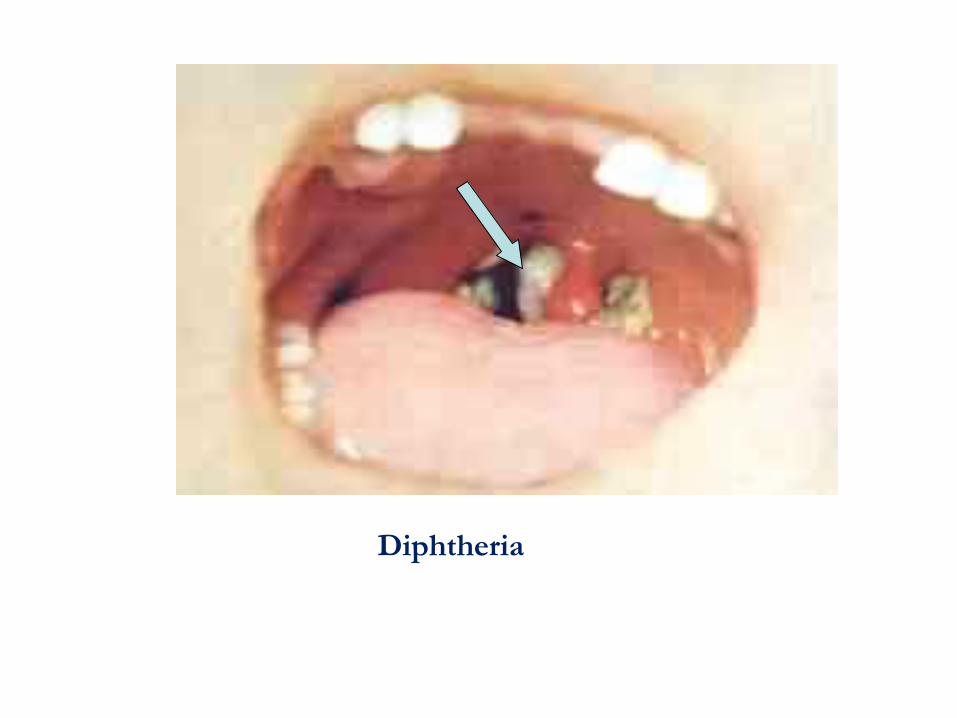
Diphtheria

“UPPER” AIRWAYS
• NOSE: Inflammation, Tumors• NASOPHARYNX: Inflammation, Tumors• PARANASAL SINUSES: Inflammation,
Tumors• LARYNX: Inflammation, Tumors

Nose
Skin of the nose;• DLE• Sebaceous hyperplasia• BCCa.
Nasal #; • Hematoma• Deviation of septum• Deviation of nose.

Nose
• Rhinitis
• Sinusitis• Epistaxis Benign nasal tumors;• Hemangioma
• Juvenile Angiofibroma
• Papilloma.• Sq & Trans. Cell ca.

Rhinitis/Sinusitis
• Very often allergic.• Very often associated with URI’s, usually
viral• about every organism has been implicated
at one time or another, bacteria, virus, fungus, etc.

NOSE/SINUS/NASOPHARYNX“TUMORS”
• “Polyps”---really NOT a tumor• Angiofibroma• Papilloma• Neuroblastoma
• Nasopharyngeal Carcinoma

INFLAMMATORY “POLYPS” OF NASAL CAVITY


Necrotizing ulcerating lesions of URT:• Acute fungal infections (e.g mucormycosis;, in
immunosuppressed patients) • Wegener granulomatosis • lethal midline granuloma and now known to be
a lymphoma of natural killer cells infected with EBV.

“NECROTIZING” Upper Airway Lesions
• “WEGENER” Granulomatosis• “Lethal” Midline Granuloma

PAPILLOMA “INVERTED” PAPILLOMA
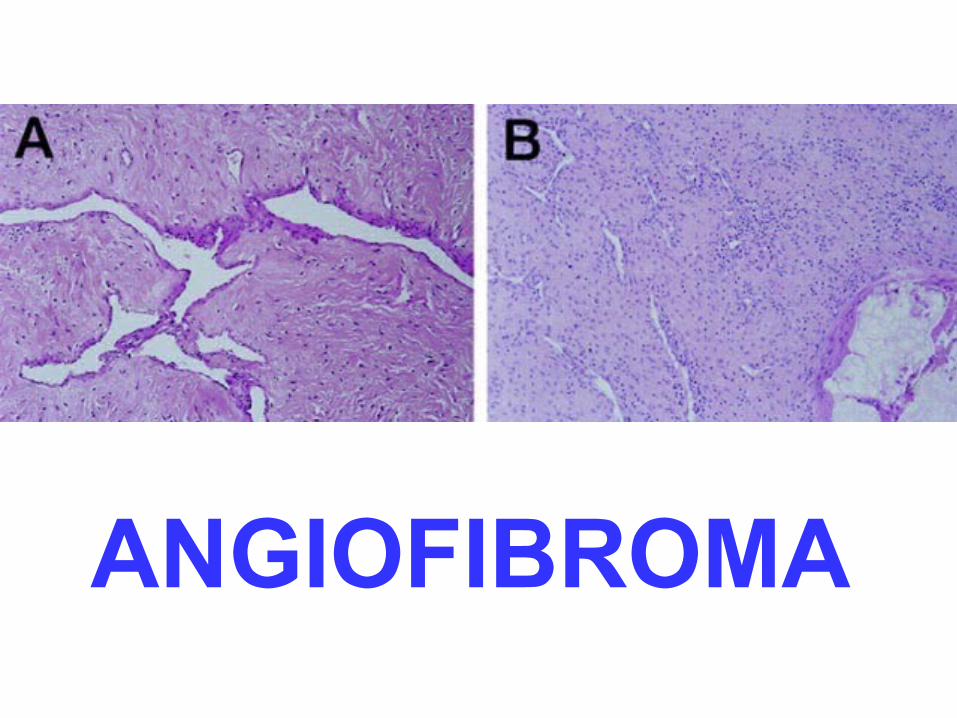
ANGIOFIBROMA

NEUROBLASTOMA(OLFACTORY)
ESTHESIONEUROBLASTOMA
ROSETTE

Nasopharyngeal carcinomas
• often clinically occult for long periods, • present as metastases in the cervical lymph
nodes in as many as 70% of the patients. • Radiosensitive
• 5 Year survival; 50% to 70%


Nasopharyngeal cancer

PET/CT Scan of a patient with nasopharyngeal cancer. Transverse slice demonstrating positive primary site

Undifferentiated nasopharyngeal Ca.
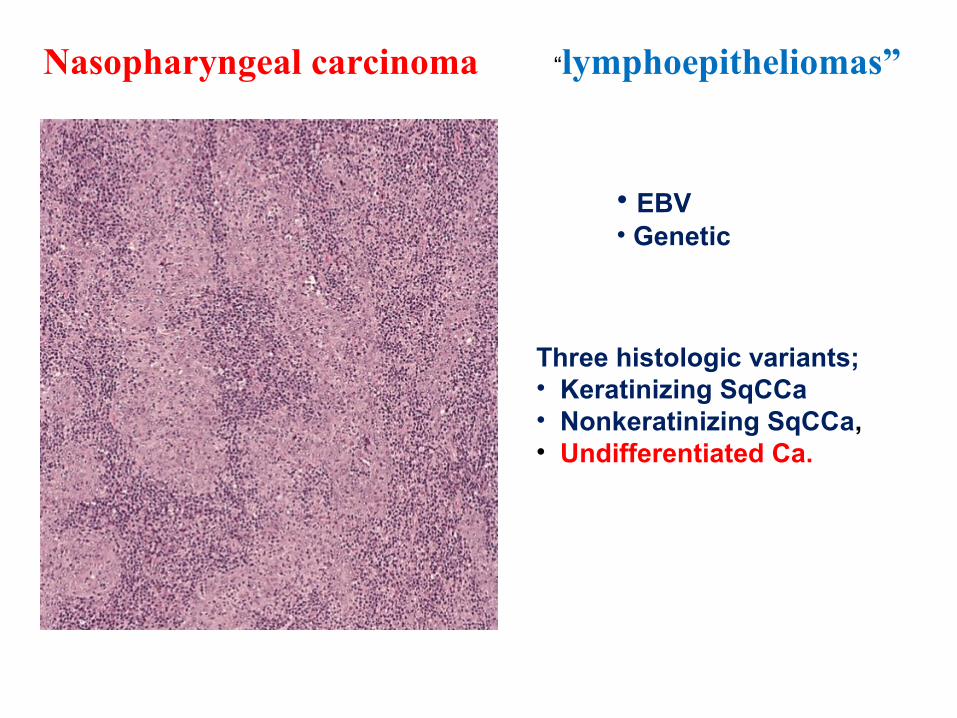
“lymphoepitheliomas”Nasopharyngeal carcinoma
Three histologic variants;• Keratinizing SqCCa• Nonkeratinizing SqCCa,• Undifferentiated Ca.
• EBV• Genetic

NASOPHARYNGEALCARCINOMA

The Larynx
Vocal Cord
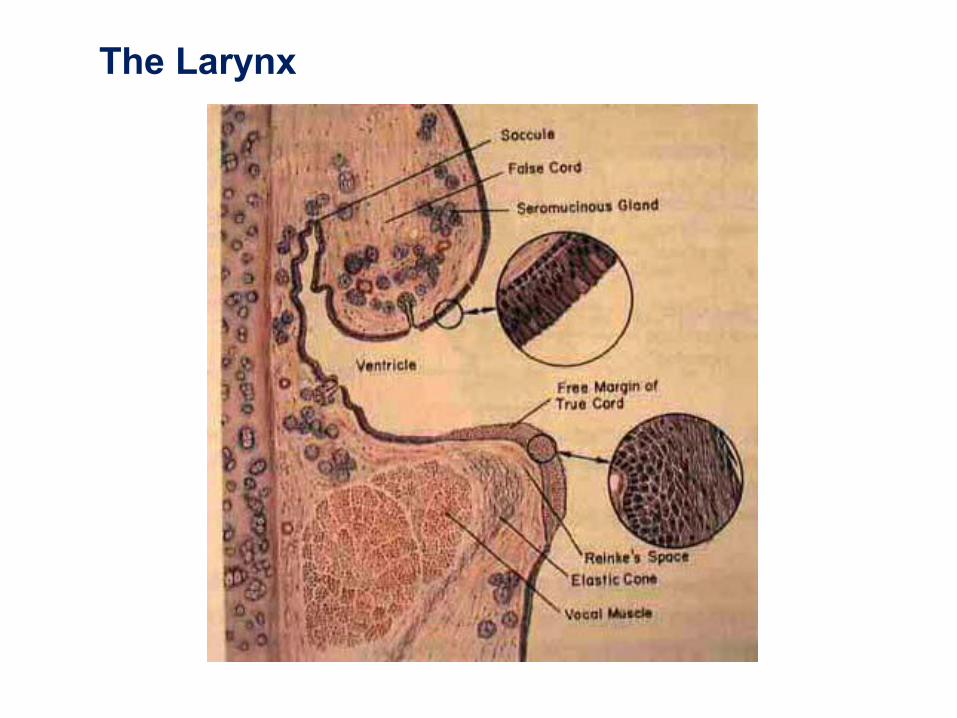
The Larynx
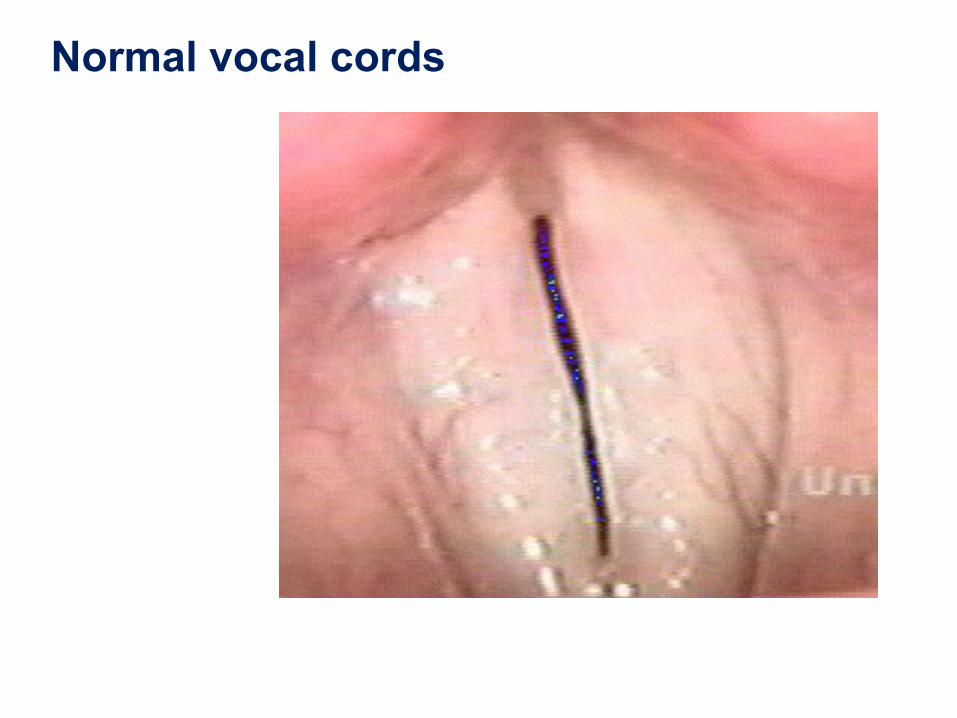
Normal vocal cords

LARYNGITIS
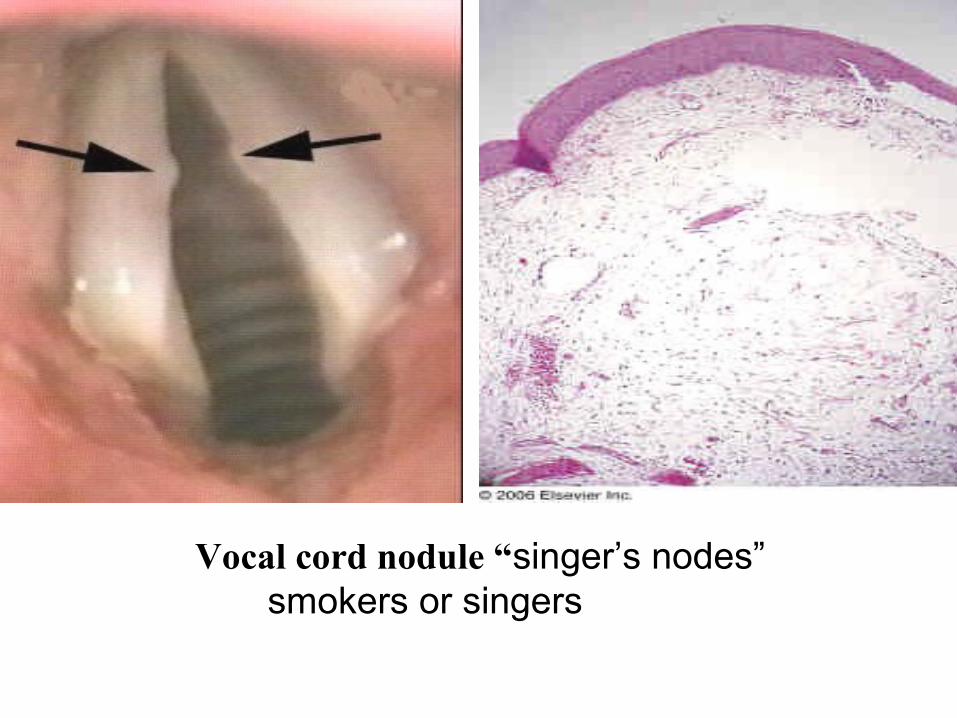
Vocal cord nodule “singer’s nodes” smokers or singers

Nodules• bilateral symmetric
epithelial swelling of ant/mid third of TVF
• More in children, adolescents, females – softer intensity
of voice causes hyperfunction
• Result of abuse or misuse, ch. Irritation in heavy smokers

Vocal fold polyps
• Unilateral • Broad-based vs. Pedunculated• Formed by capillary break with leakage of blood
resulting in local edema and organization with hyalinized stroma

Laryngeal papilloma
• HPV (6 & 11).• 2% malignant
transformation (HPV 16 &18)
• single in adults
• in childre, multiple & recurrent.
recurrent respiratory papillomatosis (RRP),
“Juvenile papillomatosis”

Laryngeal Papilloma
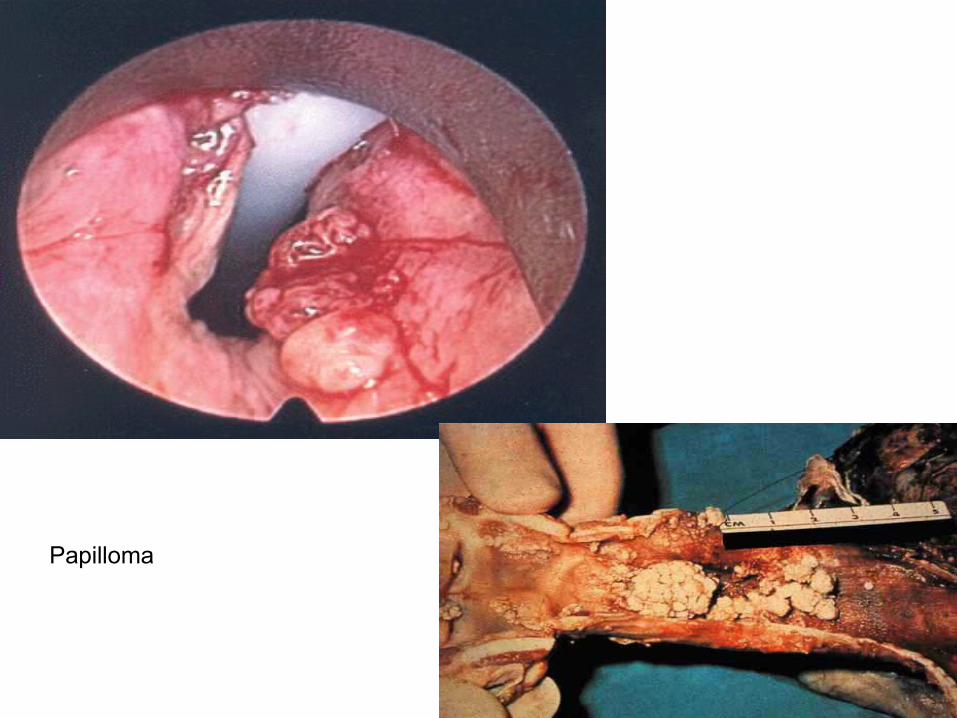
Papilloma

Leukoplakia• Spectrum of change in epithelium• HyperkeratosisDysplasia (mild, moderate, severe),CIS• 8% to 14% rate of malignant transformation

Carcinoma of larynx, Epidemiology
• > 40 years
• men /women = (7 : 1). • nearly all cases, in smokers, alcoholic, +/- asbestos • HPV• About 95% typical Sq C Ca..
• Incidence by Site • Supraglottic 25 - 40% • Glottic 60% to 75%• Subglottic < 5% • begin as in situ lesions, later appear as plaques, then
ulcerating and fungating
Carcinoma of the larynx• persistent hoarseness. • The location of the tumor has a significant bearing on
prognosis;• glottic tumors; 90% are confined to larynx at diagnosis. 1. symptoms early in the course of disease; 2. the glottic region has a sparse lymphatic supply,
and spread beyond the larynx is uncommon. • the supraglottic larynx is rich in lymphatic spaces, and
nearly a 1/3 of these tumors metastasize to regional (cervical) lymph nodes.
The subglottic tumors• remain clinically quiescent, • 1/3 die of the disease. • The usual cause of death is; - infection of the distal respiratory passages or - metastases and cachexia.
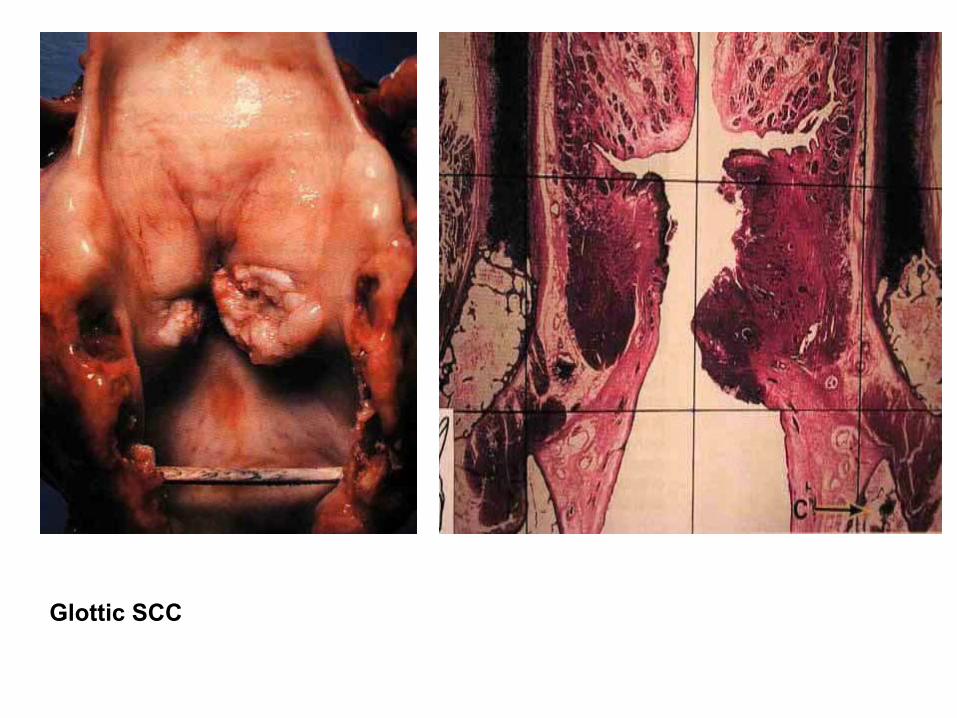
Glottic SCC
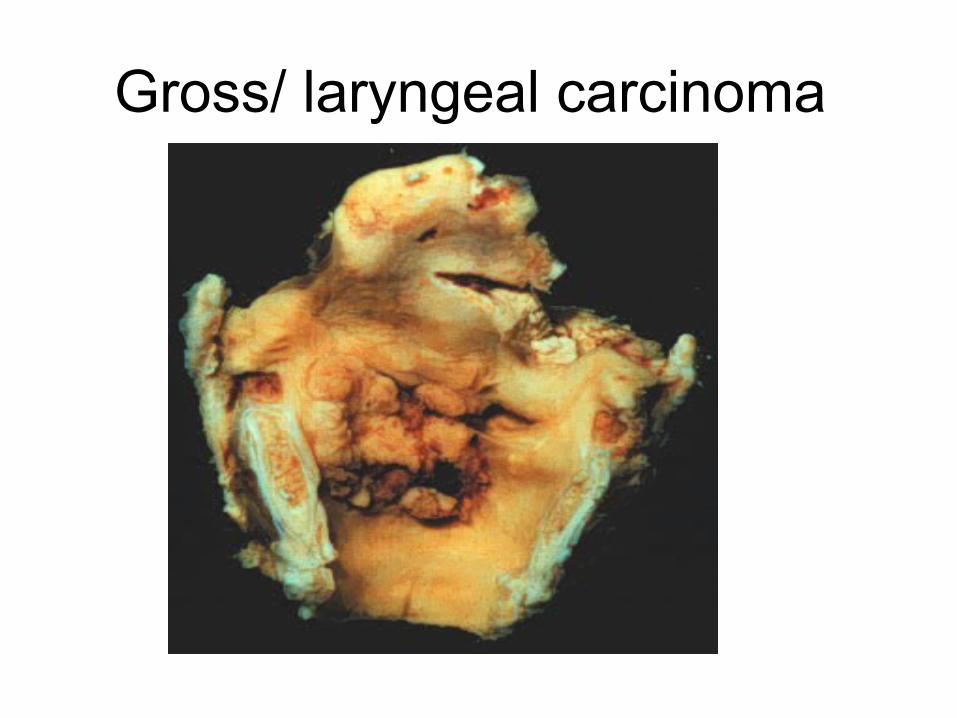
Gross/ laryngeal carcinoma


Dysplasia without Keratosis

Microinvasive or Superficially Invasive Squamous Cell Carcinoma
Invasive Squamous Cell Carcinoma
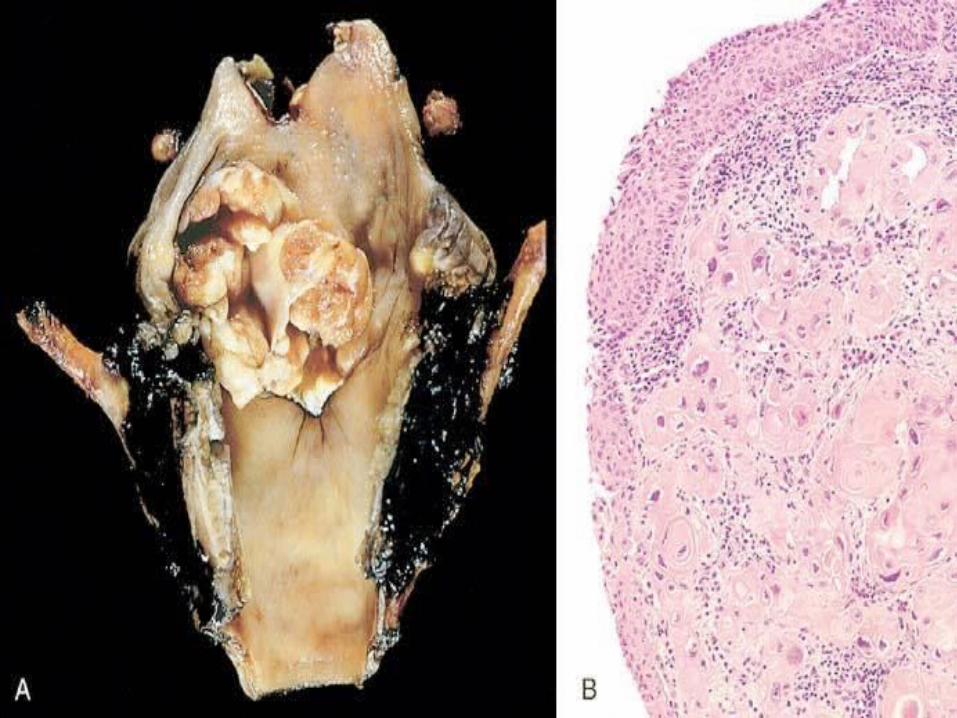

SQUAMOUS CELL CARCINOMA OF LARYNX/Mic


The 10 leading cancers by gender. site Iraqi Tumor Regestry 2007
Breast Lung & bronchus Leukemia Bladder Brain &CNS NHL Colorectal
Larynx Skin excluding Melanoma Stomach Uterus including Cervix and corpus) Hodgkin disease Thyroid Kidney, pelvis& ureter Ovary Prostate Pancreas Bone & cartilage Liver &bile ducts Esophagus
Type of cancer, in Iraq, by primary tumor site (2004)6
EARS
• DEGENERATION: OTOSCLEROSIS• INFLAMMATION:
• NEOPLASMS:



The Tympanic Cavity
Chorda Tympani N. (CN VII)
Tendon of Tensor Tympani M. (V3)
Incus
Tendon of Stapedius M. (CN VII)
Stapes
Cut edge of tympanum Malleus




CERUMEN CAST

OTOSCLEROSIS
NECK
• Lymph node• BRANCHIAL (cleft) CYST• THYROGLOSSAL (duct/tract) CYST• PARAGANGLIOMA (Carotid Body
Tumor)• Other




CAROTID BODY TUMOR“balls of cells”
“zellballen”
ZELLBALLEN

Whole-body PET scan using 18F-FDG