ent jan-march 2011
DESCRIPTION
ENT Jan-MArch 2011TRANSCRIPT
Asian Journal of
www.ijcpgroup.com
January-March 2011
Ear, NoseThroatEar, NoseThroat
Dr VP SoodEditor
Dr KK AggarwalGroup Editor-in-Chief

Dr KK AggarwalGroup Editor-in-Chief
Dr VP SoodEditor
January-March 2011
An IJCP Group Publication Contents
Asian Journal of
Ear, NoseThroatEar, NoseThroat
Advisory Body Heart Care Foundation of India
Non-Resident Indians Chamber of Commerce & IndustryWorld Fellowship of Religions
froM the DeSK of eDItor
Submucous Fibrosis 5VP Sood
froM the DeSK of GrouP eDItor-In-ChIef
Barotrauma 7KK Aggarwal
PhArMACotherAPY
Role of Corticosteroids in ENT Practice 9Aru Handa
SurGICAL APProACh
The Tongue-in-Groove Technique for Managing Nasal Tip Position 13U Raghavan
CLInICAL PrACtICe
Hashimoto’s Thyroiditis: Preoperative Diagnostic Challenge 18Sanjana V Nemade, VV Rokade, NA Pathak SD Deshmukh, SM Sonar
CLInICAL StuDY
Relationship between Parent Perception of Hearing Loss in their Wards with Different Assessment Modalities in Children with Multiple Handicaps 24Noorain Alam, Shamim Ansari, Priyanka Mishra
Dr Sanjiv Chopra Prof. of Medicine & Faculty Dean
Harvard Medical SchoolGroup Consultant editor
Dr Deepak ChopraChief editorial Advisor
Dr KK AggarwalCMD, Publisher and Group editor-in-Chief
Dr Veena AggarwalJoint MD & Group executive editor
Anand Gopal Bhatnagar editorial Anchor
editorDr VP Sood
editorial BoardDr Dinesh Mehta (USA)
Dr A Mahadevaiah (Bangalore)Dr Aru Handa (New Delhi)
Dr BS Gendeh (Kuala Lumpur)Dr PP Singh (New Delhi) Dr AK Gupta (Udaipur) Dr M Allaudin (Dhaka)
Dr Jasveer Singh (New Delhi) Dr Piyush Verma (New Delhi)
Dr Rakesh Parsad Srivastava (Kathmandu)Dr (Mrs.) Nishi Gupta (New Delhi)
Dr Amar Singh (Muscat)
IJCP editorial BoardDr Alka Kriplani Asian Journal of obs & Gynae PracticeDr VP Sood Asian Journal of ear, nose and throatDr Praveen Chandra Asian Journal of Clinical CardiologyDr Swati Y Bhave Asian Journal of Paediatric PracticeDr Vijay Viswanathan the Asian Journal of DiabetologyDr KMK Masthan Indian Journal of Multidisciplinary DentistryDr M Paul Anand, Dr SK Parashar CardiologyDr CR Anand Moses, Dr Sidharth Das Dr A Ramachandran, Dr Samith A Shetty DiabetologyDr Ajay Kumar GastroenterologyDr Koushik Lahiri DermatologyDr Georgi Abraham nephrologyDr Sidharth Kumar Das rheumatologyDr V Nagarajan neurologyDr Kamala Selvaraj, Dr Thankam Verma obs and Gyne

January-March 2011
Contents
eDItorIAL & BuSIneSS offICeSDelhi Mumbai Kolkata Bangalore Chennai hyderabad
Dr Veena Aggarwal9811036687
E - 219, Greater Kailash, Part - 1, N.D. - 110 048
Cont.: [email protected]@ijcp.com
Dinesh: 9891272006 [email protected]: 09831363901
Dr Veena Aggarwal9811036687
Building No. D-10 Flat No 43, 4th Floor Asmita Co-operative
Housing Society Marvey Road
Near Charkop Naka Malad (W)
Mumbai - 400 [email protected]
Sr. BMRitu Saigal
9831363901Flat 5E
Merlin Estate Geetanjali
25/8, Diamond Harbour Road
Kolkata - 700 008 Cont.: 24452066 [email protected]
Sr. BMH Chandrashekar
9845232974Arora Business
Centre, 111/1 & 111/2 Dickenson Road
(Near Manipal Centre)Bangalore - 560 042
Cont.: 25586337 [email protected]
Sr. BMChitra Mohan9841213823
40A, Ganapathy-puram
Main Road Radhanagar Chromepet
Chennai - 600 044Cont.: 22650144 [email protected]
Sr. BMVenugopal
9849083558H. No. 16-2-751/A/70
First Floor Karan Bagh
Gaddiannaram Dil Sukh Nagar
Hyderabad - 500 059 Cont.: [email protected]
Sr.: Senior; BM: Business Manager
editorial Policies
The purpose of IJCP Academy of CME is to serve the medical profession and provide print continuing medical education as a part of their social commitment. The information and opinions presented in IJCP group publications reflect the views of the authors, not those of the journal, unless so stated. Advertising is accepted only if judged to be in harmony with the purpose of the journal; however, IJCP group reserves the right to reject any advertising at its sole discretion. Neither acceptance nor rejection constitutes an endorsement by IJCP group of a particular policy, product or procedure. We believe that readers need to be aware of any affiliation or financial relationship (employment, consultancies, stock ownership, honoraria, etc.) between an author and any organization or entity that has a direct financial interest in the subject matter or materials the author is writing about. We inform the reader of any pertinent relationships disclosed. A disclosure statement, where appropriate, is published at the end of the relevant article.
noteAsian Journal of ear, nose and throat does not
guarantee, directly or indirectly, the quality or efficacy of any product or service described in the
advertisements or other material which is commercial in nature in this issue.
CLInICAL StuDY
Prognostic Value of Natural Antioxidant Enzymes Estimation in Treatment of Oral Submucous Fibrosis 27Bhavesh K Modi, Ashish Katarkar, Amit Tyagi
CASe rePort
Primary Tuberculosis of the Temporomandibular Joint: A Diagnostic Dilemma 30Piyush, Manisha Pal, Achal Gulati, Ishwar Singh
Use of Temporalis Myofascial Flap for Interpositional Arthroplasty in Temporomandibular Joint Ankylosis 32Amarjeet Gambhir, Gita Rani
An Unusual and Rare Case Report of External Auditory Canal Cholesteatoma 36Nishi Gupta, Nidhi Dhawan, Alok Kumar, Parul Mathur
AnnounCeMentSAnnouncements, Conferences and Courses Information 38
eMeDInewS SeCtIon
From eMedinews 39
Asian Journal of
Ear, NoseThroatEar, NoseThroat
Published, Printed and edited byDr KK Aggarwal, on behalf of
IJCP Publications Pvt. Ltd. and Published at
E - 219, Greater Kailash, Part - 1,New Delhi - 110 048
E-mail: [email protected]
Printed at IG Printers Pvt. Ltd., New Delhi E-mail: [email protected]
© Copyright 2011 IJCP Publications Pvt. Ltd. All rights reserved
The copyright for all the editorial material contained in this journal, in the form of layout, content including images and design, is held by IJCP Publications Pvt. Ltd. No part of this
publication may be published in any form whatsoever without the prior written permission
of the publisher.

Review ARticle
�Asian Journal of Ear, Nose & Throat, January-March 2011
Submucous fibrosis was first observed and described by Dr Joshi from India in 1953, in those patients who had the habit of chewing Pan Masala or Gutkha. Oral submucous fibrosis is a chronic disease. This condition also occurs within populations of Indians in South East Asian region. This condition may be
rarely seen in the Western Countries, who have adopted their Indian dietary lifestyle and habits. The condition is probably genetically determined, as not all who chew Pan Masala will be affected. Patients who chew Pan Masala have tendency to develop submucous fibrosis.
These patients first experience burning sensation and intolerance for spicy food or chillies. There are recurrent ulcers in the mouth, change in color of the oral lining and there is progressive development of tight feeling to open mouth leading on to inability to open mouth.
The etiological factor is the Areca Nut (Supari), which is incorporated within Pan, Pan Masala and Gutkha. Initially, there is white appearance of the mucous membranes of inside cheeks which subsequently results in fibrosis below the epithelial surface. The tissues reveals that it is become rigid and the mouth opening is restricted. Palpation of the buccal mucosa and pterygomandibular raphe reveals that it is stiff and hard. There is staining of the teeth which signifies a concurrent tobacco chewing habit. This condition is highly premalignant. Biopsy of the mucosa is required in suspected premalignant lesions.
It is essential that dietary habits involving chewing Pan Masala is stopped. The correction of any hematinic deficiency is also treated. Long-term follow-up is mandatory for the management.
All cases involving premalignant lesions and conditions where follow-up is required because of biopsy proven dysplasia require careful record keeping following treatment and if further clinical deterioration should occur by and large, the ENT specialist and dentist will review these patients for life and will carefully observe for any untoward changes in oral mucous membrane.
Submucous Fibrosis
Dr VP SoodEditor, Asian Journal of Ear, Nose and Throat
Secretary-cum-Managing TrusteeDr Sood Nasal Research Foundation
Past PresidentAssociation of
Otorhinolaryngologists of India
Founder Patron and Past PresidentAll India Rhinology Society
FRom the desk oF editoR
� Asian Journal of Ear, Nose & Throat, January-March 2011
Address for correspondenceDr VP SoodEar, Nose & Throat Center212, Aditya Arcade, 30, Community Center Preet Vihar, Vikas Marg, Delhi - 92Ph. No.: 011-22440011, 42420429E-mail: [email protected] [email protected]: www.drsoodnasalfoundation.com
FRom the desk oF editoR
Patients are advised to stop chewing Pan Masala or Gutkha. Prevention is better than cure in submucous fibrosis. Once submucous fibrosis is established, antioxidant vitamins A, E, C and B6, Copper and Selenium are used. Mouth opening exercises along with repeated local steroids and hyalase injection may be helpful for trismus. When trismus is significant various surgical interventions are available.
n n n

Review ARticle
�Asian Journal of Ear, Nose & Throat, January-March 2011
Barotrauma
Dr KK AggarwalPadma Shri and Dr BC Roy National Awardee
Sr Physician and Cardiologist, Moolchand MedcityPresident, Heart Care Foundation of India
Group Editor-in-Chief, IJCP GroupEditor-in-Chief, eMedinewS
Chairman Ethical Committee, Delhi Medical CouncilDirector, IMA AKN Sinha Institute (08-09)
Hony. Finance Secretary, IMA (07-08)Chairman, IMA AMS (06-07)
President, Delhi Medical Association (05-06)[email protected]
http://twitter.com/DrKKAggarwalKrishan Kumar Aggarwal (Facebook)
FRom the desk oF gRoup editoR-in-chieF
The most common cause of ear barotrauma is flying. Other causes are diving, decompression and hyperbaric oxygen chambers, and blast injuries. Barotrauma can manifest as ear pressure, pain and hearing loss, and tinnitus. Bleeding into the tympanic membrane may occur and rarely, rupture of the round or oval
window membranes can cause vertigo and sensorineural hearing loss.
TreatmentOral decongestants, antihistamines and nasal decongestant sprays used prior to flying or diving may reduce obstruction around the Eustachian tube and facilitate pressure equalization. Swallowing or the Valsalva maneuver can equalize pressures and prevent tissue injury. Chewing gum or sucking on hard candies can help adultsInfants may be helped by nursing or sucking on a bottle. Special ear plugs may help equalize pressure for flying, but cannot be used for diving. Most barotrauma injuries heal spontaneously. Antibiotics are not indicated. Analgesics should be used as needed but glucocorticoids have not been shown to be effective.Dizziness (vertigo) and sensorineural hearing loss may indicate a perilymphatic fistula.Myringotomy has been used as both prevention and treatment for barotrauma related to flying. Ventilation tubes may be needed for someone undergoing hyperbaric oxygen therapy. Tympanoplasty or patching may be needed for serious injuries such as ossicular disruption or perilymphatic fistula.
xxxxxxxxxxx
�Asian Journal of Ear, Nose & Throat, January-March 2011
Role of Corticosteroids in ENT Practice
Aru Handa
Corticosteroids are potent drugs with a wide range of application in various inflammatory and autoimmune disorders. Corticosteroids
are increasingly being used in our daily clinical practice to treat a wide range of otolaryngological disorders due to their anti-inflammatory action. Treatment with corticosteroids has been shown to be effective in the management of idiopathic facial nerve palsy, allergic rhinitis, acute sinusitis, sinonasal inflammatory polyposis and laryngotracheobronchitis. Though corticosteroids have also been used in the management of Meniere’s disease, chronic otitis media and vestibular neuronitis with good results their therapeutic efficacy in these conditions still remains controversial.
Mechanism of Action
Corticosteroids have an anti-inflammatory effect at a subcellular level by activating glucocorticoid receptors, which interact with inflammatory transcription factors resulting in suppression of proinflammatory molecules like cytokines, prostaglandins and leukotrienes.1 At a cellular level, corticosteroids reduce the quantity of inflammatory cells like eosinophils, T lymphocytes, mast cells and dendritic cells. The degree of inflammatory suppression correlates with the tissue concentration of steroid.
AbstrAct
Corticosteroids are increasingly being used to treat a wide range of otolaryngological disorders due to their anti-inflammatory action. They are effective in the management of idiopathic facial nerve palsy, allergic rhinitis, acute sinusitis, sinonasal inflammatory polyposis and laryngotracheobronchitis. Corticosteroids in ENT infections can be administered orally, intravenously, topically or by intralesional injection. The corticosteroids used in ENT practice may be short-acting like hydrocortisone, intermediate-acting like prednisolone, deflazacort and long-acting like dexamethasone and methylprednisolone. Steroid use is often based on anecdotal evidence or physician preference. There is a need to develop evidence based guidelines so that steroids can be safely used in ENT conditions.
Key words: Anti-inflammatory, allergic rhinitis, idiopathic facial nerve palsy, acute sinusitis
Co-ordinator and Senior ConsultantDept. of ENTMoolchand Medcity, New Delhi
Route of Administration
The route of administration of corticosteroids in ENT infections varies from disease-to-disease. They can be administered orally, intravenously, topically or by intralesional injection. Since, intranasal topical corticosteroids undergo rapid first-pass hepatic metabolism, they cause minimal hypothalamic-pituitary suppression and hence least side effects.2
Corticosteroids in the Armamentarium of an ENT Surgeon
The corticosteroids used in ENT practice may be short-acting like hydrocortisone, intermediate-acting like prednisolone, deflazacort and long-acting like dexamethasone and methylprednisolone.
Beclomethasone dipropionate, budesonide, fluticasone propionate, mometasone furoate and triamcinolone acetonide are some of the corticosteroids which are available for intranasal use.
Diseases of the Ear
Bell’s palsy
Bell’s palsy is a unilateral, peripheral facial paresis or paralysis that has an abrupt onset and no detectable cause. Bell palsy is one of the most common neurologic disorders affecting the cranial nerves, and it is certainly the most common cause of facial paralysis worldwide. Though the precise pathophysiology of Bell’s palsy remains an area of continuing debate, it
PHArMAcOtHErAPY

10 Asian Journal of Ear, Nose & Throat, January-March 2011
PHArMAcOtHErAPY
is thought that inflammation and swelling of the facial nerve results in compression of the nerve within the temporal bone. This has been seen in magnetic resonance imaging (MRI) scans with facial nerve enhancement.3
In Bell’s palsy, corticosteroids are frequently used either because of their possible immune modulating effect on the presumed viral etiology or because of reduction of neural edema within the facial canal due to their anti-inflammatory effect. Ramsey et al performed a meta-analysis of 27 prospective trials evaluating steroid therapy for Bell’s palsy in 2000. It was concluded that steroid therapy improved complete facial recovery by 17%, which was clinically and statistically significant.4
Further evidence to support steroid use was provided by Sullivan et al in 2007. In a double-blind, placebo-controlled, randomized trial involving around 500 patients with Bell’s palsy it was demonstrated that early use of prednisolone alone significantly increased the chances of complete facial nerve recovery at 3 and nine months.5
The effect of early steroid treatment on the evolution of IFP (idiopathic facial palsy) was evaluated in the Ear, Nose and Throat Service of the University Hospital of Alicante (Spain) with a prospective protocol from September 1991 to January 1992. The therapeutic protocol for all patients (47 patients) was an intramuscular injection of 60 mg prednisolone in the Emergency Room followed by a course of oral deflazacort that was gradually tapered-off. This Study found that clinical improvement was observed on day 149 and a complete cure by Day 3026. Full recovery of facial motor function without sequelae occurred in 95.6% of patients. These results support early steroid treatment for IFP.6
Vestibular Neuritis
Like Bell’s palsy, vestibular neuritis is presumed to have a viral etiology and has a high rate of spontaneous recovery. A retrospective study reviewed the role of steroids in the recovery of vestibular function in patients with vestibular neuritis. There was no correlation between steroid use and improvement in subjective symptoms, despite improved canal paresis recovery in the steroid group.7 However, in another prospective, double-blind, randomized controlled
trial in patients with vestibular neuritis, it was demonstrated that daily administration of systemic methylprednisolone for three weeks significantly improved recovery of peripheral vestibular function as measured by electronystagmography (ENG).8
Meniere’s Disease
Meniere’s disease is a disorder of the inner ear that can affect hearing and balance to a varying degree. It is characterized by episodes of vertigo and tinnitus and progressive hearing loss, usually in one ear. Both systemic and intratympanic steroids (ITS) are widely used empirically used in the management of Meniere’s disease. Support for their use has been demonstrated in a few studies.
A prospective randomized double-blind study using five consecutive daily intratympanic dexamethasone 4 ug/ml injections for 22 patients with unilateral intractable Meniere’s disease reported 80% vertigo control after two years compared with 60% with placebo. They also reported subjective improvement in tinnitus (48% vs 20% placebo) and hearing loss (35% vs 10% placebo).9 Another prospective study which evaluated combined use of intratympanic and systemic dexamethasone in 17 patients with Meniere’s disease reported vertigo control in 76% but no significant improvement in hearing or tinnitus.10
Idiopathic Sudden Sensorineural Hearing Loss
Idiopathic sudden sensorineural hearing loss (SSHL) is a relatively common otologic disorder of uncertain etiology. Corticosteroids alone or in combination with other therapeutic modalities have been used for treatment of SSHL with mixed response. The addition of ITS to systemic steroid therapy did not confer any hearing recovery benefit in two recent studies.11,12 Multiple retrospective studies of salvage ITS therapy after failure of systemic steroids have reported improved hearing outcomes; however, the variability of study parameters makes comparison difficult and a well-designed prospective randomized trial is required to demonstrate the efficacy of ITS.13
Otitis Media with Effusion
Systemic and intranasal corticosteroids have also been used in the management of otitis media with effusion (OME). Oral steroids alone or in combination with

11Asian Journal of Ear, Nose & Throat, January-March 2011
PHArMAcOtHErAPY
an antibiotic have demonstrated faster resolution of OME in the short-term. Similarly, topical intranasal steroids combined with oral antibiotic also showed similar results in the short-term. However, there is not much evidence which supports use of oral or topical intranasal steroids for the long-term.
Diseases of the Nose
Allergic Rhinitis
Allergic rhinitis is clinically defined as a symptomatic disorder of the nose-induced by an IgE-mediated inflammation after allergen exposure of the membranes of the nose. It affects upto 25% of the general population. Symptoms of allergic rhinitis include rhinorrhea, nasal obstruction, nasal itching and sneezing which are reversible spontaneously or with treatment. Use of nasal corticosteroids has shown to be more useful than antihistamines in allergic rhinitis and currently it is the treatment of first choice. Usually 1-6 months of intranasal steroid treatment is required to obtain optimal results.
Rhinosinusitis
In patients with acute rhinosinusitis, it has been shown that the use of intranasal corticosteroids in conjunction with oral antibiotics are more effective than antibiotics alone for achieving symptomatic improvement.14 Studies have also demonstrated that intranasal steroids alone are more effective than antibiotics in treating uncomplicated rhinosinusitis suggesting that monotherapy with intranasal steroids may be an effective treatment option for community-acquired uncomplicated acute sinusitis.15
Corticosteroids have found to be very effective in the management of chronic rhinosinusitis with nasal polyposis. A double-blind randomized controlled trial in patients with nasal polyps demonstrated the clinical efficacy of a short course of oral prednisolone.16 Another retrospective study demonstrated that a short course of oral prednisolone (1 mg/kg for 5 days) followed by daily intranasal beclomethasone was effective in 85% of patients with only 15% of patients requiring endoscopic sinus surgery.17 Oral steroids are now used preoperatively in patients undergoing endoscopic sinus surgery for nasal polyposis since they reduce vascularity and improve surgical nasal field conditions resulting in shorter operating time.
Disease of Head and Neck
Corticosteroids also have proven efficacy in a wide range of head and neck conditions. They are regularly used to reduce upper aerodigestive tract edema resulting from trauma, surgery, infections and anaphylaxis. Treatment of laryngotracheobronchitis with steroids is well-documented. Corticosteroid use as adjunctive therapy for other upper respiratory tract infections such as pharyngitis, epiglottitis and tonsillitis is common. Use of a single intravenous steroid dose (2-3 mg/kg methylprednisolone) in addition to antibiotic therapy and needle aspiration was compared with needle aspiration and antibiotics alone for the treatment of peritonsillar abscess. The steroid group had a statistically improved clinical outcome with no complications reported.18
Limitations of Corticosteroid Therapy
While anti-inflammatory effects are inseparable from their metabolic effects, the goal of corticosteroid therapy is to obtain maximum clinical benefit with minimum adverse effects. Important adverse effects of long-term corticosteroid therapy include Cushingoid appearance, osteoporosis, cataracts, psychosis, dyspepsia and immunosuppression leading to serious infections. Children are more vulnerable to their side effects, particularly to effects on growth and adrenal suppression. It is therefore, important to balance steroid treatment benefits with the potential for side effects especially when using high-dose systemic therapy.
Summary
Corticosteroids play an important role in the management of a wide-spectrum of ENT problems faced by the clinicians in their day-to-day practice. However, steroid use is often based on anecdotal evidence or physician preference. There is a need to develop evidence-based guidelines so that steroids can be safely used in ENT conditions.
ReferencesVan Cauwenberge P, Van Hoecke H, Vandenbulcke L, Van Zele T, Bachert C. Glucocorticosteroids in allergic inflammation: clinical benefits in allergic rhinitis, rhinosinusitis, and otitis media. Immunol Allergy Clin North Am 2005;25(3):489-9.
1.
12 Asian Journal of Ear, Nose & Throat, January-March 2011
PHArMAcOtHErAPY
Boner AL. Effects of intranasal corticosteroids on the hypothalamic-pituitary-adrenal axis in children. J Allergy Clin Immunol 2001;108(1 Suppl):S32-9.
Seok JI, Lee DK, Kim KJ. The usefulness of clinical findings in localizing in Bell’s palsy: comparison with MRI. J Neurol Neurosurg Psychiatry 2008;79(4):418-20.
Ramsey MJ, DerSimonian R, Holtel MR, Burgess LP. Corticosteroid treatment for idiopathic facial nerve paralysis: a meta-analysis. Laryngoscope 2000;110(3Pt1):335-41.
Sullivan FM, Swan IR, Donnan PT, Morrison JM, Smith BH, Mckinstry B, et al. Early treatment with prednisolone or acyclovir in Bell’s palsy. N Engl J Med 2007;357(16):1598-607.
Hurtado Garcia JF, Talavera Sànchez J, Lopez Richa JJ. Early corticoid treatment of idiopathic facial palsy (Bell). Acta Otorrinolaringol Esp 1997;48(3):177-81.
Ohbayashi S, Oda M, Yamamoto M, Vrano M, Harada K, Horikoshi H, et al. Recovery of the vestibular function after vestibular neuronitis. Acta Otolaryngol Suppl 1993;503:31-4.
Strupp M, Zingler VC, Arbusow V, Niklas D, Maag KP, Dieterich M, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med 2004;35:354-61.
Garduño-Anaya MA, Couthino De Toledo H, Hinojosa-Gonzalez R, Pane-Pianese C, Rios-Castaneda LC. Dexamethasone inner ear perfusion by intratympanic injection in unilateral Meniere’s disease: a two-year prospective, placebo-controlled, double-blind, randomized trial. Otolaryngol Head Neck Surg 2005;133:(2)285-94.
2.
3.
4.
5.
6.
7.
8.
9.
Hirvonen TP, Peltomaa M, Ylikoski J. Intratympanic and systemic dexamethasone for Méniere’s disease. ORL J Otorhinolaryngol Relat Spec 2000;62(3):117-20.Lautermann J, Sudhoff H, Junker R. Transtympanic corticoid therapy for acute profound hearing loss. Eur Arch Otorhinolaryngol 2005;262(7):587-91.Ahn JH, Yoo MH, Yoon TH, Chung JW. Can intratympanic dexamethasone added to systemic steroids improve hearing outcome in patients with sudden deafness? Laryngoscope 2008;118(2):279-82.Cope D, Bova R. Steroids in otolaryngology. Laryngoscope 2008;118(9):1556-60.Meltzer EO, Bachert C, Staudinger H. Treating acute rhinosinusitis: comparing efficacy and safety of mometasone furoate nasal spray, amoxicillin, and placebo. J Allergy Clin Immunol 2005;116(6):1289-95.Dolor RJ, Witsell DL, Hellkamp AS, Williams JW Jr, Califf RM, Simel DL; CAFFS Investigators. Comparison of cefuroxime with or without intranasal fluticasone for the treatment of rhinosinusitis. The CAFFS Trial: a randomized controlled trial. JAMA 2001;286(24): 3097-105.Hissaria P, Smith W, Wormald PJ, Taylor J, Vadas M, Gillis D, et al. Short course of systemic corticosteroids in sinonasal polyposis: a double-blind, randomized, placebo-controlled trial with evaluation of outcome measures. J Allergy Clin Immunol 2006;118(1):128-33.Bonfils P, Nores JM, Halimi P, Avan P. Corticosteroid treatment in nasal polyposis with a three-year follow-up period. Laryngoscope 2003;113(4):683-7.Ozbek C, Aygenc E, Tuna EU, Selcuk A, Ozdem C. Use of steroids in the treatment of peritonsillar abscess. J Laryngol Otol 2004;118(6):439-42.
n n n
10.
11.
12.
13.
14.
15.
16.
17.
18.

xxxxxxxxxxx
13Asian Journal of Ear, Nose & Throat, January-March 2011
The Tongue-in-Groove Technique for Managing Nasal Tip Position U Raghavan
Surgery of the nasal tip remains one of the most challenging aspects of esthetic nasal surgery.1-3 The main characteristics of the nasal tip can be
described in terms of shape, rotation and projection.4 Mechanisms supporting the nasal tip have been well- described (Table 1).1 Rhinoplasty approaches violate most, if not all of them.4 Studies done 15 years ago showed that all rhinoplasty techniques without tip augmentation result in loss of tip projection.5,6 If this is to be avoided, nasal tip support structures must be re-established and reinforced.7 Over the decades many authors have described a variety of techniques to maintain and or enhance nasal tip projection, however, a consistently reliable technique has so far proved elusive.
Historical Development of Tip Modification Techniques
Even in the time of Jacques-Joseph, it was known that most rhinoplasties resulted in loss of tip projection. He compensated for the loss of tip projection by lowering the dorsum. For decades excessive removal of the nasal dorsum to compensate for loss of tip projection resulted in undesirably small noses. Subsequently, techniques were developed to maintain and if necessary increase tip projection. This can be done by enhancing the height of middle crura by
AbstrAct
Despite advances in the knowledge of nasal anatomy and the ongoing development of new techniques, nasal tip modification remains a challenge. Many rhinoplasty maneuvers may result in loss of tip support. Despite the various techniques described in the literature, maintenance or improvement of nasal tip shape and position is difficult. The aim of this study was to assess the benefit of tongue-in-groove technique to maintain nasal tip projection. We examined 64 patients who had their nasal tip repositioned with a tongue-in-groove technique. The mean follow-up period was 21.1 months. The pre- and postoperative results of the nasal tip projection were measured manually using a ruler from the pre- and postoperative pictures. Among the patients studied 55% had their nasal tip projection increased by a mean of 1.4 mm and 33% had their nasal tip projection maintained at the preoperative level and 12.5% had reduction in nasal tip projection.
Key words: Rhinoplasty, nasal tip, projection, tongue-in-groove
Doncaster Royal Infirmary, UKAddress for correspondenceE-mail: [email protected]
vertical dome division type techniques.6,8-10 Cartilage tip grafts applied either as shields or as onlay grafts are strong instruments to increase nasal tip projection.11,12 Alternatively one may increase the length of medial crura by using a strut inserted in between the medial crura reaching upto but not resting on the nasal spine.13,14 Columellar struts give support to the medial crura but do not increase the nasal tip projection and hence they are often combined with tip grafts.11,15 If maximum support is needed for tip projection, a strut may be fixed on the nasal spine.16
Table 1. Tip Supporting Mechanisms1
Major
Attachment of medial crural footplate to the caudal border of the septum
Attachments of the alar cartilages to the upper lateral cartilages
Size, shape and resilience of the medial and lateral crurae
Minor
Anterior maxillary spine and soft tissue attachment of the medial crural feet
Membranous septum
Cartilaginous septal dorsum
The ligamentous attachment between both lower lateral cartilages over the septal angle
Sesamoid cartilages extending to the pyriform aperture
The attachment of skin and muscles to the lower lateral cartilages
sUrGIcAL APPrOAcH
14 Asian Journal of Ear, Nose & Throat, January-March 2011
sUrGIcAL APPrOAcH
Different suture techniques attaching the medial crura to the septum directly or to a caudal septal extension graft have been described.17,18 Alternatively, Kridel and Foda suggested increasing the height of the medial crura by borrowing from the lateral crura called the lateral crural steal technique.19,20 This may be considered as an alternative to vertical dome division.
Tongue-in-groove Technique
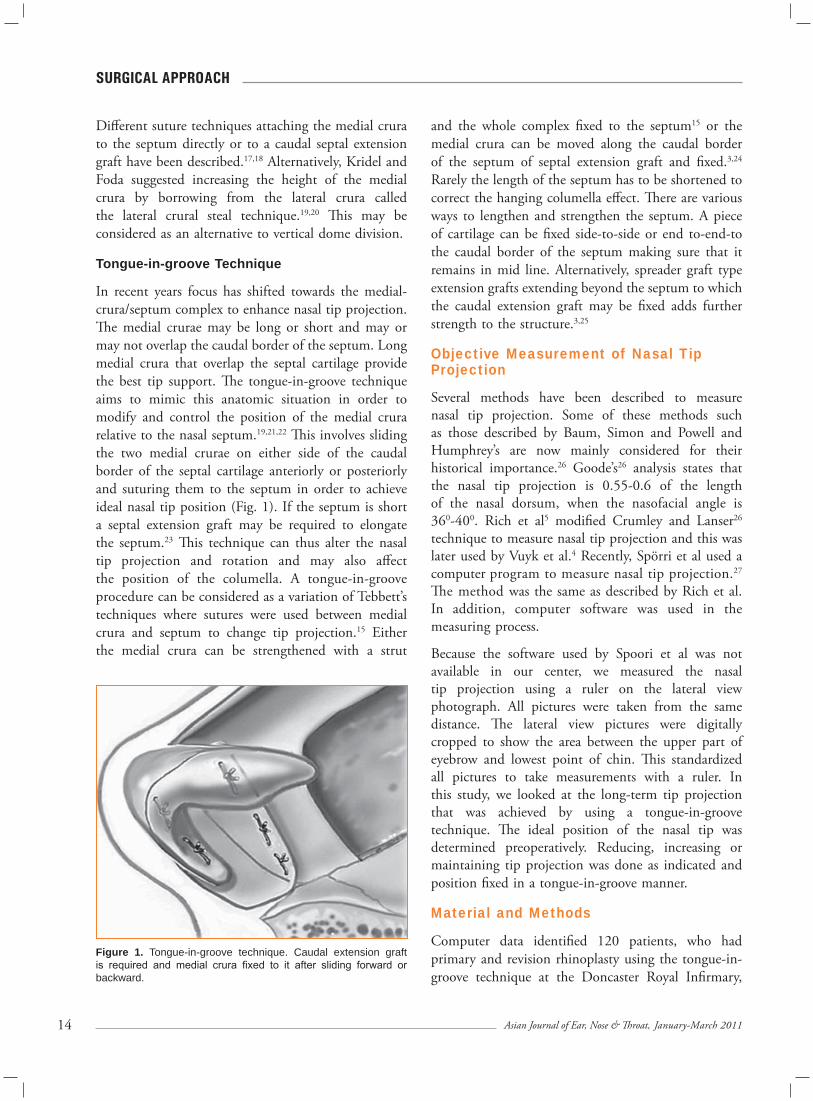
In recent years focus has shifted towards the medial-crura/septum complex to enhance nasal tip projection. The medial crurae may be long or short and may or may not overlap the caudal border of the septum. Long medial crura that overlap the septal cartilage provide the best tip support. The tongue-in-groove technique aims to mimic this anatomic situation in order to modify and control the position of the medial crura relative to the nasal septum.19,21,22 This involves sliding the two medial crurae on either side of the caudal border of the septal cartilage anteriorly or posteriorly and suturing them to the septum in order to achieve ideal nasal tip position (Fig. 1). If the septum is short a septal extension graft may be required to elongate the septum.23 This technique can thus alter the nasal tip projection and rotation and may also affect the position of the columella. A tongue-in-groove procedure can be considered as a variation of Tebbett’s techniques where sutures were used between medial crura and septum to change tip projection.15 Either the medial crura can be strengthened with a strut
and the whole complex fixed to the septum15 or the medial crura can be moved along the caudal border of the septum of septal extension graft and fixed.3,24 Rarely the length of the septum has to be shortened to correct the hanging columella effect. There are various ways to lengthen and strengthen the septum. A piece of cartilage can be fixed side-to-side or end to-end-to the caudal border of the septum making sure that it remains in mid line. Alternatively, spreader graft type extension grafts extending beyond the septum to which the caudal extension graft may be fixed adds further strength to the structure.3,25
Objective Measurement of Nasal Tip Projection
Several methods have been described to measure nasal tip projection. Some of these methods such as those described by Baum, Simon and Powell and Humphrey’s are now mainly considered for their historical importance.26 Goode’s26 analysis states that the nasal tip projection is 0.55-0.6 of the length of the nasal dorsum, when the nasofacial angle is 360-400. Rich et al5 modified Crumley and Lanser26 technique to measure nasal tip projection and this was later used by Vuyk et al.4 Recently, Spörri et al used a computer program to measure nasal tip projection.27 The method was the same as described by Rich et al. In addition, computer software was used in the measuring process.
Because the software used by Spoori et al was not available in our center, we measured the nasal tip projection using a ruler on the lateral view photograph. All pictures were taken from the same distance. The lateral view pictures were digitally cropped to show the area between the upper part of eyebrow and lowest point of chin. This standardized all pictures to take measurements with a ruler. In this study, we looked at the long-term tip projection that was achieved by using a tongue-in-groove technique. The ideal position of the nasal tip was determined preoperatively. Reducing, increasing or maintaining tip projection was done as indicated and position fixed in a tongue-in-groove manner.
Material and Methods
Computer data identified 120 patients, who had primary and revision rhinoplasty using the tongue-in-groove technique at the Doncaster Royal Infirmary,
Figure 1. Tongue-in-groove technique. Caudal extension graft is required and medial crura fixed to it after sliding forward or backward.

15Asian Journal of Ear, Nose & Throat, January-March 2011
sUrGIcAL APPrOAcH
UK, between January 2007 and January 2008. All patients who had complete records and a minimum of 12 months follow-up and a complete set of adequate photographs were included in the study. This left a total of 64 patients which could be included in this study. All patients were operated on by the author. The decision whether to increase, maintain or decrease nasal tip projection and by how much were taken preoperatively based on the analysis of face of patient and photographs.
Surgical Technique
All patients underwent an external rhinoplasty and their medial crurae were moved forwards or backwards so as to achieve the desired nasal tip position. The medial crurae were fixed to the caudal septum if the septal cartilage was long enough or otherwise to a cartilage septal extension graft fixed to the caudal border of the septum. Septal extensions were required in 35 patients (55%) as the caudal extension of septum was not sufficient for tongue-in-groove technique. The grafts were fixed to the septal cartilage side-to-side. By this method the nasal tips were fixed at an appropriate level without pulling the upper lip upwards.
Evaluation Method
Manual measurements of the nasal tip projection were done using a ruler. The pre- and postoperative frontal and lateral view photos were taken at the same focal length. The lateral views were digitally cropped to include the area between the upper part of eyebrow to the lowest point of chin. These made the pre- and postoperative pictures of the same size so that they could be measured with a ruler to find the Goode’s ratio.
Results
Sixty-four patients were studied, (there were 24 male and 40 female patients). Primary rhinoplasty was performed on 61 patients and three had revision rhinoplasty. Age ranged from 20 to 58 with a mean age of 34. The mean period of follow-up was 21.1 months (range 12-48 months). It was decided to maintain nasal tip projection at the preoperative level in 21 (33%) (Group 1) patients, increase in 35 patients (55%) (Group 2) by a mean of 1.48 mm (range 1-3 mm) and reduce the tip projection in the remaining eight patients (12.5%)
(Group 3) between 1 mm and 3 mm (mean 1.62 mm). All patients had the tip maintained at the preoperative level in Group 1 (Fig. 2). In Group 2, 32 patients had primary rhinoplasty and three patients had revision rhinoplasty.
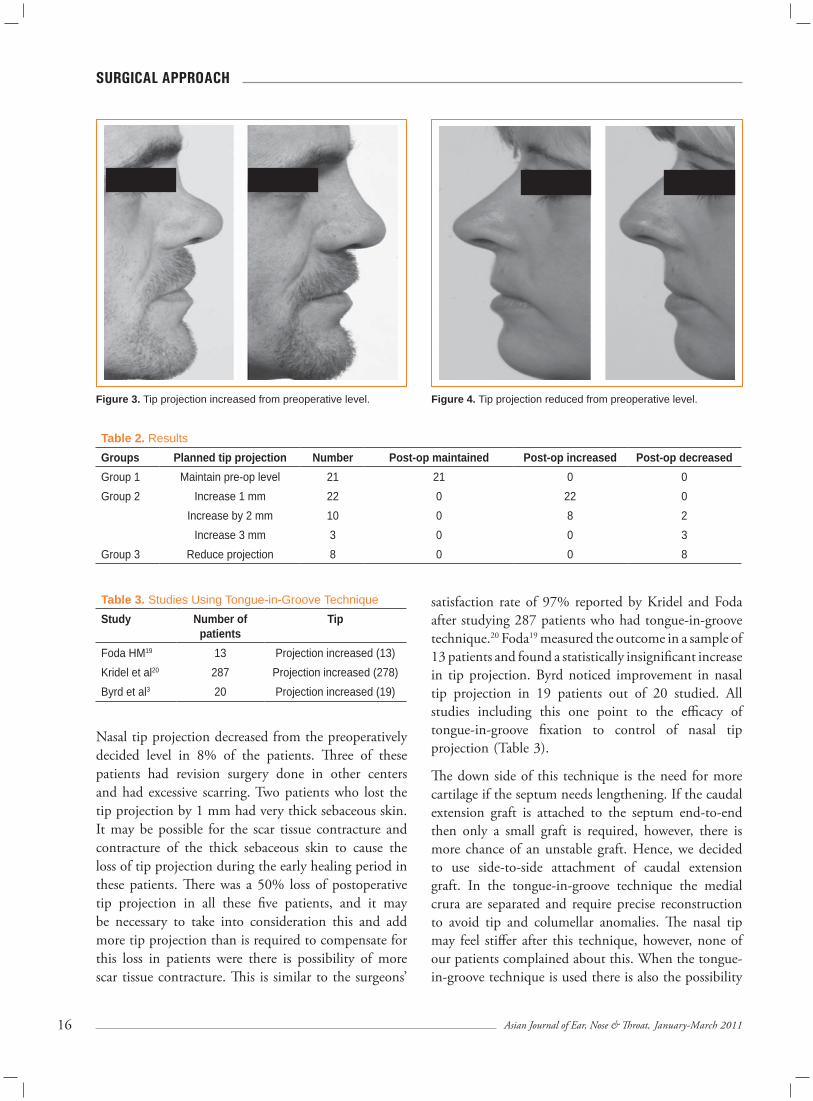
The preoperative decision was to increase the tip projection by 1 mm in 22 patients, by 2 mm in 10 patients and 3 mm in the three revision rhinoplasty patients (Fig. 3). Of these all the 22 patients who had the tip increased by 1 mm maintained it postoperatively in their subsequent follow-ups. Among the 10 patients where the tip was increased by 2 mm, eight patients (80%) maintained it and the rest two (20%) reduced the tip projection by 1 mm at the six months follow-up but maintained the tip projection at that level on further follow- up. All the three revision patients where the tip was increased by 3 mm lost the tip projection by 1.5 mm at the six months follow-up but maintained that projection at the 12 months follow-up and thereafter. In Group 3, all patients maintained the desired reduced tip projection (Fig. 4.) There were no postoperative complications (Table 2).
Discussion
The objective assessment in this study shows that 92% of the 64 patients, who had tongue-in-groove technique had their nasal tip projection increased or maintained postoperatively at the preoperatively decided level. This underscores the significance of the tongue-in-groove technique in modifying nasal tip position.
Figure 2. Tip projection maintained at the same preoperative level.
16 Asian Journal of Ear, Nose & Throat, January-March 2011
sUrGIcAL APPrOAcH
Nasal tip projection decreased from the preoperatively decided level in 8% of the patients. Three of these patients had revision surgery done in other centers and had excessive scarring. Two patients who lost the tip projection by 1 mm had very thick sebaceous skin. It may be possible for the scar tissue contracture and contracture of the thick sebaceous skin to cause the loss of tip projection during the early healing period in these patients. There was a 50% loss of postoperative tip projection in all these five patients, and it may be necessary to take into consideration this and add more tip projection than is required to compensate for this loss in patients were there is possibility of more scar tissue contracture. This is similar to the surgeons’
satisfaction rate of 97% reported by Kridel and Foda after studying 287 patients who had tongue-in-groove technique.20 Foda19 measured the outcome in a sample of 13 patients and found a statistically insignificant increase in tip projection. Byrd noticed improvement in nasal tip projection in 19 patients out of 20 studied. All studies including this one point to the efficacy of tongue-in-groove fixation to control of nasal tip projection (Table 3).
The down side of this technique is the need for more cartilage if the septum needs lengthening. If the caudal extension graft is attached to the septum end-to-end then only a small graft is required, however, there is more chance of an unstable graft. Hence, we decided to use side-to-side attachment of caudal extension graft. In the tongue-in-groove technique the medial crura are separated and require precise reconstruction to avoid tip and columellar anomalies. The nasal tip may feel stiffer after this technique, however, none of our patients complained about this. When the tongue-in-groove technique is used there is also the possibility
Figure 3. Tip projection increased from preoperative level. Figure 4. Tip projection reduced from preoperative level.
Table 2. ResultsGroups Planned tip projection Number Post-op maintained Post-op increased Post-op decreasedGroup 1 Maintain pre-op level 21 21 0 0Group 2 Increase 1 mm 22 0 22 0
Increase by 2 mm 10 0 8 2Increase 3 mm 3 0 0 3
Group 3 Reduce projection 8 0 0 8
Table 3. Studies Using Tongue-in-Groove TechniqueStudy Number of
patientsTip
Foda HM19 13 Projection increased (13)Kridel et al20 287 Projection increased (278)Byrd et al3 20 Projection increased (19)

17Asian Journal of Ear, Nose & Throat, January-March 2011
sUrGIcAL APPrOAcH
of increasing tip rotation more than when struts and tip grafts are used which should be kept in mind while fixing the medial crura. In this study all patients had open rhinoplasty even though it can be done using a closed rhinoplasty. It is possible to achieve better precision with this technique if an open approach is used. Techniques described to enhance nasal tip projection include columellar strut, nasal tip grafting, transdomal suturing and lateral crural steal.1 Columellar struts may change the position and shape of the columella.2 A previous study by Vuyk et al using ‘free-floating’ columellar struts to support nasal tip projection showed 60% of patients having increased or maintained nasal tip projection especially in the presence of a tip graft.4 The tongue-in-groove technique can be considered as an evolution from columellar struts by fixing them to caudal septum. Moreover, in the study by Vuyk et al, larger tip grafts were required to obtain optimum tip projection. Larger tip grafts have the risk of becoming visible through the skin over time.15 Byrd et al also agree that ‘free-floating’ columellar struts are incapable of providing sufficient support of the nasal tip.3 However, a recent study by Ingels et al has noted a slight increase in tip projection and rotation with columellar strut.28 This is similar to the observation by Vuyk et al4 that the columellar struts help in maintaining nasal tip projection.
Conclusion
The tongue-in-groove technique provides a reliable and reproducible method to recreate nasal tip support mechanisms. This also allows the tip to be repositioned to provide adequate nasal tip projection. The additional surgical maneuvers required are intricate but provide good tip support and a strong base for other techniques like suturing and tip grafting. If more tissue contracture is expected as in revision rhinoplasty and in patients with thick sebaceous skin it may be beneficial to increase tip projection more than required to compensate for the possible reduction. Even though there is a possibility for increased stiffness for the tip the predictability of tip position largely outweighs this risk.
ReferencesTardy ME, Toriumi DM, Hecht DA. Philosophies and principles of rhinoplasty. In: Functional and
1.
Aesthetic Surgery of the Face. 2nd edition, Papel et al (Eds.), Thieme Medical Publications Inc, New York 2002:369-89.Trenite GJN. Surgery for the nasal tip: intranasal approach. In: Functional and Aesthetic Surgery of the Face. 2nd edition, Papel et al (Eds.), Thieme Medical Publications Inc, New York 2002:414-28.Byrd HS, Andochick S, Copit S, Walton KG. Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg 1997;100(4)999-1010.Vuyk HD, Oakenful C, Plaat RE. A quantitative appraisal of change in nasal tip projection after open rhinoplasty. Rhinology 1997;35(3):124-8.Rich JS, Friedman WH, Pearlman SJ. The effect of lower lateral cartilage excision on nasal tip projection. Arch Otolaryngol Head Neck Surg 1991;117(1):56-9.Petroff MA, McCollough EG, Hom D, Anderson JR. Nasal tip projection. Quantitative changes following rhinoplasty. Arch Otolaryngol Head Neck Surg 1991;117(7):783-8.Farrior EH. Dramatic refinement of the nasal tip. Otolaryngol Clin North Am 1999;32(4):621-36.Goldman IB. The importance of the mesial crura in nasal-tip reconstruction. AMA Arch Otolaryngol 1957;65(2):143-7.Simons RL, Rhee JS. Surgery of the nasal tip: vertical dome division. In: Functional and Aesthetic Surgery of the Face. 2nd edition, Papel et al (Eds.), Thieme Medical Publications Inc, New York 2002:429-38.Baum SJ. Nasal projection. Arch Otolaryngol 1977;103(5):262-7.Peck GC. The onlay graft for nasal tip projection. Plast Reconstr Surg 1983;71(1):27-39.Sheen JH. Achieving more nasal tip projection by the use of a small autogenous vomer or septal cartilage graft. A preliminary report. Plast Reconstr Surg 1975;56(1):35-40.Anderson JR. New approach to rhinoplasty. A five-year reappraisal. Arch Otolaryngol 1971;93(3):284-91.Millard DR. Adjuncts in augmentation mentoplasty and corrective rhinoplasty. Plast Reconstr Surg 1965;36:48-61.Johnson CM Jr, Godin MS. The tension nose: open structure rhinoplasty approach. Plast Reconstr Surg 1995;95(1):43-51.Gunter JP, Clark CP, Friedman RM. Internal stabilization of autogenous rib cartilage grafts in rhinoplasty: a barrier to cartilage warping. Plast Reconstr Surg 1997;100(1):161-9.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
...Cont’d on page 26

xxxxxxxxxxx
18 Asian Journal of Ear, Nose & Throat, January-March 2011
Hashimoto’s Thyroiditis: Preoperative Diagnostic ChallengeSanjana V Nemade*, VV Rokade**, NA Pathak*, SD Deshmukh†, SM Sonar‡
Thyroiditis is a group of inflammatory thyroid disorders. Patients with chronic lymphocytic thyroiditis (Hashimoto’s thyroiditis) present
with hypothyroidism, goiter or both. The frequency of the disease appears to have increased during the past several decades.1 During the course of this disease, the cells of thyroid become insufficient in converting iodine into thyroid hormone and the gland ‘compensates’ by enlarging.
A diffuse, firm goiter without signs of thyrotoxicosis, should suggest the diagnosis of Hashimoto’s thyroiditis. Most often the gland is bosselated or ‘rubbery’. It is usually symmetrical, although much variation in symmetry as well as consistency can occur. Pain and tenderness on deep palpation may be present.2
AbstrAct
Chronic (Hashimoto’s) thyroiditis is an autoimmune disease that may be associated with varying degrees of thyroid enlargement. The primary way to treat the disease is conservative; however, surgery has its place and efficacy in patients with pressure symptoms, pain and associated malignancy. In the selection of patients for surgical treatment, a discriminatory approach is necessary to prevent unnecessary surgeries. To achieve this, definite preoperative diagnosis of Hashimoto’s thyroiditis is the need. It may coexist with other common causes of thyromegaly like benign goiter or malignant thyroid disease. Thyroiditis can make thyroid dissection more difficult and possibly increase the risk of surgical complications like inadvertent parathyroidectomy, damage to recurrent laryngeal nerve. Our approach has been to establish reliable criteria for diagnosis of thyroiditis and indications for surgery. Hashimoto’s thyroiditis was diagnosed by clinical examination, fine-needle aspiration cytology (FNAC), antimicrosomal antibody, thyroid function studies, thyroid scan and the efficacy of all these criteria was assessed. Our experience with 87 cases of thyroid swelling operated at Smt. Kashibai Navale Medical College and General Hospital, Narhe, Pune from January 2007 to December 2009 was reviewed to determine the incidence of Hashimoto’s thyroiditis, reliable criteria for its diagnosis and the need of surgical intervention.
Key words: Hashimoto’s thyroiditis, antimicrosomal antibody, thyroid scan, fine-needle aspiration cytology, serum TSH
*Assistant Professor**Associate Professor and Head, Dept. of ENT†Professor, Dept. of Pathology ‡Professor, Dept. of Nuclear MedicineSmt. Kashibai Navale Medical College and General Hospital, Narhe, PuneAddress for correspondenceDr Sanjana V NemadeC/o: R Manjarekar B-6/97, Shrikrishna Clinic, Vitthal Rakhumai Society, Apte Colony Sinhgad Road, Hingane Khurd, Pune - 411 051E-mail: [email protected]
Hashimoto’s thyroiditis is considered an autoimmune disease with a variety of antithyroid antibodies whether detected in the patient’s serum. It is not established whether these antibodies are cytodestructive. Both humoral and cell-mediated immunity are probably involved in the production of this inflammatory response. Antimicrosomal antibodies (AMA) are directed against components of thyroid microsomes, in particular peroxidase. AMA are the most useful of all antithyroid antibodies and are present in 90-95% cases of Hashimoto’s thyroiditis.2-5
Thyroid uptake measurements and scintigraphic findings (usually obtained with technetium-99m [Tc-99m] or iodine-123) play an important role in the diagnosis of Hashimoto’s thyroiditis. The radioactive uptake shows heterogenous uptake, or may be paradoxically high as the gland retains its ability to ‘take up’ or ‘trap’ iodine even after it has lost its ability to produce thyroid hormone.6 Fine-needle aspiration cytology (FNAC) shows lymphocytes and macrophages in Hashimoto’s thyroiditis.7 In the initial stage of Hashimoto’s thyroiditis, patients are euthyroid. As the fibrosis advances, eventual reduction in thyroid function takes place. Thus hypothyroidism is a late manifestation of Hashimoto’s thyroiditis.2
cLINIcAL PrActIcE

1�Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL PrActIcE
Surgery is required in patients with Hashimoto’s thyroiditis in cases of pressure symptoms, persistent pain or if malignancy is suspected to be associated with it. Thyroiditis can make thyroid dissection more difficult due to fibrosis and possibly increase the risk of surgical complications like inadvertent parathyroidectomy leading to postoperative hypocalcemia, damage to recurrent laryngeal nerve.8-10 Preoperative diagnosis makes the surgeon aware of possible fibrosis and help him to take measures during surgery to prevent the possible complications.
The present study was designed to assess the usefulness of diagnostic criteria for hashimoto’s thyroiditis. Our approach has been to establish diagnosis of thyroiditis by clinical characteristics, FNAC and thyroid function studies like elevated thyroid-stimulating hormone (TSH), positive thyroid antibodies and heterogenous uptake of radionuclide in thyroid scans. We studied the sensitivity and specificity of these criteria so as to establish a protocol for the necessary preoperative investigations in case of thyroid swelling to rule out Hashimoto’s thyroiditis. In the previous studies it has been observed that AMA is the most sensitive and specific investigation for Hashimoto’s thyroiditis.2,11,12
Thyroid hormonal profile and radioactive iodine uptake (RAIU) had been found to be helpful in assessing the functional status, but the information obtained from thyroid function tests is ‘soft’ as the secretion of TSH is influenced by many factors.12 The diagnostic accuracy of FNAC has been found to be high; however, multiple aspirations are required in almost all cases.7
Material and Methods
Eighty-seven cases that underwent thyroidectomy at Smt. Kashibai Navale Medical College and General Hospital, Narhe, Pune from January 2007 to December 2009 were retrospectively studied.
Data collected on each patient included: Age; sex; complaints of present illness; previous surgical history; family history of similar complaints; routine blood and urine analysis; serum calcium level; blood group; thyroid function tests: FT3, FT4, TSH; antimicrosomal antibody estimation; ultrasound of neck; scintigraphic scan of thyroid; FNAC of thyroid mass; computerized tomography in selected
patients like those in the huge goiter, retrosternal extension or suspected malignancy.
Histopathology reports were scrutinized for final diagnosis, presence of Hashimoto’s thyroiditis and the pathologic features of the gland. Diagnosis of Hashimoto’s thyroiditis was suspected on the basis of clinical and laboratory data, cytology, scintigraphy and was confirmed by histology of surgical specimens. We calculated the true-positive, true-negative, false-positive and false-negative values for the investigations helpful in the diagnosis of Hashimoto’s thyroiditis i.e., antimicrosomal antibodies, FNAC, thyroid scan and serum TSH. Sensitivity and specificity calculator was applied to each parameter. We also studied the indication for surgery in patients with Hashimoto’s thyroiditis.
Results
Out of 87 patients who underwent thyroidectomy, 18 included Hashimoto’s thyroiditis with goiter, three had Hashimoto’s thyroiditis associated with papillary carcinoma, five had papillary carcinoma and 61 had benign goiter. The ratio of male-to-female was 2:85. All 21 patients of Hashimoto’s thyroiditis were females. Age range was 24-68 years (mean - 41.57). Fifty-nine patients underwent hemithyroidectomy, 22 patients underwent total thyroidectomy, four underwent subtotal thyroidectomy, two had completion thyroidectomy.
Out of 21 patients of Hashimoto’s thyroiditis, 11 patients had diffuse, smooth firm rubbery swelling; eight patients had diffuse, nodular firm swelling and two patients had nodular, firm swelling with pain and tenderness on deep palpation. Antimicrosomal antibody was positive (>60 U/ml) in all 21 patients of Hashimoto’s thyroiditis. It was false-positive in three patients with no false negative (Table 1). Sensitivity of AMA was found to be 100% and specificity of 95.31%. Thus, AMA was found to be a highly sensitive and as well as a highly specific investigation in our study. FNAC was true-positive in six patients and no false positive. It was false-negative in 15 patients (Table 2). Sensitivity of FNAC was found to be 28.57% and specificity of 100%. Thus, FNAC was found to be highly specific but poorly sensitive for diagnosis of Hashimoto’s thyroiditis. Thyroid scan showed heterogenous uptake in 18 patients, and homogenous
20 Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL PrActIcE
Table 4. Sensitivity and Specificity of Thyroid-stimulating Hormone Sensitivity: 14.29% Specificity: 100%True-positive 2
False-positive 0False-negative 19True-negative 66
uptake with single cold nodule in three patients (Table 3). Increased uptake was not seen in any of our patients of Hashimoto’s thyroiditis. Sensitivity of thyroid scan was 85.71% and specificity was 100%. It was highly sensitive and specific in the diagnosis of Hashimoto’s thyroiditis.
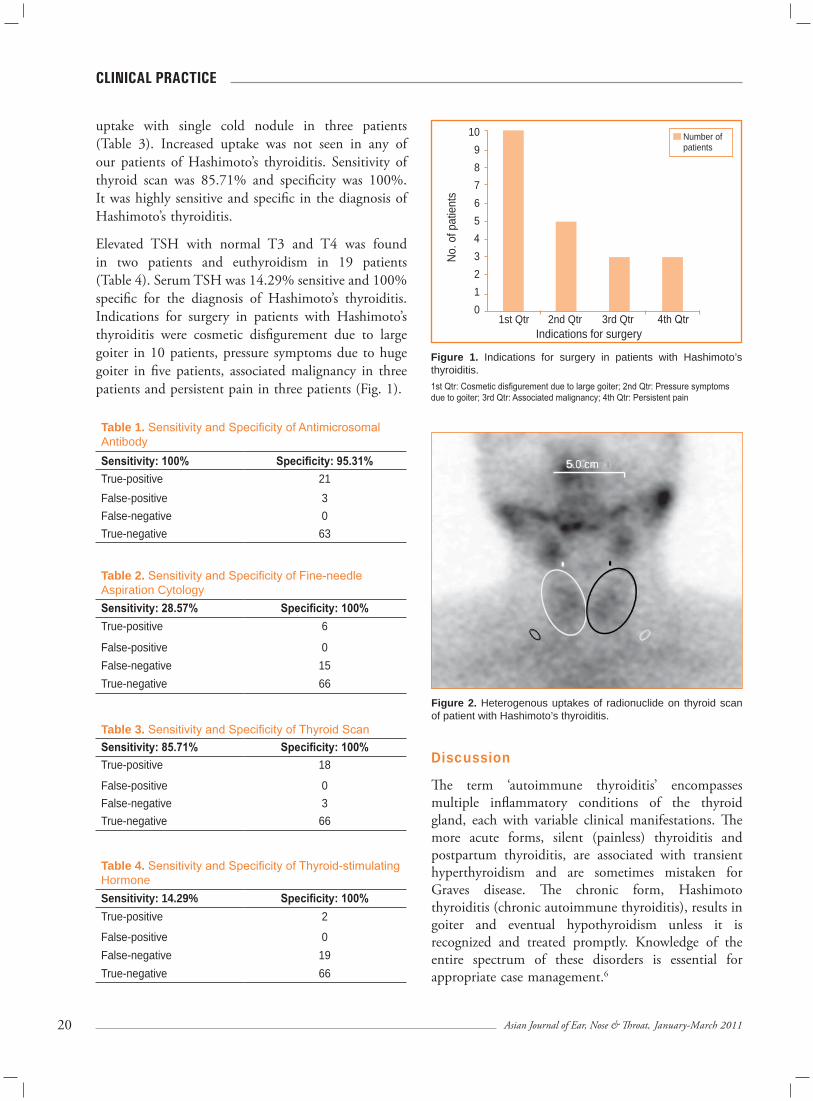
Elevated TSH with normal T3 and T4 was found in two patients and euthyroidism in 19 patients (Table 4). Serum TSH was 14.29% sensitive and 100% specific for the diagnosis of Hashimoto’s thyroiditis. Indications for surgery in patients with Hashimoto’s thyroiditis were cosmetic disfigurement due to large goiter in 10 patients, pressure symptoms due to huge goiter in five patients, associated malignancy in three patients and persistent pain in three patients (Fig. 1).
Figure 1. Indications for surgery in patients with Hashimoto’s thyroiditis.1st Qtr: Cosmetic disfigurement due to large goiter; 2nd Qtr: Pressure symptoms due to goiter; 3rd Qtr: Associated malignancy; 4th Qtr: Persistent pain
Number of patients
Discussion
The term ‘autoimmune thyroiditis’ encompasses multiple inflammatory conditions of the thyroid gland, each with variable clinical manifestations. The more acute forms, silent (painless) thyroiditis and postpartum thyroiditis, are associated with transient hyperthyroidism and are sometimes mistaken for Graves disease. The chronic form, Hashimoto thyroiditis (chronic autoimmune thyroiditis), results in goiter and eventual hypothyroidism unless it is recognized and treated promptly. Knowledge of the entire spectrum of these disorders is essential for appropriate case management.6
5.0 cm
Figure 2. Heterogenous uptakes of radionuclide on thyroid scan of patient with Hashimoto’s thyroiditis.
No. o
f pat
ient
s
10 9 8 7 6 5 4 3 2 1 0
1st Qtr 2nd Qtr 3rd Qtr 4th QtrIndications for surgery
Table 1. Sensitivity and Specificity of Antimicrosomal AntibodySensitivity: 100% Specificity: 95.31%True-positive 21False-positive 3False-negative 0True-negative 63
Table 3. Sensitivity and Specificity of Thyroid ScanSensitivity: 85.71% Specificity: 100%True-positive 18
False-positive 0False-negative 3True-negative 66
Table 2. Sensitivity and Specificity of Fine-needle Aspiration CytologySensitivity: 28.57% Specificity: 100%True-positive 6
False-positive 0False-negative 15True-negative 66

21Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL PrActIcE
(perhaps 3-5%) each year.2 Thus, hypothyroidism is the late manifestation of Hashimoto’s thyroiditis. In our study, out of 21 patients of Hashimoto’s thyroiditis, 2 patients had elevated TSH and normal T3, T4 (subclinical hypothyroidism). Nineteen patients were euthyroid with normal TSH at the time of presentation. Serum TSH is poorly sensitive (14.21%) but highly specific (100%) investigation for the diagnosis of Hashimoto’s thyroiditis.
The goiter of Hashimoto’s thyroiditis may remain unchanged for decades but usually it gradually increases in size. Sudden increase in size may arise the suspicion of associated malignancy. Clinical findings are diffuse enlargement of the gland with or without lobulations. On palpation it has rubbery feel. Pain and tenderness on deep palpation may be there. Rarely, pain is persistent and unresponsive to medical treatment like steroids and requires surgery.2,8 In our study, firm rubbery feel on palpation was present in 11 patients of Hashimoto’s thyroiditis. Pain and tenderness on deep palpation was there in three patients of Hashimoto’s thyroiditis.
Hashimoto’s thyroiditis is characterized by the destruction of thyroid cells by various cell- and antibody-mediated immune processes. The initiating process is not well-understood.3-5 Antibodies to various thyroid antigens, include AMA directed against components of thyroid microsomes, in particular peroxidase, antithyroglobulin (anti-Tg) and to a lesser extent, TSH receptor-blocking antibodies. Nevertheless, a small percentage of patients with Hashimoto’s thyroiditis (approximately 10-15%) may be antibody negative.9 AMA is the most useful of all antithyroid antibodies as they are often present in thyroid disease especially Hashimoto’s thyroiditis it is 95-99% positive when an assay of sufficient sensitivity is used. Anti-Tg antibodies are present in 55-90% of patients.2,4 AMA alone appears sufficient to detect autoimmune thyroid disease at about one-half the cost of routine of performing both AMA and anti-Tg studies. The widespread practice of performing both tests increases the cost without an offsetting diagnostic gain. AMA is much more sensitive than anti-Tg. AMA is positive in 99% of patients with Hashimoto’s thyroiditis. Mild-to-moderately elevated levels of thyroid antibodies may be found in a variety of thyroid and autoimmune disorders,
The most common type of thyroiditis - Hashimoto’s thyroiditis was first described by Hakaru Hashimoto, a Japanese surgeon working in Berlin, Germany. His report was based on the examination of four postoperative cases that he published in 1912. He is also credited with introducing the term struma lymphomatosa in reference to the syndrome. Its incidence in surgical specimens is relatively high, i.e., 13% in collected studies.1 This high incidence of thyroiditis in patients operated on to distinguish between benign and malignant thyroid disease seems to be based, primarily, on the inability to establish the diagnosis of Hashimoto’s thyroiditis before operation.1 Worldwide, the most common cause of hypothyroidism is iodine deficiency. However, Hashimoto’s thyroiditis remains the most common cause of spontaneous hypothyroidism in areas of adequate iodine intake. The incidence of Hashimoto’s thyroiditis is estimated to be 10-15 times higher in females.13 In our study all 21 patients with Hashimoto’s thyroiditis were females.
The most commonly affected age range in Hashimoto’s thyroiditis is 30-50 years, with the peak incidence in men occurring 10-15 years later. The overall incidence of hypothyroidism increases with age in men and women.4 Hashimoto thyroiditis has a strong genetic component because there is a high prevalence of thyroid antibodies among first-degree relatives.2 In our study six patients gave significant family history in the form of similar complaints in family members.
Commonest presentation of Hashimoto’s thyroiditis is euthyroidism and goiter, i.e. thyroid function studies are normal. Second common is subclinical hypothyroidism and goiter. In this, the autoimmune reaction results in lymphocytic and plasma cell infiltration with formation of lymphoid follicles, which in turn leads to thyroid follicle deterioration. A mild decline in circulating thyroid hormones is sensed by the pituitary gland, and a compensatory rise in TSH secretion stimulates the gland to synthesize more thyroid hormone so that T3 and T4 levels return to normal. Fibrosis develops over time. As a result of the ongoing replacement of the normal thyroid follicles by lymphocytes and fibrous tissue, there is eventual reduction in thyroid function because thyroid hormone production by the gland is impaired.2,10 Progression from subclinical hypothyroidism (normal FT4 but elevated TSH) to overt hypothyroidism occurs in a certain fraction

22 Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL PrActIcE
such as thyroid cancer, type 1 diabetes, rheumatoid arthritis, pernicious anemia and autoimmune collagen vascular diseases. Significantly increased concentration is considered significant and most frequently indicates thyroid autoimmune diseases such as Hashimoto’s thyroiditis or Graves’ disease.13 Young patients tend to have lower and occasionally negative levels. In this age group, even low titers signify the presence of thyroid autoimmunity.2 In our study, AMA was done by chemiluminescence immunoassay (CLIA). The value >60 U/ml was considered as positive. AMA was positive with values >150 U/ml in all 21 patients of Hashimoto’s thyroiditis. It was false positive in three patients out of which two had follicular adenoma and one had colloid goiter. Thus, AMA was found to be 100% sensitive as well as highly specific (95.31%) investigation for the diagnosis of Hashimoto’s thyroiditis.
Scintigraphy (usually obtained with Tc-99m or iodine-123) is useful in demonstrating the functional state of the thyroid at the time of clinical presentation and in differentiating autoimmune thyroiditis from other thyroid diseases, thereby influencing treatment.3
In Hashimoto’s thyroiditis, a mild decline in circulating thyroid hormones is sensed by the pituitary gland, and a compensatory rise in TSH secretion stimulates the gland to synthesize more thyroid hormone so that T3 and T4 levels return to normal. Thyroid follicles demonstrate a variable response to the chronic TSH stimulation, leading to patchy proliferation of these follicles. On a thyroid scan, this phenomenon manifests as areas of increased activity (follicles that respond to TSH) and of decreased activity (those that do not respond). This is shown as heterogenous uptake in thyroid scan. The image is characteristically that of a diffuse or mottled uptake in an enlarged gland, in striking contrast to the focal ‘cold’ and ‘hot’ areas of multinodular goiter. The uptake may be paradoxically high in few cases as thyroid follicles retain the ability to trap the iodine.2,6,7 Thus, heterogenous uptake of radionuclide should suspect Hashimoto’s thyroiditis.
At our institution, the vast majority of thyroid scintigraphic scans are done with Tc-99m per-technetate. Imaging was performed approximately
15 minutes after intravenous administration of 10 mCi of Tc-99m. In our study, 18 patients with Hashimoto’s thyroiditis showed heterogenous uptake in the scan and three patients showed cold nodule. Not a single false-positive was detected in our study.
Thus, thyroid scan was found to be highly sensitive (85.71%) as well as highly specific (100%) investigation for the diagnosis of Hashimoto’s thyroiditis.
Though, FNAC of thyroid provides a safe, simple and accurate method for diagnosis of thyroid disease, its diagnostic accuracy for Hashimoto’s thyroiditis is high only when multiple aspirations are used. The usefulness of increased number of aspirations has been stressed by Hamburger et al, who found that as the number of aspirations increase, false-negative results decrease.7 FNAC reveals lymphocytes, macrophages, scant colloid and a few epithelial cells which may show Hurthle cell change. In this study, FNAC was positive in six patients of hashimoto’s thyroiditis with no false-positive. Sensitivity of FNAC was found to be 28.57% and specificity was 100%. Thus, FNAC is highly specific but poorly sensitive for diagnosis of Hashimoto’s thyroiditis. The reason for poor sensitivity might be the single aspiration of the swelling in this study and further studies are warranted.
Although chronic inflammation, leading to neoplastic transformation, is a well-established clinical phenomenon, the link between Hashimoto’s thyroiditis and thyroid cancer remains controversial. Elevated TSH results in a stimulus for growth and function of thyroid epithelium. TSH is a recognized promoting factor in thyroid cancer.1 The possibility that an immunologic mechanism involved in the pathogenesis of papillary carcinoma stimulates lymphocytic infiltration in the thyroid tissue through an autoimmune mechanism is suggested.9 In our study, three patients of Hashimoto’s thyroiditis had associated papillary carcinoma.
Surgery has its place and efficacy in the treatment of selected patients with Hashimoto’s thyroiditis with compression symptoms, nodular forms with dominant nodules over 2 cm, suspicion for neoplasm, an unsightly neck appearance due to a large goiter or persistent pain.8,10 In this study, most of the patients of Hashimoto’s thyroiditis underwent surgery for pressure symptoms and unsightly neck appearance due to a large

23Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL PrActIcE
goiter (Fig. 1). Thyroiditis can make thyroid dissection more difficult and possibly increase the risk of surgical complications like mechanical damage, devascularization or inadvertent removal of the parathyroid glands, damage to recurrent laryngeal nerve.9 Inadvertent parathyroidectomy may lead to postoperative hypo-calcemia and tetany. We believe in doing meticulous capsular dissection in loose areolar tissue around the thyroid gland. Identification of recurrent laryngeal nerve in Behr’s triangle and tracing it upto it’s entry in the larynx is important. We tried to identify and preserve the blood supply of parathyroids in all patients.
Conclusion
Diagnosis of Hashimoto’s thyroiditis is suspected by the finding of a diffuse, smooth, firm to rubbery goiter in a young woman with euthyroid or hypothyroid metabolic status, and confirmed by high titers of AMA; heterogenous uptake of radionuclide in thyroid scan. These two are the most sensitive and specific investigations in the diagnosis of Hashimoto’s thyroiditis. FNAC is highly specific investigation but not as sensitive as AMA and thyroid scan.
Elevated TSH is also not found in significant number of patients. Thus, despite the availability of several tests for diagnosis of Hashimoto’s thyroiditis, AMA and thyroid scan remain the gold standard. When there is a dominant thyroid mass, we strongly believe in doing AMA and thyroid scan in every patient of thyroid swelling to rule out thyroiditis. Being a benign condition, accurate diagnosis reduces the rate of unnecessary operation, because hashimoto’s thyroiditis can be treated conservatively. If surgery is needed, availability of an experienced surgeon is important in order to avoid postoperative complications.
Acknowledgement
We would like to express our appreciation to Golwilkar Metropolis, Pune for doing the antimicrosomal antibody of our patients and giving prompt and cost-effective services.
ReferencesThomas CG Jr, Rutledge RG. Surgical intervention in chronic (Hashimoto’s) thyroiditis. Ann Surg 1981;193(6):769-76.Akamizu T, Amino N, Leslie J De Groot. Thyroid disease manager (Ch. 8). Hashimoto’s Thyroiditis. Last revised: August 11, 2008.McGraw-Hill Concise Dictionary of modern medicine 2002.Comtois R, Faucher L, Laflèche L. Outcome of hypothyroidism caused by Hashimoto’s thyroiditis. Arch Intern Med 1995;155(13):1404-8.Slatosky J, Shipton B, Wahba H. Thyroiditis: differential diagnosis and management. Am Fam Physician 2000;61(4):1047-52,1052.Intenzo CM, Capuzzi DM, Jabbur S, Kim SM, dePapp AE. Scintigraphic features of autoimmune thyroiditis. Radiographics 2001;21(4):957-64.Hamburger JI, Hamburger SW. Fine needle biopsy of thyroid nodules: avoiding the pitfalls. N Y State J Med 1986;86(5):241-9. Kon YC, DeGroot LJ. Painful Hashimoto’s thyroiditis as an indication for thyroidectomy: clinical characteristics and outcome in seven patients. J Clin Endocrinol Metab 2003;88(6):2667-72.Shih ML, Lee JA, Hsieh CB, Yu JC, Liu HD, Kebebew E, et al. Thyroidectomy for Hashimoto’s thyroiditis: complications and associated cancers. Thyroid 2008;18(7):729-34.Nenkov R, Radev R, Khristozov K, Kuzmanov Ia, Kornovski S, Kuzmanov S, et al. Hashimoto’s thyroiditis: indications for surgical treatment. Khirurgiia (Sofiia) 2005;(3):28-32.Nordyke RA, Gilbert FI Jr, Miyamoto LA, Fleury KA. The superiority of antimicrosomal over antithyro-globulin antibodies for detecting Hashimoto’s thyroiditis. Arch Intern Med 1993;153(7):862-5. Amino N, Tada H, Hidaka Y. Chronic (Hashimoto’s) Thyroiditis. In: Endocrinology. Volume 2. 4th edition, DeGroot LJ, Jameson JL, (Eds.), Saunder’s Publication 2001:1471-80.Lee SL, Odeke S, Nagelberg SB. eMedicine Specialties - Endocrinology - Thyroid - Hashimoto Thyroiditis. Mar 12, 2010.
n n n
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.

xxxxxxxxxxx
24 Asian Journal of Ear, Nose & Throat, January-March 2011
Relationship between Parent Perception of Hearing Loss in their Wards with Different Assessment Modalities in Children with Multiple Handicaps Noorain Alam*, Shamim Ansari**, Priyanka Mishra
Children with multiple disabilities have a combination of various disabilities that may include: Speech, physical mobility, learning,
mental retardation, visual, hearing, brain injury and possibly others. Along with multiple disabilities, they can also exhibit sensory losses and behavioural or social problems. Children with multiple disabilities - also referred to as multiple exceptionalities vary in severity and characteristics.
The judgment made by the clinician on children’s hearing abilities often involves a differential evaluation. Accurate hearing evaluations are difficult in children with multiple disabilities.
Approximately 25-33% of children with hearing loss have multiple potentially disabling conditions.1 This population requires modifications of diagnostic
AbstrAct
Aim of the study: Children with multiple disabilities have combination of various disabilities. Accurate hearing evaluation is difficult in this population. Audiologists generally employ a test battery approach which includes combining findings of parent impression with behavior observation audiometry (BOA) as well as auditory brainstem response (ABR) findings. Present study was done to find if there was any correlation between various steps in test battery for the children with multiple handicaps as well as to find out which disability is the most common among this population. Methodology: Total 103 number of children with multiple handicaps were chosen at random who were referred to AYJNIHH, Mumbai for audiological assessment. The three steps involved in assessment, that is parental impression, BOA and ABR findings were taken into account. The relationship was obtained using data analysis. Results: It was found that among children with multiple handicaps referred for audiological assessment, mental retardation was the most common (32.03%). It was also found that there were more contradictory findings between parent impression and ABR (48%) when compared with parent impression with BOA (38%). In between BOA and ABR contradictory findings were found in 41% of cases. Conclusion: There are wide contradictions among various steps involved in assessment of children with multiple handicaps. Implication: Audiologist should use a test battery approach to assess hearing ability of this population and audiologists should interpret findings carefully at each level.
Key words: Behavior observation audiometry, auditory brainstem response
*Lecturer, Dept. of Audiology and Speech CU Shah Medical College, Gujarat**Lecturer, Dept. of Audiology Ali Yavar Jung National Institute for the Hearing Handicapped, MumbaiAddress for correspondenceDr Noorain AlamLecturer, Dept. of Audiology and Speech CU Shah Medical College Surendranagar, GujaratE-mail: [email protected]
protocols as they are considered as ‘difficult to test’ population.
Different steps involved in assessing the multiple handicapped children can be summarized as:
Parental impression about the auditory status of the childBehavior observation audiometry/visual reinforce-ment audiometry (BOA/VRA)Brainstem evoked response audiometry (BERA)
To come to a proper diagnosis the audiologist needs to correlate all the information obtained from each modality of tests given above.
As parents observe children closely and are able to judge hearing status formally hence, their impression about the hearing is important. But in children with multiple handicaps they may relate lack of response to auditory stimuli to hearing loss which may be actually due to associated handicap. A skilled audiologist will decide the hearing status on BOA/VRA-based on subjective response of the client and this test shows poor test-retest reliability, and high inter- and intrasubject variability (Bench, Collyer, Mentz, and Wilson, 1976; Weber, 1969; Wilson and Thompson, 1984).2
cLINIcAL stUDY
25Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL stUDY
In auditory brainstem response (ABR), under good recording conditions, visual detection levels of wave V are usually within 10 dB of behavioral audiometric thresholds for click stimuli. Sometimes due to neuromaturational delay abnormal ABR recordings may be obtained. Whole test battery thus may show poor correlation among the different test modalities.
A study conducted by Kitagawa Kae et al3 demonstrated coincidence between a secular change in ABER and the conditioned orientation reflex (COR) audiometry in 229 multiply handicapped children with motor disorders. Improvement in behavioral hearing testing minimum response level, including mental and physical development, was observed in 111 cases. There were 92 cases of ABR, and in 37 of them there was no correlation between the ABR and COR findings. The initial diagnosis in 44 patients was moderate-to-severe hearing loss, and a secular change was observed in 37 of them. The ABR thresholds and the COR minimum reaction level decreased in 11 patients, whereas in 17 patients ABR thresholds remained unchanged and only the COR values decreased. The final diagnosis was moderate-to-severe hearing loss in 18 patients. The study shows the need of correlating different test modalities repeated over duration of time. Present study focused on the correlation of findings of different steps involved in the initial hearing assessment of children with multiple handicaps.
Aim of the Study
To provide evidence if three steps of the tests i.e., parent impression, BOA/VRA and ABR have a similar or contradictory findings.
Methodology
One-hundred three children with multiple handicaps less than three years of age, were selected and were referred to Ali Yavar Jung National Institute for the Hearing Handicapped, Mumbai for audiological assessment. The findings of all the steps involved in diagnosis of such population mainly parent impression, BOA/VRA and ABR were correlated. Descriptive data analysis was performed.
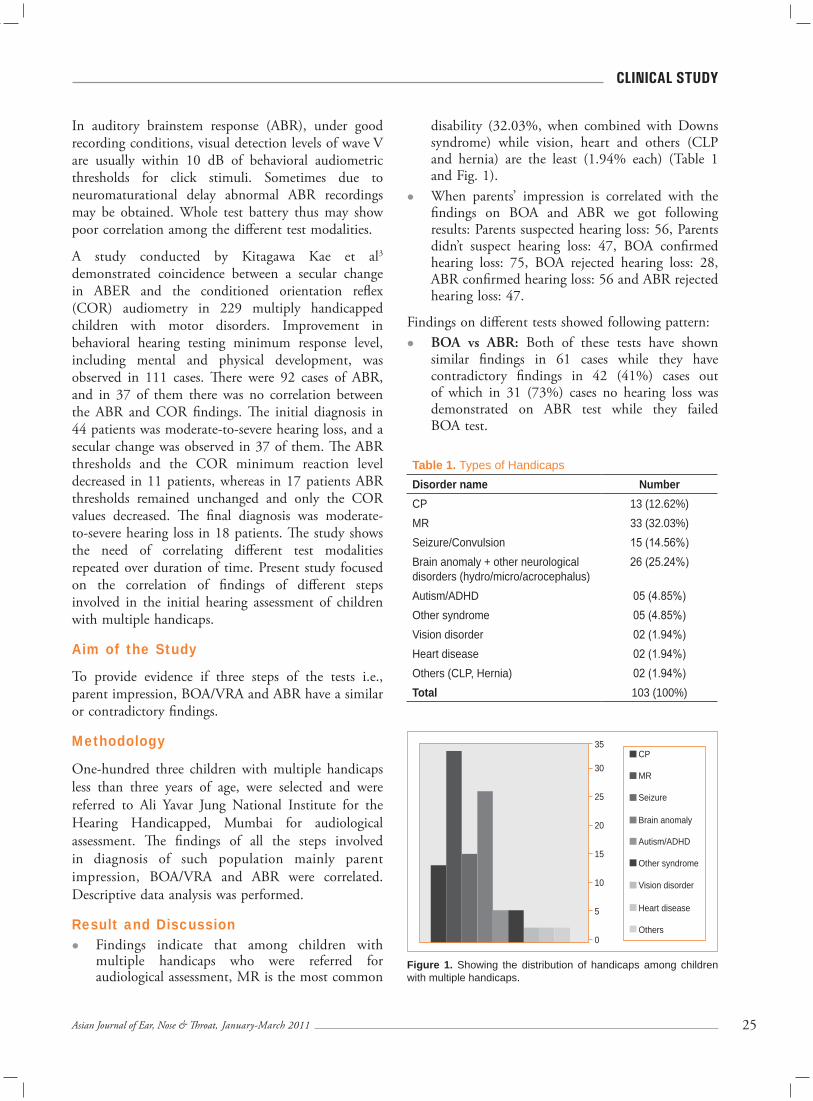
Result and DiscussionFindings indicate that among children with multiple handicaps who were referred for audiological assessment, MR is the most common
disability (32.03%, when combined with Downs syndrome) while vision, heart and others (CLP and hernia) are the least (1.94% each) (Table 1 and Fig. 1).When parents’ impression is correlated with the findings on BOA and ABR we got following results: Parents suspected hearing loss: 56, Parents didn’t suspect hearing loss: 47, BOA confirmed hearing loss: 75, BOA rejected hearing loss: 28, ABR confirmed hearing loss: 56 and ABR rejected hearing loss: 47.
Findings on different tests showed following pattern:BOA vs ABR: Both of these tests have shown similar findings in 61 cases while they have contradictory findings in 42 (41%) cases out of which in 31 (73%) cases no hearing loss was demonstrated on ABR test while they failed BOA test.
Table 1. Types of HandicapsDisorder name NumberCP 13 (12.62%)MR 33 (32.03%)Seizure/Convulsion 15 (14.56%)Brain anomaly + other neurological disorders (hydro/micro/acrocephalus)
26 (25.24%)
Autism/ADHD 05 (4.85%)Other syndrome 05 (4.85%)Vision disorder 02 (1.94%)Heart disease 02 (1.94%)Others (CLP, Hernia) 02 (1.94%)Total 103 (100%)
Figure 1. Showing the distribution of handicaps among children with multiple handicaps.
CP
MR
Seizure
Brain anomaly
Autism/ADHD
Other syndrome
Vision disorder
Heart disease
Others
35
30
25
20
15
10
5
0
26 Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL stUDY
Parent impression vs BOA: Both of these tests have shown similar findings in 64 cases but have contradictory findings in 39 (38%) cases out of which in 28 (71.8%) cases parent did not suspect hearing loss in their wards but BOA test failed them.Parent impression vs ABR: Both of these test have shown similar findings in 55 cases but have contradictory findings in 48 (46.6%) cases out of which in 24 (50%) cases parent did not suspect hearing loss in their wards but hearing loss was confirmed in them.
Conclusion
The findings clearly show that in multiple handicap population there are more number of children with mental retardation and the various steps involved in audiological assessment of this population show wide contradiction.
Implication
The study emphasises that children with multiple handicaps need to be assessed thoroughly and the outcome of the test may not be in correlation with each other.
ReferencesRobert A. Dobia, Susan Van Hemal. National Research Council (U.S.) Committee on Disability Determination for Individuals in the Hearing Impair-ments 2004:182.
Thompson G, Wilson WR. Clinical application of visual reinforcement audiometry. Sem Hearing 1984;5:85-99.
Kitagawa Kae, Go Mitsuru, Shintani Tomoko, Himi Tetsuo. Assessment of hearing in children with multiple disabilities and motor disorders. Audiol Jpn 2003;46(4):268-74.
n n n
1.
2.
3.
Tebbets JB. Secondary tip modification: shaping and position of nasal tip using non-destructive techniques. In: Primary Rhinoplasty: A New Approach to the Logic and the Techniques. Tebbetts JB (Ed.), Mosby, St Louis 1998:261-441.Fred GB. Nasal tip rhinoplasty. Ann Otol Rhinol Laryngol 1950;59:215-23.Foda HM. Management of the droopy tip: A comparison of three alar cartilage-modifying techniques. Plast Reconstr Surg 2003;112(5):1408-17.Foda HM, Kridel RW. Lateral crural steal and lateral crural overlay: an objective evaluation. Arch Otolaryngol Head Neck Surg 1999;125(12):1365-70.Guyuron B, Varghai A. Lengthening the nose with a tongue-and-groove technique. Plast Reconstr Surg 2003;111(4):1533-29; discussion 1540-1.Kridel RW, Scott BA, Foda HM. The tongue-in-groove technique in septorhinoplasty. A 10-year experience.
17.
18.
19.
20.
21.
22.
Arch Facial Plast Surg 1999;1(4):246-56; discussion 257-8.
Toriumi DM. Structure approach in rhinoplasty. Facial Plast Surg Clin North Am 2002;10(1):1-22.
Naficy S, Baker SR. Lengthening the short nose. Arch Otolaryngol Head Neck Surg 1998;124(7):809-13.
Dyer WK 2nd, Yune ME. Structural grafting in rhinoplasty. Facial Plastic Surg 1997;13(4):269-77.
Crumley RL, Lanser M. Quantitative analysis of nasal tip projection. Laryngoscope 1988;98(2):202-8.
Spörri S, Simmen D, Briner HR, Jones N. Objective assessment of tip projection and the nasolabial angle in rhinoplasty. Arch Facial Plast Surg 2004;6(5):295-8.
Ingels K, Orhan KS. Measurement of preoperative and postoperative nasal tip projection and rotation. Arch Facial Plast Surg 2006;8(6):411-5.
n n n
23.
24.
25.
26.
27.
28.
...Cont’d from page 17

xxxxxxxxxxx
27Asian Journal of Ear, Nose & Throat, January-March 2011
Prognostic Value of Natural Antioxidant Enzymes Estimation in Treatment of Oral Submucous FibrosisBhavesh K Modi*, Ashish Katarkar**, Amit Tyagi†
Oral submucous fibrosis (OSMF) is a chronic insidious process characterized by fibrosis in the submucosal layers of oral cavity and
pharynx. The condition was first described by Joshi in 1953.1 Prevalence of disease is 2-5 per 1,000 in the Indian subcontinent.
OSMF causes changes not only in the submucous layer but also in the muscles. In the beginning it gives rise to symptoms like oral ulcers and later on there is progressively decreased mouth opening which has been confirmed by previous researches.2-4 Oxygen free radicals (OFR) give rise to this condition because of their potential toxicity to the cells.
Due to their high reactive nature OFR can readily combine with other molecules such as enzymes, receptors and ion pumps causing oxidation directly
and inactivating or inhibiting their normal function. Various authors have suggested the roles of oxygen toxicity and antioxidant vitamins.5-7 Tobacco-chewing, smoking have been suggested as risk factors for the development of OSMF and carcinoma of oral cavity.
Objective
The study was to know the correlation between the estimation of enzymes in blood sample before and after antioxidant therapy and its clinical importance. Study was designed to know the prognostic value of the natural antioxidant enzymes estimation before and after therapy. The study compared the pre- and post-antioxidant therapy blood levels of antioxidant enzymes in patients with OSMF.
Material and Methods
The present study was conducted in Surendranagar district of Saurashtra region of Gujarat in India. Saurashtra region is an ideal for this study because of high prevalence of tobacco-chewing habit and high incidence of OSMF. Keeping the chewing tobacco in lower gingivolabial sulcus and chewing Gutkha is a common addiction in Gujarat.
AbstrAct
Oral submucous fibrosis (OSMF) is quite common in the Indian subcontinent particularly in western India especially Gujarat. This study was designed to know the prognostic value of the natural antioxidant enzymes estimation before and after therapy. The result showed that estimation of natural antioxidant enzymes is important in guiding the clinician to decide the further line of management. Purpose: Study was designed to know the prognostic value of the natural antioxidant enzymes estimation before and after therapy. The study compared the pre- and post-therapy blood levels of antioxidant enzymes in patients with oral submucous fibrosis. Material and methods: In the present study, we selected 25 control cases (normal) aged above 12 years without any oral habit; oral symptoms and diseases were taken to find out the normal value of enzymes in blood of 50 tobacco-chewing subjects with frank OSMF with 1-2 finger mouth opening. The subjects having smoking habits were excluded from the study. Results: After one month of antioxidant supplementation therapy the levels were reversed i.e., SOD and CAT activity were increased and GSH and MDA levels were decreased in the tobacco chewers as compared to before treatment. Conclusion: Pre- and post-antioxidant supplementation therapy a marked variation in levels of glutathione was observed. In addition, it was noticed that the levels tended to shift closer to control/normal values post-antioxidant supplementation therapy. The value of glutathione and other enzymes estimated as a prognostic marker could be ratified if further studies are carried out on a larger scale over a sustained period of time.
Key words: Oral submucous fibrosis, antioxidants, antioxidant enzymes
*Ex-Associate Professor **Associate Professor, Dept. of ENT†Assistant Professor, Dept. of BiochemistryCU Shah Medical College, Gujarat Address for correspondenceDr Ashish KatarkarB-10, Doctor’s QuartersCU Shah Medical CollegeDudhrej Road, Surendranagar - 363 001, GujaratE-mail: [email protected]; [email protected]
cLINIcAL stUDY
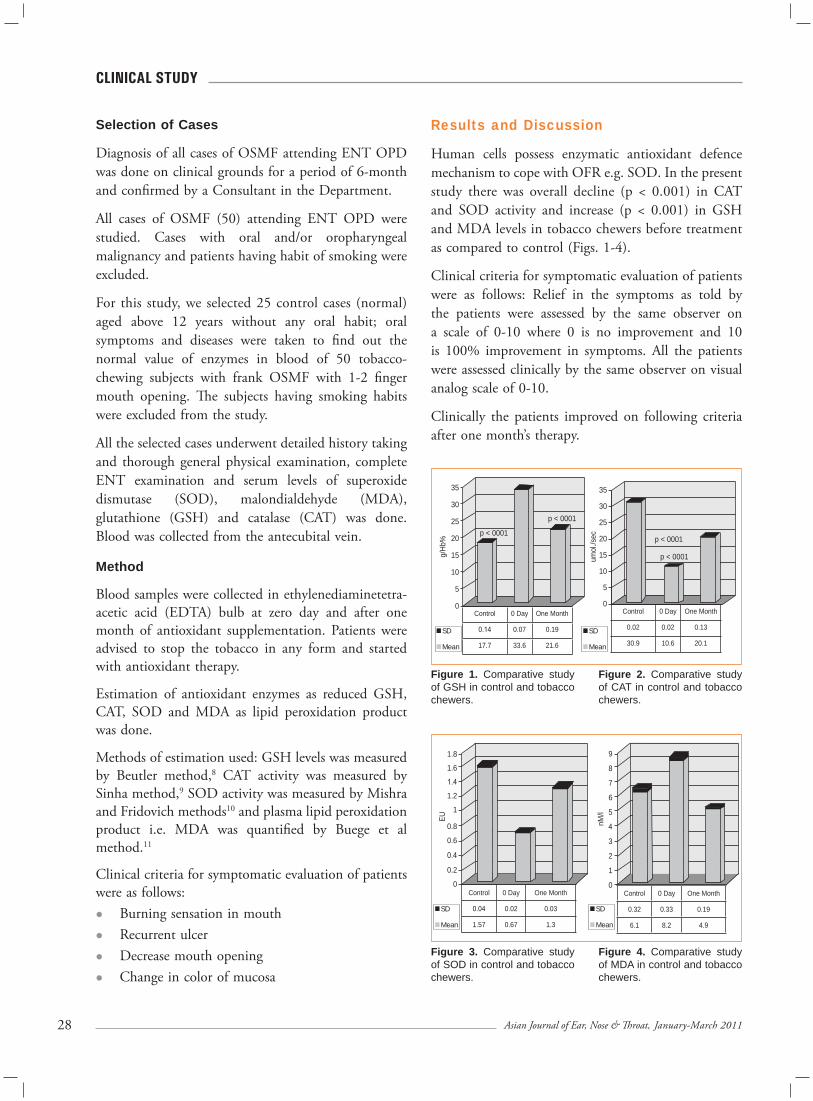
28 Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL stUDY
Selection of Cases
Diagnosis of all cases of OSMF attending ENT OPD was done on clinical grounds for a period of 6-month and confirmed by a Consultant in the Department.
All cases of OSMF (50) attending ENT OPD were studied. Cases with oral and/or oropharyngeal malignancy and patients having habit of smoking were excluded.
For this study, we selected 25 control cases (normal) aged above 12 years without any oral habit; oral symptoms and diseases were taken to find out the normal value of enzymes in blood of 50 tobacco-chewing subjects with frank OSMF with 1-2 finger mouth opening. The subjects having smoking habits were excluded from the study.
All the selected cases underwent detailed history taking and thorough general physical examination, complete ENT examination and serum levels of superoxide dismutase (SOD), malondialdehyde (MDA), glutathione (GSH) and catalase (CAT) was done. Blood was collected from the antecubital vein.
Method
Blood samples were collected in ethylenediaminetetra-acetic acid (EDTA) bulb at zero day and after one month of antioxidant supplementation. Patients were advised to stop the tobacco in any form and started with antioxidant therapy.
Estimation of antioxidant enzymes as reduced GSH, CAT, SOD and MDA as lipid peroxidation product was done.
Methods of estimation used: GSH levels was measured by Beutler method,8 CAT activity was measured by Sinha method,9 SOD activity was measured by Mishra and Fridovich methods10 and plasma lipid peroxidation product i.e. MDA was quantified by Buege et al method.11
Clinical criteria for symptomatic evaluation of patients were as follows:
Burning sensation in mouthRecurrent ulcerDecrease mouth openingChange in color of mucosa
Results and Discussion
Human cells possess enzymatic antioxidant defence mechanism to cope with OFR e.g. SOD. In the present study there was overall decline (p < 0.001) in CAT and SOD activity and increase (p < 0.001) in GSH and MDA levels in tobacco chewers before treatment as compared to control (Figs. 1-4).
Clinical criteria for symptomatic evaluation of patients were as follows: Relief in the symptoms as told by the patients were assessed by the same observer on a scale of 0-10 where 0 is no improvement and 10 is 100% improvement in symptoms. All the patients were assessed clinically by the same observer on visual analog scale of 0-10.
Clinically the patients improved on following criteria after one month’s therapy.
Figure 1. Comparative study of GSH in control and tobacco chewers.
Figure 2. Comparative study of CAT in control and tobacco chewers.
Figure 3. Comparative study of SOD in control and tobacco chewers.
Figure 4. Comparative study of MDA in control and tobacco chewers.
35
30
25
20
15
10
5
0
35
30
25
20
15
10
5
0
g/Hb
%
umol
./sec
Control 0 Day One Month
0.14 0.07 0.19
17.7 33.6 21.6
Control 0 Day One Month
0.02 0.02 0.13
30.9 10.6 20.1
1.8
1.6
1.4
1.2
1
EU
0.8
0.6
0.4
0.2
0
9
8
7
6
5
4
3
2
1
0
nM/l
Control 0 Day One Month
0.04 0.02 0.03
1.57 0.67 1.3
Control 0 Day One Month
0.32 0.33 0.19
6.1 8.2 4.9
SD
Mean
SD
Mean
p < 0001
p < 0001
p < 0001
p < 0001
SD
Mean
SD
Mean
2�Asian Journal of Ear, Nose & Throat, January-March 2011
cLINIcAL stUDY
Burning sensation in mouth - more than 90% improvementRecurrent ulcer - 90% improvementMouth opening - about 30% improvementChange in color of mucosa - about 40% improvement
After one month of antioxidant therapy supple-mentation the levels were reversed i.e., SOD and CAT activity were increased and GSH and MDA levels were decreased in the tobacco chewers as compared to before treatment. Antioxidant therapy included natural antioxidant enzymes and vitamins of synthetic agents in twice-daily dosage.12,13 Compositions of the antioxidant used are as follows.
Antioxidant vitamin A, E, C, and B6, eicosapentaenoic acid, docosahexaenioc acid, zinc sulfate, folic acid, manganese, copper, chromium and selenium.
Treatment was continued for three months and patients were followed-up to one year.
The present study showed the importance of prognostic value of the antioxidant enzymes estimation before and after the therapy as it guided to continue the therapy along with the clinical parameters given above. So, we are of the view that the estimation of antioxidant enzymes can guide the clinician whether the patients are responding to the therapy or not.
Conclusion
The present study revealed that antioxidant therapy14,15 along with estimation of antioxidant enzyme can give better results and can guide the clinician for further course of action. Also, this oral therapy can reduce the incidence of OSMF in long-term follow-up, rate of which is very high in the subcontinent thus reducing the treatment cost and morbidity and mortality.
Post-antioxidant therapy we suggest further research and study on a large population and do enzyme estimation at 3-month and one year - for considering it an evidence-based treatment for submucous fibrosis.
ReferencesJoshi SG. Submucous fibrosis of palate and pillars. Indian J Otolaryngol 1953;4:1-4.Gupta SC, Khanna S, Singh M, Singh PA. Histological changes to palatal and paratubal muscles in oral submucous fibrosis. J Laryng Otology 200;114(12):947-50.Babu S, Bhat RV, Kumar PU, Sesikaran B, Rao KV, Aruna P, et al. A comparative clinicopathological study of oral submucous fibrosis in habitual chewers of pan masala and betelquid. J Toxicol Clin Toxicol 1996;34(3):317-22.Rajendran R. Oral submucous fibrosis: etiology, pathogenesis and future research. Bull World Health Organ 1994;72(6):985-96.Maher R, Aga P, Johnson NW, Sankarnarayanan R, Wamakulasuriya S. Evaluation of multiple micronutrient supplementations in the management of oral submucous fibrosis in Karachi, Pakistan. Nutr Cancer 1997;27(1):41-7.Frei B. Reactive oxygen species and antioxidant vitamins: mechanism of action. Am J Med 1994;97(3):S5-S13.Marklund S, Marklund G. Involvement of the superoxide anion radical in the autoxidation of pyrogallol and a convenient assay for superoxide dismutase. Eur J Biochem 1974;47(3):469-74.Beutler E, Duron O, Kelly BM. Improved method for the determination of blood glutathione. J Lab Clin Med 1963;61:882-8.Sinha AK. Colorimetric assay of catalase. Anal Biochem 1972;47(2):389-94.Fridovich J. Superoxide dismutase; Adv Enzymol Relat Areas Mol Biol 1974;41:35-97.Buege et al. Estimation of malondialdehyde. Methods on Enzymology, 1975.Maxwell SR. Prospects for the use of antioxidant therapies. Drugs 1995;49(3):345-61.Gupta S, Reddy MVR, Harinath BC. Role of oxidative stress and antioxidants in aetiopathogenesis and management of oral sub mucous fibrosis. Indian J Clin Biochem 2004;19(1):138-41.Canniff JP, Harvey W, Harris M. Oral submucous fibrosis: its pathogenesis and management. Br Dent J 1986;160(12):429-34.Sen CK. Oxygen toxicity and antioxidants: state of the art. Indian J Physiol Pharmacol 1995;39(3):177-96.
n n n
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
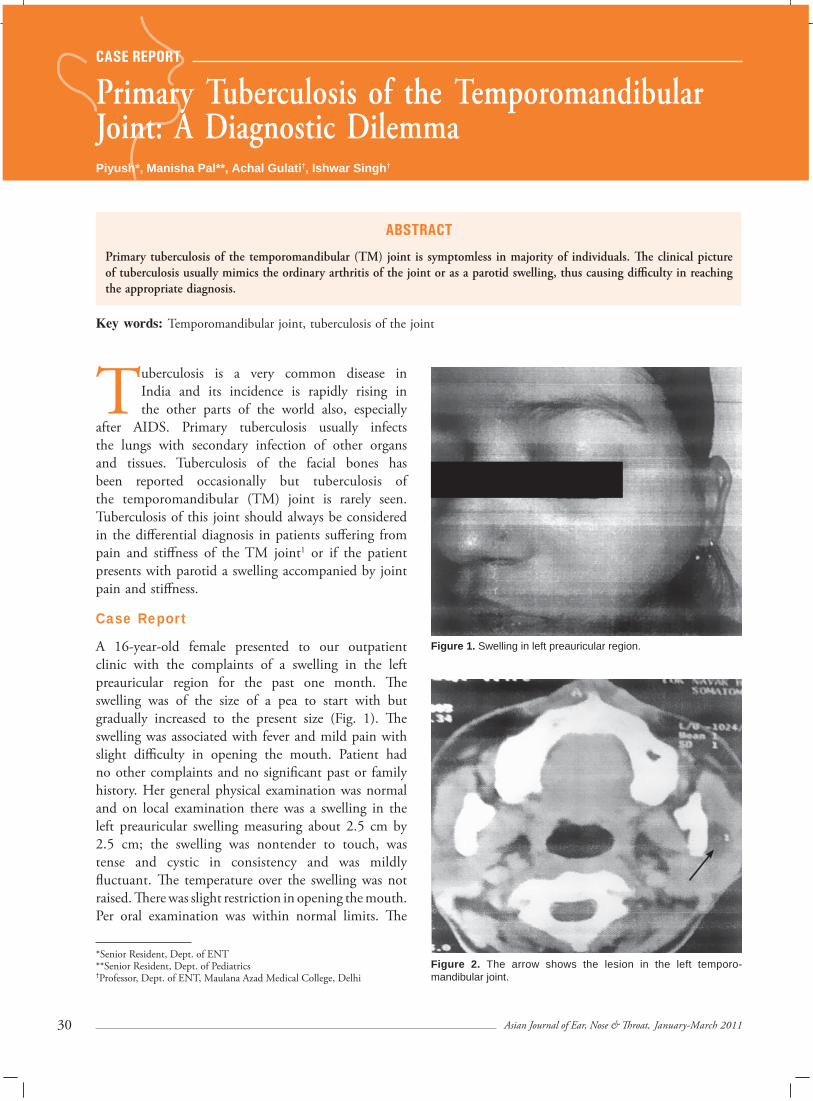
xxxxxxxxxxx
30 Asian Journal of Ear, Nose & Throat, January-March 2011
Primary Tuberculosis of the Temporomandibular Joint: A Diagnostic DilemmaPiyush*, Manisha Pal**, Achal Gulati†, Ishwar Singh†
Tuberculosis is a very common disease in India and its incidence is rapidly rising in the other parts of the world also, especially
after AIDS. Primary tuberculosis usually infects the lungs with secondary infection of other organs and tissues. Tuberculosis of the facial bones has been reported occasionally but tuberculosis of the temporomandibular (TM) joint is rarely seen. Tuberculosis of this joint should always be considered in the differential diagnosis in patients suffering from pain and stiffness of the TM joint1 or if the patient presents with parotid a swelling accompanied by joint pain and stiffness.
Case Report
A 16-year-old female presented to our outpatient clinic with the complaints of a swelling in the left preauricular region for the past one month. The swelling was of the size of a pea to start with but gradually increased to the present size (Fig. 1). The swelling was associated with fever and mild pain with slight difficulty in opening the mouth. Patient had no other complaints and no significant past or family history. Her general physical examination was normal and on local examination there was a swelling in the left preauricular swelling measuring about 2.5 cm by 2.5 cm; the swelling was nontender to touch, was tense and cystic in consistency and was mildly fluctuant. The temperature over the swelling was not raised. There was slight restriction in opening the mouth. Per oral examination was within normal limits. The
AbstrAct
Primary tuberculosis of the temporomandibular (TM) joint is symptomless in majority of individuals. The clinical picture of tuberculosis usually mimics the ordinary arthritis of the joint or as a parotid swelling, thus causing difficulty in reaching the appropriate diagnosis.
Key words: Temporomandibular joint, tuberculosis of the joint
*Senior Resident, Dept. of ENT**Senior Resident, Dept. of Pediatrics†Professor, Dept. of ENT, Maulana Azad Medical College, Delhi
Figure 1. Swelling in left preauricular region.
Figure 2. The arrow shows the lesion in the left temporo- mandibular joint.
cAsE rEPOrt

31Asian Journal of Ear, Nose & Throat, January-March 2011
cAsE rEPOrt
provisional diagnosis of parotid abscess was considered. The patient was prescribed oral antibiotics and NSAIDs and was sent for fine-needle aspiration cytology. CT scan was advised to find the extent of the swelling and to rule out any other pathology like parotid cysts. Fine-needle cytology showed tuberculosis and on CT scan it was found that the swelling was not of the parotid but an abscess involving the TM joint. There was no destruction of the joint (Fig. 2). Chest X-ray was normal, Mantoux was positive and ESR was also raised. Patient was advised a full course of antitubercular therapy; antigravity aspiration of the abscess was undertaken and physiotherapy of the TM joint was advised. Patient improved symptomatically and now after the completion of the course she has no complaints of the TM joint.
Discussion
The prevalence of tuberculosis of the bones and the joints has been on the rise and this increase is usually related to the AIDS disease. Extrapulmonary tuberculosis is a diagnostic challenge for the clinicians, especially in the absence of any pulmonary signs and symptoms. Usually the tuberculosis of the TM joint is misdiagnosed as an ordinary arthritis, and if there is a parotid swelling it is usually misdiagnosed as a parotid pathology ignoring the underlying joint pathology. Thus tuberculosis of the TM joint is a diagnostic dilemma and poses a diagnostic challenge.2
The TM joint may be affected from tuberculosis in the adjacent mandibular body or rarely by hematogenous route. The two factors cited for the rarity of the tuberculosis of the TM joint are as follows:3
High local immunity of the oral mucosaThe predilection of tubercle bacilli for the cancellous bone.
When tuberculosis presents as a lesion in the TM joint the correct diagnosis is of essence to start the appropriate treatment. The diagnosis of the joint tuberculosis in the developing countries is made on the basis of clinical and radiological examination.4
It is possible that the low frequency of the tuberculosis of the TM joint reported may be due to misdiagnosis, thus one should always keep a differential diagnosis when such a situation is presented in the clinics.
Conclusion
Tuberculosis of the TM joint is a very rare disease and has been reported very infrequently in literature of all surgical disciplines. Radiology is important in the diagnosis and the differentiation of this entity from the parotid swelling as well as from the ordinary arthritis of the TM joint, thus helping in instituting the appropriate management. Antitubercular therapy, aspiration drainage of cold abscess and physiotherapy helps in treating the disease. Open surgery may be reserved for cases not responding the above treatment. If the disease is left untreated it will cause fibrous ankylosis while a discharging abscess can lead on to infection and destruction of the joint and bony ankylosis.5,6 A corrective osteotomy may be required for bony ankylosis.7
ReferencesWU H, Wang QZ, Jin Y. Tuberculosis of the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85(3):243.
Soman D, Davies SJ. A suspected case of tuberculosis of the temporomandibular joint. Br Dent J 2003; 194(1):23-4.
Meng CM. Tuberculosis of the mandible. J Bone J Surg 1940;22:17-27.
Shanmugasundaram TK. Tuberculosis of spine. Indian J Tubercul 1982;29(4):213-21.
Tuli SM. Tuberculosis of the Skeletal System. Jaypee Brothers Medical Publishing, 3rd edition, 2003.
Matta IR, Karnik PP, Pathare PS, Potdar VV. Tuberculosis of the temporomandibular joint. Indian J Otolaryngol Head Neck Surg 2005;57(4):337-9.
Allbrook D, Kirkaldy-Willis WH. The restoration of the articular surface after joint excision; an experimental study with cartilage implants. J Bone Joint Surg 1958;40-B(4):742-64.
n n n
1.
2.
3.
4.
5.
6.
7.

xxxxxxxxxxx
32 Asian Journal of Ear, Nose & Throat, January-March 2011
Use of Temporalis Myofascial Flap for Interpositional Arthroplasty in Temporomandibular Joint AnkylosisAmarjeet Gambhir*, Gita Rani**
AbstrAct
Ankylosis of the temporomandibular joint (TMJ) is one of the most exasperating handicaps, a human being can suffer from. A variety of materials such as dermal grafts, auricular cartilage, costochondral graft and fascia lata have been used as TMJ disk replacement after surgery. The temporalis muscle and fascia flap has previously been used to support and replace orbital contents, and to reconstruct the oral cavity and maxillofacial region following ablative surgery. This article describes the successful application of temporalis muscle and fascia flap for interpositioning arthroplasty following release of TMJ ankylosis.
Key words: Ankylosis, graft, arthroplasty, recurrence
*Assistant Professor Dept. of Oral and Maxillofacial Surgery MM College of Dental Sciences and Research, Mullana, Ambala**Assistant Professor, Dept. of Prosthodontics Christian Dental College, LudhianaAddress for correspondenceDr Amarjeet GambhirA-33, Saraswati Garden Ramesh Nagar, New Delhi - 110 015E-mail: [email protected]
Bone regenerationInadequate postoperative physiotherapyIncomplete resectionNonavailability of satisfactory interpositional material
Plethora of interpositioning materials have been used with variable amount of success, yet successful rehabilitation of patients with ankylosis continues to be a challenge for surgeons. This article describes the successful use of temporalis myofascial flap as an interpositioning material for TMJ ankylosis.
Case Report
A 10-year-old male child reported to maxillofacial OPD of Nair Hospital Dental College, Mumbai with the chief complaint of restricted mouth opening and difficulty in eating and speech since five years. Patient gave history of trauma to chin due to fall at the age of five years. However, no treatment was taken for the same. Oral opening reduced gradually over the next few years to the present value.
His past medical history, family and personal history was noncontributory. Patient was thoroughly evaluated systemically and clinically. Extraoral examination revealed an obvious facial asymmetry with deviation of chin towards the left side of face (Fig. 1). There was flattening of face on right side and fullness on left side with retruded mandible and chin and an accentuated left antegonial notch. Right TMJ movements were palpable in all excursions, while left
cAsE rEPOrt
Ankylosis is a Greek terminology meaning ‘stiff joint’. Ankylosis of the temporomandibular joint (TMJ) is a serious and disabling condition
because it not only compromises joint function, but if acquired at an early age results in severe cosmetic deformity, affecting the individual’s psyche and self esteem. Left untreated, it can lead to distressing sequelae such as compromised facial growth and development, impaired speech and nutrition, respiratory distress, malocclusion and so on.
TMJ ankylosis is classified by location (intra-articular or extra-articular), type of tissue involved (bone, fibrous or fibro-osseous), and extent of fusion (complete or incomplete).1 Trauma, infection, radiotherapy, surgical excision of TMJ tumors and systemic disease can all result in mandibular hypomobility.2
Though over the years, the technique for releasing TMJ ankylosis seems to have been standardized, high recurrence rate is a persistent problem bothering patients as well as surgeons. The exact cause of recurrence is difficult to pinpoint. It has been attributed to factors such as:
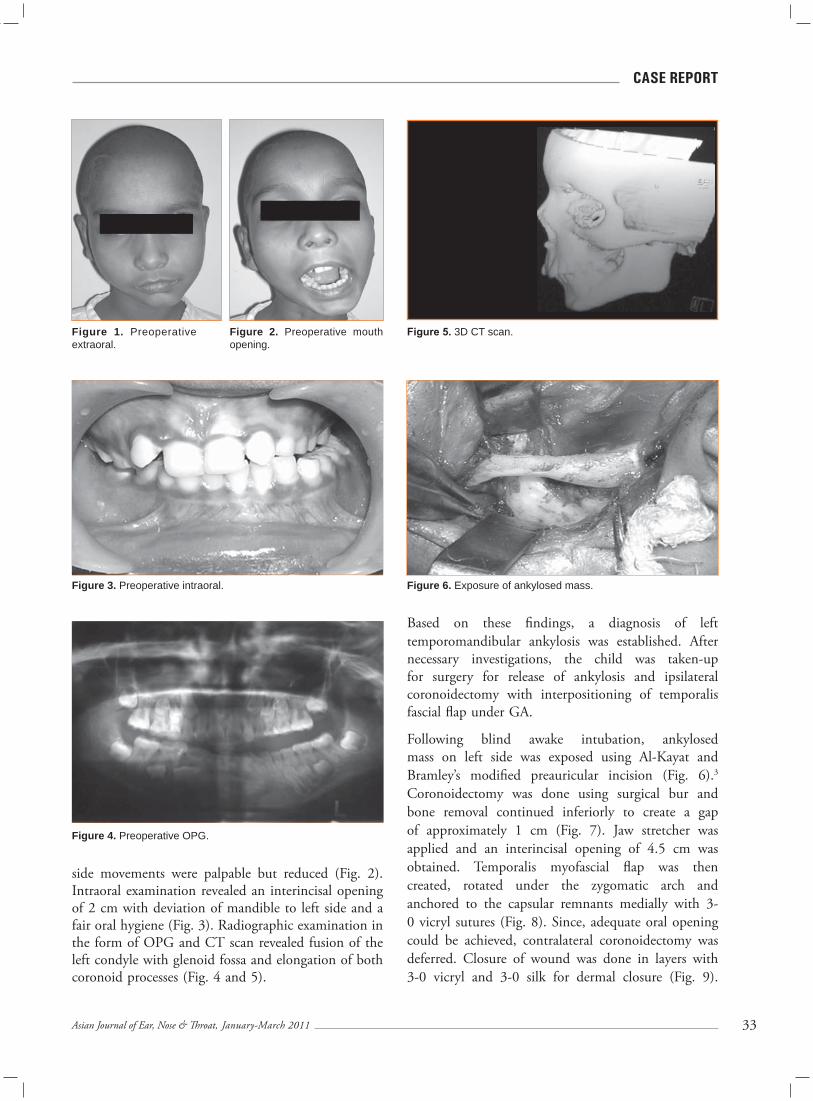
33Asian Journal of Ear, Nose & Throat, January-March 2011
cAsE rEPOrt
side movements were palpable but reduced (Fig. 2). Intraoral examination revealed an interincisal opening of 2 cm with deviation of mandible to left side and a fair oral hygiene (Fig. 3). Radiographic examination in the form of OPG and CT scan revealed fusion of the left condyle with glenoid fossa and elongation of both coronoid processes (Fig. 4 and 5).
Figure 1. Preoperative extraoral.
Figure 2. Preoperative mouth opening.
Figure 3. Preoperative intraoral.
Figure 4. Preoperative OPG.
Figure 5. 3D CT scan.
Figure 6. Exposure of ankylosed mass.
Based on these findings, a diagnosis of left temporomandibular ankylosis was established. After necessary investigations, the child was taken-up for surgery for release of ankylosis and ipsilateral coronoidectomy with interpositioning of temporalis fascial flap under GA.
Following blind awake intubation, ankylosed mass on left side was exposed using Al-Kayat and Bramley’s modified preauricular incision (Fig. 6).3 Coronoidectomy was done using surgical bur and bone removal continued inferiorly to create a gap of approximately 1 cm (Fig. 7). Jaw stretcher was applied and an interincisal opening of 4.5 cm was obtained. Temporalis myofascial flap was then created, rotated under the zygomatic arch and anchored to the capsular remnants medially with 3-0 vicryl sutures (Fig. 8). Since, adequate oral opening could be achieved, contralateral coronoidectomy was deferred. Closure of wound was done in layers with 3-0 vicryl and 3-0 silk for dermal closure (Fig. 9).

34 Asian Journal of Ear, Nose & Throat, January-March 2011
cAsE rEPOrt
Figure 7. Gap arthroplasty.
Figure 8. Flap created.
Figure 9. Flap interposed and sutured.
Figure 10. Postoperative mouth opening.
Figure 11. Postoperative OPG.
Discussion
At our institute, we have been privileged to follow-up a large number of cases of TMJ ankylosis treated by adaptation of Kaban’s protocol4 as well as using various other interpositioning materials on long-term basis. It can be concluded that no single method has produced uniform results.
Interpositional arthroplasty has become the mainstay of treatment nowadays as it possibly reduces recurrence and also maintains ramus height to certain extent.5 Till date, a variety of interpositioning materials ranging from autogenous to alloplastic have been used with variable success rate. Alloplastic materials have fallen into disfavor due to long-term complications like foreign body reaction, condylar resorption and malocclusion. Autogenous materials are the first choice. Costochondral graft is good in maintaining the ramus height and can partially
Jaw physiotherapy was started from the first post-operative day (Figs. 10 and 11). Postoperative wound healing was satisfactory and sutures were removed on 10th day. There was no evidence of facial nerve injury. Patient maintained oral opening of 4.4 cm at follow-up visit after 1-year.

35Asian Journal of Ear, Nose & Throat, January-March 2011
cAsE rEPOrt
replace the condylar growth center. But nowadays, its use is decreasing due to disadvantages like increased operating time, additional surgical site and donor site morbidity such as pneumothorax and pleuritic pain. Moreover, its growth pattern is quite unpredictable, increasing the possibility of re-ankylosis and the need for secondary corrective osteotomies.6
Temporalis muscle and/or fascia flap has given consistently good results when used as an inter-positioning material following ankylosis release. It has the advantage that its arc of rotation can be altered by basing the flap inferiorly or posteriorly. Additionally, its dependable blood supply and proximity to TMJ make it a versatile flap for lining the glenoid fossa.7 The muscle and fascia are of adequate thickness, and the long-term viability of the flap has been demonstrated.8
Conclusion
It can be concluded that the temporalis fascial flap satisfies most of the requirements of an ideal interpositioning material following ankylosis release. Its excellent blood supply, versatility and minimal donor site morbidity are the primary advantages.
Acknowledgement
We are extremely thankful to Dr Neelima Malik, Professor, and Dr Mohan Deshpandey, Associate
Professor, Oral and Maxillofacial Surgery, for their guidance and support.
References Perrott DH, Kaban LB. Temporomandibular joint ankylosis in children. Oral Maxillofac Clin North Am 1994;6:187.
Topazian RG. Etiology of ankylosis of temporo-mandibular joint: analysis of 44 cases. J Oral Surg Anesth Hosp Dent Serv 1964;22:227-33.
Al-Kayat A, Bramley P. A modified preauricular approach to the temporomandibular joint and malar arch. Br J Oral Surg 1979;17(2):91-103.
Kaban LB, Perrott DH, Fischer K. A protocol for management of temporomandibular joint ankylosis. J Oral Maxillofac Surg 1990;48(11):1145-51.
Topazian RG. Comparison of gap and interposition arthroplasty in the treatment of temporomandibular joint ankylosis. J Oral Surg 1966;24(5):405-9.
Guyuron B, Lasa CI Jr. Unpredictable growth pattern of costochondral graft. Plast Reconstr Surg 1992;90(5):880-6; discussion 887-9.
Kaban LB, Pogrel MA. Use of temporalis muscle and fascia flap in temporomandibular joint surgeries. IJOMS 1991;20:219.
Umeda H, Kaban LB, Pogrel MA, Stein M. Long- term viability of temporalis muscle/fascia flap used for temporomandibular joint reconstruction. J Oral Maxillofac Surg 1993;51(5):530-3; discussion 534.
n n n
1.
2.
3.
4.
5.
6.
7.
8.

xxxxxxxxxxx
36 Asian Journal of Ear, Nose & Throat, January-March 2011
An Unusual and Rare Case Report of External Auditory Canal CholesteatomaNishi Gupta*, Nidhi Dhawan*, Alok Kumar*, Parul Mathur*
Case History
In this case a 35-year-old woman presented to our OPD with complaint of hearing loss and pain in the right ear of 1-month duration. She had no history of ear discharge. This was her first episode of an ear disorder with no pre-existing ear disease. Her clinical examination revealed that the ear was full of wax and the external auditory canal (EAC) was obscured. The canal stenosis had been gradual and progressive. There were no significant findings in the nose or the throat. The hearing loss was of pure conductive nature. No cranial nerve abnormality was elicitable.
The patient was taken up for clearance of the EAC and examination under microscope. Her intraoperative findings showed a bony stenosis that had to be drilled out. As the stenotic segment was cleared, a soft tissue mass was detected with flakes and debris (Fig. 1). The mass was excised en sac and sent for histopathologic examination. The tympanic membrane was found to be normal. Tympanotomy revealed that the ossicles were intact and mobile.
The biopsy report was consistent with cholesteatoma for the excised soft tissue mass (Fig. 2). The bone specimen revealed necrosis without inflammatory reaction.
Discussion
External auditory canal cholesteatoma (EACC) is an extremely rare condition of the ear with an incidence
AbstrAct
External auditory canal cholesteatoma (EACC) is an extremely rare otologic disorder being seen in one out of a thousand ear patients. The pathogenesis of this rare disorder is still an enigma. Usually thought to be a geriatric disorder, we present here a case of a middle-aged woman with EACC. This case was unusual in several ways and was finally confirmed on histopathological examination. Our patient had a short history of hearing loss without ear discharge. Usual presentation of this nature is commoner in keratosis obturans where there is pain and hearing loss without otorrhea.
Key words: External auditory canal cholesteatoma, keratosis obturans, treatment options
*Dr Shroff’s Charity Eye Hospital Daryaganj, Delhi - 110 002
Figure 1. Soft tissue mass with flakes and debris.
Figure 2. Cholesteatoma.
cAsE rEPOrt
of less than 1 in 1,000 ear patients. It is usually a condition of the elderly and thought to be due to loss of lateral epithelial migration. Usually a chronic disorder, it is associated with otorrhea and a soft tissue mass in the EAC. Bony erosion of the EAC is the norm.

37Asian Journal of Ear, Nose & Throat, January-March 2011
cAsE rEPOrt
The pathogenesis of this rare disorder is still an enigma. It is proposed that poor blood supply may contribute to it in the elderly as well as the loss of epithelial migration outwards. The self-cleansing nature of the EAC being lost, the external canal gets filled with keratin debris and a soft tissue locally erosive mass that causes widening of the external canal.
Previously thought to be variants of the same disorder, EACC and keratosis obturans (KO) are now considered to be different disease entities by several scholars. Of significance is the fact that KO is usually bilateral and acute in presentation, is usually associated with pain. KO presents with painful loss of hearing with rarely a history of associated ear discharge. This is a condition of younger age group.
On the other hand, EACC is a disease of geriatric age group, usually indolent and chronic in nature and is marked by ear discharge. It is associated with hearing loss and rarely presents with pain.
It is unusual that our patient had acute presentation, no ear discharge, was a young patient and the histology was consistent with cholesteatoma. The clinical features clearly and unequivocally suggested KO while, histology confirmed EACC.
It is proposed that the distinction between the two entities be merged and the treatment be dictated by clinical picture rather than by nomenclatured diagnosis.
Suggested ReadingRoger G, Dupré M, Leboulanger N, Godey B, Thomas G, Gandemer V et al. Cholesteatoma secondary to temporal bone involvement by Langerhans cell histiocytosis: a complication amenable to curative surgery. Otol Neurotol 2009;30(2):190-3.Anthony PF, Anthony WP. The surgical treatment of external auditory canal cholesteatoma. Laryngoscope 1982;92(1):70-5.Zhao S, Han D, Wang D, Li J, Dai H, Yu Z. The formation of sinus in congenital stenosis of external auditory canal with cholesteatoma. Acta Otolaryngol 2008;128(8):866-70. Caughey RJ, Jahrsdoerfer RA, Kesser BW. Congenital cholesteatoma in a case of congenital aural atresia. Otol Neurotol 2006;27(7):934-6.Harris KC, Conley SF, Kerschne JE. Foreign body granuloma of the external auditory canal. Pediatrics 2004;113(4):e371-3.Heilbrun ME, Salzmana KL, Glastonburya. CM, Harnsberger HR, Kennedy RJ, Shelton C. External auditory canal cholesteatoma: Clinical and imaging spectrum. AJNR Am J Neuroradiol 2003;24(4):751-6.Martin DW, Selesnick SH, Parisier SC. External auditory canal cholesteatoma with erosion in to the mastoid. Otolaryngol Head Neck Surg 1999;121(3):298-300.Garin P, Jean-Christophe Degols M, Delos. External auditory canal cholesteatoma. Arch Otolaryngol Head Neck Surg 1997;123(1):62-5.Shire JR, Donegan JO. Cholesteatoma of the external auditory canal and keratosis obturans. Am J Otol 1986;7(5):361-4.
n n n
1.
2.
3.
4.
5.
6.
7.
8.
9.
xxxxxxxxxxx
38 Asian Journal of Ear, Nose & Throat, January-March 2011
Announcements, Conferences and Courses Information
10th International Tinnitus SeminarMarch 16-19, 2011Venue: Santa Catarina, BrazilE-mail: [email protected]: www.itsbrazil2011.com.br
Otology Update 2011: 14th Course on Ear and Temporal Bone SurgeryMarch 22-25, 2011Venue: Hannover, GermanyFax No.: +49 511 532 5558 E-mail: [email protected]: www.mhh-hno.de
8th International Course in Advanced Sinus Surgery TechniquesMarch 24-25, 2011Venue: Amsterdam, The NetherlandsContact: Wytske J Fokkens Tel. No.: +31 20 56 68586 Fax No.: +31 20 56 69573E-mail: [email protected]
British Cochlear Implant Group Annual Conference 201131st March to 1st April, 2011Venue: Nottingham, UKTel. No.: +44 (0) 115 9484459Fax No.: +44 (0) 115 9485560E-mail: [email protected]: www.nuh.nhs.uk/ncip
16th International Voice Workshop 2011April 8-9, 2011Venue: Paris, FranceContact: Jean AbitbolTel. No.: +33 1 46 47 91 89Fax No.: +33 1 45 27 72 30E-mail: [email protected]
17th Glasgow and Newcastle Course in ENT RadiologyFebruary 10-11, 2011Contact: Sadie SweenyTel. No.: +0141 211 0484E-mail: [email protected]
17th Annual Advances in Diagnosis and Treatment of Sleep Apnea and SnoringFebruary 18-20, 2011Venue: Disney’s Board Walk Inn Resort Orlando, USAContact: Cathy LaffertyTel. No.: +1 215 349 5382Fax No.: +1 215 662 4515E-mail: [email protected]: www.uphscepenn.edu/pennorl/ education/cme.ht
5th National Conference: Ear, Nose and Throat Hospital MedicineFebruary 24-25, 2011Venue: London, UKWebsite: www.mahealthcareevents.co.uk
7th Annual Conference of Association of Phonosurgeons of IndiaFebruary 25-27, 2011Venue: New Delhi, IndiaE-mail: [email protected] Website: www.phonocon2011.in
12th Asia-Oceania ORL-HNS ConferenceMarch 1-4, 2011Venue: Auckland, New ZealandFax No.: 64 9 360 1442E-mail: [email protected]: www.asia-oceania2011.org
British Paediatric Otolaryngology CourseMarch 3-4, 2011Venue: Glasgow, UKTel. No.: +44 (0) 141 569 7024Contact: Lorrain LeaskE-mail: [email protected]
ANNOUNcEMENts

xxxxxxxxxxx
3�Asian Journal of Ear, Nose & Throat, January-March 2011
EMEDINEws sEctION
From eMedinews
What Happens if Allergy of Nose is not Treated?
Nasal allergy leads to localized edema of the mucosa, which can block the opening of the sinus osteum thus leading to retained secretions in the sinuses which get secondarily infected thus causing sinusitis. Some cases of allergic rhinitis may progress to develop allergic nasal polyposis. Rhinitis and asthma are also closely linked i.e. about 75% of asthmatics have associated rhinitis. Patients of rhinitis who are asymptomatic for asthma have some inflammation of lower airway which can later on develop into asthma. Treatment of allergic rhinitis reduces the risk of asthma and lowers the dose of medication required to treat asthma.
What is the Treatment for Persistent Watering of the Eyes and What is the Role of ENT Surgeon in this?
Lacrimal pathway from the eyes drains into the nose. Epiphora or watering of the eyes can be due to blockage of lacrimal pathway thus not allowing outflow of tears from the eyes to nose. The blockage can present clinically as epiphora or repeated infection and swelling at the medial canthus of the eye. When the blockage is at the level of the lacrimal sac or nasolacrimal duct, dacryocystorhinostomy is done i.e. an opening of the lacrimal sac into the nose is made. Since, most of the pathway is anatomically-related to the nose, the surgery can very easily be done through nose by nasal endoscopic surgeon. The nasal endoscopic approach is a good alternative to the external approach as the results are better, there is no external scar and associated nasal pathology like deviated septum or sinusitis can be corrected in the same sitting.
—Dr Aru Handa MS, DNB (Dept. Co-ordinator and Senior Consultant Dept. of ENT Moolchand Medcity)
“OK, write this: “Fred dead.” “I’m sorry, Ma’am; I forgot to tell you there’s a five-word minimum.” “Hmmph,” came the reply, “You certainly did forget to tell me that.” A moment of silence. “Got your pencil and paper?”
“Yes, Ma’am.” “OK, print this: ‘Fred dead, Cadillac for sale.’”
Medicolegal UpdateWhat should be Experience of Training of Doctor for MTP?For the purpose of Clause (d) of Section 2, a registered medical practitioner shall have one or more of the following experience or training in gynecology and obstetrics, namely:
In the case of a medical practitioner who was registered in a state Medical Register immediately before the commencement of the act, experience in the practice of gynecology and obstetrics for a period of not less than three yearsIn the case of a medical practitioner, who was registered in a state Medical Register on or after the date of the commencement:
If he has completed six months of house surgency in gynecology and obstetrics Where he has not done any house surgency, if he had experience at a hospital for a period of not less than one year in the practice of in the case of a medical practitioner who was registered in a State Medical Register
If he has assisted a registered medical practitioner in the performance of 25 cases of medical termination of pregnancy in a hospital established or maintained, or a training institute provided for this purpose, by the government.In the case of a medical practitioner who was registered in a State Medical Register and who holds a Postgraduate Degree or Diploma in Gynecology and Obstetrics, the experience or training gained during the course of such degree or diploma.
—Dr Sudhir Gupta, Associate Professor Forensic Medicine & Toxicology, AIIMS
n
n
Laugh a While Story Begins
A local newspaper funeral notice telephone operator received a phone call. A woman on the other end asked, “How much do funeral notices cost?” “$5.00 per word, Ma’am,” came the response. “Good, do you have a paper and pencil handy?” “Yes, Ma’am.”
40 Asian Journal of Ear, Nose & Throat, January-March 2011
41Asian Journal of Ear, Nose & Throat, January-March 2011
Manuscripts should be prepared in accordance with the ‘Uniform requirements for manuscripts submitted to biomedical journals’ compiled by the International Committee of Medical Journal Editors (Ann. Intern. Med. 1992;96: 766-767).Asian Journal of Ear, Nose and Throat strongly disapproves of the submission of the same articles simultaneously to different journals for consideration as well as duplicate publication and will decline to accept fresh manuscripts submitted by authors who have done so.The boxed checklist will help authors in preparing their manuscript according to our requirements. Improperly prepared manuscripts may be returned to the author without review. The checklist should accompany each manuscript.Authors may provide on the checklist, the names and addresses of experts from Asia and from other parts of the World who, in the authors’ opinion, are best qualified to review the paper.
Covering letter
– The covering letter should explain if there is any deviation from the standard IMRAD format (Introduction, Methods, Results and Discussion) and should outline the importance of the paper.
– Principal/Senior author must sign the covering letter indicating full responsibility for the paper submitted, preferably with signatures of all the authors.
– Articles must be accompanied by a declaration by all authors stating that the article has not been published in any other Journal/Book. Authors should mentioned complete designation and departments, etc. on the manuscript.
Manuscript– Three complete sets of the manuscript should be
submitted and preferably with a CD; typed double spaced throughout (including references, tables and legends to figures).
– The manuscript should be arranged as follow: Covering letter, Checklist, Title page, Abstract, Keywords (for indexing, if required), Introduction, Methods, Results, Discussion, References, Tables, Legends to Figures and Figures.
– All pages should be numbered consecutively beginning with the title page.
Note: Please keep a copy of your manuscript as we are not responsible for its loss in the mail. Manuscripts will not be returned to authors.
Title pageShould contain the title, short title, names of all the authors (without degrees or diplomas), names and full location of the departments and institutions where the work was performed, name of the corresponding authors, acknowledgment of financial support and abbreviations used.– The title should be of no more than 80 characters and
should represent the major theme of the manuscript. A subtitle can be added if necessary.
– A short title of not more than 50 characters (including inter-word spaces) for use as a running head should be included.
– The name, telephone and fax numbers, e-mail and postal addresses of the author to whom communications are to be sent should be typed in the lower right corner of the title page.
– A list of abbreviations used in the paper should be included. In general, the use of abbreviations is discouraged unless they are essential for improving the readability of the text.
Summary– The summary of not more than 200 words. It must
convey the essential features of the paper.– It should not contain abbreviations, footnotes or
references.Introduction– The introduction should state why the study was carried
out and what were its specific aims/objectives.Methods– These should be described in sufficient detail to permit
evaluation and duplication of the work by others.– Ethical guidelines followed by the investigations should
be described.StatisticsThe following information should be given:– The statistical universe i.e., the population from which
the sample for the study is selected.– Method of selecting the sample (cases, subjects, etc.
from the statistical universe).– Method of allocating the subjects into different
groups.– Statistical methods used for presentation and analysis of
data i.e., in terms of mean and standard deviation values or percentages and statistical tests such as Student’s ‘t’ test, Chi-square test and analysis of variance or non-parametric tests and multivariate techniques.
– Confidence intervals for the measurements should be provided wherever appropriate.
Information for Authors
Asian Journal of
Ear, NoseThroatEar, NoseThroat
Review ARticle
42 Asian Journal of Ear, Nose & Throat, January-March 2011
Results– These should be concise and include only the tables
and figures necessary to enhance the understanding of the text.
Discussion
– This should consist of a review of the literature and relate the major findings of the article to other publications on the subject. The particular relevance of the results to healthcare in India should be stressed, e.g., practicality and cost.
ReferencesThese should conform to the Vancouver style. References should be numbered in the order in which they appear in the texts and these numbers should be inserted above the lines on each occasion the author is cited (Sinha12 confirmed other reports13,14...). References cited only in tables or in legends to figures should be numbered in the text of the particular table or illustration. Include among the references papers accepted but not yet published; designate the journal and add ‘in press’ (in parentheses). Information from manuscripts submitted but not yet accepted should be cited in the text as ‘unpublished observations’ (in parentheses). At the end of the article the full list of references should include the names of all authors if there are fewer than seven or if there are more, the first six followed by et al., the full title of the journal article or book chapters; the title of journals abbreviated according to the style of the Index Medicus and the first and final page numbers of the article or chapter. The authors should check that the references are accurate. If they are not this may result in the rejection of an otherwise adequate contribution.Examples of common forms of references are:
ArticlesPaintal AS. Impulses in vagal afferent fibres from specific pulmonary deflation receptors. The response of those receptors to phenylguanide, potato S-hydroxytryptamine and their role in respiratory and cardiovascular reflexes. Q. J. Expt. Physiol. 1955;40:89-111.BooksStansfield AG. Lymph Node Biopsy Interpretation Churchill Livingstone, New York 1985.Articles in BooksStrong MS. Recurrent respiratory papillomatosis. In: Scott Brown’s Otolaryngology. Paediatric Otolaryngology Evans JNG (Ed.), Butterworths, London 1987;6:466-470.
Tables– These should be typed double spaced on separate
sheets with the table number (in Roman Arabic numerals) and title above the table and explanatory notes below the table.
Legends– These should be typed double spaces on a separate
sheet and figure numbers (in Arabic numerals)
Please complete the following checklist and attach to the manuscript:1. Classification (e.g. original article, review, selected
summary, etc.)____________________________2. Total number of pages ______________________3. Number of tables __________________________4. Number of figures _________________________5. Special requests __________________________6. Suggestions for reviewers (name and postal
address) Indian 1. __________ Foreign 1. ___________ 2. __________ 2. ___________ 3. __________ 3. ___________ 4. __________ 4. ___________7. All authors’ signatures______________________8. Corresponding author’s name, current postal and
e-mail address and telephone and fax numbers _______________________________________
For Editorial Correspondence: Dr K.K. Aggarwal
Group Editor-in-Chief
Asian Journal of Ear, Nose and ThroatE-219, Greater Kailash, Part - 1, New Delhi - 110 048.
Tel: 40587513E-mail: [email protected] Website: www.ijcpgroup.com
Issue EditorDr VP Sood
Asian Journal of Ear, Nose and Throat
corresponding with the order in which the figures are presented in the text.
– The legend must include enough information to permit interpretation of the figure without reference to the text.
Figures– Two complete sets of glossy prints of high quality should
be submitted. The labelling must be clear and neat.– All photomicrographs should indicate the magnification
of the print.– Special features should be indicated by arrows or letters
which contrast with the background.– The back of each illustration should bear the first author’s
last name, figure number and an arrow indicating the top. This should be written lightly in pencil only. Please do not use a hard pencil, ball point or felt pen.
– Color illustrations will be accepted if they make a contribution to the understanding of the article.
– Do not use clips/staples on photographs and artwork.– Illustrations must be drawn neatly by an artist and
photographs must be sent on glossy paper. No captions should be written directly on the photographs or illustration. Legends to all photographs and illustrations should be typed on a separate sheet of paper. All illustrations and figures must be referred to in the text and abbreviated as “Fig.”.