health informatics and management informationjnujprdistance.com/assets/lms/lms jnu/mba/mba -...
TRANSCRIPT
Health Informatics and Management Information
This book is a part of the course by Jaipur National University, Jaipur.This book contains the course content for Health Informatics and Management Information.
JNU, JaipurFirst Edition 2013
The content in the book is copyright of JNU. All rights reserved.No part of the content may in any form or by any electronic, mechanical, photocopying, recording, or any other means be reproduced, stored in a retrieval system or be broadcast or transmitted without the prior permission of the publisher.
JNU makes reasonable endeavours to ensure content is current and accurate. JNU reserves the right to alter the content whenever the need arises, and to vary it at any time without prior notice.

I/JNU OLE
Index
ContentI. ..................................................................... II
List of FiguresII. .........................................................VI
List of TablesIII. ........................................................ VII
AbbreviationsIV. .....................................................VIII
Case StudyV. ............................................................. 105
BibliographyVI. ........................................................ 115
VII. Self Assessment AnswersVII. ........................... 118
Book at a Glance
II/JNU OLE
Contents
Chapter I ...................................................................................................................................................... 1Health Informatics ....................................................................................................................................... 1Aim ................................................................................................................................................................ 1Objectives ...................................................................................................................................................... 1Learning outcome .......................................................................................................................................... 11.1 Introduction .............................................................................................................................................. 21.2 Medical/Health Informatics ..................................................................................................................... 21.3 Importance and Significance of Health Informatics ................................................................................ 21.4 Core Competencies of Health/Medical/Biomedical Informatics ............................................................. 31.5 Functions of Health Informatics .............................................................................................................. 5 1.5.1 Health Informatics and the Skills Needed for Health Informatics Managers .......................... 6 1.5.2 Need and Demand for Health Informatics ............................................................................... 6 1.5.3 Some Pertinent Areas that Require the Need for Health Informatics Professionals ................ 71.6 Applications of Health Informatics .......................................................................................................... 71.7 Objectives of Health Informatics ............................................................................................................. 8 1.7.1 Considerations ......................................................................................................................... 81.8 Health Informatics Theories .................................................................................................................... 8 1.8.1 Theories.................................................................................................................................... 8 1.8.2 Value ........................................................................................................................................ 8 1.8.3 Implementation ........................................................................................................................ 81.9 The Advantages of a Health Informatics.................................................................................................. 8 1.9.1 Disadvantages of Health Informatics ..................................................................................... 101.10 Outlook ................................................................................................................................................ 10 1.10.1 Career Options ..................................................................................................................... 10Summary .....................................................................................................................................................11References ................................................................................................................................................... 12Recommended Reading ............................................................................................................................. 12Self Assessment .......................................................................................................................................... 13
Chapter II .................................................................................................................................................. 15Health Informatics and Information Management ................................................................................ 15Aim .............................................................................................................................................................. 15Objectives .................................................................................................................................................... 15Learning outcome ........................................................................................................................................ 152.1 Introduction ............................................................................................................................................ 162.2 History of Computing ............................................................................................................................ 162.3 Computers: The Electronic Computer ................................................................................................... 16 2.3.1 Microcomputers Arrive ......................................................................................................... 172.4 Computer Languages - Telling the Computer What to Do? ................................................................. 182.5 Health Informatics - A Discipline ......................................................................................................... 182.6 History of Health Informatics ................................................................................................................ 19 2.6.1 Technological Advances ........................................................................................................ 192.7 Health Informatics and Health Information Management ..................................................................... 20 2.7.1 Heath Care Information Technology (HIT) ........................................................................... 202.8 Difference between Health Informatics and Health Information Management ..................................... 21Summary ..................................................................................................................................................... 23References ................................................................................................................................................... 23Recommended Reading ............................................................................................................................. 24Self Assessment .......................................................................................................................................... 25

III/JNU OLE
Chapter III ................................................................................................................................................. 27Health Care Systems, Information Systems and Health Information Science ..................................... 27Aim .............................................................................................................................................................. 27Objectives .................................................................................................................................................... 27Learning outcome ........................................................................................................................................ 273.1 Introduction ............................................................................................................................................ 283.2 Economic and Political Influences ........................................................................................................ 293.3 Philosophical Aspects ........................................................................................................................... 313.4 Technological Advances ....................................................................................................................... 313.5 Health Information Science .................................................................................................................. 313.6 The Communication of Medical Information and its Management ...................................................... 32 3.6.1 Communication with Literature ............................................................................................ 32 3.6.2 Communication between Providers ...................................................................................... 33 3.6.3 Communication with Organisations ..................................................................................... 33 3.6.4 Communication between Provider and Patient ..................................................................... 333.7 Healthcare Terminologies ...................................................................................................................... 34 3.7.1 Components of a Terminology .............................................................................................. 34 3.7.2 Classifications, Hierarchies and Terminologies .................................................................... 353.8 Resources .............................................................................................................................................. 383.9 Computing ............................................................................................................................................. 39 3.9.1 User Interface and Data Capture ........................................................................................... 393.10 Electronic Communications ................................................................................................................ 403.11 Safeguards ........................................................................................................................................... 41Summary ..................................................................................................................................................... 42References ................................................................................................................................................... 42Recommended Reading ............................................................................................................................. 43Self Assessment ........................................................................................................................................... 44
Chapter IV ................................................................................................................................................. 46Standards in Health Informatics .............................................................................................................. 46Aim .............................................................................................................................................................. 46Objectives .................................................................................................................................................... 46Learning outcome ........................................................................................................................................ 464.1 Introduction ............................................................................................................................................ 474.2 What are Standards?............................................................................................................................... 474.3 Who Develops Standards? ..................................................................................................................... 474.4 Which Standards should be Developed? ................................................................................................ 484.5 Adoption of Standards ............................................................................................................................ 484.6 Health Informatics Standards and Information Transfer: Exploring the HIM Role .............................. 49 4.6.1 Framework for Developing Standards ................................................................................... 49 4.6.2 Standards Organisations......................................................................................................... 49 4.6.3 Mandatory Standards ............................................................................................................. 50 4.6.4 Voluntary Standards ............................................................................................................... 504.7 Information Transfer and Selected Standards Development Organisations .......................................... 514.8 Practical Actions for HIM Professionals ................................................................................................ 51Summary ..................................................................................................................................................... 53References ................................................................................................................................................... 53Recommended Reading ............................................................................................................................. 54Self Assessment ........................................................................................................................................... 55
IV/JNU OLE
Chapter V .................................................................................................................................................... 57Basic Applications and Expectations ........................................................................................................ 57Aim .............................................................................................................................................................. 57Objectives .................................................................................................................................................... 57Learning outcome ........................................................................................................................................ 575.1 Introduction ............................................................................................................................................ 585.2 Communicating with the Computer ....................................................................................................... 585.3 The Keyboard ......................................................................................................................................... 585.4 The Mouse and the Graphical User Interface (GUI).............................................................................. 595.5 Typing .................................................................................................................................................... 605.6 Voice Recognition and Notepads ........................................................................................................... 605.7 Specific Applications ............................................................................................................................. 61 5.7.1 Word Processing .................................................................................................................... 61 5.7.2 Spreadsheets ........................................................................................................................... 62 5.7.3 Database Applications ............................................................................................................ 62 5.7.4 Presentation Software ............................................................................................................ 64 5.7.5 Financial Tools ....................................................................................................................... 65Summary ..................................................................................................................................................... 66References ................................................................................................................................................... 66Recommended Reading ............................................................................................................................. 66Self Assessment ........................................................................................................................................... 67
Chapter VI ................................................................................................................................................. 69Electronic Medical Records ...................................................................................................................... 69Aim .............................................................................................................................................................. 69Objectives .................................................................................................................................................... 69Learning outcome ........................................................................................................................................ 696.1 Introduction ............................................................................................................................................ 706.2 Traditional Medical Record Systems .................................................................................................... 706.3 Technology and Health Care Delivery .................................................................................................. 706.4 Consequences of Using Manual-Based Record Systems ...................................................................... 706.5 Concept of Electronic Medical Record (EMR) .................................................................................... 716.6 The Institute of Medicine Study into Electronification of the Patient Care Record .............................. 716.7 Software Applications Providing Decision Support in EMRs ............................................................... 726.8 Computerised Clinical Decision Support Tools ..................................................................................... 746.9 Existing EMR Models and Confirmed Benefits of EMRs .................................................................... 766.10 Patient Care ......................................................................................................................................... 776.11 Quality Assurance ............................................................................................................................... 776.12 Research .............................................................................................................................................. 776.13 Epidemiology ...................................................................................................................................... 776.14 Administration ..................................................................................................................................... 78Summary .................................................................................................................................................... 79References ................................................................................................................................................... 79Recommended Reading ............................................................................................................................. 79Self Assessment .......................................................................................................................................... 80
Chapter VII ................................................................................................................................................ 82National Strategy for Information Management .................................................................................... 82Aim .............................................................................................................................................................. 82Objectives .................................................................................................................................................... 82Learning outcome ........................................................................................................................................ 827.1 Introduction ............................................................................................................................................ 837.2 The Information Intensive Health Services ........................................................................................... 847.3 Why a Strategy? .................................................................................................................................... 857.4 Elements of an Education and Training Strategy .................................................................................. 85

V/JNU OLE
7.5 Preparing Staff for Information Technology .......................................................................................... 86 7.5.1 Staff Education ...................................................................................................................... 86 7.5.2 Change .................................................................................................................................. 86 7.5.3 Attitudes ................................................................................................................................ 87 7.5.4 Organisational Culture .......................................................................................................... 877.6 Fact Finding Tools ................................................................................................................................ 877.7 Business Process Re-engineering ......................................................................................................... 887.8 Project Management ............................................................................................................................. 897.9 Hardware Installation ............................................................................................................................ 90Summary ..................................................................................................................................................... 91References ................................................................................................................................................... 91Recommended Reading ............................................................................................................................. 92Self Assessment .......................................................................................................................................... 93
Chapter VIII ............................................................................................................................................... 95Health Informatics in General Practice ................................................................................................... 95Aim .............................................................................................................................................................. 95Objectives .................................................................................................................................................... 95Learning outcome ........................................................................................................................................ 958.1 Introduction ............................................................................................................................................ 968.2 Relationship to other Health Workers ................................................................................................... 968.3 Variability of Primary Care Practice Style ............................................................................................ 968.4 Practice Management ............................................................................................................................ 97 8.4.1 Patient Billing ....................................................................................................................... 97 8.4.2 Appointments ........................................................................................................................ 97 8.4.3 Practice Administration .......................................................................................................... 97 8.4.4 Electronic Tools .................................................................................................................... 988.5 Clinical Records .................................................................................................................................... 998.6 Benefits of Computerising the Medical Record .................................................................................... 998.7 Real Time Information Access .............................................................................................................. 998.8 Research by Practice Audit ................................................................................................................. 1008.9 Formal Research Projects ................................................................................................................... 1018.10 Medical Education ............................................................................................................................ 1018.11 Telecommunications ......................................................................................................................... 101Summary ................................................................................................................................................... 102References ................................................................................................................................................. 102Recommended Reading .......................................................................................................................... 102Self Assessment ......................................................................................................................................... 103

VI/JNU OLE
List of Figures
Fig. 6.1 User defined flow chart of clinical data .......................................................................................... 73Fig. 6.2 Daily plot of white blood cells and platelets with chemotherapy ................................................... 76
VII/JNU OLE
List of Tables
Table 2.1 Concepts of health information management and health informatics .......................................... 21Table 2.2 Difference between health informatics and health information management ............................. 22
VIII/JNU OLE
Abbreviations
A&E - Accident & Emergency AAC - AustralianAmbulatoryClassificationACHS - Australian Council on Healthcare StandardsACTA - Automatic Computerised Transverse Axial AHCPR - Agency for Health Care Policy and Research AHMAC - Australian Health Ministers Advisory Council AIH&W - Australian Institute of Health and Welfare AIM - Advanced Informatics in Medicine AMIA - American Medical Informatics Association ANSI - American National Standards Institute APAC - AustralianPaediatricAmbulatoryClassificationARAMIS - American Rheumatologic Association Medical Information System ASC - Accredited Standards Committee ASTM - American Standards for Testing and MaterialsBIH - Beth Israel Hospital CDSS - Clinical Decision Support Systems CEN - European Standardisation Committee CEP - Care Evaluation ProgramCI - Clinical IndicatorCINAHL - Cumulative Index to Nursing and Allied Health Literature CMG - Canada uses Case-Mix GroupsCOSTAR - Computer Stored Ambulatory Record CPRI - Computer Based Patient Record Institute CT - Computed Tomography DICOM - Digital Imaging and Communications in MedicineDRG - Diagnostic Related Group EDI - Electronic Data InterchangeESPRIT - European Strategic Program for Research and Development in Information Technologies GUI - The Graphical User InterfaceHCN - Health Communication Network American HELP - Health Evaluation through Logical ProcessingHI - Health Informatics HIM - Health Information Management HIPAA - Health Insurance Portability and Accountability ActHISPP - Healthcare Informatics Standards Planning Panel HIT - Heath Care Information Technology HL-7 - Health Level-7HRG - Healthcare Resource GroupsICD - InternationalClassificationofDiseasesICPC - InternationalClassificationofPrimaryCareIEC - International Electro-technical CommissionIEEE - Institute of Electrical and Electronics Engineers IM&T - Information Management and TechnologyIMIA - International Medical Informatics Association IMS - Information Management Service INCIDE - Inaugural National Clinical Indicator Data Evaluation SystemISO - International Standards Organisation IT - Information TechnologyJHOC - Johns Hopkins Oncology Centre LAN - Local Area Networks LCSH - Library of Congress Subject Headings

IX/JNU OLE
MADC - Major Ambulatory Diagnostic Categories MDC - Major Diagnostic Categories MEDTEP - Medical Treatment Effectiveness Program MeSH - Medical Subject HeadingsMIB - Medical Information BusNCPDP - National Council on Prescription Drug Programs NCQA - National Committee for Quality Assurance NHS - National Health Service NHT - Nursing Home Type NLM - National Library of Medicine OCIS - Oncology Centre Information System OECD - Organisation for Economic Co-operation and Development OSI - Open Systems Interconnection standardsPAIS - Patient Assessment and Information SystemPERT - Program Evaluation and Review TechniquePM-DRG - PaediatricModifiedDRGPOMR - Problem Orientated Medical RecordPPC - Psychiatric Patient Classes RCI - ResidentClassificationInstrumentRMRS - Regenstrief Medical Record SystemSDO - Standards Development Organisations SNOMED - Systematised Nomenclature of Medicine STOR - Summary Time-Orientated Record TEFRA - Tax Equity and Fiscal Responsibility Act TRAM - Tasmanian Resource Allocation Model TURP - Transurethral Resections of the Prostate UMLS - UnifiedMedicalLanguageSystemURG - Urgency Related Groups WAN - Wide Area Networks WYSIWYG - What You See Is What You Get
1/JNU OLE
Chapter I
Health Informatics
Aim
The aim of this chapter is to:
explain concept of health informatics•
elucidate the importance of health informatics •
explicate core competencies of health informatics•
Objectives
The objectives of this chapter are to:
describe functions of health informatics •
elucidate need and demand for health informatics •
explicate the applications of health informatics•
Learning outcome
At the end of this chapter, you will be able to:
understand the advantages and disadvantages of health informatics •
describe the objectives behind the purpose of introducing health informatics•
identify the challenges of introducing health informatics•
Health Informatics and Management Information
2/JNU OLE
1.1 IntroductionHealth/MedicalInformaticsisoneofthefastestgrowingareasinbothacademicandprofessionalfields.Professionally,the large gap between the state of the art in computer technologies and the current state of affairs in Health IT has generated great demand in the job market for information and health professionals who can effectively design, develop, and use technologies such as Electronic Medical Records, patient monitoring systems, and digital libraries, and who can manage the vast quantity of information generated by these systems. Academically, this area poses some of the most interesting and challenging questions at the core of health and information sciences, ranging from datamanagement,cognitivesupport,andclassificationtopatientempowerment,privacy,andethics.
1.2 Medical/Health InformaticsInformationisanetherealcommodity.Onedefinitiondescribesitasthedataandknowledgethatintelligentsystems(humanandartificial)usetosupporttheirdecisions.Healthinformaticshelpsdoctorswiththeirdecisionsandactions,andimprovespatientoutcomesbymakingbetteruseofinformation—makingmoreefficientthewaypatientdataand medical knowledge is captured, processed, communicated, and applied. These challenges have become more important since the internet made access to medical information easier for patients.
HealthorMedicalInformaticsisthe“scientificfieldthatdealswithbiomedicalinformation,data,andknowledge- their storage, retrieval, and optimal use for problem solving and decision making. It accordingly touches on all basicandappliedfieldsinbiomedicalscienceandiscloselytiedtomoderninformationtechnologies,notablyinthe areas of computing and communication (medical computer science)”.
Medical information science is the science of using system-analytic tools to develop procedures (algorithms) for management,processcontrol,decisionmakingandscientificanalysisofmedicalknowledge.
Medical Informatics comprises the theoretical and practical aspects of information processing and communication, based on knowledge and experience derived from processes in medicine and health care.
Information management constitutes a major activity of the health care professional. Currently a number of forces are together focusing attention on this function.Medical informatics is thefield that concerns itselfwith thecognitive, information processing, and communication tasks of medical practice, education, and research, including theinformationscienceandthetechnologytosupportthesetasks.Itisanintrinsicallyinterdisciplinaryfield,witha highly applied focus, but it also addresses a number of fundamental research problems as well as planning and policy issues.
After many years of development of information systems to support the infrastructure of medicine, a new generation of systems and tools are aimed at physicians and other health care managers and professionals - to support education, decision making, communication, and may other aspects of professional activity. Health care institutions are beginning to make large-scale commitments to information systems and to services that will affect every aspect of their organisation’s function. Academic units of medical informatics are being established at a number of medical schools, medical informatics professionals are being sought to serve on faculties and hospital staffs, and medical informatics is emerging as a distinct academic entity. “
Therationalstudyofthewaywethinkaboutpatients,andthewaythattreatmentsaredefined,selectedandevolved.It is the study of how medical knowledge is created, shaped, shared and applied.
1.3 Importance and Significance of Health InformaticsHealthinformaticscombinesthefieldsofmedicine,informationscienceandinformationtechnologytoformulatevarious systems for generating, validating, securing and integrating health-related data. The purpose is to deliver effective health care to patients. It involves bringing together various resources, techniques and systems to maximise the use of the wealth of medical knowledge, technological advances and drug breakthroughs that are available. It isusedinawidevarietyofhealth-relatedfields,includingdentistry,pharmacy,nursing,medicalresearchclinicalcare and public health.
3/JNU OLE
Health informatics is sometimes called medical informatics. It encompasses the use of dedicated software, hardware devices and sophisticated computer networks with the capacity to gather, evaluate and transmit medical information. The items that are necessary for constructing such a system include information technology, clinical directives, medical jargon and data storage. Medical informatics can be applied in various health settings, including rehabilitation centres, hospital care, and general practice and primary care facilities.
1.4 Core Competencies of Health/Medical/Biomedical InformaticsHealth/Medical/BiomedicalInformaticsistheinterdisciplinary,scientificfieldthatstudiesandpursuestheeffectiveusesofbiomedicaldata,information,andknowledgeforscientificinquiry,problemsolvinganddecisionmaking,motivated by efforts to improve human health.
Acquire professional perspective: Summarise and explain the history and values of the discipline and its •relationshiptorelatedfieldswhiledemonstratinganabilitytoread,interpret,andcritiquethecoreliterature.Analyseproblems:Analyse,understand,abstract,andmodelaspecificbiomedicalproblemintermsofdata,•information and knowledge components.Produce solutions: Use the problem analysis to identify and understand the space of possible solutions and •generate designs that capture essential aspects of solutions and their components.Articulatetherationale:Defendthespecificsolutionanditsadvantageovercompetingoptions.•Implement,evaluate,andrefine:Demonstrateanability tocarryout thesolution, toassess itsvalidity,and•iteratively improve its design.Innovate: Create new theories, typologies, frameworks, representations, methods, and processes to address •biomedical and informatics problems.Work collaboratively: Demonstrate the ability to team effectively with partners from diverse disciplines.•Disseminate and discuss: Communicate effectively to audiences in multiple disciplines in persuasive written •and oral form.
HI develops, studies and applies theories, methods and processes for the generation, storage, retrieval, use, and sharing of biomedical data, information, and knowledge.
All involve the ability to reason and relate to health information, concepts, and models spanning molecules to populations:
Theories: Understand and apply syntactic, semantic, cognitive, social, and pragmatic theories as they are used •in biomedical informatics.Typology: Explain and analyse the types and nature of biomedical data, information, and knowledge.•Frameworks: Describe and apply the common conceptual frameworks that are used in biomedical •informatics.
A framework is a modelling approach, programming approach, representational scheme, or an architectural �design.
Representation: Understand and apply representations and models that are applicable to biomedical data, •information, and knowledge.
A representation is a method of using data structures or semantic elements in a computational �environment.
Methods and processes: Recognise and apply the methods and processes used in different contexts of biomedical •informatics.

Health Informatics and Management Information
4/JNU OLE
HI builds on computing, communication and information sciences and technologies and their application in biomedicine.
Prerequisite knowledge and skills: Assumes basic familiarity with data structures, algorithms, programming, •mathematics, and statistics.Fundamentalknowledge:Understandandgainexperienceapplyingthefundamentalsofthefieldinthecontext•of biomedical problems. For example:
Imaging and signal analysis �Information documentation, storage, and retrieval �Machine learning, including data mining �Networking, security, databases �NLP, semantic technologies �Representation of logical and probabilistic knowledge and reasoning �Simulation and modelling �Software engineering �
Procedural knowledge and skills: For substantive problems, understand and apply methods of inquiry and criteria •for selecting and utilising algorithms, techniques, and methods.
Describe what is known about the application of the fundamentals within biomedicine. �Identifytherelevantexistingapproachesforaspecificbiomedicalproblem. �Apply,adapt,andvalidateanexistingapproachtoaspecificbiomedicalproblem. �
HI investigates and supports reasoning, modelling, simulation, experimentation, and translation across the spectrum from molecules to populations, dealing with a variety of biological systems, bridging basic and clinical research and practice, and the healthcare enterprise.
Prerequisite knowledge and skills: Basic familiarity with biological, biomedical, and population health concepts •and problems including common research problems.Fundamentalknowledge:Understandthefundamentalsofthefieldinthecontextoftheeffectiveuseofbiomedical•data, information, and knowledge. For example:
Biology: Molecule, sequence, protein, structure, function, cell, tissue, organ, organism, phenotype, �populations.Translational and clinical research: Genotype, phenotype, pathways, mechanisms, epigenetic, sample, �protocol, study, subject, evidence, evaluation.Healthcare: Screening, diagnosis (diagnoses, test results), prognosis, treatment (medications, procedures), �prevention, billing, patient, consumer, provider, families, healthcare teams, quality assurance, safety, error reduction, comparative effectiveness, medical records, personal health records, information security and privacy.Population health:Detection, prevention, screening, education, stratification, spatiotemporal patterns, �ecologies of health, populations.
Proceduralknowledgeandskills:Forsubstantiveproblemsrelatedtoscientificinquiry,problemsolving,and•decision making, analyse and critically evaluate solutions based on biomedical informatics approaches.
Frame complex biomedical informatics problems in terms of data, information, and knowledge. �Analyse, select, apply, and evaluate biomedical informatics methods. �Relate such knowledge to other problems within and across levels of the biomedical spectrum. �

5/JNU OLE
HI recognising that people are the ultimate users of biomedical information, draws upon the social and behavioural sciences to inform the design and evaluation of technical solutions and the evolution of complex economic, ethical, social, educational, and organisational systems.
Prerequisite knowledge and skills: Familiarity with fundamentals of social, organisational, cognitive, and •decision sciencesFundamental knowledge:•
Design: human centred design, usability, human factors, cognitive and ergonomic engineering �Evaluation: controlled trials, observational studies, hypothesis testing, ethnographicmethods, field �observational methodsSocial, behavioural and organisational sciences: Computer Support for Collaborative Work, Social Networks, �change managementEthical, Legal, Social Issues: Human subjects, HIPAA, informed consent, secondary use of data, �confidentiality,privacyEconomic, social and organisational context of biomedical research, pharmaceutical industry, medical �instrumentation, healthcare, and public health
Procedural knowledge and skills: Develop systems approaches to the solution of substantive problems in •biomedical informatics:
Frame complex biomedical informatics problems in terms of people, organisations, and socio-technical �systemsUnderstand the challenges and limitations of technological solutions �Design, implement, and validate the biomedical informatics applications and interventions �Evaluate the impact of biomedical informatics applications and interventions in terms of people, organisations, �and socio-technical systemsRelate solutions to other problems within and across levels of the biomedical spectrum �
1.5 Functions of Health InformaticsTherearebasicallythreeareasinthehealthinformaticsfieldwheretheuseofinformationsystemsmaybeusedtocreatemoreoperatingefficienciesandeffectiveness:clinical,administrativeandmedicalinformation.Forexample,there is a tremendous emphasis on implementation of uniformed system for electronic medical records. Not only will it help cut health care cost, but also improve the overall quality of care to clients. In addition, it also has an impact on scheduling, billing, clinical research and the sharing of medical information.
Ahealthinformaticsmanagertakesonamyriadoftasksandfunctionsthatprovebeneficialtocarryoutthejobwith utmost responsibility. Like any other major position in any given career, it should be exercised with discipline, concern and thorough knowledge and skills. However, to further delve into the skill sets and functions of a health informaticsmanageritisbesttoknow,exploreandfamiliariseoneselfwithhealthinformatics,firstandforemost.
An Informatics person is a member of information technology. So many people try to say “oh, I am just a nurse”, or some other drivel as to why they are clinical but have no technical background. If you have no technical background, thenyouareaclinicalprovider,NOTaHealthInformaticist.Technologyimmatureorganisationsrarelycanfigureout the difference.
Health Informatics is also popularly known as health care informatics or medical informatics that combines the inputs of computer science, information science and health care. It caters to the resources, devices and methods needed to optimise acquisition, storage, retrieval and information usage in biomedicine and health care.
Health Informatics and Management Information
6/JNU OLE
Some of the widely known health informatics tools include:Computers & Technical Computing Knowledge•Clinical guidelines•Formal medical terminologies•Information and communication systems•
Applicationsofhealthinformaticsareevidentinthefollowingfields:Nursing•Clinical care•Dentistry•Pharmacy•Public health•Occupational therapy•Biomedical research•
1.5.1 Health Informatics and the Skills Needed for Health Informatics ManagersTheongoingneedfortheapplicationofhealthinformaticshascreatedalotofcareeropportunitiesinthisfield.One such career opportunity is that of the health informatics manager. The job entails high-end dedication and commitmentthereforeitinvolvesaselectcropofhighlyqualifiedindividualswhocanhandlethetaskswithutmostindependence.
Justsomeoftheskillsneededtobecomeaqualifiedhealthinformaticsmanager,amongothers,include:Complete (or as complete as possible) understanding of the health care industry•Communication skills•Strategic planning and management skills and leadership•Information Technology (and not just a ‘hey, I like computers’ attitude)•Information Analysis and Organisation•Health care professional training•Knowledge of system infrastructure design and networking•Programming skills•
Just like all the rest of other career paths available with health informatics, being a health informatics manager requires a lot of dedication and drive. Being a management position, a health informatics manager should possess the skills ofaleaderandarisktakerwhoisnotafraidtotakeonchallengesandsacrificesifasituationcallsforsuch.
1.5.2 Need and Demand for Health InformaticsWe are all witness to the medical advances and discoveries in health care and medicine. Along with this is the demand for medical and health technologies to augment the demand for more up to date services. Despite the delay in the adoption of health care technologies there is a continuing push to adopt innovations and this has been highly initiated by governments from developed countries all around the world.
The US Government for instance, way back in 2003 and 2004 highly recommended the adoption of technological advances in health care to reduce medical errors and also to make the health care technology standard popularly known as SNOMED CD to be widely available in the United States.
The British Government has followed suit by allocating a budget mainly towards the improvement of delivery of medical and health care services. The same scenario has been observed in Australia and Canada. Owing to this, thereisasimilarriseanddemandforqualifiedandknowledgeableprofessionalsinthefieldofhealthinformaticswho have complete grasp and understanding both of health care and information technology.

7/JNU OLE
1.5.3 Some Pertinent Areas that Require the Need for Health Informatics ProfessionalsWhilehealthinformaticscatersmainlytothemedicalfielditisnotentirelylimitedtoclinicalsettings.Afterall,itisabroadfieldthatalsoincludeselectronicmedicalrecords,digitalimagingsystemsanddigitallibraries,telemedicineas well as health policy and decision making. Therefore, health informatics professionals are likewise highly in demand in a wide array of areas.
A few of the opportunities that health informatics professionals can avail of are in areas such as the following:Pharmaceutical companies – Health informatics professionals are needed in these companies to aid in the analysis •of information gathered regarding drug use and prescription pattern reports.Hospitals and health care providers – Health informatics professionals are needed in the implementation and •management of electronic medical records systems in such institutions. Such professionals are also helpful in the analysis of systems information making it available through knowledge management skills.Public health organisations – Professionals in health informatics are highly in demand in these organisations •forthecollectionandanalysisofpopulationandcommunityinformation.Thisisbeneficialinthefunctionofthese organisations which is to carry out the design and implementation of surveillance and disease reporting systems.Insurance companies – The work of health informatics professionals involves the analysis of health records •and insurance claims.
1.6 Applications of Health InformaticsThere are many reasons for the continued growth and development of the health informatics profession. It has multiple application possibilities in delivering better and less expensive health care. Doctors can take advantage of a constantly expanding knowledge base that enables them to make better use of the latest information when making medical decisions.
This ability is further improved with the assistance of technology such as clinical decision support systems (CDSS), or electronic prescribing system, which abolishes the need for physicians to write prescriptions. It can also facilitate data mining, which provides information regarding thing like the effective of certain prescribe drugs. It may also help eliminate many prescription mistakes and lower the cost of treatments.
Public health Public health informatics focuses on how technology can help prevent injury and disease. This includes systems that track and broadcast information about disease prevention.
Clinical applicationsClinical informatics deals with how information is used, analysed and managed in clinical settings. This area of medical informatics includes work with electronic records of patients’ care, medical imaging equipment (such as x-ray and ultrasound machines), and computer programs that manage the clinical information at hospitals.
NursingNursing informatics deals with how nurses collect and manage their data-including observations that they make about patients’ and their diagnoses, and plans that nurses use for patient care.
Veterinary medicineVeterinary informatics is concerned with the use of technology to support the research and practice of veterinary medicine. It includes helping veterinarians with the use of electronic patient records, and systems that help track diseases and parasites.
DentistryHealthinformaticsinthedentalfieldisconcernedwithenhancingtheresearchandpracticesoftheprofession.Thisincludes how patient records are stored electronically, billing systems and medical databases.
Health Informatics and Management Information
8/JNU OLE
1.7 Objectives of Health InformaticsOneofthemajorpushinthefieldofhealthinformaticsistocreateastandardglobalprocesstohealthcare.Thiswouldbe accomplishedbybringing together providers, researchers andpatients to reap the benefits of healthinformatics. They will take advantage of cutting-edge methods, principles and rules to alter the way health care is currentlydelivered.Anotherpurpose is to encourage theuseof thebest practices in themedicalfield.
1.7.1 ConsiderationsOneofthemainchallengesinthehealthinformaticsfieldisthetaskofgettingmosthealthcareproviderstoimplementthe various aspects of information technology into their day-to-day practices. Widespread implementation of health informatics could create a seamless and more complete health care system. It also provides assistance to providers in the area of problem solving, decision making, and customer service and job performance. Health informatics also plays a prominent role in health law. The automation of personal medical data has legal implications related to operations and privacy.
1.8 Health Informatics Theories TheNationalLaboratoryofMedicinedefineshealthinformaticsas“theinterdisciplinarystudyofthedesign,development,adoption and application of IT-based innovations in health care services, delivery, management and planning.” Innovation iskeytothisdefinitionbecausethegoalistoinnovate,notjusttouseinformationtechnologytotrackandfindinformation.
1.8.1 TheoriesThe theories and concepts behind health informatics are threefold. It involves creating a common information management infrastructure where the medical records of anyone is electronically available to any authorised medical professional or practitioner regardless of geographical location. Second, it links medical research and clinical research databasesintothisinformationmanagementstructure.Finally,itappliesscientificandanalyticaltoolstoallthisdata with the objective of creating new decision making tools, value and innovations.
1.8.2 ValueHealth informatics theories, research and processes produces valuable new generations of systems and tools for health care professionals to aid them in their day-to-day practice as well as providing new educational, research and management value. This value can only increase as more and more data is accessible via the system.
1.8.3 ImplementationHealth care institutions are making commitments to the concept and promise of health informatics. This is evident by the fact that health care institutions are committing funding toward implementing new information systems to support and feed the health informatics infrastructure.
1.9 The Advantages of a Health InformaticsHealthinformaticsisafieldthatinvolvescollecting,analysingandtransmittingmedicalinformationtomakethedeliveryofhealthcaremoreefficientfiscally,administrativelyandclinically.Healthinformaticsprofessionalsaddressthe security and privacy concerns of electronic records and work to reduce health care disparities among various demographicgroups.Adegreeinhealthinformaticsoffersmultiplebenefitsforindividualswhowanttoenterthegrowinghealthcarefieldandwhoenjoyworkingwithcomputers.
Today’s modern medicine requires doctors to be constantly aware of new developments, new medications, and newprocedures.Withtheinfluxofpatientsintothemedicalsystem,itismoreessentialthaneverthatthehealthcare industry keep up. Health informatics is the combination of informational science, health care and computer technology. In the 1950s, health care experts realised the need to integrate health records of patients along with the use of computers. Originally, this process was called medical computing. By the 1970s, health informatics had takenoverthemedicalworldbystorm.Doctors’offices,hospitals,andsmallclinicswereallusingpatientrecordkeeping via computer to help better track treatment and patient progress.
9/JNU OLE
Therearemanybenefitstousinghealthinformatics.Throughtheuseofcomputers,theInternetandvariousmedicaldatabases, doctors can better learn how to treat patients more effectively. The data retrieved by the use of heath informatics provides statistical information that can have a profound effect on how medicine is distributed, surgeries is performed and how healing is tracked. It also helps hospitals better track patients’ past records so they can be treated faster in the future. The use of health informatics has opened up the doors for clinics to be more capable oftreatingpatientsinamoreefficientmanner,andhelpstheseclinicsrefinetheircurrentprocesstomakeitmorestreamlined.
Medical software and record keeping programs are constantly being upgraded, and new programs are provided to help keep more accurate and detailed records of patients. This can also help to speed up the check-in process for patients whentheyarriveatahospitalordoctor’soffice.Handheldportabledevicesarenowalsobeingusedsothatnursesand doctors can easily move throughout a large hospital or clinic, while still being able to access information at the touchofabutton.Healthinformaticsarealsousedatdentistofficessooralsurgeonsanddentistscancoordinatepatient treatment. This integration has provided medical professionals with an easy to use, fast method of accessing patient’s past medical history.
New technology can be an integral part of medicine, and health informatics is no exception. Through detailed patient medical records, clinics and hospitals have access to much more information, and can retrieve this information quicker than ever before. The development and combination of computer and medical science has opened the doors for medical specialists, and given patients a better chance at getting the best treatment possible.
Theadvantagesofusinghealth informatics include improvements to theefficientdelivery, cost andqualityofhealthcare.Amultidisciplinaryfield,health informaticsencompasses informationscience, informationsystems,technology and healthcare. Health informatics analysts, or health informaticians, use their expertise to help health careprovidersmanageresources,standardisemedicalcare,coordinateresearchandprovideforthemoreefficientdelivery of healthcare.
Cost reduction: In an April 2006 report to the U.S. Agency for Healthcare Research and Quality, or AHRQ, the •Southern California Evidence-based Practice Centre wrote that in the United States, 50 percent of the nation’s healthcarecostsarewastedoninefficientprocesses.Healthinformaticiansstudywhathealthcareprovidersdoand how they do it. Through health informatics, some labour-intensive medical procedures can be automated, thereby saving precious health care dollars. Procedures rife with human error, such as physician medical orders, can be computerised, reducing the potential for mistaken interpretation of written orders and possible malpractice lawsuits.Electronic health records: Perhaps the greatest advantage of using health informatics is the ability to improve •health records management. Often when a patient seeks medical treatment, especially in an emergency situation, heisunabletoprovidespecificdetailsofhismedicalhistory.Whenfamiliesrelocate,childhoodimmunisationrecords can be misplaced or past physician names forgotten. A comprehensive electronic patient health record can solve these problems. This can be a network of existing health care systems or a newly developed electronic health record, a records system that follows a patient through his entire life.Trends and threats: An electronic health record is valuable for an individual patient. Networked together, an •electronic health records system is valuable for tracking medical details for entire populations. As of December 2008, the U.S. Centres for Disease Control and Prevention began tracking health data on 75 percent of American children under age 6. This is an invaluable dataset. For instance, if an outbreak of measles occurs in a given region, health care providers can access a database to track new cases as they are diagnosed and determine how many children in the area have been vaccinated. Health informatics allows for researchers and physicians to observe disease trends and health outcomes for large populations.Patient education: Physicians know that patients do not always follow their medical advice. Health informatics •helps determine patient motivation and provides solutions. If a physician is serving a low-literacy patient population, instead of providing medical literature and written information on medication, health informaticians can develop multimedia materials and audio instructions. In “Consumer Health Informatics: Informing Consumers and Improving Health Care,” Deborah Lewis writes that the literacy level of patients with diabetes correlates directly to how they manage their disease.
Health Informatics and Management Information
10/JNU OLE
Accuracy: Health informatics allows a systematic way of storing and retrieving information. This is much •more accurate than the recollection of a patient for details of existing medications and allergies. This is a major patient safety issue. Incorrect or incomplete information from a confused patient can lead to an adverse effect. Therefore, having such accurate information provided at the point where it is needed is necessary.Efficiency:Healthinformaticsfacilitatesjoined-upcare.Thevariousdepartments,beitlaboratory,radiology,•surgery or administrative departments, are interconnected. Duplication of efforts is reduced. This speeds up processes. A patient’s hospital stay need not be extended unnecessarily. This time-saving factor is especially important with the increasingly growing health care needs.Improve patient care: Health informatics not only merely allows storage and retrieval of information, but can •infactbeadecision-makingtool.Computerisedguidelinesofferbenefitstohelpcliniciansandpatientsmakebetter decisions. With this, high quality treatment can be maintained. Moreover, less time on administrative work means that doctors and other health professionals can have more time with the patients. For instance, a large scale health screening programme would not have been feasible without the high technology implemented.Paperless technology: Health Informatics removes the need to keep recording the same date again and again •and again. It reduces wastage. This is good news for the environment.
1.9.1 Disadvantages of Health InformaticsThe following are the advantages of health informatics:
Expensive:An increasingly sophisticated health technology definitely does not come cheap.Wehave to•understandthatallfirstworldnationalhealthcaresystemsfacearangeofchallenges;oneofwhichistheageingpopulation. People are living longer. So what does this imply? This means an increased health needs but the working population generating income to pay for healthcare system is reduced. So one consideration would be, is the high cost which comes with high technology economically viable for the government?Requires time to adapt fast: As we know, technology is constantly evolving. Many a time there will be new soft •wares, new upgrades, and new way of doing things. In order to keep up with the competitive edge, hospital staff has to keep up with such changes. This can be a struggle for some, especially for the older staff.Over-dependency on technology: While once the staff has adapted to the new way of work, there comes the next •problem. It is not uncommon for a computer system to face technical errors. The health care informatics system is no exception. This problem is especially crucial in the Accident & Emergency (A&E) Department. Various departments in the hospital are interconnected by a common information system. When 1 department is down, others are affected. For example, a patient was rushed into the A&E Department. When there is an error while retrieving blood analysis information, the rest of the procedures following it will be delayed. This will cause hugeinconveniences,orworse;itmayevenhaveadverseeffectsinthepatient’shealthcondition.Susceptibility to network hackers: Patients’ medical history and other health information should be kept •confidentialforethicalandlegalreasons.Whilethehealthcaresystemnetworkisdefinitelyequippedwithsecurity measures, it is not impossible for network hacking to occur. Hence, this is certainly a vulnerability of Health Informatics.
1.10 OutlookThe demand for health informatics professionals is strong. Employment of medical records and health information technicians is expected to increase by 20 percent through 2018, which is faster than the average for all occupations, according to the U.S. Department of Labour Bureau of Labour Statistics. The federal government in 2009 invested billions of dollars in health information development and implementation through the American Health Recovery andReinvestmentActof2009.Healthcaresystemsseekhealthinformaticsdegreeholderstofulfilcriticalrolesinvolvingsettingpoliciesandmakingdecisionsinthefield.Thedemandinthisindustryisstrongbecausehealthinformatics can deliver new information technologies and systems that lead to higher quality health care at a lower cost.
1.10.1 Career OptionsWith the emergence of emphasis on the electronic health record, degree holders in health informatics have multiple career options in managing health information to ensure patient safety and quality. These opportunities are available inmanysettings,suchasnursinghomes,hospitalsanddoctors’offices.Inaddition,healthinformaticsprofessionalscan work in outpatient care centres, for home health care agencies and for government agencies.
11/JNU OLE
Summary HealthorMedicalInformaticsisthe“scientificfieldthatdealswithbiomedicalinformation,data,andknowledge- •their storage, retrieval, and optimal use for problem solving and decision making.Medical information science is the science of using system-analytic tools to develop procedures (algorithms) •formanagement,processcontrol,decisionmakingandscientificanalysisofmedicalknowledge.Healthinformaticscombinesthefieldsofmedicine,informationscienceandinformationtechnologytoformulate•various systems for generating, validating, securing and integrating health-related data.Health/Medical/Biomedical Informatics is the interdisciplinary, scientificfield that studies andpursues the•effectiveusesofbiomedicaldata,information,andknowledgeforscientificinquiry,problemsolvinganddecisionmaking, motivated by efforts to improve human health.Health Informatics develops, studies and applies theories, methods and processes for the generation, storage, •retrieval, use, and sharing of biomedical data, information, and knowledge.Health Informatics builds on computing, communication and information sciences and technologies and their •application in biomedicine.Health Informatics investigates and supports reasoning, modelling, simulation, experimentation, and translation •across the spectrum from molecules to populations, dealing with a variety of biological systems, bridging basic and clinical research and practice, and the healthcare enterprise.Health Informatics recognising that people are the ultimate users of biomedical information, draws upon the •social and behavioural sciences to inform the design and evaluation of technical solutions and the evolution of complex economic, ethical, social, educational, and organisational systems.Therearebasicallythreeareasinthehealthinformaticsfieldwheretheuseofinformationsystemsmaybeused•tocreatemoreoperatingefficienciesandeffectiveness:clinical,administrativeandmedicalinformation.Widespread implementation of health informatics could create a seamless and more complete health care •system.Health informatics also plays a prominent role in health law.•TheNationalLaboratoryofMedicinedefineshealthinformaticsas“theinterdisciplinarystudyofthedesign,•development, adoption and application of IT-based innovations in health care services, delivery, management and planning.”Health informatics is the combination of informational science, health care and computer technology•The data retrieved by the use of heath informatics provides statistical information that can have a profound •effect on how medicine is distributed, surgeries is performed and how healing is tracked.The greatest advantage of using health informatics is the ability to improve health records management.•Physicians know that patients do not always follow their medical advice. Health informatics helps determine •patient motivation and provides solutions.If a physician is serving a low-literacy patient population, instead of providing medical literature and written •information on medication, health informaticians can develop multimedia materials and audio instructions.Health informatics not only merely allows storage and retrieval of information, but can in fact be a decision-making •tool.Computerisedguidelinesofferbenefitstohelpcliniciansandpatientsmakebetterdecisions.Health Informatics removes the need to keep recording the same date again and again and again. It reduces •wastage. This is good news for the environment.

Health Informatics and Management Information
12/JNU OLE
ReferencesIntroduction to Health Informatics• , [Online] Available at: <http://www.coiera.com/> [Accessed 19 November 2012].Health Informatics, • [Online]Availableat:<http://www.ehow.com/facts_5574843_define-health-informatics.html> [Accessed 19 November 2012].Kudyba, S., 2010. • What is Healthcare Informatics? [Video Online] Available at: <http://www.youtube.com/watch?v=pzS--PaGC9o> [Accessed 19 November 2012].Shortliffe, E. 2011. • What is Informatics? [Video Online] Available at: <http://www.youtube.com/watch?v=xha0EI3r4hY> [Accessed 19 November 2012].Conrick, M, 2006. • Health Informatics, Cengage Learning Australia. Sullivan, F. & Wyatt, J., 2009. • ABC of Health Informatics, Wiley.
Recommended ReadingLorenzi, N. & Riley, R., 2004. • Managing Technological Change: Organisational Aspects of Health Informatics, SpringerRoss, D., Hinman, A., Saarlas, K. & Foege, W., 2002. • Public Health Informatics and Information Systems, Springer.Coiera, E., 2003. • Guide to Health Informatics, Arnold.

13/JNU OLE
Self Assessment Health informatics is a __________ and hence is good news to the environment.1.
pollution free technologya. paperless technologyb. less time consuming technologyc. sound free technologyd.
If a physician is serving a ________ population, instead of providing medical literature and written information 2. on medication, health informaticians can develop multimedia materials and audio instructions.
educated patient a. computer educated patientb. mentally challenged patient c. low-literacy patient d.
The greatest advantage of using health informatics is the ability to improve __________.3. patients healtha. doctor’s knowledge b. health records managementc. medical sectord.
Which of the following statements is true?4. The data retrieved by the use of heath informatics provides statistical information that can have a profound a. effect on how medicine is distributed, surgeries is performed and how healing is tracked.The data retrieved by the use of health informatics provides statistical information that has a profound effect b. on patient’s health. The data retrieved by the use of health informatics provides statistical information that has a profound effect c. on reputation of the hospital. The data retrieved by the use of health informatics provides statistical information that has a profound effect d. on smooth functioning of hospital activities.
Which of the following statements is true? 5. In 1950’s, heal informatics was also known as medical science.a. In 1950’s, health informatics was also known as medical informatics. b. In 1950’s, health informatics was also known as medical documentation.c. In 1950’s, health informatics was also known as medical computerisation. d.
The_________defineshealthinformaticsas“theinterdisciplinarystudyofthedesign,development,adoption6. and application of IT-based innovations in health care services, delivery, management and planning.”
National Laboratory of Medicinea. Indian Laboratory of Medicineb. World Laboratory of Medicinec. Multinational Laboratory of Medicined.
Health Informatics and Management Information
14/JNU OLE
_________ is concerned with the use of technology to support the research and practice of veterinary 7. medicine.
Nursing informaticsa. Clinical Informaticsb. Veterinary informaticsc. Public Health informaticsd.
__________ deals with how nurses collect and manage their data-including observations that they make about 8. patients’ and their diagnoses, and plans that nurses use for patient care.
Nursing informaticsa. Clinical Informaticsb. Veterinary informaticsc. Public Health informaticsd.
Which of the following statements is false? 9. Oneofthemainchallengesinthehealthinformaticsfieldisthetaskofgettingmosthealthcareprovidersa. to implement the various aspects of information technology into their day-to-day practices.Widespread implementation of health informatics could create a seamless and more complete health care b. system. Health informatics also plays a prominent role in health law.c. Nursing informatics is concerned with the use of technology to support the research and practice of veterinary d. medicine.
__________isthe“scientificfieldthatdealswithbiomedicalinformation,data,andknowledge-theirstorage,10. retrieval, and optimal use for problem solving and decision making.
Health or Medical Informaticsa. Clinical Informaticsb. Nursing Informatics c. Veterinary informaticsd.
15/JNU OLE
Chapter II
Health Informatics and Information Management
Aim
The aim of this chapter is to:
explain the history of health informatics•
elucidate the origins of health informatics•
explicate the difference between health informatics and health information management•
Objectives
The objectives of this chapter are to:
describe the concept of health informatics and information management•
elucidatetheeventualgrowthofHIMinmedicalfield•
explicate the differences between HIM and health informatics•
Learning outcome
At the end of this chapter, you will be able to:
identify the difference between the HIM and health informatics•
understand the history of health informatics•
describe the past and future aspects of health informatics and HIM•
Health Informatics and Management Information
16/JNU OLE
2.1 IntroductionIn considering a ‘history’ of Health Informatics it is important to be aware that the discipline encompasses a wide array of activities, products, research and theories. Health Informatics is as much a result of evolution as planned philosophy, having its roots in the histories of information technology and medicine. The process of its growth continues so that today’s work is tomorrow’s history.
As well as its successes, the history of Health Informatics is populated with visionary promises that have failed tomaterialisedespitethebestintentions.Forthosestudyingthesubjectorworkinginthefield,theexperiencesof others’ use of Information Technologies for the betterment of health care can provide a necessary perspective. This chapter starts by noting some of the major events and people that form a technological backdrop to Health Informatics and ends with some thoughts on the future.
2.2 History of ComputingWhile thousands of individuals have been part of the evolution of computing in the last century, some perspective on the history of computing development is useful in understanding the current level of development and sophistication (or lack of it) in today’s computing environment.
The desire to represent information in ways that allow real world issues to be more easily managed has been a common pursuit for centuries. As far back as in the 17th century Wilhelm Von Liebnitz was advocating the idea that itmightbepossibletorepresenttheentirenatureofhumanbehaviourinsomecodifiedform.Thisprinciplestillforms the basis on which many software developers, especially in medicine, view coding. That is, if we developed afineenoughcodingsystem,thenallthingsmaybeclassified.
Thefirstexampleofhowsuch toolsmightbecreatedand theuses towhich theycouldbeputcanreliablybeascribed to Charles Babbage in the 19thCentury.ItisgenerallyagreedthatMr.Babbagecreatedthefirstcomputer,amechanical device aimed at solving mathematical problems. The machine never succeeded in functioning as desired and he stumbled from funding source to funding source (Kings, Queens and heads of State). The issue of whether ornothis‘analyticalengine’couldeverhavesucceededismoot;howeverhismachinenotonlystillexists,buthasalso been recreated in an attempt to settle the argument. It appears that, if accurate enough engineering techniques hadbeenavailable;hislifeworkcouldhavesucceeded.
Theabovetwohistoricalfigureshighlightthefactthattheprinciplesunderlyingtoday’suseofcomputershasbeenaround for a very long time. The punch card system devised by Herman Hollerith in the 1890’s to manage the United States census data demonstrates the effectiveness of technologies that do not use the microchip capabilities of today. This system was so successful that it was still being used after World War II. It involved hundreds of workers developing the ability to punch cards and also to pass long needles through trays of such cards to perform data analysis. Even when digital (electronic) computers were developed, punch cards were still used as the major form of data input, as any computer science student of the 50’s and 60’s can verify. Despite the development of everincreasinglypowerfulcomputersoverthistime,itwasnotuntiltheendofthe1960’sthatthistechniquefinallywas laid to rest.
2.3 Computers: The Electronic ComputerThe need for information management during World War II spurred the development of electronic computers. The firstdigitalorelectroniccomputerwasENIAC,createdinthe1940’s.Thisdeviceoccupiedalargeroomandranon valves with enormous power consumption and remains at the Smithsonian institute as a reminder of the scale of changeinthiscentury.PostWWIIcomputerscontinuedtoevolveinspeed,capacity,sophisticationandreliability;they also continued to reduce in size. Due to the specialised environments, space and support needed to run these devices, the concept of mainframe computing evolved.
Mainframe computing implies a central computer which supports users at distance through the provision of ‘dumb’ terminals. Note that the idea of computing at distance (via a terminal) only occurred in the late 40’s and early 50’s.
17/JNU OLE
This centralised form of computing services supported by an Information Management Service (IMS) remained the norm until the late 60’s, early 70’s. In the late 1950’s Ledley and Lusted, living in a world of now powerful new computing devices, where among many who recognised the potential of computer-assisted medical decision making. While access, cost, and implementation were seen as limiting the ability to provide such support in a widely available fashion, the belief was evident that increasing computational power could be harnessed to model, assist and enhance health care. While the ‘dumb terminal’ - mainframe model of computing services was not able to adequately address this desire, the coming years would see the ‘personal computer’ become a reality, initially as the minicomputer.
The emergence of minicomputers in the late 60’s provided what were, in essence, stripped down mainframes with their own storage ability, aimed at supporting a small number of local user and promising a future of ‘personal’ computing. These were still very expensive but were a major leap forward from the distributed, ‘dumb terminal’ philosophy of previous decades. So enthusiastic were many of the proponents of minicomputers that advertisement fromthe60’sand70’sdescribedthedesirabilityforMedicalPractitionerstopurchasethemtoimprovetheirofficeand patient management. The promise that such technologies could so intimately assist health professionals at a personallevelremainstoday.Thatpromiseissatisfiedmoreoftentodaythenbutdisappointmentoftenremainseven with current advanced systems.
2.3.1 Microcomputers Arrive The highly personal availability of computing technologies became more possible with the advent of the microcomputer.TheAppleIImicrocomputer(6502chip,monochromedisplay,tapeorfloppystorage)providedthefirstrealpersonalcomputer,whilstmanyothermicrocomputersexisted(Tandy,Commodore,Zenithetc)thiswasthefirstthatencouragedaverageuserstoindulgeinprogrammingandtheproductionofsoftwareonalargescale destined for personal use.
While these machines initially penetrated the home / hobbyist market rather than business, the introduction of the programVISICALC (thefirst, functional, spreadsheet program) altered the perceptionofmicrocomputers andtheirusefulness.Thebusinessworldsuddenlyhadapowerfulnewtoolforfinancialmodellingofferingafamiliarparadigm (an accounting sheet) with the power of microcomputer based technologies behind it. Such applications didnotescapetheattentionofthoseresponsibleforthefinancialmanagementofhealthcare.Asforallaspectsofsociety, the personal computer found its way into practice environments, hospital systems, organisations working in epidemiological work and a host of other health related areas.
In1982IBMreleasedtheIBMPC(640K,cassetteorfloppystorage,colourdisplay).ItappearsthatIBMdidnotconsider this machine as a serious project and that the explosion of clones, acceptance by business and the massive secondary industry generated by software developers was completely unpredicted. Initial projections were for a few thousand sales. The currently installed base of machines with this architecture is well into the millions.
The release of the Macintosh computer (evolved from the Xerox PARC work and the Apple Lisa) offered a whole new principle in how users could interact with computers. Now called the WIMP interface (Windows, Icons, Mouse andPopdownmenus),thiswasthefirstpractical,commerciallyavailable,GraphicUserInterfaceorGUIanditsunderlying philosophy can be attributed in large part to Douglas Engelbart, the inventor of the mouse as a pointing device.
Asthesemicrocomputersbecameincreasinglypowerfulandpopularthroughthe1980’sIMSgroupsfinallystartedagreeing that these ‘toys’ should have some access to mainframes, usually if they agreed to behave as dumb terminals. Users also found the need to connect PC’s together resulting in the development of Local Area Networks (LANs).
Without an agreed standard for these endeavours we have the current situation with a wide (but reducing) number of ways to link PC’s together. LAN structures now communicate with each other forming Wide Area Networks (WAN) with links into mainframe services.

Health Informatics and Management Information
18/JNU OLE
Overall, this progression of increasingly powerful, smaller and faster computing possibilities has resulted in the availability of the ‘personal’ computer. Ideally, technology should be an additional tool for individuals providing connectivity to resources far greater than personal experience, education or traditional paper based repositories of information could provide. All of this is possible because of the development of the microchip or integrated circuit, predominantly developed by the companies INTEL and MOTOROLA. These ‘chips’ are evolving at a rapid pace providing more and more processing power. These ‘hardware’ advances are not matched by developments insoftware;processorsspendmuchoftheirtimedoingnothing.ThewidespreadadoptionoftheGUIinterface,larger and more sophisticated software creations and the need to enhance the means whereby users interact with the computer means that the hoped for developments of handwriting and speech recognition in a highly interactive graphic environment are now occurring.
2.4 Computer Languages - Telling the Computer What to Do? The software programs have evolved along with the hardware base itself, although at differing rates. These languages range from telling the computer what to do at a very low level, such as assembly language, to much more abstracted meansof representationprovidedbyObjectOrientatedSystems,Natural language tools,Artificial Intelligencemethodologies and a variety of others. In an inevitable progression, the increased hardware capabilities are used by developers to create more and more sophisticated means of ‘communicating’ with the computer to manage information in more and more natural ways.
While the above is promising, the actual tools we use on computers today are still in their infancy in many ways. The vast majority of computer human interaction is via the keyboard, itself an unfriendly legacy of the past. The QWERTY keyboard design aims to reduce typing speed so as to decrease the possibility of the letter ‘hammers’ jamming, despite the fact that such typewriters are now museum pieces.
Health care poses some of the greatest challenges for both the technologies and those seeking to apply them to patient care. Health care often deals with the most abstract of ideas such as ‘well’, ‘pain’, ‘happy’, ‘sad’. Health care also generates enormous volumes of information regarding the community and its needs. Thus understanding Health Informatics requires not only familiarity with the technology but, more importantly, insight into the nature in which health care delivery occurs. These questions are not yet answered but Health Informatics lays claim to someofthepossibledirectionsandsolutionsmostlikelytobeofbenefit.
2.5 Health Informatics - A Discipline Health Informatics is often described as a new discipline. It has evolved to address the desires to apply and explore the uses of these relatively new tools for the better provision of health care. This is a bold claim with some merit. Thesuccessesofthefieldinlivinguptotheclaimhavebeenlessthanexpectedandhave,attimes,disruptedthetimely delivery of health care rather than enhanced it. This is not entirely surprising given the accelerating rate of change in technologies and the relatively ‘young’ nature of a discipline which is now examining itself to clarify its role. Health Informatics began as Medical and Nursing Informatics during the 1970s, a period described as undergoing exponential development due to the growing availability of steadily less expensive hardware, more powerful software and the advent of microcomputers.
A gradual change from electronic data processing in health, through the use of informatics in medical care, to health informatics, is discernable from the types of papers presented at the three yearly World Congresses on Medical Informatics (Medinfo), which began in 1974 in Stockholm. The use of computers to support medical decision making,includingartificialintelligence,wasstrongduringthe1980s.Thelinkageofsystemsemergedin1989when multiple disciplines began to work together to develop integrated systems utilising new database technology and the power of networks. This produced synergistic applications where the whole became greater than the sum of its parts. The most popular papers presented at Medinfo’92 in Geneva were those on knowledge based work such as concepts, methodologies, software and other tools, systems and evaluations of systems and experiences. These congresses were organised by the International Medical Informatics Association (IMIA), which began as a special interest group of IFIP.
19/JNU OLE
While Health Informatics aims to articulate its place in health care, other health care professionals continue to adopt the technologies into their own areas. For example, the use of computing systems in radiological imaging is extensive. Amongst the lessons to be learned from the history of Health Informatics is that Health Informatics as a discipline must be cognisant of, and involved in, the aims and activities of health care itself. Technologies are becoming ubiquitous in their availability with ever increasingly powerful tools allowing health care workers to readily create systemsfortheirownbenefit.HealthInformaticsshouldcommunicatetothehealthcareprofessionthelessonsofits past, just as Health Informatics needs to learn from the work and activities of this same community.
Thebenefitsofthetechnologyaswellastheabilitytodemonstratesuchbenefitstoothersarebecomingcompulsory.Thereasonsforthisinclude:theeffectofcomputerusagebypractitionersonpatientsthemselves;thesecurityofmedicalinformation;theneedfornewskillstobelearned;andthepriceofthetechnologyatatimewhenrisinghealth care costs are an international concern.
Health Informatics strives to enhance all aspects of health care at all times. If this is kept in mind, the lessons of history to date will be heeded and incorporated into the future of Information Technology in health care, rather than ignored.
2.6 History of Health InformaticsHealth care informatics uses technology, such as computers and networking, and multidisciplinary health sciences, such as biomedical and pharmacy, to improve patient care. Informatics organises patient data into a coherent format suitable for smooth health care processes.
In1949,GustavWagerfoundedthefirstprofessionalorganisationforinformaticsinGermany.Informaticstrainingprograms began during the 1960s in France, spreading throughout Europe and to the United States by 1970. This early form of health care informatics focused on generating bills and patient admissions/discharges. U.S. hospitals thatimplementedthisstructureincludeLatter-DaySaintsHospitalinSaltLakeCity,Utah;MassachusettsGeneralHospitalinBoston;andKaiserPermanenteinOakland,California.
2.6.1 Technological AdvancesThe rapid rise and spread of health care informatics is linked to technology and computers advances during the 1970s. The systems of this time used a single mainframe and time-shared computers to process all patient information. By the 1980s, health care practitioners used several small computers on the same patient database. Organisations began to develop standards and protocols for health care information transmissions. This form of informatics was unabletoproducecustomisedreportsandstillfocusedonfinancialaspects.
American medical informatics associationFormed in 1990 from three other organisations, the American Medical Informatics Association (AMIA) focuses on educating health care professionals from all disciplines in health care informatics standards and systems. The organisation has around 3,200 members, and states that by 2010, 10,000 professionals will be trained to use health care informatics effectively.
Network environmentStartingin1995,highlynetworkedcomputersanddatabasesbegantofacilitatefree-flowinghealthcareinformation.Focus shifted to patient care and custom reports. Support applications for all aspects of health care, such as drug interaction alerts and electronic prescription writing, contributed to high-quality patient care. Personal computers startedtodecreaseincost,andbecameanessentialtoolinmosthealthcareoffices,easilyincorporatedexistinginformatics systems.
SpecialisationAshealth care informatics systems becomemore customisable andflexible, health careworkers have takenpersonalised approaches. Clinical specialists use the informatics systems to concentrate on individual patients. Public healthworkersusethesamesystemtoevaluatehealthconcernsinsocietyandspecificpopulations.Informaticshasalso been used in research and theory development.
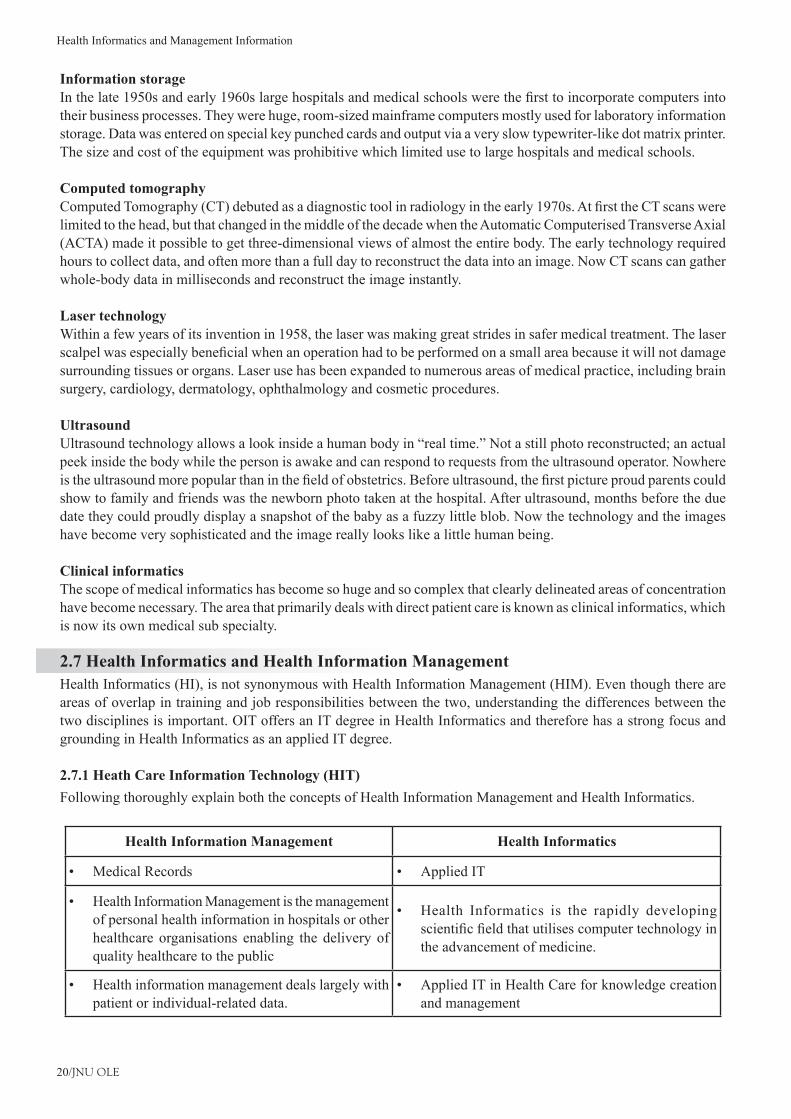
Health Informatics and Management Information
20/JNU OLE
Information storageInthelate1950sandearly1960slargehospitalsandmedicalschoolswerethefirsttoincorporatecomputersintotheir business processes. They were huge, room-sized mainframe computers mostly used for laboratory information storage. Data was entered on special key punched cards and output via a very slow typewriter-like dot matrix printer. The size and cost of the equipment was prohibitive which limited use to large hospitals and medical schools.
Computed tomographyComputedTomography(CT)debutedasadiagnostictoolinradiologyintheearly1970s.AtfirsttheCTscanswerelimited to the head, but that changed in the middle of the decade when the Automatic Computerised Transverse Axial (ACTA) made it possible to get three-dimensional views of almost the entire body. The early technology required hours to collect data, and often more than a full day to reconstruct the data into an image. Now CT scans can gather whole-body data in milliseconds and reconstruct the image instantly.
Laser technologyWithin a few years of its invention in 1958, the laser was making great strides in safer medical treatment. The laser scalpelwasespeciallybeneficialwhenanoperationhadtobeperformedonasmallareabecauseitwillnotdamagesurrounding tissues or organs. Laser use has been expanded to numerous areas of medical practice, including brain surgery, cardiology, dermatology, ophthalmology and cosmetic procedures.
UltrasoundUltrasoundtechnologyallowsalookinsideahumanbodyin“realtime.”Notastillphotoreconstructed;anactualpeek inside the body while the person is awake and can respond to requests from the ultrasound operator. Nowhere istheultrasoundmorepopularthaninthefieldofobstetrics.Beforeultrasound,thefirstpictureproudparentscouldshow to family and friends was the newborn photo taken at the hospital. After ultrasound, months before the due date they could proudly display a snapshot of the baby as a fuzzy little blob. Now the technology and the images have become very sophisticated and the image really looks like a little human being.
Clinical informaticsThe scope of medical informatics has become so huge and so complex that clearly delineated areas of concentration have become necessary. The area that primarily deals with direct patient care is known as clinical informatics, which is now its own medical sub specialty.
2.7 Health Informatics and Health Information ManagementHealth Informatics (HI), is not synonymous with Health Information Management (HIM). Even though there are areas of overlap in training and job responsibilities between the two, understanding the differences between the two disciplines is important. OIT offers an IT degree in Health Informatics and therefore has a strong focus and grounding in Health Informatics as an applied IT degree.
2.7.1 Heath Care Information Technology (HIT)Following thoroughly explain both the concepts of Health Information Management and Health Informatics.
Health Information Management Health Informatics
Medical Records• Applied IT•
Health Information Management is the management •of personal health information in hospitals or other healthcare organisations enabling the delivery of quality healthcare to the public
Health Informatics is the rapidly developing •scientificfieldthatutilisescomputertechnologyinthe advancement of medicine.
Health information management deals largely with •patient or individual-related data.
Applied IT in Health Care for knowledge creation •and management
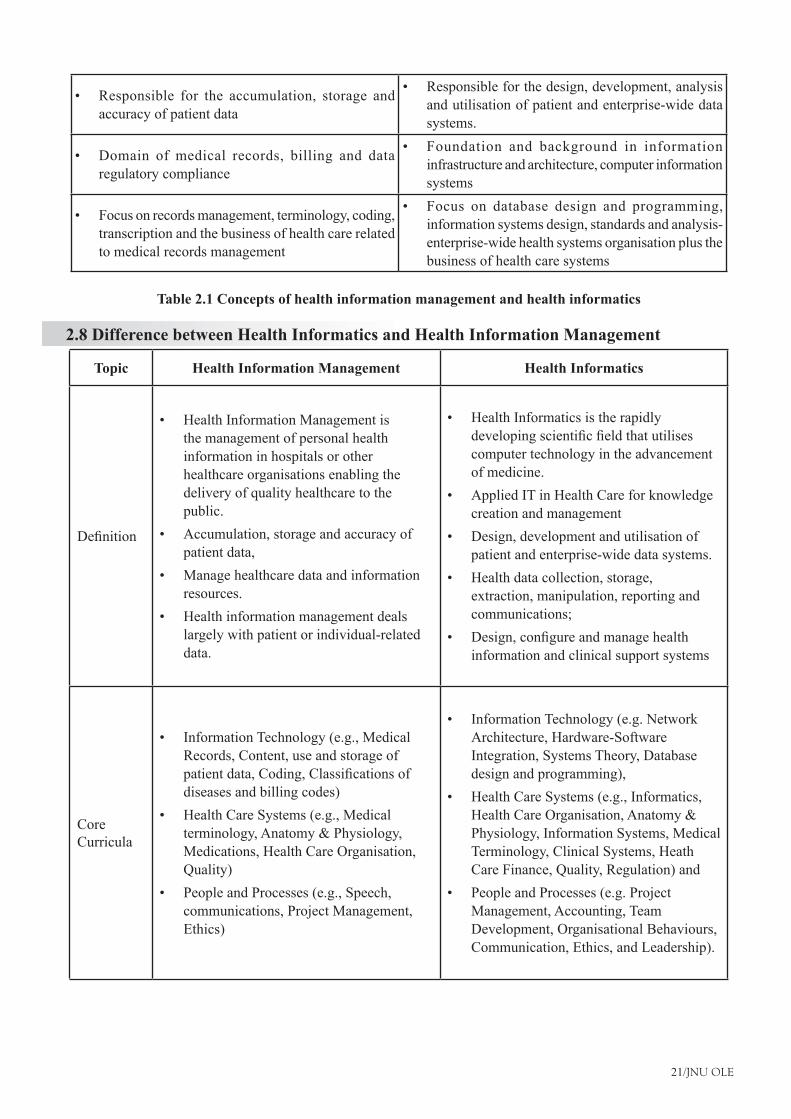
21/JNU OLE
Responsible for the accumulation, storage and •accuracy of patient data
Responsible for the design, development, analysis •and utilisation of patient and enterprise-wide data systems.
Domain of medical records, billing and data •regulatory compliance
Foundation and background in information •infrastructure and architecture, computer information systems
Focus on records management, terminology, coding, •transcription and the business of health care related to medical records management
Focus on database design and programming, •information systems design, standards and analysis-enterprise-wide health systems organisation plus the business of health care systems
Table 2.1 Concepts of health information management and health informatics
2.8 Difference between Health Informatics and Health Information Management
Topic Health Information Management Health Informatics
Definition
Health Information Management is •the management of personal health information in hospitals or other healthcare organisations enabling the delivery of quality healthcare to the public.Accumulation, storage and accuracy of •patient data,Manage healthcare data and information •resources.Health information management deals •largely with patient or individual-related data.
Health Informatics is the rapidly •developingscientificfieldthatutilisescomputer technology in the advancement of medicine. Applied IT in Health Care for knowledge •creation and managementDesign, development and utilisation of •patient and enterprise-wide data systems. Health data collection, storage, •extraction, manipulation, reporting and communications;Design,configureandmanagehealth•information and clinical support systems
Core Curricula
Information Technology (e.g., Medical •Records, Content, use and storage of patientdata,Coding,Classificationsofdiseases and billing codes)Health Care Systems (e.g., Medical •terminology, Anatomy & Physiology, Medications, Health Care Organisation, Quality)People and Processes (e.g., Speech, •communications, Project Management, Ethics)
Information Technology (e.g. Network •Architecture, Hardware-Software Integration, Systems Theory, Database design and programming), Health Care Systems (e.g., Informatics, •Health Care Organisation, Anatomy & Physiology, Information Systems, Medical Terminology, Clinical Systems, Heath Care Finance, Quality, Regulation) andPeople and Processes (e.g. Project •Management, Accounting, Team Development, Organisational Behaviours, Communication, Ethics, and Leadership).

Health Informatics and Management Information
22/JNU OLE
Job Titles
Medical Records Managers•Patient Information Coordinator•Billing Coder•Medical Biller•PrivacyOfficer/Manager•ComplianceOfficer•Data Quality Manager – Clinical and •AdministrativeHealth Information Management Director•
Health Information System Manager•Interoperability, Interfacing And Usability •ManagementApplications Software Consulting•Database Analyst / Administrators•Systems Analysts•Application Coordinators•Application Support Services•Knowledge manager•
Job Duties/Roles
Organise and manage patient data contained •in the medical recordCode health information for reimbursement •and research.Ensure compliance to governmental •regulations related to patient dataEnhance the quality and uses of data within •the health care industry. Summarise data into useful information. •Comply with standards and regulations •regarding health information. Protect the privacy and security of patient •health information. Ensure health information is complete and •available to legitimate users. Monitoring electronic and paper based •documentation, processing and using health data for billing and reporting purposes.
Design and develop information systems and •processes that improve quality, effectiveness andefficiencyofcareDesign, develop and assess emerging •technologiesProviding data management and analytical •skills as well as ensuring data security and qualityDesign and maintain medical databases, •computer networks, and internet or multimedia applicationsStandard-setters for electronic health •records and other emerging technologies Design and maintenance of protocols based •on evidence Development of terminology, standards, and •classificationsystemsEvaluation of the impact of information •technology on the clinical process, clinical outcome, organisations, and resources.
Employers
Hospitals•Medical groups and clinics•HMOs•Health insurance organisations•research•policy organisations•accountingandlegalfirms•
Hospitals•Medical groups and clinics•HMOs •Health insurance organisations•research•policy organisations•medical research laboratories•Internet companies•Hardware and software vendors•health information technology suppliers•consulting organisations•
Table 2.2 Difference between health informatics and health information management
23/JNU OLE
SummaryHealth Informatics (HI) is not synonymous with Health Information Management (HIM). •Health Information Management is the management of personal health information in hospitals or other healthcare •organisations enabling the delivery of quality healthcare to the public.HealthInformaticsistherapidlydevelopingscientificfieldthatutilisescomputertechnologyintheadvancement•of medicine.Health Information Management relates medical records whereas Health Informatics• relates to applied IT.Health Information Management is responsible for the accumulation, storage and accuracy of patient data.•Health Informatics is responsible for the design, development, analysis and utilisation of patient and enterprise-•wide data systems.Health Information Management is a domain of medical records, billing and data regulatory compliance.•Health Informatics is the foundation and background in information infrastructure and architecture, computer •information systems.Health Information Management focus on records management, terminology, coding, transcription and the •business of health care related to medical records managementHealth Informatics focus on database design and programming, information systems design, standards and •analysis –enterprise-wide health systems organisation plus the business of health care systems.Health Information Management is the management of personal health information in hospitals or other healthcare •organisations enabling the delivery of quality healthcare to the public.Health information management deals largely with patient or individual-related data.•Health Informatics is as much a result of evolution as planned philosophy, having its roots in the histories of •information technology and medicine.ThefirstdigitalorelectroniccomputerwasENIAC,createdinthe1940’s.•Understanding health informatics requires not only familiarity with the technology but, more importantly, insight •into the nature in which health care delivery occursHealth Informatics began as medical and nursing informatics during the 1970s, a period described as undergoing •exponential development due to the growing availability of steadily less expensive hardware, more powerful software and the advent of microcomputers.Health care informatics uses technology, such as computers and networking, and multidisciplinary health •sciences, such as biomedical and pharmacy, to improve patient care. Informatics organises patient data into a coherent format suitable for smooth health care processes.Support applications for all aspects of health care, such as drug interaction alerts and electronic prescription •writing, contributed to high-quality patient care.
ReferencesThe History of Health Informatics, • [Online] Available at: <http://healthinformatics.uic.edu/history-of-health-informatics/> [Accessed 20 November 2012].The Difference between Health Informatics and HIM• , [Online] Available at: <http://healthinformatics.uic.edu/difference-between-health-informatics-and-him/> [Accessed 20 November 2012].Dr. Kellogg. D., 2012. • USM HIM – What is HIM? [Video Online] Available at: <http://www.youtube.com/watch?v=zwzNayEFVfY> [Accessed 20 November 2012].2012. • What is Health Informatics? [Video Online] Available at: <http://www.youtube.com/watch?v=rFxewUq1cE4> [Accessed 20 November 2012].Kuehn, L., 1997. • Health Information Management: Medical Records Process in Group Practice, Medical Group Management Assn. Huffman, E., 1994. • Health information management, 10th ed., Physicians’ Record Co.

Health Informatics and Management Information
24/JNU OLE
Recommended ReadingJohns, M., 2002. • Health Information Management Technology: An Applied Approach, American Medical Records Association. Gartee, R., 2010. • Health Information Technology and Management, Pearson.Whetton, S., 2005. • Health Informatics: A Socio-technical Perspective, Oxford University Press.
25/JNU OLE
Self Assessment Which of the following statements is true? 1.
Health care informatics uses technology, such as computers and networking, and multidisciplinary health a. sciences, such as biomedical and pharmacy, to improve doctor’s health.Health care informatics uses technology, such as computers and networking, and multidisciplinary health b. sciences, such as biomedical and pharmacy, to improve patient care.Health care informatics uses technology, such as computers and networking, and multidisciplinary health c. sciences, such as biomedical and pharmacy, to improve hospital facilities. Health care informatics uses technology, such as computers and networking, and multidisciplinary health d. sciences, such as biomedical and pharmacy, to improve the reputation of the hospital.
Health Informatics began as __________ during the 1970s, a period described as undergoing exponential 2. development due to the growing availability of steadily less expensive hardware, more powerful software and the advent of microcomputers.
medical and nursing informaticsa. clinical and medical informaticsb. medicine informaticsc. nursing informaticsd.
___________________ focus on database design and programming, information systems design, standards and 3. analysis -enterprise-wide health systems organisation plus the business of health care systems
Health Information Management a. Health Informaticsb. Clinical Informaticsc. Nursing Informaticsd.
__________ focus on records management, terminology, coding, transcription and the business of health care 4. related to medical records management
Health Information Managementa. Health Informaticsb. Clinical Informaticsc. Nursing Informaticsd.
Which of the following statements is true? 5. Health Informatics is the foundation and background in information infrastructure and architecture, computer a. information systemsHealth Information System is the foundation and background in information infrastructure and architecture, b. computer information systemsClinical Informatics is the foundation and background in information infrastructure and architecture, computer c. information systemsHealth Information Management is the foundation and background in information infrastructure and d. architecture, computer information systems
Health Informatics and Management Information
26/JNU OLE
Which of the following statements is false? 6. Health Information Management is a Domain of medical records, billing and data regulatory compliancea. Health Information Management is Responsible for the accumulation, storage and accuracy of patient b. dataHealth Information Management focus on records management, terminology, coding, transcription and the c. business of health care related to medical records managementHealth Information Management is the foundation and background in information infrastructure and d. architecture, computer information systems
Health Information Management is the management of __________ in hospitals or other healthcare organisations 7. enabling the delivery of quality healthcare to the public.
personal health informationa. personal problemsb. person’s professionc. personal decisiond.
Health Information Management relates to medical records then Health Informatics relates to __________.8. applied ITa. applied knowledgeb. applied techniquesc. applied medicinesd.
The area that primarily deals with direct patient care is known as __________. 9. nursing informaticsa. clinical informatics b. health or medical informaticsc. health information managementd.
__________ use has been expanded to numerous areas of medical practice, including brain surgery, cardiology, 10. dermatology, ophthalmology and cosmetic procedures.
Computed tomographya. Laser technologyb. Network environmentc. Information storaged.
27/JNU OLE
Chapter III
Health Care Systems, Information Systems and Health Information Science
Aim
The aim of this chapter is to:
explain the concept of health care systems•
elucidate the concept of health information systems•
explicate the health information science•
Objectives
The objectives of this chapter are to:
explaintheinfluenceofeconomic,political,philosophicalaspectsandtechnologicaladvancesonhealthcare•
systems
elucidate the importance of communication of medical information and its management•
explicate various healthcare terminologies •
Learning outcome
At the end of this chapter, you will be able to:
describe various healthcare terminologies•
understand the concept of healthcare and information system •
identify the attributes of communication in healthcare informatics•

Health Informatics and Management Information
28/JNU OLE
3.1 IntroductionHealth care service delivery could be described as an information intensive industry. In contrast the banking industry istransactionintensive.Bothareabletobenefitgreatlyfromtheuseofcomputing,informationandcommunicationstechnology. Yet the banking industry is much further advanced in this regard. A transaction based system relies predominantly on data. These are observations or facts which when collected, evaluated and organised become information or knowledge. Data are computer input elements. Information on the other hand consists of data which are:‘Processedorganisedorclassifiedintocategoriestoserveausefulpurpose.NobelLaureateKennethArrowdefinedinformationas‘areductioninuncertainty’.
Information as an intellectual construct which is subject to constant change. Its importance depends on who makes any information based transactions and when. It is both resource and commodity but unlike matter and energy is not consumed by use.
Communicationsiscentraltoinformationflowandessentiallysubsumedinit.‘Information’dependsheavilyon‘information technology’ (IT) but is a far wider concept, with educational, social, economic, employment and cognitive implications. Data, information, knowledge and intelligence ascend hierarchically.
The concept of encoded data organised as ‘information’ is the common feature of genetics, biotechnology, language, communications, mathematics, electronics, computing and robotics’.
In the banking industry data consists of numbers whilst in the health care industry data takes many forms including numbers, text, concepts (coded data), graphics, images, physiological measures (signals), and sound. Health care professionals rely on all their senses, including smell to collect assessment data from individuals. These data are recorded in a person’s medical history or health record. Now that technology has progressed to the point where all types of data, with the exception of smell, may be produced in digital form it has become feasible to develop fully integrated health information systems. This should assist greatly in meeting the functional needs for health information. Dick (1992) noted that ‘we lack the evidence to make more informed decisions in health care today across the spectrum from the bedside up to the formulation of national health care policy’. He went on to say that ‘most of the evidence needed to make more informed decisions remains embedded in fragmented, irretrievable, and often illegible paper-based patient records”.
Todefinethehealthproblemonemustbeabletoidentifyanddescribethepopulationorgroupsforwhomtheproblem exists as well as various aspects denoting health status, such as incidence of disease, ill health, and deaths, quality of life, plus functional, emotional and mental health status. An understanding of the problem requires data whichareidentifiedasbeingdeterminantsofhealthsuchasreasonsforoccurrence,predisposingfactors,causes,accesstohealthcareservicesandriskfactors.Arrivingatsolutionstotheproblemrequirestheidentificationofeffective interventions provided directly to individuals and to communities, including management protocols, resourceandserviceutilisation.Allinterventionsmustthereforebeidentifiedanddescribedandlinkedtodefinedoutcomesinordertodetermineeffectiveness.Inessenceoutcomemeasuresareidenticaltoproblemidentificationmeasures. These then are the functional health information requirements irrespective of the economic, political, philosophical or organisational considerations of any country’s health care system. The latter will determine the health information systems detailed architectural framework, although in broad terms this should be standardised to suit any health care system.
The Australian Institute of Health and Welfare (AIH&W) has as its mission to inform community discussion and to support public policy-making on health and welfare issues by coordinating, developing, analysing and disseminating national statistics on the health of Australians, and health and welfare services, and by undertaking and supporting related research and analysis. An important mechanism for improving Australia’s health information has been the National Health Information Agreement between the Commonwealth, State and Territory health authorities, the Australian Bureau of Statistics and the AIH&W. This has resulted in a National Health Information Work Program (AIH&W 1993) which incorporates those health information activities that both meet agreed national priorities and have either a national focus or national implications.
29/JNU OLE
Projects cover data collections describing health service institutions, primary care and community health, mental health, medical services, health service outcomes, pharmaceuticals, health insurance, national health expenditure, health labour force, vital statistics, population surveys, surveillance, population health outcomes, national health information policy and infrastructure. In the process a health data dictionary has been developed and is expanding. Thisrepresentsamajorinitiativetowardstheprovisionofanauthoritativesetofnationaldefinitions.TheAIH&Wisdevelopinganationalhealthinformationplandesignedtoovercomeidentifieddeficienciesinitsdatacollectionsto support its mission. For example Harper et al (1994) note that quality of life and most of the behavioural aspects of illness are very poorly described and not available for whole populations.
Similar activities are taking place in other countries. For example in the United States of America the Agency for HealthCarePolicyandResearch(AHCPR)consistsofseveralcomponentsoneofwhichistheOfficeofScienceandData Development which supports and conducts activities designed to increase the amount and usefulness of data (such as that from health insurance claims data bases and computer based patient research) for outcomes and other health services research. The Computer-Based Patient Record Institute (CPRI) was established in 1991 following a report by the Institute of Medicine’s committee for improving the patient record to provide a sustained, coordinated and concentrated effort to establish the widespread use of computer-based patient records. One of a number of high priorities for the CPRI is the development of health data standards.
Three factors have determined the characteristics and development of health information systems. These are economic considerations, technological advances and changes in philosophies regarding health service delivery. The last decade has seen enormous change in all three areas. Various approaches aimed at controlling health care expenditure have emerged. Technological advances in medicine, computing, and communications technology can onlybedescribedasexplosive.Globalchangesregardingsocialstructures,attitudesandvaluesareinfluencingandchanging the expectations of recipients of health care services. In Australia and elsewhere a paradigm shift from a medical model with a physical ill health focus of health service delivery, towards a social, community based model isclearlyevident.Astateofhealthmaybedefinedasageneralsenseofphysical,socialandpsychologicalwellbeing.Whereasillhealthdenotesadeficiencyinwellbeinginoneormoreoftheseaspectswhichmayresultinaninability to function at one’s usual level.
Thestructureandtypeofhealthinformationsystemsdevelopedandimplementedtendtoreflectacountry’shealthcaresystem.Thisinturnisgreatlyinfluencedbythephilosophical,politicalandeconomicunderpinningsofthatsystem. The dominant value driving information system development in industrialised countries has been that of economic constraints, competing pressures regarding resource allocation whilst focusing on the treatment of ill health fromamedicalperspective.Thussystemshavetendedtosupportadministrativeandfinancialactivitiesassociatedwith the treatment of disease and physical ill health. Until more recently clinical management considerations did not feature in most health information system development efforts.
3.2 Economic and Political Influences In 1992 the Organisation for Economic Co-operation and Development (OECD) noted that ‘in recent decades, the growth in health care expenditures has exceeded the growth in gross domestic product across the OECD area. Thishasresultedinagrowingemphasison,andinterestinefficiencyandeffectivenessofhealthservicedelivery.Itistheconcernabouteffectivenesswhichisfinallystimulatingthedevelopmentofclinicalinformationsystems.Tomaximisethebenefitsofthesesystemstheymustlinkwithotherhealthfocusedsystemstogainathoroughunderstandingofthemanyvariableswhichinfluencethegeneralhealthofapopulationandofthemeasuresorcircumstances which successfully improve health.
The Commonwealth, State and Territory health authorities have committed themselves to improving the health outcomes of Australians. Their aim is to achieve optimal individual and population health within available resources throughthisfocus.TheAustralianHealthMinistersAdvisoryCouncil(AHMAC)definedahealthoutcomeas‘achange in the health of an individual, a group of people or population, which is attributable to an intervention or seriesofinterventions’.Asaresultofthisinitiativenationalgoalsandtargetsformakingsignificantimprovementsin the health status of Australian were established. These focus on cardiovascular disease, cancers, mental health and injuries. These were chosen because they are of major concern as a result of their contribution to a high level of death, illness or premature loss of life. Furthermore effective interventions to improve health outcomes were perceived to be possible and the measurement of progress towards these was seen to be feasible.

Health Informatics and Management Information
30/JNU OLE
OthercomponentsoftheAHCPRincludetheMedicalTreatmentEffectivenessProgram(MEDTEP),theOfficeofHealthTechnologyAssessmentwhichevaluatesthesafety,efficacy,effectivenessandwherepossible,thecosteffectivenessofhealthcaretechnologiesandtheOfficeoftheForumforQualityandEffectivenessinHealthCare.Thelatterarrangesforthedevelopment,periodicreview,andupdatingofclinicalpracticeguidelines.Thisofficealso supports the development of performance measures, standards of quality, and medical review criteria for use by health care practitioners and others in reviewing health care quality and services. McCormick notes that the impetus forpracticeguidelinedevelopmentcomesfromidentifiedpracticepatternvariations,concernwithinappropriatenessof care and high healthcare costs.
TheUnitedStatesofAmericaimplementedoutputbasedfundingbasedonpatientclassification,diagnosisrelatedgroups (DRGs), in 1983 to control health care expenditures. Their prospective payment system using DRGs was mandated by the passage of the Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA). In Australia the second round of Medicare Agreements negotiated in 1988 between the Commonwealth, State and Territory health authorities included the introduction of the Casemix Development Program. Its purpose was to develop casemix (output) based approachestohospitalmanagementandfinancingwhichwasacomponentofmicro-economicreformwithinthehealth care industry.
The third round of Medicare Agreements negotiated in 1993 provided for the continued development of casemix related activities.Victoriawas thefirst State to introduce casemix funding in July 1993.NSWuses casemixas a component of its Resource Allocation Formula which is used to fund all health services. It is also a major componentoftheNSWEfficiencyIndexusedtocomparerelativeefficiencybetweenareasanddistricts.Casemixbased budgeting and funding models are used within NSW Area Health Services, districts and hospitals. South Australia introduced casemix based funding in July 1994 and the Queensland Government intends to do so from January 1995. In Tasmania casemix information is used for program reporting and evaluation and as a component oftheTasmanianResourceAllocationModel(TRAM)usedforthepurposeofcostinginter-regionalpatientflows.Western Australia uses casemix as a performance indicator to appraise and compare provider organisations as well as to monitor hospital performance.
In Australia a number of different casemix systems have been developed or are in use including the Australian NationalDiagnosisRelatedGroups(AN-DRGs),AustralianPaediatricAmbulatoryClassification(APAC),AustralianAmbulatoryClassification(AAC),MajorAmbulatoryDiagnosticCategories(MADCs),MajorDiagnosticCategories(MDC),Non-acuteInpatientClassificationSystem(NAIPs),NeonatalDRGs,Nursinghometype(NHT),PaediatricmodifiedDRGs(PM-DRGs),PatientAssessmentandInformationSystem(PAIS)whichisapatient/nursedependencysystem,PsychiatricPatientClasses(PPCs),ResidentClassificationInstrument(RCI)usedbynursinghomesandUrgency Related Groups (URGs) for emergency services. These casemix systems combined with their intended usagegreatlyinfluencethetypesofdatacollectedthroughoutthehealthcaresystem.
TheUnitedKingdom initiateda seriesofprojectsdesigned to introducebusinesspractices regardingfinancialcontrol and budgeting following a management inquiry into the National Health Service (NHS) in the late 80s. RecommendationsincludedtheuseofclassificationsystemssuchasICD9,ICD9-CM,andDRGstoprovideclinicalworkload information. This marked the beginning of major structural reforms within the NHS. Their Resource Management initiative introduced a new approach to resource management within the NHS aimed demonstrating measurable improvements in patient care. The UK now uses Healthcare Resource Groups (HRGs) which represent aUKmodification ofDRGs.Other countries includingNewZealand,Canada andSwedenhave experiencedsimilar major reforms to their health system. Canada uses Case-Mix Groups (CMGs) as its output measure. These andsimilarpolicyinitiativeshavehadasignificantimpactuponhealthinformationsystemdevelopmentandthediscipline of health informatics.
31/JNU OLE
3.3 Philosophical Aspects There is a growing realisation that social structures, the economic, social, occupational and environmental circumstancesofindividuals,methodsofhealthservicedeliverypluspublichealthmeasures,greatlyinfluencetheincidenceofdiseaseandillhealthepisodesandthequalityoflifeexperienced.Diseaseandillhealthmaybedefinedby the prevalence of physical, social or psychological problems experienced. Medical interventions are designed to respond to the physical aspect of ill health and to a lesser extent to the mental aspect of ill health. Health outcomes, as measured by the general health and well being of a population or the impact of disease or ill health upon daily living, are determined not only by the possible underlying disease or medical interventions but also by the management of the response to these problems within the context of the whole person in their environment.
Thus a population’s health is not a discrete domain of medical practice. According to Harper et al (1994 p.11) health dataservethreebroadpurposes,todefinetheproblem,tounderstandtheproblemandtheidentificationofeffectiveinterventions, preventative and curative.Thepolitical influences andfinancial considerations togetherwith anunderlying desire by Governments towards a philosophy of a health service delivery system which has a primary health care focus are driving health care services away from institutional care towards community based care. This reorientation of the health care system from a medical model of health care towards a social model began in 1977 at the 30thWorldHealthAssembly,followedbythe1978DeclarationofAlmaAta;the1986OttawaCharterforHealthPromotion;the1988AdelaideConferenceStatementonHealthyPublicPolicyandthe1991SupportiveEnvironments for Health: The Sundsvall Statement.
Australia is a signatory to the Global Strategy for Health for all by the Year 2000, thus accepting international obligations. Thus increasingly more health services are expected to promote health and there is an expectation to involve the community in health care decision making. Health care services required for any one episode of care may be provided by any number and combination of community and institution based services. Consequently there is a greater need to inform the community about health related concepts and interventions and to make provision forthecontinuityofcare.Thishasmajorimplicationsforhealthinformationsystemsincludingdatadefinitionsand collections.
3.4 Technological Advances Advances incomputing,communicationsandmedical technologiesareexplosive. It is increasinglydifficult tokeep up with the enormous volume of new knowledge created by medical advances and needed for the purpose of informed decision making. Medical advances are forcing changes in attitudes and values regarding the sanctity of human life, creating many dilemmas associated with resource allocation. Much is possible but is it worth doing? Computing and communications technological advances on the other hand are making what wasn’t realistically possible previously more feasible, cost effective and in some instances common place. High performance computing andnetworkingtechnologyplusadvancedsoftwaretechnologyandalgorithmswillprovideenormousbenefitstohealth care in the areas of research, imaging and telemedicine. Communications technology needs to be embraced to ensure continuity of care as health care recipients move through the system and are serviced by any number of providers during any one episode of care.
3.5 Health Information Science The communication of information is fundamental to healthcare. In pre-history, knowledge and skills were passed from healer to apprentice by talking and example. Early cuneiform writing on clay tablets record some medical techniques and remedies. In more recent times, medical books have documented an accumulating human knowledge. Currently, journals, magazines, books, proceedings and pamphlets deliver a daily avalanche of written healthcare information,whileaudioandvideotapes,radio,television,CD-ROM,video-discsandfilmsproduceamountainof audio-visual material.
There is a well established communication between healthcare providers, between the nurse and the doctor, the doctor and the pharmacist, the radiologist and the pathologist, and so on. A healthcare system must also be managed and funded.Thisrequiresaflowofinformationfromthehealthcarerecipientandtheprovidertovariousorganisationsfor fund and resource allocation, and for management.
Health Informatics and Management Information
32/JNU OLE
All the above information is small compared to that which passes between the recipient of healthcare and the provider. This intercourse contains the daily application of healthcare. In it, and too often hidden, are the clues to new diseases, complications and interactions. Some clues are recorded. They form actual or potential food for researchers.
Healthcare is about people and mostly one-to-one relationships between recipients and a provider. However, the domain is steeped in information and its management. In this, technology will have an ever increasing role to play.
There is no point in applying information technology unless advantages result which outweighs any associated disadvantages.Letusbrieflyconsidersomeoftheseandthebuildingblocksrequiredforadvancestooccur.
3.6 The Communication of Medical Information and its Management The following explains attributes of communication in different ways in health informatics.
3.6.1 Communication with Literature The overwhelming volume of printed healthcare information has, from the turn of the century, been indexed in libraries. In recent years, these indices have been created and stored on computers. The key concepts within the text areidentifiedandnamedaccordingtoastandardisedlistofterms.Onecontrolledvocabularyusedforthispurposeby the National Library of Medicine (NLM) in Washington DC is called MeSH (Medical Subject Headings). It evolved for computer use from Index Medicus, the original list of terms used to index a catalogue of the publications in the US army medical library. It was compiled and published by Surgeon General Dr John Shaw Billings, in 1879. Some medical and other health related literature is indexed using a different vocabulary, for example the Library of Congress Subject Headings (LCSH), and the Cumulative Index to Nursing and Allied Health Literature (CINAHL). These and others are discussed in greater detail in another chapter.
The volume of new written material has long been far beyond any one person’s capacity to read, let alone learn and apply. The challenge for information technology is to present relevant information to the healthcare worker when it is needed. For example, if combinations of disease and medications have potential side effects, then the provider should be warned of these at the moment of prescribing. For this to occur, an up to date database of drug interactions must be provided to the computing industry. The electronic medical record must also record a person’s details in terminology equivalent to that used by the database. In the future, the literature may be searched (in a semi-automated process) according to the contents of a person’s electronic medical record. This would save the provider compiling searches, and would thus save time and effort. The major obstacle to be overcome before this is a reality is the difference in terminology used by the healthcare provider and the library indexing system.TheUMLS (UnifiedMedicalLanguageSystem, a research projectsponsored by the NLM) is attempting to provide a solution. All people will inevitably have greater access to current literature and databases. Searching will be easily done from the home computer or local library. Some more aware patients will result. An informed recipient of care is a two edged sword more able to self-care, but more demanding of new investigations, therapies and procedures. To avoid increasing costs, coordinated education programs may be needed.
Thus requirements for improved literature communication are: Increased awareness of the existence of available resources •Wider use of computers •Unificationofhealthcareterminologies•Improved searching programs •Educational programs which improve user interpretation of the literature •
33/JNU OLE
3.6.2 Communication between Providers Healthcare is very much a team game. Communication between players is constant - between general practitioners, physicians, surgeons, pathologists, radiologists, nurses, pharmacists, therapists, lawyers and many more. The essence of any communication should be recorded. The background history of the person concerned, and a summary appropriate to the provider is usually required. The management of a person seeking care can evolve into a complex round of repetitive forms and letters. With each communication, the risk of inaccurate information increases. If there is a coordinator such as a general practitioner, or a case manager from a hospital, or other health care agency who compiles and collates all documents into a person’s record, then this record can become a confusing collection of difficulttofinddocuments.Itsusefulnessdeclinesasitsthicknessincreases.
Electronic communication between members of the team such that each has a view of, and some access to a person’s medical or health record, would save time, increase accuracy, and result in better management. In general terms, asthenumberofpiecesofpaperarereduced,sotheefficiencyincreases.Thepharmacist’sprescriptionshouldbean electronic message sent directly by the doctor to the pharmacist. Likewise the laboratory and radiology requests and reports should not involve paper. For this to materialise:
Providers must use computers. •The terminology used by each provider must be consistent and universally understood. •All involved must agree as to what will be transmitted. •An adequate communications network must exist. •Each network node must adhere to standardised message protocols. •Adequatesecurity,confidentialityandintegritysafeguardsmustexist.•The provision of up-to-date information resources in a standardised form which are computer understandable. •
3.6.3 Communication with Organisations Current communication with funding and resource management organisations involves a complex paper trail with an occasional interspersed computer. Medicare slips, discharge details, workers compensation forms are posted by the millions. Wishes, advice, warnings, demands, rules and regulations issue forth from administrative and professional organisations or associations to healthcare providers, on pieces of paper, brochures and books. Muchofthistrafficcouldbereplacedifahealthcarenetworkofprovidercomputersexisted,andeachcomputerunderstood the concepts or facts used by the other. Wishes, advice, warnings, demands, rules and regulations could be composed in a computer understandable way, such that when appropriate, the provider would automatically be advised, prompted or warned. Electronic fund transfer is already well established (for example,EFTPOS). It will inevitably be used by the healthcare industry. For these things to eventuate the same conditions listed previously as required for electronic communication between members f the health care team apply.
3.6.4 Communication between Provider and Patient The role of the front line providers of healthcare involves listening, questioning, examining, provisionally diagnosing, investigating,confirmingthediagnosis,caring,supporting,providing,educatingandtreating.Thefactsgleanedandthe events which ensue must be recorded. These are required:
for accurate management and resource allocation and•for future reference by a person’s current provider or future providers, and •for potential medico-legal requirements. Traditionally this record is the written medical record•
Medical records are certainly the hub of information management for each recipient of health care. They should form the hub of the entire healthcare system and possibly become health records. However, in their written form they are generally speaking illegible, disorganised, inaccessible, mislaid, and impossible to quickly digest. They offer to the provider, no timely, useful and current medical information. No prompts. No warnings. They cannot be easilycommunicated(inwholeorinpart)toothers.Ontheotherhand,theyareasconfidentialastheinverseoftheir understandibility. They are cheap to initiate, and are created in a medium familiar to all.

Health Informatics and Management Information
34/JNU OLE
There is a real potential for information technology, if applied to the medical record, to change the health service. Goodinformationmanagementdemandsthatdataarerecordedonceonly,bythepersonbestqualifiedandatitssource.Thus,forexample,theofficesecretaryshouldenteradministrativeanddemographicinformation;thedoctorthemedicalhistory,examinationandorders;thenursethedailyobservationsandevents;thepathologist(ortechnicianorautomatedanalyser)thelaboratoryresults;theradiologiststheinterpretationofx-raysetc.Transcriptionofdatashould not occur.
In the Australian environment of unconscripted and unregimented private healthcare providers, the EMR must be desired by potential users if it is to succeed. This means it must offer the provider advantages over the competing alternative pen and paper system. It must generate less tedium, more speed, timely and current clinical information and, diagnostic and management assistance. It should prompt the provider so as to avoid excesses and omissions. Automated case summaries and views of any aspect of patients’ previous records should be available. Form and letter generationshouldbesemi-automated.Itshouldmanagefinancialmatters.Itshouldbeaccurate,secure,accessibleyetconfidential.
Thefollowingmustcometogethertoenableasignificantimprovementinhealthcareinformationmanagement:Healthcare terminologies:Consistent healthcare terminology, and standard coding and classification of•concepts. Resources: Computer understandable, current, useful and useable information, data and knowledge resources. •Computing: Adequate computing hardware, and software development tools •User interface & data capture: Optimised user interface and data capture methods. •Electronic communications: Adequate electronic communications. •Safeguards:Adequatesecurity,confidentialityandintegritysafeguards.•Benefits:Theremustbebenefitstoallconcernedtothecomputingindustry,thehealthcarefundingorganisations,•the healthcare providers, and to the patients.
Let us now glance at each of the components necessary for improved healthcare information management. Several of the topics will be considered at length in other chapters. This chapter is designed to offer an overview of the “science” involved. This should help in the formation of a perspective of the subject.
3.7 Healthcare TerminologiesThe following explains the healthcare terminologies
3.7.1 Components of a Terminology As we have seen, there is a need to describe healthcare concepts in a consistent manner. We, as humans, are able to assimilate, without confusion, many variations of description. Computers, on the other hand are very poor at recognising concepts from inconsistent descriptions. To manage this, a standard list of terms is collected and divided into preferred terms and alternative descriptions (or synonyms). For example, the preferred term “sub acutethyroiditis” could have as its synonyms “de Quervain’s thyroiditis” and “granulomatous thyroiditis.” Within anyterminology,thepreferredtermsshouldbeunique;howevereachpreferredtermmayhavesynonymswhichare shared with other preferred terms. For example, “cold” could be a synonym for both “hypothermia” and the common viral infection “coryza.”
The preferred term is an agreed short description of a concept. A concept is the image created by the words which describeit.Adefinition,oftheconceptmaybeneeded.Toooftenthewordingofthepreferredtermmeanssomethingdifferent to different users.
As healthcare is ever-changing, the preferred description of a concept may change. For example, an international terminology has recently changed the preferred term “maturity onset diabetes mellitus” to “non insulin dependent diabetes mellitus.” The concept has remained unchanged (i.e. the disease is the same).
35/JNU OLE
Auniqueidentifier(orcode)foreachconceptisrequired.Anythingwoulddoaslongasitisuniqueandsuitable.Ifthe preferred term is used, its description could not change. As we have seen, this can happen. Thus the preferred termisnotsuitableasacode.Infact,wordsarenotefficientwaystostoreidentifiersincomputers,asthecomputermayberequiredtostoreanidentifiermanytimes.Thecodeshouldthusbereasonablycompact-a“number”ofsome sort. It need not be seen by users, as the computer can always display its equivalent descriptive words. The process of matching a healthcare entity to a term in a terminology and assigning a code to it is called coding.
The terminology may be called a coding system. Some terminologies or coding systems describe themselves as (a) a“controlledvocabulary”suchasMeSH(NationalLibraryofMedicine1994)),(b)a“classification”suchastheInternationalClassificationofDiseases9thRevision(ICD9)(WorldHealthOrganisation1977),ICD9withClinicalModifications(ICD9-CM)(CommissiononProfessionalandHospitalActivities1978),InternationalClassificationofProcedure Codes (ICPC) (Lamberts & Wood 1987)), or (c) a “nomenclature” such as the Systematised Nomenclature of Medicine (SNOMED) (Cote & Robboy 1980).
Sometimes rules are offered to improve the accuracy of coding. These instruct the user to consider certain other concepts under various conditions.
Thus far we have seen that a terminology is composed of a code, a preferred term to describe each concept (ideally defined),andvarioussynonyms.Rulesmaybeprovidedtodirecttheuser.
3.7.2 Classifications, Hierarchies and Terminologies Knowledge enables us to refer to something and unconsciously all related things come to mind thus if we consider the concept of “appendicitis” we think of those conditions which we have learnt are included, for example “acute, sub acute, chronic and relapsing appendicitis.” We also know that “diseases of the large intestine” include appendicitis. Thisorganisationofconceptsintogroups(orclasses)suchthatonegroupincludesothersiscalledclassification.The resulting structure can be visualised as a branching tree (perhaps turned up-side-down!), and is described as a hierarchy (for which the adjective is hierarchical). When the concepts of a terminology are arranged to form a hierarchy, some concepts, by their nature, will be found to belong in more than one place.
Forexample,“tuberculosisofthelung”isbothan“infectiousdisease”anda“lungdisease.”Anotherfinding,whenbuildinghierarchies,isthatconceptsbelongindifferentclassesdependingonthecontextoftheclassification.Forexample,varioustypesofapplescanbeclassifiedaccordingtotheirsize,colour,ortimeofripeningetc.andeachgrouping would be different. Many healthcare concepts can have multiple hierarchies. For example, “bleeding disorders” include some diseases from “congenital, infectious, allergic, nutritional and metabolic” conditions, and each of these groups of conditions belongs to a hierarchy of their own.
Thepracticalimportanceofclassificationsorhierarchiesisintheirabilitytoincludeallsubordinateconcepts.Theycan thus specify the detail (or granularity) of the data.
An organisation may need to know how many operations were performed, while an association may be interested in the number of hysterectomies. If the obstetrician records the details of each type of hysterectomy, using an appropriate terminology, then the less detailed requirements of the association and the organisation can be automatically supplied by utilising the hierarchy of the terminology.
Information resources which can be harnessed by healthcare computing systems need to be able to include various groupsof concepts.For example, if the indications for ablood test are required, and theyare specified in theresource as “bleeding disorders,” the hierarchy of the terminology should be able to determine which conditions are included in the concept “bleeding disorders.” As computing systems become “smarter,” their internal use of hierarchies increases.
Health Informatics and Management Information
36/JNU OLE
Specifying hierarchies in terminologies Aclassificationorhierarchymaybespecifiedbyanumberingsystem:
2 level one concept (for example,“diseases of the large intestine”)•27 level two concept (for example,“appendicitis”)•271 level three concept (for example,“acute appendicitis”)•272 level three concept (for example,“chronic appendicitis”)•273 level three concept (for example,“relapsing appendicitis”)•
In this example there can only be ten concepts at any level. This method is used by ICD9 and ICD9cm systems.
Note: A hierarchy can be described in terms of parents, siblings, and children. In the above example, the parent of “appendicitis” is “diseases of the large intestine.” The children of “appendicitis” are “acute appendicitis,” “chronic appendicitis,” and “relapsing appendicitis.” The siblings of “chronic appendicitis” are “acute appendicitis,” and “relapsing appendicitis.”
By allocating several digits to a level, more space can be reserved (for example,200700100, where 100 concepts canoccurateachlevel).Theresultingstringofcharactersmaybeinefficientandunwieldy.
Another method is to count using the base 16 (hexadecimal), and the numbers 0-9 and A-F. This compacts the string of characters, but lack of room between levels may continue to be a problem.
Furthercompactioncanbeobtainedbyusingthecharacters0-9,A-Z,anda-z,makingabout58levelsbetweeneachcharacter (confusion between the numbers one and zero and upper and lower case “o” and lower case “l” (el), may need to be avoided). This method is used by RCC-1 and RCC-2 (Computer Aided Medical Systems 1993).
Another approach is to use a series of numbers of any size each one of which is separated by a delimited character (for example, “D.12.98.21.7”). This method is used by the “tree numbers” of MeSH (National Library of Medicine 1994).
Itispossibletospecifyhierarchiesinacomputerfile(ortable).Twofields(orcolumns)arerequired,onefor“theconcepts,”andtheotherfor“theparentofeachconcept.”Bydirectingthecomputerinitssearchofthisfile,theparents, siblings and children of any concept can be determined. Repeated searches allow the full hierarchy to be displayed. Multiple hierarchies can be represented. A concept is simply given more than one parent. Certain cyclic references must be forbidden (for example, a concept cannot have itself as a parent). This computing structure (or graph) is called a “directed acyclic graph”. It is used by RCC-3 (Computer Aided Medical Systems 1993).
Single and multiple axes and terminologies Healthcare concepts can be expressed by concepts from a single list (or module or axis), however this list becomes extremely long, as more clinical detail is coded.
Consider the diagnosis of “acute infection of a bone.” The site of the infection will be required and will need to be coded. Thus, there needs to be a list of concepts for “acute infection” of “each part” of “each bone” in the body. Now consider a diagnosis of “fracture.” Again the bone will be required. An additional list of “fractures” to “each part” of “each bone” will be required. Thus two complete lists of sites for two diagnoses results.
Another approach is to use multiple axes, and combine them. Thus, if there is a single list of “site” codes containing the bones and their parts, then this can be combined with the code for “acute infection” or the code for “fracture” to form compound codes. Thus one complete list of sites can be used for all diagnoses.
The need to combine axes may be even more apparent when considering a laceration, an abrasion, a bruise, a rash, or an itch, to any part of the body.
37/JNU OLE
The more atomic approach of combining elements from various axes to form compound codes, requires the definitionofextensiverulesorrelationshipstoavoidthepossiblegenerationofnonsense(forexample,a“fracturedeyebrow”).
Qualifiers (or modifiers) and terminologies Somesystemsofferqualifiers.Thesearemodifyingconceptswhichcanbelinkedtoachosenconcept.Theyenableincreasedclinicaldetailtobecoded.Ineffectqualifiersareanadditionalaxis.Iftheycanbeassociatedwithonlyspecifiedconceptstheycanbecalledlegalqualifiers-otherwisegeneralqualifierswouldbestdescribethem.Forexample,legalqualifiersforbacterialagentsusingtheSNOMED-2terminologyare:
“0=nototherwisespecified”•“1 = growth present” �“2 = growth absent” �“3 = growth contaminated,” etc. �
Thequalifiercodenumber(forexample,“1”)isaddedtotheconceptcodenumber.(Forexample,ifthecodefor“actinomyces israellii” is “E10730,” then “E10730_1” would specify “actinomyces israellii growth present.”)
Mapping terminologies Therehaveevolvedseveralcodingsystems.Eachhasbeendesignedforitsspecificpurpose.ForexampleICD9cm(InternationalClassificationofDisease,9threvisionwithclinicalmodification)isusedbyhealthcaremanagerstocode hospital discharge diagnoses and procedures which may then be grouped to become diagnosis related groups (DRGs).TheMedicareBenefitSchedule(MBS)(AustralianGovernmentPublishingServices1994))isusedbydoctors to code their procedures for payment claims. MeSH is used to code the contents in biomedical literature in the National Library of Medicine, Washington DC. There is often a need to translate or map or cross reference the codesfromonesystemtoanother.Iftheabovesystemsweremapped,aprocedureidentifiedbyaMBScodecouldbe also described in terms of ICD9cm for the hospital manager, and MeSH for literature research. Some coding systems offer mappings to other systems. Maps to ICD9cm are virtually mandatory for hospital coding systems in Australia and the USA.
Mapping one terminology to another is not an easy task. Various types of cross references result. Terms are found whichareexactmatches,whileothershavethesamemeaningusingdifferentwords,somearelessspecific,andsomemorespecific,othertermsdonotmatchatall.
TheUnifiedMedicalLanguageSystem(UMLS),asmentionedearlier,isanattempttodevelopaterminologyinterfaceto biomedical literature, healthcare records, health related databanks and knowledge bases in the USA. The UMLS has developed a Metathesaurus (Sherertz et al 1989), a Semantic Network (McCray 1989) and a Resource Map (National Library of Medicine 1990). These enable a single query to obtain information from multiple data sources. The Metathesaurus is a large compilation of several terminologies which are mapped to MeSH. The Semantic Network consists of hierarchies of “semantic types” which have heritable relationships. They form a network. Examples of these relationships are: “is a,” “exhibited by.” “Carried out by.” “forms,” “is an evaluation of .”, etc. The Resources Map supplies the information required to access various data sources.
Subsets and terminologies Healthcare terminologies are large. They often exceed 100,000 terms. Their use requires a coding process. A few words, or beginnings of words, are typed into a computer and used to search the terminology. A list results, from which the user picks the most suitable preferred term. If the entire terminology is searched every time, the resulting list may be long and contain many terms which are obviously unwanted, for example a medical practice is unlikely torequireveterinaryterms.Thecontentsofaterminologycanbeidentified(bytheuseofasimplescoringsystem)to show the concepts more likely to be used in various contexts. Application programs (for example, medical record systems)canthenusethecontextscoretoreducethesizeofpickinglists.Thus,forexample,ifaterminologyidentifiesits concepts for age, and the age of the patient is known by the computer, then only those terms appropriate for the ageoftheparticularpatientneedbelisted.Togiveaspecificexample,ifthepatientisanadult,and“penicillin”isrequired, paediatric versions of penicillin could be omitted from the initial list of options. Likewise, female diseases and operations should be omitted from lists when the patient is a male.
Health Informatics and Management Information
38/JNU OLE
The context scores applied to terminologies can include the type of provider (for example, nurse, general practitioner, surgeon) the component of the task in hand (for example, history, examination, diagnosis, investigation, procedure, medication, operating theatre reports, midwifery reports, etc.), and the race, age, and sex of the patient.
The scoring system can enable picking list to be graded to show “the probable,” “the possible,” “the improbable” and “the lot, regardless.”
Usage frequency may dictate the picking list. Systems may thus learn-as-they-go. This is achieved by scoring the frequently used terms so they sort to the top (where they are more accessible). This process may be made user specifici.e.thosetermsmostusedbyaparticularuser(provider)canbeshownfirst.
The application program should consider the previous history of the patient, and attempt to present previously used terms. Thus presenting lists of terms appropriate for the provider, the recipient of care and the task, can be a non-trivial undertaking. Some systems offer micro-glossaries (SNOMED (Cote & Robboy 1980)) or specialty subsets (RCC-3), subject types (RCC-3), sorting numbers. (RCC-3) (Computer Aided Medical Systems 1993), Sex and age groupings (ICD9cm (Commission on Professional and Hospital Activities 1978)).
3.8 Resources Information resources are essential ingredients of any quality healthcare information management systems. It is generally beyond the scope of system builders and vendors to generate and maintain these resources. Bodies with the appropriate authority and domain expertise are required for their creation. They need to be supplied in a form that is predictable and readily useable by the system developer, and potentially useful to the end user. Examples of resources include:
Library contents containing indexes of authors, and keywords and text of the contents (all or a summary) of •each publication. Medicines data which enable items to be searched from several aspects (e.g., generic name, brand name, •composition, indications, contraindications, interactions, side effects, etc.). Drug and disease interaction warning, descriptionandexplanationdatafilesarerequired.Defaultvaluesusefultotheprescriberareessential.Promptsto remind the user of current rules and regulations are valuable. Laboratory data, which provides information about available tests, their indications, alternatives, costs, •requirements, availability, default values, prompts and warnings. Procedure data which describes each procedure in a manner suitable for the patient (using lay language), the •provider (using professional language), and the account (a shortened form). Indications, contraindications, default values, prompts and warnings should supplement the usually extensive instruction text. These should enable the provider to be prompted and helped at the moment of recording a procedure. They would reduce the time spent on the study of organisational and healthcare rules, regulation, preferences, or advice. Provider data, which list healthcare resources and providers, what they do and their contact details. •Management protocols which remind the user of the preferred management for a disease or situation. •
Theaboveresourcescanvaryfromsimpletextdatafilestoknowledgewhichcanbeutilisedbyacomputer.Therepresentationofknowledge(knowledgerepresentation)isacomplexfield,anddiscussedlaterinthisbook.Iftheknowledge is mixed in with a computer program it is called hard coded, and maintaining it becomes impossibly difficult.Theknowledgeshouldbeinaseparateknowledge-base,wherenon-programmerswhoareexpertinafieldmay create and change it. It may be presented in a knowledge frame. The knowledge is represented using a standard hierarchical terminology, and carefully thought out rules. These usually take the format of “if this, then that or else something.” The creation of these rules requires expert domain knowledge and the help of a knowledge engineer. Often the logic of the rules is expressed in terms of probability or likelihood, requiring a numeric scoring system (for example, 0-4). It is thus somewhat fuzzy hence the term fuzzy logic. A computer program (or engine) is specially designed to utilise the knowledge in the knowledge base. The required answer may have to be deduced or inferred from the rules and their fuzzy logic. A knowledge base or expert system is thus driven by an inference engine.

39/JNU OLE
Healthcare providers are constantly making decisions about the management of an individual’s health care. The numerousfactorsrequiringconsiderationmakethetaskdifficult.
Any system which aids in the decision process can be called a decision support system. For example the timely presentation of relevant information in an easily understood form can help a graph for instance, or a case summary. Thus, the optimal organisation and presentation of data is a large component of a decision support system. They may also contain extensive expert knowledge and apply this to give results which rival that of a panel of experts. These concepts are discussed in more detail in another chapter.
Some computer diagnostic systems are designed to present a list of possible diagnoses based on a given history, examination and results of investigations. The differential diagnosis is shown in order of probability. An explanation as to why each diagnosis is included is available. Some of these systems are able to tell the user what is the best thing to ask or do next. They may consider the risks and the costs. They are useful training systems, but are no match for an experienced clinician. Their future may be to run in the background of a system, and provide helpful messages when it is appropriate, or when called upon.
The electronic medical record is destined to evolve from a relatively simple database of coded events and facts, to an information resource centre and decision support system. As its complexity and expert knowledge increases, its ability to be created and maintained by one author or organisation will decrease. It may have to be built from modules (or be modular in design). Each module would be created and maintained by an organisation which has the necessary expertise. Modules could “plug into” a basic database system. They could be called, have messages passed to them, and return results to the calling system i.e. the basic database system. For this to occur, agreed communication protocols and message standards must be established. These may be proprietary standards, or a national standard. The latter is preferable, but usually later in coming. Each of the above resource examples could be a module.
3.9 Computing Adequate computing hardware (the boxes and touchable parts), and software (the programs) must exist before computers can be used to their potential. The hardware manufacturers provide computers which can do many things. An operating system is used to make the hardware “go.” A programming environment which contains development tools, allows the system designer and programmer develop application programs. These are sold to the public.
The evolution of programming environments and development tools has enabled complex programs to be written in a relatively short time and at little cost. This evolution will effect healthcare information management. It is a reasonable thought that doctors create their own simple electronic medical record systems using a modern database environment. Doctors and nurses in hospitals are now able to create their own prototype systems. The development and demonstration of their requirements is invaluable to the system designer.
3.9.1 User Interface and Data Capture The appearance of the computer screen, where things are, how they function and what happens next, can be described as the human machine interface, or user interface. It is a vital part of quality software, and is, in a way, an art-form and a science. If all else is equal, the interface sells the product. The design should be such that things are where expected, and happen as expected. This is called intuitive design. It involves human dynamics, taste and consistency of presentation. A well designed interface can greatly reduce the time taken to learn how to “drive” an application program. Help is usually provided in a manual. The better the software, the less the manual is used. Helpful instructions on the use of the program are provided by on-line-help. This should be context sensitive (i.e. the help changes in accordance with the computer screen or screen object).
Computerised healthcare information management requires that data be captured by the computer. This is traditionally done via the key board by typing. This can be fast, accurate and quiet. However it does require keyboard skills. A pointing device is helpful and enables (by a “point and click and drag” action) the selection of an object or a part of the screen. Pointing devices include the mouse, trackball, drawing pad, joy stick and touch sensitive screen, etc.
Health Informatics and Management Information
40/JNU OLE
The chore of typing can be greatly reduced by the automatic entry of “what is probably required” (for example,“today’s date”inadatefield).Theseprobableanswersarecalleddefaults.Complexandintelligentdefaultsmaybeprovided.These can greatly improve data capture accuracy and speed. For example, the list of medications used by a particular patient would make sensible defaults for the medications possibly required at each consultation, (as a repeat of a previous medication is a frequent event).
Complex management protocols can be designed to improve data capture, reduce typing, improve accuracy, and improvemanagement.Userdefinedprotocolsandresourceprotocolsshouldbe(orwillbe)afeatureofanyelectronicmedical record system.
Data may also be captured by the computer analysis and recognition of handwriting and the spoken word (speech recognition). These methods require much computing power, are inaccurate, and are currently in their infancy. Some systems however show promise. The smaller the vocabulary, better are the result. Systems can be designed so at any time only a small vocabulary is required, yet the total vocabulary is large.
Bar-coding is widely used in non-medical arenas. It is very easy to create the bar-code equivalent of any text. Reading the printed bar-coded text back into the computer, with the use of a wand, is just as easy.
Printed text may be captured from an electronic copy of the document (via a scanner) and the application of optical character recognition (OCR) software.
3.10 Electronic Communications Adequate electronic communications are necessary. More details regarding data communications, standards and privacy issues are provided in other chapters. Some basic requirements are listed here:
Physical connection between hardware apparatus. Cables are commonly used (telephone lines, twisted pair, •co-axial,opticglassfibretransmittinglaserlight).Raysarenotuncommon(infrared,radioandmicrowaves).Organisation and infrastructure. Hardware joined together forms a network. If the area involved is local (for •example, a hospital), then a local area network is formed. If the connections involved a wide area, then a wide area network is the result. Sometimes the data involved resides on a central computer to form a central database. It is possible to distribute the data so parts of it reside on many different and widely separated computers. A distributed database results, provided the computer knows the whereabouts of the required data, a distributed database can be made to behave very much like a central database. The creation, organisation, regulation and maintenance of complex national networks represent a major infrastructure. Expansion of these networks or data highways to carry vast quantities of information (for example,a moving picture to every home) has coined the phrase super data highways. Nations are currently negotiating their construction. They will have the capacity to carry all the required medical and educational data for the nation’s healthcare. Standards. An electronic message must be packaged so the network knows who sent it and where it is to go. On •arrival,themessagemustbecorrectlyprocessed.Thisrequiresthatspecificinstructionbeincludedwithinthemessage. Standard message formats and transmission protocols are the essential ingredients.
International and national organisations devote their existence to the creation and maintenance of standards. Without themmuchofourcomplexcivilisationcouldnotfunction.Inthehealthcarecommunicationfield,thefollowingstandards may be encountered:
OSIorOpenSystemsInterconnectionstandards.Thisspecifiesasevenlayeredstructurewithmanyoptions.•Optionsmaybespecifiedtoformanoptimisedprofileforaspecificpurpose.OneexampleisGOSIP.GOSIP,ortheGovernmentOSIProfile,hasbeenspecifiedforpublicsectoruseinAustralia,Europe,andNorth•America. EDI or Electronic Document Interchange is a standard for message transmission. Currently EDIFACT standard •messages are evolving.
41/JNU OLE
EDIFACT, or EDI for Administration, Commerce and Transport is a message standard adopted by the UK and •ofinteresttoEuropeandNewZealandandAustralia.Ithasawelldefinedsetofmessagestructuresandrulesforthedevelopmentofnewmessages.Standardhealthcaremessagesarelargelyundefinedatthisstage.MEDIXorMedicaldataexchangeisalanguagespecificationfortheoutputofhardwareusedinhealthcare.It•has North American origins. HL-7orHealthLevel-7referstotheseventhleveloftheOSIstandard.Itisalanguagespecificationforthe•output of hardware used in healthcare. North America has widely adopted HL-7. It is of interest to Australia andNewZealand.MIBorMedical InformationBus is adefineddata exchangeprotocol to enable laboratory equipment and•computers to be interconnected. ASTM or American Standards for Testing and Materials which has a Clinical Data Interchange Standard •(E1238).
3.11 Safeguards Adequatesecurity,confidentialityandintegritysafeguardsmustevolvewithimprovedinformationmanagement.Securityreferstotheeasewithwhichnon-authorisedpeoplecanaccessdata.Confidentialityreferstotheanonymityof the patient or healthcare provider. Integrity refers to the accuracy of the data.
Asthedataheldwithinasystembecomemoresecureandmoreconfidential,thelessaccessibleitbecomestothosewho have authority to access it. Any system is a compromise. Security is attained by locks (on doors, windows and computers)anduseridentification(bytheuseofpasswords,magneticstripebadges,smartkeysandPINnumbers,security beam emitting badges, thumb print recognition, voice imprint recognition). Once a system has granted access, only that information and those actions allowed by the access code will be made available to the user. Thus anaccountantmayseeallfinancialdata,butnoclinicaldata.Thedataitselfcanbedisguisedbyencryption.Thisprocess jumbles the data according to a formula which contains an access code supplied by an authorised user. The unjumbling process (decryption) can occur only if the access code is supplied. A system of smart keys (using “smartcardtechnology”)andpersonalidentificationnumbers(PIN)canbeusedtoencryptanddecryptdataforsecure transmission.
Confidentialitymayappeartoresult ifonlyauthorisedpeopleaccessdata,andpatientandprovideridentifyinginformation has been removed to create anonymity. However, it is possible to electronically cross match data from several sources and determine with a possibly high degree of accuracy, the name of the provider or patient. Legislation is designed to prevent government authorities unlawfully cross matching data.
Integrity of data involves the accuracy of the data received (for example, from the patient), and the accuracy of its interpretation (for example, by the doctor), and the accuracy with which it is entered into, and stored and transmitted by the computer. Elaborate mathematical data integrity checking occurs as a computer manages its data. During processing, the hardware is unlikely to change data by error without notifying the user. However the program (software) may be instructing the computer incorrectly. To ensure a program acts correctly it must be tested. It is not possible to test a complex program in all combinations of circumstances. Thus, no program is absolutely error free.

Health Informatics and Management Information
42/JNU OLE
SummaryInformation consists of datawhich is: ‘Processedorganised or classified into categories to serve a useful•purpose. NobelLaureateKennethArrowdefinedinformationas‘areductioninuncertainty’.•Information as an intellectual constructs which is subject to constant change.•Information is both resource and commodity but unlike matter and energy is not consumed by use. •In the banking industry data consists of numbers whilst in the health care industry data takes many forms including •numbers, text, concepts (coded data), graphics, images, physiological measures (signals), and sound.Technology has progressed to the point where all types of data, with the exception of smell, may be produced •in digital form it has become feasible to develop fully integrated health information systems.Todefinethehealthproblemonemustbeabletoidentifyanddescribethepopulationorgroupsforwhomthe•problem exists as well as various aspects denoting health status, such as incidence of disease, ill health, and deaths, quality of life, plus functional, emotional and mental health status.Anunderstandingoftheproblemrequiresdatawhichareidentifiedasbeingdeterminantsofhealthsuchas•reasons for occurrence, predisposing factors, causes, access to health care services and risk factors.National Health Information Work Program incorporates health information activities that meet agreed national •priorities and have either a national focus or national implications. TheAIH&Wisdevelopinganationalhealthinformationplandesignedtoovercomeidentifieddeficienciesin•its data collections to support its mission. For example, Harper et al notes that quality of life and most of the behavioural aspects of illness are very poorly described and not available for whole populations. In the United States of America the Agency for Health Care Policy and Research (AHCPR) consists of several •componentsoneofwhichistheOfficeofScienceandDataDevelopmentwhichsupportsandconductsactivitiesdesigned to increase the amount and usefulness of data (such as that from health insurance claims data bases and computer based patient research) for outcomes and other health services research.The Computer-Based Patient Record Institute (CPRI) was established in 1991 following a report by the Institute •of Medicine’s committee for improving the patient record to provide a sustained, coordinated and concentrated effort to establish the widespread use of computer-based patient records.Three factors that determine the characteristics and development of health information systems are economic •considerations, technological advances and changes in philosophies regarding health service delivery.Thestructureandtypeofhealthinformationsystemsdevelopedandimplementedtendtoreflectacountry’s•health care system.
ReferencesHealth Informatics• , [Online] Available at: <http://www.authorstream.com/Presentation/bawells-1264433-health-informatics/> [Accessed 26 November 2012].Health Informatics,• [Online] Available at: <http://www.authorstream.com/Presentation/Opluviose-1404677-health-informatics-presentation/> [Accessed 26 November 2012].2012. • Health Information Technology [Video Online] Available at: <http://www.youtube.com/watch?v=0MfJ3VmoqvE> [Accessed 26 November 2012].2011. • Electronic Health Records: What’s in it for Everyone? [Video Online] Available at: < http://www.youtube.com/watch?v=FAaeCYyAxl0&feature=related> [Accessed 26 November 2012].McSean, T., Loo, J. & Coutinho, E., 1995. • Health Information: New Possibilities, Springer.1997. • Protecting Electronic Health Information, National Academies Press.

43/JNU OLE
Recommended ReadingJohns, M., 2002. • Health Information Management Technology: An Applied Approach, American Medical Records Association.Gartee, R., 2010. • Health Information Technology and Management, Pearson.Johns, M., 2002. • Information Management for Health Care Professions, Cengage Learning.
Health Informatics and Management Information
44/JNU OLE
Self Assessment__________definedahealthoutcomeas‘achangeinthehealthofanindividual,agroupofpeopleorpopulation,1. which is attributable to an intervention or series of interventions’.
The Australian Health Ministers Advisory Council (AHMAC)a. Medical Treatment Effectiveness Program (MEDTEP)b. Electronic Medical or Health Record (EMR)c. The Australian Institute of Health and Welfare (AIH&W)d.
The Australian Health Ministers Advisory Council (AHMAC) focus on __________ because these were chosen 2. because they are of major concern as a result of their contribution to a high level of death, illness or premature loss of life.
environmental diseasea. cardiovascular diseaseb. contagious diseasec. airborne diseased.
AccordingtoHarperetal,__________servethreebroadpurposes,todefinetheproblem,tounderstandthe3. problemandtheidentificationofeffectiveinterventions,preventativeandcurative.
technical dataa. medical datab. senses datac. health datad.
__________ generate less tedium, more speed, timely and current clinical information and, diagnostic and 4. management assistance.
The Australian Health Ministers Advisory Council (AHMAC)a. Medical Treatment Effectiveness Program (MEDTEP)b. Electronic Medical or Health Record (EMR)c. The Australian Institute of Health and Welfare (AIH&W)d.
Which of the following statements is true? 5. The communication of the patient and the doctor is fundamental to healthcare.a. The communication of the patient and the provider is fundamental to healthcare.b. The communication of information is fundamental to healthcare.c. The communication of provider and the funding organisation is fundamental to healthcare.d.
Healthcare is about people and mostly one-to-one relationships between __________.6. recipients and a providera. patient and the doctorb. family and the patientc. doctor and the organisationd.

45/JNU OLE
Which of the following statements is true? 7. Electronic communication between members of the team such that each has a view of, and some access to a. a person’s medical or health record, would save time, increase accuracy, and result in better management.Face to face communication between members of the team such that each has a view of, and some access to b. a person’s medical or health record, would save time, increase accuracy, and result in better management.Verbal communication between members of the team such that each has a view of, and some access to a c. person’s medical or health record, would save time, increase accuracy, and result in better management.Non verbal communication between members of the team such that each has a view of, and some access to d. a person’s medical or health record, would save time, increase accuracy, and result in better management.
Goodinformationmanagementdemandsthatdataarerecordedonly_________,bythepersonbestqualified8. and at its source.
thricea. twiceb. oncec. our timesd.
__________ offers the provider advantages over the competing alternative pen and paper system.9. The Australian Health Ministers Advisory Council (AHMAC)a. Medical Treatment Effectiveness Program (MEDTEP)b. Electronic Medical or Health Record (EMR)c. The Australian Institute of Health and Welfare (AIH&W)d.
The process of matching a healthcare entity to a term in a terminology and assigning a code to it is called 10. _________
codinga. modellingb. software developmentc. technical advancementd.
Health Informatics and Management Information
46/JNU OLE
Chapter IV
Standards in Health Informatics
Aim
The aim of this chapter is to:
explain the concept of standards in health informatics•
elucidate the reasons for developing standards in health informatics•
explicate the standards that are to be developed and why•
Objectives
The objectives of this chapter are to:
explain health informatics standards and information transfer•
elucidate the framework for developing standards•
explicate types of standards formed in health informatics•
Learning outcome
At the end of this chapter, you will be able to:
describe various standards development organisations•
understand the reasons for developing standards in health informatics•
identify the challenges while implementing the various standards in health informatics•
47/JNU OLE
4.1 IntroductionStandards are the key towards facilitating the sharing and exchange of information between departments, health agencies and health workers. They are needed for the information content, language used, database and system architectures to facilitate linkage between systems through an apparently seamless integration of highly distributed systems. This is often referred to as ‘interoperability’. Electronic medical or health records need standards, to index and to catalogue health related information for rapid retrieval and to obtain uniform clinical data for research purposes.Withoutstandards,classificationandcodingsystemsweareunabletocomparethehealthstatus,processesof health care, costs and outcomes between various treatment options, health agencies, regions or countries in a meaningful way.
In industry generally the adoption of standards has resulted in an increase in market opportunities and lower costs for equipment and services to users. In health informatics the widespread adoption of standards is expected to improve the health of the nation’s population at a lower cost by improving the ability of health professionals, public and health service administrators to share and make better use of the information generated.
4.2 What are Standards?Astandardmaybedefinedasaprescribedsetofrules,conditionsorrequirementsconcerningdefinitionsofterms,classificationofcomponents,specificationsofmaterials,performanceofoperations,delineationofprocedures,ormeasurement of quantity and quality in describing materials, products, systems, services or practices. Standards are benchmarks. Effective standards are needed to guide conditions of data access and data usage and to make it technicallyfeasibletoexchangedataelectronically.Thisisaprerequisitetocostefficientandaccuratedatacollectionand storage, which enhances the retrieval of quality health information needed to obtain the correct knowledge on which to base decisions. Information exchange requires standards which provide a mutual understanding of the meaning of the data used. That is a standard language is needed and the context within which health data are collected orotherrelatedinformation,suchasapersonalidentifier,dateandtimewhicharerelatedtoclinicalobservations,must not be lost. Standards may be mandated or be adopted voluntarily.
According to Megargle (1991) the quality of the knowledge thus obtained is dependent upon three factors, reliability, relevancy and responsiveness. This can only be delivered when standards dealing with for example electronic compatibility, character encoding and message structuring, are adhered to by the many different computer environments and software programs which may need to be connected to make for example one hospital network. Standards development for health informatics requires input from discipline experts that is those who need to use the information and knowledge provided by a system. Much of this knowledge now resides in medical records and the health related literature.
4.3 Who Develops Standards?Various health and related professional groups, public and private organisations have established standards for paper based health records, for health information systems, for health service delivery and for the health professions. Many such organisations have also implemented mechanisms by which compliance with these standards could be measured. As the automation of health information and communication technology is progressing it has become more apparent that standards for documentation and electronic data interchange within the healthcare sector are urgently requiredifwearetomaximisethebenefitsofferedthroughtheuseofthesenewinformationandcommunicationtechnologies. The health care sector has special communication needs.
Several organisations nationally and internationally are addressing this issue from various perspectives. Many standards applicable to information and communication technology generally need to be adopted within the healthcare sector.Butadditionalstandardsarerequiredspecificallytomeettheuniqueneedsofthehealthcaresectorespeciallyintheareasofdataspecifications,dataintegrityandsecurity.Increasinglythesearebeingdevelopedthroughthewellestablished standards organisations such as Standards Australia, the European Standardisation Committee (CEN), the Institute of Electrical and Electronics Engineers (IEEE), the American Society for Testing Materials (ASTM), the American National Standards Institute (ANSI), the European Strategic Program for Research and Development in Information Technologies (ESPRIT), the International Standards Organisation (ISO), and many others or through
Health Informatics and Management Information
48/JNU OLE
ad hoc groups such as health level 7 (HL7). In 1991 Mandil (1991) noted that ‘despite progress in recent years, the lack of standards remains a major impediment to technical and international collaboration in health and health informatics’. He went on to say that standards ‘tend to liberate cornered clients but (that) they also increase uses of the technology and hence its clientele’.
European standardisation activities for health informatics began in 1990 when the CEN established Technical Committee 251. Standards Australia established its IT/14 committee on health informatics early in 1991. A Healthcare Informatics Standards Planning Panel (HISPP) was established by ANSI late 1991 to bring together the many standards groups which had been developing medical informatics for nearly a decade. Since then many more activities have taken place. In 1993 CEN’s Technical Committee 251 published a directory of the European standardisation requirements for health care informatics which includes a program for the development of standards. Also in 1993 CEN TC251 and ANSI/HISPP produced a publication detailing the worldwide progress made in standardisation in healthcare informatics. There is considerable collaboration between the various standards organisations. Priorities forstandarddevelopmentareguidedbyconsiderationsregardingfeasibility,userrequirements,medicalbenefits,and economical impact (CEN/TC 251 1993).
4.4 Which Standards should be Developed?Individualneedsforstandardsarebeing identifieddailyandconcurrentlywithactivitiessuchas theAdvancedInformatics in Medicine (AIM) project and the Health Care Information and Communication Network (RICHE) in Europe, the Australian Health Communication Network (HCN), the development of systems to support electronic health records, and with the introduction of new Government policies which aim to provide greater accountability and contain costs. There is consensus that ultimately we will need longitudinal (from birth to death) electronic health records to overcome the problems and costs associated with a highly mobile population, increasing specialisation within the health sector, duplication of data collection, incomplete and inaccurate medical histories, incomplete data for research and policy development purposes. Three years ago Murphy reported that a standard description for the content and structure of an automated longitudinal health record was under development. European countries and the United States of America have allocated millions towards standards development in recognition of this need. It is postulated that accurate and complete information will lead to improved knowledge, better decision making, improved quality of care, less cost and better use of available resources.
Gabrielli(1991)identifiedthreereasonsforwhythemedicalrecordwasslowtobeautomated.Thefirstisbecauseof the extensive use of narrative text, secondly because of a lack of a standard medical terminology and thirdly the lack of a medically useful taxonomic code scheme. As a result he notes that clinical experiences are available to others only via expensive research studies, manual monitoring of the quality of care is labour intensive, and health care policies are more intuitive than fact driven.
4.5 Adoption of StandardsThe adoption of standards may be mandatory or voluntary. Various types of standard exist. This is based on who has developed or adopted the standard or the purpose for which the standard was developed. For example many activities are directed towards the development of a common medical (health) language which is the subject of the previous chapter. There are corporate standards developed and used by one company, industry standards which represent the standards used by an entire industry, Government standards such as GOSIP (Government Open Systems InterconnectionProfile)orconsensusstandards.Thelatteraretheresultofinputfromallstakeholdersandarethemost useful but may take years to develop.
The adoption of standards is achieved more rapidly when users or potential users insist that suppliers comply with consensus standards. One of the reasons the health care industry in Australia and possible other countries, is so far behind other industries in this regard is because purchasers have continued to acquire propriety systems. As these vendors are unable to satisfy all health information needs, there is a proliferation of disparate systems and an industry devoted to connecting them with tailor made solutions (interfaces). On the other hand a generic and ultimately more cost effective solution providing faster connectivity is to adopt what is referred to as the ‘open’ solution, which requires only minor adjustments to link machines.
49/JNU OLE
Open systems are those with which other systems can communicate via highly distributed systems. However, the extentofsuch‘openness’appears tovary.Bakker (1994) identifiedfivedifferentmeanings for the term.Opensystems may be characterised by the possibility to communicate with other systems, extract data for external use, import data from external systems in the database, run the system on different hardware platforms or to extend an information system with modules from another supplier. The latter is possible only if different suppliers produce identical modules. Bakker provided an analogy with cars. Both cars and health information systems are made up ofmanyparts,howevertheenginemeantforonecardoesnotnecessarilyfitanother.Henotesthatforsomeoftheessential aspects of openness consensus of users and standardisation are indispensable. Although open systems are highly desirable, the degree of openness, or rather access to various components of such connected systems, needs to becontrolledtomaintainpatientprivacy.Standardsarerequiredspecificallytoensurethatsystemsenableadherenceto privacy and freedom of information legislation, where applicable for system security, and to deter unauthorised access to information. Another chapter is devoted to this topic.
From a user perspective, standards are also required for the user interface. These are emerging slowly. The aim is to allow users to quickly navigate and use any system with minimal training as users within the health sector often need to access a number of different computer applications.
4.6 Health Informatics Standards and Information Transfer: Exploring the HIM RoleHIM professionals need knowledge and tools to advance the use and value of health information. Technology can improve methods to collect, maintain, and transfer patient health information in electronic formats. To take advantage of what technology has to offer, we need to develop uniform practices, common techniques, or standards so that information can be communicated between individuals or points of care with disparate information systems. Institutional and inter-institutional strategies help the HIM industry to move beyond paper to safe, secure electronic methods to exchange health information. Standards development organisations help by offering guidelines and the experience of others for benchmarking change.
4.6.1 Framework for Developing StandardsStandards are models approved by an authority or by general consent and specify hardware or software, communicationsprotocols,ordatadefinitions.Theyaredetailedguidesthataddresshealthinformationandtechnologyfor text, images, instrumentation, and more. We adopt these standards to:
Enable the electronic exchange of data between two or more computer systems by establishing the format •andsequenceofdataduringtransmissiontomoreefficientlyaccomplishinteroperabilitybetweencomputersystemsReflect theexistingclinicalandadministrativedatacontained inbothpaperandelectronicdatasystems to•maintain patient data consistently in growing electronic health record systemsTransfer health data using predictable business processes and accommodate necessary ethical and regulatory •demandsFoster electronic transmission as a business strategy•Promoteefficientinformationsharingamongindividualcomputersystemsandinstitutions.•
Standards are is organised in four general categories: vocabulary, structure and content, messaging, and security. The categories of standards related to information transfer discussed in this practice brief are messaging and security standards and, in particular, selected organisations involved in these standards.
4.6.2 Standards OrganisationsStandards oversight in the United States is managed through the American National Standards Institute (ANSI), aprivate,nonprofitsmembershiporganisationthatservesasaclearinghousefornationallycoordinatedvoluntarystandards, provides information on foreign standards, and represents US interests in international standardisation work. In addition, ANSI is the sole US representative and member of the two non-treaty international standards organisations: the International Organisation for Standardisation (ISO) and the International Electro-technical Commission (IEC)
Health Informatics and Management Information
50/JNU OLE
Standards development organisations (SDOs) address a variety of aspects of health information and informatics. For example, the American Society for Testing and Materials (ASTM) and Health Level 7 (HL7) target clinical data standards. Insurance and remittance standards are a focus of the Accredited Standards Committee (ASC) X12N Insurance Subcommittee. Standards to transmit diagnostic images are developed through ACR-NEMA, also known as DICOM (Digital Imaging and Communications in Medicine). Community pharmacy messages are represented by the National Council on Prescription Drug Programs (NCPDP.) The Institute of Electrical and Electronics Engineers (IEEE), HL7, ASTM, and others develop data models and frameworks.
4.6.3 Mandatory StandardsHistory tells us that legislation and regulation rely on established standards to form the expectations of the industry and the public. Regulatory developments frequently correspond to recognised healthcare standards such as those of the Joint Commission on Accreditation of Healthcare Organisations. Accreditation requirements for the Joint CommissionandtheNationalCommitteeforQualityAssurance(NCQA)callforspecifiedcontentofpatientrecordsaswellascontainpolicyrequirementsforconfidentialityandsecurity.
The most recent and major regulatory requirements for standards applications are contained in the Health Insurance Portability and Accountability Act of 1996 (HIPAA). This legislation and resulting regulations call for data standards in the following eight claims and billing transactions as well as security standards in preparation and implementation of these transactions:
Healthcare claim or encounter•Enrolment and disenrollment in a health plan•Eligibility for a health plan•Healthcare payment and remittance advice•Health plan premium payments•Health claim status•Referralcertificationandauthorisation•Coordinationofbenefits•
The mandatory transaction standards are adopted from the ASC X12N. In addition to these, standards for retail pharmacy transactions were adopted from NCPDP.
Explicit mandatory standards in the area of privacy and security were released in the proposed HIPAA privacy andsecurityrules.ASTMstandardsthataddresspolicyandtechnicalprovisionsforconfidentialityandsecuritygenerally correspond to the privacy and security provisions contained in the HIPAA legislation. Of particular interest in this area are the ASTM standards that address electronic authentication of healthcare information, guides for confidentiality,privacy,accessanddatasecurityprinciples,authenticationofhealthcareinformationusingdigitalsignatures, technical security frameworks, information access privileges and more.
4.6.4 Voluntary StandardsA voluntary consensus process gathers interested individuals from industry, consumer groups, specialty domains, agencies, professional organisations, and vendors to develop a concept and express it in a recommended course of actionorstandard.Then,adocumentisdraftedtofurtherrefinetheconceptandworkthroughdetailsbyaninteractivevoting process to assure that the completed standard has been accorded fair review prior to publishing.
The particular value in this process is that it brings together key players and allows the industry at large to come to agreements. When this happens in ways that further the public good, the federal government tends to look to these standards when regulation needs arise. Even though progress is in evidence in the HIPAA requirements’ application of X12N transactions standards and PCPDP pharmacy transactions standards, voluntary work continues to develop standardsforthebenefitoftheindustryinvocabulary,structureandcontent,messages,andsecurity.Refinementsofexistingpublishedstandardsareongoing;newstandardsareproposedasneedsareidentified.
51/JNU OLE
4.7 Information Transfer and Selected Standards Development OrganisationsMessage format development is addressed by the following organisations: ASC X12N, ASTM, DICOM, HL7, IEEE, and NCPDP. We will consider the following SDOs for their role in information transfer:
ISO: An ISO standard for worldwide communication, the open systems interconnection (OSI) reference model •is designed to organise standards within seven layers to provide a framework that ensures that devices and softwarefromdifferentvendorscanworktogether.Thismodeldefinestherulesfortransmittingdataacrossanetwork. Each layer is responsible for a particular aspect of communicating data. While transmission details for the lower levels may be used across industries and applications outside of healthcare, HL7 has developed standardstoaddressthespecificapplicationlevelforhealthcare.ASC X12N: The ASC X12N Insurance Subcommittee develops and maintains X12 standards, standards •interpretations and guidelines, and UN/EDIFACT* messages relating to personal and corporate insurance, pension funds, medical records associated with insurance administration, state and federal reporting requirements, and reinsuranceadministration.ThesestandardsareidentifiedforusewithHIPAAimplementation.ASTM:Organisedinl898,ASTMpublishesstandardtestmethods,specificationspractices,guides,terminologies,•andclassifications.ASTME1384andE1633StandardCodedValuesforElectronicHealthRecordDataprovidea model for data dictionary development for institutional electronic health records. These standards specify data dictionarydefinitionsandcharacterisationsthathavebeenreconciledwithdataelementsinHL7andX12N.ASTME1869StandardGuideforConfidentiality,Privacy,Access,andDataSecurityPrinciplesforHealthInformation Including Computer Based Patient Records provides explicit direction to policy design in this area. Examples of additional E31 standards subjects are transcription, XML, terminology, personal health records, and technical security provisions.HL7: Founded in l987, HL7 refers to the application level or the highest level of the ISO model for worldwide •communication. HL7 has developed detailed messaging standards, which enable the electronic exchange of data between two or more disparate computer systems by establishing the format and sequence of data during transmission.Theseprovidespecifications forexchanging informationamongcomputer systemsandwhensending information between organisations. The term “HL7 compliant” refers to vendor capability to offer interoperability using HL7 standards and the language HL7 compliance may be included in contract language for commercial vendors.NCPDP:NCPDPdevelopsstandardsthatdefinehowtosendprescriptioninformationfrompharmaciestopayers,•for prescription management services, and for receiving approval and payment information back in near real time. By the late 1990s, more than 90 percent of community pharmacies and nearly 70 percent of outpatient prescription services used NCPDP standards. Like ASTM, this organisation strives to coordinate and work with HL7 and X12N to improve coordination of drug prescription messages of HL7 and billing messages of X12.
4.8 Practical Actions for HIM ProfessionalsHealthinformaticsstandardswillplaysignificantrolesaselectronicdatamanagementincreases.ItisimportantthatHIMprofessionalsmovebeyondgeneralfamiliaritywithinformaticsstandardstospecificknowledgeacquisitioninorder to serve as a professional resource to healthcare organisations. Following are practical steps to consider:
Establishafileonhealthinformaticsstandardsandbegintobuildyourknowledgelevelinthisarea.Becomean•expert on standards that affect patient data and health information business processes. Even though standards are evolving, we cannot afford to defer to others on this topic. At a minimum, understand the relationship and major topic areas for X12N, ASTM, HL7, and NCPDP. Exploring additional standards can follow.Acquire information about the HIPAA regulatory requirements for eligibility, claims processing, and •billing. Become familiar with HIPAA compliance plans and understand how these requirements affect your organisation. Understand the implementation timelines.Investigate the data systems in your organisation that are used in eligibility, claims, and billing processes •governed by HIPAA. Verify HIM business processes that connect to these functions. Determine whether data definitionorformatchangesneedtobeplannedinpreparationforregulatoryimplementation.SeethatrelatedHIM processes are updated as necessary.
Health Informatics and Management Information
52/JNU OLE
InvestigatetheASTMpolicyandtechnicalstandardsforconfidentialityandsecurity.Correlatethesewiththe•HIPAA privacy and security regulations to help develop organisational compliance plans (14). Serve as a resource toyourorganisationforrequirementsonprivacyprinciplesandpractices,patientauthorisation,notification,andother provisions. A recent Health Key Privacy Advisory Group report, “A Framework and Structured Process for Developing Responsible Privacy Practices,” includes tables that compare HIPAA requirements with several SDOs’ recommendations.AccessinformationonHL7andunderstandhowHL7fitsintotheinformationsystemsenvironmentgenerally•in healthcare organisations.Determine if HL7 standards are used in your organisation. Note that although HL7 message standards may be •adopted in your organisation, the manner in which the standards are used can be highly customised so those vendors can accommodate product variability, among other reasons. Investigate how your organisation uses message standards.Keep pace with the healthcare industry’s standards development and professionally endorse these efforts. NCVHS •calls for recommendations to strengthen government roles in standards development and acceleration though funding and agency accountability. The guiding principles for selecting Patient Medical Record Information Standards for NCVHS employ the following criteria:
Improvetheefficiencyandeffectivenessofthehealthsystemfordeliveringhigh-qualitycare �Meet the data needs of the health community, particularly providers, patients, health plans, clearinghouses, �and public health organisationsWillsupportmakingpatientdataavailableintheleastpersonallyidentifiableformpracticalwhenusedor �disclosed for intended purposesWill include strong protections for privacy of patients where applicable �Will be consistent with the other HIPAA standards �
Join a standards development organisation. HIM professionals’ contribution to this work is essential to assure •comprehensive attention to health information business processes. Membership fees are often nominal and progress can be tracked through mailings or through personal participation in development sessions. ASTM meetings are held in conjunction with the American Medical Informatics Association and the “Toward an Electronic Patient Record” annual meetings.
HIM professionals are in a position to reinforce the application of standards in the healthcare community and educate their colleagues about them. Their priorities and emphasis on health informatics standards helps set expectations for health information customers-from patients to providers of all kinds. Standards advocates contribute to the longitudinal viewofhealthinformationwithinandamongsystemsbycallingforunifiedexpectationsabouthowdataisdefined,stored, and transferred to meet the users’ needs. Become an activist in development and application.
The development of standards for use in health informatics is pivotal to more and better use of information and communications technology in the health industry. Considerable progress has been made to date, however the widespread adoption of standards has been slow. Purchasers especially need to include the need for standard complianceintheirsystemspecifications.

53/JNU OLE
SummaryStandards are the key towards facilitating the sharing and exchange of information between departments, health •agencies and health workers.Electronic medical or health records need standards, to index and to catalogue health related information for •rapid retrieval and to obtain uniform clinical data for research purposes.Astandardmaybedefinedasaprescribedsetofrules,conditionsorrequirementsconcerningdefinitionsofterms,•classificationofcomponents,specificationsofmaterials,performanceofoperations,delineationofprocedures,or measurement of quantity and quality in describing materials, products, systems, services or practices.Various health and related professional groups, public and private organisations have established standards •for paper based health records, for health information systems, for health service delivery and for the health professions.Gabrielli(1991)identifiedthreereasonsforwhythemedicalrecordwasslowtobeautomated.Thefirst is•because of the extensive use of narrative text, secondly because of a lack of a standard medical terminology and thirdly the lack of a medically useful taxonomic code scheme.Standards are models approved by an authority or by general consent and specify hardware or software, •communicationsprotocols,ordatadefinitions.Standards oversight in the United States is managed through the American National Standards Institute (ANSI), •aprivate,nonprofitsmembershiporganisationthatservesasaclearinghousefornationallycoordinatedvoluntarystandards, provides information on foreign standards, and represents US interests in international standardisation work.Standards development organisations (SDOs) address a variety of aspects of health information and •informatics.The most recent and major regulatory requirements for standards applications are contained in the Health •Insurance Portability and Accountability Act of 1996 (HIPAA).A voluntary consensus process gathers interested individuals from industry, consumer groups, specialty domains, •agencies, professional organisations, and vendors to develop a concept and express it in a recommended course of action or standard.
ReferencesPractice Brief: Health Informatics Standards and Information Transfer: Exploring the HIM Role• , [Online] Available at: <http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_000024.hcsp?dDocName=bok1_000024 [Accessed 26 November 2012].Standards in Medical Informatics, • [Pdf]Availableat:<http://wang.ist.psu.edu/course/07/IST497/files/CH06-FINAL.pdf> [Accessed 26 November 2012].2011. • Building a successful Health Information Exchange [Video Online] Available at: <http://www.youtube.com/watch?v=ZUhm2VZ8h_8&feature=related>[Accessed26November2012].2011. • The usability (or not) of Health Informatics Standards [Video Online] Available at: <http://www.youtube.com/watch?v=JM-EpHVB_7k> [Accessed 26 November 2012].Moor, G., McDonald, C. & Noothoven van Goor, J., 1993. • Progress in Standardisation in Health Care Informatics, IOS Press. Conrick, M., 2006. • Health Informatics, Cengage Learning Australia.
Health Informatics and Management Information
54/JNU OLE
Recommended ReadingO’Carroll, P., Yasnoff, W., Ward, E., Ripp, L. & Martin, E., 2002. • Public Health Informatics and Information Systems, SpringerRoss, D., Hinman, A., Saarlas, K. & Foege, W., 2002. • Public Health Informatics and Information Systems, Springer.Conrick, M., 2006. • Health Informatics, Cengage Learning Australia.
55/JNU OLE
Self Assessment__________ are the key towards facilitating the sharing and exchange of information between departments, 1. health agencies and health workers.
Standardsa. Technologyb. Computersc. Peopled.
Electronic medical or health records need __________, to index and to catalogue health related information for 2. rapid retrieval and to obtain uniform clinical data for research purposes.
technologya. computersb. standardsc. peopled.
Which of the following statements is true?3. In industry generally the adoption of latest technology has resulted in an increase in market opportunities a. and lower costs for equipment and services to users.In industry generally the adoption of standards has resulted in an increase in market opportunities and lower b. costs for equipment and services to users.In industry generally the use of IBM computers has resulted in an increase in market opportunities and lower c. costs for equipment and services to users.In industry generally the adoption of children has resulted in an increase in market opportunities and lower d. costs for equipment and services to users.
The quality of the knowledge thus obtained from standards is dependent upon three factors, __________.4. reliability, relevancy and responsivenessa. accuracy, clarity and precisenessb. effectiveness,efficiencyandelaborationc. Talent,knowledgeandefficiencyd.
__________ is one of the well established standards organisations in the world.5. The American National Standards Institute (ANSI) a. Medical Treatment Effectiveness Program (MEDTEP)b. Electronic Medical or Health Record (EMR)c. The Australian Institute of Health and Welfare (AIH&W)d.
One of the reasons for the medical records were slow to be automated was the extensive use of __________.6. computer illiterate staffa. expensive computersb. narrative textc. technologyd.
Health Informatics and Management Information
56/JNU OLE
__________ may be characterised by the possibility to communicate with other systems, extract data for external 7. use, import data from external systems in the database, run the system on different hardware platforms or to extend an information system with modules from another supplier.
Open systemsa. Close systemsb. Open-ended systemsc. Close ended systemsd.
Although open systems are highly desirable, the degree of openness, or rather access to various components of 8. such connected systems, needs to be controlled to maintain __________.
discipline a. silence b. cleanliness c. patient privacyd.
Which of the following statements is false? 9. Standards are organised in four general categories: vocabulary, structure and content, messaging, and a. security.Standards are adopted to transfer health data using predictable business processes and accommodate necessary b. ethical and regulatory demands.Standards oversight in the United States is managed through the American National Standards Institute c. (ANSI).Standards for use in health informatics are not important for more and better use of information and d. communications technology in the health industry.
__________ gathers interested individuals from industry, consumer groups, specialty domains, agencies, 10. professional organisations, and vendors to develop a concept and express it in a recommended course of action or standard.
Mandatory standardsa. Voluntary standardsb. Standard organisationsc. Compulsory standards d.
57/JNU OLE
Chapter V
Basic Applications and Expectations
Aim
The aim of this chapter is to:
explain the concept of communicating with the computers•
elucidatespecificapplicationsofcomputersinhealthinformatics•
explicate how information technology can bring about improvements in health care sector•
Objectives
The objectives of this chapter are to:
explain basic applications of computer in health informatics•
elucidate the concept of Graphical User Interface (GUI)•
explicate the importance of word processing•
Learning outcome
At the end of the chapter, you will be able to:
enlist database applications •
understand why information system is necessary in health care sector•
identify the challenges in introducing IT in health care sector•

Health Informatics and Management Information
58/JNU OLE
5.1 IntroductionMost health professionals would agree that computer technology could help most aspects of their work. The problem is in using the computer. The focus of undergraduate and post graduate training is on delivering healthcare. Information management and information technology have had a low priority in this process. Many health professionals complete their tertiary education with little or no exposure to computers.
We are all busy. Keeping up with our professional work and continuing education takes time. Developing computer skillsrequiresacommitmentintime.Gainingashorttermbenefitfromasimpleusefulcomputerapplicationwillenable a new user to maintain interest. From this point skill can be developed further into more serious use of the technology.
Thefirstproblemiscommunicatingwiththecomputer.Inthepastlearningtotypewasaskillreservedforthosemovinginto clerical tasks. Keyboard skills are required to use a computer well. This is rapidly changing. Speech will soon be the major form of communication between the computer and its user. This will break down many of the barriers faced by health professionals in the past. The next problem is what immediate use do you have for computer? If we look at surveys of computer usage amongst medical practitioners the major usage is in the simple tasks. Essentially thischapterlooksatthesesimpletasks.Whatarethey,whatdoyouneedandwhatarethebenefits.
5.2 Communicating with the ComputerThe keyboard and screen is still the major communication vehicle between us and the computer. In the early 1980s we all thought we would be talking to computers before the end of that decade. The task of identifying all the variations ofhumanspeechprovedmoredifficultthanfirstanticipated.Thecomputerhasproblemswithouraccents,withwordsthat are phonetically similar and when minor illness effects our pronunciation. It takes a great deal of processing power to incorporate these variations. Despite the rapid advance in hardware technology it took some time to deliver sufficientpowerinalowcostpersonalcomputerformat.Evenwithspeechrecognitionandtouchscreentechnologynow well established in the personal computer world, keyboard skills are still an essential element.
5.3 The KeyboardThe design of the original QWERTY keyboard is to slow down the user. The frequently used letters are relatively inaccessible.Letterplacementdefieslogictoauserfacedwiththekeyboardforthefirsttime.
The computer keyboard has added complexity. There are at least twelve function keys labelled F1 - F12. These have different roles in different software packages. The only constant is pressing F1 will generate the help information in most software packages.
In addition to the Shift key there is an Alternate (ALT) and a Control (CTRL). These are relatively easy to use. Like a Shift key, they are used with letters, numbers or the function (F1 - F12) keys. They differ from the shift key in that they generate commands to the computer instead of simply placing characters on the screen. The commands vary depending on what computer software package you are using. For instance in a common word processing package Control A generates a command to format all the characters as capitals. In a common database package Control a meanslocatethenextfieldinthedatabase.
In addition to a numeric keypad and arrow (direction) keys there are usually eleven other keys. These are easier to understand. The Enter key is the most important. It tells the computer to accept what the user has typed or to run a particular task offered by the computer. Esc is a favourite key - it means escape out of here. It is particularly important to the new user when exploring the unknown. Pressing escape will return the user back to the previous step or out of the programme. Page up, page down, delete, insert, home and end mean what they say. Print screen, scroll lock and the pause or break are little used.

59/JNU OLE
Combining the Control Alternate and Delete key generates a command used often by the new user. This essentially restarts the computer erasing the current tasks. This re-sets the computer back to the state it was in when it was initiallyswitchedon.Themajordisadvantageisthatonelosesanynewworkcreatedbutnotfiled.Essentiallyallthe keys beyond the standard type-writer keyboard generate commands not characters. Most computer programs give guidance on how to use the extra keys.
5.4 The Mouse and the Graphical User Interface (GUI)Older design software relied on the user learning or becoming at least familiar with the command keys and when to use them. This added greatly to the barrier for the new user. Unfortunately most of the common medical record software has retained this system. With the advent of the mouse it has become much easier to drive modern software.
The mouse and a screen layout called the Graphical User Interface changed the face of personal computing. A Graphical User Interface (GUI) is where the computer software produces pictures and pull-down menus to indicate the choice of commands available to the user. A mouse (or other pointing devices) controls a moving arrow on the screen. The user points at the command and presses a button on the mouse or presses the computer enter key to request that the computer runs the command.
No longer did the user have to learn which keys to press to generate a command. Instead it is available on the screen. “Point and click” reduced the learning time for new users. The Graphical User Interface made it easy for anyone to learn to use a computer.
Touch screen technology was available prior to the common use of the Graphical User Interface and the mouse. Hardware technological development usually precedes software innovation. A sophisticated computer screen can provideinputtothecomputer.Whentheusertouchesthescreen,thescreenidentifiesthelocationofthetouch.The software processes the location of the touch and uses this information to generate a particular response. The computer can then use this information to respond to a command or the input of information.
This is particularly good for situations where non-computer users need to communicate. Shopping centre location mapsandautomatedpostofficesprovidegoodexamplesoftheuseofthisformofinterface.Thedisadvantagesincludetheslowspeeds,thecostofthescreensandthelimitationsofsizeindefiningthelocationofthetouchpoint.Modern electronic diaries have taken this technology to the next stage. They have combined touch screen technology with the Graphical User Interface.
Applewas thefirst toeffectivelymarket theGraphicalUser Interface. Itdidnot take theIBMandcompatiblepersonalcomputerworldlongtoseethebenefitoftheGUIenvironment.MicrosoftdesignedWindowstofilltherole. This is now the major GUI interface around the world.
The real advantage of GUI is that the command format is the same across a wide range of computer software applications.Forinstanceauserwillfindthatawordprocessingpackage,adatabase,acashbookandaspreadsheetalllookmuchthesameinaGUIsystem.Pulldownmenusforfilingnewandfindingoldmaterialarethesame.Common tasks such as the cut, copy and paste editing tools are requested from the same pull down menus across differentpackages.Onceauserhaslearnedbasiccommandsinonepackagetheyfindthattheycaneasilydriveothers.
The GUI controls the printer and printing initiated by any software package. The process of printing is standard from any application running under the GUI. Learning new software becomes a matter of understanding the principles of what it can do rather than learning yet another detailed set of commands.
Having learned to drive a word processing package one can move easily into driving a database or spreadsheet. It is simply a question of understanding what a database is and how it can help you. Prior to the GUI it would take many weeks of use to learn to drive a database even when the concepts were understood. Today it may take one to two days to get to a level of reasonable productivity.

Health Informatics and Management Information
60/JNU OLE
The medical software industry has been slow to develop within the GUI environment. This has contributed to the slow implementation of medical records in practices. This situation is rapidly changing and most major suppliers have or are developing for the Graphical User Interface.
The GUI allows the user to drive the commands. The user still has to type to enter information and data. In medical records and other health applications there is a lot of information. Typing skills to some level are still essential.
5.5 TypingThe computer itself has proved a useful tool in teaching people to type. One can run any number of typing tutor programs on a computer and learn to type without taking the time to travel to lessons. Few health professionals takeadvantageoftheseprograms.Mostprefertohuntandpeck.Thisisusingonefingeroneachhandandhuntingaround the keyboard looking for letters in the manner of a chook in a yard. Gradually their speed improves. They starttolearnwherethekeysareandusemorethanthetwoindexfingers.Eventuallyonecanslowlyprogresstotyping without looking at the keyboard (touch typing).
Thereisgoodevidencethatlearningtotouchtypefromthestartismoreefficient.Healthprofessionalsspendmostof their time consulting and communicating with other people. A computer can be a tremendous barrier in this communication. Most write notes as they go and loose eye contact with the patient or client. To type can be even worse. A health professional skilled in touch typing can maintain eye contact and still generate notes.
Typing tutor programs make reasonable claim to teach basic touch typing with less than a day of user time. In learning to type the user needs to be in a situation where they can continue to use and build on the skill immediately. Moving straight into word processing can be an easy way to accomplish this. Having a skilled word processing person build the format for a letter or document and then the user enter the text is a productive way to build skill.
5.6 Voice Recognition and NotepadsVoice input has been available in various forms since the late 1970s’. It is now available at reasonable cost for the average user. The current programs are useful in word-processing. They are only just starting to be useful for commanding the computer and running other software programs.
English has a large vocabulary. Many words with different meanings sound the same. We have many quite different pronunciations within the English speaking world. Minor upper respiratory illness further alters the pronunciation. Extraneous noise compounds the problems.
We can speak quite rapidly. As we speak the computer has to compare each word with its own phonetic list. The computing power required to do this at reasonable speed is enormous. It is only in the last few years that the average personal computer user has had access to the power required to run voice recognition. Many companies are developing in this area. Voice recognition programs draws heavily on the computer power and the memory storage. Typical example requires a computer with 12 Megabytes of Random Access Memory to run and occupies 22 Megabytes of hard disk space with an additional 5 megabytes required for each individual user.
Most voice systems come with both software and hardware. The software consists of the programs to run the system andthedictionary.Thehardwareincludesthevoicecardtofitinsidethecomputerandtheheadsetmicrophone.Thisraisesanotherissueforthehealthprofessional-aheadsetmicrophoneisadefiniteintrusionintotheconsultation.New directional microphones are now being designed that attach to the computer terminal. These are likely to be more acceptabletopatients.Currentlythesesystemsarestilllessefficientthanlearningtotype.Typingisstillrequiredfordifficultwords.Onestillneedstolearntousethenormalcomputerapplications.Notepadsareanothermodeofentry. This is a small hand held personal computer. The user can print or write using a special pen on the notepad. The software then interprets that writing and converts it to text. It will respond to a command written with the pen. This is slower than moderate typing speeds. This technology is designed for the electronic diary type application
61/JNU OLE
For the new user a Graphical User Interface as seen in the Apple or Windows environments is an essential starting point. One can then focus on understanding the concepts and functions of the software application. Gone is the need to spend endless hours learning the complex commands to drive the computer.
5.7 Specific ApplicationsHealth professionals have found a number of basic software applications important to their everyday needs. The relative importance depends on the nature of their work.
5.7.1 Word ProcessingThis is still the major software application of the personal computer. Old type written and hand written letters no longerfittheimageofthemodernhealthprofessional.
A word processor is a software package that combines a text editor with sophisticated formatting and page layout tools. Fifteen years ago to be able to bold, centre and underline were the new important features. Today the modern programs can format and produce a full text book ready for the printer. For health professionals there have been further changes to word processors that are important. Take producing a letter. When comparing word processing with dictating to a clerical person, the dictating consumes less time. The time consuming task for the professional is the formatting and layout of the document, particularly a letter. Modern word processors solve this with document templates and intuitive help tools.
The program already contains basic formats for letters, memos, faxes, agendas, reports presentations, résumé andanynumberofotherbasicofficedocuments.Theusercanchoosetheappropriatelayoutandsimplyfill inthe details. The software automatically creates the page and document layout. The software can also produce the envelope information and send it to the printer.Some of the help tools will take a user through producing their own version of a letter or other document. By asking the user a series of questions the software designs the appropriate documentformat.Thisfurtherexpandstheflexibilityoftheprogram.Theusercanfocusonthecontentandforgetthe extraneous formatting detail.
The programs retain mailing names and addresses. One can quickly recall these details for use in future letters. This includes merging one letter with an address list sending out any number of personalised letters from one typed letter. An average typing speed and working knowledge of the word processing package enables the health professional to match the speed of clerical personnel when producing documents.
The Graphical User Interface has made a big difference to the word processing software. Altering a margin is simple. Point and grab at the edge of the margin and then drag it to the new position. A page layout view is available when editing a document. The screen then provides the same layout on the page as will be seen on the printed document. Called What You See Is What You Get (WYSIWYG) this tool has enhanced the ease of using a word-processor.
One can use many different fonts and sizes of fonts throughout one document. One can place lines, drawings, tables and graphs anywhere in the document. Tools such as spelling checkers, grammar checkers and on-line thesaurus add to the value of using a word processing package. A spelling tool can go through and check the document. It will learn new words or names from the user’s response to corrections. One can add a medical dictionary to the word-processing dictionaries.
In addition the word processor can trap common spelling errors as the user types. It can then be set to correct these errors automatically. It can also retain common abbreviations converting them to the full version (e.g. type GP computer responds general practitioner). It will keep track of documents retaining the most recently used documents on a simple list for recalling. With the advent of the Fax one can now set the computer up to fax straight from the word processing package into the telephone.
The current major packages include Word and WordPerfect. Both are available in a Windows and an Apple format. Each one leaps the other with additional features in the new versions. Using a word-processor even at a sophisticated level is easy. A few hours of training and the new user can expect to feel comfortable with most of the tasks described. For the health professional a word processor is an essential tool.
Health Informatics and Management Information
62/JNU OLE
5.7.2 SpreadsheetsFor the organised and mathematically minded the spreadsheet is a creative tool. In its simplest form it is a table of columns and rows. The intersecting space is a cell. A cell can retain text, numbers, formulas or a macro. A macro is a small program that performs a simple task. Formulae and macros can be combined to make the spreadsheet one of the most powerful basic computing tools.
The spreadsheet program builds a large number of functions around this basic table structure. A single cell can contain a large amount of information. The user controls how much is displayed and in what format. A cell may contain a formula to average the contents of a number of other cells. One can set the cell to display either the formula or the resulting number. The user can then manipulate the formula and assess the result.
Alargerangeofmathematical,statistical,logical,date/time,specialandfinancialformulasareavailableforuseinacell.Thesevaryfromsimplesum,averageandstandarddeviationtocomplexfinancialtools.Eachformulacaninclude data from a range of other cells in the table. Formulas can be combined to achieve a vast range of function. Inadditionspreadsheetscanbeusedtocalculate“whatif”solutionstoresearch,financialandothermathematicalproblems. “What If” functions allow the user to build up a set of information and then use the computer to model the outcome of different sets of conditions or events.
Theproblemforthenewspreadsheetusercomprehendsthepowerandflexibility.Ittakestimetobuildupmorethan a basic range of formulas and functions. Often there are short cuts in handling a problem that the user will not know. Modern spreadsheet software actually monitors what the user is doing and will offer these short cuts as an alternative. This allows the user to build skills as they use the tool.
ThereareunlimitedwaystouseaSpreadsheet.Themostcommonuseisforfinancialtasks-buildingbudgetsandfinancialmodels.Inthehealtharenatheusesextendtoresearch(datacollectionandstatisticalanalysis),graphinginformationandanalysingdatadirectfromdatabases(medicalrecordsoftware).Itismoredifficulttolearntouseaspreadsheetthanmostothercomputertools.Forthenon-computeruseritisdifficulttounderstandtheconceptof a spreadsheet. There is no equivalent non-computer based tool. The range, size and complexity of spreadsheets defy our capacity to conceptualise them.
Asinglesheettablecanbeeightthousandrowsbytwohundredandfifty-sixcolumns.Thisistwomillioncells.Onecanexpandthisbyhavingmorethantwohundredsuchtablesintheparticularspreadsheetfile.Onecanuseaformulaormacrotobuildarelationshipbetweenonecellandanyothercellinthewholefileofmorethanfourhundred million cells. In addition one can relate the information in a cell or range of cells to a completely separate spreadsheetfile.Considerthatforamulti-dimensionalmathematicalpuzzle.
In large organisations a number of people will build a particular spreadsheet. They will share their spreadsheet over acomputernetwork.Theycanuseinformationfromsectionsofthefilecreatedandupdatedbyanothermemberofthe team. One needs to foster true team management in these circumstances. Issues such as data security and back up of data are of paramount importance.
The current major spreadsheet tools available are Microsoft Excel for Windows or Apple, Lotus 123 for Windows and Borlands Quattro for Windows. Like the word-processing programs the newest version of each of these will leap frog the other two in terms of function. For the Health professional interested in research, administration or practice management learning to use and working with spreadsheets is challenging, productive and fun.
5.7.3 Database ApplicationsAt a conceptual level a database is easier to understand than a spreadsheet. We have a non computer equivalent. It isafilingcabinet.Eachdrawercontainsasetofinformation.Withineachdrawerisasetoffiles.Ineachfilearepagesofinformationrelevanttothatfile.
63/JNU OLE
Thecomputerbasedfilingcabinetismorerigid.Thedrawersaresimilar.Atthefilelevelthereisadefinedstructure.Thetermfortheindividualfileisatable.Thetableconsistsofcolumnsandrows.Eachcolumndefinesthenatureof the information (e.g., Surname, initials, Date of Birth). Each row is a record in the table (e.g., Bloggs, JH, 24 January 1952).
Adatabaseprogramallowstheusertobuildtheirowntables.Theuserdefinesthefieldsofinformation.Whatwillgointhefield(e.g.,anumber,adate,text),itslengthandanyspecialproperties(e.g.,defaulttofemale,defaulttotoday’sdate).Onceatableandtheinformationaredefined,theusercanenterthedata.Thisdatathenformstherecords in the table.
Themoststartlingdifferencebetweenafilingcabinetandthecomputerdatabaseisinthewaythecomputercanhandle the information. The computer can quickly sort the table into any required order. The user may want to sort bypostcodeorbydateofbirth.Knowingthestructureofthetableonecanquicklydeterminethefieldcontainingpostcode.Thecomputercanthensortthewholetablebythatfield.Itcansortbymorethanonefield(e.g.,listthepatientsbythefieldageandthenbythefieldsex).
Onecanaskthecomputertopulloutasub-setoftheinformation.Onedefinesthefieldandtypeofinformationrequired(e.g.inthetableofpatients,listallthepatientswherethefieldsexcontainsthetermfemale).Thisprocessisfilteringoftheinformation.Bysortingandfilteringonecanmanipulateandanalysetheinformationinacomputerdatabase to an extent not possible in the paper equivalent.
Thereisanadditionalconceptnotsoevidentinthepaperfilingsystem.Onecanlinktables.Inthepaperworldwe do this by making a reference in a computer database this is much more powerful. We can relate one table to anothertablethroughacommonfieldofinformation.Thisfieldwillneedtobepresentineachtable.Inamedicalrecord system we may wish relate the table containing patient medication records to the table containing the patients’ details.Todothiswewouldneedacommonfieldorfields.Theeasiestcommonfieldwouldbeapatientnumber.By having the patient number in the table of patient details and in the table of medication records one can relate the two tables.
A database program with this facility is a relational database. A single table is limited. Consider a medical record. Definingfieldsforthenameaddressanddateofbirthiseasy.Howdoweincorporatetheneedtohaveamedicationlistoralistofallergies?Thetablebecomesverylargewithafieldeachforonemedication,oneallergy,onehealthproblem, etc. What if the patient is on two medications?
When one can build relationships between tables then a table can be small and simple with a limited number of fields.Medications,allergies,healthproblemsandpatientdetailswouldeachbeintheirowntables.Therelationshipsbetween the tables allow the computer to put the information together.
Thesortingandfilteringfunctionscanbeaddedtothisrelationaldatabase.Thisproducesapowerfulinformationmanagement tool. List all the female patients over forty with hypertension and on medication is a massive task in apapermedicalrecordfilingsystem.Inarelationalcomputerdatabaseitissimpleandfast.There is a vast range of database tools. A Medical Record system is usually based on a relational database. Companies developing this type of software use these database tools and often programme a great deal of the database themselves.
The average health professional does not always need that level of performance. There are now simple modern database tools that are easy to use and will service most need. Dbase was the original major personal computer based tool. There is now a range of easy to use Microsoft Windows and Apple based databases. They combine all the simple Windows based functions with a full relational database.
The graphical user interface has made a big difference to the ease of use. One can see the relationships between tablesonthescreen.Atableisaphysicaltable.Thefieldscanbemovedandre-definedbypointingwiththemouseanddraggingthemacrossthescreen.Therelationshipsareseenasgraphicallinesbetweenfieldsinthetables.

Health Informatics and Management Information
64/JNU OLE
There are help tools that take the user through building a query or report. No longer does the user have to type a carefully prepared sentence in a strange version of English to retrieve information.
One could build a medical record system using the “over the counter” database tools. It takes some time and considerable skill with the chosen product to do this. It is the design, layout and relationships of the tables that cause themostproblems.Apoorinitialdatastructurewilldiminishtheefficiencyofthesystem.Asthesystemdevelopsthisunderlying weakness will become more obvious. This is a major frustration for amateur medical record designers. Another problem is the speed of the software when under the loads of large complex medical record tables. Poor design will reduce the speed of the program. In health care the speed of information management is a key feature.
Not all health professionals want full medical records. One may wish to create a subset of a medical record. For example an infant health nurse may wish to track some aspect of children’s health. Building a data collection and reporting for this type of application is now quite easy with the modern tools. A three day course on a typical relational database would allow the average user to build such an application.
A new feature of the modern programs is the ability to integrate with other databases. This includes mainframe systems. A user with a commercial medical record system could attach tables from the medical records to tables in their own database. By building relationships between the tables from both systems they have access to composite data. For example one may build a simple table containing information about diabetic patients in a personal computer database. One could then attach the patient names and address table from the main medical record system. The personal computer can now use the address information combined with the list of people with diabetes to mail out a letter to all diabetics.
Caremustbetakenwhenconnectingdifferentdatabases.Firstlyconfidentialitymaybeanissue.Whohasaccessto what information? How will it be used? In a commercial medical record package the designers have usually thought through these issues and set safeguards. By networking one database to another one can by-pass some of these safeguards.
An additional problem is in the potential to corrupt data in the host database. If one uses a personal computer database to alter data on the main medical record computer then it is possible to seriously damage the medical record information. One needs to understand the structure and function of both databases before using one to alter information on the other. It is relatively safe to use different tools to read and report on information. For changing or adding information it is important to use the original product that created and is responsible for maintaining that data.
Objectlinkingaddsanextrabenefitinusingamoderndatabase.Objectlinkingiswhereinformationcreatedandstored in one application is used in another. For instance one may create a Diabetic mailing list in a database. With Object Linking that information can be linked to a letter in a word processing tool. When the letter is created, the word-processing package can open the database and retrieve the latest mailing list. Another example is in creating a budgetinaspreadsheet.Onecanlinkthetablesfromthatbudgettoafinancialplanningdocumentinwordprocessing.Analterationtothefiguresinthespreadsheetappearsthenexttimethewordprocessorprintsthefinancialplandocument. These features add a great deal to productivity in the administration, practice management and research areas. They are an important function within the Windows environment. Most major software producers are taking advantage of this Object Linking feature.
5.7.4 Presentation SoftwareHealth professionals have to communicate well. Modern presentation software provides some real solutions. Take the typical presentation to a group of people. One needs an outline, speaker’s notes, slides or overheads and a handout. Modern presentation software allows the user to create all these with a minimum of duplication.
The modern laser and the colour ink jet printers can create overhead templates direct from the software in colour. The computer can place the images on a disk for colour slide production. The tools automatically process the computer image onto 35mm slides and now relatively in-expensive.
65/JNU OLE
The software can correct spelling. It can use Object Linking to grab charts from the spreadsheet or text from a documentcreatedinthewordprocessor.Largefilesofdiagramsandillustrationscomewiththesoftware.Thesecanbe quickly incorporated into the overhead. The software comes with tutorials on the computer and on-line help. A courseisnotnecessarybutismoreefficient.Ahalfdaywillassisttheaverageusertogeneratesimpleandeffectivepresentations.
The modern software will produce miniature copies of each overhead. It then places speaker’s notes beneath these. These can then be used as prompts during the presentation. The software can produce a handout by combining two or three overheads on one page, printing them out for photocopying. The time taken to generate a full quality presentation is reduced considerably. With all the information on the computer, updating and modifying the presentation is easy.
The slide show is another feature. Most presentation packages can link direct to video projection units. The presentation is transported to a notebook computer. The presenter then connects this to a video projection unit. The overheads run on the notebook as a slide show. The presenter uses a mouse to change slides as the presentation proceeds.
5.7.5 Financial ToolsThesimplefinancialtoolshaveledthewayineaseofuse.Thecomputerisparticularlygoodatmanipulatingnumbers.When this is combined with a graphical user interface one can change the face of small business management. There isaproliferationofallthefinancialtools.Fromsimplecashbookstofullaccountingandpayrolltools,thechoiceisenormous.Forlessthanonehundreddollars,userscanfinallybringsomeordertotheirpersonalfinances.
Some of these tools act as cheque books. They can print cheques ready for you to sign. They keep track of all income and expenditure. They can then provide reports. One can group expenditure under tax deductible and non-tax deductible. All accounts and credit cards are entered and reconciled within the package.
In addition they can take the user through the process of producing a budget. One can build this from the preceding year’sfigures or from scratch.The computerwill then convert this to a quarterly,monthlyorweeklybudget.Informationenteredduringtheyearisreportedalongsidetheexpectedbudgetfigure.Onecanimmediatelyseethevarianceandtakecorrectiveaction.Inadditiontopersonalfinancesthesepackagesareadequateforsmallcompaniessuch as medical practice, health-care centre, community service agency.
More sophisticated packages are available for the larger business. These carry additional features such as general ledger facilities, accrual accounting, payroll, etc. With increasing sophistication there is an associated increase in price. Ease of use is inversely proportional to sophistication. It is often tempting to go to these higher level packages.
The new user should choose a product that suits current needs. Such a product is likely to be easier to use. With the development of one’s own business there is usually a parallel development of the selected computer software. Thecashbookisagoodapplicationforthenovicecomputeruser.Itprovidesimmediatetangiblebenefitsforlittlelearning time. The tutorials in the manuals and on-line are usually adequate to get a good grasp of the product.
Payrollproductshavebeenslowtodevelop.TheyarespecifictoAustralianconditionsandithasnotbeeneasytoreviseapopularAmericanproductasisthecasewithcashbooks.Payrollisadifficultareatomanageformostsmall business. Many health professionals practice through small business structures. The modern medium to high end cashbooks is adding payroll tools. For any business with more than a few employees this tool is easy to set up and can save considerable time.

Health Informatics and Management Information
66/JNU OLE
SummaryGainingashort termbenefitfromasimpleusefulcomputerapplicationwillenableanewusertomaintain•interest.The computer has problems with our accents, with words that are phonetically similar and when minor illness •effects our pronunciation.There are at least twelve function keys labelled F1 - F12. These have different roles in different software •packages.In a common word processing package Control A generates a command to format all the characters as •capitals.The Enter key is the most important as it tells the computer to accept what the user has typed or to run a particular •task offered by the computer.Combining the Control Alternate and Delete key generates a command used often by the new user.•Essentially all the keys beyond the standard type-writer keyboard generate commands not characters.•With the advent of the mouse it has become much easier to drive modern software. •The mouse and a screen layout called the Graphical User Interface changed the face of personal computing.•A Graphical User Interface (GUI) is where the computer software produces pictures and pull-down menus to •indicate the choice of commands available to the user.Touch screen technology was available prior to the common use of the Graphical User Interface and the •mouse.ApplewasthefirsttoeffectivelymarkettheGraphicalUserInterface.•The real advantage of GUI is that the command format is the same across a wide range of computer software •applications.The GUI controls the printer and printing initiated by any software package.•Typing tutor programs make reasonable claim to teach basic touch typing with less than a day of user time.•A word processor is a software package that combines a text editor with sophisticated formatting and page •layout tools.What You See Is What You Get (WYSIWYG) this tool has enhanced the ease of using a word-processor. •
ReferencesLord, T.,• Basic Applications and Expectations, [Pdf] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_06.pdf> [Accessed 27 November 2012].Competencies for Public Health Informaticians 2009. • [Pdf]. Available at: <http://www.cdc.gov/informaticscompetencies/downloads/phi_competencies.pdf> [Accessed 27 November 2012].Dr. Zitner, D., 2010.What is Health Informatics. • [Video Online]. Available at: <http://www.youtube.com/watch?v=VKPSuDG_bTU>[Accessed 27 November 2012].2011. • Health Informatics Overview. [Video Online]. Available at: <http://www.youtube.com/watch? v=au1OFMyVP0Q> [Accessed 27 November 2012].Hovenga, E., Kidd, M., Cesnik, B. & Livingstone, C., 1996. • Health Informatics: An Overview, Australia. Sullivan, F. & Wyatt, J., 2009. • ABC of Health Informatics, Wiley.
Recommended ReadingShortliffe, H. E. & Cimino, J. J., 2006. • Biomedical Informatics: Computer Applications in Health Care and Biomedicine, Springer.Lazakidou, A. A., 2006. • Handbook of Research on Informatics in Healthcare & Biomedicine, Idea Group Inc (IGI).Maeder, J. A. & Martin-Sanchez, J. F., 2012. • Health Informatics: Building a Healthcare Future Through Trusted Information, IOS Press.
67/JNU OLE
Self AssessmentAlternate (ALT) and a Control (CTRL), like a __________, they are used with letters, numbers or the function 1. (F1 - F12) keys.
shift keya. function keyb. tab keyc. page down (Pg Dn) keyd.
__________ tells the computer to accept what the user has typed or to run a particular task offered by the 2. computer.
Shift keya. Function keyb. Tab keyc. Enter keyd.
__________ is particularly important to the new user when exploring the unknown3. Shift keya. Esc keyb. Tab keyc. Enter keyd.
With the advent of the __________ it has become much easier to drive modern software. 4. mousea. keyboardb. computersc. technologyd.
The mouse and a screen layout called the __________ changed the face of personal computing.5. Graphical User Interfacea. Graphical User Designb. Graphical User Technologyc. Graphical User Desktopd.
A __________ is where the computer software produces pictures and pull-down menus to indicate the choice 6. of commands available to the user.
Graphical User Interfacea. Graphical User Designb. Graphical User Technologyc. Graphical User Desktopd.
__________ technology is particularly good for situations where non-computer users need to communicate.7. Hardware a. Software b. Touch screen c. Computerd.
Health Informatics and Management Information
68/JNU OLE
__________ is still the major software application of the personal computer.8. Word Processinga. Spreadsheetsb. Database Applicationsc. Presentation Softwared.
_________ this tool has enhanced the ease of using a word-processor. 9. What You See Is What You Get (WYSIWYG)a. Graphical User Interfaceb. Graphical User Designc. Graphical User Technologyd.
For the organised and mathematically minded the __________ is a creative tool.10. spreadsheeta. word processingb. spreadsheetsc. database applicationsd.
69/JNU OLE
Chapter VI
Electronic Medical Records
Aim
The aim of this chapter is to:
explain the concept of electronic medical records•
elucidate the concept of traditional medical record systems•
explicate relation between technology and health care delivery•
Objectives
The objectives of this chapter are to:
explain the consequences of using manual-based record systems•
elucidatethebenefitsofEMR•
explicate various computerised clinical decision support tools•
Learning outcome
At the end of the chapter, you will be able to:
describe the software applications providing decision support in EMR•
understanduserdefinedflowchartofclinicaldata•
identify the challenges in introducing EMR in health care sector •
Health Informatics and Management Information
70/JNU OLE
6.1 IntroductionThe importance of medical records in health care delivery has been recognised for a long time. Its relevance to patient care and health administration was documented by Florence Nightingale in 1873 a book entitled Notes on a Hospital. Health care is a continuous process in which data is progressively accumulated, therefore the record must function as a ‘pre-birth to post-death system that meets the requirements for any clinical setting-whether intensive care or primary care.
Ideally the medical record should be the primary repository of all information regarding patient care, provide decision-support, and be a tool for supporting and maintaining ancillary health care activities such as administration, quality assurance, research and epidemiology.
Shortliffehasdefinedmedical(health)practiceasmedicaldecision-making,anditisrecognisedthatthereisanintegral relationship between medical decision making, the accumulation of clinical data, health care costs, patient outcomes,andthequalityofcare.Thedeliveryofquality,cost-effectivehealthcarerequiresefficientdecision-support tools based on the medical record system if these end points are to be achieved.
6.2 Traditional Medical Record Systems Current medical record systems are predominantly hard copy paper-based models with or without variable components of electronic data such as laboratory results and X-ray reports. The paper chart can be read by only one person at a timeandtheymusthaveitphysicallyintheirpossession.Itisdifficulttostoreandretrieve,requiringspace,timeand effort. It can be organised in one format at a time yet the demands of the users of the record require it to be in a multitude of formats to meet the individual’s needs. To reorganise the record into a variety of formats requires major time commitments and the schematic format is easily corrupted. The paper record is not always legible, is ofteninaccurate,lacksclinicalsensibility,andisnotcompatiblewithspecifieddatastandardsorotherinformationstoredintherecord.Poorindexingofdatamakesthefindingofinformationdifficultorimpossible.
Reproduction of the manual record by transcription and photocopying adds to the costs of health care services withoutanycorrespondingprovenbenefit.ItwasrecentlycalculatedintheU.S.A.tocostanadditional$15billionper year to manually reproduce the medical record by transcription. Use of the paper chart as a medical record impedeseffortstomonitorandimprovehealthcarebytheinherentdifficulty,time,andexpenserequiredtoaccessindividual charts.
6.3 Technology and Health Care Delivery Since the 1960s there has been a rapid growth in the technology used to support medical care and this has resulted in the creation of enormous volumes of data and information that is available to assess and manage the delivery of health care. Weed estimated that an individual patient can generate up to 50,000 data items during their life (Weed 1989), and to support good decision-making individuals who provide health care require timely integration of this data. New and evolving technologies continue to produce and store large volumes of data and information for patient care, but there only a few systems that provide information processing tools which support clinical decision making.
It is recognised that information processing capacity of the human brain is limited in its ability to accurately decipher this clinical data and information in a timely manner without errors. Errors in decision making are further increased when there is random noise data, for example, with unexpected data input in stressful situations, a common occurrence in health care.
6.4 Consequences of Using Manual-Based Record Systems The use of predominantly manual, non-integrated medical records systems has led to increasing costs in patient care and administration, decreased compliance with health care standards, inappropriate variation in health care delivery and possible negligent behaviour by health care providers. A Harvard study into the incidence of adverse events during hospitalisation led the authors to conclude that, ‘Lawyers generally believe that investigation of substandard careonlybeginswiththemedicalrecord;thatinmanyinstancesthemedicalrecordevenconcealssubstandardcare;andthatsubstandardcareisnotreflectedin,or“discoverable”inthemedicalrecord’.

71/JNU OLE
6.5 Concept of Electronic Medical Record (EMR) What is the Electronic Medical Record (EMR)? It is the storage of all health care data and information in electronic formats with the associated information processing and knowledge support tools necessary for the managing the health enterprise system.
In the early 1970s several institutions investigated the concept of creating an EMR to improve patient care. An important feature each of these projects was the concept that the medical record should be the cornerstone for all information systems within the health care environment and that the data supporting ancillary patient care activities such as administration, pharmacy, laboratories, etc., could and should be generated as a by-product of the patient care process.
One of the earliest successful implementations of EMR functions was at the Regenstrief Institute, Indianapolis. Using the Regenstrief Medical Record System (RMRS) McDonald demonstrated that the use of computer-generated remindersbasedonpatient-specificlaboratorydataresultedinareductionofphysicianserrorsinthedetectionoflife-threateningevents,andalsoconfirmedthatbusyphysicianswereoftenunabletodetectmanyofthecriticalabnormalities occurring in the patient record. He concluded that, ‘the amount of data presented to the physician per unit time is more than he can process without error. The computer augments the physician’s capabilities and thereby reduces his error rate. It is very likely that the physicians in these studies were simply unable to detect all themultitudinousconditionsspecifiedbythestandards.’Computer-generatedremindersarenowusedasstandardtools for patient care in the RMRS and other EMR systems used in hospitals and ambulatory care environments.
6.6 The Institute of Medicine Study into Electronification of the Patient Care RecordIn 1992 the Institute Of Medicine of the American National Academy of Sciences, published the results of its study intocomputerisedmedicalrecords,theirfunctionality,andhowtechnologycouldbringthebenefitsoftheserecordswithin the reach of all those within the health care system. The recommendations from this study are summarised in the following list:
Health care professionals and organisations should adopt the computer based patient record (CPR) as the standard •for medical and all other records related to patient care. To accomplish Recommendation 1, the public and private sectors should join in establishing a Computer based •Patient Record Institute (CPRI) to promote and facilitate development, implementation, and dissemination of the CPR. Both the public and private sectors should expand support for the CPR and CPR system implementation through •research, development anddemonstrationprojects. Specifically, the committee recommends thatCongressauthorise and appropriate funds to implement the research and development agenda outlines herein. The committee further recommends that private foundations and vendors fund programs that support and facilitate this research and development agenda. The CPRI should promulgate uniform national standards for data and security for facilitate implementation of •the CPR and its secondary databases. The CPRI should review federal and state laws and regulations for the purpose of proposing and promulgating •model legislation and regulations to facilitate the implementation and dissemination of the CPR and its secondary databases and to streamline the CPR and CPR systems. ThecostsofCPRsystemsshouldbesharedbythosewhobenefitfromthevalueoftheCPR.Specifically,the•full costs of implementing and operating CPRs and CP systems should be factored into reimbursement levels of payment schedules of both public and private sector third-party payers. In addition, users of secondary databases should support the costs of creating such databases. Health care professional schools and organisations should enhance educational programs for students and •practitioners in the use of computers, CPRs, and CPR systems for patient care, education, and research.

Health Informatics and Management Information
72/JNU OLE
Publication of this report has resulted in wide range of activities directed towards standardised EMR developments. In North America, the US department of Health and Human Services has implemented a national policy on a health information communication infrastructure based on automation of the patient record (US. Department of Health and Human Services). This group sees a national interconnected communication network linking all participants in the health care system via their own ‘computer-based patient record system -an information system that would have the ability to create, store, retrieve, transmit and manipulate patients ‘ health data in ways that best support decision making about their care.’ These record systems would be linked to reference bases of aggregated patient data and computerised knowledge-based systems which use decision support logic and practice guidelines to help caregivers make better decisions about diagnosis and treatment options.
6.7 Software Applications Providing Decision Support in EMRsNo complete EMRs currently exist however standards for software functionality and decision-support have been definedandareseenascoreelementsforfutureEMRdevelopments.ThebasicsoftwarecomponentsnecessaryforfutureEMRsasdefinedbyMcDonaldareshowninFig6.1,andadescriptionofthesetermsisoutlinedinthefollowing text.
Maintain a data dictionary •Orientation •Introspection •Selectivity of data input •Query languages •
Insystemswhichmaintainadatadictionary,alldataandobservationsarestoredinrecords,whichincludefieldsthatlinkorpointtothedictionaryfiles.Thismeansthatthedataisstoredincodedformatswhichprovidesformoreconsistentrecordingandeaseofdataentry.Theyalsoprovidefacilitiesfordeclaringthedataentryfieldspriortotherecordingandstorageofdata,withouttheneedtodefineinadvancethespacetobeoccupiedbytherecordeddata, thus providing a much more economical use of computer storage space, and more rapid access to the data.
Orientationprovidesthefacilitytoproduceanarrayoftime-orientedflowsheetsfromthestoreddata.Fig.6.1showssummaryflowchartofclinicaldatatakenfromapatientonchemotherapyforleukaemia.Thecapacityfordisplayingclinicaldatainuser-defined,timeorientedformatsisadecisionsupporttoolfundamentaltogoodclinicalpractice.
Introspection is a decision support tool where the computer is able to examine data and information stored within the EMRdatabaseusingpre-definedclinicalrules,andidentifycertainconditionsthatrequireattention.Theserecordsystemsautomaticallyproducedrug-alerts,warnings,protocol-generatedremindersandareabletodetectsignificantalterations in data elements which complement the medical decision making process.
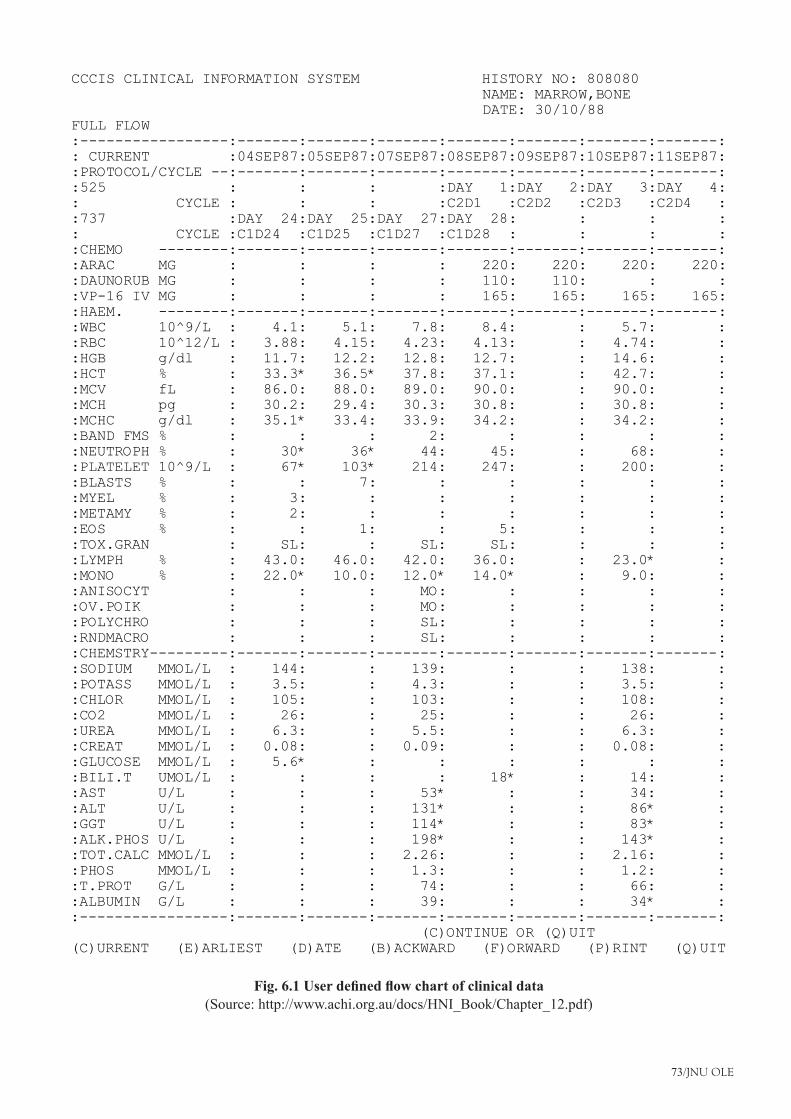
73/JNU OLE
CCCIS CLINICAL INFORMATION SYSTEM HISTORY NO: 808080NAME: MARROW,BONEDATE: 30/10/88
FULL FLOW:-----------------:-------:-------:-------:-------:-------:-------:-------:: CURRENT :04SEP87:05SEP87:07SEP87:08SEP87:09SEP87:10SEP87:11SEP87::PROTOCOL/CYCLE --:-------:-------:-------:-------:-------:-------:-------::525 : : : :DAY 1:DAY 2:DAY 3:DAY 4:: CYCLE : : : :C2D1 :C2D2 :C2D3 :C2D4 ::737 :DAY 24:DAY 25:DAY 27:DAY 28: : : :: CYCLE :C1D24 :C1D25 :C1D27 :C1D28 : : : ::CHEMO --------:-------:-------:-------:-------:-------:-------:-------::ARAC MG : : : : 220: 220: 220: 220::DAUNORUB MG : : : : 110: 110: : ::VP-16 IV MG : : : : 165: 165: 165: 165::HAEM. --------:-------:-------:-------:-------:-------:-------:-------::WBC 10^9/L : 4.1: 5.1: 7.8: 8.4: : 5.7: ::RBC 10^12/L : 3.88: 4.15: 4.23: 4.13: : 4.74: ::HGB g/dl : 11.7: 12.2: 12.8: 12.7: : 14.6: ::HCT % : 33.3* 36.5* 37.8: 37.1: : 42.7: ::MCV fL : 86.0: 88.0: 89.0: 90.0: : 90.0: ::MCH pg : 30.2: 29.4: 30.3: 30.8: : 30.8: ::MCHC g/dl : 35.1* 33.4: 33.9: 34.2: : 34.2: ::BAND FMS % : : : 2: : : : ::NEUTROPH % : 30* 36* 44: 45: : 68: ::PLATELET 10^9/L : 67* 103* 214: 247: : 200: ::BLASTS % : : 7: : : : : ::MYEL % : 3: : : : : : ::METAMY % : 2: : : : : : ::EOS % : : 1: : 5: : : ::TOX.GRAN : SL: : SL: SL: : : ::LYMPH % : 43.0: 46.0: 42.0: 36.0: : 23.0* ::MONO % : 22.0* 10.0: 12.0* 14.0* : 9.0: ::ANISOCYT : : : MO: : : : ::OV.POIK : : : MO: : : : ::POLYCHRO : : : SL: : : : ::RNDMACRO : : : SL: : : : ::CHEMSTRY---------:-------:-------:-------:-------:-------:-------:-------::SODIUM MMOL/L : 144: : 139: : : 138: ::POTASS MMOL/L : 3.5: : 4.3: : : 3.5: ::CHLOR MMOL/L : 105: : 103: : : 108: ::CO2 MMOL/L : 26: : 25: : : 26: ::UREA MMOL/L : 6.3: : 5.5: : : 6.3: ::CREAT MMOL/L : 0.08: : 0.09: : : 0.08: ::GLUCOSE MMOL/L : 5.6* : : : : : ::BILI.T UMOL/L : : : : 18* : 14: ::AST U/L : : : 53* : : 34: ::ALT U/L : : : 131* : : 86* ::GGT U/L : : : 114* : : 83* ::ALK.PHOS U/L : : : 198* : : 143* ::TOT.CALC MMOL/L : : : 2.26: : : 2.16: ::PHOS MMOL/L : : : 1.3: : : 1.2: ::T.PROT G/L : : : 74: : : 66: ::ALBUMIN G/L : : : 39: : : 34* ::-----------------:-------:-------:-------:-------:-------:-------:-------:
(C)ONTINUE OR (Q)UIT(C)URRENT (E)ARLIEST (D)ATE (B)ACKWARD (F)ORWARD (P)RINT (Q)UIT
Fig. 6.1 User defined flow chart of clinical data(Source: http://www.achi.org.au/docs/HNI_Book/Chapter_12.pdf)

Health Informatics and Management Information
74/JNU OLE
The users of EMR systems must decide on the selectivity of data input and how it will be entered into the medical record, manually, electronically, or by other processes. Quality data input can be expensive to maintain because it requires disciplined, well-trained staff. However, once data are stored the users have access to the computers powerful report generator functions that provide useful data and information displays and reports that support all components of health care delivery
It is now possible to access these large volumes of clinical data stored in electronic formats using medical query languages for the purposes of research, epidemiology, health care planning, and for producing reports based on dataanalysis.Thecollectionofinformationonlargenumbersofpatientstoanswerspecificproblemsisexpensive,time consuming and personnel intensive and is often restricted to small numbers of patients for a limited range of conditions. For example, to answer the question whether the postmenopausal oestrogen use protected women against cardiovascularmorbidityandmortality,Stampferandothershadtoreceiveregularmailedreportsonspecificclinicalevents from more than 48,000 women for 10 years. These tasks could have been performed more easily and cheaply if the data were available in a single EMR database or accessible over a range of standardised EMR systems.
6.8 Computerised Clinical Decision Support ToolsSpecificdecisionsupporttoolsforusewithinEMRshavebeendefinedwhichprovidebenefitstohealthcare,andthese are as follows:
Alerting •Interpretation •Assisting •Critiquing •Diagnosing •Management •
Alerting automatically provides decision makers with data and information in situations where rapid, sometimes life threatening, decisions are required. Examples are abnormal laboratory values, vital sign trends, failure to perform nursing procedures and medication contraindications. These clinical situations often have episodes of unpredictable random noise data which impair the decision making process leading to errors in patient care.
A system of alerts is used routinely in the HELP (Health Evaluation through Logical Processing) and Regenstrief MedicalRecordSystems(RMRS)establishedbenefitsfromtheuseofalertsareareductioninphysicianandnursingerrorsinpatientmanagement,increasedcompliancewithpredefinedstandardsofcare,decreasedlengthofstayinhospital and time spent in life-threatening situations.
Using automated alerts in the HELP system during surgery for non-indicated and no ordered antibiotics Classen demonstrated a fall in the post-operative infection rate from 13% patients per day to 5.5%, and a fall from 35% to 18% in the percentage of patients receiving antibiotics late for surgery. As a consequence there was a reduction in the number of patients receiving antibiotics for an excessive time post-operatively which produced overall savings
Interpretation is where stored clinical data is assimilated leading to an improved understanding of what the data means.ExamplesareECGinterpretation,bloodgasdataanalysisandtheinterpretationofX-rayfindings.
Assisting is where the use of decision-support tools speed up or simplify some clinical action. This technique is used in the production of clinical orders, nursing assessment of patients, and history and physical examination. Patient pre-printed encounter forms improve history taking and standardise data recording. Assisting also facilitates direct data entry onto computer terminals making the data immediately available to authorised users of the EMR.
Where assisting is used in the ordering of blood samples the specimen is ordered ‘online’ and the EMR system indicates the tube type, laboratory to which the specimens are to be sent and when the last specimen was ordered. In this situation the system may also recommend how many times and on what dates a given sample is to be collected

75/JNU OLE
withinaspecifiedtimeinterval.AttheJohnsHopkinsOncologyCentre(JHOC),computerisedprotocol-directedcareplanswereusedtomanageblood-productfacilitiesbyrecommendingspecificnumbersofplateletunitsforthrombocytopenicpatientswhowereatriskofbleeding.Thisproducedcostsavingsof$250,000peryear,decreasedthe use of a limited resource (platelets), and improved patient outcomes (no increase in bleeding).
CritiquingiswheredecisionsareanalysedwithintheEMRusingdefinedknowledgerulestoverifytheappropriatenessof those decisions. The system is able to recommends to the physician, nurse, etc., the most appropriate decision to make. Examples of critiquing include clinical orders, protocol-directed care plans, diagnosis making and management plans.
Diagnosingiswhereaspecificclinicalmodelisappliedforthepurposeofunderstandingacomplexclinicalsituation.In these situations the computer may provide a probability list for a range of differential clinical diagnoses based on the data has stored within it. Currently these systems are limited to small clinical domains, such as intensive care, and are expensive because of the expertise needed to maintain the knowledge rules within them.
Management is the generation of action oriented decisions designed to improve the functionality of the current system state. Examples include hospital operations, resource allocation (including personnel) and the current status of changing clinical disease patterns, either acute or chronic. In HELP the decision support system will recommend changes in FI02 (Fraction of Inspired Oxygen) with patients on respiratory support and suggest when to draw the next blood gases based on existing laboratory and clinical data (Kuperman et al 1991). Pooled data from HELP made available to surgeons performing uncomplicated prostatic resections resulted in reduced length of stay and costs of the procedure over a range of hospitals in the region.
The Oncology Centre Information System (OCIS) system uses nurse generated patient dependency ratings to allocate staff during hospital admissions, and patients are scheduled in outpatient clinics according to the procedures performed so that the doctor-patient encounters coincide with the availability of the clinical data.
Many decision-support applications coexist within EMR systems and they must be integrated to the continuously expanding database of individual patients and groups of patients. Data required for patient care must be available in a timely, reliable and complete manner with the user being able to extract data they require in the format that best suits their decision making. Timeliness of data retrieval is critical in patient care and it has been recommended that data recall times of less than two seconds should be achieved irrespective of the complexity of the decision support function. An example of how access, storage, and manipulation of clinical data is able to assist all levels of health care is illustrated in Fig.6.2:

Health Informatics and Management Information
76/JNU OLE
CCCIS CLINICAL INFORMATION SYSTEM PRINCE OF WALES/PRINCE HENRY HOSPITALS
888888: WALKER, LUKE HEMATOLOGY PLOT FOR CYTOPENIC PATIENTS 03/11/89 WBC,PLATELETS,HGB,TEMP FOR CYTOPENIC PATIENTS
:---------------------------------------------------------:10.0W: :
: :1000P: :
:WwW:W8:wWw:P005:www::wppPpww:P052:PPpww::ppWww:P521:PpWww::PpwpP:W4
50.0P:----P---P------------------------------------------------::pWwpppPPwP:
31.25P: Ww Pp pppPp pP wPwWpP :1.0W:------W-W---------P-----P-----------P---P----------------:
:PwPwWwwwPwWwWwwwWwWwwwW:P526.510W: :
:---------------------------------------------------------:ARAC :AAAAAAAAAA:DAUNORUB :DDDDD:VP-16 IV :VVVVVVVVVV:
:---------------------------------------------------------:PESGUA7891
DATE 12 14 16 18 20 22 24 26 28 30 01 03 05 07 09 11 13(N)EXT (B)ACK (F)ORWARD (D)ATE (E)VENT (R)EDO (P)RINT (Q)UIT
Fig. 6.2 Daily plot of white blood cells and platelets with chemotherapy(Source: http://www.achi.org.au/docs/HNI_Book/Chapter_12.pdf)
Thisisaplotofwhitebloodcellsandplateletsonapatientundergoingchemotherapy.Thedisplayshowsuser-definedlevels (horizontal dashed lines) at which decisions relating to platelet or white cell transfusion, or prophylactic antibiotic therapy may be made. Using accumulated data from groups of patients based on the time interval in which they have a low cell counts, the length of stay in hospital can be predicted by treatment and diagnosis, thus aiding bed allocation and roistering of nursing staff based on patient dependency status. Resource utilisation such as the number of tests ordered, medications utilised and bed occupancy can be evaluated from the data accumulated during the patient care process, demonstrating how administrative and health planning data can be generated from the patient care record. The data displayed is linked to the complete medical record so complex interrelationships of data within the EMR can also be evaluated.
6.9 Existing EMR Models and Confirmed Benefits of EMRs Complete automation of the medical record system has not yet occurred, however there are arrange of EMR systemswhichprovideinformationdemonstratingtherealandpotentialbenefitsofelectronicallystoredmedicalinformation. Recent advances in technology relating to data and information storage, such as Compact Disks—Read Only Memory (CD-ROM), provide facilities for life-long repositories of medical data. There are functioning EMR systems storing in excess of 1 million patients on line, representing billions of data points accessible within seconds andtheabilitytomanagetheselargevolumesofdataisanotherareawherethebenefitsofcomputerisationcanbeseen.Forexample;
Fries and his co-workers, using the American Rheumatologic Association Medical Information System •(ARAMIS),showedthatphysiciansusingacomputeriseddataflowsheetwereabletofindspecifiedinformationtwiceasfastasphysiciansusingthetraditionalpaperrecord.Thephysiciansinthisstudywereabletofindtherelevantinformationvirtuallyallthetimewiththecomputerrecordbutfailedtofind10%oftheinformationin the paper chart,

77/JNU OLE
Whiting-O’Keefe and his colleagues used the Summary Time-Orientated Record (STOR) to show that physicians •were better able to predict their patient’s laboratory results when using the computerised record.Computer-generated reminders used in the RMRS have improved compliance with practice standards particularly •in the area of preventive care. HELP has an extensive alerting system based on data generated from laboratory auto analysers which has resulted •in shorter length of stay in hospital, reduced costs and time spent in life-threatening situations.ResearchusingOCIShasconfirmedthebenefitsofprotocol-directedcareplansbyreducingresourceutilisation•and costs without reducing the quality of care.Use of the Beth Israel Hospital (BIH) system has improved access to medical records, provided decision support •through rapid access to bibliographic databases and to cumulative patient data subsets via its medical query language.
Thebenefits fromeffective automationofhealth caredeliveryusingEMRsystemsbasedon the IOMcriteriacan be viewed from different domains namely, patient care, quality assurance, costs, epidemiology, research, and administration.
6.10 Patient Care Preventive care is recognised as one area for providing major cost savings in health care delivery. The effective use of an electronic reminder system based on the patient record has resulted in the more effective implementation of preventive care protocols, immunisation procedures, better utilisation of vaccines, and a reduction in morbidity and mortality from infectious diseases.
6.11 Quality Assurance Effective quality assurance in health care requires a reduction of inappropriate variation in health care delivery and adequate documentation of procedures to improve the processes involved in health care delivery. At the Regenstrief Institute rheumatologists use the RMRS to identify patients with rheumatoid arthritis and other connective tissue disorders who are being treated with “second line” drugs such as gold, methotrexate, azathioprine, and penicillamine. The monitoring program detects whether the appropriate pre-treatment haematology and urine tests have been performed, if the results are abnormal and whether the drugs were held or given in reduced dosages.
Patients whose records do not meet these standards have their outpatients charts reviewed and, if substandard care hasbeendelivered,theprovidersarecontacted.Thesamesystemusingdataaccumulatedwithinthefirst24hoursfollowing admission has been used to identify patients who are likely to have high hospital costs. Tierney and others demonstratedhowtheuseofanelectronicmedicalrecordsystemtocontrolordersforinpatientssignificantlyloweredpatient charges and hospital costs. In this situation the ordering of blood tests, medications, etc, was performed at the computerterminalbythemedicalofficersandthejustificationforrequestingeachtestwaspromptedbyremindersfrom the EMR.
6.12 Research Researchcostsrepresentasignificantcomponentofthehealthcarebudgetastheacquisitionofaccuratedataisdifficultandcostlyinbothtimeanddollars.Paynedemonstratedthecostandtimesavingsbenefitsoftheelectronicmedical record system Computer Stored Ambulatory Record (COSTAR) over the paper record when evaluating the effects of anti arthritic medications in hypertensive patients. The costs saving were in the tens of thousands of dollars and the time savings were measured in hundreds of person hours.
6.13 Epidemiology As chronic diseases become more prominent in modern health care, larger patient populations will need to be studied to detect variations in diseases and changes in health outcomes resulting from therapeutic interventions and the size of these populations make it impractical to undertake studies using existing paper-based medical record systems. Effective studies of these large patient populations will require new analytical methodologies to be created so we can harness all the information they contain.

Health Informatics and Management Information
78/JNU OLE
EMRsystemshavebeenusedtoidentifythosepatientswithhypertensionprescribednosteroidalanti-inflammatorydrugsthatarelikelytodeveloprenalinsufficiencyandidentifyclinicalfactorsthatpredictwhichpatientstakingdiuretics are likely to develop hypokalemia and ventricular ectopy.
6.14 Administration Data stored within the HELP clinical system has been used in the Utah Intermountain Health Centre to evaluate the costs and quality of care for a variety of medical and surgical procedures. The EMR provided information on variations in length of stay, surgical procedure time and costs for uncomplicated surgical resections of the prostate. This information was relayed to the medical practitioners who performed the operations in a range of institutions and they co-operated in altering their surgical techniques and procedures to reduce the mean length of stay and costs of routine Transurethral Resections of the Prostate (TURP). In the evaluation process it was found that certain preoperative procedures such as chest X-rays, were unnecessary if a patient had an uncomplicated medical history. The same clinical data generated from the patient care process is being used to measure and evaluate the effectiveness of Diagnostic Related Group (DRG) studies, and has led to a reduction in DRG costings. Similar hospitals not using a patient-basedEMRsystemhaveexpandingDRGandotherhealthcosts.ThisconfirmsHowardBleich’sobservationthat 90% of administrative cost data can be generated as a by-product of the patient care process.
To achieve these results EMR systems must provide standardisation of data recording so that data and information can be shared across institutions and internationally. Achieving the end points of EMR integration is not easy, howeversuccessfulimplementationshavebeencompletedandtheyprovideanswerstomanyofthedifficultiesfaced and how they can be overcome.
With the knowledge that established models of EMRs have been shown to improve the health care process, what is the recommended course for future EMR projects? Developers, project directors and users of clinical information systems must begin to share the experiences, and use existing and evolving software tools to reduce implementation costs. This will result in the most effective delivery quality health care.

79/JNU OLE
Summary Medical records in health care have relevance to patient care and health administration.•The medical record is the primary repository of all information regarding patient care, provide decision-support, •and be a tool for supporting and maintaining ancillary health care activities such as administration, quality assurance, research and epidemiology. Shortliffehasdefinedmedical(health)practiceasmedicaldecision-makinganditisrecognisedthatthereis•an integral relationship between medical decision making, the accumulation of clinical data, health care costs, patient outcomes, and the quality of care.Current medical record systems are predominantly hard copy paper-based models with or without variable •components of electronic data such as laboratory results and X-ray reports.Since the 1960s there has been a rapid growth in the technology used to support medical care and this has •resulted in the creation of enormous volumes of data and information that is available to assess and manage the delivery of health care.New and evolving technologies continue to produce and store large volumes of data and information for patient •care, but there only a few systems that provide information processing tools which support clinical decision making.It is recognised that information processing capacity of the human brain is limited in its ability to accurately •decipher this clinical data and information in a timely manner without errors.The use of predominantly manual, non-integrated medical records systems has led to increasing costs in patient •care and administration, decreased compliance with health care standards, inappropriate variation in health care delivery and possible negligent behaviour by health care providers.The amount of data presented to the physician per unit time is more than he can process without error. The •computer augments the physician’s capabilities and thereby reduces his error rate. It is very likely that the physicians in these studieswere simplyunable to detect all themultitudinous conditions specifiedby thestandards.Health care professionals and organisations should adopt the computer based patient record (CPR) as the standard •for medical and all other records related to patient care.
ReferencesHannan, J. T., • Electronic Medical Records, [Pdf] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_12.pdf > [Accessed 28 November 2012].Medical Web Experts, • What is EMR? Information to Improve the Patient Experience, [Online] Available at: <http://www.medicalwebexperts.com/blog/what-is-emr/> [Accessed 28 November 2012].Emedikon. 2010. • What is EMR? [Video Online] Available at: <http://www.youtube.com/watch? v=MOwML1N3TpM> [Accessed 28 November 2012].Emedikon. 2010. • BenefitsofEMR[Video Online] Available at: <http://www.youtube.com/watch?v=TiQ8c11dkU0> [Accessed 28 November 2012].Hovenga, E., Kidd, M., Cesnik, B. & Livingstone, C., 1996. • Health Informatics: An Overview, Australia. Skolnik, S. N., 2010. • Electronic Medical Records: A Practical Guide for Primary Care, Springer.
Recommended ReadingScott, T., Rundall, G. T., Vogt, M. T. & Hsu. J., 2007. • Implementing an Electronic Medical Record System: Successes, Failures, Lessons, Radcliffe Publishing.Carter, H. J., 2001. • Electronic Medical Records: A Guide for Clinicians and Administrators, ACP Press.Varshney, U., 2009. • Pervasive Healthcare Computing: EMR/EHR, Wireless and Health Monitoring, Springer.
Health Informatics and Management Information
80/JNU OLE
Self Assessment __________is a continuous process in which data is progressively accumulated, therefore the record must function 1. as a ‘pre-birth to post-death system that meets the requirements for any clinical setting-whether intensive care or primary care.
Health carea. Health/Medical informaticsb. Clinical informaticsc. Electronic Medical Recordsd.
Medical(health)practiceisdefinedasmedicaldecision-makinganditisrecognisedthatthereisanintegral2. relationship between __________, the accumulation of clinical data, health care costs, patient outcomes, and the quality of care.
health informaticsa. electronic medical recordsb. medical decision makingc. medical datad.
Current medical record systems are predominantly hard copy __________ models with or without variable 3. components of electronic data such as laboratory results and X-ray reports.
paper-baseda. technology basedb. software basedc. hardware basedd.
__________ is the storage of all health care data and information in electronic formats with the associated 4. information processing and knowledge support tools necessary for the managing the health enterprise system.
Health informaticsa. Electronic Medical Recordsb. Medical decision makingc. Medical datad.
Using the __________ McDonald demonstrated that the use of computer-generated reminders based on patient-5. specificlaboratorydataresultedinareductionofphysicianserrorsinthedetectionoflife-threateningevents
(HELP) Health Evaluation through Logical Processinga. (OCIS) Oncology Centre Information System b. (STOR) Summary Time-Orientated Record c. (RMRS) Regenstrief Medical Record Systemd.
_________ are now used as standard tools for patient care in the RMRS and other EMR systems used in hospitals 6. and ambulatory care environments.
Computer-generated remindersa. Machine generated remindersb. Logically generated remindersc. Paper based generated remindersd.
81/JNU OLE
In EMR the data is stored in _________ which provides for more consistent recording and ease of data entry.7. word formata. JPG formatb. PNG format c. coded formatsd.
__________ is a decision support tool where the computer is able to examine data and information stored within 8. theEMRdatabaseusingpre-definedclinicalrules,andidentifycertainconditionsthatrequireattention.
Introspectiona. Interceptionb. Interpretationc. Integrityd.
__________isoneofthedecisionsupporttoolsforusewithinEMRswhichprovidebenefitstohealthcare.9. Introspectiona. Interceptionb. Interpretationc. Integrityd.
A system of alerts is used routinely in the __________.10. (OCIS) Oncology Centre Information Systema. (HELP) Health Evaluation through Logical Processingb. (STOR) Summary Time-Orientated Record c. (RMRS) Regenstrief Medical Record Systemd.

Health Informatics and Management Information
82/JNU OLE
Chapter VII
National Strategy for Information Management
Aim
The aim of this chapter is to:
explain the national strategies framed for introduction of IT in health sector•
elucidate the concept the information intensive health services•
explicate the purpose of framing strategies in health care informatics•
Objectives
The objectives of this chapter are to:
explain the purpose of framing strategies in health care informatics•
elucidatethebenefitsofbusinessprocessre-engineering•
explicate the advantages of project management in health care sector•
Learning outcome
At the end of the chapter, you will be able to:
describethefactfindingtools•
understand various elements of an education and training strategy•
identify the challenges in introducing IT in health care sector •

83/JNU OLE
7.1 IntroductionInformation management in the health services has been with us ever since we have had health services! As soon as one records patient details, there is some, albeit elementary, need to manage information. The use of information technology (IT) to manage information is of much more recent origin. With the advent and widespread availability of affordable mainframe computers in the 1960s, the health services, along with other major organisations, quickly usedthemforalimitednumberoftasks-inthefirstinstance,mainlyforthepayroll.Inthebeginninginformationtechnology and computers affected relatively few administrative staff in the health services. Clinical and medical staff gradually developed their own departmental computing facilities and acquired the skills necessary to use computers as they went along.
In the last decade information, information management, and the use of IT to manage information affects over 90% of the workforce in health services. There is now multibillion dollars spend on IT in health services throughout the developed world. It is generally recognised that the health services are behind other sectors of business and industry (for example, airlines, service industries, some government departments) in the deployment of IT to assist in the management of information.
Education and training for the use of IT for information management has been relatively neglected, perhaps more so in the health services than in other sectors of the economy. But even outside the health services, for many decades educationandtrainingwasusuallythelastlineinthecorporatebudget;andintimesofcutbackandscarcityitwastheeducationandtrainingbudgetwhichsufferedfirst.
It is now a familiar cry that there is an enormous wasted investment in IT in all sectors of the economy, particularly in healthcare.StoriesaboutITequipmentlyingidleunderutilised,andinefficienciesinitsusearelegion.It’sparadoxicalthattheincreasingamountsspentonIT,accompaniedbyincreasingclaimsofITsuppliersaboutitsefficacyandcostbenefits,occursatthetimeofdocumentedstudiesonwastageandinefficiencies.WearestillwaitingforthedefinitivestudythatproveswithoutdoubtthatinvestmentinITiscosteffective!Atoneextreme,mostpeoplewouldagree that the airline industry today could not function without the deployment of computers and communication technologies;andmorerecentlythesamecanbesaidofsomemanufacturingprocesses.
However, in many other service industries, in government departments, in the administration of universities, andinthehealthservices,thebenefitsthathavebeenpromisedforsolonghaveyettobefullydocumentedandsubstantiated.
For many, in complex administrative environments, investment in IT is still an act of faith and the take up of IT and EDI (Electronic Data Interchange) is slow. We live in a world in which computers are regarded as a good thing, an indication of modernity, and a necessity for us all to know about. We have been told for a long time that everybody will be affected by computers during their life time. Until about thirty years ago it was generally accepted that the learning of Latin at school was a good thing. We were told that it would help us learn other languages, help with spelling, and all sorts of other goodies were paraded. But there was little evidence to back up these claims. UniversitiesdemandedthatallapplicantshadschoolleavingqualificationsinLatin.Suchdemandsareunthinkabletoday. The overselling and the over enthusiasm of the past decade for IT and computing will no doubt be unthinkable intwentyyearstime.InthefutureweshallnotinvestinITunlesstherearedemonstrablebenefitstobegained.Abetter educated and trained workforce will ensure that this is so!
In the health services the public knowledge that now exists, wasted millions of dollars on IT investment has had a beneficialeffect.ThereismorecautionaboutITinvestment,abetterplannedapproachtoITisabsolutelyessentialfor most of the healthcare workforce.

Health Informatics and Management Information
84/JNU OLE
7.2 The Information Intensive Health ServicesThe provision of health services has always been an information intensive activity. Medical and healthcare knowledge, dataandinformationcontinuetogrowatagreatpace;patientsgenerateinformationandmorepatientsthanevercontinuetobeseeneachyearinhospitalsandwithinthecommunity;themanagementofhealthcarecontinuestogrow in complexity.
Therearemanyfactors,bothwithinandoutsidehealthcare,thatareinfluencingthegeneration,capture,processingand storage, and use of information for healthcare management and for clinical practice, as well as for accessing healthcare requirements and meeting the increasing sophisticated information demands of patients, their relatives, and, indeed, the general public. Health promotion as an allied activity is also predominantly information intensive.
Activitiesandfactorsofthelastfewyearsthathavehadatremendousinfluenceuponthedevelopmentofnewinformation systems for healthcare include:
Resource allocation formulae •Cost centre and accrual accounting for costing and cost modelling •Relative Stay Index •DRGs, and AN - DRGs •PatientClassification:e.g.NurseDependency;HealthInsurance;NursingHomes(RC1)•Medicarebenefitscheme,andpharmaceuticalbenefitsscheme•Medical audit •Assessment of healthcare needs of populations •Performance indicators•Care Evaluation Program (CEP) •Clinical Indicator (CI) •Inaugural National Clinical Data Evaluation System (INCIDE) •Outsourcing/contracting. •Health data dictionary •Health information agreements between Commonwealth States •Development of a National Health Information Plan •
Performance indicators in medical audit, as well as assessment of outcomes, are all part of the new culture of quantifying activity and performance, both at the aggregate level and also in terms of individual performance. These activities form part of a new management culture which can only operate successfully with the aid of a new generation of information services. Many of the measures and performance indicators listed above are included in the Australian Council on Healthcare Standards (ACHS) Care Evaluation Program (CEP), which aims to improve the quality of patient care by measuring the processes and outcomes of patient care. Lawson and Callopy (1993) describe the progress made with the national Clinical Indicator (CI) and the CEP Inaugural National Clinical Indicator Data Evaluation System (INCIDE). All these measurements, indicators, and databases could have been recorded andconstructedbyhand,atleastinprinciple,beforetheadventofcomputersandinformationtechnology;butinpractice, it would have been impossible.
The long term value of the CEP and INCIDE systems (as indeed is the case with all performance indicators) is the potentialtoprovidefeedbacktohealthcareprofessionalsaboutlevelsandefficacyofpractice.Theultimatevaluetoboth practitioners and patients is the educational value of feedback: as McIntyre and Popper (1983) note “knowledge grows more by the recognition of error than the accumulation of new facts.” Healthcare professionals continue to be suspicious and resistant to new, so called, management information systems. Insights into the educational and training spin offs of new information systems have been played down. There are good reasons to support education and training programs aimed at the basics of data collection, storage, retrieval, and presentation, but if the programs can in addition address the spin offs for better and more informed practice, the value of information management education and training will be seen as essential, rather than desirable.
85/JNU OLE
Wheneducationandtrainingwasstillseenasanexpendableresourcethatcouldbedispensedwithindifficulteconomic times, this is just what happened. But when the skills, competencies, and knowledge in information management are seen to be part of the key ingredients of a successful healthcare strategy, training and education likewise are placed high on the corporate agenda.
Many senior managers in health have resisted the wide scale introduction of IT. But in recent years, in many countries, outsourcing and contracting of services (sometimes between sectors of the health services) have increased the perceived need for IT to facilitate the outsourcing and contracting processes. In the early days of outsourcing and contracting it soon became evident that inadequate information systems could be extremely costly.
Thereafter, senior management that was formerly cool towards the information management and technology (IM&T) movement and a new generation of information systems began to embrace them enthusiastically!
7.3 Why a Strategy? Strategies (of any nature) are often resisted by an organisation’s workforce. It is necessary in such cases to enumerate the reasons for developing, and subsequently implementing a strategy. Some attractions of a strategy are given below:
Enablesadetailedplanofactivitytobeagreed,facilitatesfinancialplanning,andallowsprogresstobeassessed•against objectives Assists in justifying expenditure of large sums •Provides a vehicle for publicity •Helps develop local ownership and motivation •Reduces the chance of duplicated effort and wasted resources •Provides coherence to a national, state, or international activity •Helps plan for future direction •
In many organisations the single most important aspect of a strategy is that it enables organisations to devote large amountsofmoneytospecificplans,andsometimestoobtainconsiderablefunds,whichnogovernmentdepartmentwould agree to allocate in the absence of a strategy.
7.4 Elements of an Education and Training Strategy A training strategy, in its most simple form, addresses the following factors:
The skills, knowledge and competencies required of healthcare workers •The existing distribution of skills, knowledge and competencies across the workforce •The training needs, ordered according to priority levels, for different groups of employees •Trainingplans,overtimeperiods;e.g.Immediate,middletermandlongtermtrainingplans•Delivery of training, both from within the health services, and also from outside •Types of training and education currently available •Evaluation of training and education •Evaluation of the strategy •Dissemination of information about the strategy •The development of a local training infrastructure •
Strategies and plans range from the very general through to the very detailed and explicit. Certainly, at some stage in the implementation of an education and training strategy it is necessary to produce a detailed assessment of training needs and existing provision, and a detailed plan for the local delivery of training and education. In large organisations local ownership and local plans are essential. The task is too large to be operated at a national/federal level. However, a general strategy provides guidance and motivation, and can be instrumental in the development of a local training infrastructure, and also in the allocation of both central government funds and local health authority funds.
Health Informatics and Management Information
86/JNU OLE
7.5 Preparing Staff for Information TechnologyThe health system is expanding its use of IT to complete tasks within the health system. To manage these changes, staff education, staff attitudes and the management of changes require addressing. There are many barriers in the path of Information Technology. The health system relies heavily on the visible print and paper culture. Biscoe (1986) states, the key to overcoming this are the recognition that computers merely act as a mechanism for the storage and retrievalofinformation.Otherfactorsthatinfluencethehealthsystemstemfromthefearoflosingcontroloverthepowerofknowledgeandconfidence.Tosucceed,computersneedtobeirresistible.
7.5.1 Staff Education ItisessentialtothesuccessofanITimplementationthatallstaffobtainssufficienttraining,toquellthefearoflosingcontrolandthelossofconfidence.Thehealthsectorhasrecognisedthis.Theeducationnotonlyencompassestraining in the new software, it also includes the introduction of new terminology and basic computer skills to all staff. On commencement of employment, new staff is introduced to computer terminology or jargon.
Terminologyeducationrelevanttothehardwareconfigurationinuseisprovidedfornewemployeesthroughtheorientationprogram,fore.g.terminalorclientserverenvironment.Thefirstsessiondoesnotrequirehandsonbythe participants and aims to alleviate some of the technophobia that relates to computer jargon. A second education session,involveshandsonexperiencefortheparticipants.Thissecondsessionintroducesfirsttimecomputeruserstoconceptsandterminology,specificallyrelatedtothehardwareenvironmentincludingtheloggingonprocedure.Switches and lights on a terminal and personal computer are described together with what these mean to the user. A practice session using the keyboard allows the users to put into practice what they have learnt.
Troubleshooting problems is also covered, for e.g. how to solve problems with printing and when to contact the Help Desk and what to tell them. Data security and privacy consideration, such as password security and detecting security violations are covered as are ergonomic and occupational health and safety issues that relate to computers. Advances in information technology provide exciting opportunities for education in the health sector Future courses must direct user education at several levels, the emphases being on course that provide practical, hands-on approach.
7.5.2 Change Change is continuous and necessary to respond to internal and external changes in technology, attitudes, organisational structures, policies, consumer expectations and many other internal and external factors. These factors initiate change. Change is becoming a more common event in the work place. The changes in technology in the past twenty years have been enormous. ‘Technology has realised such wonders as penicillin, open heart surgery and the birth control pill’. Changes in the size and cost of computers allow users to have a computer in the work place or at home. The changes in technology have occurred with increasing frequency and speed, ‘every new technology is a force of creative destruction’. The transistors displaced the vacuum-tube industry and videos have displaced the movies. It is,ofcourse,futiletofightthefactthatchangeisgoingtooccur.
External forces for change like government cutbacks, rapidly increasing costs of labour, and services can impact on the health system. Internal forces, particularly from new strategies, technologies are pressures for change. Service changesinfluenceorganisationalchanges.Someservicechanges‘involveradicalreconfigurationoftheservice’.For example, the Domiciliary Midwifery Program has remodelled obstetric nursing, changing its focus from the traditional health institution to caring for the patient at home. The introduction of fresh business ideas such as day surgery has radically changed the face of health services by decreasing the length of stay. This has relieved some of the time pressures that are prevalent in society. ‘All of these forces for change come about because of changes in the business requirement’.
Many changes in the health system are coming about because of the development of an increasing number of clinical computing systems. The systems range in size from a PC stand alone to a full scale hospital information system. Recognition of the changes by the health system is already evident. The technology revolution has traditionally broughtintechnologytofitaroundthework.Nowworkpracticesneedtochangetomaximisethepotentialbenefitsof technology. In conjunction with Information Technology changes to the health care system can be radically rethought, from the current work practices to the delivery of service.
87/JNU OLE
7.5.3 Attitudes Resistance to change has not lessened with the introduction of Information Technology. Indeed the pace of the technology revolution has heightened fears that users are becoming subservient to machines and stiffened user resistance to technology. Detecting resistance to a computer environment may be noticed by a drop in service, failure to meet service requirements, increased absenteeism, high staff turnover, complaints and low morale and a reluctance to learn new job skills. Resistance to information technology at the managerial level can be that managers feel hemmed in by information technology, and that the computer systems limit their choices because they are central to important decision making.
Theuseofbehaviouralterationstrategiesfacilitatesthechangesinattitude.Thefirstoftheseisthedirectivechange,imposed by management. Compulsory sessions performed that all staff are to attend. Resistors co-opted, play an active role, for example, identifying problems and planning solutions. Hussain et al. 1988, state that a climate receptive to change is vital when new information technology is being introduced to an organisation. Without human cooperation, the new technology is unlikely to live up to its productivity potential.
7.5.4 Organisational Culture The philosophy that underlies organisation policy determines organisational culture. There are three levels of organisational culture and each has its own interaction with the organisation. Every organisation, regardless of size,hasaformalandclearlydefinedsetofrelationships.Thefirstlevelofanorganisation’scultureisitsartefactsand creations. This includes the physical layout of the premises, the technology, the signs, rituals and stories. The second level of organisational culture consists of the values.
Thesebeingthesenseofwhatoughttobe,asdistinctivefromwhatis.Thethirdleveloforganisationalculturereflectsthe basic underlying assumptions. These assumptions develop when organisational values become entrenched, taken for granted, and assumed to be unchanging. To achieve an understanding of the organisation’s culture there is a need tocollectinformation.Efficientandeffectivecommunicationisarequirementforthegatheringanddistributionofinformation.
7.6 Fact Finding Tools The most important element of an information system is people are more important than anything else. People want inclusion regarding things that are going to affect their work. ‘Consulting the staff on decisions’ prior to implementation is the reason for interviewing employees. As employees are most knowledgeable about their work, they have many good ideas that need acknowledgement and respect. In this process one needs to determine who performs the work, what and when the work is being done, where the information goes, why does it happen that way, and how complete it is.
There are many different evaluation tools employed to affect the gathering of information. There is no single source that describes in detail the steps and numerous tools available to help the investigator carry out and interpret the documentation collected some of the tools available are:
Samplingexistingdocumentation,forms,andfiles•Research and site visits •Observation of the work environment •Interviews and group work sessions •Time - motion analysis •Personal record of activities •Subjective evaluations•
Thedocumentationrequiredtogainanunderstandingofworkflowincludesdocumentsthatdescribethebusinessfunctionbeingstudied.Thesedocumentsmayincludepolicymanualsthatplacerestraintsontheinformationflow,completed forms that represent transactions at various points of the process, standard operating procedures, job descriptions,taskinstructionsfromproceduremanualsthatspecifyday-to-dayoperations.Thesecondfact-finding
Health Informatics and Management Information
88/JNU OLE
tool includes the researching of the processes. This involves visiting other sites, other companies or departments that have completed implementation to assess potential for implementation in the health system. The objective of the visit is to document the delivery of patient care and monitoring quality of delivered patient care (IRMC - Nursing Consultants 1992).
Observance of the work environment is one of the most effective tools for data collection and for obtaining an understandingoftheworkflows.Theuseofthistechniqueistovalidatedatacollectedthroughthesemethods.Complex tasks are often difficult to explain clearly.The use of observation to identify the complex tasks ofworkflowalleviatesthedifficultyofclearoralexplanation.Atthistimethecollectionofdatadescribingthephysicalenvironment,suchasphysicallayout,traffic,lighting,noiselevel,etcwillcompletetheobservationstudy.Workflowsidentify how and by whom the system is used. How much time is spent using the system? Before commencing any observation permission from the appropriate supervisor or managers is obtained. Inform the people that you are intending to observe and state the purpose of the observation. There are three rules to strictly follow when observing workflow.Theseare:
Do not under any circumstances interrupt individuals at work•Do not focus on trivial activities •Do not make any assumptions •
Interviews are another beneficial and often used fact-finding technique.The purpose of interviews is for factverification and clarification ofworkflows.To generate enthusiasm and get the user involved. Identify userrequirements and solicit ideas and opinions from users. The structured interview has some planned questions and others are spontaneous to clarify the answers provided by the interviewee.
Time - motion analysis provides a direct measurement of activities. There are a number of work measurement techniquesavailable.Thebenefitoftimeandmotionstudyisthattheseprovideaccuratetimevaluesregardinghowlongaqualifiedworkershouldtaketoperformtheselectedactivitytoachievethedesiredresult.Thedisadvantagesoftimeandmotionstudiesarethattheyrequirequalifiedpeopletoconductthem.
Alternatively the self reporting of activities and the time required to perform them rely heavily on the subject’s memory and are prone to error. This method is a subjective evaluation of time estimates. Self reporting and the use of questionnaires are useful for job analysis purposes and relatively easy to administer, interpret and obtain valuable information concerning work activities. Such methods provide imprecise measurements of work activities but the useofquestionnaires inconjunctionwithoneormoreof theother factfindingmethods,doprovide importantinformation. It is essential that the user provides the most appropriate and relevant information using one or all of the methods discussed.
7.7 Business Process Re-engineering The health system is endeavouring to take full advantage of the potential offered by new technologies. One method that provides an opportunity to radically rethink health care delivery is business process re-engineering. This uses an enterprise wide approach to identify key business outcomes and to determine both the value and the quality of services Business process re-engineering approaches projects from a three pronged viewpoint:
the personnel•the technology•the process itself•
Business process re-engineering controls change at three levels in the organisation. The sponsor levels determine the scope of the changes, the executive of the organisation sponsors the enterprise-wide changes Enterprise wide changes initiated by the executive of the organisation are usually components of the organisational strategic plans. A single executive steering committee oversees the enterprise wide projects and address issues that cross departmental boundaries. Process improvement changes proposed by the teams involved with change, for example, departmental managers or supervisors. Process improvements initiated can improve a single process or a group of interrelated processes.
89/JNU OLE
Finally, the users initiate the task level changes, with some management co-ordination. Task level changes are creative responsestotheneedtogetthejobdone.Theseareoftensubtlechangesormodificationstoexistingworkflows.One or more objectives drive the re-engineering effort. The organisation drives each objective linked to the business goal. The common criteria for re-engineering objectives are that they support the organisation business plan. The objectives reduce time in completing tasks, reduce the number of staff to complete the task or establish a new service. Theyalsoimprovestandardsandthequalityofaprocessandorimproveservice.Putsimply,workflowcompletestasksthewaytheorganisationexpects.Therearethreemaintypesofworkflowcontingencies.Theorganisationmustchoosethemostappropriateworkflowsystemtoachieveitsobjective.Thefirstoftheseworkflowsisthesequentialworkflows,whichcompletetheworkinastrictorder.Thesecondworkflowisthepooledworkflowsthatareunrelatedbutcontributetotheworkgroupobjective.Thethirdworkflowisthereciprocalworkflowsthatproduce an output that is an input for other jobs.
The design of work should have two objectives. Functional effectiveness, that increase the productivity and to enhance the effectiveness of work. •Human values, focussing on the maintenance or enhancement of job satisfaction and health and safety. •
The two objectives closely relate to one another and to achieve one without the other is virtually impossible. The question is how to design work that will achieve these objectives.
It is impractical to consider the whole organisation can be re-engineered at one time. It is therefore necessary to increment the changes. There are nine steps to business process re-engineering.
Identify possible efforts for business process re-engineering •Identifyworkflowcategoriesandconducttheinitialimpactanalysis•Selectaneffortanddefinethescopeofthechanges•Identify business and work processes •Definealternatives,simulatenewworkprocessesandworkflowswithinthedepartment•Definepotentialimpactofeachalternative•Select best alternative•Implement the selected alternative update the positioning baseline models and information•
Once there is the need to commit any plan to paper a suitable notation must be chosen. Plans can be drawings, specificationsorflowdiagrams; thesemustallberegardedasameansofcommunicating information.Severalnotational methods and languages have been devised for timescale planning.
7.8 Project Management Project management functions are, planning, organising, controlling and leading. The planning function states the activities, estimates how long it will take, and projects what it will cost. The organising function staffs the project team and brings together team members, users, and managers to achieve the project plan. The controlling function monitors progress reports and documents deliverables. It compares plans with what actually happens. Two popular project management tools are the program evaluation and review technique (PERT) and Gantt, named after Henry Gantt. A PERT chart estimates, schedules and controls numerous interdependent tasks. The PERT chart determines the minimum amount of time required to complete the project or a phase. A Gantt chart is a bar chart that illustrates phases or tasks. On the left hand side of the Gantt chart the tasks or phases are shown, whilst the number of days, weeks, months are shown across the top of the chart. The Gantt chart compares planned performance with actual performance, to determine whether the project schedule is on time. Gantt charts are simple to understand, however, they fail to show relationships with interrelated tasks. This is why the Gantt chart schedules a complete system project, while the PERT chart schedules interrelated tasks.
Records kept by the project management, inform users how the business process has changed. These records will detail the design of the change and construction of the changes. For ease of access and physical security the project library houses this documentation.
Health Informatics and Management Information
90/JNU OLE
The aim of the project leader is to “bring the project to a successful conclusion.” “Successful” being, giving the user what they want, working on time and to budget. Project leadership is out of the scope of this chapter, except in so far as it affects business process re-engineering.
TheroleofconfidantisaproperonefortheBusinessprocessengineerandcanbeuseful,providedtheBusinessprocess engineer performs it well. Affecting a relationship, where users can approach the Business process engineer anddiscussmattersinconfidenceconcerning,forexample,mistakesmade,canonlybenefittheproject.
There are two types of delegated authority that can be given to theBusiness process engineerfirst is formaldelegation.
Authoritytoeffectsmallchanges;(smalldefinedbycostandresources)•Thedeploymentofresourceswithinwelldefinedlimits•Initiatingstudiesandformulatingcostbenefitanalysis•Halting any changes that are established as a waste of effort•
The second type of authority is informal delegation. The effect of informal delegation is to protect the project leader from unnecessary stress and an excess of information, by the Business process engineer reporting to the project leader on a regular basis.
ThetaskofidentifyingchangewillinevitablycomethewayoftheBusinessprocessengineer,particularlytofulfiltheroleofconfidant.Ifachangeistoolargeorwillclearlyuseasubstantialamountofresourcesevenbeforetheidentificationofcostbenefits,thenthebusinessprocessengineersubmitsabrief.Thisbriefistoestimatetheamountof time and resources to complete the analysis before commencement on the changes.
The Business process engineer will at times act as an instructor, carrying out a great deal of informal education and training for users and their departments. Thorn (1989) states that staff require adequate training and gain the skills and knowledge required to perform the jobs changed by the redesign. If the organisation has not had access to computers prior to the implementation then a new education program, as outlined previously, will need to be developed. The Business process engineer needs to continue to perform walk-through and subsequent follow up discussions with user departments and or individual users.
7.9 Hardware Installation Wehavediscussedatlengththeprocessforchangeinrelationperformanceofwork.Thefinaldiscussionwiththeuser is where to install the hardware for the new system. The involvement of the Occupational Health and Safety Officer is essential to thisprocess as theywillprovide theexpertknowledgeconcerningergonomically soundplacementofthehardware.TheBusinessprocessengineerwillhavecompletedstudiesoftheworkflowsandthecollection of data in the earlier phases of implementation. Securing the change decisions as close to the action as possible. That knowledge will also assist in the appropriate placement of the hardware. Without the essential aspect of this process, communication, the enabling role of information technology becomes redundant.
In summary, when an organisation is looking at changing, the work environment and work practices, the major tool usediscommunication.Businessprocessreengineeringfitswiththecontinuousqualityimprovementconceptwherecommitment for change must be fully supported the executives. A system for informing everyone about any planned changes needs to be set-up. Information is ideally disseminated on a regular and frequent basis. This will ensure that the organisation is up to date and really knows what is happening. It is important that the business process engineer performs regular visits to the areas where change is having the greatest impact. This will ensure the involvement of the staff in the decisions that need to be made, for these are the people who will be using the system. The provision of training to these people will ensure that they receive adequate training to gain the new skills and knowledge. Providing the ability to work in the changed work environment and perform the job affected by change. Finally, the changes made require monitoring and evaluating to ensure development of best work practice. In so doing, learn fromchanges,bothsuccessfulandfailures.Theexpectedoutcomesfrombusinessprocessengineeringare,first,faster delivery of patient care services, second, a higher quality of care. The third expected outcome, reduced costs andfinallygreaterpatientandemployeesatisfaction.
91/JNU OLE
SummaryWith the advent and widespread availability of affordable mainframe computers in the 1960s, the health services, •alongwithothermajororganisations,quicklyusedthemforalimitednumberoftasks-inthefirstinstance,mainly for the payroll.In the last decade information, information management, and the use of IT to manage information affects over •90% of the workforce in health services.Education and training for the use of IT for information management has been relatively neglected, perhaps •more so in the health services than in other sectors of the economyThe long term value of the CEP and INCIDE systems (as indeed is the case with all performance indicators) is •thepotentialtoprovidefeedbacktohealthcareprofessionalsaboutlevelsandefficacyofpractice.The ultimate value to both practitioners and patients is the educational value of feedback: as McIntyre and Popper •(1983) note “knowledge grows more by the recognition of error than the accumulation of new facts.”In many organisations the single most important aspect of a strategy is that it enables organisations to devote •largeamountsofmoneytospecificplans,andsometimestoobtainconsiderablefunds,whichnogovernmentdepartment would agree to allocate in the absence of a strategy. The changes in technology have occurred with increasing frequency and speed, ‘every new technology is a •force of creative destruction’.Domiciliary Midwifery Program has remodelled obstetric nursing, changing its focus from the traditional health •institution to caring for the patient at home.Hussain et al. 1988, state that a climate receptive to change is vital when new information technology is being •introduced to an organisation.Everyorganisation,regardlessofsize,hasaformalandclearlydefinedsetofrelationships.•Project management functions are, planning, organising, controlling and leading.•The planning function states the activities, estimates how long it will take, and projects what it will cost.•The organising function staffs the project team and brings together team members, users, and managers to •achieve the project plan.The controlling function monitors progress reports and documents deliverables.•
ReferencesBrittain, M. J., • National Strategy for Information Management, [Pdf] Available at: < http://www.achi.org.au/docs/HNI_Book/Chapter_23.pdf>[Accessed 28 November 2012].Feeny, P., • Preparing staff for information Technology, [Pdf] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_24.pdf>[Accessed 28 November 2012].2012. • Introducing Health Informatics, [Video Online] Available at: <http://www.youtube.com/watch? v=5gKspYFAc9Q>[Accessed 29 November 2012].2012. • Introduction to Health Informatics, [Video Online] Available at: <http://www.youtube.com/watch? v=leWE5fx8aZs>[Accessed29November2012].Borycki, M. E., 2011. • International Perspectives in Health Informatics - Studies in Health Technology and Informatics, IOS Press.Wager, A. K., Lee, W. F. & Glaser, P. J., 2009. • Health Care Information Systems: A Practical Approach for Health Care Management, John Wiley & Sons.

Health Informatics and Management Information
92/JNU OLE
Recommended ReadingWinter, A., Haux, R., Ammenwerth, E., Brigl, B., Hellrung, N. & Jahn, F., 2010. • Health Information Systems: Architectures and Strategies, Springer. Hovenga, J. S. E. & Mantas, J., 2004. • Global Health Informatics Education, IOS Press.Steele, A., 2002. • Medical Informatics Around The World: An International Perspective Focusing On Training Issues, Universal-Publishers.

93/JNU OLE
Self Assessment Activitiesandfactorsofthelastfewyearsthathavehadatremendousinfluenceuponthedevelopmentofnew1. information systems for healthcare include __________.
Care Evolution Program (CEP)a. Care Evaluation Program (CEP) b. Care Revolution Program (CRP)c. Care Resolution Program (CRP)d.
______ aims to improve the quality of patient care by measuring the processes and outcomes of patient care.2. (ACHS)Australian Council on Healthcare Standards a. (IT) Information Technologyb. (EDI) Electronic Data Interchangec. (INCIDE) Inaugural National Clinical Data Evaluation Systemd.
The long term value of the CEP and INCIDE systems is the potential to provide __________ to healthcare 3. professionalsaboutlevelsandefficacyofpractice.
valuable insighta. guidance b. feedbackc. complaintsd.
As __________ are often resisted by an organisation’s workforce, it is necessary in such cases to enumerate the 4. reasons for developing, and subsequently implementing a strategy.
technologya. rulesb. regulationsc. strategiesd.
__________ is continuous and necessary to respond to internal and external changes in technology, attitudes, 5. organisational structures, policies, consumer expectations and many other internal and external factors.
Changea. Computersb. Consistencyc. Contingencyd.
__________ has remodelled obstetric nursing, changing its focus from the traditional health institution to caring 6. for the patient at home.
(IT) Information Technologya. (EDI) Electronic Data Interchangeb. (INCIDE) Inaugural National Clinical Data Evaluation Systemc. (DMP) Domiciliary Midwifery Programd.

Health Informatics and Management Information
94/JNU OLE
The use of __________ strategies facilitates the changes in attitude.7. behaviour alterationa. behaviour improvement b. psychology alterationc. counselling d.
Thefirstlevelofanorganisation’scultureisits__________whichincludesthephysicallayoutofthepremises,8. the technology, the signs, rituals and stories.
staffa. unionb. artefacts and creationsc. managementd.
Which of the following are the requirements for the gathering and distribution of information? 9. Efficientandeffectivecommunicationa. Efficientandeffectivetechnologyb. Efficientandeffectiveemployeesc. Efficientandeffectivemechanismd.
__________ of the work environment is one of the most effective tools for data collection and for obtaining an 10. understandingoftheworkflows.
Securitya. Cleanlinessb. Observancec. Privacyd.
95/JNU OLE
Chapter VIII
Health Informatics in General Practice
Aim
The aim of this chapter is to:
explain the scope of health informatics in general practice•
elucidate the variability of primary care practice style•
explicate four major components of practice management•
Objectives
The objectives of this chapter are to:
explain the concept of practice management•
elucidatebenefitsofcomputerisingthemedicalrecord•
explicate the concept of real time information access•
Learning outcome
At the end of the chapter, you will be able to:
describe the four major components of practice management•
understand the importance of clinical records•
identify the areas where there is a need for medical education •

Health Informatics and Management Information
96/JNU OLE
8.1 IntroductionThe aim of this chapter is to describe the scope of health informatics in general practice. In so doing four principal organisationalstructuresingeneralpracticeisidentified,theneedtodocumentmedicalrecordsdescribed,andtheundertakingofresearchingeneralpracticeisexplainedtogetherwiththebenefitsassociatedwithusinginformationtechnologyforthispurpose.Manyoftheprinciplesofpracticemanagement,documentationandresearchidentifiedin this chapter apply equally to other types of community health practices.
General Practice forms the core of patient information management in primary care and covers a broad range of issues. The general practitioner or family physician must care for all patients who present, treating all ages, socioeconomic classes, ethnic backgrounds, and states of health. The information presenting to the doctor is often undifferentiated resultinginclassificationdifficulties.Thereisusuallymorethanoneproblempresentingatanencounterrequiringa comprehensive approach to information gathering. The family doctor needs to maintain a longitudinal record of the patient’s history with the ability to succinctly summarise the record if the patient moves to another area. There canbelegalrequirementstokeeprecordsforspecifictimeperiods.Thismayrequireduplicationofinformationifa patient wishes to attend another practitioner.
8.2 Relationship to other Health Workers General Practitioners relate to almost all other personnel in the health area to a greater or lesser extent. Patients may attend their family doctor for general medical care, but attend primary care clinics with special interests such as Women’s’ Health clinics, Family Planning clinics, Pain clinics, or Sports Medicine Clinics. Communication between community nurses, paramedical staff such as physiotherapists or podiatrists, pharmacists, dentists, counsellors and alternative medicine practitioners, demonstrate the range of communication which occurs between primary health care workers.
Communication also occurs between the primary care doctor and secondary and tertiary care health workers. Communication between specialists and primary care doctors forms a major component of health information communication for the primary care doctor. This may be directly to the specialist as the treating doctor, to a secondary referral hospital such as a local mental health clinic or geriatric after-care hospital, or to the major tertiary teaching hospitals both within and outside the local community. Much of this information is in the form of admission assessments and discharge summaries.
The secondary referral centres of diagnostic imaging and pathology, transfer information with the primary care physician on a daily basis. Much energy is expended in primary care dealing with this area of health informatics.
8.3 Variability of Primary Care Practice Style Clinics operate in a range of different administrative structures. The style of a primary care practice relates to the method by which it attracts funds. Clinics can be owned by doctors, funded directly from government expenditure, funded from hospital budgets, or owned by non medical commercial organisations.
Fee payments for patient primary care services can be either the direct responsibility of the patient, the government, or the hospital. Patient fees may involve third parties such as governments, health insurance agencies including work related insurance claims or primary care health claims associated with road accidents. These organisations may be responsible in part or all of the accounts on behalf of the patient.
As funding arrangements vary, so can the style of practice. Episodic care is more appropriate to accident and emergency departments provided by hospitals. Comprehensive continuous care is a feature of the traditional family practice or the hospital outpatient clinics. Community clinics, funded through local or regional governments, are able to offer a public health perspective. These clinics are likely to employ nurse practitioners and other paramedical staff such as social workers, physiotherapists and health educators. This clinic style encourages group education and isbetterabletoassistthesociallydisadvantagedandpeoplewhosefirstlanguageisnotthenativetongue.
AnalternativesystemforgeneralpracticefinancialmanagementisthatofthefundholdingstructurebeingtrailedinEngland.Thisplacesthefinancialresponsibilityfortotalpatientcareinthehandsoftheprimarycareproviders.

97/JNU OLE
The principal organisational structures in primary care are practice management, clinical record keeping, clinical research and medical education.
8.4 Practice Management Practice Management has four major components in the General Practice setting: Patient Billing, Appointments, Practice Administration and Electronic Tools.
8.4.1 Patient Billing Eachstyleofgeneralpracticewillhaveitsownpatientbillingmethod.Thishasbeenthefirstareapracticeshavetaken to computerise. In a recent Australian survey on the attitudes of general practitioners to computerised medical records, 35% of general practices were using computers in the practice. Of these 78% were using word processing functionsand63%wereundertakingfinancialmanagement.ThisisinlinewiththeuptakeofcomputeruseinSingapore where between 30 - 50% of practices have computerised for routine practice management activities. The UK experience differs in this regard as patient billing does not fall within the province of the family doctor but 50% of practices are using computers in an administrative capacity.
Originally the medical packages were adapted from off the shelf accounting systems, but it was soon realised themodificationsrequiredwereextensiveforthegeneralpracticeenvironmentorthesystemfailedtosatisfytherequirements of the practice. Modern systems software now has been purpose written for the style of practice accounting. A good accounting system should be structured on a Clinic Master Patient File. Every member of each family should be individually listed. Each patient should be able to have multiple account types depending on their reason for presentation. An example would be a patient attending as a member of a family with a parent as the account payer, as an individual, as a patient funded under a direct account to the government, as a work injured memberorasapatientrequiringaninsurancereport.Muchflexibilityisrequiredwithintheaccountingsystem.Any system selected by a practice will need to consider ease of use, as this will determine the amount of time taken byofficestafftotrainnewandrelievingstaff.Abusypracticeneedstobeabletogiveimmediateaccounts,receiptpayments over the counter and resolve account queries. Costs of stationery need to be determined as some systems rely on expensive pre-printed stationery while others enable the use of plain paper.
A computerised accounting system can form the basis of a general clinic patient register and enable the use of patient demographics. An age/sex register can be developed and from this age/sex register preventive care and recall programs can be developed.
8.4.2 Appointments Theuseofcomputerisedappointmentshasenabledgreaterflexibilityintotheorganisationofreception.AppointmentscanberunfromtheMasterPatientIndex.Thisenablescorrectidentificationoftheparticularpatientandtheappropriatehistorypulledinreadinesspriortothepatientattending.Newpatientsarereadilyidentifiedensuringextraallottedtimeif necessary. Cancelled appointments can be removed and logged and the appointment chart will remain uncluttered byalteredappointments.Clarityoftypingversushandwritingfurtherreduceserrorsofidentification.
Some appointment systems are able to time when a patient arrives and give information on waiting room times. This can assist all members of the clinic with the problem of those visits running over time and with the management of the ‘drop in’ patient.
For systems using computers in the consulting room for clinical records, the appointment system can be integrated andeliminatetheneedforthepaperrecordanditssundryretrievingandfilingtasks.Thisisamajortimeandcostsaving in the general practice environment releasing the receptionist for other activities. In the integrated system, the clinician has ready access to the appointment system and is able to keep abreast of changes to the appointment list. Afurtherbenefitofanetworkedormultiusersystemistheflexibilityofanystaffmembertoanswerthetelephonecall when an allocated member has become preoccupied with other tasks.
8.4.3 Practice AdministrationThe administrative tasks of a modern general practice have become more complex over recent years and in order tomanageapracticeefficientlytightcontrolneedstobemaintainedonincomeandexpenses.

Health Informatics and Management Information
98/JNU OLE
Day end procedures TheDayendproceduresforeitheramanualorcomputerisedofficeincludeadailylistofpatientconsultations,account status of each consultation, receipts paid to the practice that day, and the banking report for the day or period including that day. A similar series of information could be generated per doctor, and per branch practice. Similarly lists of clinical services can be produced.
Month end procedures ThereportsgeneratedforMonthEndshouldalsobeabletobegeneratedoverapracticedefinedperiod.ThisEOMprocess should print statements to all account holders. A facility for tracking overdue debts should be instituted and form part of the EOM procedure.
Clinics may choose to include service audits in their EOM function and others use the EOM as a time to generate recall letters to patients for due clinical services. Computerisation can enable these additional EOM functions to besetautomaticallygreatlyassisting thepractice incomprehensivelymanagingboth thefinancialandclinicalresponsibilities of the practice.
Service item maintenance General practices are required to document the services performed within a consultation by means of a service item coding system. Each country has its own government determined schedule for fee paying to clinics, hospitals or individual patients. These schedules are updated regularly and the general practices must upgrade their own lists as changes occur. Computerisation of the Item Service database enables clinics to audit their practice and their individualdoctorsforservicesperformed,comparepractitioners’practiceprofilesanddeterminefeesgeneratedperservice type or per doctor or clinic.
Batching Practices which directly bill the government for an individual consultation (fee for service), are required to prepare them in a batched format to the responsible agency for processing and payment. Accounting systems need to be able toperformthistaskefficiently.Computersdealwiththistaskmostefficiently,informingaccountingstaffwhentherequired batch number is reached, calculating the total moneys owing and maintaining a ledger of moneys owing and moneys receipted. Each doctor will require his own batch number and the computer should be able to allocate the particular direct bill payment to the individual doctor.
Salaries General Practices are required to manage the salaries of their staff, both medical and non medical. This may be a task performed by the practice manager or in a smaller practice by one of the principals. Payroll including taxation, superannuation, holiday leave pay, work cover insurance and where required payroll tax can be performed as a manual bookkeeping task or can be managed using a payroll computer program which may be integrated with the clinic accounting system in the form of a practice ledger.
Stock control Larger practices undertake a formal stock control and document items purchased and items utilised. This may be performed as either a manual or computer task. Larger organisations such as hospitals have sophisticated computerised stock control systems.
8.4.4 Electronic Tools By far the most useful tool in use in general practice today is the telephone. This piece of technology has changed the way information has moved across the health community. Recently the facsimile (fax) machine has further extended the use of this telephone system enabling the transfer of the printed word, either directly or through the computer to anywhere in the world. The introduction of the computer, initially in the form of a dedicated word processor, has further increased the scope of how information is managed in primary care. Word processing also occurs within anygeneralpracticeofficesparticularlyintheformoflettersofreferral,medicalreports,andclinicalnotes.Useofthe mail merge feature can generate recall letters.

99/JNU OLE
Practices with multi-user networked systems can use the feature of in house electronic mail or messaging service (E-Mail). These clinics are able to leave messages electronically for clinic staff. General practitioners have a high interest in using this facility.
8.5 Clinical Records Some of the issues concerning the computerised medical record as it relates to general practice are noted here. The development of a computerised medical record which can replace the paper record has eluded many a medical record developer.Whyitthatdoctorisquitereadytocomputerisetheirofficebutnottheirconsultingroom?Arecentsurveygives us some insight into the attitudes of the doctors in Australia to computerisation. This study revealed a high degreeofconcernwiththeconceptofcomputerisingtheconsultingroom;despitethefact30%wereperformingword-processing tasks at home. Manual systems were considered adequate and there was little understanding of benefitstobegainedfromacomputerisedmedicalrecordsystem.SimilarlyintheUnitedKingdom,90%ofprimarycare physician’s work in computerised practices but only 50% use the computer for recording progress notes.
There are three major reasons for creating medical records: Aide-Memoir: This is to refresh our memory of the past consultation. It may be adequate for another doctor •touseoritmaysimplysufficeasamemoryjogforthedocumentingdoctor.Ifhandwrittentheremaybelittledecipherable to any other clinician. This form of record is gradually becoming less used. Patient care: Managing patient care has increased in complexity. There is now more health workers involved in •an individual’s care. Diagnosing has become more sophisticated, often depending on test results to determine a diagnosis. There is an ever increasing number of drugs with their various functions and side effects which need to be considered. Doctors are being encouraged to practise proactively requiring recognition that a patient should have particular preventive services, or certain routine pathology performed. This creates a heavy demand on the doctor to have the information readily available at the time of the consultation for optimum health care. The paper record struggles under this demand. Legal documentation: The patient’s medical record needs to be able to serve as a true historical document of •the consultation. The courts have often accepted the hand written paper record as the doctor’s true record. It is necessary for the electronic record to demonstrate it is a true representation of the patient’s care. Electronic records need a method of demonstrating whether information has been altered after the initial input, what changes have been made, and the ability to produce the original documentation. These issues are addressed in the more sophisticated electronic record packages with date and time signatures.
8.6 Benefits of Computerising the Medical Record Information retrieval is the major reason for computerising the medical record. Retrieval is used for rapid real time access of clinical information, practice auditing and research. To retrieve information the data must be collected inastructuredformat.Thiswillentailsomedegreeofcodingandclassification.ThemostfrequentlyusedcodingsystemsusedforprimarycarearetheInternationalClassificationofPrimaryCare(ICPC),InternationalClassificationofDisease,NinthRevision,ClinicalModifications(ICD-9-CM)(UnitedStatesNationalCentreForHealthStatistic1980), and the READ codes. These coding systems are being mapped to each other so that the issue of which coding system used is not of great importance. Of more importance is the user interface.
8.7 Real Time Information Access To decide what information needs to be accessed in real time one needs an understanding of the information that is collected in the medical record. Patients have information related to their registration including such details as their name, address, and telephone number, date of birth, sex, social security number, account status, medical insurance status, and Medicare number. The primary care doctor can utilise any combination of this registration information on documents, forms and prescriptions
A patient health summary can provide the doctor with a precise during a consultation. This information could include social information, family history, allergies, past history, life risk factors and current medial ills and medications. As this is computer based, changes to data can be readily updated giving a clear picture of the patient’s current health and past history.

Health Informatics and Management Information
100/JNU OLE
Computer programs have been designed to manage preventive care with on screen reminders for anticipatory care and the facility to produce mail merge recall letters for those patients who have not attended the practice and wouldmisstheirscreenprompts.Thesesystemshavebeentrialledandfoundtoincreasetheuptakeofinfluenzavaccinations and papanicolaou smears.
A computer program which includes a Problem Orientated Medical Record (POMR) structure (Weed L Case Western Reserve Press) can provide a list of current problems readily updated when the patient’s history is altered. Systems incorporating a computerised script writer can keep a database of current medications, and rapidly provide the history of past medications. Checking for patient allergies should reduce the inadvertent prescribing of allergic drugs, by providing an onscreen warning to the doctor. Results of tests ordered can be incorporated into an associated database.
This information can be presented by test, by date or by problem in real time. Some systems can present this information in a graphical format on a time scale. For example blood glucose levels or blood pressure levels can be plotted against time. General practice information systems can include databases of other providers. These providers may be referring specialists, hospitals, paramedics, or companies. Reports to these sources can be documented in the system, and if created by a word processor integrated into the computerised record, and is available for ready reference. Similarly database entries can be made for reports received. This may be by summary entry, by fax or scanning with indexing for access.
8.8 Research by Practice Audit Research in Primary Care can be performed by practice audit and by formal research projects such as clinical trials.
Audit functions Practice audit can be performed manually or by computerisation. Manual audits are usually based on sampling practicepopulationsandmayrequiretheskillsofaresearchofficer.Theyaretimeconsumingandconsequentlyperformed infrequently. Computerisation of the clinical record opens a new dimension to practice audit. Whole practice populations can be included with a range of inclusion and exclusion criteria. Practices can use audits for a number of purposes.
Patient care management The principal purpose is to improve patient management. The availability of a new diagnostic test for a particular condition may require the practice to know which patients have this condition and arrange to communicate with thesepatients.Newvaccinesforpatientswithparticularriskscanbeidentifiedandnotified.
Preventive care management Practices are now being required to be more proactive in their approach, taking some responsibility for ensuring thosepatientsoverdueforcertainpreventiveservicesarenotified.Fromanauditprogrammailmergeletterscanbecreated and personalised letters of invitation can be produced.
Doctor education An audit serves as a powerful tool for continuing medical education of doctors. Auditing rates of particular services performed such as vaccinations, blood pressure recording, pap smears or test ordering, make for interesting comparisonbetweencolleagues.The resultscanbeprovidedconfidentiallyallowingdoctors to reflecton theirpractice behaviour.

101/JNU OLE
8.9 Formal Research Projects Researchisanewfieldofprimarycare.Untiltheintroductionofthecomputer,generalpracticeresearchhadbeenlimited to the academic institutions that had a particular interest in community medicine. Computerisation has enabled the anonymous collection of whole population data. As some medical conditions in general practice occurs relatively infrequently large population numbers need to be used to gain enough statistical power for useful conclusions. With the costs of medical care ever increasing, governments are looking to primary care for information solutions and outcomes. From a community perspective general practice will need data collected into computerised records to achievethesegoals.Datacollectionwillneedtobeorganised,requiringtheuseofclassificationandcoding.Thetopicsof‘Research’and‘ClassificationandCoding’arediscussedelsewhereinthisbook.
8.10 Medical Education Medical education includes the education of the undergraduate, the new graduate and the experienced general practitioner. It also includes the education of the patient and this has been a major role in family medicine since its inception.
New Graduates When the new graduate enters general practice there is much information to be learnt. Community services, practice providers, trade names of drugs, preventive care management, relevant test ordering and administrative tasks to undertake. Each different community will have its own services and each practice its own style. Computerisation can help assist the new graduate by providing ready access to databases of information, screen prompts for preventive care and reference to protocols of management
Experienced General Practitioners Themore experienceddoctors benefit fromaccess to up to date knowledgebasis.There are severalCDROMprograms now available based on authorities sources. Other knowledge base programs present doctors with clinical case scenarios, predictive indices of diseases, and knowledge bases incorporated into the system. These systems can be utilised in the consulting room with the aid of a CDROM drive incorporated into a PC or by access via modem to a site with a CDROM bank of resources.
Patients The computer can be incorporated most effectively into patient education. The simplest of these is the personalised patient hand out. Handouts can be indexed to illnesses and when appropriate printed out for the patient’s use. The doctor can then explain details to the patient. The information is readily accessible reducing the frustration of searching through myriads of papers. Another means of educating patients is to empower them by noting screen prompts.
Preventive care prompts display to both the patient and the doctor that certain services are due for review. This may motivate both patient and doctor even when this may not be on the original agenda for the visit. Vaccinations rates for tetanus can be increased utilising this technique. Medication information is an ideal topic for computer education and pharmacists are using this widely with dispensed medications. Sophisticated programs have been created by specialists to educate patients on particular topics. Diabetes and low fat diets are topics that the computer can manage for this purpose.
8.11 Telecommunications Theuseoftelecommunicationforhealthinformationisanewfield.Doctorsinvolvedinresearchhaveusedmodemconnections to bulletin boards and networks for research information, communication with colleagues via E-mail, and to authority’s databases. Some clinics are now transferring their direct bill accounts via modem eliminating the physical task of collating accounts. Many computer software suppliers use modem connection for maintenance to reduce costs of onsite visits. In the future general practitioners will transfer their pathology and radiology requests and results via modem. They will have connections to hospitals for admission and discharge information, access toknowledgebases,andreadycommunicationwithcolleaguesas theirresearchpeershavetoday.Thefieldoftelecommunications will open up a whole new dimension to the practising family physician.

Health Informatics and Management Information
102/JNU OLE
SummaryCommunication between community nurses, paramedical staff such as physiotherapists or podiatrists, pharmacists, •dentists, counsellors and alternative medicine practitioners, demonstrate the range of communication which occurs between primary health care workers.As funding arrangements vary, so can the style of practice and therefore, episodic care is more appropriate to •accident and emergency departments provided by hospitals.Practice management has four major components in the General Practice setting which are Patient Billing, •Appointments, Practice Administration and Electronic Tools. Modern systems software now has been purpose written for the style of practice accounting.•A computerised accounting system can form the basis of a general clinic patient register and enable the use of •patient demographics.MasterPatientIndexenablescorrectidentificationoftheparticularpatientandtheappropriatehistorypulled•in readiness prior to the patient attending.For systems using computers in the consulting room for clinical records, the appointment system can be integrated •andeliminatetheneedforthepaperrecordanditssundryretrievingandfilingtasks.Computerisation of the Item Service database enables clinics to audit their practice and their individual doctors •forservicesperformed,comparepractitioners’practiceprofilesanddeterminefeesgeneratedperservicetypeor per doctor or clinic.General Practices are required to manage the salaries of their staff, both medical and non medical.•Recently the facsimile (fax) machine has further extended the use of this telephone system enabling the transfer •of the printed word, either directly or through the computer to anywhere in the world.Wordprocessingalsooccurswithinanygeneralpracticeofficesparticularlyintheformoflettersofreferral,•medical reports, and clinical notes.Legal Documentation is one of the major reasons for creating medical records.•
ReferencesHealth Informatics in General Practice, • [Pdf] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_26.pdf>[Accessed 29 November 2012].Introduction to Health Informatics, • [Online] Available at: <http://www.philblock.info/hitkb/h/health_informatics.html>[Accessed 29 November 2012].2012. • ROBYN TAMBLYN (FUTURE OF HEALTH SERVICES), [Video Online] Available at: <http://www.youtube.com/ watch?v=MJQScqyZzLE>[Accessed29November2012.2009. • Future Vision of Healthcare, [Video Online] Available at: <http://www.youtube.com/watch?v=SWiuBK-_WY0&playnext=1&list=PL78ECD634611C11BE&feature=results_main>[Accessed 29 November 2012].Hovenga, E., Kidd, M., Cesnik, B. & Livingstone, C., 1996. • Health Informatics: An Overview, Australia.Ball, J. M., Douglas, V. J., Walker, H. P., DuLong, D., Gugerty, B., Hannah, J. K., Kiel, J., Newbold, K. S., •Sensmeier, E. J., Skiba, J. D. & Troseth, R. M., 2010. Nursing Informatics: Where Technology and Caring Meet, Springer.
Recommended Reading Maeder, J. A. & Martin-Sanchez, J. F., 2012. • Health Informatics: Building a Healthcare Future Through Trusted Information, IOS Press.Bushko, G. R., 2009. • Strategy for the Future of Health, IOS Press.Bushko, G. R., 2002. • Future of Health Technology, IOS Press.
103/JNU OLE
Self AssessmentCommunication between community nurses, paramedical staff such as physiotherapists or podiatrists, pharmacists, 1. dentists, counsellors and alternative medicine practitioners, demonstrate the range of __________ which occurs between primary health care workers.
communicationa. conversationb. controversyc. contrastd.
The style of a __________ practice relates to the method by which it attracts funds.2. secondary carea. personal careb. primary carec. motherly cared.
__________hasbeenthefirstareapracticeshavetakentocomputerisation.3. Patient billinga. Appointments b. Electronic tools c. Clinical recordsd.
_________enablescorrectidentificationoftheparticularpatientandtheappropriatehistorypulledinreadiness4. prior to the patient attending.
Mater Patience Indexa. Master Patient Indexb. Master Pets Indexc. Master Poetic Indexd.
__________foreitheramanualorcomputerisedofficeincludeadailylistofpatientconsultations,account5. status of each consultation, receipts paid to the practice that day, and the banking report for the day or period including that day.
Month end procedures a. Batchingb. Day end proceduresc. Stock control d.
Computerisation of the __________ enables clinics to audit their practice and their individual doctors for 6. servicesperformed,comparepractitioners’practiceprofilesanddeterminefeesgeneratedperservicetypeorper doctor or clinic.
Month end procedures a. Batchingb. Day end proceduresc. Item service databased.
Health Informatics and Management Information
104/JNU OLE
Larger organisations such as hospitals have sophisticated computerised __________ systems. 7. month end procedures a. batchingb. stock controlc. item service databased.
__________ is one of the major reasons for creating medical records. 8. Accuracya. Efficiencyb. Efficacyc. Legal documentationd.
Thefieldof__________willopenupawholenewdimensiontothepractisingfamilyphysician.9. telecommunicationsa. telephoneb. internetc. emaild.
___________ can be indexed to illnesses and when appropriate printed out for the patient’s use.10. Handoutsa. Pamphletsb. Papersc. Cardsd.

105/JNU OLE
Case Study I
Health Information Systems in Developing Countries
Thissectionprovidesanunderstandingofthechallengesandthepotentialbenefitsassociatedwithhigh-performing,interoperable health information systems in the developing world, as observed in case study research in India. Particular focus is given to how HIS can be structured to give frontline health care providers the information they need to provide quality care and education to their patients and to local populations. This section will also illustrate some of the themes described in the previous section of this report, the Landscape Analysis.
Overview of Case Study MethodologyThe HIS projects chosen as case studies: the National Rural Health Mission (NRHM) Health Management Information System(HMIS)inIndia.Theseprojectswerechosenbecausetheyaresignificanteffortstoimprovehealthinformationmanagementindevelopingcountries;becausetheyhavebeenrolledoutincountriesthataremarkedlydifferent,intermsofgeographyandincomelevel;andalsobecausetheyrepresentthreemajortypesofHISdeployments.Casestudy research included extensive review of secondary literature on the health information systems, interviews with expertsfamiliarwiththesystem,andin-countryfieldresearch.ThefieldresearchontheHISprojectswascarriedout between December 2008 and January 2009 in India. Field research included interviews with the Ministry of Health, project management, implementing partners, system end users, and other health informatics experts in India. It included visits to sites that use the HIS under study, and in some cases, visits to sites that use alternate health information systems.
Thefieldresearchhadthreeareasobjectives.First,itaimedtoestablishthebasicfactsaboutthehealthinformationsystem: the reason for the system’s development, the problem it was designed to solve, the system’s champion and itsfunder(s),itsobjectives,itsstructureandimplementation,anditsimpact,ifany.Second,thefieldresearchsoughtto understand the factors that have helped or hindered the health information systems as they were developed or scaled. Research focused on understanding which parts of the health information “value chain,” or the factors that influencethehealthinformationsystem,weremostinfluential.Thesefactorscanincludegovernmentpolicyandregulation,organisisationalstructureandenvironment,oravailablehumanandfinancialresources.Third,thefieldresearch focused on understanding how health care providers used health information, and whether and in what ways each health information system supported pre-existing operational or decision-making processes.
Thissectionprovidesaprofileofeachofthehealthinformationsystemsstudied.Eachprofilebrieflydescribesthe reason for which the HIS was developed, what its goals and/or objectives are, how it is structured and what its primary uses are, how the system has been implemented, what its results are (if measured), and what the outstanding implementation challenges or next steps are. The case study ends with a discussion of the major lessons from analysis ofthethreehealthinformationsystemsprofiled.
IntroductionIndia’s Health Management Information System (HMIS) is just as much an effort to employ technology to improve people’s health as it is a mission to convince health workers at each level of government that good data can pave the way to better health care.
Home to a surging population of more than one billion people spread throughout megacities and 600,000 villages, India faces health care challenges of a scale and diversity unmatched in the developing world. Although the country’s economy has surged in recent years as a technology industry thrives in major Indian cities, and the central government seeks to attract foreign investment, much of the urban and rural population remains poor and without adequate access to quality health care services. The Indian government created the National Rural Health Mission (NRHM) in 2005 “with an aim to achieving the targets set by the Millennium Development Goals (MDGs) 4, 5, and 6 and making the health delivery system more responsive to the health care needs of the people of India.”The program is part of the government’s broader effort to increase health care spending from 0.9% to 2-3% of GDP.

Health Informatics and Management Information
106/JNU OLE
The NRHM seeks to empower communities and health workers through feedback and participatory mechanisms designed to improve the quality of health services. Recently, the agency launched initiatives to improve basic health in rural areas, with a focus on maternal and child health and infectious diseases, the most critical health issues in rural India. With the NRHM introducing several major programs, a strong monitoring and evaluation (M&E) effort is essential for tracking program performance. At the heart of the M&E effort is the Health Management Information System (HMIS), focused on improving the collection and use of data related to core programs.
The HIS evaluated here is India’s HMIS. Field research focused on Chhattisgarh state, a newly created heavily rural state in eastern central India at the forefront in implementing the HMIS. The HMIS is designed to streamline and automate the data entry process. The system also introduced new analytical tools. The tools will allow analysis of ruralhealthtrends,specifichealthproblems,andtheperformanceoftheprogramscreatedtoaddressthoseproblems.The HMIS can also provide health workers with a clearer picture of health conditions in their area as compared to other areas and enable the workers to request more resources to improve care.
India’s Rural Health System: Underfunded and OvertaxedDespite the rapid growth of its large cities, India remains a predominantly rural nation, with more than 70% of its people residing in rural areas. The vast publicly funded rural health system serves this population, in accordance with the NRHM’s commitment to be more responsive to the health needs of rural Indians. States are divided into districts, which are in turn divided into blocks. The system is organised hierarchically, with each level reporting to the level above it, and is comprised of: 145,000 sub centers, staffed by Auxiliary Nurse Midwives (ANMs), who provide care primarily for women and children, and Multi-Purpose Workers (MPW), male workers who usually treat malepatientsandprovidethemwithreferrals.Eachsub-centerservesfivetosevenvillages,orapproximately5,000-7,000 people, 24,000 Primary Health Centers (PHC), staffed by a doctor and paramedical staff, with one PHC per 30,000people.EachPHCcoversfivetosevensubcenters.!3,400CommunityHealthCenters(CHC),block-level(the administrative unit just below the district level), staffed by basic medical specialists (such as pediatricians) and nurses and containing 30 beds. Each CHC serves 100,000 people, 600 District Hospitals, staffed by more advanced medical specialists (such as urologists). Each hospital serves one to two million people. Although the NRHM aims to improve health services for India’s rural population, the system is severely overextended. Many who can afford to do so seek treatment at private hospitals and clinics, which are growing rapidly and which, by some estimates, constitute 68% of all hospitals in India.
Issues with Existing Data Collection SystemsWhile the Ministry of Health and Family Welfare (MOHFW) in India has long collected data on health statistics from all public and many private health care facilities, it lacks a coherent strategy for integrating, synthesising, and analysing data to allow faster responses from the government. The reporting process focuses on a top-down imposition of data requirements and pays little attention to the need for information that can help health care workers improve patient treatment. Data quality is poor, with little institutional incentive for health care workers and functionaries to improve it. Most data entry is manual, forcing repeat data entry across as many as seven different layers of government and causing untold hours of wasted time. Data analysis is also manual, which often results in the government misunderstanding trends in health statistics. Finally, health care workers must collect up to 3,000 data points, according to divergent requirements laid down by central, state, and local governments. These problems – consistent with those observed across developing countries – point to the need for reform of the NRHM health information system.
Impetus for HMIS ReformThe HMIS initiative began with the launch of the NRHM itself. As the agency unveiled a host of new programs to improve rural health, the M&E division of the NRHM, as well as at the National Informatics Centre (NIC), a key partner in the HMIS, agreed that the ineffective data collection and analysis process described above had to be improved in order to determine the effectiveness of these new programs.
Mr. Pravin Srivastava, a director at the NIC, laid the foundation for the system in 2006, though initial planning began earlier.TheNRHMhadfourmajortasks:buildM&Ecapacityatthenational,state,andregionallevel;rationalisedataanddeterminethenumberandfrequencyofnecessaryindicators;contractwithasoftwareprovidertodevelopaWeb-basedsystem;andbuildphysicalinfrastructuretotransmitandhousedata.

107/JNU OLE
Datarationalisationprovedtobethemostdifficulttask.TheM&Edivisiondeterminedapproximately200criticalindicators by exhaustively reviewing the indicators collected by each program area and then identifying both redundanciesandtheminimumfrequencyofcollectionforeachindicator.ThefinallistwasapprovedbycommitteeandacceptedbytheAdditionalSecretaryoftheMOHFW.AsadirectoroftheM&Edivisionreports,“itwasadifficultand often ruthless exercise, and often acrimonious” since program heads tend to try to protect their data elements.
HMIS Overview The HMIS initiative of the NRHM, implemented in conjunction with the NIC, seeks to: Improve the data collection and analysis process by taking steps to streamline data collection, namely by identifying data points related to the NRHM’s primary goals and reducing the data points from nearly 3,000 to about 200. Frequency of collection will be reduced from monthly to quarterly, or annually, for most data points. Automate the data process by introducing a Web-based system that can be accessed at all levels of government through the deployment of computer hardware and Internet connectivity at facilities nationwide. Validate data by triangulating other data sources to verify and improve data quality. Validation will also be achieved through the introduction of dedicated data managers, as far down as the Primary Health Centre (PHC) level, which can identify and analyse data and work with providers to improve collection and quality. Introduce analytical tools, starting at the central government and trickling down, that allowhealthcareworkersandgovernmentofficialstoseeandunderstandhealthtrendsandformulateaneffectiveresponse.
HMIS DescriptionThe HMIS is designed to aggregate data based on health indicators compiled by rural health care workers. At the system’s core are approximately 200 indicators related to the areas of child and maternal health and infectious diseases. (India has “siloed” programs for monitoring diseases such as HIV/AIDS, malaria, tuberculosis, and leprosy.) The data are collected at the facility level and fed progressively up to block, district, state, and central government levels, where it can be analysed and used to make decisions. Core indicators are entered digitally into the system at the block or district level and aggregated to provide a statistical snapshot of India’s health indicators at each level ofthesystem.HMISdataqualityisverifiedthroughatriangulationprocess,asdescribedinthe“Triangulation”box on the next page.
How the HMIS is used?Rural health care workers use the data to effect changes in policy and treatment and to allocate resources more effectively. The HMIS has two key features that enhance system usability: (1) enhanced analysis and (2) two-way informationflows.Enhancedanalyticalfeaturesallowauthoriseduserstoviewandcomparetheperformanceofdifferenthealthcentresandhospitals.Usersareabletogeneratereportsondifferentindicatorsforspecifictimeperiods and compare them to earlier periods, and reports can be viewed in both graphical and tabular format.
Thesystemalsoincludesback-end,SAS-basedanalyticaltoolsforhigher-levelusers.Two-wayinformationflowsallow health care providers at all levels to access data. The dedicated data managers funded by the NRHM at the district, block, and PHC levels will be able to access data for use in monthly meetings, where information collected in the previous month is discussed with health workers and administrators. The data will also be provided to the newly empowered gram panchayats, or village health councils, which are charged by the NRHM with developing community health action plans for their villages. Village health councils will be assisted by female Accredited Social and Health Activists (ASHA). The ASHA is a NRHM created position that will act as a liaison between ANMs and villages to improve data collection and the response to community health needs. The gram panchayats and ASHAs will have access to HMIS-generated data related to their areas, empowering them to create stronger community health action plans.
While the Indian HMIS is intended to capture comprehensive data about reproductive and child health and infectious diseases, it will not cover all health encounters. Chronic diseases such as heart disease and diabetes, which are growingproblemsinIndiaandChina,willnotbecomprehensivelytracked,afactacknowledgedbyhealthofficialsinterviewed for this study: “We are aware of the growth of chronic disease issues, but they are a greater problem in urbanareas,whicharenotourfocus,”saidoneNRHMofficial.

Health Informatics and Management Information
108/JNU OLE
The system is, however, designed to accommodate expansion and could eventually include such conditions as the government continues to address them. The HMIS is currently integrated with the Gujarat Hospital Management Information System (see the example mentioned below). The HMIS is not yet integrated with India’s Integrated Disease Surveillance Program (IDSP), the nation’s main surveillance program, though the system’s architects are working to develop an integration plan.
Example The Gujarat HMIS: Patient Record Capability, National Interoperability. While the NRHM HMIS will eventually cover all of India, it is a system of limited scope, designed to collect information on indicators related to the NRHM’s core programs. At the state level, there is innovation encompassing other HIS functions. Gujarat state in western India, for example, deployed a Hospital Management Information System at its 25 district-level hospitals in 2007. Thesystemisamodule-basedapplicationwhichincludesapatientidentificationnumberthattrackspatients’medicalhistories. It contains laboratory, pharmaceutical, human resources, and equipment management units. The system is designed to give administrators the ability to comprehensively oversee all aspects of hospital management and patientflowwhileprovidingphysicianswitheasyaccesstopatienthistoryasameansofimprovingcare.Despiteits complexity, the system is still able to feed required indicators to the NRHM system. The Gujarat experiment illustrates the need forflexibility inHISdesign, allowing for local innovationwhile accommodatingnationalreporting requirements.
Project Implementation to DateThe national HMIS went “live” in October 2008. While the HMIS will eventually be expanded to cover the entire country, it is currently being deployed in the 18 states designated “high-focus” by the NRHM (because they are the most heavily rural states). Automation will be introduced gradually at lower levels, as infrastructure allows. In Chhattisgarh, for example, automation initially will be limited to the block level, where all facilities are installing computers that will be connected to the Internet (connectivity has just been fully established at the district level). Data collection at the sub centre and PHC level will remain manual for now and will be aggregated and digitised at the block level. With the national system online and operational, all states are entering data they collected between April and October 2008 in order to provide a historical record and basis for comparison.
Many of the activities to date have focused on the operational and infrastructure requirements of the HMIS. States vary in their progress, however. Chhattisgarh is one of several states that have already achieved several milestones, includingcomputerdeploymentatnearlyallblocks;Internetconnectivityinall16districts;completionofHMIStrainingforallresponsiblestate-anddistrict-levelstaff;andongoingtrainingforblockprogrammanagers(BPMs)at the block level.
Intended ResultsThe newness of the NRHM initiative means that there is very little data on outcomes. The deployment of the system isongoing,andtherewasnopilotprojectperse.ThehopeisthattheHMISwillprovideseveralbenefitstothehealth system, including: The ability to view up-to-date health data on individual administrative units, which will helppolicy-makersalignneedswithresourcesandallowlower-levelhealthofficialsanddatamanagerstocomparetheir units’ conditions. This will ease the burden of arguing for increased resources. Reduced data entry at the block level and above (when automation becomes available at the lowest levels). Improved data accuracy via the reduction of required data points, the enhanced validation methods used by the NRHM and the addition of data staff at lower levels! Better data, which, in concert with the empowerment and feedback mechanisms being instituted, will arm health workers with better information to “argue their case.”
Remaining ChallengesMajorchallengesremain,severalofwhichcouldstymietheHMISimplementation.Officialsagreethatpoordataquality is a serious problem, adding that the data streamlining and validation efforts noted above are an attempt to mitigate the problem. There are several factors that contribute to poor data quality. Perhaps the primary reason for poordataqualityistheshortageofqualifiedpersonnel,particularlythoseresponsibleforserviceprovision,suchasdoctors,nurses,andANMs.Bysomeestimates,only30%ofnursingpositionsinruralhospitalsarefilled,andasingleANMoftencoversfivevillages.TheseoverworkedANMstypicallyspendfourtofivehoursenteringdata
109/JNU OLE
eachweek.NRHMofficialshopethatthetrainingofASHAsforeachvillagewillrelievetheANMsandimprovedata collection and quality, as part of the ASHAs’ responsibility is keeping ANMs appraised of vital events. The useoffinancialincentivesformeetingspecificgoals,suchaschildhoodimmunisations,alsoencouragessomeusersto provide false data. The volume and duplication of data and data entry have also impeded past efforts to improve health information systems. ANMs in India must maintain up to 14 separate registries for different types of data and are required to re-enter this information into forms that are sent to the PHC level for further aggregation. The current HMIS initiative seeks to reduce the frequency and number of data points collected, but until automation is introducedatthelowestlevelofserviceprovision,re-entrywilladverselyaffectefficiency.
Perhapsthebiggest“soft”challengefacingtheHMISprojectiscultural.SeveralMOHFWofficialslamentthelackofrespectfordatainIndiangovernment.Top-downdatarequirementswithlittledownwardflowhavelefthealthworkers with little incentive to accurately collect data. Instead, the system could be used to ensure that the data are usedtoempowerhealthworkers,thusmotivatingthemtocollectdataaccurately.Officialsbelievethatinvolvingthecommunity in creating village health plans will create a demand for better data. The logic is that health care workers will gain a clear understanding of community needs, which will in turn motivate them to collect better data to address those needs. Pravin Srivastava, a director of the NIC and an HMIS leader, said, “Indian government employees have been just told what to do for so long that they don’t feel that they can create change. They’ve forgotten how to make decisions. And so a type of devolution is essential. If workers are empowered, they will learn that they have to use data to make their case for more resources and assistance.”
The success of this HIS initiative – and the hopes of its sponsors – hinges on the notion that (1) the feedback mechanisms created for workers and community members will incentivise them to collect better data, (2) the addition of ASHAs and data staff will relieve the burdens on rural medical staff, and (3) potential data validation strategies willimprovetheabilitytoidentifysourcesofbaddata.OneNRHMdescribedIndianofficialsas“nervous”aboutthe implementation of the project. If India follows through on its commitment to triple health-care spending, and if resources for workers are improved, then the HMIS might suggest that data have the power to improve health outcomes.
(Source: 2009. Health Information Systems in Developing Countries, [Pdf] Available at: <http://www.minsa.gob.pe/ogei/conferenciaops/Recursos/43.pdf>[Accessed 30 November 2012]).
QuestionsList at least 3 issues with existing data collection system of health sector in India.1. AnswerThe issues with existing data collection system in India are as follows:
Thefirstandthemajorissuesisthatitlacksacoherentstrategyforintegrating,synthesising,andanalysing•data to allow faster responses from the government. The reporting process focuses on a top-down imposition of data requirements and pays little attention to •the need for information that can help health care workers improve patient treatment. Most data entry and data analysis is manual. •
What are the two key features of HMIS that enhance system usability?2. AnswerThe HMIS has two key features that enhance system usability:
enhanced analysis and •two-wayinformationflows•
Health Informatics and Management Information
110/JNU OLE
ListfewbenefitsofHMIStohealthsysteminIndia?3. AnswerThebenefitsofHMIStohealthsysteminIndiaare:
The ability to view up-to-date health data on individual administrative units, which will help policy-makers •alignneedswithresourcesandallowlower-levelhealthofficialsanddatamanagerstocomparetheirunits’conditions which will ease the burden of arguing for increased resources. Reduced data entry at the block level. •Improved data accuracy via the reduction of required data points. •Better data, which, in concert with the empowerment and feedback mechanisms being instituted, will arm •health workers with better information to “argue their case.”

111/JNU OLE
Case Study II
Fletcher Allen Leverages EMR Connectivity for Optimised Imaging
Chuck Podesta, senior vice president and CIO at 500-bed Fletcher Allen Health Care in Burlington, Vt., is dogged in his determination to use IT to improve care for patients across the state. Relatively small, Vermont’s population is mostly rural and broadly scattered.
FletcherAllen,anaffiliateoftheUniversityofVermontMedicalSchool,isuniquelypositioned.Otherwidely-scatteredfacilities often send patients to Fletcher Allen for tertiary - even, quaternary care. Podesta saw an unusual opportunity with regard to his relationship with his core EMR vendor, Verona, Wis.-based Epic Systems Corporation.
“Typically,Epic’smarkethasbeenlargeacademicmedicalcentresandhealthsystemsandlargemedicalpractices;they haven’t been that interested in smaller hospitals,” Podesta says. “And because we are the only academic medical centre in Vermont, they’ve allowed us to extend our Epic product license to other hospitals in the state. I call it a ‘group-purchase, hosted’ solution, because we host the single database,” he says.
Podesta and his colleagues have developed PRISM Regional, a core clinical information system whose capability extendsthroughoutVermontandacrosstheborderintothestateofNewYork.ThesystemhasgoneliveatfiveofVermont’s 13 hospitals, as well two in upstate New York. In order to provide imaging access to hospitals throughout the region, the PRISM/Epic EMR is regionalising imaging communications state-wide, he says.
And this is true even though Fletcher Allen’s RIS is the Image Cast product from GE Healthcare (Waukesha, Wis.) and its PACS is from McKesson Corporation (Alpharetta, Ga.), according to Podesta.
In terms of diagnostic imaging, Fletcher Allen’s PRISM Regional initiative is improving clinicians’ access to, and use of, diagnostic images as well as other clinical data in the broader context of clinical IT development. Any physician linked into the PRISM system can access any archived image by clicking on an icon on the main EMR screen and can launch the PACS Web viewer onscreen. And for patients in a state such as Vermont with low-density populations, improving such access inherently means improving patient care. In many cases, it can make the difference between an ambulance transfer and the ability to care for patients tele-medically, improving the speed and effectiveness of care.
In many cases, it can make the difference between an ambulance transfer and the ability to care for patients tele-medically, improving the speed and effectiveness of care.
“For example,” Podesta says, “often, a physician three hours away in a community hospital isn’t sure whether to transferapatientornot;andifthedecisionisbeingmadeduringatelephone-basedconsultwithaphysicianhere,and the diagnostic images aren’t available to the physicians in both facilities, then there can be uncertainty as to what to do. In that case, if you’re not sure, you’ve got to transfer the patient. Then later on after the patient is transferred, sometimes you discover that the patient could, in fact, have stayed in the community hospital and not taken a three-hour ambulance ride, with the family driving behind.
“Now, with the ability of physicians in all the linked facilities to access those diagnostic images, the radiologist here at Fletcher Allen, and sometimes the ED physician here, can be on the phone with the ED physician at the outlying hospital, and all can be looking at the same set of images and come to a more optimal decision.” Podesta says its more point-to-point than traditional teleradiology. “And in places like Vermont, New Hampshire, and upstate New York, this kind of technology has a huge impact, especially since the EMR is wrapped around everything.”
“We were very aggressive in terms of upgrading our infrastructure and our network, both inside the facilities and between and among them.”
Health Informatics and Management Information
112/JNU OLE
Could this model of IT-supported care delivery be replicated elsewhere? Podesta says it’s certainly a possibility, and Judith Faulkner, founder and CEO of Epic, agrees. “Actually, a few of our customers have extended their software to small neighbouring hospitals over the past half-dozen years or so with our full support,” she says. Faulkner says Epic is set to release Sonnet, its inpatient EMR for smaller hospitals this month (an ambulatory version came onto the group practice market in the fall). In the meantime, Podesta and his colleagues will be busy for the next few years broadening and deepening the reach of their clinical information systems to further enhance care delivery across mostly rural Vermont.
(Source: Health Informatics Healthcare IT Leadership, Vision & Strategy. Fletcher Allen leverages EMR connectivity for optimised imaging,[Online] Available at: <http://www.healthcare-informatics.com/article/part-1-making-it-count> [Accessed 30 November 2012]).
QuestionsWhat is the advantage of computer linked facilities to the physicians at the health care centre?1. What did PRISM/Epic EMR do to provide imaging access to hospitals throughout the region?2. How can a physician linked into the PRISM system access any archived image? 3.
113/JNU OLE
Case Study III
In The Rural West, a Community Hospital System Advances
In contrast to the situations at Fletcher Allen Health Care in Vermont, the Roseville, Calif.-based Adventist Health system is comprised entirely of community hospitals, most of which are in smaller cities and towns, and in rural areas. What’s more, only three of the system’s 16 hospitals, spread out across California, Oregon, Washington, and Hawaii, are larger than 300 beds, while the majority are smaller than 200. Further, it is commonplace for patients tohavebeenadmittedtomorethanoneAdventisthospitalovertime;andforAdventistclinicianstoconsultwithoneanotherovergreatdistances.SotheneedforaunifiedimagearchiveandanintegratedclinicalISinfrastructurehas been a top goal of Alan Soderblom, Adventist’s vice president and CIO, and Greg McGovern, the system’s assistant vice president and CTO.
“I thinkourmost significant areaof progress has been the creationof a central archive for the images,” saysSoderblom. “That then allows us to take the next step, which is the integration into the electronic health record, so thatessentially,aphysicianonthefloorcangointoourProjectIntellicare(KansasCity,Mo.-basedCerner)andpullup the image from that system rather than going to a separate PACS system. So it provides more ease of access to that image.” (Adventist has implemented Cerner’s core EMR across its entire system, as well as Cerner’s Cedara RIS product system-wide, while its hospitals use GE’s PACS product.)
ThecentralimagearchivefirstwentliveinAdventist’shospitalinWallaWalla,Wash.,inearly2007.Thatinitiative,which has integrated all the PACS at all the hospitals into a central archive, is set to complete integration work this month.
Of course, even with a clear overall objective and a well-planned strategy, there are always tactical challenges to imaging integration, notes CTO McGovern. “You start off a project like this thinking that the primary objective is, as Alan has said, integrating the image into the primary EMR, so that doctors have one-stop shopping,” he says. “But thenyourealisetherearecompetingaudiences;theradiologistdoesn’tcaresomuchabouttheEMRbutaboutthePACS.Andthenyoumighthaveorthropodsthatarefarawaywhojustwanttorummagequicklythroughimages;or you might have teleradiology going at the same time. So your primary objective is nice, but doesn’t scratch everybody’s itch. We’ve struggled with trying to meet performance standards.”
Soderblom says they are working to meet the needs of the different types of physicians. “Once we have that issuefiguredout,havingthatsingleplacemakesiteasiertoworkthroughthechallenges,”hesays.Soderblom,McGovern, and their colleagues have also integrated the imaging functionality around echocardiography and digital mammography into the overall architecture.
Another issue that Adventist’s team has been working on, in common with the folks at Alegent and Fletcher Allen, istheloomingstorageissue.Inthecaseoftheunifiedimagearchive,thevolumehasdoubledjustinthepastyear,leaping from four terabytes to eight, with every indication it will continue at a rapid pace.
McGovern says it’s no easy task. “One thing that people don’t realise until they’re doing it is the huge challenge ofimagingmanagement,”hesays“Thesearen’tlittledatabits;you’refacingbigimagingstorageproblems.So,in regard to just the basic mechanics per the size of your WAN or storage network, and the other practical issues, youjustdon’trealisehowmuchisinvolved.”Inaddition,hesays,ensuringtheproperlevelofstaffingtosupportenterprise-wide imaging management is crucial.
(Source: McGovern, G., In the rural West, a community hospital system advances, [Online] Available at: <http://www.healthcare-informatics.com/article/part-1-making-it-count?page=2> [Accessed 30 November 2012]).

Health Informatics and Management Information
114/JNU OLE
QuestionsWhat are the 3 competing audiences to be considered while integrating the image into the primary EMR?1. What is the advantage of creation of a central archive for the images? 2. What have been a top goal of Alan Soderblom, Adventist’s vice president and CIO, and Greg McGovern, the 3. system’s assistant vice president and CTO?

115/JNU OLE
Bibliography
References2009. • Future Vision of Healthcare, [Video Online] Available at: <http://www.youtube.com/watch?v=SWiuBK-_WY0&playnext=1&list=PL78ECD634611C11BE&feature=results_main>[Accessed 29 November 2012].2011. • Building a successful Health Information Exchange [Video Online] Available at: <http://www.youtube.com/watch?v=ZUhm2VZ8h_8&feature=related>[Accessed26November2012].2011. • Electronic Health Records: What’s in it for Everyone? [Video Online] Available at: < http://www.youtube.com/watch?v=FAaeCYyAxl0&feature=related> [Accessed 26 November 2012].2011. • Health Informatics Overview. [Video Online]. Available at: <http://www.youtube.com/watch? v=au1OFMyVP0Q> [Accessed 27 November 2012].2011. • The usability (or not) of Health Informatics Standards [Video Online] Available at: < http://www.youtube.com/ watch?v=JM-EpHVB_7k> [Accessed 26 November 2012].2012. • Health Information Technology [Video Online] Available at: <http://www.youtube.com/watch? v=0MfJ3VmoqvE> [Accessed 26 November 2012].2012. • Introducing Health Informatics, [Video Online] Available at: <http://www.youtube.com/watch?v=5gKspYFAc9Q>[Accessed 29 November 2012].2012. • Introduction to Health Informatics, [Video Online] Available at: <http://www.youtube.com/watch? v=leWE5fx8aZs>[Accessed29November2012].2012. • ROBYN TAMBLYN (FUTURE OF HEALTH SERVICES), [Video Online] Available at: <http://www.youtube.com/watch?v=MJQScqyZzLE>[Accessed29November2012.2012. • What is Health Informatics? [Video Online] Available at: <http://www.youtube.com/watch?v=rFxewUq1cE4> [Accessed 20 November 2012].Ball, J. M., Douglas, V. J., Walker, H. P., DuLong, D., Gugerty, B., Hannah, J. K., Kiel, J., Newbold, K. S., •Sensmeier, E. J., Skiba, J. D. & Troseth, R. M., 2010. Nursing Informatics: Where Technology and Caring Meet, Springer.Borycki, M. E., 2011. • International Perspectives in Health Informatics - Studies in Health Technology and Informatics, IOS Press.Brittain, M. J., • National Strategy for Information Management, [PDF] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_23.pdf>[Accessed 28 November 2012].Competencies for Public Health Informaticians 2009. • [PDF]. Available at: <http://www.cdc.gov/informaticscompetencies/downloads/phi_competencies.pdf> [Accessed 27 November 2012].Conrick, M., 2006. • Health Informatics, Cengage Learning Australia. Dr. Kellogg. D., 2012. • USM HIM – What is HIM? [Video Online] Available at: <http://www.youtube.com/watch? v=zwzNayEFVfY> [Accessed 20 November 2012].Dr. Zitner, D., 2010.What is Health Informatics. • [Video Online]. Available at: <http://www.youtube.com/watch? v=VKPSuDG_bTU>[Accessed 27 November 2012].Emedikon. 2010. • BenefitsofEMR[Video Online] Available at: <http://www.youtube.com/watch?v=TiQ8c11dkU0> [Accessed 28 November 2012].Emedikon. 2010. • What is EMR? [Video Online] Available at: <http://www.youtube.com/watch? v=MOwML1N3TpM> [Accessed 28 November 2012].Feeny, P., • Preparing staff for information Technology, [PDF] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_24.pdf>[Accessed 28 November 2012].Hannan, J. T., • Electronic Medical Records, [PDF] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_12.pdf> [Accessed 28 November 2012].Health Informatics in General Practice, • [PDF] Available at: <http://www.achi.org.au/docs/HNI_Book/Chapter_26.pdf>[Accessed 29 November 2012].

Health Informatics and Management Information
116/JNU OLE
Health Informatics• , [Online] Available at: <http://www.authorstream.com/Presentation/bawells-1264433-health-informatics/> [Accessed 26 November 2012].Health Informatics,• [Online] Available at: <http://www.authorstream.com/Presentation/Opluviose-1404677-health-informatics-presentation/> [Accessed 26 November 2012].Health Informatics, • [Online]Availableat:<http://www.ehow.com/facts_5574843_define-health-informatics.html> [Accessed 19 November 2012].Hovenga, E., Kidd, M., Cesnik, B. & Livingstone, C., 1996. • Health Informatics: An Overview, Australia.Huffman, E., 1994. • Health information management, 10th ed., Physicians’ Record Co.Introduction to Health Informatics• , [Online] Available at: <http://www.coiera.com/> [Accessed 19 November 2012].Introduction to Health Informatics, • [Online] Available at: <http://www.philblock.info/hitkb/h/health_informatics.html>[Accessed 29 November 2012].Kudyba. S., 2010. • What is Healthcare Informatics? [Video Online] Available at: < http://www.youtube.com/watch? v=pzS--PaGC9o> [Accessed 19 November 2012].Kuehn, L., 1997. • Health Information Management: Medical Records Process in Group Practice, Medical Group Management Assn. Lord, T.,• Basic applications and expectations, [PDF] Available at: < http://www.achi.org.au/docs/HNI_Book/Chapter_06.pdf> [Accessed 27 November 2012].Medical Web Experts, • What is EMR? Information to Improve the Patient Experience, [Online] Available at: < http://www.medicalwebexperts.com/blog/what-is-emr/ > [Accessed 28 November 2012].Moor, G., McDonald, C., Noothoven van Goor, J., 1993. • Progress in Standardization in Health Care Informatics, IOS Press. Practice Brief: Health Informatics Standards and Information Transfer: Exploring the HIM Role• , [Online] Available at: <http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_000024.hcsp?dDocName=bok1_000024 [Accessed 26 November 2012].Shortliffe. E. 2011. • What is Informatics? [Video Online] Available at: <http://www.youtube.com/watch?v=xha0EI3r4hY> [Accessed 19 November 2012].Skolnik, S. N., 2010. • Electronic Medical Records: A Practical Guide for Primary Care, Springer.Standards in Medical Informatics, • [Online]Availableat:<http://wang.ist.psu.edu/course/07/IST497/files/CH06-FINAL.pdf> [Accessed 26 November 2012].Sullivan, F. & Wyatt, J., 2009. • ABC of Health Informatics, Wiley.The Difference between Health Informatics and HIM• , [Online] Available at: <http://healthinformatics.uic.edu/difference-between-health-informatics-and-him/> [Accessed 20 November 2012].The History of Health Informatics, • [Online] Available at: <http://healthinformatics.uic.edu/history-of-health-informatics/> [Accessed 20 November 2012].Wager, A. K., Lee, W. F. & Glaser, P. J., 2009. • Health Care Information Systems: A Practical Approach for Health Care Management, John Wiley & Sons.
Recommended Reading1997. • Protecting Electronic Health Information, National Academies Press.Bushko, G. R., 2002. • Future of Health Technology, IOS Press.Bushko, G. R., 2009. • Strategy for the Future of Health, IOS Press.Carter, H. J., 2001. • Electronic Medical Records: A Guide for Clinicians and Administrators, ACP Press.Coiera, E., 2003, • Guide to Health Informatics, Arnold. Conrick, M., 2006. • Health Informatics, Cengage Learning Australia.Gartee, R., 2010. • Health information technology and management, Pearson.

117/JNU OLE
Hovenga, J. S. E. & Mantas, J., 2004. • Global Health Informatics Education, IOS Press.Johns, M., 2002. • Health Information Management Technology: An Applied Approach, American Medical Records Association. Johns, M., 2002. • Information Management for Health Care Professions, Cengage Learning. Lazakidou, A. A., 2006. • Handbook of Research on Informatics in Healthcare & Biomedicine, Idea Group Inc (IGI).Lorenzi, N. & Riley, R., 2004. • Managing Technological Change: Organisational Aspects of Health Informatics, SpringerMaeder, J. A. & Martin-Sanchez, J. F., 2012. • Health Informatics: Building a Healthcare Future Through Trusted Information, IOS Press. McSean, T., Loo, J., Coutinho, E., 1995. • Health Information: New Possibilities, Springer.O’Carroll, P., Yasnoff, W., Ward, E., Ripp, L., & Martin, E., 2002. • Public Health Informatics and Information Systems, SpringerRoss, D., Hinman, A., Saarlas, K., & Foege, W., 2002. • Public Health Informatics and Information Systems, Springer.Scott, T., Rundall, G. T., Vogt, M. T. & Hsu. J., 2007. • Implementing an Electronic Medical Record System: Successes, Failures, Lessons, Radcliffe Publishing.Shortliffe, H. E. & Cimino, J. J., 2006. • Biomedical Informatics: Computer Applications in Health Care and Biomedicine, Springer.Steele, A., 2002. • Medical Informatics Around The World: An International Perspective Focusing On Training Issues, Universal-Publishers.Varshney, U., 2009. • Pervasive Healthcare Computing: EMR/EHR, Wireless and Health Monitoring, Springer. Whetton, S., 2005. • Health informatics: a socio-technical perspective, Oxford University Press. Winter, A., Haux, R., Ammenwerth, E., Brigl, B., Hellrung, N. & Jahn, F., 2010. • Health Information Systems: Architectures and Strategies, Springer.

Health Informatics and Management Information
118/JNU OLE
Self Assessment Answers
Chapter I b1. d2. c3. a4. b5. a6. c7. a8. d9. a10.
Chapter IIb1. a2. b3. a4. a5. d6. a7. a8. b9. b10.
Chapter IIIa1. b2. d3. c4. c5. a6. a7. c8. c9. a10.
Chapter IVa1. c2. b3. a4. a5. c6. a7. d8. d9. b 10.

119/JNU OLE
Chapter Va1. d2. b3. a4. a5. a6. c7. a8. a9. a10.
Chapter VIa1. c2. a3. b4. d5. a6. d7. a8. c9. b10.
Chapter VIIb1. a2. c3. d4. a5. d6. a7. c8. a9. c10.
Chapter VIIIa1. c2. a3. b4. c5. d6. c7. d8. a9. a10.