hypermetropia aphakia pseudophakia - srisoftssrisofts.com/cosi/para-medical/hypermetr… · ppt...
TRANSCRIPT

• The term hypermetropia is derived from hyper meaning “In excess” met meaning “measure” & opia meaning “of the eye”.
• Also called hyperopia / longsightedness
• First suggested in 1755 by KASTNER

DEFINITION• It is the refractive state of eye where in
parallel rays of light coming from infinity are focused behind the sentient layer of retina with accommodation being at rest
• The posterior focal point is behind the retina which receives a blurred image


ETIOLOGY1) AXIAL• Most common• Total refractive power of eye is normal• Axial shortening of eyeball• 1mm short- 3 D of HM• Physiologically more than 6D HM are
uncommon • At birth +2.5 – 3 D of HM (physiologically)• Pathologically seen in cases like orbital tumour,
inflammatory mass , oedema, coloboma and microphthalmos.

2) CURVATURAL• Flattening of cornea, lens or both• 1mm increase in Radius of curvature-
RESULTS IN 6D of HM• Never exceed 6D HM physiologically • Congenitally flattened (cornea plana)• Result (trauma and disease )3) INDEX • Change in refractive index with age • Physiologically in old age• Pathologically in diabetics under treatment

4)POSITIONAL• Posteriorly placed crystalline lens• Occurs as congenital anomaly • Result of trauma or disease5)ABSENCE OF LENS• Seen in aphakia

CLINICAL TYPES
• SIMPLE HYPERMETROPIA,• PATHOLOGICAL • FUNCTIONAL HYPEROPIA

SIMPLE HYPERMETROPIA
• Commonest form• Results from normal biological variations
in the development of eyeball• Include axial and curvatural HM• May be hereditary
PATHOLOGICAL HYPERMETROPIA• Anomalies lie outside the limits of biological
variation• Acquired hypermetropia
– Decrease curvature of outer lens fibers in old age
– Cortical sclerosis
• Positional hypermetropia • Aphakia • Consecutive hypermetropia
FUNCTIONAL HYPERMETROPIA• Results from paralysis of accommodation
• Seen in patients with 3rd nerve paralysis & internal ophthalmoplegia

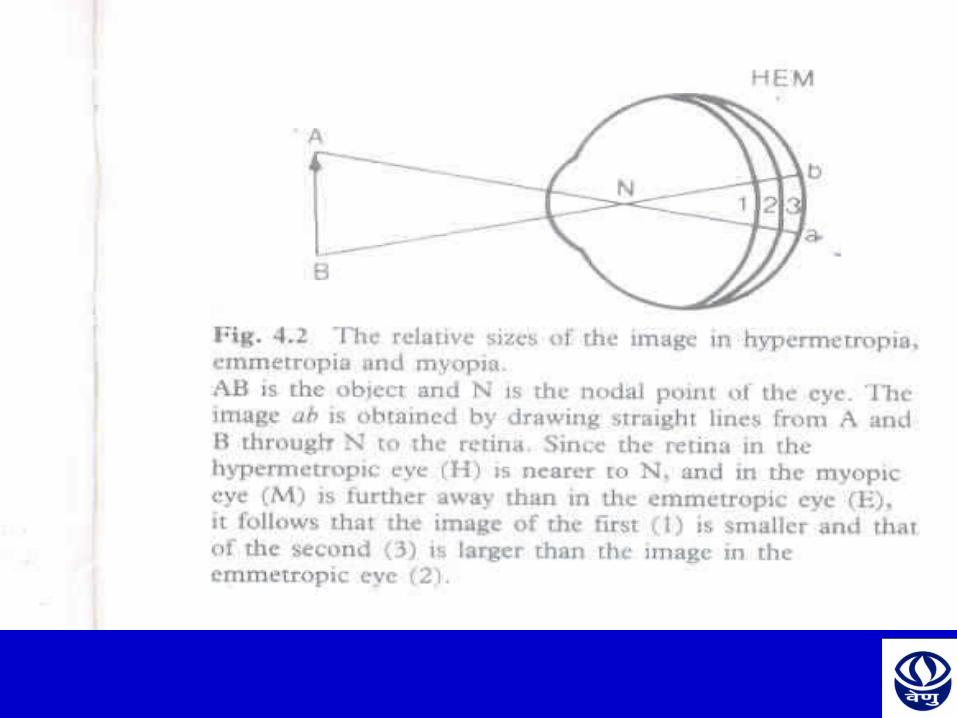
OPTICAL CONDITION• Parallel rays focus behind retina• Diffusion circles produce blurred & indistinct
images• Retina is nearer to nodal point• Image is smaller than in emmetropic• Rays diverge from retina• Formation of clear image is possible only when
converging power of eye is increased


NOMENCLATURE
TOTAL HYPERMETROPIA= LATENT + MANIFEST (facultative + absolute)

TOTAL HYPERMETROPIA
• It is the total amount of refractive error,estimated after complete cycloplegia with atropine
• Divided into latent & manifest

LATENT HYPERMETROPIA
• Corrected by inherent tone of ciliary muscle
• Usually about 1D• High in children • Decreases with age• Revealed after abolishing tone of ciliary
muscle with atropine

MANIFEST HYPERMETROPIA• Remaining part of total hypermetropia• Correct by accommodation and convex lens• Measure by add strongest lens with max. vision• Consists of facultative & absoluteFACULTATIVE HYPERMETROPIA• Corrected by patients accommodative effort ABSOLUTE HYPERMETROPIA• Residual part not corrected by patients
accommodative effortAbsolute hypermetropia can be measured by the weakest convex lens with which maximum visual acuity

MANIFEST HYPERMETROPIA CONT…
• Manifest HM – absolute HM = Facultative HM(Strongest lens) – (weakest lens)• Total HM – Manifest HM = Latent HM

NORMAL AGE VARIATION At birth +2+3D HM• Slightly increase in one year of life, • Gradually diminished untill by the age 5-10 years In old age after 50 year again tendency to HM
Ton of ciliary muscle decreases Accommodative power decreases Some amount of latent HM become manifest More amount of facultative HM become absolute Practically after 65 year all of it become absolute
SYMPTOMS• Principal symptom is blurring of vision for close
work• Symptoms vary depending upon age of patient &
degree of refractive error ASYMPTOMATIC• small error produces no symptoms• Corrected by accommodation of patient
ASTHENOPIA• Refractive error are fully corrected by
accommodative effort • Thus vision is normal• Sustained accommodation produces symptoms• Asthenopia increases as day progresses • Increased after prolonged near workSYMPTOMS Tiredness Frontal or fronto temporal headache Watering Mild photophobia

DEFECTIVE VISION WITH ASTHENOPIA
• Not corrected by accommodation • Defective vision for near more than
distance• Asthenopia due to sustained
accommodation• Refractive error more(>4D)

DEFECTIVE VISION ONLY
• Refractive vision more than 4D • Adults usually do not accommodate • Marked defective vision for near and
distance
SIGNS
• VISUAL ACUITY : Defective• EYEBALL: small or normal in size• CORNEA : may be smaller than normal.
There can be CORNEA PLANA• ANTERIOR CHAMBER : may be shallow • LENS: could be dislocated backwards• A Scan ultrasonography (biometry) reveal
short axial length

FUNDUS:A) DISC: Dark reddish color, irregular
margins ,confused with Papillitis so termed as PSEUDO-PAPILLITIS
B) MACULA: Situated further from the disc than usual, large positive angle alpha, apparent divergent squint
C) BLOOD VESSELS: Show undue tortuosity & abnormal branchings
D) BACKGROUND: SHOT- SILK RETINA

COMPLICATION • Recurrent styes m blepharitis or chalazia • Accommodative convergent squint• Amblyopia
– Anisometropic– Stravismic– Uncorrective bilateral high hypermetropia
• Predisposition to develop primary narrow angle glaucomas
Care should be taken while instilling mydriatics
BASIS FOR TREATMENT• No TreatmentError is smallAsymptomaticVisual acuity normalNo muscular imbalance
TREATMENT

Young children(<6 or 7yrs)Some degree of hypermetropia is physiological so
no correctionTreatment required if error is high or strabismus is
present working in school small error may require
correction In children error tends normally to diminish with
growth so refraction should be carried out every six month and if necessary the correction should be reduced, ortherwise a lens which is overcorrecting their error may induce an artificial myopia
No deduction of tonus allowance in strabismus

ADULTSIf symptoms of eye-strain are marked,we
correct as much of the total hypermetropia as possible,trying as far as we can to relieve the accommodation
When there is spasm of accommodation we correct the whole of the error
Some patients with hypermetropia do not initially tolerate the full correction indicated by manifest refraction so we undercorrect them
Exophoria hyperopia should be under correct by 1 to 2D

Patients with absolute hypermetropia are more likely to accept nearly the full correction because they typically experience immediate improvement in visual acuity
In pathological hypermetropia the underlying cause rather than the hypermetropia is chief concern
MODE OF TREATMENT
• SPECTACLES
• CONTACT LENS
• SURGICAL
OPTICAL TREATMENT

SPECTACLES
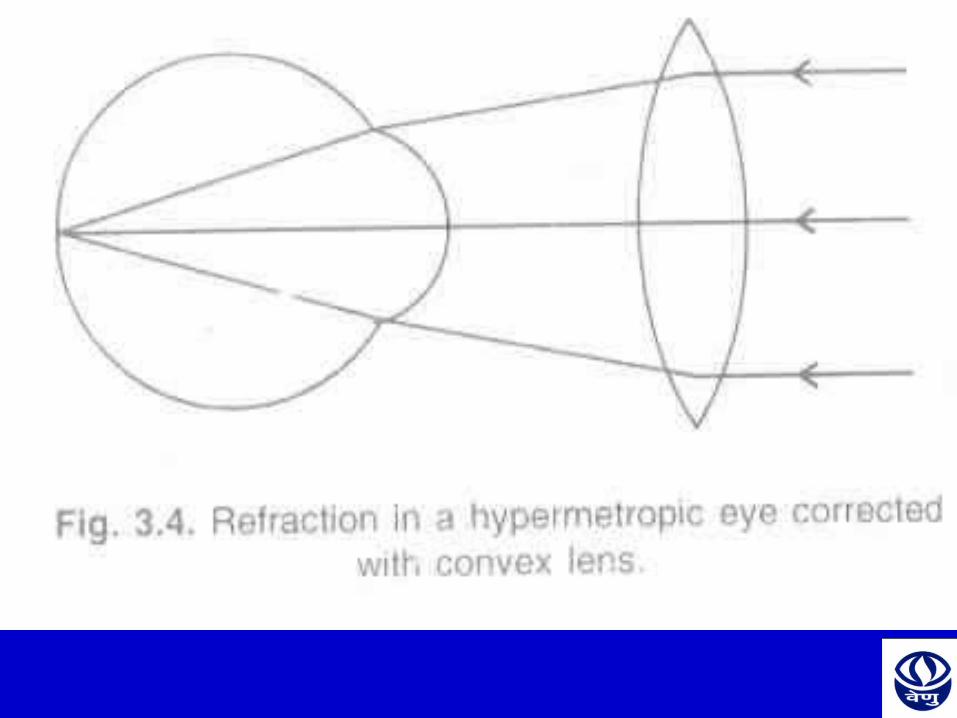
Basic principlePrescribe convex lenses(Plus lenses) so that rays are brought to focus on the retina
Advantages• Comfortable• Easier method• Less expensive• Safe idea

CONTACT LENS
ADVANTAGESCosmetically good
Increased field of view
Less magnification
Elimination of aberrations & prismatic effect

REFRACTIVE SURGERY• Refractive surgery is not as effective as in
myopia
TYPES:
(1)HEXAGONAL KERATOTOMY(HK)• Low to moderate degrees of hypermetropia• Its risk /benefit ratio is not low enough to warrant
its continued use


LASER THERMAL KERATOPLASTY(LTK)
• Procedure done using laser energy to heat the cornea (contraction of collagen) and increase its curvature
• Central heating of cornea results in central corneal flattening thereby resulting in hyperopic shift
PHOTOREFRACTIVE KERATECTOMY(PRK)
• Direct laser ablation of corneal stroma after removal of corneal epithelium mechanically
• Done using EXCIMER LASER

LASER IN SITU KERATOMILEUSIS(LASIK)
• Anterior flap of cornea lifted with keratome and excimer laser is used to sculpt the stromal bed to change the refractive error of eye
• It can correct up to 4D of hypermetropia and 8D of astigmatism

PHAKIC IOL AND CLEAR LENS EXTRACTION
• Done by Phaco technique • Clear lens extraction with the implantation of an
IOL-----Preferably foldable IOL or a Piggyback IOL is implanted

VISUAL HYGIENE• While reading or doing intensive near work take
a break about every 30 min• When reading maintain proper distance that is
the book should be at least as far from your eyes as your elbow when you make a fist and hold it against your nose
• Sufficient Illumination• Place a limit spent watching television &
watching videogames• Sit 5-6 feet away from the television

• Appropriate optical correction almost always leads to clear and comfortable single binocular vision
• Younger children who have significant hyperopia associated with amblyopia, strabismus,or anisometropia require treatment, starting as early as 3-6 months of age
CONCLUSION• Hyperopia is a common refractive disorder that
has been overshadowed by myopia in public perception,vision research & the scientific literature
• Although uncorrected myopia has a greater adverse effect on visual acuity than uncorrected hyperopia,the close association between hyperopia,amblyopia & strabismus,especially in children,makes hyperopia a greater risk factor for more permanent vision loss than myopia

• The early diagnosis & treatment of significant hyperopia & its consequences can prevent a significant amount of visual disability in the general population

For Further Queries Contact :Ms. Priyanka SinghHead – Optometry ServiceEmail – [email protected]