iaea code of practice patientdosimetri - linköping university · iaea code of practice ... ct...
TRANSCRIPT
CPD/ST- and PhD course Linköping 2014 04 15 Gudrun Alm Carlsson
IAEA Code of practice Patient dosimetry in projection
radiography
Why is patient dosimetry important?
X-ray diagnostics provides the largest population dose from artificial sources (90% of all medical irradiations)
Besides the need for jusitification there is need for optimizing
imaging techniques so that sufficient image quality is obtained at the lowest possible patient doses
Dose reductions of 10-15 % are considered wortwhile if
diagnostic information remains sufficient
Which requirements must be put on dose measurements?
Goals of the Code of Practice (2007) and ICRU 74 (2005) Accuracy in dose measurements to be within 7% (k=2) Increased demands for dosimetry it has become
important to provide traceability to primary standards for dose measurements
Main aims of patient dosimetry (1) to determine dosimetric quantities for establishment of diagnostic reference levels (DRL) as check of good practice (2) to assist in assessing detriment or harm
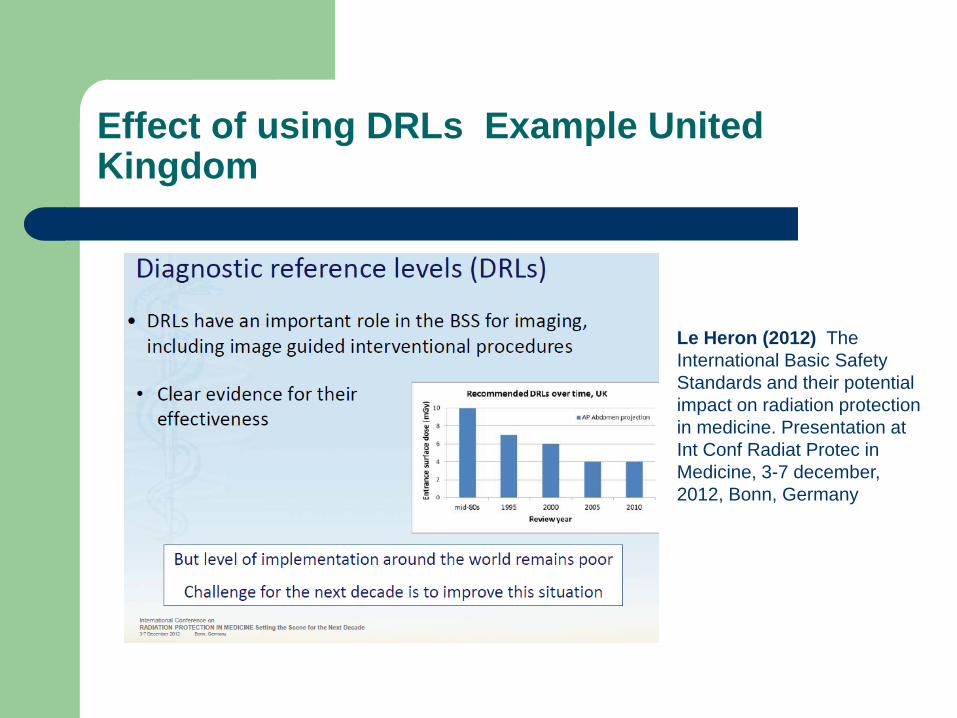
Effect of using DRLs Example United Kingdom
Le Heron (2012) The International Basic Safety Standards and their potential impact on radiation protection in medicine. Presentation at Int Conf Radiat Protec in Medicine, 3-7 december, 2012, Bonn, Germany
Dose quantities for ionizing radiation
Two types of dose quantities Fundamental quantities - ICRU (2011)
Application specific quantities - ICRU (2005) - IAEA (2007)
Fundamental quantities and units Energy imparted
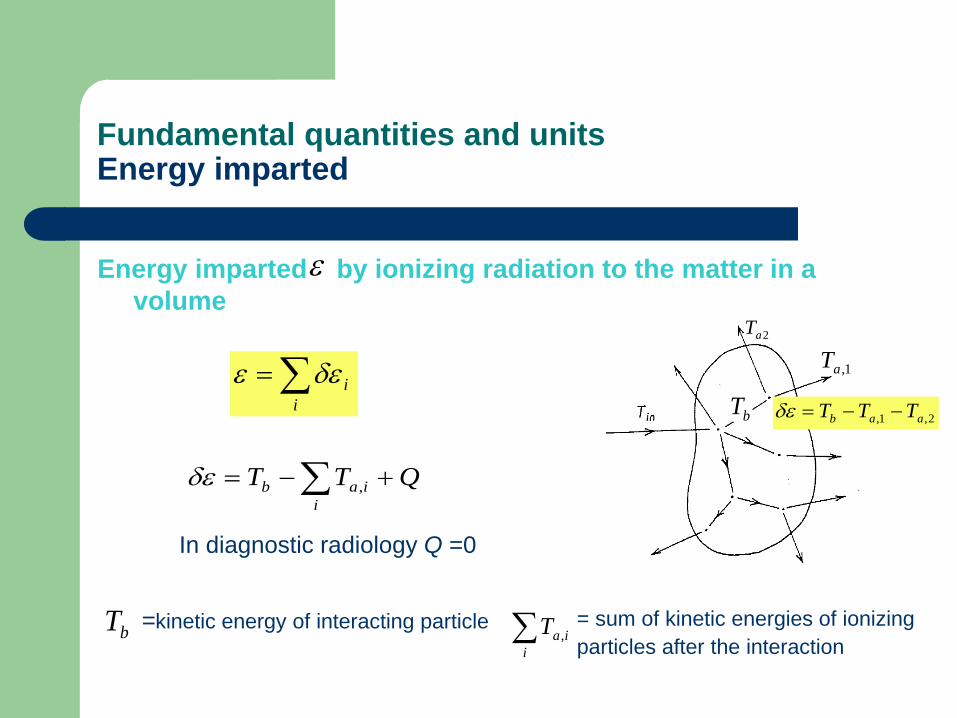
Energy imparted by ionizing radiation to the matter in a volume
ε
∑=i
iδεε
QTTi
iab +−= ∑ ,δε
In diagnostic radiology Q =0
=kinetic energy of interacting particle bT ∑i
iaT ,= sum of kinetic energies of ionizing particles after the interaction
bT
2aT
1,aT
2,1, aab TTT −−=δεbT
Fundamental quantities Absorbed dose
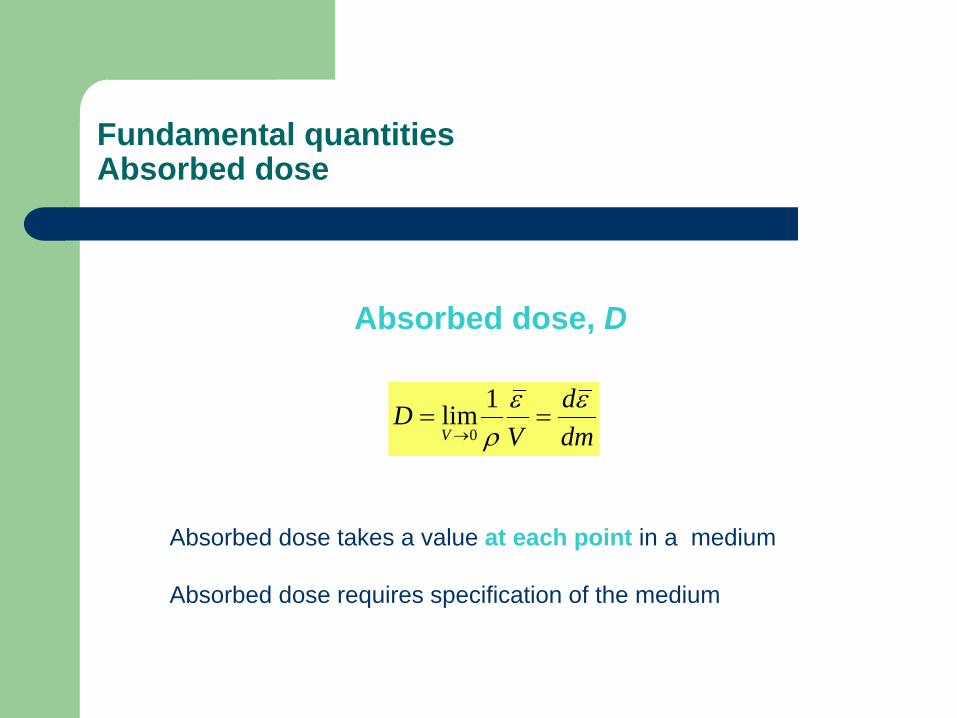
Absorbed dose, D
dmd
VD
V
εερ
==→
1lim0
Absorbed dose takes a value at each point in a medium Absorbed dose requires specification of the medium
Fundamental quantities Kerma and Collision kerma
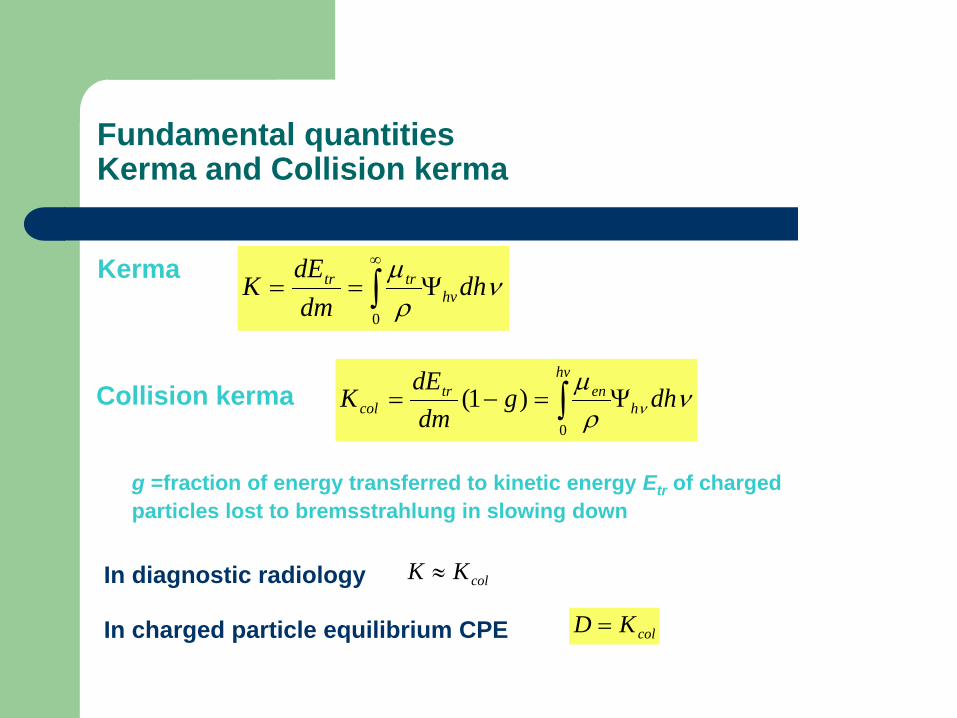
Kerma νρµ
dhdmdE
K hvtrtr Ψ== ∫
∞
0
Collision kerma νρµ
ν dhgdmdE
K h
hventr
col Ψ=−= ∫0
)1(
g =fraction of energy transferred to kinetic energy Etr of charged particles lost to bremsstrahlung in slowing down
In diagnostic radiology
In charged particle equilibrium CPE
colKK ≈
colKD =
Application specific dose quantities ICRU 2005 and IAEA 2007
The latest definitions of Application specific dose quantities have been published by ICRU 2005 and IAEA 2007 The documents are harmonized so that definitions and formalisms are the same ICRU Report No 74 (2005): Patient dosimetry for x-rays used in
medical imaging IAEA (2007): Dosimetry in diagnostic radiology: An international
Code of Practice, Technical Report Series No 457
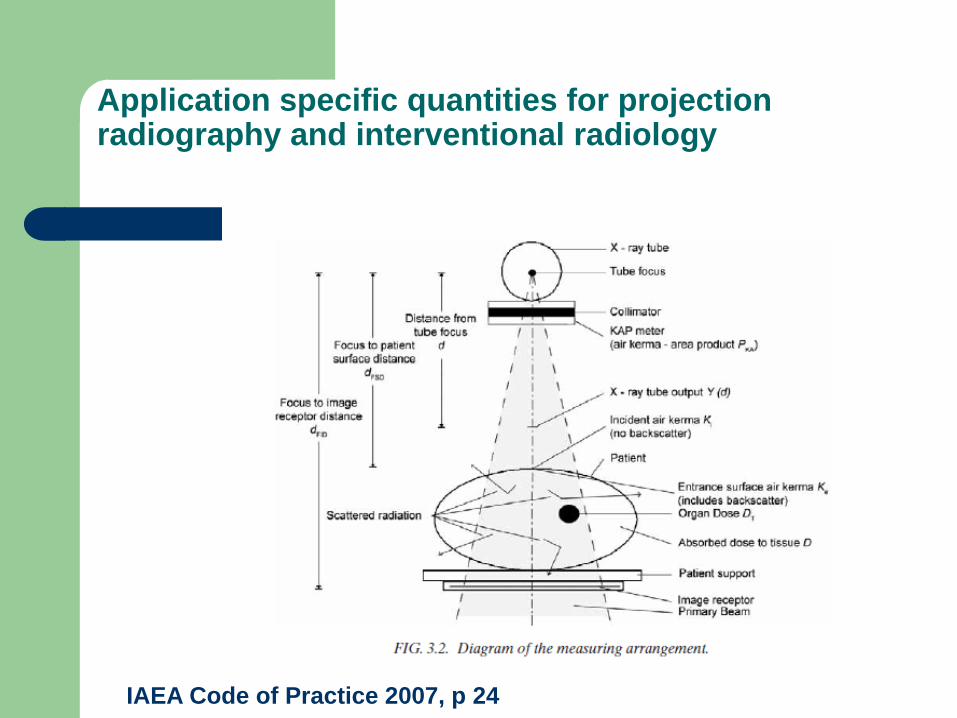
Application specific quantities for projection radiography and interventional radiology
IAEA Code of Practice 2007, p 24
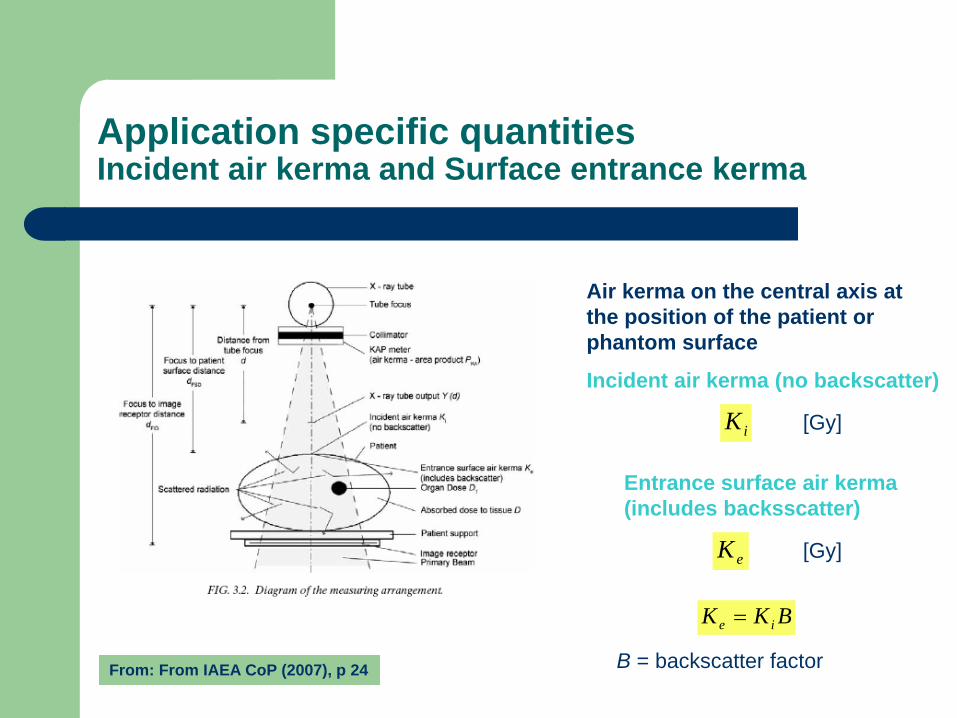
Application specific quantities Incident air kerma and Surface entrance kerma
From: From IAEA CoP (2007), p 24
Air kerma on the central axis at the position of the patient or phantom surface
Incident air kerma (no backscatter)
iK [Gy]
Entrance surface air kerma (includes backsscatter)
eK [Gy]
BKK ie =
B = backscatter factor
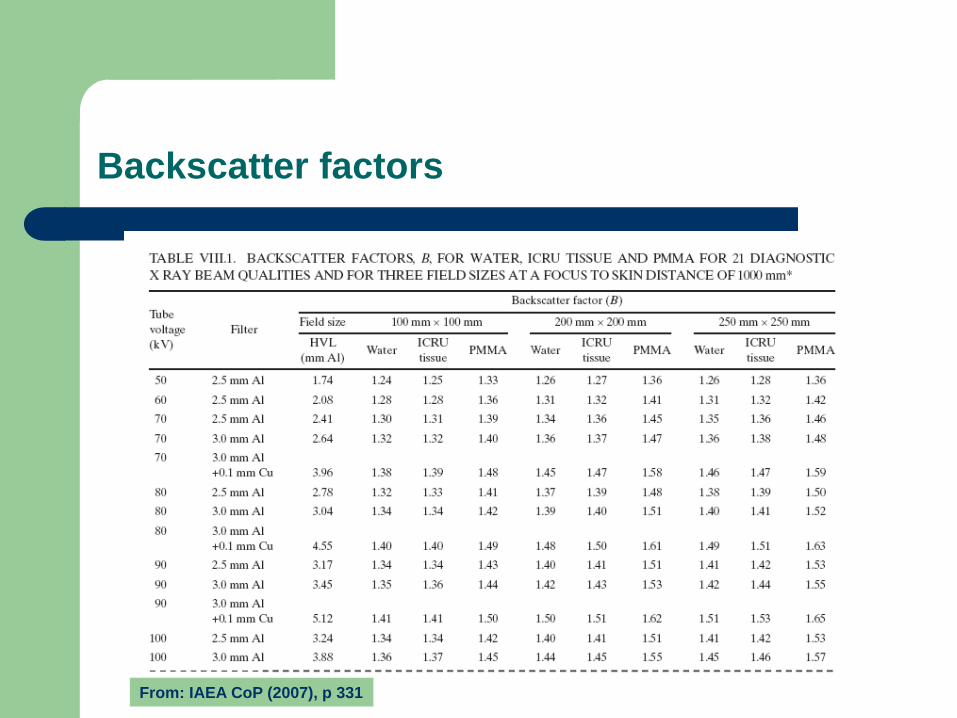
Backscatter factors
From: IAEA CoP (2007), p 331
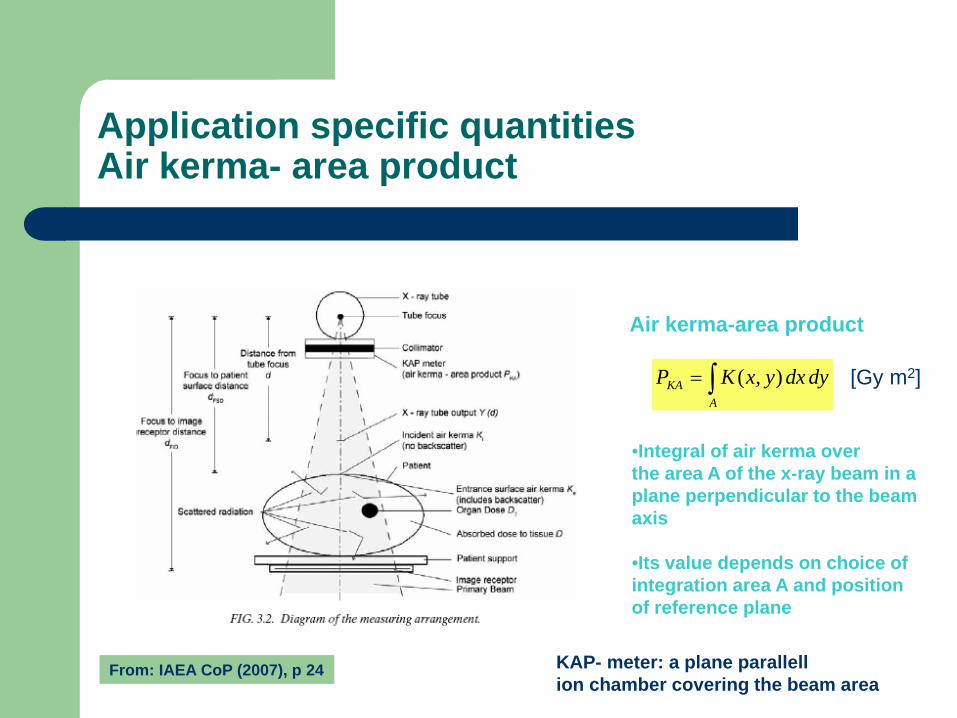
Application specific quantities Air kerma- area product
From: IAEA CoP (2007), p 24
Air kerma-area product
∫=A
KA dydxyxKP ),(
•Integral of air kerma over the area A of the x-ray beam in a plane perpendicular to the beam axis •Its value depends on choice of integration area A and position of reference plane
KAP- meter: a plane parallell ion chamber covering the beam area
[Gy m2]
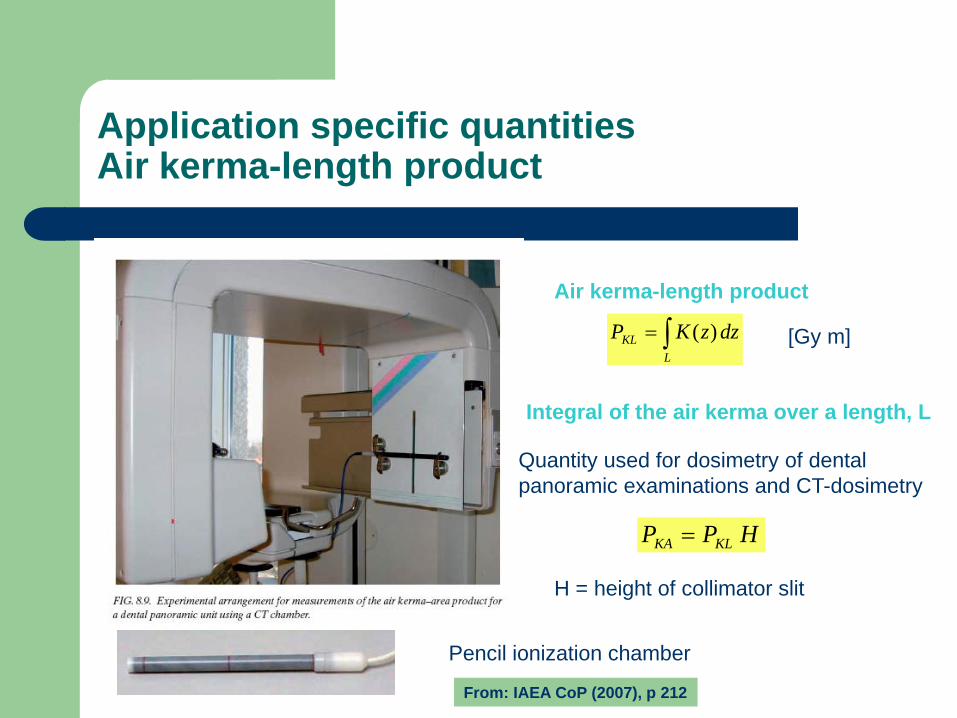
Application specific quantities Air kerma-length product
Air kerma-length product
∫=L
KL dzzKP )( [Gy m]
Integral of the air kerma over a length, L
Quantity used for dosimetry of dental panoramic examinations and CT-dosimetry
HPP KLKA =
H = height of collimator slit
Pencil ionization chamber
From: IAEA CoP (2007), p 212
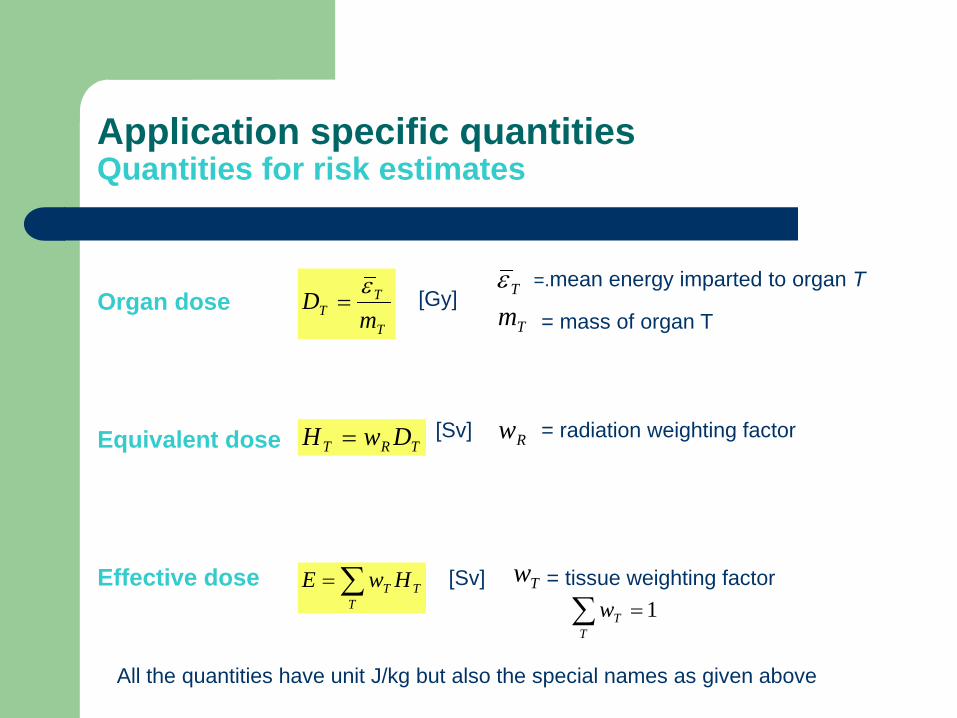
Application specific quantities Quantities for risk estimates
Organ dose Equivalent dose Effective dose
T
TT m
D ε= Tε
Tm=.mean energy imparted to organ T
= mass of organ T
TRT DwH = Rw = radiation weighting factor
[Gy]
[Sv]
TT
T HwE ∑= [Sv]
All the quantities have unit J/kg but also the special names as given above
Tw = tissue weighting factor 1=∑
TTw

How can effective dose be used?
Effective dose may be used as a tool to compare and optimize imaging tecniques
Effective dose must not be used for estimating the risk to individual patients to develop cancer after an examination or to predict the number of cancer cases induced in a population from x-ray diagnostics
The tissue weighting factors, depending on age and gender,
are associated with large uncertainties
How can effective dose be determined?
We need to be able to determine organ doses!
How can conversion coefficients that convert measurable
quantities into organ doses be determined?
Phantoms for dose measurements
Standardized physical phantoms for measurement of incident air kerma
Antropomorphic phantoms for measurement of organ doses
Monte Carlo calculations and virtual phantoms for determining organ doses
Two types of phantoms (1) mathematical phantoms (2) voxel phantoms constructed from post mortem CT images
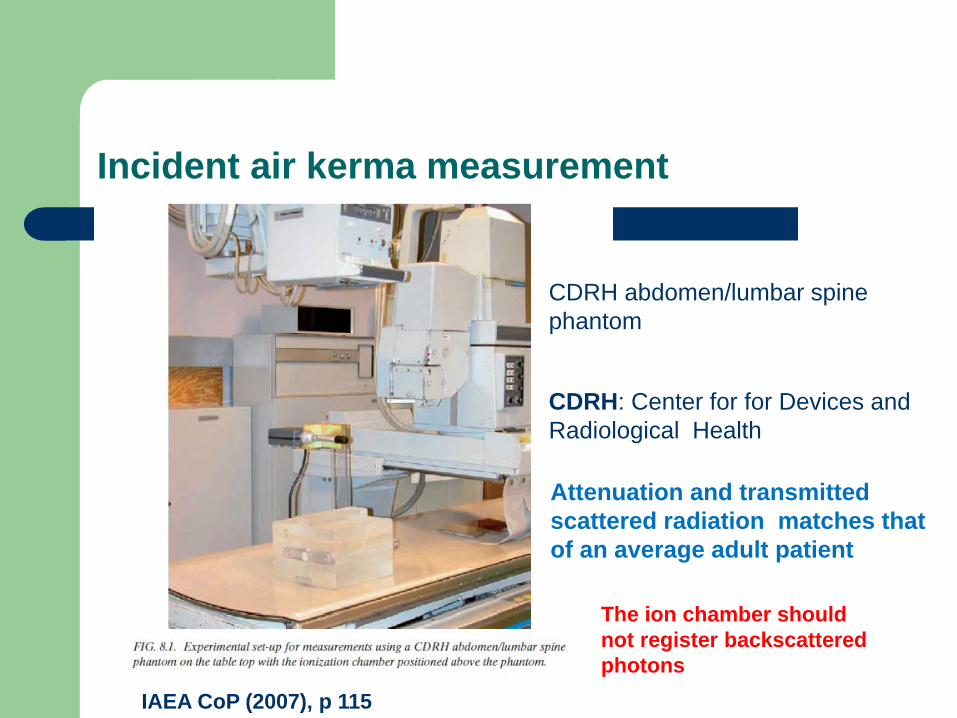
Incident air kerma measurement
CDRH abdomen/lumbar spine phantom
CDRH: Center for for Devices and Radiological Health
Attenuation and transmitted scattered radiation matches that of an average adult patient
IAEA CoP (2007), p 115
The ion chamber should not register backscattered photons
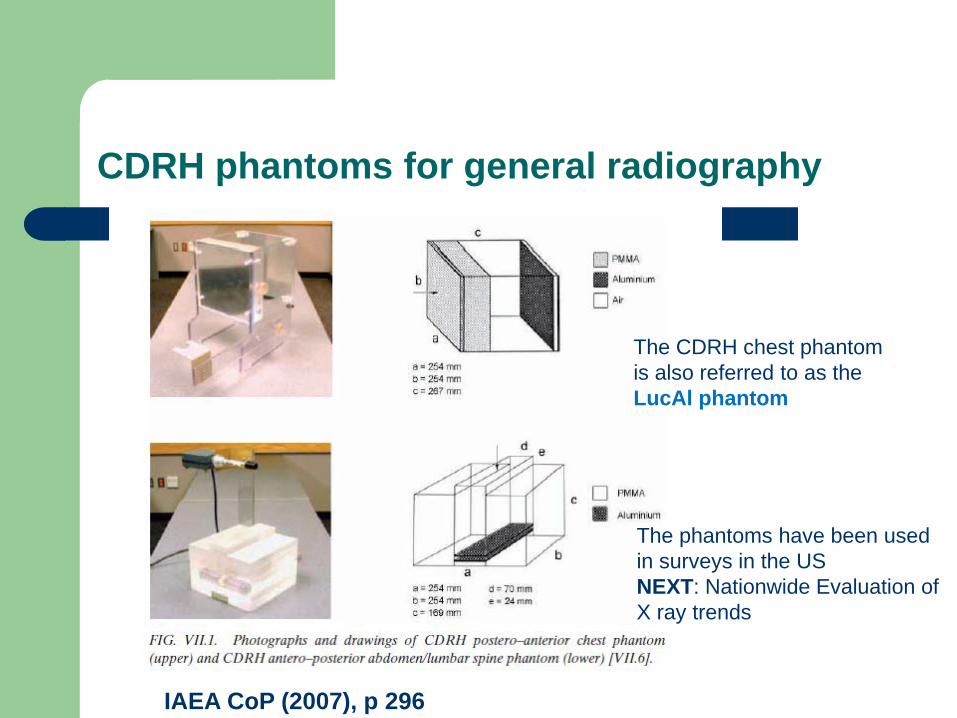
CDRH phantoms for general radiography
IAEA CoP (2007), p 296
The phantoms have been used in surveys in the US NEXT: Nationwide Evaluation of X ray trends
The CDRH chest phantom is also referred to as the LucAl phantom

Phantoms for fluoroscopy – measurement of entrance surface air kerma
IAEA CoP (2007), p141 After Martin et al (1998) Br J Radiol 71, 1283-1287
Water phantom c standard adult c+d thick patient
IAEA CoP (2007), p 300
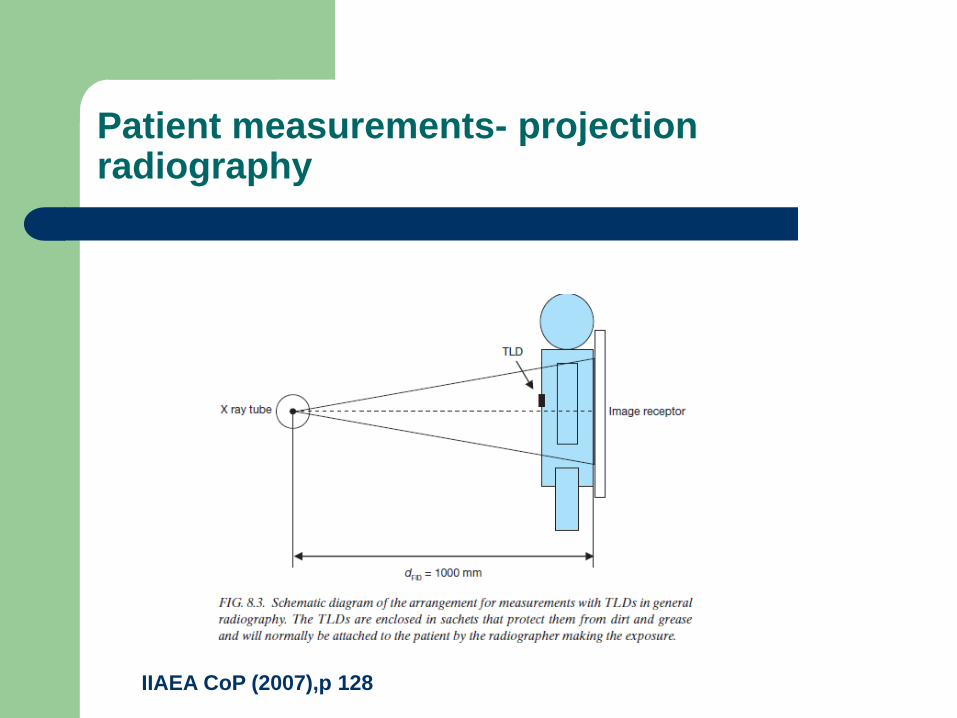
Patient measurements- projection radiography
IIAEA CoP (2007),p 128
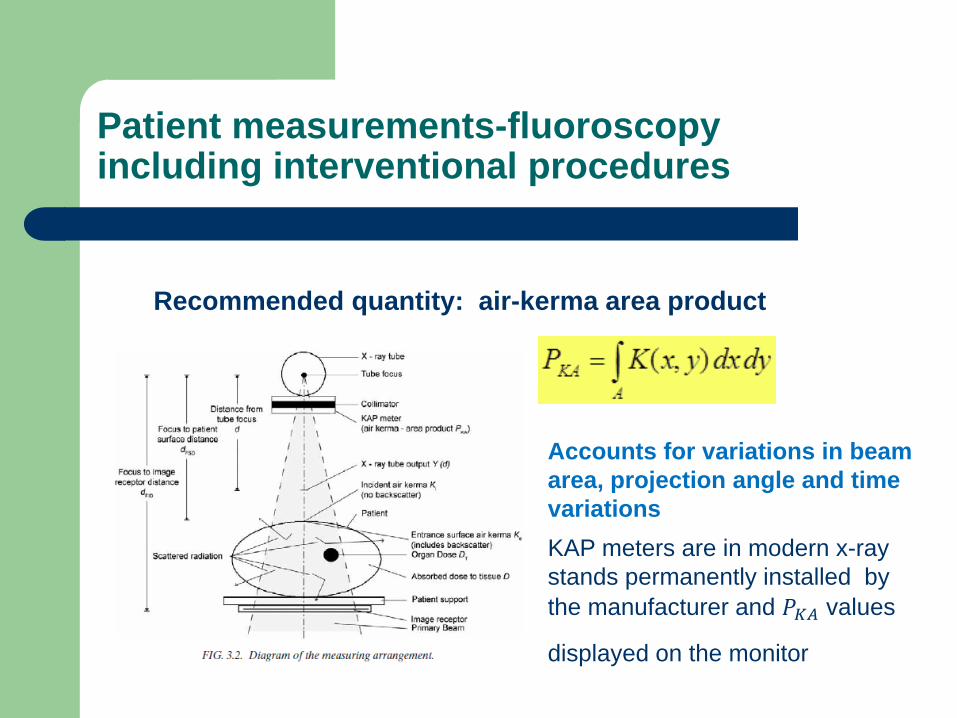
Patient measurements-fluoroscopy including interventional procedures
Recommended quantity: air-kerma area product
Accounts for variations in beam area, projection angle and time variations KAP meters are in modern x-ray stands permanently installed by the manufacturer and 𝑃𝐾𝐾 values
displayed on the monitor

Determination of organ doses- physical phantoms
Anthropomorphic phantoms with inserts for dosimeters are useful in estimating organ doses from complex examinations such as fluoroscopy (including interventional procedures) Drawbacks: Tedious measurements Difficult to determine mean absorbed
doses to distributed and large organs such as the red bone marrow and the lungs
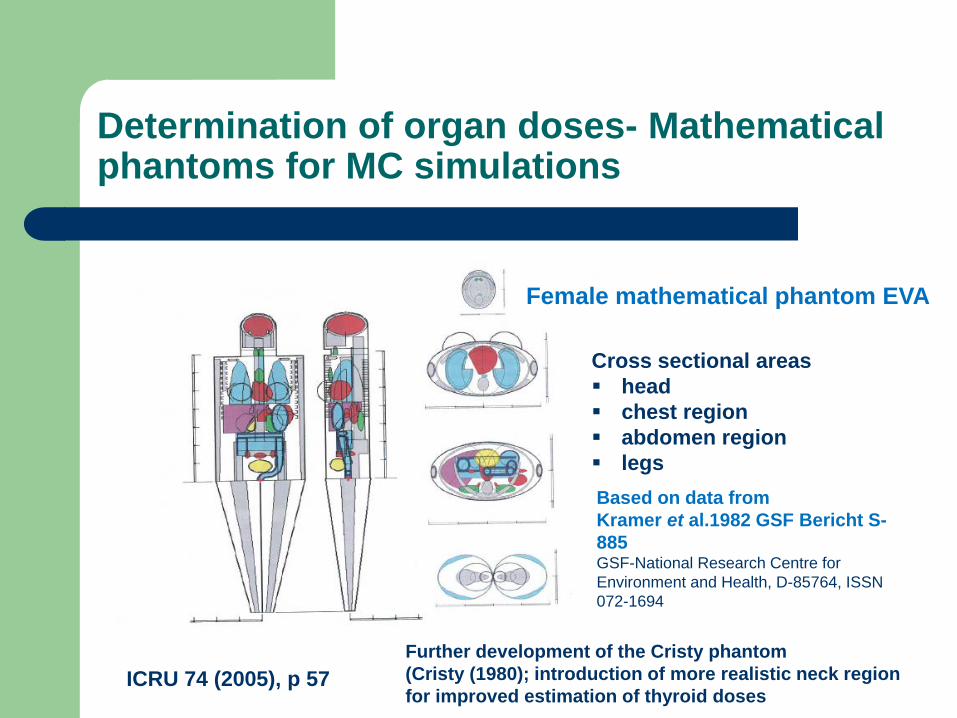
Determination of organ doses- Mathematical phantoms for MC simulations
ICRU 74 (2005), p 57
Female mathematical phantom EVA
Cross sectional areas head chest region abdomen region legs Based on data from Kramer et al.1982 GSF Bericht S-885 GSF-National Research Centre for Environment and Health, D-85764, ISSN 072-1694
Further development of the Cristy phantom (Cristy (1980); introduction of more realistic neck region for improved estimation of thyroid doses
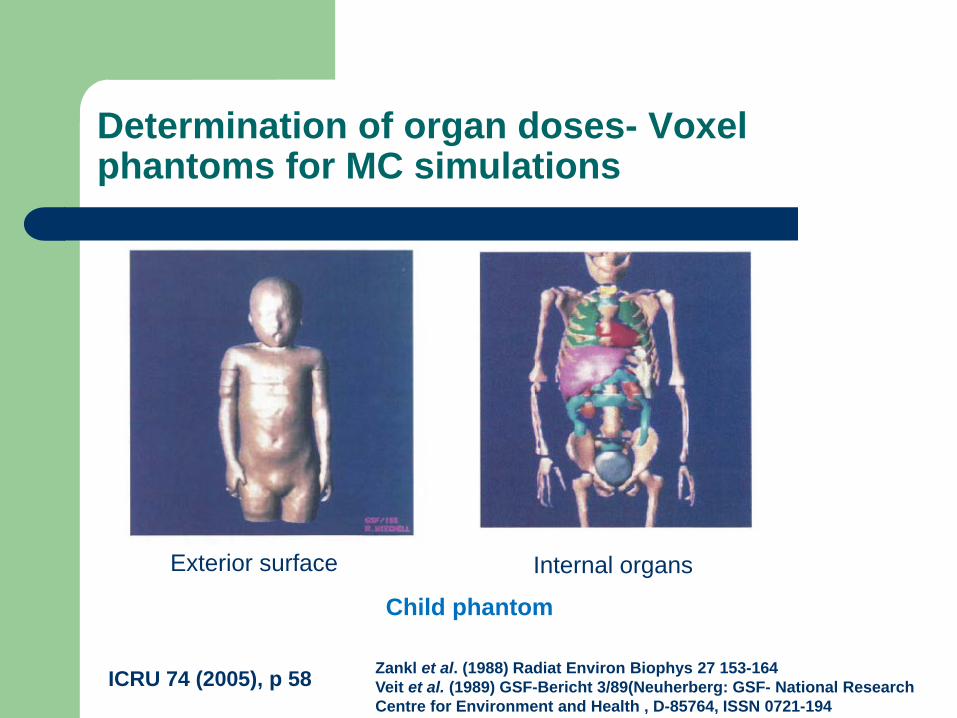
Determination of organ doses- Voxel phantoms for MC simulations
Exterior surface Internal organs
ICRU 74 (2005), p 58
Child phantom
Zankl et al. (1988) Radiat Environ Biophys 27 153-164 Veit et al. (1989) GSF-Bericht 3/89(Neuherberg: GSF- National Research Centre for Environment and Health , D-85764, ISSN 0721-194

Voxel phantoms developed at GSF
IAEA CoP (2007), p 269
The PCXMC program (STUK)
PC based Monte Carlo program for calculating organ doses (radiography and fluoroscopy Cristy mathematical phantoms (Cristy 1980) for patients of different age and size • Freely adjustable projections and examination conditions • Phantom sizes can be scaled by changing weight or height • Data on 𝑲𝒂,𝒊 or 𝑷𝑲𝑲 must be supplied by the user of the program
Tapiovaara et al. (1997) Report STUK A139 (Helsinki)

Uncertainties in Monte Carlo organ-dose calculations
Uncertainties are due to (1) Statistics of the MC simulations - depends on the number photons simulated and the position of the organ/tissue (if inside or far away from the primary beam)
(2) Accuracy of interaction coefficients used in MC simulations (of minor importance)
(3) The model of the human anatomy (phantom) used
Uncertainties in calculated organ doses
Type of examination and position in relation to field boundaries Example: Chest radiography (Schultz et al. (1994) Br J Radiol 67, 775-785) Uncertainty <0.3 to 0.9% in lungs >19-48% in the lower large intestines Tissue characterization In ADAM and EVA: 4 tissue types (lung, skeletal, skin, soft tissue) Voxel BABY and CHILD: 5 and 6 tissue types Voxel GOLEM: 8 tissue types (Zankl and Wittman (2001) Radiat Environ Biophys 40, 153-162) Calculations with 4 and 18 tissue types indicates that the uncertainty of considering only a small number of tissue types do not exceed 10% (Pani et al. (1987) Nucl Instrum Meth Phys Res A255, 360-364)
Uncertainties in calculated organ doses
Type of phantom: Mathematical or Voxel phantoms Difficulty to position the simulated radiation field using mathematical phantoms Example: Chest imaging The lungs are not curved at the mediastinum in the mathematical phantom. Small shifts in height for chest radiography can result in large changes in organ doses, for example, a factor of 3 for the spleen dose (due to smaller fractions of the organ in the primary beam than in real patients). Gosch and Gursky (1992) Radiat Prot Dosim 43, 115-117 Schultz et al. (1994) Br J Radiol 6, 775-785
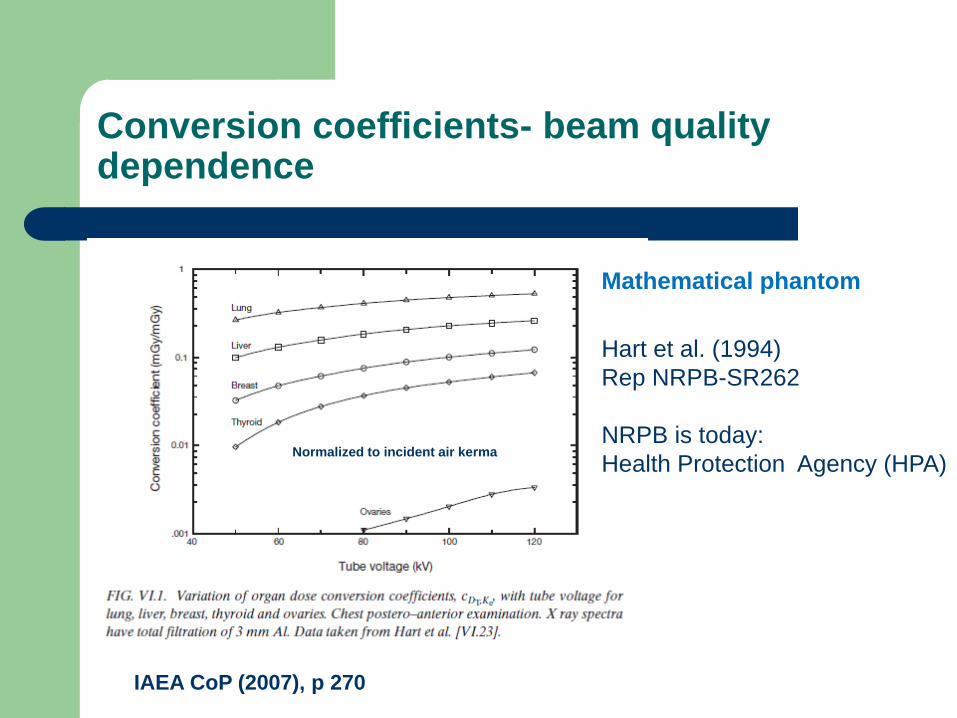
Conversion coefficients- beam quality dependence
IAEA CoP (2007), p 270
Hart et al. (1994) Rep NRPB-SR262 NRPB is today: Health Protection Agency (HPA) Normalized to incident air kerma
Mathematical phantom
Uncertainties in calculated organ doses
Conversion coefficients from different institutes
Chest imaging Schultz et al. (1994) Br J Radiol 67, 775-785 (Delfts, Netherlands) Drexler et al. (1990) GSF-Bericht 11/90, ISSN 0721-1694) CDRH Rosenstein (1988) HHS Publication FDA 89-8031 (US) Jones and Wall; Hart et al. (1994,1996) NRPB -R186; -SR 262, -SR 279 (UK) GSF and Schultz et al. ADAM, Five organs of highest doses within 10% CDHR and Schultz et al. Male phantoms, 100 kV, BM doses, excellent agreement Thyroid doses up to 50% difference , strongly depending of the vertical position of the field NRPB and Schultz et al. NRPB hermaphrodite phantom and ADAM, within 20% for the most irradiated organs PCXMC and NRPB (same phantom models) Differences typically within <10% Tapiovaara et al. 1997; Jones and Wall 1985; Hart et al.(1994,1996)
Uncertainties in calculated organ doses
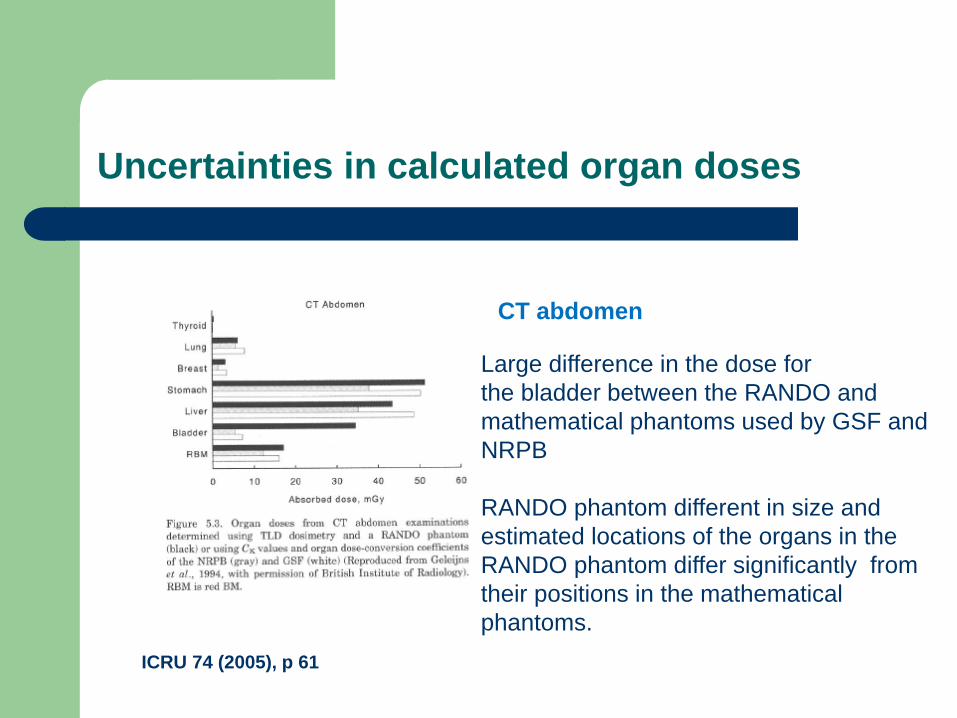
ICRU 74 (2005), p 61
Large difference in the dose for the bladder between the RANDO and mathematical phantoms used by GSF and NRPB RANDO phantom different in size and estimated locations of the organs in the RANDO phantom differ significantly from their positions in the mathematical phantoms.
CT abdomen
Availability of calculated organ doses
Tabulated conversion coefficients are available as derived from MC calculations for a large number of projections (examinations) and varity of beam qualities (for details see ICRU 74 (2005) Appendices B, C, D) CDHR Handbooks, US NHA (former NRPB), UK GSF, Germany Drawback Field sizes and positions are fixed PCXMC (STUK) allows the user to choose projections, exposure parameters and possibility to change the dimensions of the phantom (since 2012 also CT scanning)
Seidenbusch MC et al. (2008) Fortshr Röntgenstr 180, 1061 Reports paediatric conversion coefficients using PCXMC program

Paetriatic radiology
IIAEA Human Health Series No. 24 (2013) Dosimetry in diagnostic radiology for paedriatic patients
Complement to the IAEA CoP (2007)
MC calculations of organ doses are available for paediatric patients in terms of age specific anthropomorhic phantoms (see ICRU 74 (2005)
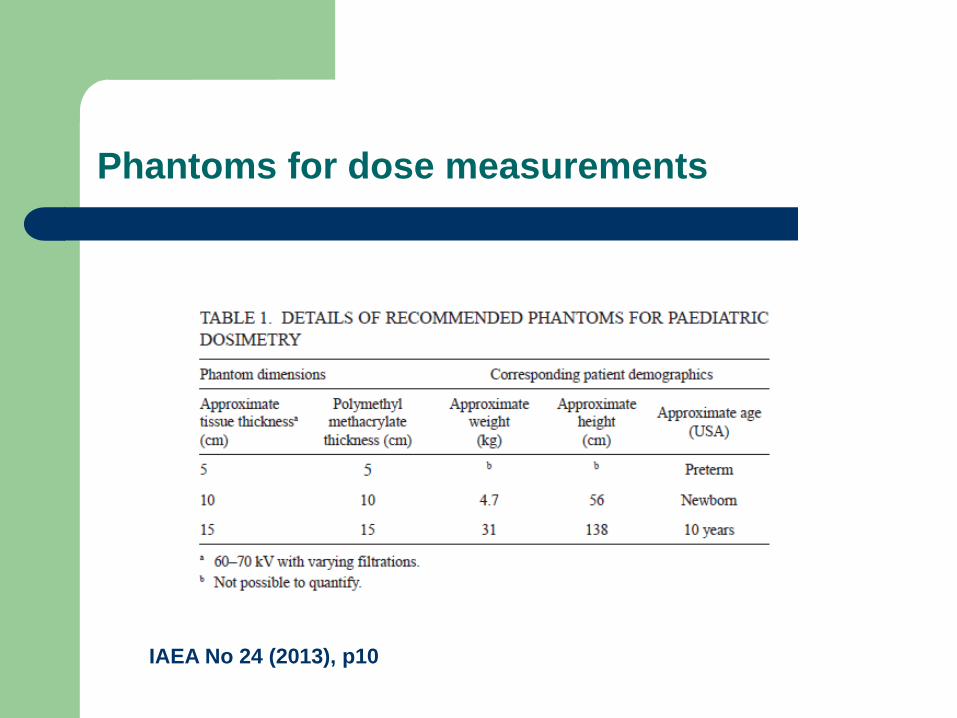
Phantoms for dose measurements
IAEA No 24 (2013), p10

Characterization of patient size
Concerns are raised as to the metric for the size of the paediatric patient . Age is a bad metric since weight and height vary considerably among
children of the same age The size of the patient is an important parameter for settings of the
technique parameters in CT. Use of protocols for adult patients results in excessive doses without a corresponding gain in image information.
CT examinations are of particular concern in paediatric radiology due to the relatively high doses
The concept of equivalent patient diameter
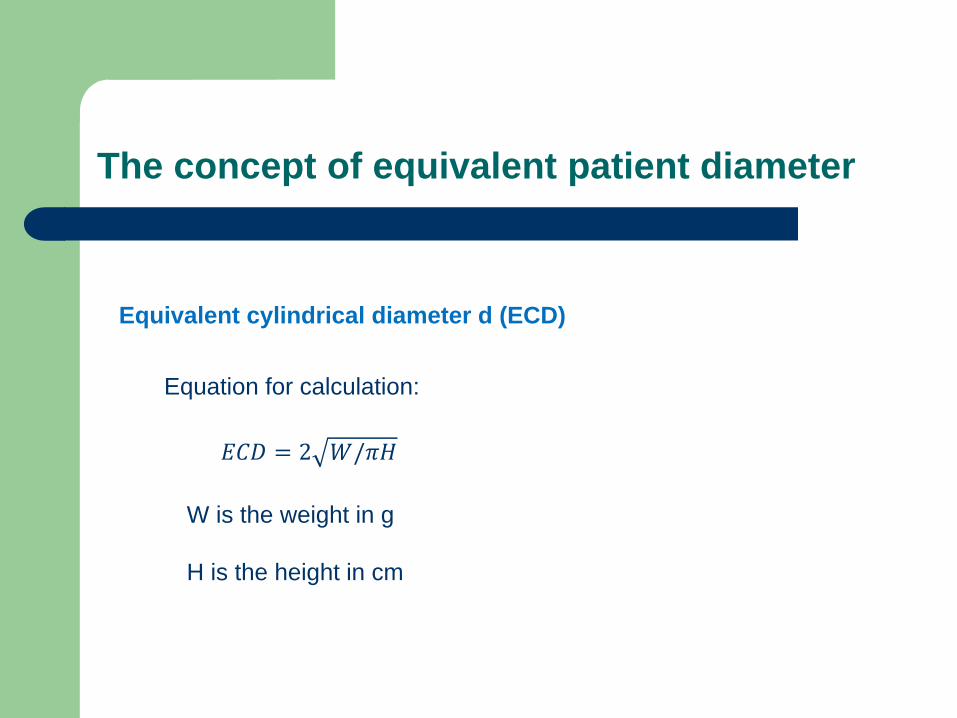
Equivalent cylindrical diameter d (ECD)
𝐸𝐸𝐸 = 2 𝑊/𝜋𝜋
W is the weight in g H is the height in cm
Equation for calculation:
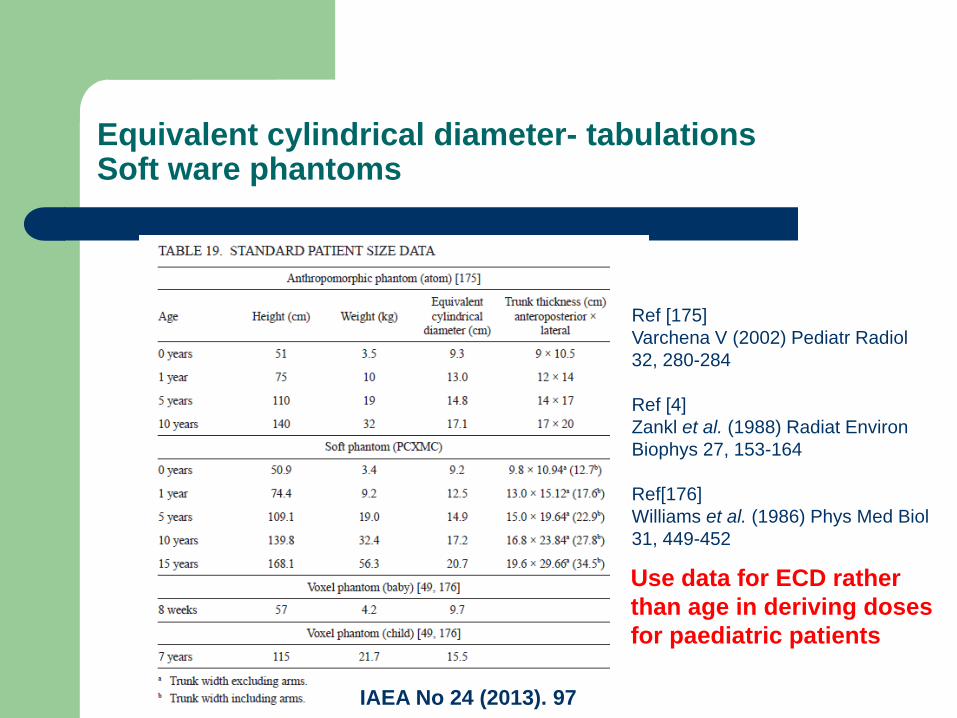
Equivalent cylindrical diameter- tabulations Soft ware phantoms
IAEA No 24 (2013). 97
Ref [175] Varchena V (2002) Pediatr Radiol 32, 280-284 Ref [4] Zankl et al. (1988) Radiat Environ Biophys 27, 153-164 Ref[176] Williams et al. (1986) Phys Med Biol 31, 449-452
Use data for ECD rather than age in deriving doses for paediatric patients
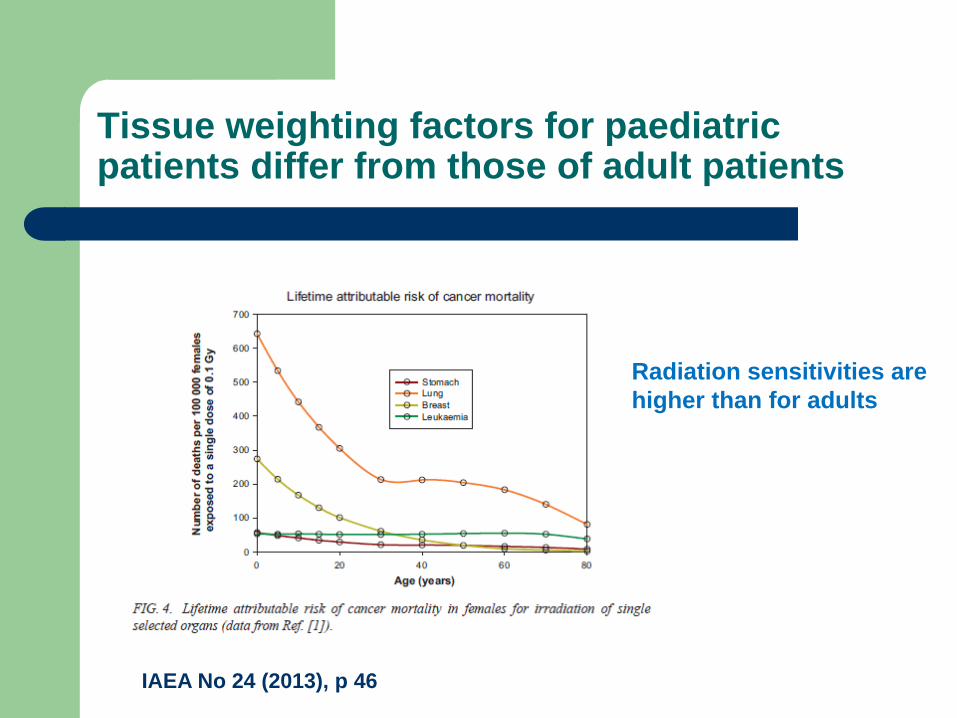
Tissue weighting factors for paediatric patients differ from those of adult patients
IAEA No 24 (2013), p 46
Radiation sensitivities are higher than for adults
The software phantom PCXMC
The PCXMC software package estimates age- and sex specific cancer risks for projection radiography/fluoroscopy and can modify the size of the phantom using a scaling factor for weight (M) and height (h) Scaling factors 𝑠𝑧 = ℎ/ℎ0 𝑠𝑥𝑥 = ℎ0𝑀/ℎ𝑀0
0.5
Index 0 indicates the corresponding values for basic phantom z-axis = phantom height xy- plane gives phantom width and thickness
Thank you for your attention!