incidental adnexal masses at ct
TRANSCRIPT

Incidental Adnexal Masses Detected at Low-Dose Unenhanced CT in Asymptomatic Women Age 50 and Older: Implications for Clinical Management and Ovarian Cancer Screening
©RSNA, 2010 • radiology.rsna.org
ByDr. Naglaa Mahmoud
Registrar of Clinical RadiologyKCCC

Introduction:
Ovarian cancer remains the leading cause of gynecologic
cancer–related deaths in the United States.
Five-year survival for ovarian cancer is greater than 90% for
localized disease, but the overall survival is well below 50%
because the majority of cases are advanced at diagnosis.
Introduction:
Unlike transvaginal ultrasonography or MR imaging, CT is
not intended for primary pelvic or gynecologic evaluation in
women. However, the widespread use of abdominal / pelvic
CT for a variety of other indications unavoidably includes
adnexal evaluation, often resulting in incidental lesion
detection.

Introduction:
In the case of CT colonography screening in asymptomatic
postmenopausal women, the identification of adnexal
lesions nearly always represents an unsuspected
incidental finding which allows for a unique opportunity to
investigate this well-suited cohort.

The purpose of this study was:
To determine the prevalence, work-up, and outcomes of
indeterminate adnexal masses identified at low-dose
unenhanced CT scan in asymptomatic women age 50 and
older undergoing colonography screening.

Materials and Methods:
This study was institutional review board approved.
Informed consent was waived.
The fate of indeterminate adnexal lesions identified at
unenhanced CT in 2869 consecutive women (mean age,
57.2 years; age range, 50–97 years) undergoing
colonography screening between April 2004 and
December 2008 was evaluated.

CT Technique
CT imaging of the abdomen and pelvis was performed for
the purpose of colorectal cancer screening by using a
colonographic technique.
The preimaging protocol for colonography includes bowel
preparation the evening before examination and gaseous
distention of the colon during the examination.

CT Technique
Supine and prone acquisitions were obtained with 8 or 16-
detector CT scanners by utilizing 1.25-mm collimation, 120
kVp, static (50–75 mAs) tube current technique, and 1-mm
reconstruction interval.
For extracolonic evaluation, the supine series was
reconstructed with a 5-mm section thickness at 3-mm
intervals.

CT Technique
Extracolonic CT interpretation was performed alongside the
prospective colorectal evaluation by one of five board-certified
abdominal radiologists, all with at least 10 years of experience
in gastrointestinal and genitourinary body CT interpretation.
Prospective categorization of extracolonic findings was applied
in all cases by utilizing the CT Colonography Reporting and
Data System (C-RADS).

CT Technique
According to C-RADS, E1 (normal finding) and E2
(unimportant finding) categories do not require further
work-up, whereas E3 (likely benign but incompletely
characterized) and E4 (potentially or definitely important)
findings often necessitate further evaluation.

Identification of the Study Cohort
The positive study cohort was defined by the presence
of an adnexal lesion with a C-RADS category of E3 or
E4.

Results:
One hundred eighteen women (mean age, 56.2 years),
representing 4.1% of the screening cohort, had an
indeterminate adnexal mass (108 unilateral, 10 bilateral; Mean
size, 4.1 cm) at prospective CT interpretation.
A total of 80 women underwent some combination of further
imaging evaluation (n = 76) (transvaginal ultrasonography [ n =
71], pelvic magnetic resonance imaging [ n = 7], contrast
material– enhanced CT [ n = 7]) and/or surgery ( n = 26).

Results:
Mean serum CA-125 level in 33 women was 12.8 U/mL;
levels were normal ( < 35 U/mL) in 32 (97%) cases (range,
3–26 U/mL) and mildly elevated (41 U/mL) in 1 case.

Results:
Final pathologic findings of surgically excised lesions were
cystadenoma or cystadenofibroma ( n = 14; 11 serous, three
mucinous); non neoplastic cysts ( n = 5; two
endometriomas); mature teratoma ( n = 3); hydrosalpinx ( n =
2); fibroma (n = 1); and benign Brenner tumor ( n = 1).
Three additional teratomas were diagnosed at index CT only.
No ovarian cancers were prospectively identified.

Various adnexal pathologic findings identified at routine CT colonography screening and surgically removed after further work-up. CT colonographic images in six women (age range, 51–63 years) show (a)mucinous cystadenoma,(b)bilateral serous cystadenomas,
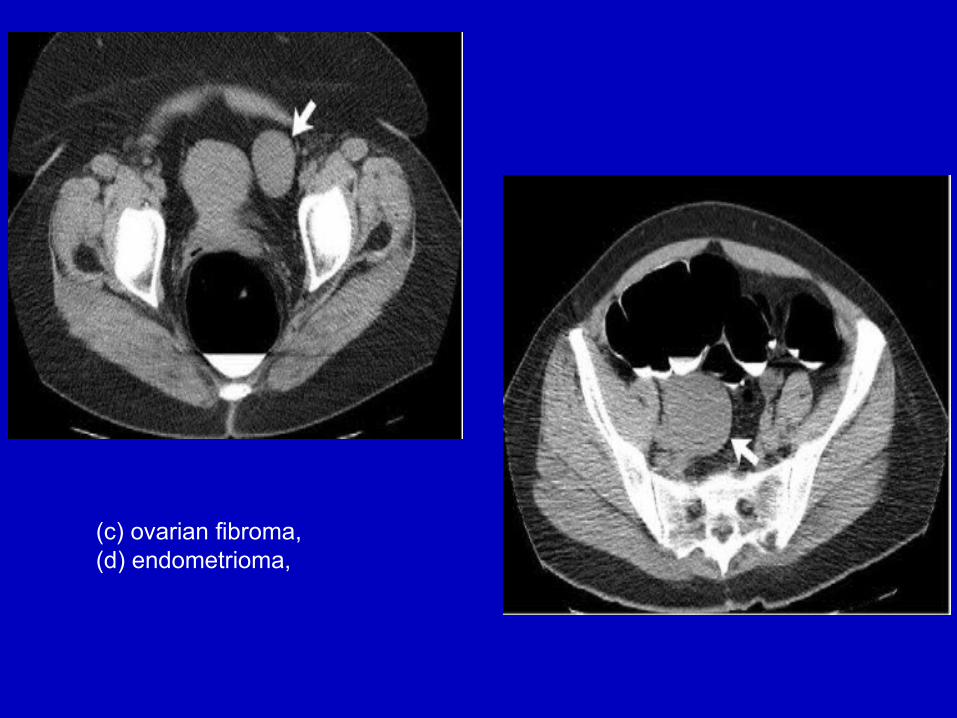
(c) ovarian fibroma, (d) endometrioma,

(e) paraovarian inclusion cyst, and (f) hydrosalpinx
Results:
A systematic search for subsequent diagnosis of ovarian
cancer in the larger cohort of 2751 women without an
adnexal mass of C-RADS category E3 or E4 at CT
colonography revealed 4 cases of ovarian cancer that
manifested 15–44 months (mean, 26.8 months) after a
negative finding at CT examination.

Results:
Pathologic diagnoses included 2 cases of mucinous
cystadenocarcinoma, 1 case of papillary serous carcinoma,
and 1 case of a poorly differentiated adenocarcinoma for
which ovarian versus peritoneal origin could not be
ascertained.

Mucinous cystadenocarcinoma that manifested 3 years after negative findings at CT colonography screening examination in 67-year-old woman. (a) Index CT colonographic image demonstrates symmetric-appearing normal ovaries. (b) Diagnostic contrast-enhanced CT image obtained 3 years later shows a large complex solid and cystic mass, which originated from the left ovary.


Discussion:
Ovarian cancer has a greater annual mortality than cervical and
endometrial cancers combined.
Prognosis remains poor in most cases because the disease is
usually advanced at diagnosis.

Discussion
Although effective screening for ovarian cancer is highly
desirable, there is currently no convincing evidence that it can
reduce mortality among average-risk women. The findings of
this study further support this unfortunate situation.
Furthermore, a negative finding at CT was not protective
against subsequent development of ovarian cancer, with all
four cases occurring in this cohort.

Discussion:
The main factors that diminish the potential utility of
screening are that indolent benign adnexal lesions are
relatively common in postmenopausal women, but ovarian
cancer is relatively rare and tends to grow rapidly.
Management algorithms generally recommend further work-
up of nearly all discrete adnexal masses detected at CT in
postmenopausal women.

Discussion:
In contrast to ovarian cancer, a number of other
extracolonic cancers have been identified at CT
colonography screening, generally at an early
presymptomatic stage with a favorable outcome.
This suggests that ovarian cancer is an aggressive tumor
that has a rather narrow window for presymptomatic
screening that may preclude effective screening detection in
the general population.

Discussion:
More sophisticated risk factor assessment may be required
to effectively identify and manage high-risk cases to improve
the overall yield of ovarian cancer screening.
Established risk factors include BRCA mutations, Lynch
syndrome, family history of ovarian or breast cancer, and a
personal history of breast cancer.

Limitations of the study
All CT examinations were performed by using a colonographic
technique with low-dose imaging and without intravenous
contrast material.
With the exception of ovarian teratomas, the ability to fully
characterize adnexal masses at low-dose unenhanced CT is
limited.

Conclusion:
Incidental indeterminate adnexal lesions were relatively
common at unenhanced CT scan (4.1%), but subsequent
work-up revealed no ovarian cancers.
Furthermore, a normal finding at CT was not protective
against short-term development of ovarian cancer.
More sophisticated risk factor assessment is needed to
identify women at higher risk.

Thank you