individualised systems medicine - labcyte.com and genetic aberrations that explain the drug ... and...
TRANSCRIPT
Cancer therapy increasingly involves the useof smart drugs with high specificity andlow toxicity in selected patients based on a
precision or personalised medicine paradigm. Thetargeted smart drug revolution can be considered tohave started in the late 1990s and early 2000s withthe approval of trastuzumab (Herceptin®) forbreast cancer patients with HER2 amplificationsand shortly thereafter imatinib (Gleevec®) forpatients with BCR-ABL1-driven chronic myeloid
leukaemia (CML). These examples marked thebeginning of rational drug design, which takes intoaccount knowledge of disease pathogenetics andhas lead to the concept of personalised cancer med-icine. In oncology, personalised medicine entailsoptimisation of the entire treatment strategy for anindividual patient with the help of genetic informa-tion as well as molecular and cellular analysis. Thepersonalised tailored treatment is expected to behighly effective and better tolerated in comparison
By Tea Pemovska,Päivi Östling,Caroline Heckman,Olli Kallioniemi andKrister Wennerberg
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine
INDIVIDUALISEDSYSTEMS MEDICINE next-generation precisioncancer medicine and drug positioningA growing number of oncology drugs are currently clinically available and morethan a thousand compounds are being developed for oncology indications.Thus, the challenge is to systematically develop all these drugs to optimalindications across all cancer types and subtypes as well as to tailor treatmentsof individual patients based on the underlying mechanisms of disease and driversignals. We describe here how coupling of genomic and molecular profiling ofcancer with functional testing of drugs in patient-derived cell samples will makeit possible to customise patient treatments as well as to identify biomarkerpatterns and genetic aberrations that explain the drug responses. This approachmay also facilitate rapid clinical translation and optimised development of drugcandidates and investigational drugs through identification of the patientsubgroups that are most likely to respond and systematic evaluation ofefficacious drug combinations.
to conventional chemotherapeutics, thus resultingin an improvement of the quality of life.
The characterisation of the genome andepigenome of many tumour types has been one ofthe focus areas of cancer research in recent years.However, despite the progress in developing newtargeted agents and increased knowledge of cancergenomics, the majority of cancers do not harbourmutations that can readily be linked to currentlyapproved or investigational oncology drugs. Forexample, even though a large percentage of cancersare driven by mutations in the RAS genes (>30%),targeting RAS signalling by small molecules,directly or indirectly, remains an elusive therapeu-tic goal. Translation of a genotype to a phenotype(ie drug response) is not a straightforward exercise.Even when drugs that inhibit the desired targetexist, meaningful responses in patients may be lim-ited due to cell plasticity, tumour heterogeneity andcompensatory signals. For instance, BRAFinhibitors (eg vemurafenib; Zelboraf® anddabrafenib; Tafinlar®) achieve rapid and effectiveresponses in melanoma patients with V600E BRAFmutations, whereas their effects in colorectal can-cer patients harbouring the same mutation are neg-ligible (<5% response rate) due to upregulation ofEGFR signalling in response to BRAF inhibitorexposure. Given that cancers are extremely hetero-
geneous between individual patients and within thetumour itself, optimised, personalised and combi-natorial treatments are often required to achievesignificant responses. Such treatments remain veryhard to predict based solely on our current knowl-edge of the genomic properties of cancer cells.Therefore, there is an urgent need for increasedfunctional understanding of cancer. This can beaccomplished by directly examining cells derivedfrom cancer patients to systematically determineboth the cancer genotype and the drug responsephenotype.
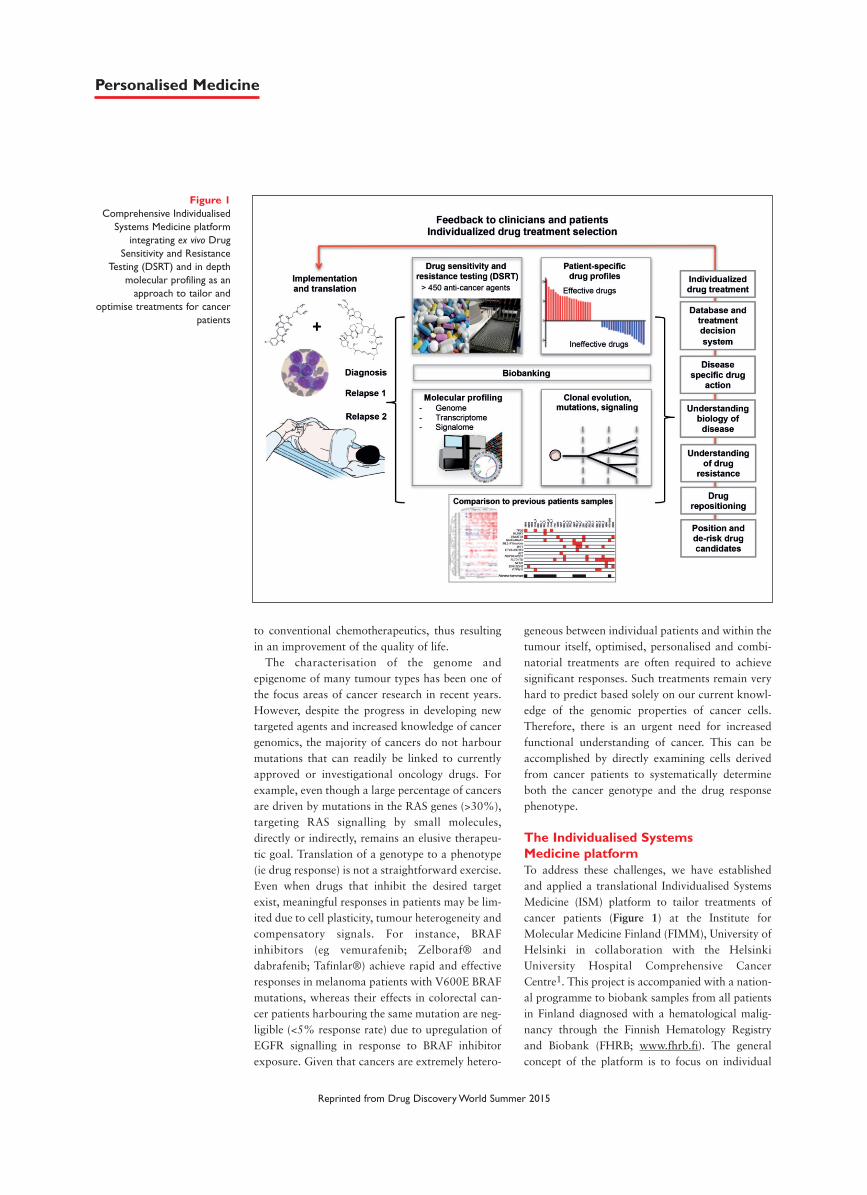
The Individualised Systems Medicine platformTo address these challenges, we have establishedand applied a translational Individualised SystemsMedicine (ISM) platform to tailor treatments ofcancer patients (Figure 1) at the Institute forMolecular Medicine Finland (FIMM), University ofHelsinki in collaboration with the HelsinkiUniversity Hospital Comprehensive CancerCentre1. This project is accompanied with a nation-al programme to biobank samples from all patientsin Finland diagnosed with a hematological malig-nancy through the Finnish Hematology Registryand Biobank (FHRB; www.fhrb.fi). The generalconcept of the platform is to focus on individual
Figure 1Comprehensive Individualised
Systems Medicine platformintegrating ex vivo Drug
Sensitivity and ResistanceTesting (DSRT) and in depth
molecular profiling as anapproach to tailor and
optimise treatments for cancerpatients
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine
patients where personalised therapy options areidentified and linked to disease- and patient-specif-ic molecular markers. This is achieved by integrat-ing functional profiling from ex vivo drug sensitivi-ty testing of patient cancer cells with genomic andmolecular profiling. Exome sequencing is used toidentify somatic mutations and copy number varia-tions, whereas RNA sequencing is used to definegene expression patterns as well as to identify generearrangements and fusion genes. This enables link-age of drug responses to genetic aberrations andbiomarkers. Thus we carry out real-time transla-tional research where scientists work to generateand analyse data to inform clinicians on individu-alised treatment possibilities. The suggested newtherapies can be implemented after an informedconsent and ethical approval in patients withadvanced disease and no alternative treatmentoptions. Consecutive sampling of patients over timeand genomic and molecular profiling of the cancersamples will then make it possible to monitor dis-ease progression, response to therapy, as well as tounderstand mechanisms of drug resistance andclonal evolution during treatment.
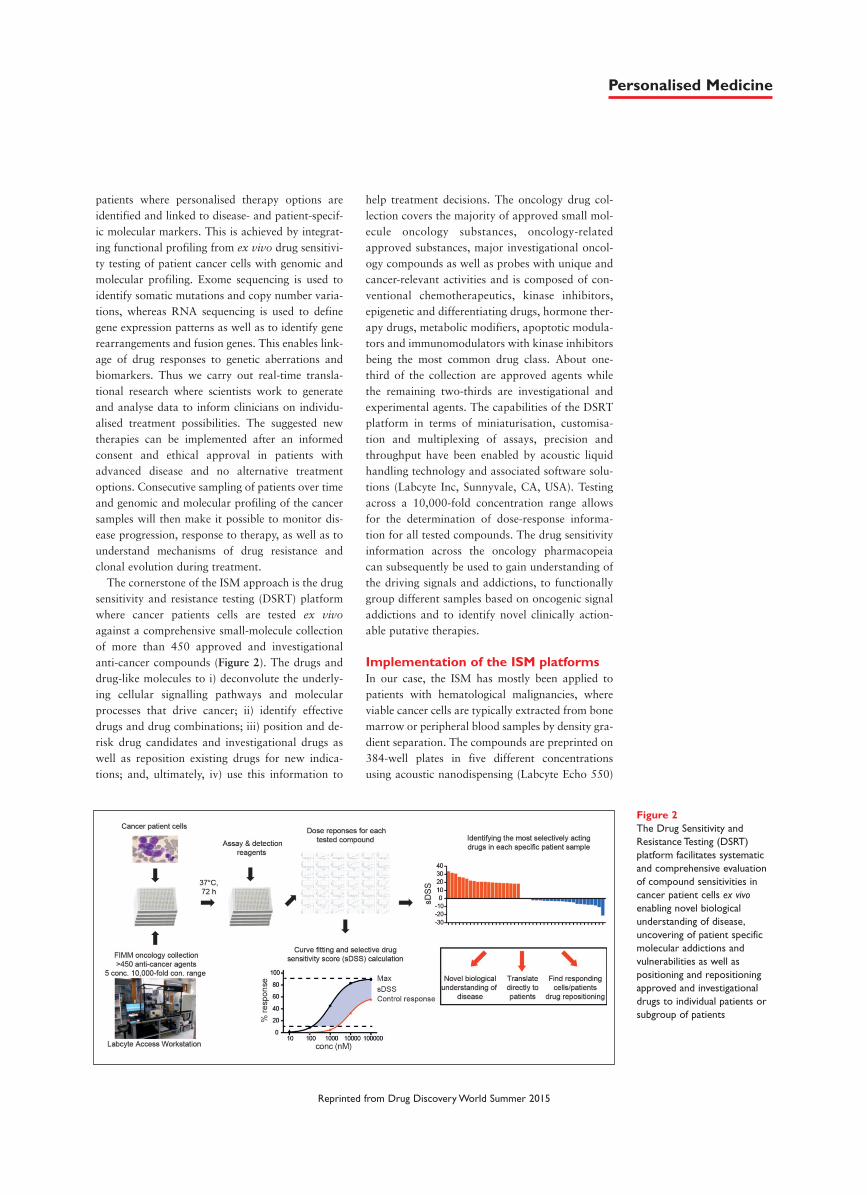
The cornerstone of the ISM approach is the drugsensitivity and resistance testing (DSRT) platformwhere cancer patients cells are tested ex vivoagainst a comprehensive small-molecule collectionof more than 450 approved and investigationalanti-cancer compounds (Figure 2). The drugs anddrug-like molecules to i) deconvolute the underly-ing cellular signalling pathways and molecularprocesses that drive cancer; ii) identify effectivedrugs and drug combinations; iii) position and de-risk drug candidates and investigational drugs aswell as reposition existing drugs for new indica-tions; and, ultimately, iv) use this information to
help treatment decisions. The oncology drug col-lection covers the majority of approved small mol-ecule oncology substances, oncology-relatedapproved substances, major investigational oncol-ogy compounds as well as probes with unique andcancer-relevant activities and is composed of con-ventional chemotherapeutics, kinase inhibitors,epigenetic and differentiating drugs, hormone ther-apy drugs, metabolic modifiers, apoptotic modula-tors and immunomodulators with kinase inhibitorsbeing the most common drug class. About one-third of the collection are approved agents whilethe remaining two-thirds are investigational andexperimental agents. The capabilities of the DSRTplatform in terms of miniaturisation, customisa-tion and multiplexing of assays, precision andthroughput have been enabled by acoustic liquidhandling technology and associated software solu-tions (Labcyte Inc, Sunnyvale, CA, USA). Testingacross a 10,000-fold concentration range allowsfor the determination of dose-response informa-tion for all tested compounds. The drug sensitivityinformation across the oncology pharmacopeiacan subsequently be used to gain understanding ofthe driving signals and addictions, to functionallygroup different samples based on oncogenic signaladdictions and to identify novel clinically action-able putative therapies.
Implementation of the ISM platformsIn our case, the ISM has mostly been applied topatients with hematological malignancies, whereviable cancer cells are typically extracted from bonemarrow or peripheral blood samples by density gra-dient separation. The compounds are preprinted on384-well plates in five different concentrationsusing acoustic nanodispensing (Labcyte Echo 550)
Figure 2The Drug Sensitivity andResistance Testing (DSRT)platform facilitates systematicand comprehensive evaluationof compound sensitivities incancer patient cells ex vivoenabling novel biologicalunderstanding of disease,uncovering of patient specificmolecular addictions andvulnerabilities as well aspositioning and repositioningapproved and investigationaldrugs to individual patients orsubgroup of patients
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine
and the prepared plates are stored under nitrogengas to maintain compound integrity until a newpatient sample will be tested. The patient’s cells arethen added and incubated at 37°C for three daysand cell response is measured with CellTiter-Gloviability and CellTox Green cytotoxicity assays(Promega). As part of the DSRT analysis pipeline,we have developed a novel drug sensitivity quanti-fying metric termed ‘Drug Sensitivity Score’ (DSS)2.The DSS describes the full dose response to a com-pound as a modified ‘area under the curve’ metricso that selective responses are favoured over off-tar-get responses2. The patient-specific drug sensitivityprofiles are compared with responses of cellsderived from healthy bone marrow to identifydrugs that exhibit cancer-selective responses. TheDSRT data provide insights into novel biologicalunderstanding of disease, identify respondingcells/patients to particular drugs and hence facilitatedrug repurposing and can be translated directly topatients. Optimally, results are delivered to clini-cians within four days.
The ISM approach has allowed us to establish
selectively responding patient subpopulations to alarge number of targeted drugs and to identify com-pounds and compound combinations that havebeen utilised by our clinical collaborators on refrac-tory acute myeloid leukaemia (AML) patients incompassionate use/off-label setting with significantsuccess. In about 80% of the patient cases, selectiveresponses with approved drugs are seen such thatISM tailored treatment is possible. Up to this point,translation of ISM data has led to meaningful andevaluable responses, including complete remissionand morphologic leukaemia-free states in morethan 40% of cases, which is a solid response ratefor high-risk relapsed and refractory AML patients.Importantly, in the cases where in vivo resistancesto the selected targeted therapies have emerged,those have also been reflected in the DSRT respons-es in the relapsed samples.
Drug repositioning opportunitiesThe ISM platform comprehensively validates can-didate drugs that would only be hypothesisedfrom genomic profiles. We have also discovered
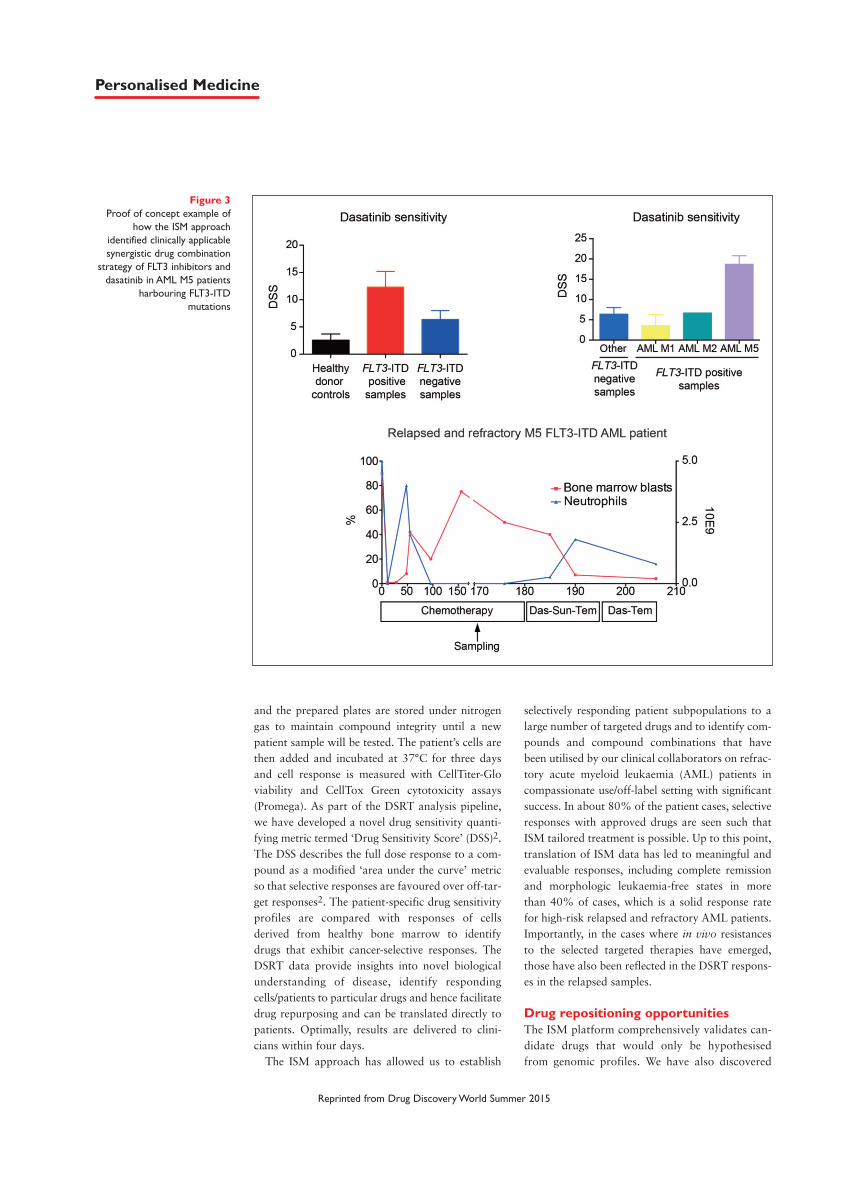
Figure 3Proof of concept example of
how the ISM approachidentified clinically applicablesynergistic drug combination
strategy of FLT3 inhibitors anddasatinib in AML M5 patients
harbouring FLT3-ITDmutations
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine

cancer cell addictions and vulnerabilities thatcould not have been uncovered solely fromgenomic information. Systematic integrated evalu-ation of cancer cell functional and molecular pro-files of consecutive samples from individualpatients enables identification of personalisedtherapy options for patients with refractory andrelapsed disease, aids disease monitoring and fol-low up of the clonal architecture of the cancer.Moreover, by studying the sensitivities to a largenumber of compounds in a large number of cancerpatient samples, the ISM strategy facilitates de-risking, pin-pointing and repositioning drug can-didates, investigational and approved drugs interms of identifying the most strongly respondingpatient subpopulations, optimal drug combina-tions and biomarkers predicting those.
Signal transduction inhibitors display strong can-cer selective effects in subgroups of patient sampleswith small or no effects in control samples. This isin contrast to conventional chemotherapeutics,which tend to exhibit broad effects on both patientand control cells. The sensitivity to conventionalcytotoxic chemotherapy agents ex vivo is also high-ly challenging to interpret and translate to the invivo setting, as their responses often correlate withex vivo proliferation rates or cellular stress levels.Hence, responses to molecularly targeted drugs exvivo are more likely to be predictive of the in vivopatient response. Still the in vivo predictiveness ofdrug responses largely depends on culture condi-tions and the ability to model the tumour microen-vironment and its interaction with the patient’s can-cer cells.
In our study of adult chemorefractory AML1, weidentified to a number of approved kinaseinhibitors such as dasatinib (Sprycel®), sunitinib(Sutent®), ponatinib (Iclusig®), ruxolitinib(Jakavi®), sorafenib (Nexavar®) temsirolimus(Torisel®) and trametinib (Mekinist®), none ofwhich are currently utilised for AML treatment.Thus, these results suggest that already approvedoncology drugs, for example dasatinib (CML andPh+ ALL), sunitinib (renal cell carcinoma and gas-trointestinal tumours), and temsirolimus (renal cellcancer), could be repositioned for subgroups ofAML patients.
Unsupervised clustering of the drug sensitivityprofiles creates functional taxonomy of both thesamples and drugs tested and thus provides infor-mation on how patient samples functionally relateto each other and how the drugs relate to eachother in a disease-specific context. Links betweendrugs whose known target profiles differ often clus-ter unexpectedly together, which may reflect effects
on the same or linked signalling pathways. Thiscould provide opportunities to identify synergisticeffects. For example, we have identified an associa-tion between inhibition of the FLT3 receptor tyro-sine kinase and dasatinib (a tyrosine kinaseinhibitor that does not target FLT3) sensitivity inAML patients with an acute monocytic leukaemia(M5) subtype with activating FLT3-ITD mutations.This implies that AML of the monocytic subtypedriven by FLT3-ITD is also dependent on addition-al tyrosine kinase signals. Hence, combinatorialtreatment of FLT3 inhibitors and dasatinib in thisparticular patient population could have a synergis-tic effect. Indeed, in vivo treatment of a heavilyrefractory AML patient harbouring a FLT3-ITDmutation with dasatinib and sunitinib (a tyrosinekinase inhibitor with potent activity against FLT3)led to a complete remission after failure of threeconsecutive induction chemotherapy regimens(Figure 3). This specific case highlights the power ofthe ISM platform to not only optimise treatmentsfor patients with no treatment options in the clinic,but also to identify unexpected drug-drug interac-tions in a distinct patient subpopulation.
A final powerful example of ISM-driven drugrepositioning is how we recently identified that therenal cancer drug axitinib (Inlyta®) exhibits anti-cancer activity in drug resistant gatekeeper mutantCML patients (Figure 4)3. The DSRT-driven dis-covery of the activity in drug resistant primarypatient cells led to a i) new molecular understand-ing of kinase gatekeeper mutants and drug-targetinteractions; ii) proof of concept validation inpatients; and, most importantly, iii) the opportuni-ty to reposition an approved drug for a patientgroup with an unmet therapeutic need. Morespecifically, we were able to demonstrate that axi-tinib potently and selectively inhibits ABL1(T315I)kinase activity as well as the growth of BCR-ABL1(T315I)-driven cells. Furthermore, structuraldata revealed that while axitinib is an establishedbinder of the inactive conformation of VEGFR2, itbinds to the active conformation of ABL1(T315I)and the inhibitor itself takes on different confor-mations when binding to ABL1(T315I) versusVEGFR2. Additionally, axitinib occupies a uniquebinding space in ABL1 in comparison to otherABL1 inhibitors, which is expected to translate todistinct resistance profile. Overall the structuralinformation highlights the complexity of kinase-inhibitor interactions and illustrates the impor-tance to profile inhibitors against clinically rele-vant samples/assays. Most importantly, when axi-tinib was administered to a patient with a BCR-ABL(T315I)-driven CML, it was able to cause a
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine
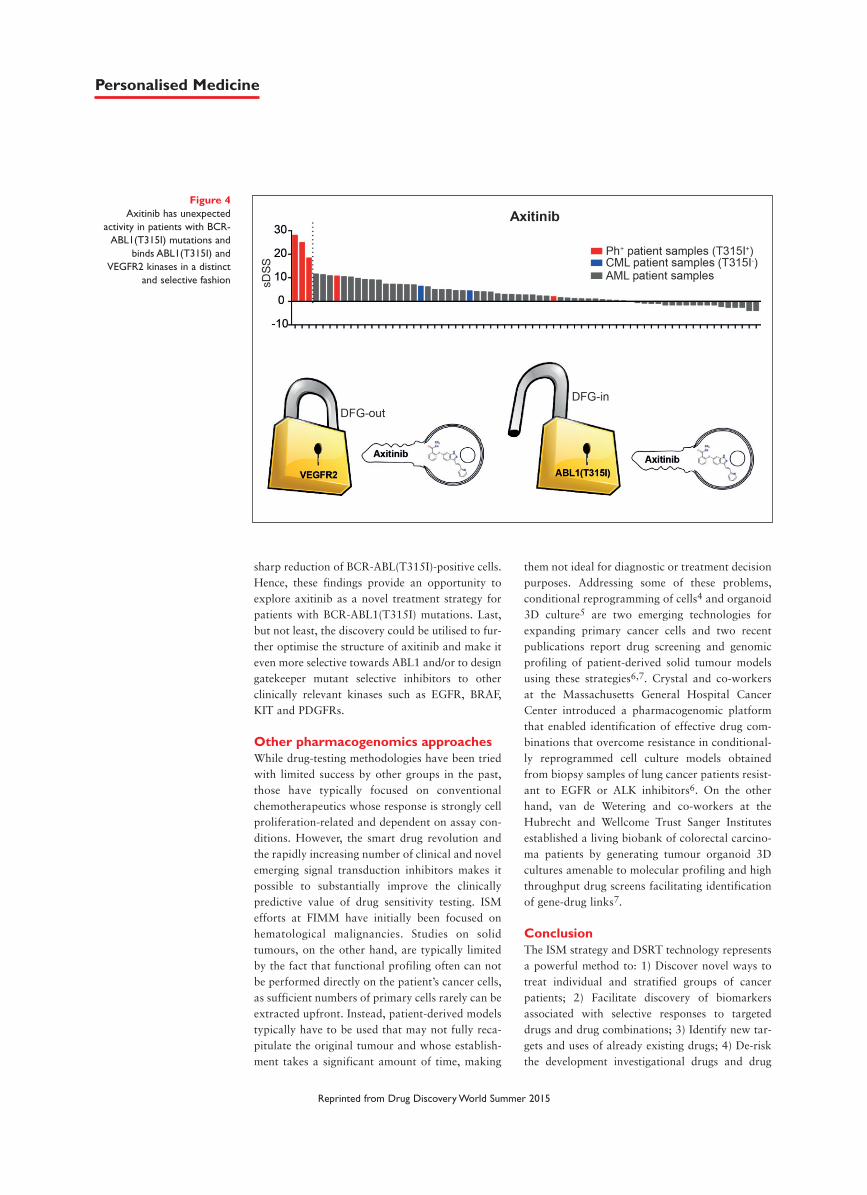
sharp reduction of BCR-ABL(T315I)-positive cells.Hence, these findings provide an opportunity toexplore axitinib as a novel treatment strategy forpatients with BCR-ABL1(T315I) mutations. Last,but not least, the discovery could be utilised to fur-ther optimise the structure of axitinib and make iteven more selective towards ABL1 and/or to designgatekeeper mutant selective inhibitors to otherclinically relevant kinases such as EGFR, BRAF,KIT and PDGFRs.
Other pharmacogenomics approaches While drug-testing methodologies have been triedwith limited success by other groups in the past,those have typically focused on conventionalchemotherapeutics whose response is strongly cellproliferation-related and dependent on assay con-ditions. However, the smart drug revolution andthe rapidly increasing number of clinical and novelemerging signal transduction inhibitors makes itpossible to substantially improve the clinicallypredictive value of drug sensitivity testing. ISMefforts at FIMM have initially been focused onhematological malignancies. Studies on solidtumours, on the other hand, are typically limitedby the fact that functional profiling often can notbe performed directly on the patient’s cancer cells,as sufficient numbers of primary cells rarely can beextracted upfront. Instead, patient-derived modelstypically have to be used that may not fully reca-pitulate the original tumour and whose establish-ment takes a significant amount of time, making
them not ideal for diagnostic or treatment decisionpurposes. Addressing some of these problems,conditional reprogramming of cells4 and organoid3D culture5 are two emerging technologies forexpanding primary cancer cells and two recentpublications report drug screening and genomicprofiling of patient-derived solid tumour modelsusing these strategies6,7. Crystal and co-workersat the Massachusetts General Hospital CancerCenter introduced a pharmacogenomic platformthat enabled identification of effective drug com-binations that overcome resistance in conditional-ly reprogrammed cell culture models obtainedfrom biopsy samples of lung cancer patients resist-ant to EGFR or ALK inhibitors6. On the otherhand, van de Wetering and co-workers at theHubrecht and Wellcome Trust Sanger Institutesestablished a living biobank of colorectal carcino-ma patients by generating tumour organoid 3Dcultures amenable to molecular profiling and highthroughput drug screens facilitating identificationof gene-drug links7.
ConclusionThe ISM strategy and DSRT technology representsa powerful method to: 1) Discover novel ways totreat individual and stratified groups of cancerpatients; 2) Facilitate discovery of biomarkersassociated with selective responses to targeteddrugs and drug combinations; 3) Identify new tar-gets and uses of already existing drugs; 4) De-riskthe development investigational drugs and drug
Figure 4Axitinib has unexpected
activity in patients with BCR-ABL1(T315I) mutations and
binds ABL1(T315I) andVEGFR2 kinases in a distinct
and selective fashion
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine

combinations where the appropriate use can bepinpointed to the patient groups most likely torespond; and 5) Optimise lead compounds andtheir target profiles in cancer-relevant tissue mod-els. Hence, we believe the ISM approach is a pow-erful method for molecular dissection of cancerprogression in individual patients and identifyingputative treatments in real time where new drugscould be more systematically developed to the bestindications and tumour subgroups. DDW
Tea Pemovska is a cancer researcher at theInstitute for Molecular Medicine Finland, FIMM,at the University of Helsinki. She is interested ininvestigating signalling networks driving tumourdevelopment and progression with small moleculesto uncover biology of disease, drug repositioningopportunities and tailored treatment strategies forindividual or subgroups of patients.
Päivi Östling is a senior researcher at FIMM. Hergoal is to bring the drug sensitivity and resistancetesting and in-depth molecular profiling frombench to bedside. Her research aims to develop theex vivo drug testing not only for leukaemiapatients but to enable the platform also for solidtumours.
Caroline Heckman is principal investigator andleader of the Translational Research andPersonalized Cancer Medicine group at FIMMfocused on hematologic malignancies. The groupapplies state-of-the-art research technologies and asystems-wide approach to understand disease pro-gression and drug resistance mechanisms, directlytranslating results to patient care.
Olli Kallioniemi is professor and director ofFIMM, a part of the Nordic EMBL MolecularMedicine Partnership. His research group is focus-ing on translational cancer research and molecularprecision medicine approaches to leukaemia andsolid tumours.
Krister Wennerberg has been a FIMM-EMBLGroup Leader since 2010. His Cancer ChemicalSystems Medicine research group at FIMM focuseson delineating individualised molecular vulnerabil-ities in cancers, how these vulnerabilities relate tothe cancer cell genetics and how this can be turnedinto new effective therapeutic strategies.
References1 Pemovska, T et al.Individualized systemsmedicine strategy to tailortreatments for patients withchemorefractory acutemyeloid leukemia. Cancerdiscovery 3, 1416-1429,(2013).2 Yadav, B et al. Quantitativescoring of differential drugsensitivity for individuallyoptimized anticancertherapies. Scientific reports 4,5193, (2014).3 Pemovska, T et al. Axitinibeffectively inhibits BCR-ABL1(T315I) with a distinctbinding conformation. Nature519, 102-105, (2015).4 Liu, X et al. ROCK inhibitorand feeder cells induce theconditional reprogramming ofepithelial cells. The Americanjournal of pathology 180, 599-607, (2012).5 Sato, T et al. Long-termexpansion of epithelialorganoids from human colon,adenoma, adenocarcinoma, andBarrett’s epithelium.Gastroenterology 141, 1762-1772, (2011).6 Crystal, AS et al. Patient-derived models of acquiredresistance can identify effectivedrug combinations for cancer.Science 346, 1480-1486,(2014).7 van de Wetering, M et al.Prospective derivation of aliving organoid biobank ofcolorectal cancer patients. Cell161, 933-945, (2015).
Reprinted from Drug Discovery World Summer 2015
Personalised Medicine
www.labcyte.com@LabcyteInc