intensive care training program radboud university medical centre
TRANSCRIPT

Intensive Care Training ProgramRadboud University Medical Centre Nijmegen
Prediction and prevention of delirium

• Acute mental disorder: develops over hours/days and fluctuates during
the day
• Disturbed consciousness: decreased ability to concentrate
• Cogni2ve changes (memory disturbances, disorienta9on, language
problems)
DSM-‐IV criteria = gold standard
Delirium

• 30-‐50% of all ICU pa9ents develop symptoms of delirium
• Delirium increases ICU mortality
• Delirium independent predictor for mortality
• Delirium increases hospital length-‐of-‐stay
• Delirium increases ICU costs with 39% and hospital costs with
31% depending on severity
Delirium


Delirium screening with CAM-ICU
0
25
50
75
100
Sensitivity Specificity PPV NPV
%
Total population (N=181) Hypoactive (N=36) Hyperactive (N=7) Mixed type (N=32)
van Eijk MM. Am J Respir Crit Care Med 2011;184:340-344

Delirium (n=411)
Non-‐delirium (n=1202)
p-‐value (corrected for
APACHE-‐II score)
Associa2on of delirium with outcome*
Dura9on of MV (days) 4,6 [1-‐11] 0,3 [0-‐1] <0,0001 O.R. 7,0(95%CI 4,7-‐10,5)
Reintuba9on 10% 0,5% <0,0001
Accidental removal of ET and catheters 23,1% 0,6% <0,0001
LOS-‐ICU (days) 6 [2-‐13] 1 [1-‐2] <0,0001 O.R. 8,6 (95%CI 5,8-‐12,7)
LOS-‐hospital (days) 20 [10-‐39] 7 [5-‐14] <0,0001 O.R. 2,1(95%CI 1,5-‐3,0)
Hospital mortality (%) 73 (17,8%) 40 (3,3%) <0,0001 O.R. 2,1(95%CI 1,2-‐3,5)
van den Boogaard et al., 2011 IJNS
Short term consequences
* mul9variate logis9c regression analysis with covariates: delirium, admission category, history of pulmonary disease, reintuba9on and sepsis.

van den Boogaard. Crit Care Med 2012;40:12-118
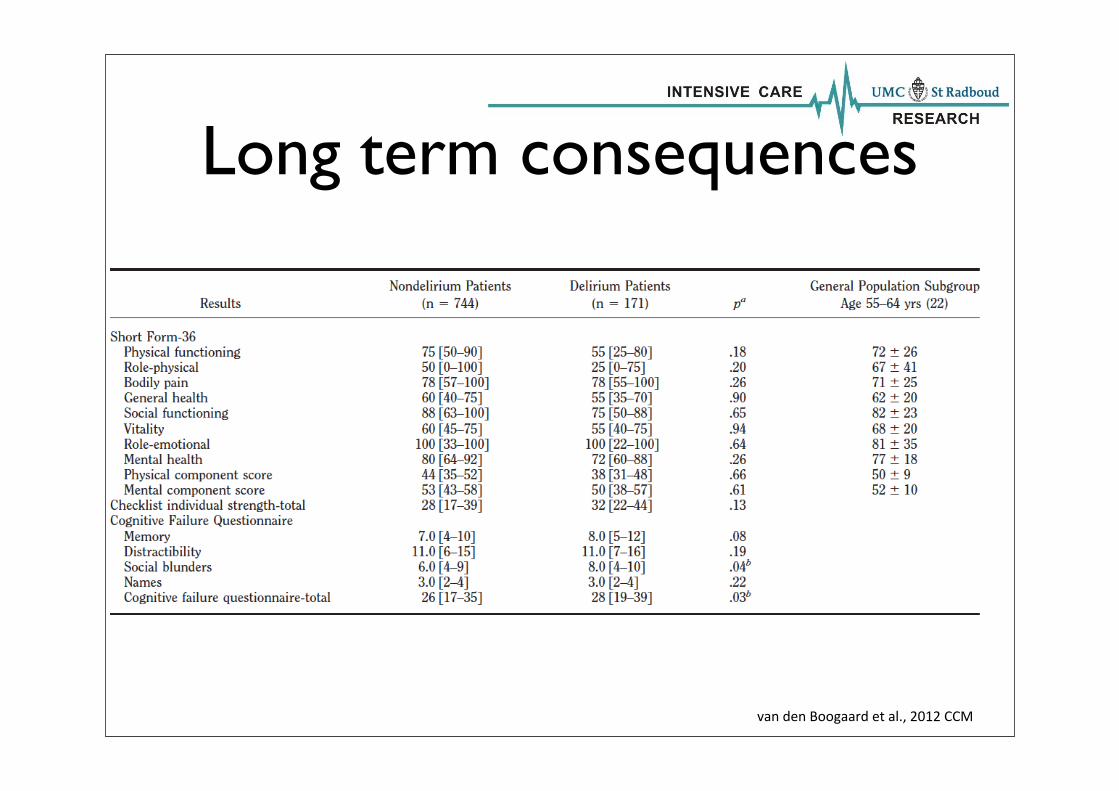
van den Boogaard et al., 2012 CCM
Long term consequences

N = 225Age > 60
Cardiac surgery
MM
SE
Saczynski JS. N Engl J Med 2012;367:30-39
Prevention
• Inefficient in all patients
• less effective
• labour intensive
• side-effects
Prediction model necessary to identify high risk patients

• Developed and validated in a total of 3056 pa9ents in 5 centra in
NL (UMCN, UMCU, MCL, OLVG and Gelre zkh)
• PRE-‐DELIRIC consists of 10 predictors: age, APACHE-‐II, coma,
admission category, infec2on, metabolic acidosis, use of morphine,
seda2ves , plasma urea and emergency admission
• Predic9on of delirium in 24 hours
• High predic9ve value (AUC 0,85)
• Predic9ve value medical personnel is low (AUC 0,56)van den Boogaard et al., 2012 BMJ
Iden9fy high risk pa9ents with PRE-‐DELIRIC
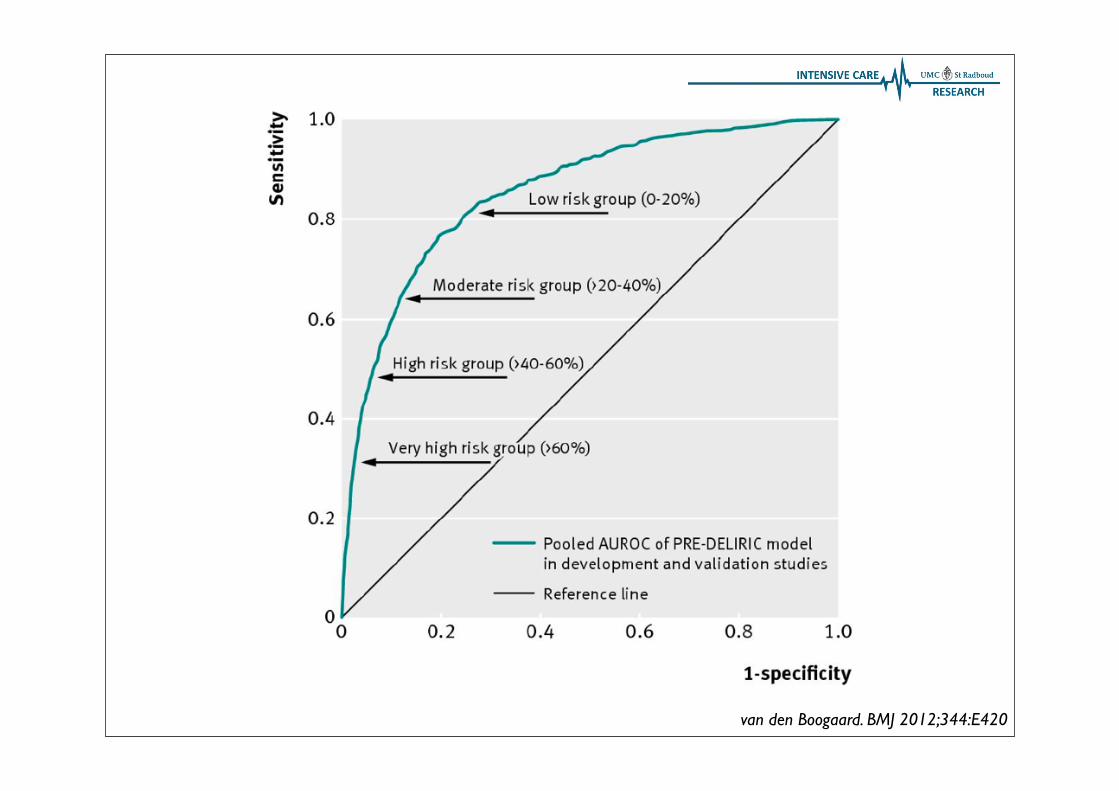
van den Boogaard. BMJ 2012;344:E420
• No differences in studies using Donezepil, Gabapen9n, Ci9coline
• Haloperidol preven9on in hip surgery: decreases dura9on, delirium less severe, shorter admission dura9on
• Haloperidol preven9on in surgical and medical ICU-‐pa9ents: ↓incidence 23-‐15% and ↑delirium free days 5,7-‐ 6,2 days (no risk-‐stra9fica9on)
• Most experience with haloperidol
• First choice in most guidelines -‐ dose dependent side effects
Choice of agent

Haloperidol prevention
Wei Wang. Crit Care Med 2012;40:731-739
Critically ill elderly after non-cardiac surgery0.5 mg bolus + 0.1 mg/hr for 12 hours

Wei Wang. Crit Care Med 2012;40:731-739

Wei Wang. Crit Care Med 2012;40:731-739

• PRE-‐DELIRIC ≥ 50% or history of demen9a or alcohol abuse
• Haloperidol 3x1 mg
• Preven9on stops with ICU discharge or occurrence delirium
• No preven9on if:
• Already delirium
• Haloperidol contraindicated
Delirium preven9on program

• Controle 2008-‐2009
• Interven9on 2010-‐2011
• End-‐points
• Delirium incidence
• Delirium free days without coma in 28 days
• 28-‐day mortality
• Accidental removal ET/catheters
• Dura9on of MV
• Reintuba9on
• ICU readmission
• LOS-‐ICU and hospital
Primary measure
Secondary measure
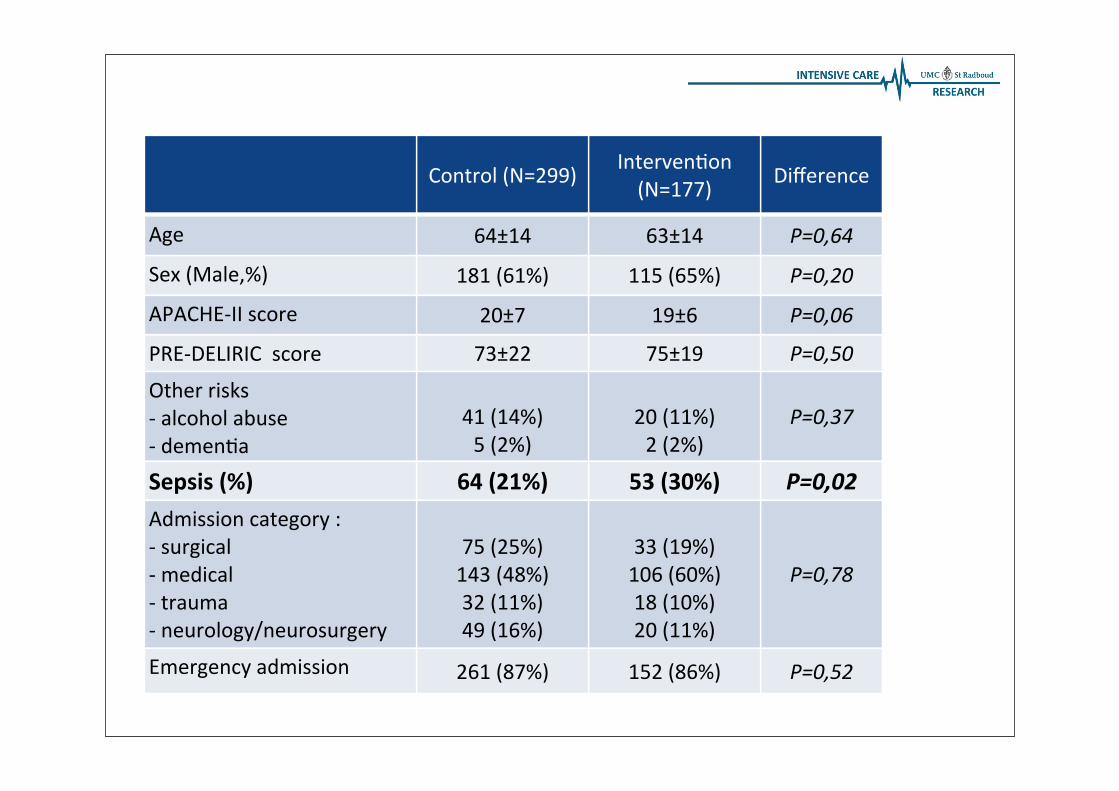
Control (N=299) Interven9on (N=177) Difference
Age 64±14 63±14 P=0,64
Sex (Male,%) 181 (61%) 115 (65%) P=0,20
APACHE-‐II score 20±7 19±6 P=0,06
PRE-‐DELIRIC score 73±22 75±19 P=0,50
Other risks-‐ alcohol abuse-‐ demen9a
41 (14%)5 (2%)
20 (11%)2 (2%)
P=0,37
Sepsis (%) 64 (21%) 53 (30%) P=0,02Admission category :-‐ surgical-‐ medical-‐ trauma -‐ neurology/neurosurgery
75 (25%)143 (48%)32 (11%)49 (16%)
33 (19%)106 (60%)18 (10%)20 (11%)
P=0,78
Emergency admission 261 (87%) 152 (86%) P=0,52

Control (N=299) Interven9on (N=177) Difference
PRE-‐DELIRIC score 73±22 75±19 P=0,50
Delirium incidence (N,%) 225 (75%) 115 (65%) P=0,01
Delirium-‐free-‐days without coma in 28 days (median, IQR)
13 [3-‐27] 20 [8-‐27] P=0.003
Dura9on mechanical ven9la9on in hrs [median, IQR]
118 [39-‐250] 90 [36-‐229] P=0.24
Re-‐intuba9ons (N,%) 25 (8%) 15 (9%) P=0.51
Unplanned removal of tubes(N,%)
-‐endotracheal tube-‐ Gastric tube-‐ CVC/arterial-‐katheter
58 (19%)
8 (3%)26 (9%)24 (8%)
21 (12%)
4 (2%)14 (8%)1 (<1%)
P=0.02
ICU re-‐admissions (N,%) 55 (18%) 20 (11%) P=0.03

Controle (N=299) Interven9on (N=177) Difference
LOS-‐IC [median, IQR] 7 [3-‐13] 6 [3-‐12] P=0,65
LOS-‐ziekenhuis [median, IQR] 21 [11-‐41] 20 [11-‐31] P=0,16
28-‐day mortality 38 (12.5%) 6 (6.3%) P=0.03
Number Needed to Treat: 16

Survival duration
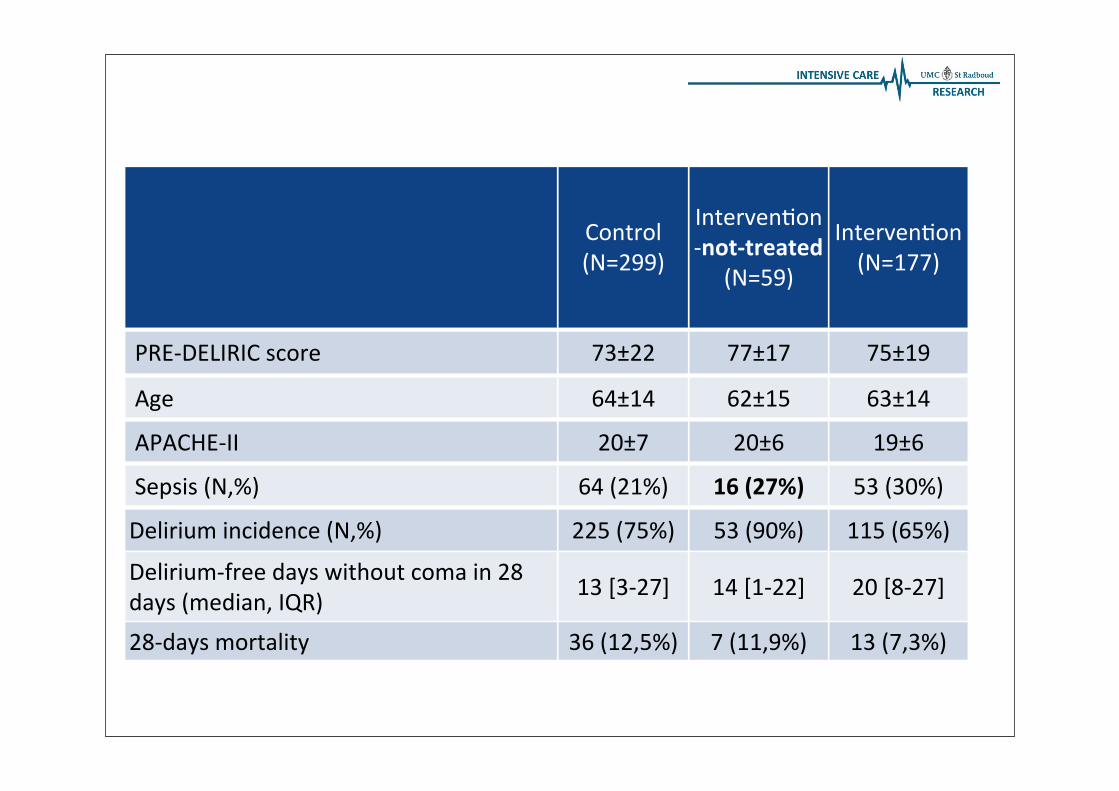
Control (N=299)
Interven9on -‐not-‐treated
(N=59)
Interven9on (N=177)
PRE-‐DELIRIC score 73±22 77±17 75±19
Age 64±14 62±15 63±14
APACHE-‐II 20±7 20±6 19±6
Sepsis (N,%) 64 (21%) 16 (27%) 53 (30%)
Delirium incidence (N,%) 225 (75%) 53 (90%) 115 (65%)
Delirium-‐free days without coma in 28 days (median, IQR) 13 [3-‐27] 14 [1-‐22] 20 [8-‐27]
28-‐days mortality 36 (12,5%) 7 (11,9%) 13 (7,3%)

Interven9on(N=177)
Haloperidol dose changed:-‐ Drowsiness-‐ Rigidity-‐ Suspicion NMS-‐ Parkinsonism
13 (3%)2 (2%)
1 (0,2%) 1 (0,2%)
Haloperidol stopped: -‐ Increase QTc-‐ Seda9ve effect-‐ Renal failure
11 (2%) 3 (0,6%) 1 (0,2%)