international symposium summary
TRANSCRIPT
March 2018
International Symposium Summary Turning value theory into practice – an international perspective October 2017, London

Healthcare Costing for Value Institute
2
Contents
Foreword
3
Section 1 - Building value around the patient pathway
4-6
Section 2- Harnessing the power of patient-level costing to support improvements in patient care
7-9
Section 3 - Benchmarking value between six hospitals – a practical approach
10-12
Section 4 - Linking costs and outcomes at the patient level in three acute hospitals – the Value challenge pilot
13
Section 5- Measuring value across health and social care systems
14-16
Section 6 - Delivering value at the population level
17-19

Healthcare Costing for Value Institute
3
Foreword
Our first International symposium held in October 2016 was a great success with seven different countries providing a top-level view of their approach to costing and value-based healthcare. In 2017 we continued with the theme of delivering value-based healthcare but explored more of the operational level in international systems, looking practically at ‘Turning value theory into practice – an international perspective.’ Delegates heard from six different countries on how they are practically embedding value-based healthcare at both the individual and population level. Our second symposium demonstrated that value-based healthcare is already a practical solution to current healthcare challenges. Many systems are pursuing similar goals - healthcare services that are built around patients and delivering outcomes that matter to patients. But there's no single approach that can be parachuted into existing, differently structured health systems.
However, there is a growing consensus that making value the aim of all decision making (rather than looking at quality and cost improvements in isolation) is the right thing to do. In fact it is probably the only solution to the growing demand facing all health systems.
And while there may not be a ‘one size fits all’ solution, there is huge benefit from being in a room of like-minded people excited about the potential of refocusing healthcare management on the delivery of value and sharing ideas. There were certainly plenty of examples of where value-based approaches have already delivered tangible results.
This document provides a summary of some of the key points from each session together with links to the videos and slides. We encourage you to watch the videos and share them with interested colleagues within your organisation. Value-based healthcare means taking account of a range of outcomes and cost. It is a concept that few would argue with – but turning it into practice is far harder. There are major issues still to crack – ensuring value is viewed across populations not simply within a part of the patient pathway for example. Nobody has all the right answers and there are huge opportunities for practitioners and organisations to learn from each other within and across health systems. The HFMA’s international symposium provides the perfect platform to showcase developments across the world.
Catherine Mitchell Head of Healthcare Costing for Value Institute, hfma
Healthcare Costing for Value Institute
4
Section 1 Building value around the patient pathway
Key points
The hospital recognises it faces a number of challenges:
• Healthcare spend as a percentage of GDP is increasing at a significant rate in Sweden.
• Their services are fragmented and do not provide a holistic overview.
• There are big differences in treatment methods and care outcomes.
• They continue to face budget pressures.
We were delighted to welcome the Swedish Karolinska University Hospital who are at the forefront of value-based healthcare thinking and have been implementing value-based healthcare since 2011. The hospital, responsible for highly specialised health care in Stockholm County Council, is introducing a value-based operating model which is based on the patient’s health care journey and focuses on the outcomes that matter to patients. This presentation is a must-see for anyone interested in how patient-level costing data can be used as a tool to forecast the change in resources required as a result of service redesign. It is also an excellent practical example of how you can start to turn the theory of value into practice.
Claes Ruth (MSE) Head of central controlling Karolinska University Hospital, Sweden
Dr Michael Melin (M.D.) Manager of the Patient Flow for Heart Failure Karolinska University Hospital, Sweden
Healthcare Costing for Value Institute
5
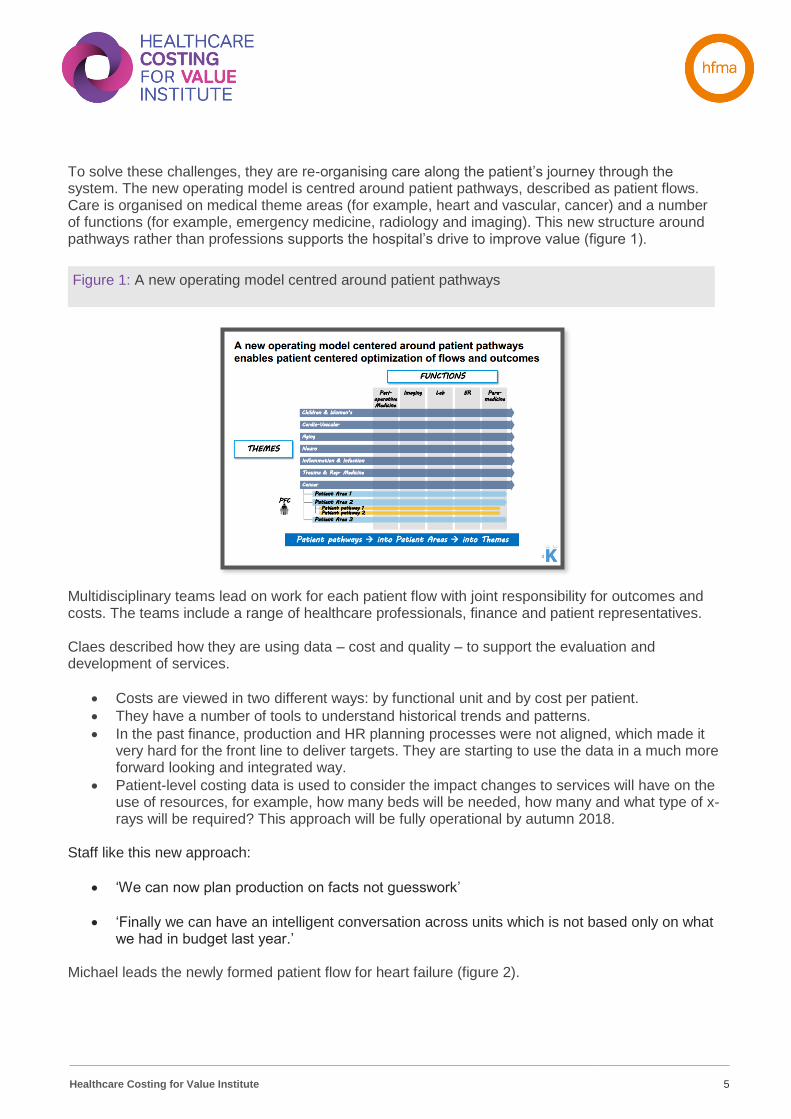
To solve these challenges, they are re-organising care along the patient’s journey through the system. The new operating model is centred around patient pathways, described as patient flows. Care is organised on medical theme areas (for example, heart and vascular, cancer) and a number of functions (for example, emergency medicine, radiology and imaging). This new structure around pathways rather than professions supports the hospital’s drive to improve value (figure 1).
Multidisciplinary teams lead on work for each patient flow with joint responsibility for outcomes and costs. The teams include a range of healthcare professionals, finance and patient representatives. Claes described how they are using data – cost and quality – to support the evaluation and development of services.
• Costs are viewed in two different ways: by functional unit and by cost per patient.
• They have a number of tools to understand historical trends and patterns.
• In the past finance, production and HR planning processes were not aligned, which made it very hard for the front line to deliver targets. They are starting to use the data in a much more forward looking and integrated way.
• Patient-level costing data is used to consider the impact changes to services will have on the use of resources, for example, how many beds will be needed, how many and what type of x-rays will be required? This approach will be fully operational by autumn 2018.
Staff like this new approach:
• ‘We can now plan production on facts not guesswork’
• ‘Finally we can have an intelligent conversation across units which is not based only on what we had in budget last year.’
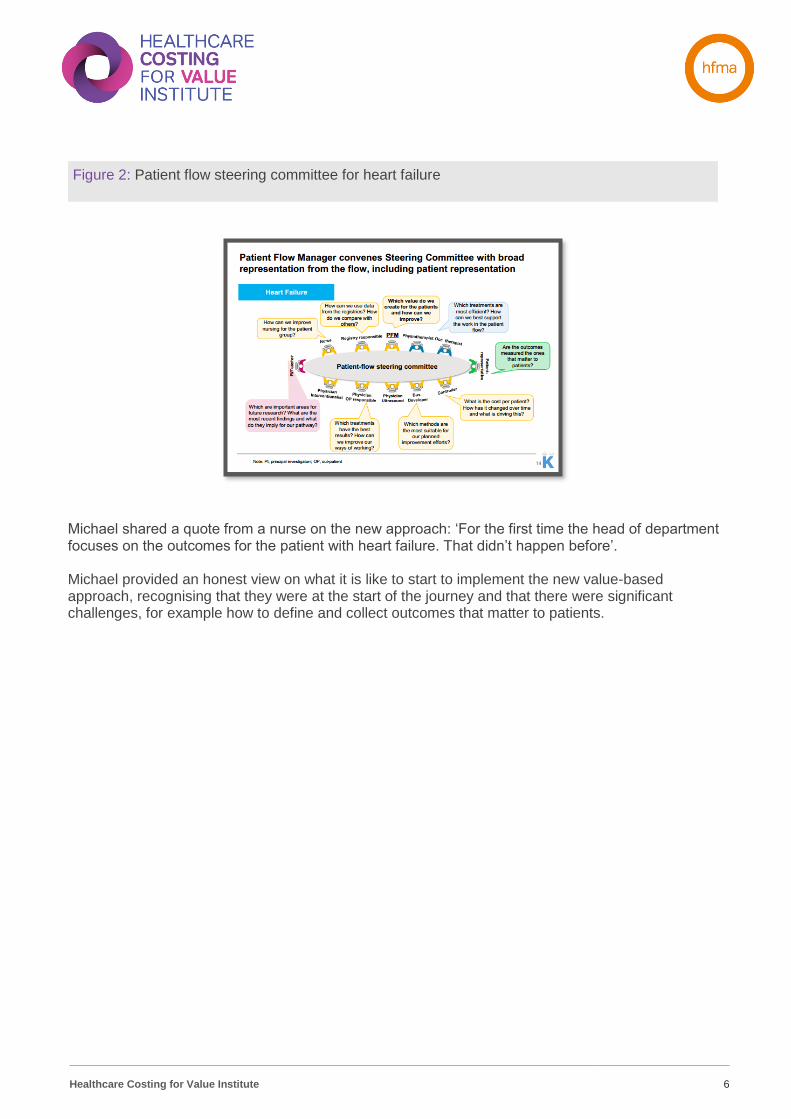
Michael leads the newly formed patient flow for heart failure (figure 2).
Figure 1: A new operating model centred around patient pathways
Healthcare Costing for Value Institute
6
Michael shared a quote from a nurse on the new approach: ‘For the first time the head of department focuses on the outcomes for the patient with heart failure. That didn’t happen before’. Michael provided an honest view on what it is like to start to implement the new value-based approach, recognising that they were at the start of the journey and that there were significant challenges, for example how to define and collect outcomes that matter to patients.
Figure 2: Patient flow steering committee for heart failure
Healthcare Costing for Value Institute
7
Section 2 Harnessing the power of patient-level costing to support improvements in patient care
With the roll-out of patient-level costing across the NHS as part of NHS Improvement’s costing transformation programme, providers of NHS services have increasingly detailed information about the cost of caring for individual patients. However, the data is not consistently being used to support improvements in the efficiency and effectiveness of how patient care is delivered. We were very pleased to welcome Alfa back to provide us with insight into how Australia is harnessing the power of patient-level costing to support improvements in patient care. This presentation will be of particular interest to those trusts
starting to explore NHS Improvement’s national PLICS portal.
Alfa D’Amato Director of Activity Based Management New South Wales Health, Australia
Julia Heberle Deputy director of Activity Based Management (patient costing improvements) New South Wales Health, Australia
Susan Dunn Deputy director of Activity Based Management (stakeholders and clinical engagement) New South Wales Health, Australia
Healthcare Costing for Value Institute
8
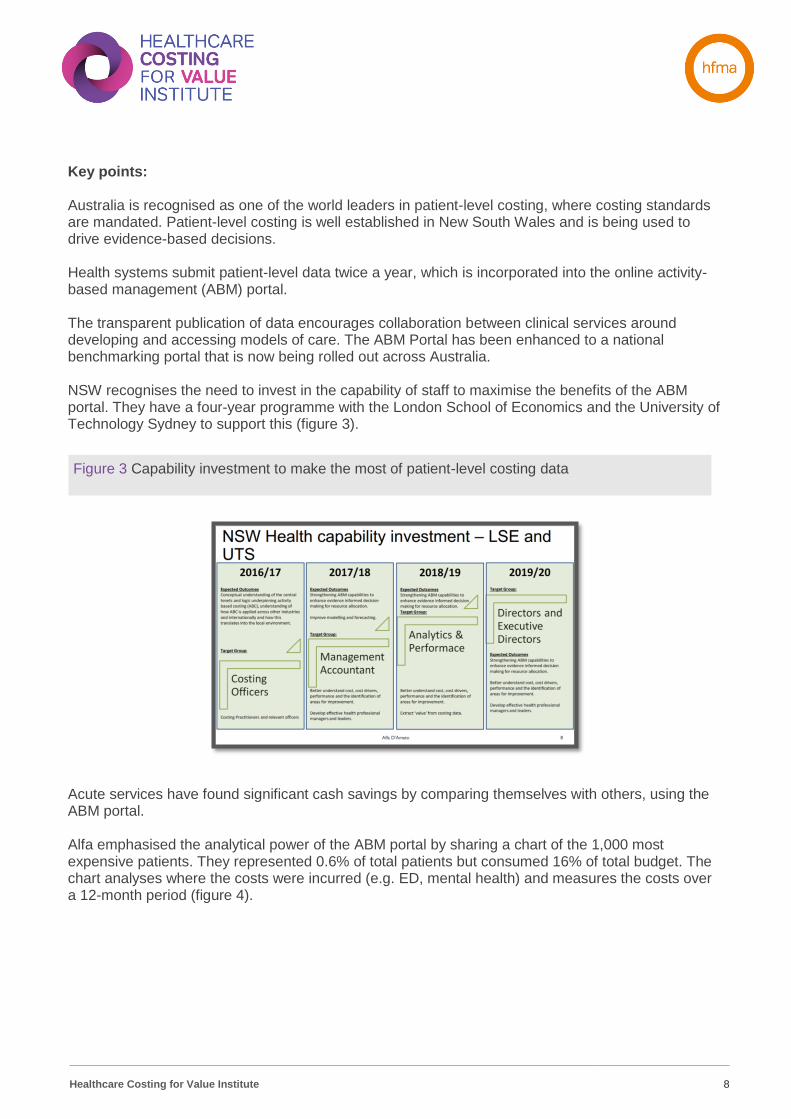
Key points: Australia is recognised as one of the world leaders in patient-level costing, where costing standards are mandated. Patient-level costing is well established in New South Wales and is being used to drive evidence-based decisions. Health systems submit patient-level data twice a year, which is incorporated into the online activity-based management (ABM) portal. The transparent publication of data encourages collaboration between clinical services around developing and accessing models of care. The ABM Portal has been enhanced to a national benchmarking portal that is now being rolled out across Australia. NSW recognises the need to invest in the capability of staff to maximise the benefits of the ABM portal. They have a four-year programme with the London School of Economics and the University of Technology Sydney to support this (figure 3).
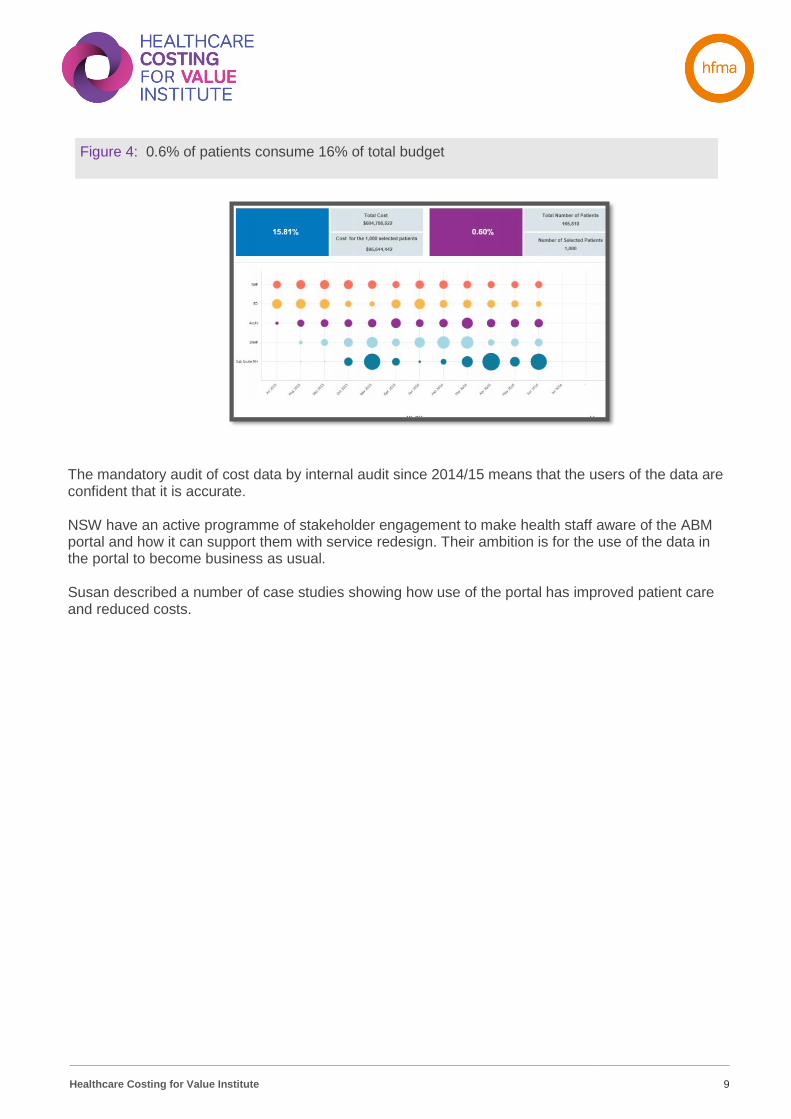
Acute services have found significant cash savings by comparing themselves with others, using the ABM portal. Alfa emphasised the analytical power of the ABM portal by sharing a chart of the 1,000 most expensive patients. They represented 0.6% of total patients but consumed 16% of total budget. The chart analyses where the costs were incurred (e.g. ED, mental health) and measures the costs over a 12-month period (figure 4).
Figure 3 Capability investment to make the most of patient-level costing data
Healthcare Costing for Value Institute
9
The mandatory audit of cost data by internal audit since 2014/15 means that the users of the data are confident that it is accurate. NSW have an active programme of stakeholder engagement to make health staff aware of the ABM portal and how it can support them with service redesign. Their ambition is for the use of the data in the portal to become business as usual. Susan described a number of case studies showing how use of the portal has improved patient care and reduced costs.
Figure 4: 0.6% of patients consume 16% of total budget
Healthcare Costing for Value Institute
10
Section 3 Benchmarking value between six hospitals – a practical approach
Key points
In 2007, six independently-run hospitals in The Netherlands decided to form an alliance that would enable close collaboration around patient care and quality improvement initiatives. The alliance was formalised in 2010 with agreements signed to collaborate under the umbrella organisation Santeon. There are now seven hospitals in the alliance. Santeon’s value-based healthcare initiative is aimed at improving health outcomes for patients in the main disease areas, and at the same time reducing costs. A key focus of the initiative is to make the comparison of results and the improvement of clinical practice part of the daily routine of the hospitals. The value-based healthcare initiative started in 2012 with the measurement, benchmarking and publication of outcomes for four oncological conditions. Using the Michael Porter outcome framework, with a focus on outcomes that matter to patients, they used data that was already being collected. Comparison of outcomes led to some improvements in the way that care delivered to patients. https://www.santeon.nl/Santeon_CareForOutcome2014.pdf
The Institute’s Value challenge pilot started to explore the challenges of translating the theory of value into practice. We were very pleased to welcome the Santeon group of hospitals, who have explored similar challenges but in a more systematic way and have started to embed value-based healthcare within their organisations. This presentation is an excellent practical example of a group of hospitals turning value theory into practice.
Dr Samyra Keus Project leader value-based healthcare, OLVG Amsterdam (part of the Santeon group of hospitals), The Netherlands
Healthcare Costing for Value Institute
11
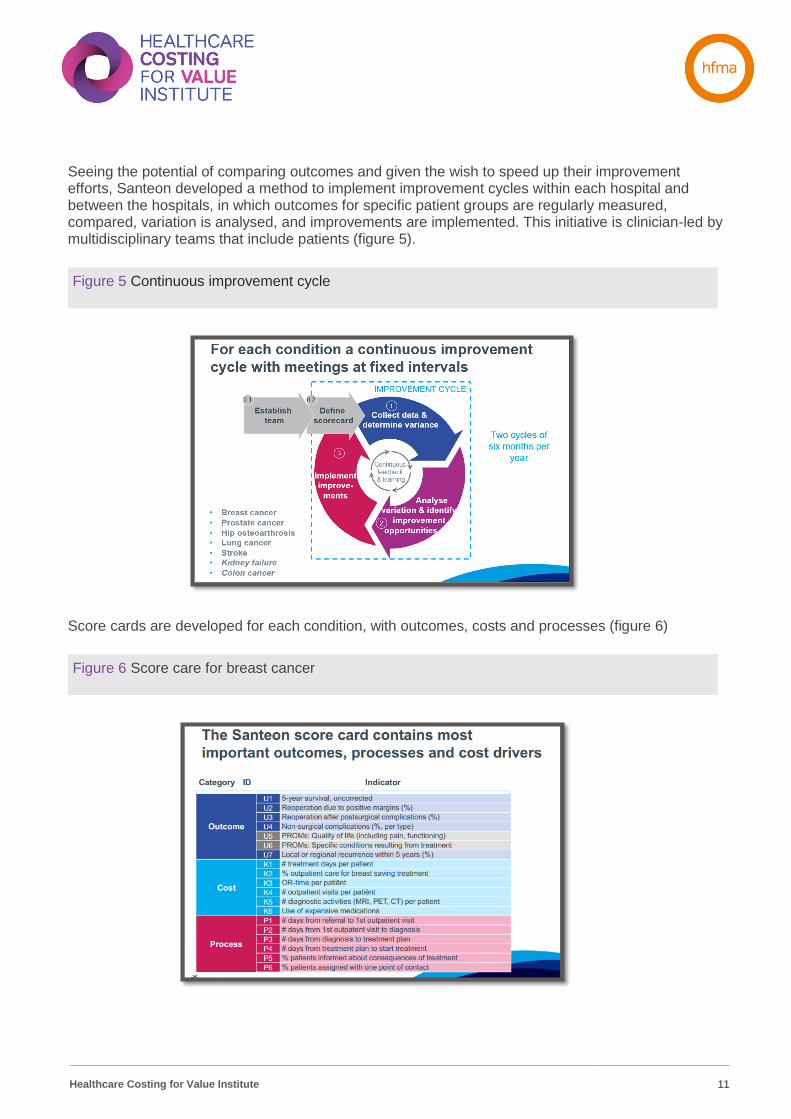
Seeing the potential of comparing outcomes and given the wish to speed up their improvement efforts, Santeon developed a method to implement improvement cycles within each hospital and between the hospitals, in which outcomes for specific patient groups are regularly measured, compared, variation is analysed, and improvements are implemented. This initiative is clinician-led by multidisciplinary teams that include patients (figure 5).
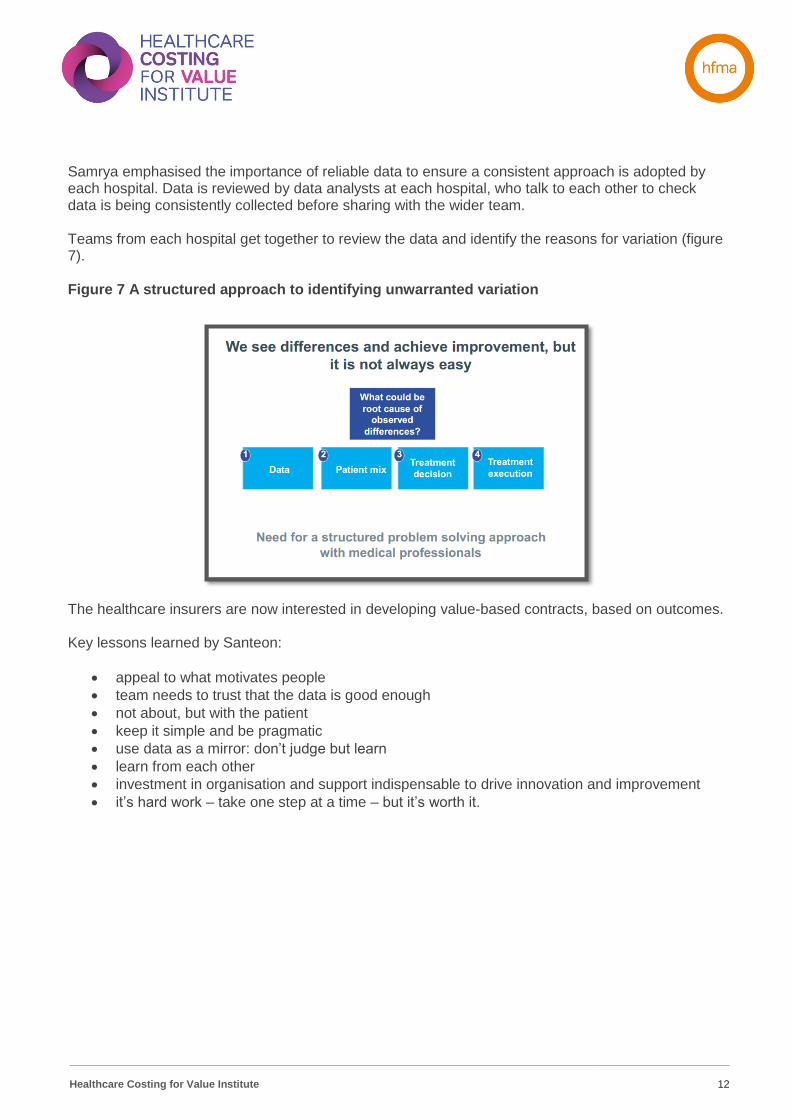
Score cards are developed for each condition, with outcomes, costs and processes (figure 6)
Figure 5 Continuous improvement cycle
Figure 6 Score care for breast cancer
Healthcare Costing for Value Institute
12
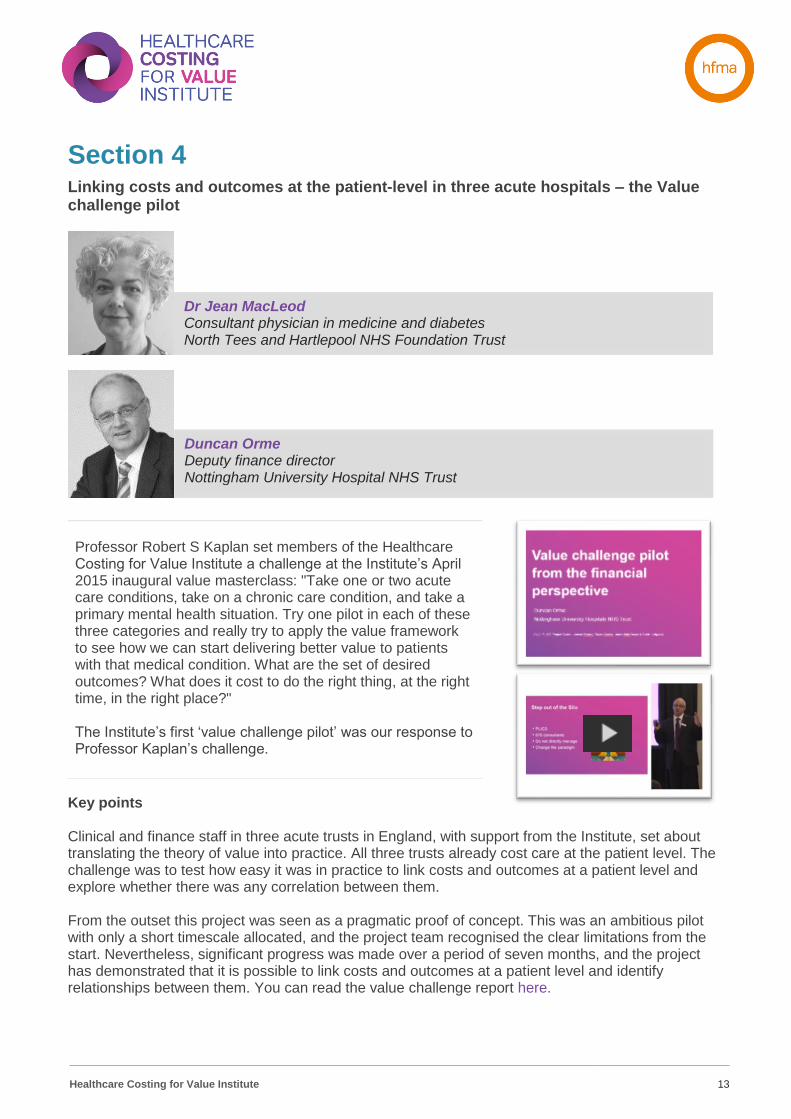
Samrya emphasised the importance of reliable data to ensure a consistent approach is adopted by each hospital. Data is reviewed by data analysts at each hospital, who talk to each other to check data is being consistently collected before sharing with the wider team. Teams from each hospital get together to review the data and identify the reasons for variation (figure 7). Figure 7 A structured approach to identifying unwarranted variation The healthcare insurers are now interested in developing value-based contracts, based on outcomes. Key lessons learned by Santeon:
• appeal to what motivates people
• team needs to trust that the data is good enough
• not about, but with the patient
• keep it simple and be pragmatic
• use data as a mirror: don’t judge but learn
• learn from each other
• investment in organisation and support indispensable to drive innovation and improvement
• it’s hard work – take one step at a time – but it’s worth it.
Healthcare Costing for Value Institute
13
Section 4 Linking costs and outcomes at the patient-level in three acute hospitals – the Value challenge pilot
Key points Clinical and finance staff in three acute trusts in England, with support from the Institute, set about translating the theory of value into practice. All three trusts already cost care at the patient level. The challenge was to test how easy it was in practice to link costs and outcomes at a patient level and explore whether there was any correlation between them. From the outset this project was seen as a pragmatic proof of concept. This was an ambitious pilot with only a short timescale allocated, and the project team recognised the clear limitations from the start. Nevertheless, significant progress was made over a period of seven months, and the project has demonstrated that it is possible to link costs and outcomes at a patient level and identify relationships between them. You can read the value challenge report here.
Professor Robert S Kaplan set members of the Healthcare Costing for Value Institute a challenge at the Institute’s April 2015 inaugural value masterclass: "Take one or two acute care conditions, take on a chronic care condition, and take a primary mental health situation. Try one pilot in each of these three categories and really try to apply the value framework to see how we can start delivering better value to patients with that medical condition. What are the set of desired outcomes? What does it cost to do the right thing, at the right time, in the right place?" The Institute’s first ‘value challenge pilot’ was our response to Professor Kaplan’s challenge.
Dr Jean MacLeod Consultant physician in medicine and diabetes North Tees and Hartlepool NHS Foundation Trust
Duncan Orme Deputy finance director Nottingham University Hospital NHS Trust
Healthcare Costing for Value Institute
14
Section 5 Measuring value across health and social care systems
Key points 2015 reforms in Quebec created integrated health and social care networks. The network CIUSSS, West Central Montreal is responsible for the health and wellbeing of the network population. This includes the health and social services for the continuum of the episode i.e.:
• acute hospital
• rehabilitation centres
• nursing homes
• ambulatory centres
• intellectual and physical deficiency centres The network also works with about 50 GP practices, who are not part of the network. The network has built an integrated IT platform which measure the whole care cycle across all network services. The network is experiencing financial challenges. Quebec has the lowest spend per capita on health in Canada, and in the past three years the network has experienced significant budget cuts. It is expected that the integration reforms will produce cost reductions and improve the use of resources, but this will be in the medium term. In this context improving value is very important. (figure 8).
We are becoming increasingly aware in the UK that to drive value we need to be able to measure costs and outcomes across whole patient pathways, which are likely to cover more than one organisation. The challenge is how to do this. We were delighted that Anne could attend our symposium to talk about how her integrated network of health and social care is starting to create a value-based healthcare system across the network. This presentation will be of particular interest to those health economies starting to look at integrated care systems.
Dr Anne Lemay Associate executive director for support, administration and performance CIUSSS, West Central Montreal, Quebec, Canada
Healthcare Costing for Value Institute
15
The network is adopting the Michael Porter approach to creating a value-based healthcare system with the establishment of multi-disciplinary teams around patient groups. The first integrated practice units (IPUs) include coronary care, neurology and mental health. Alongside the establishment of IPUs, the network is focusing on the collection of outcomes. They are looking at the ICHOM standard sets as well as outcomes collected already locally. The challenge is collecting outcomes that matter to patients. They have pockets of good practice e.g. one psychiatrist collects data from patient iPhones, and cardiology has a pilot project where patient-reported outcomes are collected on iPads. The network is currently considering how to adopt a more comprehensive approach to outcome collection. The acute hospital has had patient-level costs for a number of years. The network now plans to expand this approach across all services (figure 9).
Figure 8: The importance of measuring and improving value
Healthcare Costing for Value Institute
16
Anne believes that there are three existing elements in the network which will support the delivery of value:
• leadership - their CEO is committed to a value approach
• tradition of quality improvement
• well-established patient experience office to advise on outcome improvement
Figure 9: Measuring costs across a healthcare system
Healthcare Costing for Value Institute
17
Section 6 Value-based population health – a preventative proactive approach
Key points Gesundes Kinzigtal (meaning ‘healthy Kinzigtal’) is a joint venture between a network of clinicians in Kinzigtal and OptiMedis AG. Gesundes Kinzigtal is responsible for organising care and improving the health of nearly half of the population of Kinzigtal in southwest Germany. Since 2006, Gesundes Kinzigtal has held contracts to integrate health and care services for their insured populations, covering all age groups and care settings. Around a third of this population has actively enrolled in Gesundes Kinzigtal which is free to all those insured, and which allows access to a number of health improvement programmes. Gesundes Kinzigtal clinicians’ vision was to develop a population-based regional and independent concept of healthcare without sector boundaries (figure 10).
There is much discussion within UK healthcare about population health and many of the current initiatives are being developed with population health in mind. However, there are no simple solutions to this complex problem which will involve a wide range of different services and sectors working collaboratively with the best healthcare interests of the population in mind. We were very pleased to welcome representatives from the Gesundes Kinzigtal initiative to the symposium to share details of the work that has been carried out in Germany to operate a regional integrated care system which is responsible for all healthcare outcomes for a specific region. This presentation will be of particular interest to those health economies starting to look at integrated care systems.
Dr Martin Wetzel GP and head of Kinzigtal GP Federation Germany and Dr Nicholas Hicks, director of OptiMedis-COBIC UK
Healthcare Costing for Value Institute
18
The Gesundes Kinzigtal approach has generated savings against the population budget, compared with other regions. One of the main drivers of these savings is a slower increase in the number of emergency hospital admissions. Gesundes Kinzigtal contracts with traditional health and care providers as well as collaborating with a range of community groups, e.g. sports clubs, education centres, to provide a good primary prevention system. It also runs health promotion programmes in schools and workplaces (figure 11).
Figure 10: Objectives of Gesundes Kinzigtal
Figure 11: The local network
Healthcare Costing for Value Institute
19
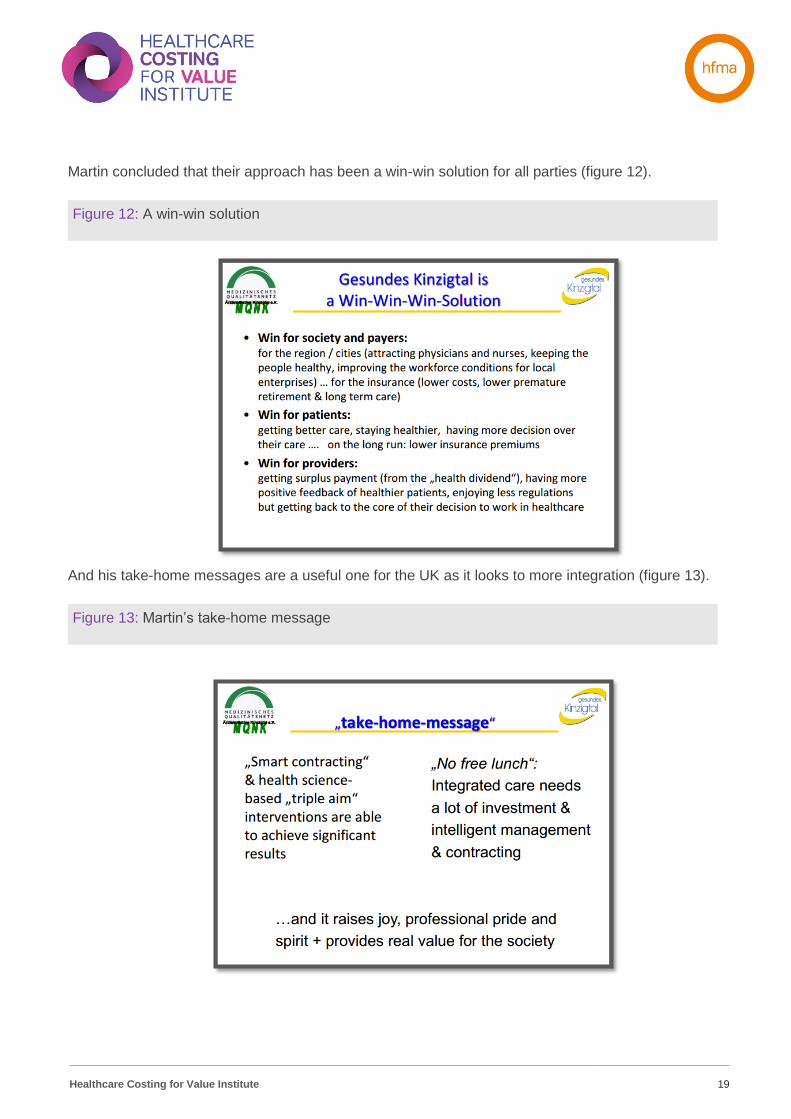
Martin concluded that their approach has been a win-win solution for all parties (figure 12). And his take-home messages are a useful one for the UK as it looks to more integration (figure 13).
Figure 12: A win-win solution
Figure 13: Martin’s take-home message
Healthcare Costing for Value Institute
20
Published by the Healthcare Financial Management Association (HFMA) 1 Temple Way Bristol BS2 0BU T 0117 929 4789 F 0117 929 4844 E [email protected] W www.hfma.org.uk While every care has been taken in the preparation of this publication, the publishers and authors cannot in any circumstances accept responsibility for errors or omissions and are not responsible for any loss occasioned to any person or organisation acting or refraining from action as a result of any materials within it. © Healthcare Financial Management Association 2018. All rights reserved. The copyright of this material and any related press material featuring on the website is owned by the Healthcare Financial Management Association (HFMA). No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form by any means, electronic, mechanical, photocopy, recording or otherwise without the permission of the publishers. Enquiries about reproduction outside of these terms should be sent to the publishers at [email protected] or posted to the above address. Healthcare Financial Management Association (HFMA) is a registered charity in England and Wales, no 1114463 and Scotland, no SCO41994. HFMA is also a limited company registered in England and Wales, no 5787972. Registered office: 110 Rochester Row, Victoria, London SW1P 1JP.