introducing computerized alert systems into clinical practice in the or and icu azriel perel in...
TRANSCRIPT

Introducing computerized alert Introducing computerized alert systems into clinical practice systems into clinical practice
in the OR and ICUin the OR and ICU
Azriel PerelAzriel Perel
in collaboration within collaboration with Kantor G, Toderis L, Eden A*, Pizov R*, Segal EKantor G, Toderis L, Eden A*, Pizov R*, Segal E
Department of Anesthesiology and Intensive Care,Department of Anesthesiology and Intensive Care,Sheba Medical Center, Tel Aviv University, Sheba Medical Center, Tel Aviv University,
and *Carmel Hospital, Technion Medical School, Haifa, and *Carmel Hospital, Technion Medical School, Haifa, IsraelIsrael
ESCTAIC 2005 AalborgESCTAIC 2005 Aalborg
DisclosureDisclosure
The speaker cooperates with the following companies The speaker cooperates with the following companies
CritiSenseCritiSense
Drager-SiemensDrager-Siemens
iiMDMDsoft soft **
InSightecInSightec
PhilipsPhilips
Pulsion Medical SystemsPulsion Medical Systems

An advanced feature of the automated record- keeper and the patient data-management system.
A configurable rule-based system that identifies pre-defined events in real time.
Triggers specific messages / alarms / waveform capture / diagnosis and treatment suggestions.
Improves response of care-giver to the ‘event’.
An example of how information-technology can improve patient safety.
The Event Manager

WANSupport
Ethernet
Switch
HISLabsADT
MV Cluster / ServerMVBS & Database
Printer
Pump
AnesthesiaMachine
Terminal server
Client
RemoteWorkstation
Monitor
Hospital network
Medical Devices Segment
Pager, E-mail, Cellphone
EVENTEVENT
Disregard of available data
Failure to seek appropriate data
Incorrect respone to available data due to lack of knowledge
The Event Manager is a tool that can potentially improve patient safety by preventing errors* that are mainly due to :
* In this context ‘error’ may be due to either commission or omission.

Proc AMIA Symp. 2000

Event definitions for intracranial pressure
and cerebral perfusion pressure were
studied by implementing a reliable system
to automatically deliver alerts to
alphanumeric pagers.
Closing the loop in ICU decision support: physiologic event detection, alerts, and documentation.
Norris PR, Dawant BM. Proc AMIA Symp. 2001;:498-502

A growing collection of medication safety rules….may be applied to each medication order message to provide an additional layer of protection beyond existing order checks, reminders, and alerts available within our computer-based record system.
Use of a clinical event monitor to prevent and detect medication errors.
Payne TH et al, Proc AMIA Symp. 2000;:640-4.

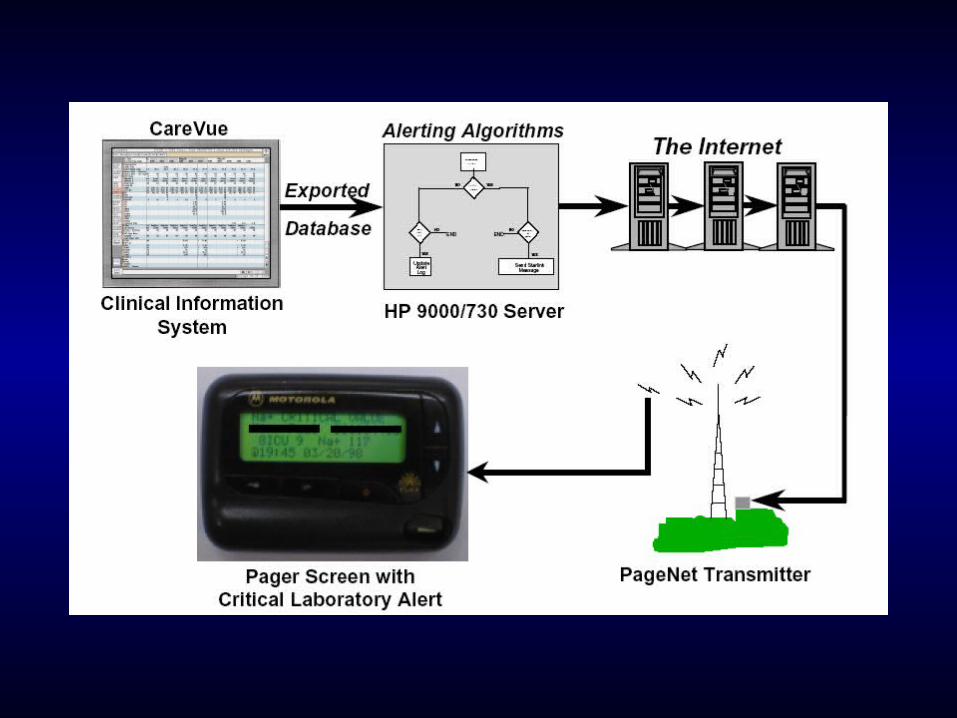
An automatic alerting system reduced the time
until an appropriate treatment was ordered for
patients who had critical laboratory results.
Information technologies that facilitate the
transmission of important patient data can
potentially improve the quality of care.
Improving response to critical laboratory results with automation: results of a randomized controlled trial
Kuperman GJ et al, J Am Med Inform Assoc. 1999;6:512-22

All these examples are
usually ‘house-made’ and are
not a part of a commercially
available information system
Potential use of the Event Manager in the ICU
• Medical– Diagnosis-related information – Improved detection of clinical events– Procedure reminders– Knowledge-base (algorithms, drugs, etc)
• Nursing – Follow routines– Follow protocols
• Pharmacy– Drug dosing, interactions, allergies

Medical
• Chest x-ray following central line placement
• Anticoagulants following trauma
• Thyroid replacement in hypothyroidism
• Corticosteroids in sepsis
Nursing
• GCS after admission
• Norton scale (prevention of pressure sores)
• IV line set changes every 96 hours
Examples of clinical implementation of the Examples of clinical implementation of the MetaVision Event Manager in our ICU MetaVision Event Manager in our ICU
Use of a computerized guideline for glucose regulation in the ICU improved both guideline adherence and
glucose regulation
E. Rood et al, J Am Med Inform Assoc 2005; 12: 172-80
Department of Intensive Care, Onze Lieve Vrouwe Gasthuis,
Amsterdam, The Netherlands
First published report on the use of the MetaVision Event Manager
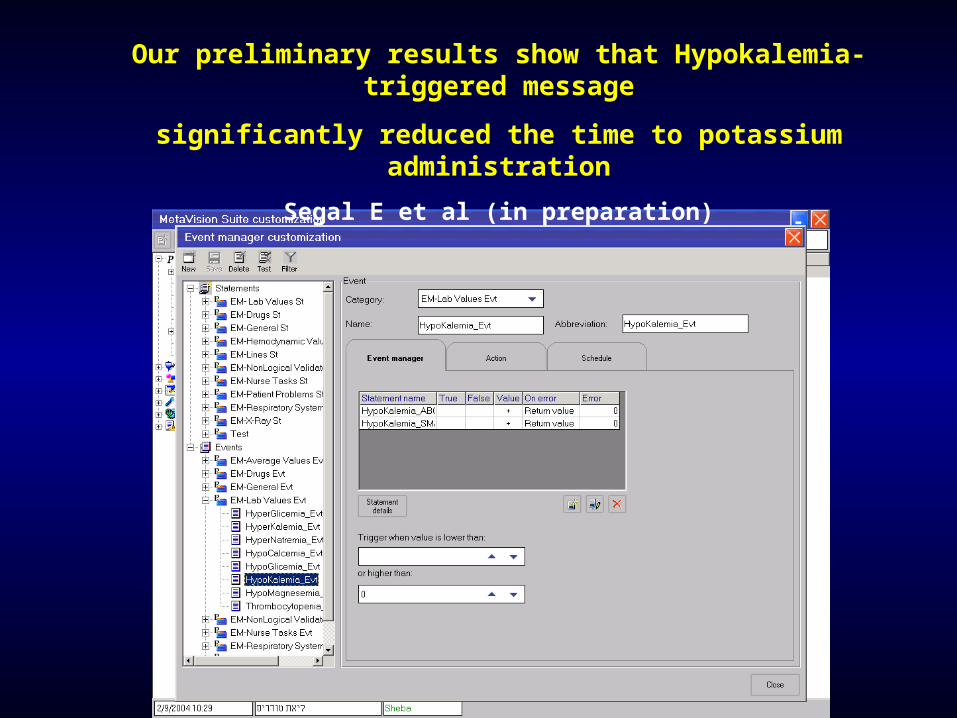
Our preliminary results show that Hypokalemia-triggered message
significantly reduced the time to potassium administration
Segal E et al (in preparation)
A ‘persistent decrease in SaO2’ event
A reduction in SaO2 of more than 4% lasting for more
than 6 minutes
The monitor default alarm for SaO2 is normally set to 90%
The following event is being used in our ICU…..The following event is being used in our ICU…..
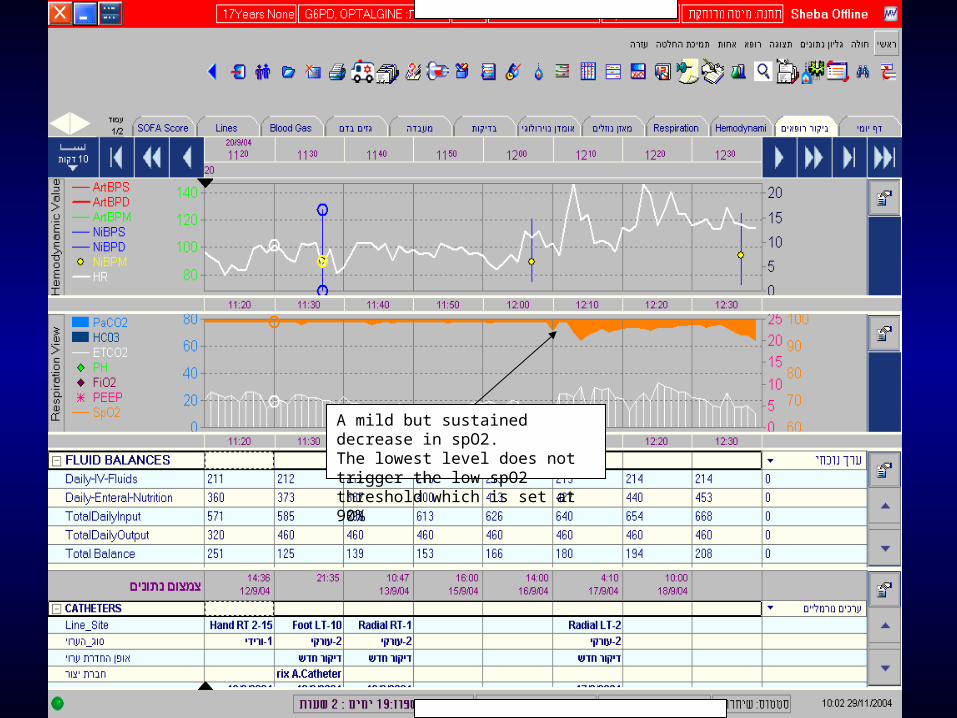
A mild but sustained decrease in spO2.The lowest level does not trigger the low spO2 threshold which is set at 90%
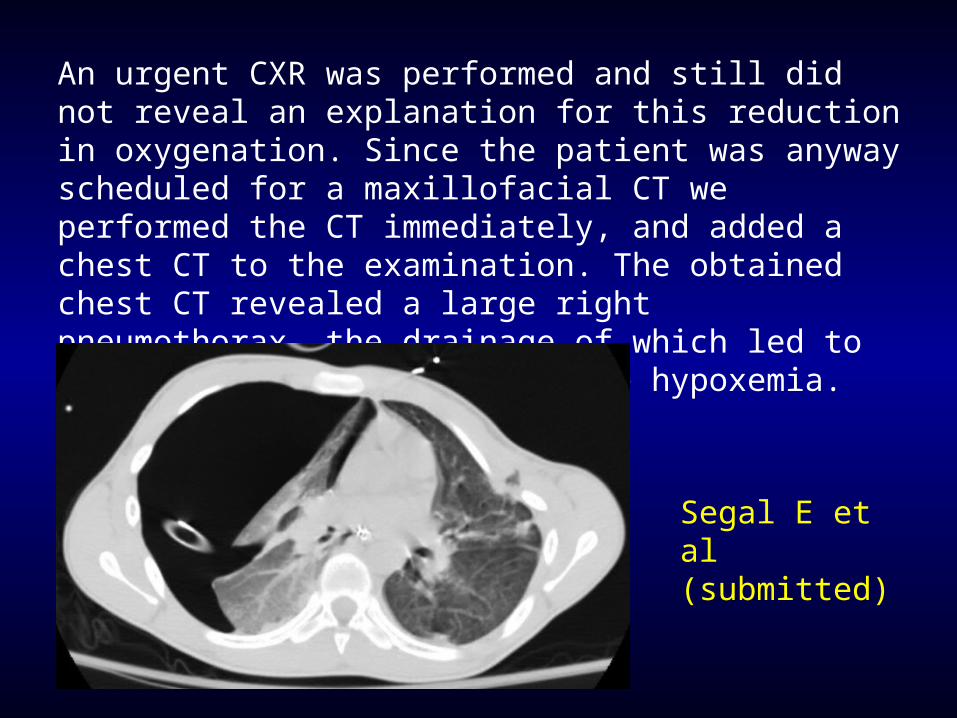
An urgent CXR was performed and still did not reveal an explanation for this reduction in oxygenation. Since the patient was anyway scheduled for a maxillofacial CT we performed the CT immediately, and added a chest CT to the examination. The obtained chest CT revealed a large right pneumothorax, the drainage of which led to an immediate resolution of the hypoxemia.
Segal E et al (submitted)

Comparing the OR to the ICU vis-a-vis the Event Manager -
Similarities
Acute care environments with abundance of life-
threatening situations and decisions.
Overload of information (intense monitoring,
frequent lab tests).
Variety of sources of information.
Comparing the OR to the ICU vis-a-vis the Event Manager -
Differences
OR - single care-giver; ICU - complex team.
Continuous anesthesiologist’s presence in the OR (qualifications may not always be adequate).
Time-constant of events during anesthesia is usually shorter.
Different workflow (in the OR you frequently do first and record later - no orders).
Potential use of the Event Manager in the OR
Administrative (e.g., reminders)
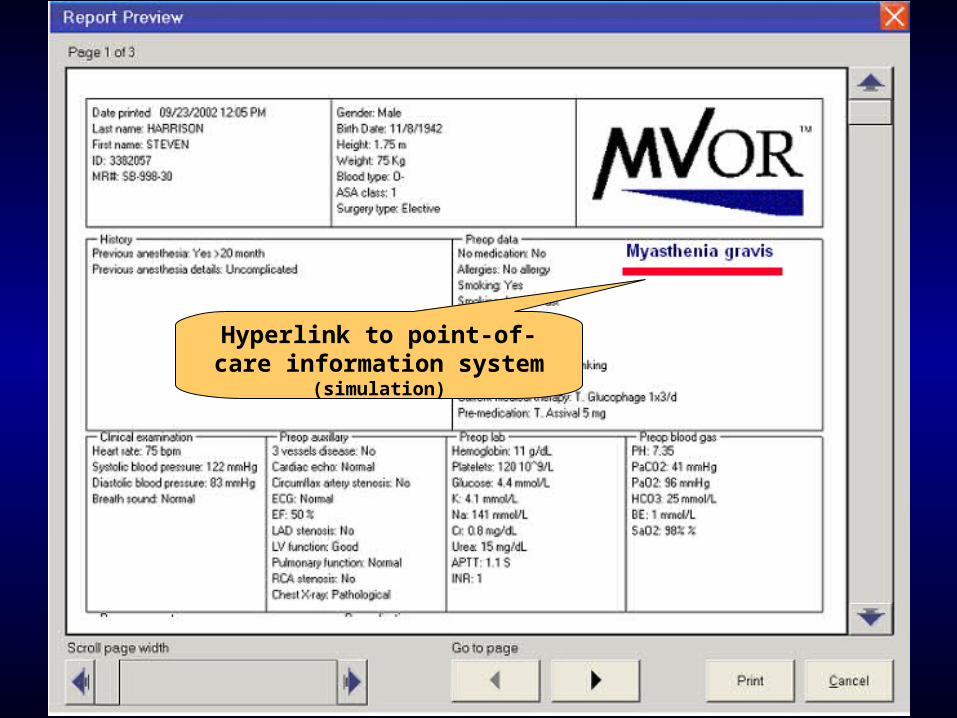
Diagnosis-related (e.g., preop clinic)
Pattern recognition of vital signs trends (e.g., MH)*
‘Smart alarms’ (e.g., low FiO2 **)* Remember that MVOR stores only one data point per minute
** The low FiO2 alarm threshold in the GE ADU anesthesia machine is 18%!?!
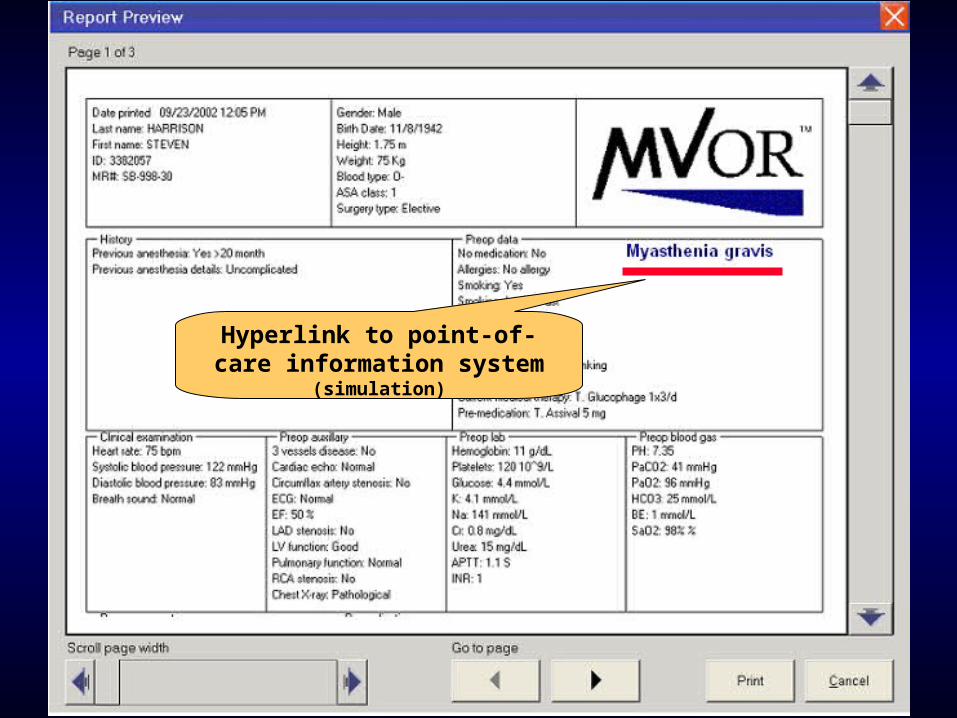
Hyperlink to point-of-care information system
(simulation)

Hyperlink to point-of-care information system
(simulation)

Hyperlink to point-of-care information system
(simulation)

The “AirEmbolism”
Event Definition
The Event’s Statements
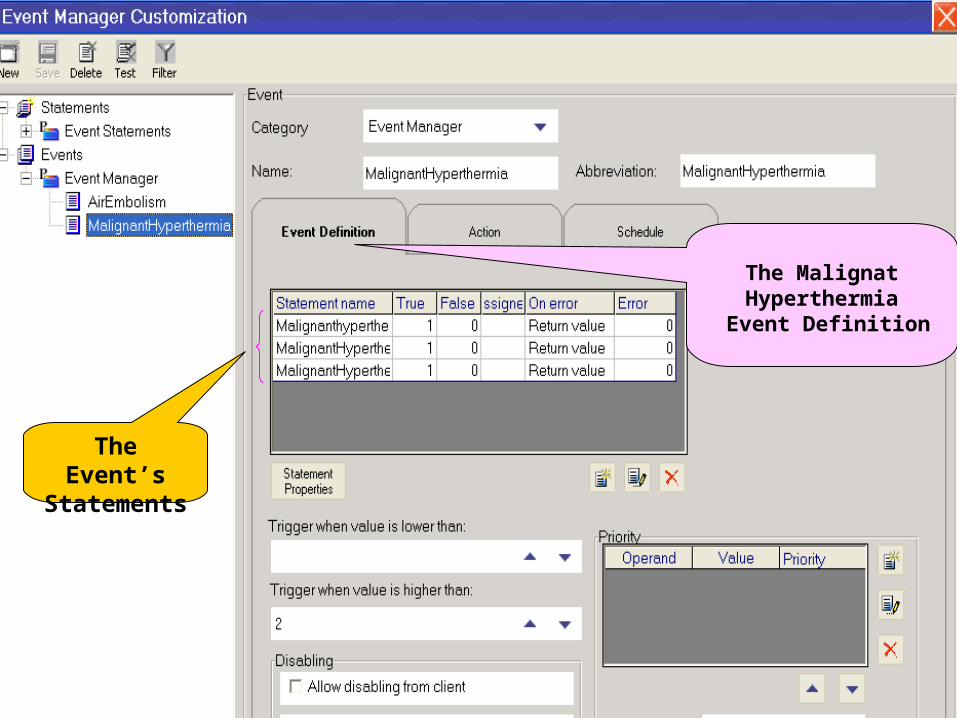
The Malignat Hyperthermia
Event Definition
The Event’s Statements


A potential application of the Event manager in the OR:
Scenario A
Patient goes off cardiopulmonary bypass.
Surgeon: “You can start to ventilate”
Anesthesiologist hooks ventilation circuit but forgets to turn on the ventilator.
All alarms are “ Off ”.
After a few minutes surgeon says: “The blood is very dark”.
Scenario B
Patient goes off cardiopulmonary bypass.
The Event Manager identifies the combination “Bypass on” +
“Alarms off” + evidence of pulsations >>>>
““Please turn on alarms”Please turn on alarms”““Please turn on alarms”Please turn on alarms”““Please turn on alarms”Please turn on alarms”““Please turn on alarms”Please turn on alarms”““Please turn on alarms”Please turn on alarms”““Please turn on alarms”Please turn on alarms”
““Please turn on alarms”Please turn on alarms”
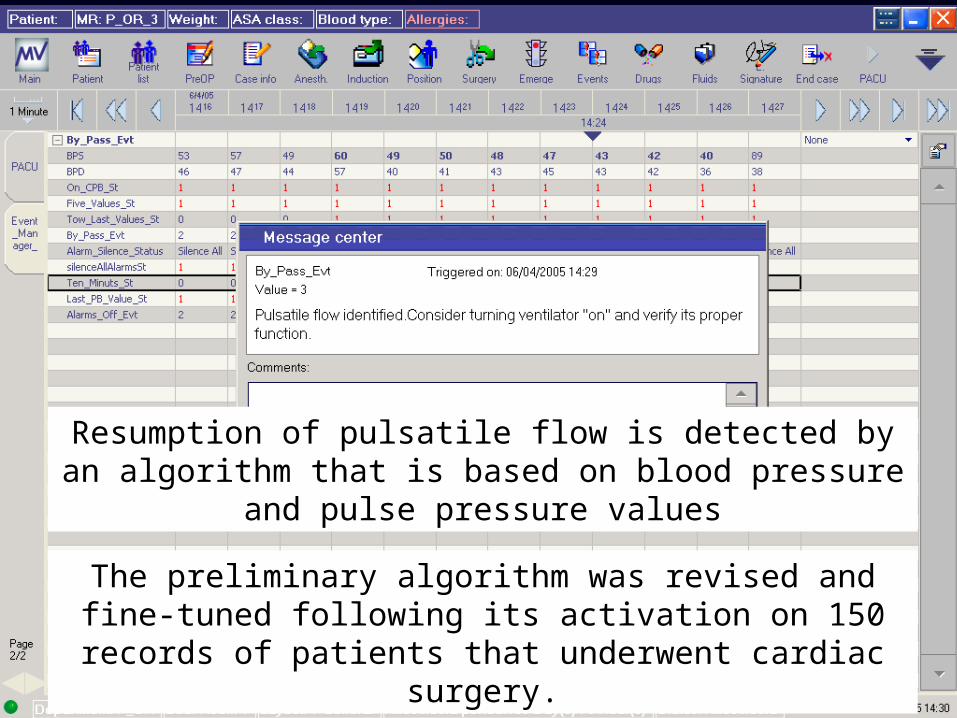
Resumption of pulsatile flow is detected by an algorithm that is based on blood pressure and pulse pressure values
The preliminary algorithm was revised and fine-tuned following its activation on 150 records of patients that
underwent cardiac surgery.
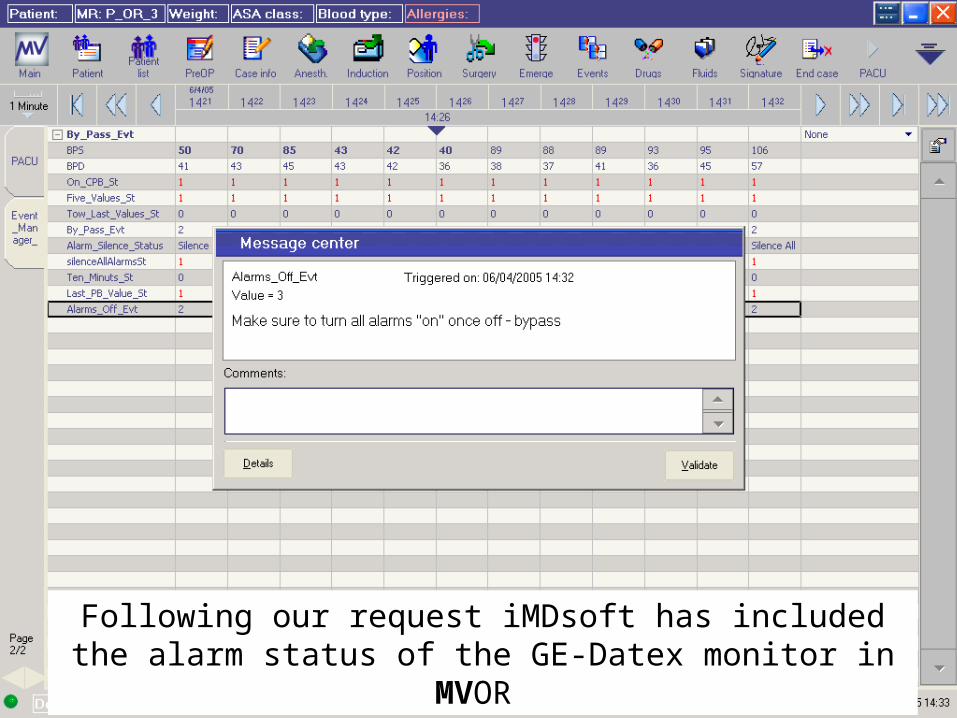
Following our request iMDsoft has included the alarm status of the GE-Datex monitor in MVOR
Off-bypass check-list
Another potential application of the Event Manager:
“Bypass on” +
evidence of pulsations >>>>
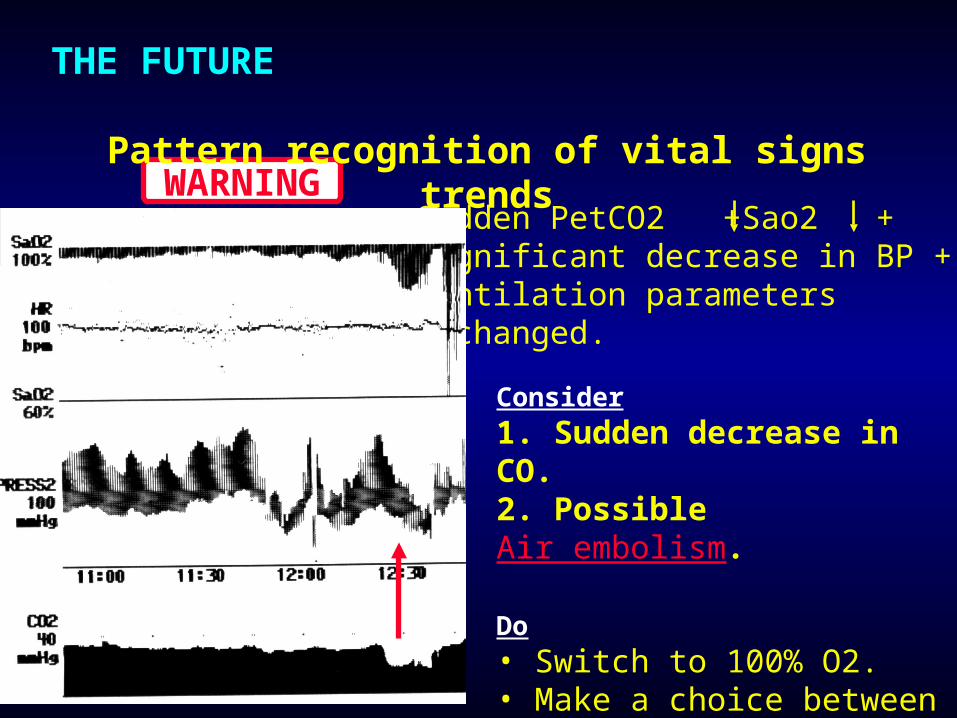
Sudden PetCO2 +Sao2 +significant decrease in BP + ventilation parameters unchanged.
WARNING
THE FUTURE Pattern recognition of vital signs trends
Consider
1. Sudden decrease in CO.2. Possible Air embolism.
Do• Switch to 100% O2.• Make a choice between 1 & 2.

A ‘good’ Event should fulfill the following criteria:
1. Clinically significant
2. Offer opportunity for corrective action
3. Come out of necessity, i.e., the recognition that it may be missed due to overload of tasks or information
4. Well defined
5. Not too common
6. High sensitivity and specificity
Limitations and pitfalls
The concepts of clinical significance and opportunity for
corrective action are difficult to define in automated systems
The definition of a successful event may prove to be
difficult and time-consuming
Overloading the system with too many events is
unwelcome by users
Events should not be trivial
Lack of sensitivity (false negative) and/or specificity (false
positive) are both dangerous and annoying
A growing collection of medication safety rules….may be applied to each medication order message to provide an additional layer of protection beyond existing order checks, reminders, and alerts available within our computer-based record system.
During a typical day the event monitor receives 4802 messages, of which 4719 pertain to medication orders. We have found the clinical event monitor to be a valuable tool for clinicians and quality management groups charged with improving medication safety.
Use of a clinical event monitor to prevent and detect medication errors.
Payne TH et al, Proc AMIA Symp. 2000;:640-4.

Event definitions for intracranial pressure and cerebral perfusion pressure were studied by implementing a reliable system to automatically deliver alerts to alphanumeric pagers.
During a 6-month test period in the trauma ICU 530 alerts were detected in 2280 hours of data spanning 14 patients.
Retrospectively classifying documentation based on therapeutic actions taken, or reasons why actions were not taken, provided useful information about ways to potentially improve event definitions and enhance system utility.
Closing the loop in ICU decision support: physiologic event detection, alerts, and documentation.
Norris PR, Dawant BM. Proc AMIA Symp. 2001;:498-502
Nearly 90% of clinicians thought drug alerts would be helpful to identify interactions yet 55% of clinicians perceived that the most significant barrier to utilizing existing alerts was poor signal to noise ratio, meaning too many non-relevant warnings.
CONCLUSIONS: The perceived poor specificity of drug alerts may be an important obstacle to efficient utilization of information and may impede the ability of such alerts to improve patient safety.
Improving recognition of drug interactions: benefits and barriers to using automated drug alerts.
Glassman PA et al, Med Care. 2002 ;40:1161-71
A total of 15,066 alert pages were sent, including alerts for physiologic condition (6,163), laboratory data (4,951),blood gas (3,774), drug allergy (130), and toxic drug levels (48).
Wireless clinical alerts and patient outcomes in the SICU
Major K, Shabot MM, Cunneen S. Am Surg. 2002; 68:1057-60
The Cedars-Sinai experienceThe Cedars-Sinai experience
Too many alerts?

Cedars-Sinai Doctors Cling to Pen and Paper Cedars-Sinai Doctors Cling to Pen and Paper By Ceci Connolly, Monday, March 21, 2005; Page A01 washingtonpost.com
LOS ANGELES -- The marriage of information technology and medicine is all the rage in health policy circles…. Five years after the Institute of Medicine issued a landmark report cataloguing the life-and-death consequences of medical errors, corporate leaders, politicians and physicians are embracing computer-assisted health care.
(However) ….an array of problems that grew into a full-blown staff rebellion in the fall of 2002 forced Cedars-Sinai to shelve its $34 million computer system after three months.
…..the biggest complaint -- with potentially dangerous
implications -- involved the automatic alerts that flashed
on the screen every time a doctor made an out-of-the-
ordinary request. Designed to catch errors before they
occur, the alerts became an unending series of
questions, reminders and requests on fairly basic
decisions.
Cedars-Sinai was unable to strike a balance between
useful computer warnings and a machine that seemed
to constantly cry wolf….
washingtonpost.com Monday, March 21, 2005; Page A01
Conclusions
The introduction of the Event Manager offers exciting possibilities in using information technology to improve task performance and patient safety.
Preliminary lessons from its implementation in the ICU environment are very promising.
Introducing this powerful tool into the OR may improve decision making and help prevent errors.
The careful selection and design of new ‘events’ is the key to the successful implementation of this new tool.
“If we truly want safer care,
we will have to design
safer systems”
Berwick, Leape BMJ 1999;319:136-7
Thank you!Thank you!

Thank You!Thank You!