ipras journal 7th issue
DESCRIPTION
he purpose of THE IPRAS JOURNAL is to provide a rapid reporting of things of interest to IPRAS members. This includes all members of national societies who participate in the IPRAS organization. Because of the broad umbrella of IPRAS this includes matters of interest across a broad spectrum of sub-specialties including burn surgery, microscopic and reconstruction surgery, hand surgery, craniofacial surgery, and aesthetic surgery. In many instances it will include matters of interest to all specialties of plastic surgery combined. Matters of interest include, but are not limited to surgical techniques, patient care, patient safety, recognition and treatment of complications of surgery, humanitarian contributions, and schedules of pending meetings. Authors are encouraged to submit manuscripts for publication which will be evaluated by a peer review process. Letters to the Editor are encouraged and will be published if deemed contributory to the aims and scope of the Journal.TRANSCRIPT
ISSN: 2241-1275

2 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 3
C O N T E N T S
PAGE55IPRAS Booth at the 1st Chinese European Congress of Plastic Reconstructive and Aesthetic Surgery
PAGE77Historical Account of BAPRAS
Issue 7 www.ipras.org IPRAS Journal 3
PAGE36Humanitarian mission in Togo
PAGE14IPRAS Presentation from Mr. Zacharias Kaplanidis (IPRAS Executive Director) during the 48th Brazilian Congress of Plastic Surgery
• President’s Message . . . . . . . . . . . . . . . . . . . . . . . . . . 5
• The PIP Breast Implant Scandal . . . . . . . . . . . . . . . 6
• General Secretary’s Message . . . . . . . . . . . . . . . . . . 9
• Editor-in-Chief’s Message . . . . . . . . . . . . . . . . . . . 12
• IPRAS Management office Report . . . . . . . . . . . 14
• Pioneers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
• Rising Star . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
• Senior Ambassador . . . . . . . . . . . . . . . . . . . . . . . . 24
• Humanitarian Works . . . . . . . . . . . . . . . . . . . . . . . 26
• Surveys . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
• National Associations’ & Plastic surgery organizations’ news . . . . . . . . . . . . . . . . . . . . . . . . 50
• Historical Accounts . . . . . . . . . . . . . . . . . . . . . . . . 63
• Certificate of Membership . . . . . . . . . . . . . . . . . . 86
• Congresses and Events . . . . . . . . . . . . . . . . . . . . . 90
• National & co-opted societies future events . . . 114
• IPRAS website . . . . . . . . . . . . . . . . . . . . . . . . . . . 116
• Industry news . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
• IPRAS Benefits for National Associations & individual members . . . . . . . . . . . . . . . . . . . . . 119
4 IPRAS Journal www.ipras.org Issue 7
• To promote the art and science of plastic surgery
• To further plastic surgery education and research
• To protect the safety of the patient and the profession of Plastic, Reconstructive and Aesthetic Surgery
• To relieve as far as it is possible the world from human violence or natural calamities through its humanitarian bodies
• To encourage friendship among plastic surgeons and physicians of all countries
A I M S A N D S C O P E

Issue 7 www.ipras.org IPRAS Journal 5
I P R A S J O U R N A LP R E S I D E N T ’ S M E S S A G E
Board of Directors
PresidentMarita Eisenmann-Klein - Germany
General SecretaryNelson Piccolo - Brazil
TreasurerBruce Cunningham - USA
Deputy General SecretaryYi Lin Cao - China
Deputy General SecretaryBrian Kinney - USA
Deputy General SecretaryAhmed Noureldin - Egypt
Deputy General SecretaryAndreas Yiacoumettis - Greece
ParliamentarianNorbert Pallua - Germany
Executive DirectorZacharias Kaplanidis - Greece
Prof. Marita Eisemann-KleinPresident of IPRAS
Dear colleagues,2011 was the year of solidarity.Solidarity with our brave colleagues in Japan – while we felt powerless and helpless; solidarity with our colleagues during the unrests in the Arab world, with our colleagues in countries which had to face crisis and disasters.Solidarity with patients in developing countries: the number of missions and the number of active collaborators in our humanitarian projects increase considerably every year.Solidarity with patients who became victims of the PIP crime, is our latest challenge. These patients need all our support in their anxieties and in their search for implant removal at affordable expenses.Solidarity with our young residents: the evaluation form about training conditions will be launched soon and the first “Residents World Congress” will be held on November 1st , 2012 in Athens, Greece. There, we also plan to start the Academy for Residents Training.With the foundation of our Board of Trustees, we span the generations from the youngest to our senior role models, our giants, our heroes. Recently we honoured our new Board of Trustees members during the Brazilian Congress of Plastic Surgery: Ricardo Baroudi and Ivo Pitanguy. They do not only stand for progress and technical excellency in plastic surgery, they are charismatic philosophers as well.2012 will be the year of pioneers in Plastic Surgery: Sydney Coleman has composed a fantastic program for the 1st International Congress of ISPRES in Rome, March 9-11, 2012. I am excited about the incredible amount of research programs in plastic surgery which will be presented in Rome. We feel overwhelmed by the interest of our members in these innovative future oriented techniques. I never before experienced having to close the registration two months prior to the start of a congress!
For all those who missed registration: We decided to offer online-participation. Just watch out for further announcements!Keep monitoring at our other congress announcements too: exciting topics and exciting locations are offered to you.There is a lot to look forward to this year! There is also a lot to thank for during the past year:Thanks, from the bottom of my heart, to all of you
Presentation of Prof. Marita Eisenmann-Klein, Germany (IPRAS President) during the 48th Brazilian
Congress of Plastic Surgery
who supported and assisted to develop IPRAS further – our humanity, our skills, our identity. Thank you for your confidence in the IPRAS leadership and in me personally.It is such a pleasure to serve you as your President.I wish you all a year of happiness and joy and full of chances to develop your identity as a plastic surgeon even further!
Cordially yours
Marita Eisenmann-Klein
IPRAS President

6 IPRAS Journal www.ipras.org Issue 7
Chronology:
As early as in May 2000 the US Food and Drug Administration performed an inspection of the PIP production site in Southern France. As a result of this inspection the sale of PIP implants was stopped in the US. In a letter to Jean-Claude Mas, the owner of PIP, the FDA stated that the implants were “adulterated” along with eleven other deviations from good manufacturing practices such as lack of sufficientinvestigation of deflation rate and failure of reporting 120complaints.Whether the French Health Authority AFSSAPS was informed by the FDA, about the results of their inspection or not, is unclear.PIP must have started to exchange the medical grade silicone for industrial silicone probably in 2003. For a while, PIP used both types of gel but probably stopped using medical grade gel around 2005. From that time on, most likely they only used industrial silicone. Roughly estimated: there must have been around 200 000 kilograms of industrial silicone delivered to PIP and nobody considered this suspicious!Inspections were performed by TÜV Rheinland regularly but they all were announced ten days prior to their visit, which is in accordance with the requirements of the European Medical Device Law. Starting in 2008, more and more plastic surgeons reported a high failure rate in PIP implants. After an investigation by AFSSAPS, the French Health Authorities banned PIP implants in spring of 2010.Obviously the PIP implant stock or at least part of it was sold to the Netherlands and the distribution was continued by Rofil Medical under the name “M-implant”.When the Dutch health authorities found out that PIP and M were identical, M-implants were banned in June 2010.Obviously, it was still possible to continue with the distribution of M-implants. The last report we received was about an M-implant inserted as late as October 2011! The distributing company claims that this M-implant has nothing to do with PIP. Only the name would be the same, but the new product would be produced in Cyprus. The report from our colleagues in Cyprus revealed that there was no production site in Cyprus. Subsequently, the company claimed that the production site was in Korea (North Korea??).There are also hints that these products were sold to Middle and South America. Hopefully through our well functioning network with the help of our colleagues we can trace them down.In November of 2011 a patient with PIP implants in France died from Anaplastic Large Cell Lymphoma, which developed in the scar capsular tissue around the implants.Subsequently, AFSSAPS released a warning that patients with PIP implants should be examined regularly but they did not suggest a prophylactic implant removal. After
thorough evaluations the French Society of Plastic Surgery decided to recommend a prophylactic explantation of all PIP implants.Finally, on December 23rd 2011, AFSSAPS also announced, that all PIP implants should be removed prophylactically.Most of the Health Authorities in Europe were hesitant to follow this recommendation, while plastic surgery societies took the lead and recommended explantation. For example, the German Association of Plastic, Reconstructive and Aesthetic Surgeons convinced the German Cancer Society and the Gynaecological Society to hold a press conference together on January 6, 2012 to announce the recommendation for explantation. BfArM, the German Health Authorities followed and released a recommendation for explantation a few hours later. In many other countries, health authorities are still hesitant to come up with a recommendation for explantation. In a telephone conference of most of the European Health Authorities the majority recommended to wait for more data.They claim that the potential risks of surgery and anaesthesia might be higher than the potential risk of leaving the implants in. There is an error in this logic: considering the high failure rate of these implants, the probability, that these implants rupture within the next few years is extremely high, which means that there is an almost 100% probability that these implants will have to be removed within the life span of the patient, but then under much worse conditions.
What do we know about the health risks of PIP implants?
We can only estimate the number of PIP implant patients to be around 500.000 worldwide. We know that PIP also produced other implants such as Testicle implants, buttock implants and chest implants for men. We know that the industrial gel which was used by PIP has been tested and found not to be toxic. However, there are signs that the gel might have been manipulated after it was delivered to PIP. So, in fact, we do not know for sure whether or not it contains toxic elements. This issue is still under investigation.We know that the rupture rate of these implants is considerably higher than the normal rupture rate for breast implants which is considered to be 1%.Most of the Health Authorities declared rupture rates between 5 and 10% for PIP, but the declarations vary.We also know that the inflammatory reaction in PIP implants seems to be unusually high in case of rupture. But even without rupture, patients may develop lymphadenopathy with painful and enlarged lymph nodes as far away as in the groin, mediastinum and neck. Axillary lymph nodes are enlarged in many patients.Although there were 16 cases of breast carcinoma reported in France in PIP implant patients, there seems to be no relation between PIP and breast cancer. These cases are
The PIP Breast Implant Scandal
Issue 7 www.ipras.org IPRAS Journal 7
within the range of statistically expected cases.Anaplastic Large Cell Lymphoma (ALCL) is a tumor of the immune system. Worldwide 75 patients with breast implants out of an estimated number of more than 10 million patients with breast implants have developed this disease. Four of these patients died.It seems that the pre-disposition to develop this very rare disease is multi-factorial and not yet completely understood. Chronic inflammation usually plays a role inthe development of an ALCL. The risk of developing ALCL for patients with breast implants is, according to the FDA, 1 in 500 000 to 1 million patients. The FDA states: “Patients with breast implants may have a small but increased risk in developing this disease”.
What we still need to find out:
We still don`t know the exact number of patients with PIP implants and M-implants.The estimation is around 500 000 worldwide.We still do not know whether more M-implants are still in use, may be even under a third name, either in Europe or South America.
IPRAS conclusions:
1. There is no further room for discussion. It is mandatory to recommend the explantation of PIP and M-implants.
2. Law suits against plastic surgeons should not be successful according to our legal advisors, since a stockholder must rely on the quality of a product that has been granted a CE mark.
3. It is unnecessary to call for new laws. The existing Medical Device Laws are sufficient.
The policies, however, should be changed e.g. inspections without previous announcements.
The European Commission invited me today to join their SCIENTIFIC COMMITTEE ON EMERGING AND NEWLY IDENTIFIED HEALTH RISKS WORKING GROUP ON PIP IMPLANTS.
The first teleconference will be held tomorrow. I am veryimpressed by the ambitious time table of our chairman Philippe Martin, with a deadline for the scientific opinionto be completed by January 30.
4. This is not a scandal of the breast implant industry. This is a scandal of a group of criminal individuals who don`t mind to harm the health of 500 000 women.
The high quality and safety standards of our breast implant industry deserve to be relied on.
5. We have to negotiate with health insurance companies and convince them to provide the expenses for explantation. We also have to negotiate with our managers to provide replacement of implants at the lowest possible expenses.
6. We all need to cooperate in order to implement patient registries in order to get reliable data and to have a tool for postmarket surveillance.
7. Please bear in mind that our patients have to undergo a period of fear and insecurity. It is essential that we avoid public controversies regarding this issue.
Therefore we appeal to all of you to accept the following organizations as the legitimate representation of all plastic surgeons in the world:1. On national level: the national society of plastic surgery
exclusively. The national societies should also look for partners e.g.
medical associations, health care providers, government, cancer societies, other scientific societies and consumergroups, which could be involved.
The President of the German Association of Plastic, Reconstructive and Aesthetic Surgeons, Prof. Peter Vogt, was very successful in presenting the statement of the society together with the German Cancer Society and the Gynaecological Society in a press conference.
2. On regional level (such as African, Asian Pacific,European, Ibero-Latin-American, Pan-Arab): the section to which this area belongs should be responsible for statements.
3. For global activities and cooperation with WHO: IPRAS and its quality assurance committee, IQUAM, are the legitimate representatives of plastic surgeons.
IPRAS is committed to serve the national societies and the sections with its network and expertise. We continue to prepare drafts for media releases and send them to you. We shall only approach the media if you ask us to do so.Thank you all for reporting back to us. All the useful information we received from you helped to clarify the situation and come up with important information which no other institution or organization can provide.Please continue to inform us!Cordial thanks to all of you who supported our work. We are very grateful for your cooperation and proud of our network excellency!
Daniel MarchacIQUAM General Secretary
Andreas YiacoumettisESPRAS President
Marita Eisenmann-KleinPresident IPRAS
Nelson PiccoloIPRAS General Secretary
Constance Neuhann-LorenzIQUAM President

8 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 9
48th Brazilian Cοngress of Plastic Surgery Homage to ExPresidents
G E N E R A L S E C R E T A R Y ’ S M E S S A G E
I am very happy to say that, once more, Plastic Surgery has demonstrated its internationality and its boundless features. Over 2150 surgeons from 14 countries came to Goiania, in the central part of Brazil, to attend the 48th Brazilian Congress of Plastic Surgery. For me, this was an extra special moment, since I have been living in Goiania since 1963. Although I had lived away for 7 ½ years, coming back to establish my practice and also to continue my family’s work in burns, in 1989, I certainly consider this my town. And it was a great honor and and unique pleasure to see this mega event happen here.
For the Sociedade Brasileira de Cirurgia Plástica it was also a most special moment. There was a great homage to Past Presidents, which brought honor and great value to their deeds in improving all aspects of Plastic Surgery in our country. Also, IPRAS President, Marita Eisenmann-Klein and IPRAS Executive Director, Zacharias Kaplanidis, were closely involved with all official ceremonies and also had opportunities to present their work, as well as the work of IPRAS, in several
fields. Dr Eisenmann-Klein took a moment during the opening ceremony to honor Profs. Baroudi and Pitanguy as Members of the IPRAS Board of Trustees – certainly one of the night’s highlights.
Prof. Nelson PiccoloIPRAS General Secretary
During the plenary session on “Women in Plastic Surgery”

10 IPRAS Journal www.ipras.org Issue 7
Prof. Nelson PiccoloIPRAS General Secretary
continuously searching (and finding) ways of ensuring that this very precious aspect of Plastic Surgery is distributed as uniformly as possible.
There is, however, a lot of work still to be done for us to attain that goal – Sarah Lorenz of Munich, Germany and some colleagues of her, also residents in Plastic Surgery, are launching a worldwide survey to ascertain the quality, uniformity and content of training in Plastic Surgery. When the survey reaches you, please make sure you take a moment and help this dedicated group of young surgeons to plan the world map in Plastic Surgery Training. We need to know, so we can continue to improve the equality of our already established internationality.
48th Brazilian Congress of Plastic Surgery Opening Ceremony
Another first was the plenary session on Women in Plastic Surgery, when the audience had a chance to hear from Connie Neuhann-Lorenz (Germany), Lucie Lessard (Canada), Antonia Marcia Cupello (Rio de Janeiro) and Vera Lucia Cardim (São Paulo) presenting their experience and trajectory as Plastic Surgeons and the differences and similarities with their male colleagues, in relation to career, profession and life.
As I have mentioned in the past, I believe one of the most beautiful aspects of Plastic Surgery as a Specialty is its internationality – how one can perform procedures aiming at similar benefits for the patient, with knowledge acquired though training and collective experience of our colleagues and professors. We must, however, work harder to ensure adequate and uniform training for our residents, as well as adequate and uniform continuation of education for ourselves, practicing Plastic Surgeons.
IPRAS is truly engaged in this! Our Board of Directors, under the leadership of Marita Eisenmann-Klein, is
Issue 7 www.ipras.org IPRAS Journal 11

12 IPRAS Journal www.ipras.org Issue 7
EDIT
ORIA
L During the fall months, from September into early December, your Editor-in Chief has had the pleasure and honor of travel to various parts of the world and lecture, as well as speak with, colleagues on four continents. My first stop was Lake Baikal, in Eastern Siberia, near the city of Irkutsk, whichwas a geographic experience. The meeting was hosted by our able colleague Vadim Zelenin and had an attendance that exceeded 300 Surgeons. The faculty consisted of Brian Kinney from Los Angeles, Roberto Pizzamiglio from Marbella, Spain and your Editor. Also on the faculty were strong representatives from St. Petersburg and Moscow, Irina Khrustaleva and Natalia Manturova. The vast majority of the attendees were Plastic Surgeons from all parts of Siberia and the major topic of discussion was the face, but all areas of Plastic Surgery were discussed. When I attend a meeting as a lecturer I always try to give valuable information to the attendees and at Lake Baikal I was told this was the case. But likewise, when I attend as a listener, I hear the points of view of the other faculty and I leave a net winner in the information exchange.In all my trips I try to learn something about the area to which I’ve come. Lake Baikal was a hidden treasure. Sadly for me, my knowledge of the geography of that part of the world was underdeveloped and I was not aware of the magnitude of Lake Baikal. There are too many aspects of it to be covered in this short essay but it is known as the second largest lake in the world (the Caspian Sea is larger). At one mile deep it is among the deepest and, by my own viewing, one of the clearest. It is a geographic masterpiece and relatively unknown to the Western World.After Siberia I went to Madrid, where I participated as the only non-faculty member in a meeting put on by Jose Luis Martin Del Yerro, unquestionably one of the most skillful and knowledgeable Plastic Surgeons I know and someone whose worldwide recognition will soon soar .
I P R A S J O U R N A LE D I T O R - I N - C H I E F ’ S M E S S A G E
The bonds that unite us
Dr. Thomas M. Biggs, M.D.Editor-In-Chief
Dr. Riccardo Mazzola, IPRAS Historian, Dr. Thomas Biggs, IPRAS Journal Editor in Chief

Issue 7 www.ipras.org IPRAS Journal 13
After Madrid came Beijing, China, for the first Chinese-European Congress, with Yi Lin Cao as our host. Those who saw the Opening Ceremony of the 2008 Olympic Games immediately appreciated the powerful arrival of China as a world player, and this Congress was of similar style.Afterwards on to Puerto Vallarta for the 38th Annual Meeting of Jose Guerrerosanto, a major institution in the world of Latin American Plastic Surgery, put on by one of the titans of worldwide Plastic Surgery, who has been kind enough to invite me for many years.From Mexico, I went on to Goiania, Brazil, for their Annual Meeting and this, my 37th visit to Brazil, confirmed what I hadlearned on my first visit in 1972: that Brazil is inferior to nonein Plastic Surgery. During this visit, I enjoyed the company of friends I have made over many decades. Among them was Ivo Pitanguy, who was my gracious host on my first visit there, 39years ago. The multitude of friends there is too great to name individually, but I was pleased to visit with our Secretary General, Nelson Piccolo, and felt the pleasure of knowing his hand will be on the wheel of IPRAS for several years.Finally I attended a meeting in the U.S. In New York City, The Cutting Edge Meeting of old friends Sherrell Aston and Dan Baker. It was a booming success with attendees from 60 countries. They had a large and diverse faculty, each speaker being limited to 10-15 minutes, but each session being followed by an intense questioning by either Dr. Aston or Dr. Baker. The questions being those the moderators felt were probably foremost in the minds of the attendees.Finally, this message is being written from Miami, where I’ve come to visit Roger Khouri (the first “Frontiersman” in thisJournal). I’ve been staying with him, seeing new patients, short and long term follow ups, and spending many long hours in the operating room. In between, I’ve been working to help him assemble his thoughts for future publications.All of the above experiences have added immensely to my body of Plastic Surgery knowledge. My travels have exposed me to the fact that many of our colleagues around the world are performing operations in a way very similar to the way we perform them in our own facilities; there are also colleagues doing things differently, often with outstandingly good results. I’ve met colleagues with huge experience, who have never spoken of their findings, nor have they published, but theirwork is outstanding. As Editor-in Chief, I’m making it a project to bring these people out into the light, so we can all benefit
from their excellence.What you’ve just read is true and extremely important to me….but there’s more.During my travels, I have found a great similarity in my life and the lives of those colleagues from half a globe away….from people with whom I often need a translator to adequately communicate. There’s a similarity in the fact that our patients come to us with a need and they carry with them the faith in us that we can help resolve that need. I’ve found we share the same deep misery when some aspect of our surgery doesn’t go as we had planned, but we also share the same joy when we see a smiling face walking into our clinic and we know things are going well. The pink nipple rather than a blue one…a fingerwith full flexion and extension….a soft, well-shaped breastrather than one that is firm and contracted…..a happy smilefrom a young girl whose retruded maxilla is now in the right place. You, as surgeons, know what I mean…..the joys of our work…the Holiday card that says “Thank You”.All these things we share…whether it may be in Houston or Hong Kong, Moscow or Montevideo, Denver or Dubai, Stockholm or Sydney.These are bonds, similarities of purpose, works done in rooms that have a similar appearance the world over, the same relationship between the patient in need with the skillful physician who has the tools and experience to care for this human being with some kind of pain. We also share the knowledge, that in some areas our colleagues lack the tools to adequately play their role in healing and we share the desire to reach out and help.We, as Plastic Surgeons, are separated by languages, by borders and boundaries, and in some instances by cultures…..but the bonds that unite us are far, far greater than those factors that separate us. We truly are a family, brothers and sisters, all working to take care of the family business.What is the family business?The family business is to make people’s lives better through Plastic Surgery.
Dr. Thomas M. Biggs, M.D.Editor-In-Chief
Dr. Thomas Biggs, USA (IPRAS Journal Editor in Chief) with Ms. Maria Petsa, Greece (IPRAS Assistant Executive Director) at the IPRAS booth during the 48th Congress of the Brazilian Society of
Plastic Surgery.
Prof. Ivo Pitanguy, Brazil (IPRAS Trustee), Dr. Thomas Biggs (IPRAS Journal Editor in Chief) on 2007.
14 IPRAS Journal www.ipras.org Issue 7
I P R A S M A N A G E M E N T O F F I C E R E P O R T
October 2011 - December 2011Let’s give our answers to the Challenges
I P R A S M A N A G E M E N T O F F I C E R E P O R T
Mr. Zacharias Kaplanidis IPRAS Executive Director
There is no doubt that the international community is facing multiple and, perhaps, the most complicated challenges of the last decades.
Europe continues to tackle, with limited success until now, its fiscal issues; unemployment has reached dangerouslevels, especially in Southern Europe (in Greece alone it has reached 20%), Europe and America’s problems have began to burden China’s exports and developmental rate (less than 9% in 2011). Northern African and Middle East countries continue to be socially agitated, despite the collapse of the dictatorship regimes (Egypt, Iraq, Libya and Tunisia)
And if all the above were not enough, the PIP scandal was added to the list of issues that trouble the International Plastic and Aesthetic Surgery Community.
So, where does all this lead us??
- To the foresight of the Maya ancient tribe that the world will come to an end in 2012???
- Or, on the contrary, to the perception that the “ship of humanity” needs a change of course, so that it is not left stranded.
Despite my utmost respect for the advanced civilization of the Maya tribe, it is my belief that “we are going the wrong way”.
It is entirely up to the leadership of the European countries to solve their economical problems immediately and, at the same time, Southern Europe must learn to comply with the rules of a prudent management. The “Arab Spring” must quickly come to the day-after decisions for the benefit of its people. China, Brazil and all the otherrapidly developing countries must understand that they are not “de facto” almighty, but depend on the peace and financial progress of other countries.
Regarding the PIP case, the industry must respect the common interest, especially public health and focus on meeting the needs of the public and not risk the public’s health in order to make a larger profit.
Finally, we, the people, are obliged to visit our doctors on a regular basis, whether we have undergone surgery (even for aesthetic reasons) or not.
The example was clearly set by our International Confederation (IPRAS) which responded immediately and positioned itself effectively on the PIP issue, by sending its assessments to 101 National Associations and 37000 Plastic Surgeons around the world. The main points of the IPRAS statement were the condemnation
Dr. Gregory Evans, USA (ASPS President Elect) during his presentation at the 1st Chinese European Congress of Plastic,
Reconstructive and Aesthetic Surgery.

Issue 7 www.ipras.org IPRAS Journal 15
of the irresponsible companies, the recommendation to all doctors and patients to keep a calm status, the support to the healthy and serious industry of Plastic Surgery and the urge towards preventive check-ups of the patients.
Conclusion: All of the above complicated challenges can be confronted with a wise and willing attitude, but can also lead the “humanity ship” to much more “tranquil ports” with a social, political and economical complexion. IPRAS, in the last 3 months of 2011, came closer to its members and to the National Associations of nations such as China, Brazil, Russia and Italy.
The 1st Chinese European Congress of Plastic, Reconstructive and Aesthetic Surgery took place in Beijing, China, from October 27th to October 29th with the utmost success and attracted approximately 200 Chinese and more than 300 distinguished foreign Plastic Surgeons. Apart from the scientific and organizingsuccess, this Congress could certainly be characterized as a grand rehearsal for the IPRAS World Congress of 2015. Important conclusions were drawn, which will be utilized when the time comes.
Mr. Zacharias Kaplanidis (IPRAS Executive Director). IPRAS presentation during the 48th Brazilian Congress of Plastic Surgery.
From the left: Dr. Theodoros Voukidis, Greece (ISPRES founding member), Mrs. Katherine Lee Tai, USA, Prof. Marita Eisenmann- Klein, Germany (IPRAS President), (at the back) Mr. Fabian Wyss (Crisalix Chief Marketing & Sales Officer), (at the front) Dr. Josef Fedeles, (member of the Training and Accreditation IPRAS sub-committee, IQUAM member), Prof. Yilin Cao, China (President of CSPS, IPRAS Deputy General Secretary), Dr. Paul Ling Tai, USA, Dr. Pericles Serafim Filho, Brazil (member of the Scientific Advisory Board of
IPRAS), Dr. Ricardo Mazzola, Italy (IPRAS Historian).

16 IPRAS Journal www.ipras.org Issue 7
Mr. Zacharias Kaplanidis (IPRAS Executive Director), Mrs. Carol L. Lazier, USA (Staff Vice President and Chief Membership Officer American Society of Plastic Surgery), Dr. Phillip Haeck, USA ( Former President of ASPS) at the IPRAS booth during 48th Brazilian
Congress of Plastic Surgery
Furthermore, the IPRAS Executive Committee and the Board of Directors convened during that time, with a large participation of its members and important decisions were made, such as the 2012 Budget approval. Our President, Prof. Marita Eisenmann-Klein, our General Secretary, Dr. Nelson Piccolo, the Deputy General Secretaries, Dr. Yilin Cao and Dr. Ahmed Adel Noureldin, our Parliamentarian, Dr. Norbert Pallua and our Treasurer, Dr. Bruce Cunningham were all present at this very important event. Additionally, we must point out the impressive participation of the Brazilian Plastic Surgeons (approximately 60) and the Russian (approximately 70).
We would like to thank the Scientific and OrganizingCommittee of the Congress, Prof. Yilin Cao, Prof. Andreas Yiacoumettis, the greatly missed (due to a personal issue) and NIKE Med, Polytech, Crisalix and Silimed for its substantial contribution.
Immediately after China, we traveled to the other side of the planet, to Brazil, for the 48th Brazilian Congress of Plastic Surgery, which took place in the adorable city of Goiania, the homeplace and permanent residence of our General Secretary from November 10th to November 15th, Dr. Nelson Piccolo. With more than 2000 participants, Brazil proved once more that, not only is it one of the largest associations (2nd after USA)
From the left: Mr Alexey Kovalsky, POLYTECH Health & Aesthetics Director POLYTECH Health & Aesthetics Ukraine, Mr. Wilfried Hüser, founder and owner of POLYTECH Health & Aesthetics, Mrs. Katherine Lee Tai, USA, Dr. Paul Ling Tai, USA, Prof. Yilin Cao, China (President of CSPS, IPRAS Deputy General Secretary), Prof. Marita Eisenmann- Klein, Germany (IPRAS President), Mrs. Vivian Breinhild, POLYTECH Health & Aesthetics Director International Sales, EMEA, Dr. Albert de Mey, Belgium (member of the Scientific Advisory Board of IPRAS), Dr. Philippe Blondeel, Belgium (member of the Scientific Advisory Board of IPRAS), Dr. Pericles Serafim Filho, Brazil (member
of the Scientific Advisory Board of IPRAS).

Issue 7 www.ipras.org IPRAS Journal 17
in the world, but also that it is a great country on a scientific level and dedicated to more ethical values. For approximately 3 hours during the opening ceremony, important personalities were honored, such as Prof. Ivo Pitanguy, Prof. Baroudi and all the past Presidents of the Association.
It was the most beautiful and emotional Opening Ceremony that I have ever attended so far.
CONGRATULATIONS
Let us hope that all the other National Associations will follow this bright example of acknowledgement of personalities who have honored the field of PlasticSurgery in their countries with their achievements and ethos.
The truth is that I indeed experienced that same atmosphere again in Cesme, Turkey, during the Congress of the Turkish Association of Plastic and Aesthetic Surgery. It is truly a remarkable feeling.
Our President, Prof. Marita Eisenmann-Klein, Executive Director, Mr. Zacharias Kaplanidis and Assistant Executive Director, Mrs. Maria Petsa, represented IPRAS in Brazil and had the opportunity to speak to hundreds of participants on issues concerning the Confederation’s co-operation with the Brazilian Association and its members.
We thank them all for their absolutely wonderful hospitality, but especially we would like to thank the
President of the congress Dr. Carlos Calixto the Scientific committee Member of the Brazilian Society of Plastic Surgery, Dr. Pericles Filho, and, of course, our General Secretary, Dr. Nelson Piccolo and his truly beautiful family.
In mid-December (12th - 15th), the executive Director, Mr. Zacharias Kaplanidis, traveled to Moscow, where he met with members of the Russian Association of Plastic and Aesthetic Surgery and discussed the potential for organizing a workshop based on new developments in the field. Another great opportunityto exchange scientific knowledge with a great country.We would like to express our gratitude to the NIKE med Company for its hospitality and support.
Our last journey in these 3 months took us to Italy and specifically Rome (December 15th to December 17th), where we participated in a special scientific event with highlydistinguished scientists from the Italian and International World of Plastic Surgery, the 3rd International Conference on Regenerative Surgery. The President of the Conference, Prof. Valerio Cervelli, Dr. Sydney Coleman and Prof. Marita Eisenmann-Klein, Dr. Dan Del Vecchio and Dr. Gino Rigotti were just a few of the basic speakers of the Conference, which focused on the contemporary issue of Regenerative Surgery and Fat-Grafting.
After all the above, 2011 comes to an end. It has been a year with tremendous challenges for all to face, but with the appropriate response by the bodies of IPRAS and its mechanisms.
Zacharias KaplanidisIPRAS Executive Director
IPRAS Management OfficeZITA Congress
Mr. Zacharias Kaplanidis (IPRAS Executive Director) with Mrs. Liudmila Antonova, Russia (General Director of Nike-Med) and Mrs. Anna Pimenova, Russia (Nike-Med) addressing to Russian Plastic Surgeons concerning IPRAS benefits at the “NIKE-MED’s 15th Anniversary
Conference “Happy to be Together”.

18 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 19
Dr. Biggs: Dr. Rohrich, with your work as Editor-in-Chief of the official Journal of the American Societyof Plastic Surgery, you play what I, and many others, see as the most significant role in education of PlasticSurgeons in the world and thus, the course into the future of Plastic Surgery. For this, we are proud to designate you as our “PIONEER” for this issue of the IPRAS Journal.
We would like to use this interview as an opportunity for the 37,000 recipients of our journal, to get a better understanding of you and what is behind your drive…and how you see the future.
Let’s begin by your giving us a bit on your background.
Dr. Rohrich: I grew up on a ranch in North Dakota and did not speak English until the age of five. Ilearned early on, that the best way to succeed was to be focused, work hard, and that it does not matter where you are coming from, it’s where you are going that’s most important. This is indeed the ultimate American dream.
I did my Plastic Surgery training at the University of Michigan after completing Medical School at Baylor College of Medicine. I was highly motivated and stimulated by Dr. Mel Spira, head of Plastic Surgery at Baylor, who became one of my early Plastic Surgery mentors. At the University of Michigan, I worked with Drs. Grabb and Dingman and was vastly influenced by these gentlemen, whoboth subsequently died during my six-year Plastic Surgery residency. I will never forget their total focus and dedication to the excellence in Plastic Surgery. Dr. Dingman instilled a sense of duty and
to always do the right thing: he was amazing. I was strongly encouraged by Drs. Grabb and Dingman to write, to promote and to give back to Plastic Surgery, because we get so much from Plastic Surgery. There is always time to give back and to contribute to the advancement of the art and science of Plastic Surgery. I was then brought under the tutelage of Dr. Steve Mathes, who was my Chairman while I was Administrative Chief in Plastic Surgery at the University of Michigan.
These were highly formative years. I also spent a significant amount of time doing Pediatric andCraniofacial Surgery in my elective year. I spent time at Oxford University with Dr. Michael Poole doing Craniofacial Surgery and then met Drs. Marshac and Tessier, two outstanding Plastic Surgeons, in multiple trips to Paris. I also had the opportunity to spend time with Dr. Fernando Ortiz-Monasterio in Mexico City, in the pinnacle of his career.
At the Massachusetts General Hospital/Harvard in Boston, Dr. James May taught me to focus on excellence in all I do and always be better each day. This continues to be a valuable life lesson. I rapidly learned that Plastic Surgery, as a specialty, does not have its own organ, such as the prostate for Urology or the brain in Neurosurgery. Instead, we have our own innovation and that is something that has been the glue that’s actually been the foundation for our specialty. This has guided me in my role as A Plastic Surgeon and has motivated me to give back to this wonderful specialty as a teacher, as a Program Director and as a Chairman. We must teach the next generation to pursue excellence, be innovative, create an environment for innovation and to give back by
An interview with Dr. Rod Rohrich
P I O N E E R S

20 IPRAS Journal www.ipras.org Issue 7
doing, not only superb clinical work, but to give back by innovating and publishing in peer-reviewed journals, as well as presenting our work worldwide. My interest in writing began as a medical student at Baylor College of Medicine, while working with Dr. Mel Spira.
Dr. Biggs: I certainly agree with you about Mel Spira. I met him in the emergency room the afternoon of my first day as a resident at Baylor in Houston. I wasthe Surgery resident on call and he was the plastic surgery resident on call, on his first day workingthere, like me. We became great friends then and still are. He will always be my number one mentor….but to get on with the interview: tell us about what you’re doing in Dallas. You run probably the most proficient and productive training programs in theU.S. and even the world. Tell us about it.
Dr. Rohrich: You can always become and be better, no matter how good you are at what you do. It is helpful always to surround yourself with people that have the same philosophy. I find thatthe key to success is in picking great people, both in residency and faculty, that are better than myself. You have to be very selective and selfless in doingso; it demands conducting a regular 360-degree re-evaluation of yourself, so you can re-focus and rethink on areas which are important. You have to be focused long-term. For example, at UTSW, we have taken a small division of Plastic Surgery with a couple of faculty and staff, to a staff of over one hundred and thirty, with twenty full-time faculty, nine part-time faculty, six residents per year and multiple fellows in Craniofacial, Hand, Cosmetic, Micro and Breast Surgery and research. We have multiple NIH grants and one of the most largely productive clinical and academic faculty departments in the U.S. Becoming a Department of Plastic Surgery at UT Southwestern was pivotal and has provided us with a basis for growth and an example for other divisions and departments around the country to succeed as well.
How can we become better at what we do in Plastic Surgery? An “expert” is someone who is focused on excellence through practice, focus and dedication for over 10,000 hours. This type of training and commitment holds true whether you want to be a concert pianist or Plastic Surgeon. If you want to be an expert in what you do, you have to focus on it
and dedicate a significant part of your career to thiseffort. The time to start doing this is now, while you are a young Plastic Surgeon.
As I mentioned previously, I spent my formative years growing up on our ranch in North Dakota, with limited resources, but my parents wanted a better life for all of us. They imparted to my two brothers and me a tremendous work ethic and that one must lead by example, like my parents did for us. I certainly never ask a faculty member, resident, or anyone else to do anything I would not do myself. It keeps me grounded as well. One must lead by example to become a role model or mentor. We are influencedby and pattern our lives after these role models and mentors. I certainly remember one of my earliest role models, besides my parents, was one of my science teachers, Mr. Schimcke, who challenged me to find a new way to study Mendelian Geneticsusing fruit flies. He allowed me to do things I hadnever done before and to do them by myself. Just remember that you have to aim high in life if you want to succeed. Therefore, aim very high because you will get where you aim. If you don’t aim high, you’ll always get there, too, and you will not be happy for aiming so low. You must aim higher than you think is attainable and it will get you there. A good work ethic is strong encouragement both at home, at school and in your personal life and we certainly try and gender that into our residents.
Coming from a high school class of twenty four students, where I was one of the only ones that actually finished college and went on to highereducation, helped me focus on setting high goals, working hard, and pushing myself to a higher level. That is what makes you succeed in life.
Dr. Biggs: For the past few years I’ve heard you speak passionately about Evidence-based Medicine. Please bring us up to date on that matter and how it’s being reflected in the Journal:
Dr. Rohrich: I think one of the epic changes in Medicine and in Plastic Surgery is that we are owning our specialty, as we become more evidence-based. Plastic Surgery has been an “expert-based” specialty, where experts have driven the specialty through innovation. These experts are incredibly valuable and continue to be, but we must now go to the next level of excellence. That next level

Issue 7 www.ipras.org IPRAS Journal 21
of excellence is that of evidence-based medicine (EBM), where we must prove that what we learned as experts can truly be done, not only by ourselves, but by others and can be shown to work in both a prospective and randomized manner. Whether it is a product, a technique or a technology, it must now be shown to truly work sufficiently, in a scientificmanner. That is the next level of excellence we must achieve. Since becoming Editor-in-Chief of the journal of Plastic and Reconstructive Surgery in 2005, we have pushed the technological envelope, evolving the journal from being a print-only version to being online in all aspects (including the peer review process to the upcoming development of the iPad app). Today, you can see, feel, and look at our videos in the PRS journal instantaneously. That is the natural evolution. Innovation, aiming high and seeking new challenges brings you higher caliber articles, as well as a higher caliber type of evidence-based Plastic Surgery, which will help drive Plastic Surgery to a better place in Medicine. The bar in Plastic Surgery is being raised and we are pushing that bar with evidence-based medicine. We need to push our entire specialty of Plastic Surgery to come and join us, to make sure that we truly are and remain at the cutting edge, not only of innovation but that of EBM, so we can show the rest of Medicine that what we have done and what we continue to do is evidence-based.
So, as a Plastic Surgery leader in the United States, I think it is important for us to show and lead by example, not only by our journal, but now in our clinical practice. EBM is rapidly changing how we practice Medicine and how we practice Plastic Surgery. It will make us better. The goal is to provide a foundation for doing evidence-based Plastic Surgery. There is no better way than mandating that Plastic Surgery programs become their own departments; this must be solidified, sowe can allow for true innovation to occur, separate and apart from General Surgery, which, I think, is so critical. We are now, and have been for a long time, our own specialty. Because EBM has proven to be a highly effective methodology, the American Society of Plastic Surgeons and the American Society of Aesthetic Plastic Surgery, along with other Plastic Surgery and related specialty journals and societies, convened at the first Plastic Surgery
Evidence-Based Medicine Summit in Colorado Springs, Colorado in August 2010 (see Figure 1). At that meeting we strongly encouraged all of the journal editors to work with the ASPS and the journal of Plastic and Reconstructive Surgery to have a single grading system for evidence-based medicine, similar to what we use in PRS, so we can move forward together. A year later, in May 2011, at the Plastic Surgery Journals Editor Round Table Meeting in Vancouver, Canada (see Figure 2), PRS was joined by other international Plastic Surgery journals and we all agreed to work on establishing uniform global EBM standards and Levels of Evidence grading systems. At the Vancouver meeting, we agreed to invite all of the world editors of Plastic Surgery journals, as well as those of our other related specialties, in Facial Plastic Surgery, Dermatology, Oculoplastic Surgery, to attend our next EBM strategic planning meeting in Colorado Springs in July, 2012. EBM is for Plastic Surgery worldwide, and Plastic and Reconstructive Surgery stands as an advocate for unified, global EBMstandards among all Plastic Surgery and sister-specialty journals.
Dr. Biggs: How do you see the future of Plastic Surgery?
Dr. Rohrich: The future of Plastic Surgery is very bright. It lies in innovation, autonomy, becoming departments, developing and expanding evidence-based medicine through the entire world, and developing a uniform platform for the language in space medicine. We will focus on where we are going to take EBM in Plastic Surgery in the future, how we will become better: better in what we do, better in our practice and better in improving EBM, because that is our future. After all, the goal is to improve patient care, drive innovation, drive cost efficienciesand only then can we say we have given our best, given back and left the world a better place, both for Medicine and for PLASTIC SURGERY. That is my goal and that is what I will continue to do.
It pleases me to get this message out to your 37,000 recipients and I want them to join me in this adventure of the EBM world of Plastic Surgery. It will be a better place for all of us as Plastic Surgeons and for Plastic Surgery as well.
Dr. Biggs: Thank you Dr. Rohrich
22 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 23
R I S I N G S T A R
Dr. Biggs: Congratulations on being chosen as our RISING STAR for this issue of the IPRAS Journal. As you know, we select someone under the age of 45, who has shown great promise in their pursuit of excellence in Plastic Surgery. Tell the readers a bit about yourself. Begin by telling us your background and your education.
Dr. Kotti: I was born in 1977 in Tunisia, a country of 11 million people and 80 plastic surgeons. My primary education was undertaken there, as well as my medical education. I graduated in June, 2000, from the Medical School of Tunis and followed that by a broad medical/surgical internship for one year. From 2002 to 2006 I did a residency in Plastic Surgery and completed a dissertation on “Plastic Surgery for the Management of Pressure Sores”. I graduated Summa Cum Laude from the Tunisian Public Health Department and the Tunisian Higher Education, Scientific researchand Technology Department in Plastic Reconstructive & Aesthetic Surgery (October 2007) and made the decision to move to France, where I continued my studies. I worked in Nice and Paris in services including breast reconstruction, maxillofacial surgery, head and neck surgery, and general Plastic Surgery, including Aesthetic Surgery. I spent most of last year (to February, 2009) with Dr. Claude Lassus in Nice. My studies and work in France allowed me to be Certified from the FrenchCollege of Plastic Reconstructive and Aesthetic Surgery (November 2007) and, in May 2008, by the European Board of Plastic Reconstructive and Aesthetic Surgery.
Dr Biggs: And then you returned to Tunisia ?
Dr. Kotti: Yes, and in 2009 I joined the “Salah Azaiz” institute (an anti-cancer centre) and have become Head
An interview with Dr. Bouraoui Kotti
of the unit of Plastic Surgery in the Surgery Department.
Dr. Biggs: What Societies do you belong to?
Dr. Kotti: Tunisian Society of Plastic, Reconstructive, Maxillofacial, and Aesthetic Surgery (STCPRMFE), ASPS, SOFCPRE, and ISAPS of which I’m National Secretary.
Dr. Biggs: I looked over your list of publications and presentations, over twenty in all, and fifteen posters.I noticed you have run the table on topics from digital reattachment to abdominoplasty and blepharoplasty, breast reduction and reconstruction, to extensive maxillofacial reconstructions, and to burns. That’s a lot of production for a young man and very impressive.
Dr. Kotti: And there is a lot more to do
Dr. Biggs: Tell me about that. What do you predict and where do you see yourself in five years?
Dr. Kotti: I see myself still in pursuit of better ways to do more for people. My interest lies more in reconstruction, but with an increased attention to its aesthetic aspects. My great hope is that the political situation in Tunisia will be such, that I can expand my research capabilities and impart progress made there into clinical applications.
Dr Biggs: Thank you Dr. Kotti. Your great hope is shared by members of our Plastic Surgery family around the globe and this is why I so often say that “the bonds that unite us are greater than the borders, boundaries, and languages that divide us”
Again, congratulations on being chosen our “RISING STAR”.

24 IPRAS Journal www.ipras.org Issue 7
Dr. Biggs: Dr. Mazzola, to those of us who have been on the Plastic Surgery scene for a while you are a legend, but this is an International Journal and many of our readers are somewhat new to the field, so please give us a review ofyour educational and training background.Dr. Mazzola: I obtained my medical degree at the University of Pavia in 1967, magna cum laude. I passed my Board examination in ENT in 1970 at the University of Ferrara and my Board in Plastic Surgery at the University of Milan in 1974 (head Prof. G. Sanvenero Rosselli). I became an Assistant Professor of Plastic Surgery at the University of Milan in 1971 and I am currently Professor for Plastic and Reconstructive Surgery at the Postgraduate School of ENT, and Maxillofacial and Plastic Surgery at the School of Medicine of the University of Milan.Dr. Biggs: Tell us about your Foundation.Dr Mazzola: In April 1975, I established the “Fondazione G. Sanvenero Rosselli” for Plastic Surgery, as a tribute to my late uncle Gustavo Sanvenero Rosselli, founder of Plastic Surgery in Italy. The institution promotes various forms of teaching, fulfilling a continuous postgraduate trainingprogram, by arranging meetings, seminars and courses in the field of Plastic Surgery. Directed by a Board of Trustees,the Fondazione has coordinated more than 150 meetings and seminars and organized 48 theoretical and practical courses, with live surgery over the years. I am currently the Vice-President of this Institution. The Fondazione houses more than 4,000 books and boasts certainly one of the most important rare book collections on Plastic Surgery in the world. We have volumes dating from 1490 onward. Dr, Biggs: Tell us about your professional life.Dr. Mazzola: I am a Founding Member, Secretary General (from 1995 to 2001) and President (from 2005 to 2006) of the EURAPS (European Association of Plastic Surgeons). I was Secretary of the Italian Society of Plastic Surgery (SICPRE) from 2001 to 2004, and am a member of over 15 National and International societies, among them the prestigious American Association of Plastic Surgeons (AAPS).Dr. Biggs: How about presentations and authorships?Dr. Mazzola: I have participated in 450 invited panels, lectures, conferences and courses at National or International Meetings and Congresses. I have organised 52 Congresses
Dr. Riccardo F. Mazzola
and Courses.I’ve been honoured to be the Keynote speaker in numerous International Congresses, and was awarded the Maliniac lectureship at the 2006 ASPRS Congress in San Francisco, USA.I am the co-Author of 3 textbooks (“Craniofacial Malformations”, Churchill Livingstone 1990; “Velopharyngel Incompetence”, Masson 1995, in Italian, “Fat Injection, from Filling to Regeneration”, Quality Medical Publishing, 2009), 12 book chapters and 112 publications, 38 of them in peer reviewed scientific journals.Dr. Biggs: What are your primary surgical interests now?Dr. Mazzola: My primary interests include Cleft Lip and Palate, Head and Neck reconstruction, Nasal Reconstruction, Fat injection, Rhinoplasty and History of Plastic Surgery.Dr. Biggs: Where do you see us going in Plastic Surgery?Dr. Mazzola: That is a good question, because I am both optimistic and, at the same time, somewhat despondent. I’m the latter because Plastic Surgery, by not being independent, has less opportunity for research. Modern day Plastic Surgery began with a collection of ENTs, General Surgeons, and several others who had a common talent: innovation. Innovation was necessary to deal with the massive wounds resulting from World War I, wounds never seen before, because these unfortunate victims were the beneficiaries of medicine whichwas advanced enough to keep them alive but still lacking in skills to reconstruct them. My despondency lies in the fact that our lack of independence limits us in our quest for advanced solutions plaguing modern surgical problems.My optimism lies in the wonders that await us. These wonders include wound healing, tissue regeneration, concepts of neurogenesis, and many others.Dr. Biggs: Do you have any advice for our younger readers?Dr. Mazzola: Yes. Go back several centuries and see how brilliant minds were dealing with some of the same problems we are dealing with now. See how Leonardo Da Vinci understood anatomy, how concepts of wound healing have evolved. Study the Masters and extrapolate their creative thought processes into your own.Dr. Biggs: Thank you Dr. Mazzola. You truly are a Senior Ambassador for IPRAS and for physicians of all types.
S E N I O R A M B A S S A D O R
Issue 7 www.ipras.org IPRAS Journal 25
© 2
011
PO
LYTE
CH
Hea
lth &
Aes
thet
ics,
Ger
man
y.
26 IPRAS Journal www.ipras.org Issue 7
H U M A N I T A R I A N W O R K S
Developing Islamic countries are quiet and peaceful areas, most of the time. In some cases however, the work of humanitarian teams is not as easy as that… The following lines try to analyze the specific problems thatcould be encountered in some places, where the religion is dominating and ruling the public life and the cultural habits in such a way, that things are becoming so different and thus more difficult to understand for an occidentalmind. And after all, if we want to help them, we first haveto understand them….
SPECIFICITY OF WORKING CONDITIONS FOR THE HUMANITARIAN TEAMS
The teams are faced, most of the time, with a triple specific deal: the religion, the women’s condition and thecorruption …
The religion
• About Islam: Islam is a beautiful religion, spread all over the world. However, the territory where it is the
predominant religion geographically extends, more or less horizontally, from the western part of Africa to the Far East end of the southern Asian continent, including Malaysia and Indonesia. Historically and theologically, there are several “families” of Islam, such as Shiites, Sunnites, Kharijists… all of these groups coexist in a more or less complex harmony in the many developing countries, where humanitarian teams are performing surgical camps or missions.
Moreover, Islam is, most of the time, a state religion and therefore this religion often becomes a real political-religious rule.
In fact, there are, as far as geography and culture are concerned, several Islams… Because of local political and cultural factors, Islam in Maghreb is not exactly the same as the one in Indonesia and is also different from the Islamic beliefs of central Asia or Turkey, for instance.
The medical and surgical humanitarian teams working in different parts of the world will be faced with a “soft” or “moderate” Islam in some places, or with a “hard” or “strong” Islam in other countries…
• The Muslim population: it seems that the actual number of Muslims in the world reaches approximately 1.5 billion people. Etymologically, the word Muslim comes from the Persian “Musilman”, plural of Musilm, whose root is the verb “Aslama” (to be resigned, to be submitted … to God, of course). This great number of people and the strength of their faith put Islam as one of the major religions in the world, especially in the poorest parts of the world.
• Their position towards illness and medical care is not identical everywhere. Muslims of the world, though they cannot really read and deeply study the enormous amount of rules of the Koran, are very faithful and, most of the time, respect the 5 main rules (five prayersa day, pilgrimage, Ramadan…) As far as illness and medical care are concerned, there is, in fact, no
How to conciliate religion and humanitarian surgery
in Islamic developing countries
A man in Kabul…
Dr. Christian Echinard President, HumaniTerra International
President, IPRAS Foundation

Issue 7 www.ipras.org IPRAS Journal 27
specific rule. For some of them, illness is consideredas a punition of God and requires little care, for some others, on the opposite, it is something that must be treated absolutely immediately.
The women, of course, have a special status… In some remote places they should not be touched by a male doctor… The problem is that, very often, there is no female doctor… This is very frequently the case in Afghanistan, where women die because their husbands refuse the help of a male doctor, especially for delivery. This is, of course, an extreme point of view. In most cases things are much simpler and the real rule in the Islamic religion is that, when there is a necessity, women can be treated by any male doctor, Muslim or of any religion. Necessity creates the law and the rule… a safe and good advice…
The women’s condition: female mortality creates a terrible disorder
• Gender mortality: this is a real economical and demographical problem. In most of the Islamic developing countries, the female to male ratio is, on average, 900/1000; It is the opposite in occidental areas: 100 females for 90 males in Europe, whereas in Bangladesh and Pakistan the ratio is 100 women for 106 males. Another interesting sign is that, in those two countries, the average duration of life is the same in men and women (56 years); in Europe and America females live approximately ten years longer than males…
This over-mortality in the female population is due to several factors, such as the way of life, the number of children, the amount work done by women… but also due to the high maternity mortality and the increased level of violence towards them.
• Materity mortality: in Afghanistan, one woman dies every 21 minutes due to delivery problems! In central Asia Islamic areas, 2000 female patients die in 100 000 births! In Europe the average is only 10-20/100 000.
• Violence towards women is also an important cause of female over-mortality.
It can be in the form of domestic and marital abuse. It reaches 50% in some of these countries, the champion being Bangladesh, where more than one wife out of two is regularly beaten. In Pakistan, 300 women are killed every year by their husband, brother or son, in the name of honor.
Among the worst crimes, forced or induced suicides by flame are very frequent in Iran, Afghanistan(especially the Herat area), Pakistan, Iraq, but also in Africa (Zimbabwe, Egypt…)
In Pakistan and Bangladesh, there are many acid attacks against women, committed by jealous or unsatisfiedhusbands. This type of acid burn on the face leads to extremely severe contractures and real disfigurations ofthe wives. Two NGOs have been created to fight againstthat, the “Acid Survivors Foundation” ran by Valerie Khan in Pakistan and Monira Rahman in Bangladesh.
Apart from marital aggressions, these gender crimes can also be the result of abusive punishment or usual violence such as stoning, rape, excision, any kind of mutilation (hand or nose…), sexual slavery and forced pregnancy.
Moreover, many rapes have been committed in these countries as a war weapon, in order to humiliate the enemy. In Kuwait, over 5000 rapes were committed against the local women by the Iraqi forces, when they invaded this country in 1990. In Algeria, between 1995 and 1998, rapes were committed in the name of the Jihad in order to render the females impure and dishonored…
Women from the mountains in Afghanistan

28 IPRAS Journal www.ipras.org Issue 7
The corruption and … the narcotics business
• Corruption: last year, the UNDP (United Nations Development Program) classified Afghanistan atthe 155th rank out of 169 countries in the world for development and economy. Meanwhile, the NGO “Transparency International” stated that this country was placed third as far as corruption is concerned !
• Narcotic trafficking: most of the time, corruption isconnected to drug trafficking … Afghanistan is by farthe first opium producer in the world; before the Talibanperiod (during the soviet domination) production was estimated at 2500 tons per year. In 1999, at the end of the dramatic Taliban government, it reached 4600 tons per year, proving that they did not do anything against drug trafficking… In 2007, under the currentgovernment, opium production in Afghanistan nearly doubled, and was evaluated yearly to 8200 tons! And this was of course very much to the benefit of thepolitical elite. The resulting gain from opium traffickingis probably one billion dollar per year. One gram is sold in the country about 2 or 3 dollars. It is re-sold in Europe or America for 70 dollars. At the same time, we found that it is still difficult to find narcoleptics foranesthesia in a hospital in Kabul or Herat …
• Position of the medical team faced to this problem: this shows how the task of the humanitarian medical teams can be difficult in such countries… corruption mustnot touch our teams. Everything possible must be done in order to avoid any kind of collision with anyone. And everyone must be aware that the manipulation of the team about this problem can be very easy and can be a source of conflicts…
WHAT MUST BE THE BEHAVIOR OF THE HUMANITARIAN TEAM?
In the face of such a situation, the behavior of the foreign surgical team must comprise of understanding and adaptation, as long as we keep in minds the ethical
rules of our action. We must understand what they are and what they need and therefore respect their identity. But we must never betray our principles. We must adapt them to the local situation. The most important rule is to respect three important things: the political and religious authorities, the local medical teams and, above all, the patients whom we are suppose to treat.
Respect of the political and religious authorities
• In every one of these countries the humanitarian teams, or their delegates, must try to have a meeting with the local or regional political authorities (governor, president of local assemblies, Shuras…). A complete agreement must be established before any action is taken on the field. This makes things much easier for the rest of themissions and always clarifies the situation.
• Mullahs and religious assemblies should also be contacted, in order to explain to these dignitaries what the aim of the mission is and get a complete approval from them. This is particularly useful when a NGO is working on a prevention campaign, in which women are involved, such as campaign against suicide by flame or against acid attacks. It is very important todiscuss with them, explain to them the work that will be done, ask their opinion, see how they can help… Communication is extremely important and, with the consent of the Mullahs, the behavior of men and women in the area will be very much in favor of the NGO. On one hand we must absolutely avoid being considered as neo-colonizers by the local population. On the other hand, when we are supposed to deal with situations related to women, we must avoid any kind of frustration or dishonor from the men. This is also the reason why it might be useful to work in collaboration with a local NGO.
Respect of the local surgical teams
• Most of the time, the NGO surgical team is totally welcome by the local medical teams, which are
Teaching women rights in Bangladesh
A men session during the anti self immolation campaign

Issue 7 www.ipras.org IPRAS Journal 29
very often requesting this collaboration. Sometimes, however, there is no local medical team and the problem is different… Sometimes the local team is not really expecting the arrival of a foreign team of surgeons and, therefore, is not in complete empathy with the NGO and vice versa…
In any case, there must not be any rivalry with the local medical group. The NGO is there to take care of the patients together with the local surgeons and to teach them how to do better and how to improve the quality of surgery and hospitalization. Religion must not be a brake to relationship. The NGO team must absolutely respect the faith of the local host: prayers during the day, Ramadan period, alimentary habits, time and menus of the meals…
There usually are few women surgeons or anesthetists in these countries. However, in some of them, when we have to work or train a female doctor, care must be strictly taken not to disturb her in her religion habits (no direct contact, no rudeness, respect of the veil, the hidjab or the burka…)
Moreover, there must be complete cooperation between the two teams, with respect, friendship, harmony and mutual comprehension. The NGO teams must be very humble. Respecting the religion and the culture of our medical partners is essential. They must become friends and feel a complete cohesion between the two teams.
In many cases, we have invited them to come to Europe (France in particular) for a more complete training in surgery or hospital management, with their expenses covered. For instance, HumaniTerra has completed the medical or surgical training of 12 Afghan doctors in France for two months or more. In each case, we paid attention to their religion and faith when they were in our universities or hospitals.
• Nurses and paramedical teams must also be treated with a great deal of deference, respect and kindness. This does not exclude friendship and convivial behavior. We all need that. Again, total respect of their religious convictions must be observed, particularly concerning the the female dresses or the veil that they can wear on their head. On the same topic, it seems normal to us that our own nurses, female paramedics or doctors wear a veil in public or when they work at the hospital.
Respect of the patients
• A veil for the women of the NGO team is, as mentioned before, an important thing if our nurses and women surgeons want to be in perfect harmony with the Muslim female patients. It makes the patients more confidentand it becomes easier to take care of them. They will indeed appreciate the fact that we respect their beliefs
and habits (showing that we are open-minded people, which, at first glance, is not evident to them) andtherefore will be, in return, very open to our treatment. Culturally, philosophically and for religious reasons women (and men sometimes) are very shy and pudic. Some of them are naturally modest and chaste. Others are extremely reluctant to be clinically examined and to be shown half naked … More often, the reason for this is that their husband strictly forbids this. Some men are totally opposed to the fact that a male doctor (Muslim or non-Muslim) can even touch their wife. In some parts of Afghanistan, they would prefer that the pregnant mother dies and sometimes the baby too, instead of consulting a male doctor or gynecologist, in case of emergency or imminent delivery! Fortunately, this is less and less often the case and this behavior can only be seen in some remote areas, for instance high in the mountain. In Chagcharan, 3200 meters high in the Afghan mountains, we have seen that it sometimes took two or three days for a mother to reach the nearest hospital on her own means…!
In any case, the attitude of the surgical team must pay attention to all this and always respect the chastity and modesty of the patients.
• We must always show great professionalism: surgical NGOs are considered as a type of ultra specialized NGO. People constituting the team are very often senior surgeons or very well trained practitioners. And this is always the case. Our attitude towards the patients is to prove to them that we are good professionals. Nothing is worse than doubt. If we are top level at home, we must also be top level in missions. Good training of the local doctors can only be achieved under these conditions.
A young woman after a suicide attempt by flame
30 IPRAS Journal www.ipras.org Issue 7
They must be confident. Security is one of the mostimportant things. We must not appear as arrogant cowboys invading the country, and giving orders. Our role is to do the job as well as we do at home, or better, although the conditions are often much more difficult,due to a precarious situation or a lack of modern material. Of course, professionalism goes together with safety… “Safety first” is one of the phrases that wemust keep in mind. A small number of operations with good results and good functional outcome is always better than many operated cases with bad or mediocre results… bad results are always interpreted and felt as bad work or, sometimes, as a humiliation.
PROVIDE AN ADAPTED HELP: Considering all these parameters… what can we do…?• Build or Rebuild and help them to work in good
conditions: very poor countries, often belonging to the Islamic area, have rather seldom good hospital accommodations. There is often a lack of hospitals or surgical wards, a lack of well trained surgeons, a lack of paramedics…
A good occidental NGO must be aware of that. Therefore, it is important for them to restore or even to build specific wards for surgery. Reconstructivesurgery in particular is not well developed in these countries. Our goal must be to help them to get new buildings. In Islamic countries we try to build or restore specific departments where physically abused women
can be treated. HumaniTerra, for instance, has built a pilot burn center, in which women have a completely separate ward from the men, just as if we had build two burn centers… Physical rehabilitation is also done in a specific area.
We have also been the leaders and initiators of the HOT program (Herat Operating theatre, 6 very modern operating rooms), together with the help of the Japanese and Italian cooperation. This allows women to be operated in conditions as good as the men…
An adapted help is, to try to study what will fit the bestto a specific situation, integrating the Islamic laws andhabits… To women, treatment is given by women.
• Prevent them from bad habits and help them to get a better life: are we allowed to change the rules…? Certainly not… just because we are foreigners there is no reason why we should try to make new laws. Nothing is justifying the fact that democracy is better for countries that are used to live under tribal laws… why would we interfere…? And after all, is Islam compatible with democracy…? This is a question difficult to answer, although Turkey, for instance, is agood example showing that it is possible… on the other hand, the Islamic countries of the “Arabic Spring” ( Libya, Tunisia, Egypt…) have also shown proof of that… but we still don’t know what the outcome will be in a few months…
However, even if we do not feel authorized to give them lessons in life, the role of a NGO is to try to induce a better way of life, a better equity between women and men, a more reasonable sharing of knowledge, an equal chance of happiness for everyone and dignity for every human being.
Towards this aim, we have set up several Campaigns for the dignity of women. In Afghanistan Two campaigns were organized, in cooperation with the local NGO “Voice of Women”, in order to fight against thishorrible endemic disaster of women forced to commit suicide by flame. During the first campaign, Lecturesand discussions were organized for Women and for men, separately, pointing out the unjustified reasonsof the crime, the expansive, long and painful treatment and the horrible outcome with so many sequelae … after one year, the percentage of suicide by burn in the Herat Province, decreased from 43% of the total amount of burn patients to 11%... very good results, but still not sufficient.. A second campaign is currentlyunder way with TV videos and meeting, aimed at an even larger amount of people.
In Bangladesh, a campaign against acid attack is also actually being set up, for the numerous women attacked by jealous men…
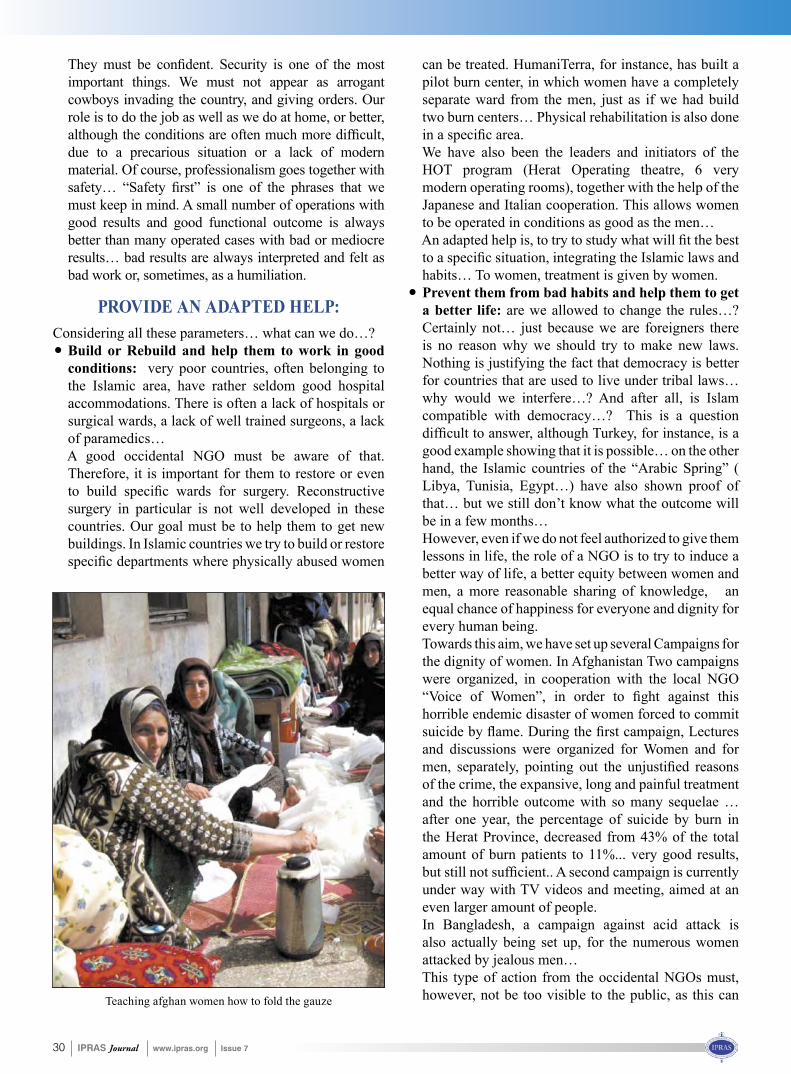
This type of action from the occidental NGOs must, however, not be too visible to the public, as this can Teaching afghan women how to fold the gauze

Issue 7 www.ipras.org IPRAS Journal 31
lead to local problems with the NGO. This is a reason why actions should only be performed after a total agreement with the political and religious authorities. They should also be carried out mostly by local NGOs, under the control of the occidental NGO.
• Provide them with better surgical care and help them to survive: In the remote areas of some Islamic countries, illness or trauma are sometimes still considered a normal thing or a punishment of god (remember that the word Islam comes from the word Aslama, “to be submitted”…) In the poorest Islamic
countries, we see a lot of congenital malformations, traumas, awful burns, post-delivery problems… Our goal must be to reach these isolated people who cannot pay for a hospital stay and get in touch with them, wherever they are.
Illness must not be considered for them as a malediction or a fatality anymore. The poorest of them don’t even know that they can be treated. Burn contractures can be treated, acid attacks must be cured, post delivery vaginal fistulas must be operated, care should be takenof cleft palates at any age, in any of these remote areas… whatever the religion is, whatever the strength and the power of religious fanaticism is…
Together with its partner NGO, Friendship, HumaniTerra is providing high quality proximity surgical care in northern Bangladesh, where the Chars population cannot move from their semi-floodedislands, using two river hospital boats, on which they can be operated in good conditions. This hands-on surgery, in the small Islamic villages, is also performed in Pakistan, and southern Bangladesh, close to the sea. Very soon it will be also done in the Bengal gulf, thanks to a new sea hospital boat , the former “Rainbow Warrior”, that has actually been transformed into a surgical boat, on which every NGO teams of SHARE (Surgical Humanitarian Aid Resources Europe) and HUGS ( Humanitarian Union for Global Surgery) will be able to operate all year long.
Afghan women outside the mosque
Consulting the local assembly in Asad Kashmere , Pakistan

32 IPRAS Journal www.ipras.org Issue 7
The ConceptIt was during the visit of Dr. Rajeev B. Ahuja, to inspect the newly introduced burn unit at the Tanda Medical College, on behalf of the Government of India, that the idea of having a surgical camp at this location was mutually discussed between him and the Principal, Prof. Anil Chauhan. The Principal showed enthusiasm for a free Plastic Surgery camp, as the area has a lot of poor patients requiring Plastic Surgery and such facilities are not available in the region, including the college.
The LocationThe historical town of Kangra nestles in the valley of Himachal Pradesh. For the believers it is a place of pilgrimage, devoted to the Goddess Parvati, the consort of Lord Shiva. Over the years it has seen numerous invasions, a grim reminder of its strength being the Kangra Fort, which sits atop a steep 1000-foot cliff, rising like a phoenix from the river bed. Kangra is derived from word “Kanghara” which means “doctors who repair ears”. As per hearsay, in ancient times, this town was famous for its Plastic Surgeons. The RPG Medical College is a fledglingCollege, which has only recently introduced post-graduate courses. The College is a boon for the city and the surrounding areas, which have scarce health care.
The PlanningDr. Ahuja requested Dr. Chanjiv Singh (Chairman, Humanitarian Committee, IPRAS) from Jalandhar to visit the college and issue a feasibility report. Dr. Chanjiv visited the college in June 2011. He assessed the patient load and the facilities available for the venture. The Principal deputed Prof. Sanjeev Sharma (General Surgery) to co-ordinate the planning of this camp with Dr. Chanjiv.Dr. Ahuja, as Secretary General of IPRAS (Asia-PacificSection), invited senior surgeons from the Asia- Pacificregion to volunteer for this humanitarian mission. As this
was the first mission of its kind in the area and the Hospitalis a governmental facility, the organizers went through a lot of red tape to make arrangements for the camp.The team co-ordinated with the Lions Club of the nearby town of Dharamshala to publicize the event and to accomodate the visiting team. The Lions Club did extremely well in sending out information to district hospitals in the region, and publicized the camp to the public through banners and posters. Their efforts landed an overwhelming number of patients for surgery at the camp.Dr.Chanjiv Singh visited the college again in July to oversee the boarding and lodging arrangements, to co-ordinate with the hospital authorities for the provision of supplies, to discuss with the anaesthetists and to co-ordinate with the Lions Club.
The TeamsThe Indian team, lead by Dr. Rajeev B. Ahuja, comprised of other senior Plastic Surgeons, Dr. Vimla Rajan, from New Delhi and Dr. Chanjiv Singh from Jalandhar. Senior residents from Lok Nayak Hospital, New Delhi (Dr. Dhirendra Suman, Dr Vinish Shrivastava, Dr Manish Chopra); DMC & Hospital, Ludhiana (Dr. Manish Sehgal); Amandeep Hospital, Amritsar (Dr. Seema Mittal, Dr.Sandeep Kansal); and PGIMER, Chandigarh (Dr. Anil Kumar, Dr.Raja Tiwari) had volunteered for the camp through their respective Heads of Department. OT assistants Mr. Harpreet, Mr. Gurnam Singh and Mr. Vikramjit Singh volunteered from DMC Ludhiana, Civil hospital, Jalandhar and Amandeep Hospital, Amritsar, respectively. The staff of the College itself worked around the clock, beyond their duty time to assist in the camp. The team from Thailand was headed by Prof. Apirag Chuangsuwanich from Mahidol University, the President of the Association of Plastic Surgeons of Thailand. The team consisted of a Plastic surgeon, an Anaesthesiologist, an OT assistant, nurses and volunteers and included
IPRAS (Asia-Pacific Section) organized a free Plastic Surgery Camp
at the Dr. Rajindra Prashad Government Medical College of Kangra, at Tanda (Himachal Pradesh) India from 21st to 28th (31st)August 2011.

Issue 7 www.ipras.org IPRAS Journal 33
Mr. Sirichai Kamnerdnakta, Mr. Thara Tritrakarn, Mr. Poom Tritrakarn, Mrs. Pensri Noocharoen, Ms. Thitima Channawa, Ms. Susiri Charloenmit, Mr. Thanatpant Manosittisak and Ms. Panipak Vareevanichaphan.Dr. Fong Poh Him from the Institute of Plastic Surgery represented Singapore. The foreign teams provided their own instruments and materials. All overseas team members covered their own expenses of travel to the surgical camp site.
The MissionThe first day,August 21st, was used to inspect all facilities,instruments, autoclaving procedure, and instrument turnaround after surgery, and the number of theatres that could be available. An informal inauguration of the camp
was done on the 22nd, with the visitors being welcomed by the Principal and the President of the Lions Club, Mr. P.C. Dhiman. Although patient registration had started in July, the formal OPD for short-listing patients for surgery and registering fresh patients started in the morning of August 22nd. In spite of bad weather and constant rain, the OPD was bursting at the seams with the crowds. More than 140 patients were examined on the first day ofthe camp. Nearly 100 more patients were seen during the next few days. Seeing the gush of patients, it was decided to have four OT tables, as there were enough surgeons and supporting staff. Dr Sudarshan Choudhary (HOD Dept. of Anaesthesia) and his senior colleague, Dr Shelly, joined with Dr Thara’s team and anaesthetists from Delhi to manage anaesthesia for the four tables.
Camp inauguration in the hospital corridor.
Team members

34 IPRAS Journal www.ipras.org Issue 7
The surgeries started on the 23rd and continued until the 26th. A total of 91 surgeries were performed. The OPD continued seeing the patient inflow on all days.The hospital authorities admitted all patients free of charge and also did not charge for the investigations. The documentation and case recording was also done on the hospital stationery as per the prescribed norms.The spectrum of surgeries included patients with severe post-burn contracture and deforming disabilities, cleft lip and palate, syndactly, deforming scars, non healing ulcers etc. Thirty-three beds were made available by the hospital exclusively for this camp. Due to the sheer numbers of patients that were operated, many of them had to be accommodated as day care patients. Postoperative examinations and change of dressings started on the 25th in the OPD area and in the wards. Patients were instructed in post op care and physiotherapy. Two residents stayed back after the camp for postoperative care, stitch removal and advice on follow up until August 31st.
Dr Fong Poh Him lighting the inaugural lamp. Dr Apirag Chuwangsuwanich on extreme left.
EntertainmentThe organizers were particularly concerned about providing quality leisure time for all volunteers, to avoid fatigue set-in over the week, especially for foreign participants. The evenings were occupied by visits to Mcleod Ganj (abode of His Holiness The Dalai Lama), Dharamshala, nearby temples and rivers. A couple of popular Bollywood movies (with English subtitles) were screened on two days. A lot of friendship and bonding developed between all participants and all of them pledged to attend future camps also.
Press CoverageThere was extensive coverage in the press and media about the camp. This further generated keen enquiries about future camps.
Organizational structurePublicityThe Lions Club played a major role in the publicity campaign for the camp, which started about a month and a half earlier. The pamphlets were distributed to peripheral hospitals and schools. The routine patients visiting the surgical OPD were also handed pamphlets.
Press Conference Press reports

Issue 7 www.ipras.org IPRAS Journal 35
ManpowerThe visiting team comprised of 22 members (14 doctors, 6 paramedics and 2 volunteers).Ten staff nurses from the Medical College were posted with the team for operations and there were separate nurses on shift duties for postoperative wards.Two OT assistants were deputed from the hospital strength.Two consultant anaesthetists and two residents from the hospital joined an equal number of anaesthetists of the visiting team to provide anaesthesia on 4 tables simultaneously.Autoclaving was managed by one linear autoclave and one table top autoclave in the side room of the operation theatre. All autoclave linen and dressing material was prepared in the evening just after the day’s work was over.
Boarding & Lodging arrangementsAll visiting members were accommodated by the Principal in the guest house of the Medical College. A kitchen was set up in the guest house by the Lions Club for all catering requirements.
ExpensesThe hospital spent more than 0.4 million Rupees on medicines, sutures and accessories for the patients. Publicity and boarding costs was borne by the Lions Club, Dharamshala.International travel expenses were covered by individuals or sponsors.IPRAS Asia- Pacific Section covered license fees foroverseas doctors, transport of Indian teams and other miscellaneous expenses.
Future and PastAs this area has no facility for Plastic Surgery, it is proposed to have a camp at this same location every year. Earlier, Dr. K.S. Goleria had been conducting free Plastic Surgery camps with his team at Zonal hospital, Dharamshala for 22 years, in association with the Lions Club. This was discontinued due to health reasons about 4 years ago.
Seeing the need of the people, IPRAS “Women for Women” team also did a free camp in Jannani Hospital at Paprola (Palampur) a few years ago. You can view the documentary on www.youtube.com. The camp was the brainchild of Dr. Marita Eisenmann-Klein, Secretary General of IPRAS and was organized by Dr. Chanjiv Singh.
The idea of “Mission India”, a NGO, was floated by Dr.Chanjiv Singh, so that American Plastic Surgeons of Indian origin could work for the poor. It was created by Dr. Kusuma Shashidhar, President of ASIPS and his colleagues. They did a free Plastic Surgery camp in SR Hospital, Kalheli, Bajaura, dist Kullu, Himachal Pradesh last year. The camp report is on www.facebook.com as Kullu mission.
Pictures from the Kangra camp can be viewed at www.iprasaps.org
Sponsoring:1. Principal, Dr. Rajindra Prashad Govt. Medical
College, Kangra
2. IPRAS-Asia Pacific Section
3. Lions club, Dharamshala
4. Bangkok Botanica, Thailand
Report submitted by: Report prepared by:
Dr Rajeev B. Ahuja(Secretary General,
IPRAS-APS)
Dr Chanjiv SinghChairman-IPRAS,
Humanitarian Committee
Prof. Anil Chauhan(Principal, RPG
Medical College, Tanda)
Prof. Sanjeev Sharma(Dept. of Surgery, RPGMC, Tanda)
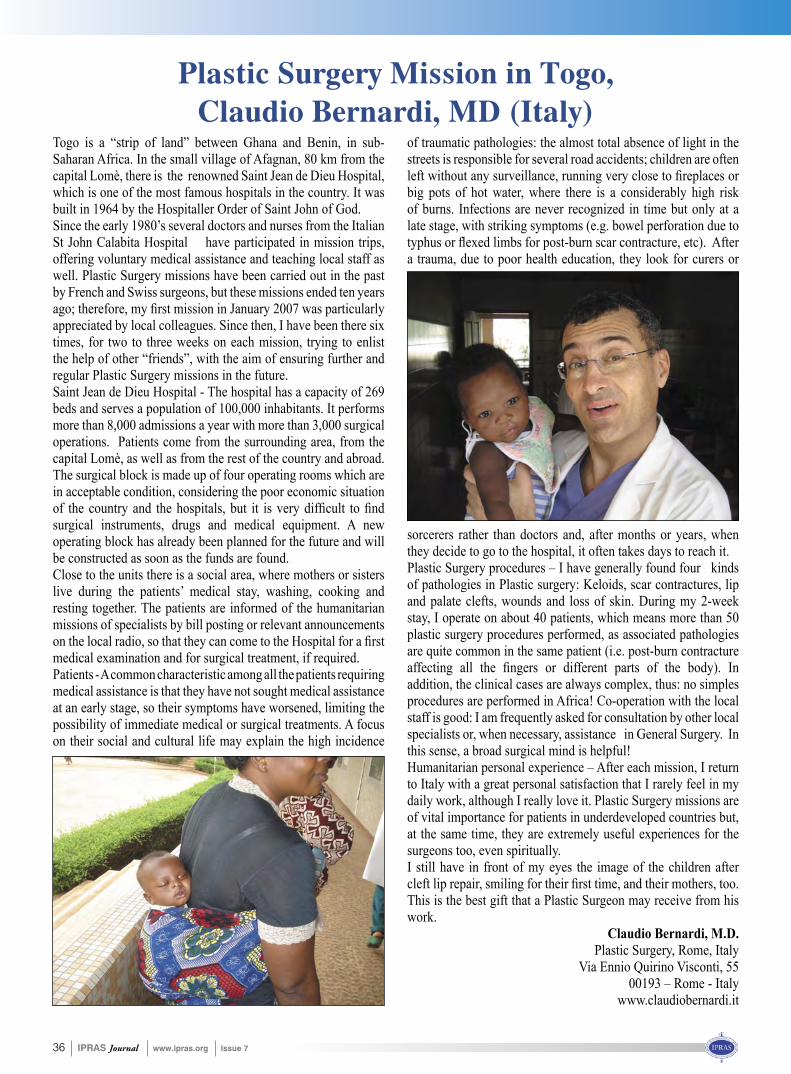
36 IPRAS Journal www.ipras.org Issue 7
Togo is a “strip of land” between Ghana and Benin, in sub-Saharan Africa. In the small village of Afagnan, 80 km from the capital Lomè, there is the renowned Saint Jean de Dieu Hospital, which is one of the most famous hospitals in the country. It was built in 1964 by the Hospitaller Order of Saint John of God. Since the early 1980’s several doctors and nurses from the Italian St John Calabita Hospital have participated in mission trips, offering voluntary medical assistance and teaching local staff as well. Plastic Surgery missions have been carried out in the past by French and Swiss surgeons, but these missions ended ten years ago; therefore, my first mission in January 2007 was particularlyappreciated by local colleagues. Since then, I have been there six times, for two to three weeks on each mission, trying to enlist the help of other “friends”, with the aim of ensuring further and regular Plastic Surgery missions in the future. Saint Jean de Dieu Hospital - The hospital has a capacity of 269 beds and serves a population of 100,000 inhabitants. It performs more than 8,000 admissions a year with more than 3,000 surgical operations. Patients come from the surrounding area, from the capital Lomè, as well as from the rest of the country and abroad. The surgical block is made up of four operating rooms which are in acceptable condition, considering the poor economic situation of the country and the hospitals, but it is very difficult to findsurgical instruments, drugs and medical equipment. A new operating block has already been planned for the future and will be constructed as soon as the funds are found. Close to the units there is a social area, where mothers or sisters live during the patients’ medical stay, washing, cooking and resting together. The patients are informed of the humanitarian missions of specialists by bill posting or relevant announcements on the local radio, so that they can come to the Hospital for a firstmedical examination and for surgical treatment, if required.Patients - A common characteristic among all the patients requiring medical assistance is that they have not sought medical assistance at an early stage, so their symptoms have worsened, limiting the possibility of immediate medical or surgical treatments. A focus on their social and cultural life may explain the high incidence
of traumatic pathologies: the almost total absence of light in the streets is responsible for several road accidents; children are often left without any surveillance, running very close to fireplaces orbig pots of hot water, where there is a considerably high risk of burns. Infections are never recognized in time but only at a late stage, with striking symptoms (e.g. bowel perforation due to typhus or flexed limbs for post-burn scar contracture, etc). Aftera trauma, due to poor health education, they look for curers or
Plastic Surgery Mission in Togo, Claudio Bernardi, MD (Italy)
sorcerers rather than doctors and, after months or years, when they decide to go to the hospital, it often takes days to reach it. Plastic Surgery procedures – I have generally found four kinds of pathologies in Plastic surgery: Keloids, scar contractures, lip and palate clefts, wounds and loss of skin. During my 2-week stay, I operate on about 40 patients, which means more than 50 plastic surgery procedures performed, as associated pathologies are quite common in the same patient (i.e. post-burn contracture affecting all the fingers or different parts of the body). Inaddition, the clinical cases are always complex, thus: no simples procedures are performed in Africa! Co-operation with the local staff is good: I am frequently asked for consultation by other local specialists or, when necessary, assistance in General Surgery. In this sense, a broad surgical mind is helpful! Humanitarian personal experience – After each mission, I return to Italy with a great personal satisfaction that I rarely feel in my daily work, although I really love it. Plastic Surgery missions are of vital importance for patients in underdeveloped countries but, at the same time, they are extremely useful experiences for the surgeons too, even spiritually. I still have in front of my eyes the image of the children after cleft lip repair, smiling for their first time, and their mothers, too.This is the best gift that a Plastic Surgeon may receive from his work.
Claudio Bernardi, M.D.Plastic Surgery, Rome, Italy
Via Ennio Quirino Visconti, 5500193 – Rome - Italy
www.claudiobernardi.it

Issue 7 www.ipras.org IPRAS Journal 37
The Lazio Regional Agency for Organ and Tissue Transplantation, in collaboration with the University of Rome “Tor Vergata”, has organized the Third International Conference on Regenerative Surgery, which took place on 14th - 16th December 2011, in Rome.
Third International Conference on Regenerative Surgery
S.Coleman, G. Rigotti, D. Del Vecchio, M. Lafontan focused their speeches on fat transplantation, while E. Anitua, I. Martin, M. Marazzi, G. Stacy, G. Bauer, together with other researchers, presented the edge of progress on laboratory work.Plastic Surgeons, such as J. Planas, R. Mazzola, T. Tiryaki,
Prof. Valerio Cervelli, Director of the Plastic Surgery Department at the University of Rome “Tor Vergata” during the conference dinner of the
3rd International Conference on Regenerative Surgery
From the left: Dr. Dan Del Vecchio, USA (ISPRES Founding Member), Mr. Zacharias Kaplanidis, Greece (IPRAS Executive Director), Dr. Gino Rigotti, Italy (ISPRES President), Prof. Marita Eisenmann-Klein (IPRAS President), Dr Sydney Coleman, USA (ISPRES General
Secretary), Dr. Theodore Voukidis, Greece (ISPRES Founding member)
The Conference President, Prof. Valerio Cervelli, Director of the Plastic Surgery Department at the University of Rome “Tor Vergata”, offered the participants a unique opportunity to follow the lectures of some of the world’s most prominent authorities in the field of Regenerative Surgery.Not only Plastic Surgeons, but also the most active scientists on the relative topics, biologists, ENT, orthopedics, gynecologists, hematologists, dermatologists and trauma surgeons, were present there, to announce and discuss their latest achievements and experience, on the most promising and upraising field of tissue regeneration, bioengineeringand nanotechnology.The rich Faculty of more than 80 scientists and doctors have thoroughly covered all the topics of the meeting.
P. Gentile, V. Cervelli, F. Moschella, M. Klinger, K. Schlaudraff, T. Voukidis shared their experience on everyday surgical praxis, emphasizing Aesthetic Regeneration on new critical areas.Laboratory researchers, such as S. Pek, S. Akita, M. Dominici and A. Orlandi gave their lectures on Bioengineering and Nanotechnology and the new ways of pharmaceutical administration through new regenerative technologies. Practical issues on the application of the new medical procedures, in Europe and worldwide, were raised and answered by experts, according to the present status on moral, ethical and of course legislative data.The Conference, strongly supported by the Province of Rome, the Lazio Region and the Italian Ministry of Health, offered the opportunity to all the participants to enjoy the famous excellent Italian hospitality together with typical Roman entertainment.The appointment has been renewed for December next year and the organizers guarantee a scientific meeting of equallyhigh standards. In the meantime, a more Plastic Surgery-orientated meeting will be organized by the newly founded ISPRES (International Society of Regenerative Surgery) on the 9th– 12th of March in Rome, where all the new ideas and developments on Regenerative Plastic Surgery will be presented and discussed by an international faculty of experts.
Theodore Voukidis MD, PhD, FACSISPRES Founding member

38 IPRAS Journal www.ipras.org Issue 7
S U R V E Y S
Liposuction is one of the most popular aesthetic surgeries performed worldwide, but its long-term impact on body composition and on the metabolic profile remains unclear.It has been speculated that the immediate decrease in body fat may trigger feedback mechanisms of body-fat regain. In several species, surgical fat removal is accompanied by fat regain within a few weeks, mostly due to compensatory fat growth in the intact depots. Recent data has confirmedthat women undergoing liposuction gain upper-body fat within six months, which may be associated with increased cardiovascular risk. Importantly, no study of the long-term effects of liposuction has controlled for the subjects’ physical activity levels which may be considered an important confounder because exercise per se is believed to improve body composition. Thus, the purpose of this study was to investigate the effects of small-volume abdominal liposuction on body fat distribution in normal-weight women, who were either exercise-trained or not after surgery. We hypothesized that liposuction surgery would cause body-fat regain in physically inactive subjects, whereas a supervised exercise training program would counteract such detrimental outcomes. A six-month randomized controlled trial was conducted. Thirty-six women underwent a small-volume abdominal liposuction (20 to 35 years old; BMI: 23,8 ± 2.2 Kg/m2). Two months after surgery, the subjects were randomly allocated into one of the two groups (trained, T, n=18; or non-trained, NT, n=18). Trained subjects undertook a four-month exercise program. Non-trained subjects remained physically inactive throughout the study period. Prior to the intervention (PRE), immediately before the beginning of the exercise program (i.e., two months after surgery, or POST2) and at the end of the study (POST6), food intake and body composition were assessed. Energy expenditure, dynamic strength and aerobic fitness were assessed at PRE and POST6. POST6 assessments were performed 60 to 72 hours after the last training session in the trained group. Subjects were instructed to maintain their food intake pattern throughout the study. Liposuction was effective in reducing body
weight, fat mass, and subcutaneous abdominal fat (SAT) (PRE vs. POST2, p=0.0001). Despite the sustained SAT decrease at POST6 (p=0.0001), body weight returned to baseline values in both groups. The NT group showed a significant 10% increase in visceral fat (p=0.04) anddecreased energy expenditure (p=0.01) when compared with TR. TR showed an increased fat-free mass (p=0.03) and improved physical capacity (p<0.05) when compared with NT at POST6. The dietary intake was not different between groups and remained unchanged over time. In conclusion, abdominal liposuction does not induce re-growth of fat, but it does trigger a compensatory increase of visceral fat, which is effectively counteracted by physical activity. Given the clinical significance of thesefindings, Plastic Surgeons and health professionals arestrongly advised to recommend exercise training as a mandatory intervention for those subjects submitted to liposuction to avoid the possible long-term deleterious effects of body fat redistribution to the visceral cavity. This study was supported by FAPESP (2007/53318-7).
CT scan images showing the compensatory growth of adipose tissue in the abdominal cavity (arrows)
at 6 months post op (above right).
Author: Eduardo Montaga Sub-authors: Fabiana Braga Benattib; Fábio Lopes Saitoa; Rolf
Gemperlia; Antonio Herbert Lancha Juniorb
a) Division of Plastic Surgery and Breast Surgery Group, University of Sao Paulo School of Medicineb) School of Physical Education and Sport –
University of Sao Paulo
Liposuction induces a compensatory increase of visceral fat which is effectively counteracted by physical activity
Honoured with the award of “Ivo Pitanguy” during the 48th Brazilian congress of plastic surgery
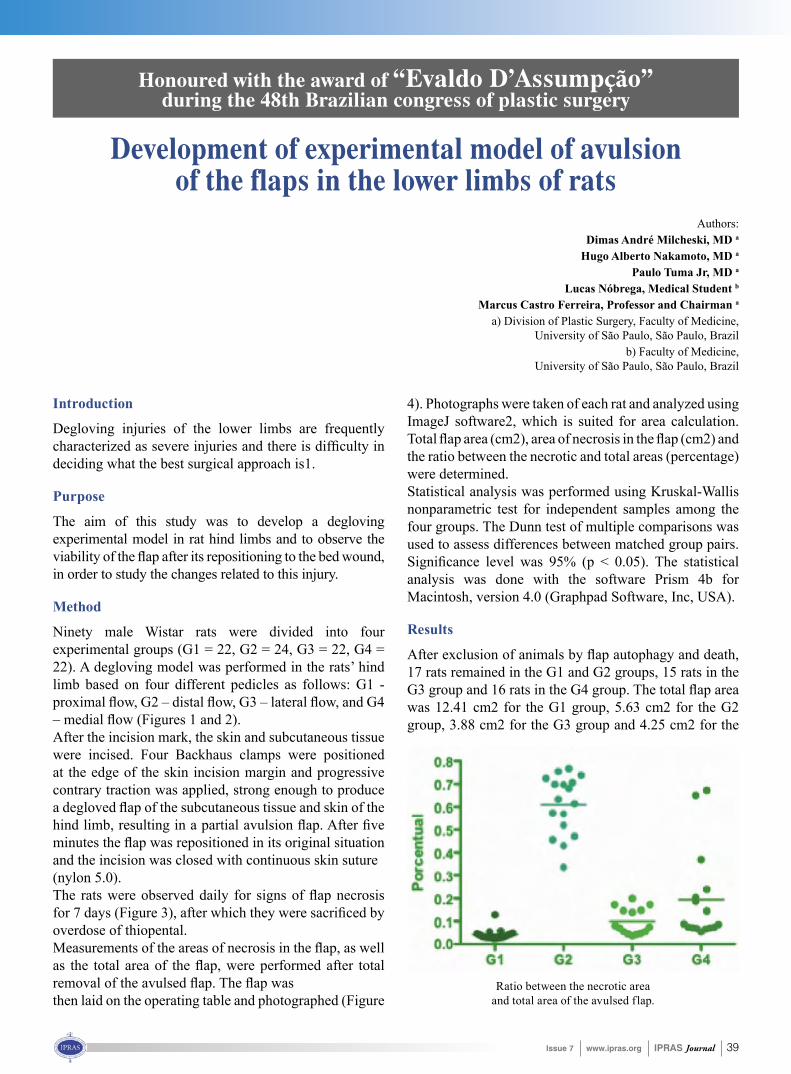
Issue 7 www.ipras.org IPRAS Journal 39
Introduction
Degloving injuries of the lower limbs are frequently characterized as severe injuries and there is difficulty indeciding what the best surgical approach is1.
Purpose
The aim of this study was to develop a degloving experimental model in rat hind limbs and to observe the viability of the flap after its repositioning to the bed wound,in order to study the changes related to this injury.
Method
Ninety male Wistar rats were divided into four experimental groups (G1 = 22, G2 = 24, G3 = 22, G4 = 22). A degloving model was performed in the rats’ hind limb based on four different pedicles as follows: G1 - proximal flow, G2 – distal flow, G3 – lateral flow, and G4 – medial flow (Figures 1 and 2).After the incision mark, the skin and subcutaneous tissue were incised. Four Backhaus clamps were positioned at the edge of the skin incision margin and progressive contrary traction was applied, strong enough to produce a degloved flap of the subcutaneous tissue and skin of thehind limb, resulting in a partial avulsion flap. After fiveminutes the flap was repositioned in its original situationand the incision was closed with continuous skin suture(nylon 5.0).The rats were observed daily for signs of flap necrosisfor 7 days (Figure 3), after which they were sacrificed byoverdose of thiopental.Measurements of the areas of necrosis in the flap, as wellas the total area of the flap, were performed after totalremoval of the avulsed flap. The flap wasthen laid on the operating table and photographed (Figure
4). Photographs were taken of each rat and analyzed using ImageJ software2, which is suited for area calculation. Total flap area (cm2), area of necrosis in the flap (cm2) andthe ratio between the necrotic and total areas (percentage) were determined.Statistical analysis was performed using Kruskal-Wallis nonparametric test for independent samples among the four groups. The Dunn test of multiple comparisons was used to assess differences between matched group pairs. Significance level was 95% (p < 0.05). The statisticalanalysis was done with the software Prism 4b for Macintosh, version 4.0 (Graphpad Software, Inc, USA).
Results
After exclusion of animals by flap autophagy and death,17 rats remained in the G1 and G2 groups, 15 rats in the G3 group and 16 rats in the G4 group. The total flap areawas 12.41 cm2 for the G1 group, 5.63 cm2 for the G2 group, 3.88 cm2 for the G3 group and 4.25 cm2 for the
Development of experimental model of avulsion of the flaps in the lower limbs of rats
Honoured with the award of “Evaldo D’Assumpção” during the 48th Brazilian congress of plastic surgery
Authors:Dimas André Milcheski, MD a
Hugo Alberto Nakamoto, MD a
Paulo Tuma Jr, MD a
Lucas Nóbrega, Medical Student b Marcus Castro Ferreira, Professor and Chairman a
a) Division of Plastic Surgery, Faculty of Medicine, University of São Paulo, São Paulo, Brazil
b) Faculty of Medicine, University of São Paulo, São Paulo, Brazil
Ratio between the necrotic area and total area of the avulsed flap.
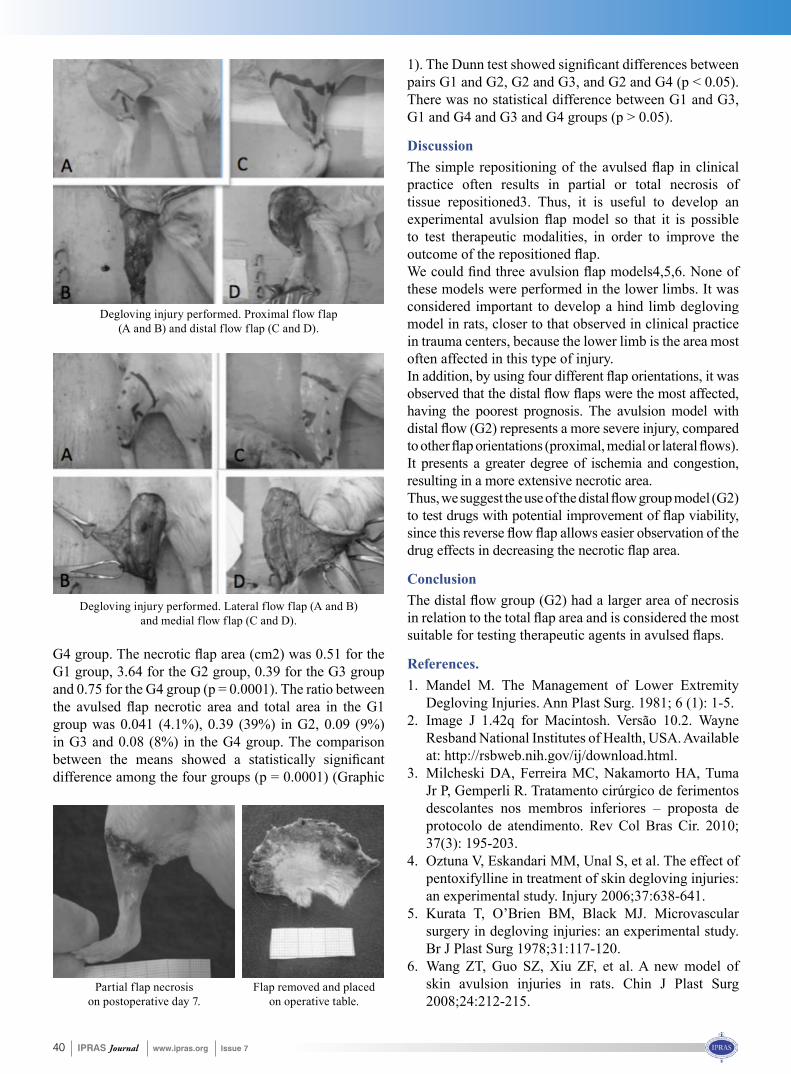
40 IPRAS Journal www.ipras.org Issue 7
G4 group. The necrotic flap area (cm2) was 0.51 for theG1 group, 3.64 for the G2 group, 0.39 for the G3 group and 0.75 for the G4 group (p = 0.0001). The ratio between the avulsed flap necrotic area and total area in the G1group was 0.041 (4.1%), 0.39 (39%) in G2, 0.09 (9%) in G3 and 0.08 (8%) in the G4 group. The comparison between the means showed a statistically significantdifference among the four groups (p = 0.0001) (Graphic
1). The Dunn test showed significant differences betweenpairs G1 and G2, G2 and G3, and G2 and G4 (p < 0.05). There was no statistical difference between G1 and G3, G1 and G4 and G3 and G4 groups (p > 0.05).
DiscussionThe simple repositioning of the avulsed flap in clinicalpractice often results in partial or total necrosis of tissue repositioned3. Thus, it is useful to develop an experimental avulsion flap model so that it is possibleto test therapeutic modalities, in order to improve the outcome of the repositioned flap.We could find three avulsion flap models4,5,6. None ofthese models were performed in the lower limbs. It was considered important to develop a hind limb degloving model in rats, closer to that observed in clinical practice in trauma centers, because the lower limb is the area most often affected in this type of injury.In addition, by using four different flap orientations, it wasobserved that the distal flow flaps were the most affected,having the poorest prognosis. The avulsion model with distal flow (G2) represents a more severe injury, comparedto other flap orientations (proximal, medial or lateral flows).It presents a greater degree of ischemia and congestion, resulting in a more extensive necrotic area.Thus, we suggest the use of the distal flowgroupmodel (G2)to test drugs with potential improvement of flap viability,since this reverse flow flap allows easier observation of thedrug effects in decreasing the necrotic flap area.
ConclusionThe distal flow group (G2) had a larger area of necrosisin relation to the total flap area and is considered the mostsuitable for testing therapeutic agents in avulsed flaps.
References.1. Mandel M. The Management of Lower Extremity
Degloving Injuries. Ann Plast Surg. 1981; 6 (1): 1-5. 2. Image J 1.42q for Macintosh. Versão 10.2. Wayne
Resband National Institutes of Health, USA. Available at: http://rsbweb.nih.gov/ij/download.html.
3. Milcheski DA, Ferreira MC, Nakamorto HA, Tuma Jr P, Gemperli R. Tratamento cirúrgico de ferimentos descolantes nos membros inferiores – proposta de protocolo de atendimento. Rev Col Bras Cir. 2010; 37(3): 195-203.
4. Oztuna V, Eskandari MM, Unal S, et al. The effect of pentoxifylline in treatment of skin degloving injuries: an experimental study. Injury 2006;37:638-641.
5. Kurata T, O’Brien BM, Black MJ. Microvascular surgery in degloving injuries: an experimental study. Br J Plast Surg 1978;31:117-120.
6. Wang ZT, Guo SZ, Xiu ZF, et al. A new model of skin avulsion injuries in rats. Chin J Plast Surg 2008;24:212-215.
Flap removed and placed on operative table.
Degloving injury performed. Proximal flow flap (A and B) and distal flow flap (C and D).
Degloving injury performed. Lateral flow flap (A and B) and medial flow flap (C and D).
Partial flap necrosis on postoperative day 7.

Issue 7 www.ipras.org IPRAS Journal 41
Summary
А novel technique is presented for mastering skills in Plastic Surgery, using only improvised means, particularly the self-adhesive Duoderm®CGF®, which is very similar to the human skin. An example of its application for syndactyly correction by trilobed flap is shown. Theso-called Duoderm-plasty is an easy and cost-effective method, which allows mastering and perfection of different Plastic Surgery ‘tricks’, planning a scheduled surgery and can also serve as a measure for such skills of the medical students and residents.
Keywords
Residency training; Surgery planning; Z-plasty; Syndactyly
Introduction
Training in the specialty of Plastic Surgery deals with the resection, repair, replacement and reconstruction of defects of form and function of the integument and its underlying anatomic structures. It is a long-lasting and laborious process, requiring not merely an excellent, advanced knowledge of medical science, but also a well-developed spatial reasoning and ‘sleight of hand’. The latter can be improved using different contemporary technologies and equipment offered by many companies.Prior to the 1950’s, the operating room (OR) represented the only place to visualize surgery outside the classroom. The introduction of film allowed residents to build andintegrate verbal and pictorial representations of disease. Movies became particularly useful in surgical learning to help describe anatomic relationships and procedures. In the 1980’s computers became an additional tool, with the potential to model the complexity of real tissues and to
gain insight into surgical outcomes through simulation.1 It is known that learners retain 10 to 15% of what is read, 10-20% of what they hear, and 20-30% of what they see, but when audiovisual materials are integrated, knowledge retention increases to 40-50%.2 Therefore, simple inanimate models have been developed for practice of basic surgical skills. Synthetic skin suturing models and computer simulations of surgery are emerging as a prime education tool at several surgical skills centres in the West.5,6 Despite all these advances, the system of surgical skills teaching in Armenia, as well as in many other developing countries still remains on the 1980’s level because the abovementioned training systems are too expensive. Maintenance of well-equipped dissecting rooms and biomedical laboratories is impossible in the present economic status. Residents can hone their skills only at the OR, which is not so simple, because each expert surgeons seek to achieve the best results and he/she will rarely agree to ‘rely’ on a novice’s skills. On the other hand, patients or patients’ relatives always want to be operated by the best, famous expert surgeons. Another problem is that trainees often ‘wait’ for a specific case fora long time: there are many residents and trainees, more than the specific cases.All this forced the authors to propose a model, which would facilitate and improve the skill acquisition process, at least to some extent, in one of the basic sections of Plastic Surgery – integument (cutaneous) surgery.
Model description
The proposed model is based on the use of self-adhesive hydrocolloid dressings (Duoderm®CGF®) as human-skin-substitutes. That is why we called this method ‘Duoderm-plasty’. The unique elastic properties of Duoderm®CGF®
Syndactyly Correction by “Duoderm-plasty”: An Original Model for Mastering Plastic Surgery
G.V. Yaghjyan, D.O. AbrahamyanPlastic Reconstructive Surgery and Microsurgery Centre, University Hospital № 1.
58 Abovyan street, Yerevan, 375025, Republic of Armenia e-mail: [email protected]
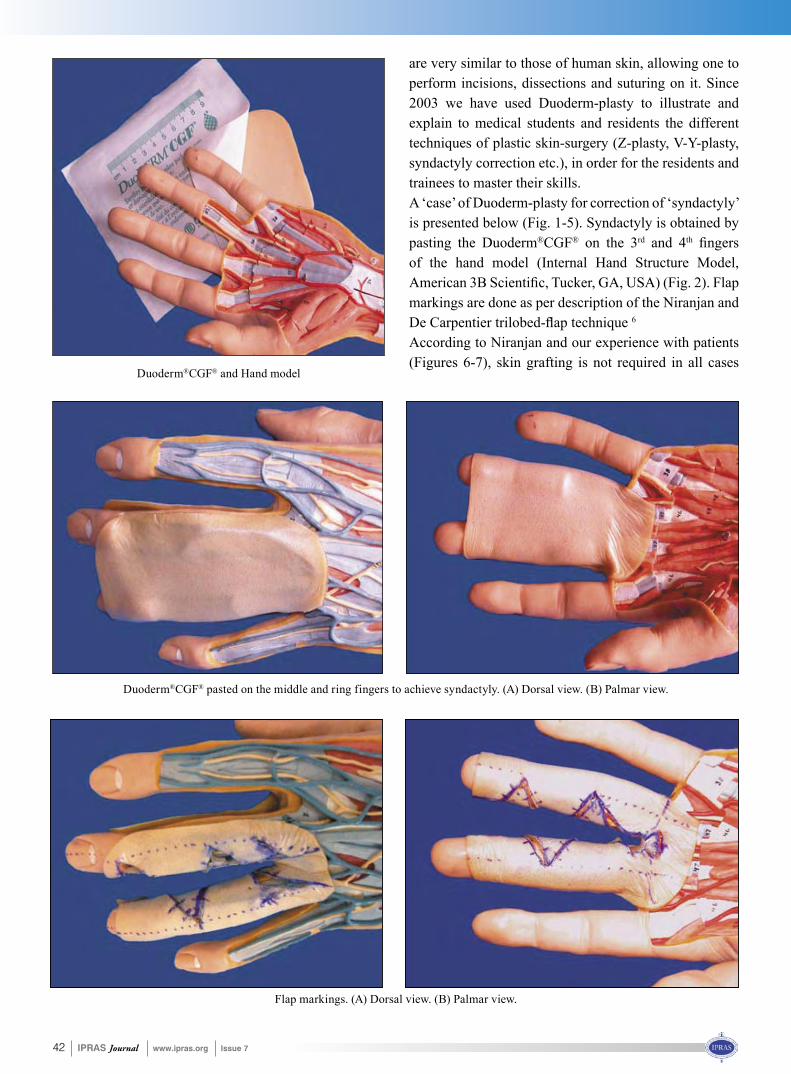
42 IPRAS Journal www.ipras.org Issue 7
Duoderm®CGF® and Hand model
Duoderm®CGF® pasted on the middle and ring fingers to achieve syndactyly. (A) Dorsal view. (B) Palmar view.
Flap markings. (A) Dorsal view. (B) Palmar view.
are very similar to those of human skin, allowing one to perform incisions, dissections and suturing on it. Since 2003 we have used Duoderm-plasty to illustrate and explain to medical students and residents the different techniques of plastic skin-surgery (Z-plasty, V-Y-plasty, syndactyly correction etc.), in order for the residents and trainees to master their skills.A ‘case’ of Duoderm-plasty for correction of ‘syndactyly’ is presented below (Fig. 1-5). Syndactyly is obtained by pasting the Duoderm®CGF® on the 3rd and 4th fingersof the hand model (Internal Hand Structure Model, American 3B Scientific, Tucker, GA, USA) (Fig. 2). Flapmarkings are done as per description of the Niranjan and De Carpentier trilobed-flap technique 6 According to Niranjan and our experience with patients (Figures 6-7), skin grafting is not required in all cases
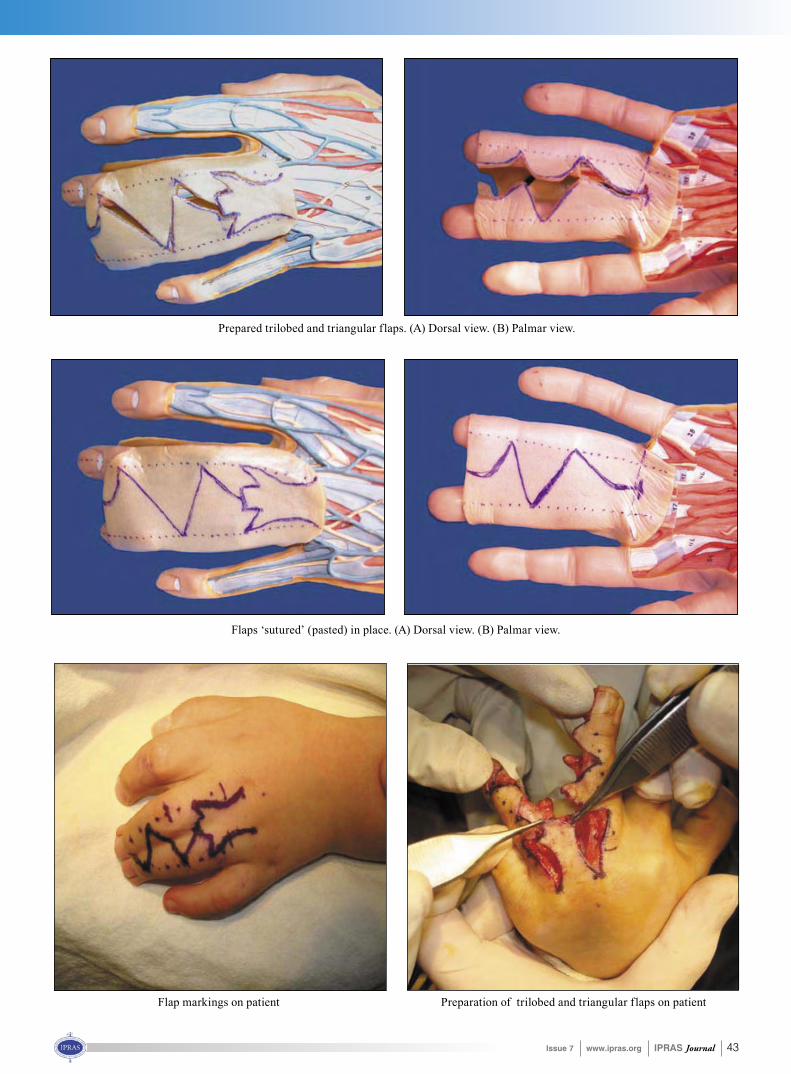
Issue 7 www.ipras.org IPRAS Journal 43
Preparation of trilobed and triangular flaps on patient
Prepared trilobed and triangular flaps. (A) Dorsal view. (B) Palmar view.
Flaps ‘sutured’ (pasted) in place. (A) Dorsal view. (B) Palmar view.
Flap markings on patient

44 IPRAS Journal www.ipras.org Issue 7
where the trilobed flap6 is used. Therefore, if any uncovered ‘defect’ remains after the performed Duoderm-plasty, it means that there has been an omission in the technique of flap harvesting and one should repeat the Duoderm-plasty until the ideal result is obtained.
Discussion
Research shows that motor skill acquisition occurs in three phases.7 Ideally, only the last phase of learning should be performed on actual patients. In the first phaseof motor-skill acquisition, or ‘cognitive phase’, the learner gains an understanding of the task through explanation and demonstrations. Cognitive science studies show that the power of a teaching tool is directly related to the level of interactivity and the method of information delivery.8 The second phase of motor-skill learning is the ‘associative phase’, where the learner practices the task and eliminates error from the performance. This phase could utilize the suggested ‘Duoderm-plasty’ model that places the learner in a lifelike situation providing almost real-time feedback on decisions, actions and questions.Our choice focused on Duoderm®CGF® as this was the only dressing available at our Centre at that time. In other words, any self-adhesive hydrocolloid dressing similar to Duoderm®CGF® can be used for Duoderm-plasty. The benefits of this model are different for novices andexperts. Residents in training can avoid causing iatrogenic complications in real patients, while still being exposed to a wide range of scenarios and complications posed by the expert surgeon. It helps to develop the manual dexterity of the future Plastic Surgeon. Repetition and learner feedback, neither of which are easily accomplished in the OR, improve skill acquisition. Wanzel and Matsumoto found improved execution of Z-plasty skin closure by residents in response to immediate faculty feedback.5 Scott and Young showed it took an average of 32 repetitions to reach the 90th percentile in performance.4 Thus, Duoderm-plasty can serve as a measure for skills of the residents.For expert surgeons, Duoderm-plasty can be used to maintain proficiency during times of absence from theoperating room, an academic sabbatical or family leave. It is also very useful for planning the scheduled operations,
as well as to show and explain to the patient and his/her relatives the plan of the surgery to be performed.Thus, the so-called Duoderm-plasty is an easy and cost-effective method allowing the mastering and perfection of different Plastic Surgery skills and the planning of a scheduled surgery and can also serve as a measure for such skills of the trainees.
References
1. Kawabata H, Kawai H, Masada K, Ono K. Computer-aided analysis of Z-plasties. Plast Reconstr Surg 1989;83:319–325.
2. Mehrabi A, Gluckstein C, Benner A, Hashemi B, Herfarth C, Kallinowski F. A new way for surgical education--development and evaluation of a computer-based training module. Comput Biol Med 2000;30:97–109.
3. Dunnington GL, DaRosa DA. Changing surgical education strategies in an environment of changing health care delivery systems. World J Surg 1994;18:734–737; discussion 733.
4. Scott DJ, Young WN, Tesfay ST, Frawley WH, Rege RV, Jones DB. Laparoscopic skills training. Am J Surg 2001;182:137–142.
5. Wanzel KR, Matsumoto ED, Hamstra SJ, Anastakis DJ. Teaching technical skills: training on a simple, inexpensive, and portable model. Plast Reconstr Surg 2002;109:258–263.
6. Niranjan NS, Azad SM, Fleming AN, Liew SH. Long-term results of primary syndactyly correction by the trilobed flap technique. Br J Plast Surg 2005;58:14–21.
7. Rogers DA, Elstein AS, Bordage G. Improving continuing medical education for surgical techniques: applying the lessons learned in the first decade ofminimal access surgery. Ann Surg 2001;233:159–166.
8. Edmond CV, Jr, Wiet GJ, Bolger B. Virtual environments. Surgical simulation in otolaryngology. Otolaryngol Clin North Am 1998;31:369–381.

Issue 7 www.ipras.org IPRAS Journal 45
iPhone and iPad applications for plastic surgeons
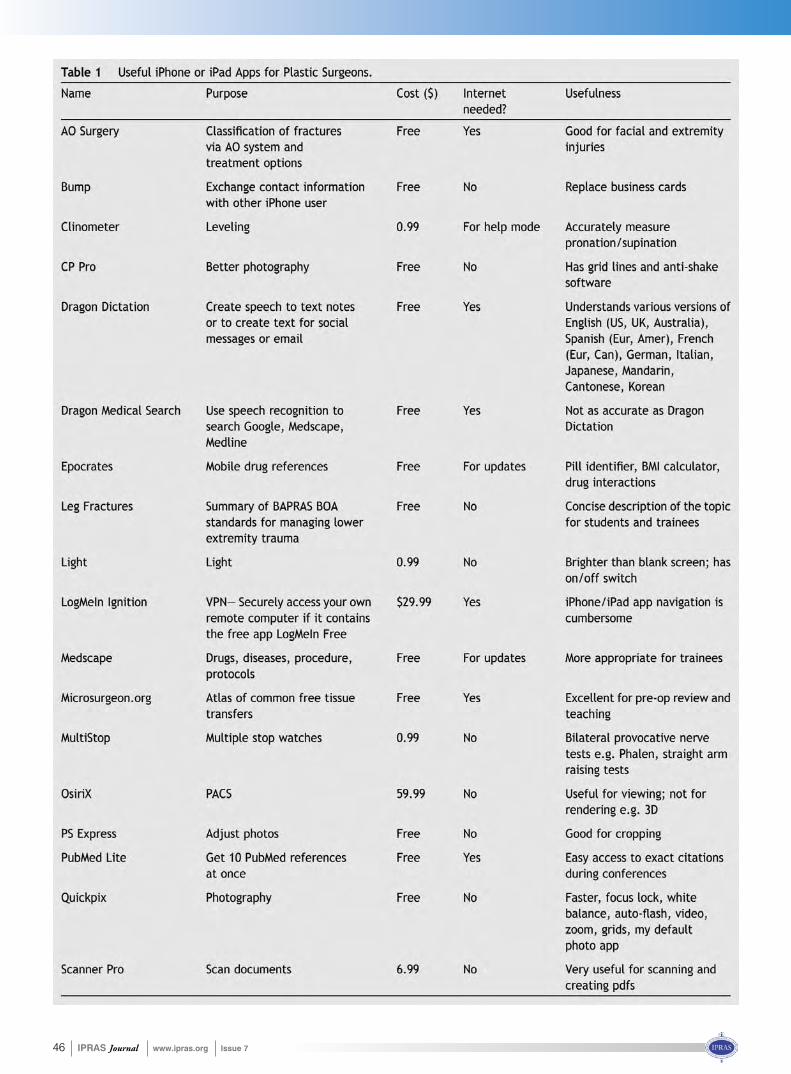
46 IPRAS Journal www.ipras.org Issue 7
Issue 7 www.ipras.org IPRAS Journal 47
By kind permission of JPRAS

48 IPRAS Journal www.ipras.org Issue 7
The Plastic Surgery Hyperguide® is a free interactive continuing medical education (CME) Web site for plastic surgery professionals. It is available at any time from any computer with an Internet connection. This site was established in 2006 and is sponsored by Vindico Medical Education, an ACCME level 3 accredited provider of AMA PRACategory 1 Credit(s)TM .
The Plastic Surgery Hyperguide® is overseen by Chief Medical Editor Seth Thaller MD, DMD, Professor and Chief of Plastic Surgery at the University of Miami, Florida, and Associate Chief Medical Editor Mimis Cohen, MD, FACS, FAAP, Professor and Chief of Plastic Surgery at the University of Illinois at Chicago. Assisted by an Editorial Board of experts from across the plastic surgery specialty, we ensure that the Plastic Surgery Hyperguide® contains the most recent educational material that will benefit the practice of any plastic surgeon. The site isconstantly updated and expanded to ensure that the most recent information is available, allowing users to target the information that is most relevant to their practice.
The Plastic SurgeryHyperguide® currently contains educational material in the following modules: Aesthetic Surgery, Bariatric Surgery, Breast, Congenital; Cleft/
Plastic Surgery Hyperguide: An Interactive Continuing
Medical Education Web Site
Craniofacial, Craniofacial Trauma, Head and Neck Tumors, Patient Safety. Each module contains peer-reviewed educational content focusing on cutting-edge treatments, novel surgical techniques, and clinical reviews. All content submitted for publication goes through a rigorous editorial and review process, which includes a peer-reviewed step where the content is reviewed by 1-2 plastic surgery physicians.
To register, one just needs to go to: www.plasticsurgery.hyperguides.com, select the Login button and follow the instructions. Once registered and logged in, you will have access to hundreds of articles, lectures and video’s to help keep you updated in the field of plastic surgery. Much ofthe content on the site is available for CME credit; you will just need to complete a pretest, posttest and evaluation in order to receive your credit. All credit earned on the site will be stored in your “MyCME” section so that you can always go back and print out the certificates when youneed to submit them for you maintenance of certificationor maintenance of licensure.
We hope that members of IPRAS will take advantage of this opportunity and register to the Plastic surgery Hyperguide®.
Dr. Mimis Cohen MD, FACS, FAAP
Associate Chief Medical Editor of the Plastic Surgery Hyperguide®
Professor and Chief Division of Plastic, Reconstructive and
Cosmetic SurgeryAnd Director Craniofacial Center
University of Illinois Medical CenterChicago, Illinois
Dr. Seth Thaller MD, DMD, FACSChief Medical Editor
of the Plastic Surgery Hyperguide®
Chief and ProfessorDivision of Plastic Surgery
The DeWitt Daughtry Family Department of Surgery
University Of Miami Health SystemMiami, Florida
Issue 7 www.ipras.org IPRAS Journal 49

50 IPRAS Journal www.ipras.org Issue 7
Plastic surgeons are perfectionists by nature. As such, it makes sense that complications associated with cosmetic and reconstructive surgical procedures performed by board-certified plastic surgeons are rare; it’s also why,when something does go wrong, it can be devastating for both physician and patient.
While no plastic surgeon expects a complication to surface in his or her O.R., no procedure is 100 percent safe – and the best surgeons need to be prepared to deal with problems as they arise.
A new symposium developed by ASPS members Maurice Nahabedian, MD, Washington, D.C., and J. Peter Rubin, MD, Pittsburgh, takes a bold approach toward a subject few want to discuss by shining a light on plastic surgical complications. Challenging Complications in Plastic Surgery: Successful Management Strategies, slated for July 13-14 in Washington, D.C., is designed to foster a frank discussion of what goes wrong in common plastic surgery procedures and challenge surgeons to re-think their various approaches on issues ranging from where to place a scar to how they communicate with patients. The symposium is supported by an educational grant from Synovis Surgical Innovations.
“Complications are underemphasized in most meetings where the focus is primarily on how to do a specificprocedure,” says Dr. Nahabedian. “This meeting will focus on providing useful information to help the average surgeon in the day-to-day management of complications with an emphasis on breast and body contouring – two areas in which the number of operations is increasing every year.”
Specific solutionsMore than anything, Challenging Complications in Plastic Surgery intends to dive deep into specific,algorithmic approaches to correcting unfavorable
scars and managing complications in the areas breast augmentation, breast reconstruction, body contouring procedures and abdominoplasty. A wide range of panels and case discussions will cover subjects such as “tips and traps” in the management of capsular contracture, flap salvage and alternative approaches when a flap dies,cardinal rules for liposuction safety and revision surgery for recurrent laxity after body contouring.
“This meeting will be far more concrete than theoretical,” adds Dr. Rubin. “Attendees will receive information that can be implemented overnight and used to make an immediate impact on their practices by managing techniques and communication.”
The meeting will also feature a module dedicated to abdominoplasty complications, the area of plastic surgery in which problems are statistically most likely to occur. Course topics include “The Seven Deadly Sins of Abdominoplasty,” managing and avoiding wound breakdown and infectious complications, and a comprehensive approach to diagnosing and treating abdominoplasty complications.
A complicated facultyThe esteemed faculty members assembled for Challenging Complications in Plastic Surgery are renowned for their exemplary surgical techniques, but this meeting will call on them to share what has gone wrong with their patients and subject their own problematic cases to analysis and debate.
“The faculty is an outstanding group of thought leaders who can provide up-to-date and useful algorithms in managing complications,” says Dr. Nahabedian. “They were hand-picked for their experience, integrity and standing in the specialty – these are people who aren’t afraid to air their dirty laundry and know how to treat complications.”
New symposium aims to confront complications, offer concrete fixes
NATIONAL ASSOCIATIONS’ & PLASTIC SURGERY ORGANIZATIONS’ NEWS
By Mike Stokes, Plastic Surgery News

Issue 7 www.ipras.org IPRAS Journal 51
Attendees are also encouraged to submit questions and their own challenging cases as part of what organizers expect to be a truly interactive dialogue between the faculty and those in attendance.
For many ASPS members, an increasingly common source of surgical complications is the population of patients seeking corrective surgery for operations performed by someone else. Amid the current climate of “white coat deception” – where practitioners without core training in plastic surgery are dabbling in cosmetic procedures – organizers hope the symposium will also give ASPS members greater confidence in dealing with the surgicalmistakes of others by bringing these complications into the open where surgeons can discuss how to correct them if – and when – they occur.
A cut aboveThe symposium will also cover the fundamentals of evidence-based medicine and its potential impact on health quality and pay-for-performance metrics amid a changing regulatory landscape.
The meeting will also feature medico-legal tips to “bulletproof” your informed-consent process and the “do’s and don’ts” of going on the record when a complication occurs. A keynote lecture on VTE prophylaxis as well as panels that explore outcomes measurement in breast and body procedures, establishing your own quality measures in your practice and techniques for benchmarking complications will also be included in the symposium.Additional meetings offered by ASPS include: • From Residency To Tenure: A Road Map For Success
for the Academic Surgeon , June 16-17, 2012, Ann Arbor, Michigan
• Breast & Body Symposium: August 22-25, 2012/Downtown Santa Fe, New Mexico
• Annual meeting: Plastic Surgery THE Meeting: October 26-30, 2012/New Orleans, Louisiana
For information on how to register for any of these conferences, visit www.plasticsurgery.org/meetings, email [email protected] or call 847-228-9900, ext. 471.
July 2012
CHALLENGING COMPLICATIONS IN PLASTIC SURGERY SYMPOSIUM: SUCCESSFUL MANAGEMENT STRATEGIES
Dates: 7/13/2012 - 7/14/2012Meeting Location: Grand Hyatt Washington, Washington DC
Contact: American Society of Plastic Surgeons444 E. Algonquin Road Arlington Heights, IL 60005
P: 847-228-9900 F: 847-228-9131 Sponsored by: ASPS

52 IPRAS Journal www.ipras.org Issue 7
It was a sunny begining of the southern hemisphere summer, between November 10th and 15th, when the 48th edition of the Brazilian Congress of Plastic Surgery took place in Goiania, Brazil. The host city, Goiania, boasts to be the heart of the huge brazilian agricultural infrastructure, the birthplace of important traditions that, even to this day, markedly permeates the brazilian culture with flavors, colors, accents, trends and fados. Hospitalitywas a the most abundant comodity!With 2146 registered participants this year, the Brazilian Congress has secured its place between the most acclaimed
Plastic Surgery Continued Education events on the planet. The Brazilian Society of Plastic Surgery, founded in 1948, has topped the 5000-member mark, and currently certifies 81 plastic surgery training facilities throughoutthe nation. Today, with many different departments to fullfil its needs, simultaneous translation to English inall the presentation rooms and an ever growing number of foreign registered participants, its main goal is to go global.Evidence-based Medicine has played a key role in the selection of the topics and new, different presentation formats were introduced with a variable degree of overall satisfaction. This certainly reflects a worldwidetrend towards boosting the credibilty of our Specialty, saves money and assures that our patients will have good Medicine at their disposal. The Brazilian Scientific
It took place at the Brazilian “Planalto Central”...
Brazilian Society of Plastic Surgery (SBCP)
Opening ceremony of the 48th Brazilian Congress of Plastic Surgery. Next to Prof. Marita Eisenmann-Klein (IPRAS President) on the left Prof. Sebastiao Nelson Edy Guerra, Brazil (Former President of the Brazilian Society of Plastic Surgery),
and on the right, Prof. Ivo Pitanguy (IPRAS Trustee)
48th Brazilian Congress of Plastic Surgery Goiania, Brazil, November 10-15, 2011

Issue 7 www.ipras.org IPRAS Journal 53
Prof. Sebastiao Nelson Edy Guerra, Brazil (Former President of the Brazilian Society of Plastic Surgery) with Ms. Maria Petsa, Greece
(IPRAS Assistant Executive Director) at the IPRAS Booth. Commitee, composed by seven members and chaired by Dr. Osvaldo Saldanha, is actively involved with Continued Education and has worked hard to innovate, stimulate, access and control the processes involved in this large Plastic Surgery gathering. This was the result of a complex series of brainstorming and benchmarking from previous editions, along with the knowledge acquired from other national Plastic Surgery Societies.This Congress also marked, during the opening ceremony, the triumphant come-back of IPRAS as an active world confederation and major player. Dr. Marita Eisenmann-Klein, IPRAS President, alongside Goiania-born Dr. Nelson Piccolo, IPRAS Secretary General, on behalf of our World Confederation, together with Dr. Sebastião Nelson Guerra, President of the Brazilian Society of Plastic Surgery, honored colleagues like Dr. Ivo Pitanguy and Dr. Ricardo Baroudi for their body of work throughout their lives as Plastic Surgeons. Former Presidents of the Brazilian Society of Plastic Surgery were also honored during that ceremony. The IPRAS
coming back to the scene has everything to do with a display of good management principles and orthodoxy. IPRAS has recently pursued its goals by means of what seems to be a mix of pragmatism and a globally oriented vision, focused on inclusion.For the years to come, the project of the Brazilian Society is to upgrade its ties with other national Plastic Surgery Societies in order to be able to share the expertise in Aesthetic Plastic Surgery and other related topics that we have acquired through the years, with colleagues from
During the opening ceremony of the 48th Brazilian Congress of Plastic Surgery. Prof. Ricardo Baroudi (IPRAS Trustee),
Prof. Marita Eisenmann-Klein (IPRAS President)
distant corners of the world. We all, who compose the body of the Brazilian Society of Plastic Surgery, await our colleagues from different countries, to visit us in the Brazilian Plastic Surgery booth, which is set to be present at major Plastic Surgery Congress venues, during the year of 2012.For the colleagues who came to Goiania this year, thank you once again for your invaluable presence and for those who couldn’t make this year, our hearts and minds will allways be open to receive you in future meetings. “Planalto Central” stands for “Central Highlands” in Portuguese.Love from Brazil!
Pericles Serafim FilhoBrazilian Society of Plastic Surgery,
Scientific Committee MemberIPRAS, EXCO Member
IPRAS, Scientific Committee Member

54 IPRAS Journal www.ipras.org Issue 7
Dear Colleagues,It gives me great pleasure to report back on the success of the 1st International Meeting of the Cyprus Society of Plastic Reconstructive and Aesthetic Surgery, which took place under the auspices of IPRAS on the 14th and 15th October 2011, in Limassol. This is the first time such a
meeting has been hosted in Cyprus, and we hope that this will be the start of a fruitful and productive cooperation between our society and IPRAS.Close to 45 delegates participated in the Conference, with a large number of international attendees and over these 2 days, a variety of extremely interesting topics were presented by our invited speakers, as well as by local Plastic Surgeons. Of great interest were the talks pertaining to the exciting field of stem cell research and fat grafting,as related to all aspects of Reconstructive Surgery.Such meetings are of great importance to our Society and its members, not only because they provide us with a unique chance to present our work to the wider medical community, but more importantly because we have the opportunity to expand our knowledge, interact with experts and discuss clinical issues within an appropriate setting.
From the left: Dr. Dana Jianu, Romania, Dr. Katharina Russe-Wilflingseder, Austria, Dr. Marco Klinger, Italy, Prof. MaritaEisenmann-Klein, Germany (IPRAS President), Prof. Andreas Yiacoumettis, Greece (IPRAS Deputy General Secretary), Dr. Roger Khouri, USA (ISPRES Vice President), Dr. Theodoros Voukidis, Greece ( ISPRES Founding member), Dr. Hatem May, Lebanon
Among others: Dr. Kenan Arifoglu, Cyprus, Dr. Andreas Foustanos, Greece (Former President of HESPRAS), Dr. Lefteris Dimitriou, Cyprus, Dr. Georgia Koulermou, Greece, Dr. Michail Stampos, Greece, Dr. Zavrides Harris, Cyprus, Dr. Anastasios Tsekouras, Greece, Prof. Andreas Yiacoumettis, Greece (IPRAS Deputy General Secretary), Prof. Marita Eisenmann-Klein, Germany (IPRAS President), Dr. Marco Klinger, Italy, Dr. Katharina Russe-Wilflingseder, Austria, Dr. Christos Merezas,Cyprus (President of the Symposium), Dr. Giorgos Psaras, Cyprus (President of the scientific committee of the symposium),Dr. Dana Jianu, Romania, Dr. Sofoclis Nicolaides, Cyprus
From the left: Dr. Christos Merezas, Cyprus (President of the Symposium), Dr. Kenan Arifoglu, Cyprus, Prof. Marita Eisenmann-Klein, Germany (IPRAS President), Prof. Andreas Yiacoumettis, Greece (IPRAS Deputy General Secretary), Dr. Borman Huseyin, Turkey
The breadth and variation of Plastic Surgery makes it the central link between many other medical disciplines and it is our duty to ensure that we maintain this diversity and educate our colleagues correctly. Aesthetic Surgery forms a small part of our profession, and it is therefore essential that, as Plastic Surgeons, we protect this multifaceted specialty and expand our autonomy. Through such meetings we are able to stay up to date with ever changing practices, share our experiences and join forces on how we can improve patient care.
Christos Merezas, President of the Cyprus Society for PRAS
1st International Meeting of the Cyprus Society of Plastic Reconstructive and Aesthetic Surgery

Issue 7 www.ipras.org IPRAS Journal 55
The first Chinese-European Congress of Plastic,Reconstructive and Aesthetic Surgery was held in Beijing from 27 to 29, October, 2011. It was the first Congress thatco-organized by the Chinese Society of Plastic Surgeons (CSPS), The European Society of Plastic, Reconstructive and Aesthetic Surgery (ESPRAS) and the International Confederation for Plastic, Reconstructive and Aesthetic Surgery (IPRAS). In addition, it was supported by the
cooperation between Prof. Andreas Yiacoumettis in Greece and Prof. Zunli Shen in China, a comprehensive program was made with a wide coverage of many important fields. These were complications in plastic surgery,breast reconstruction, anti-aging, liposuction, tissue engineering, breast augmentation, ear reconstruction, facial aesthetic surgery, stem cells, genitalia, torso, extremity reconstruction, rhinoplasty, facial rejuvenation, hand, laser,
The First Chinese-European Congress of Plastic, Reconstructive and Aesthetic Surgery
Beijing, China, October 27-29, 2011
Opening Ceremony of the 1st Chinese European Congress of Plastic, Reconstructive and Aesthetic Surgery
American Society of Plastic Surgery, the Brazilian Society of Plastic Surgery, the European Society of Preventive, Regenerative and Anti-Aging Medicine (ESAAM), as well as the International Society of Aesthetic Plastic Surgery (ISAPS).
It was a big international congress which attended by approximately 300 plastic surgeons outside of China with 48 accompanying persons, while the international faculty number was consisted of approximately 100 prominent plastic surgeons. 146 Chinese plastic surgeons attended the congress, in which 20 Chinese plastic surgeons held keynote speeches. 57 international and Chinese companies had exhibitions and provided financial support for thecongress. The Plastic Surgery Hospital, affiliated toPeking Union Medical College and Chinese Academy of Medidical Sciences, offered a substantial support for the congress with translations and entertainment programs during the opening ceremony.
Due to scientific committees’ hard work, especially close
From the left: Dr. Pericles Serafim Filho, Brazil (member of the Scientific Advisory Board of IPRAS), Prof. Marita Eisenmann-Klein, Germany (IPRAS President), Dr. Albert de Mey, Belgium (member of the Scientific Advisory Board of IPRAS), Prof. Yilin Cao, China (President of CSPS, IPRAS deputy General Secretary), Dr. Sukwha
Kim, Korea (IPRAS representative of Asian-Pacific region).

56 IPRAS Journal www.ipras.org Issue 7
scars, maxillofacial, craniofacial, burns, eyelids and orbit, oncology and reconstruction, experiment, fat and so on. The master classes, keynote lectures and oral presentations were well selected with high academic standard.
There were also some round tables such as ESPRAS/SHARE round table (Humanitarian), Laser round table, Brazilian round table (facial aesthetic surgery in Brazil), ESAAM round table and ASPS round table. These round tables provided a nice chance for Chinese plastic surgeons understood more deeply about the related international societies.
During the congress, Marita Eisenmann-Klein, President of IPRAS and Yilin Cao, President of CSPS, Zuoliang Qi, President-elect of CSPS, signed a Memorandum of Understanding. This indicated that CSPS would have full support of IPRAS on establishing a Chinese Society of Preventive, Regenerative and Anti-Aging Medicine as a chapter of the CSPS.
Prof. Zuoliang Qi, President-elect of CSPS, Prof. Marita Eisenmann-Klein, IPRAS President and Prof. Yilin Cao, President of CSPS, signing a Memorandum of Understanding, establishing a Chinese Society of Preventive, Regenerative and Anti-Aging Medicine as a
chapter of the CSPS
Faculty Dinner of 1st Chinese European Congress of Plastic, Reconstructive and Aesthetic Surgery
It was also the first time for Zita congress S.A. to organizea Chinese European Congress in China with the help by Shanghai Hongbo company (China). After mutual understanding and close cooperation, we believe that the world congress of IPRAS will be held successfully in Shanghai in 2015.
In a word, IPRAS and other international societies became well-known in China after this great congress. And the international societies also learned more about Chinese plastic surgeons and the CSPS. The congress has strengthened our cooperation and friendship.
More information available at www.China-europe2011.com
Prof. Yilin CaoPresident of CSPSCo-President of the Congress
Prof. Zunli ShenEXCO member in China
Opening Ceremony of the 1st Chinese European Congress of Plastic, Reconstructive and Aesthetic Surgery
Anti Aging meeting during the 1st Chinese-European Congress of Plastic, Reconstructive and Aesthetic Surgery for establishing a Chinese Society of Preventive, Regenerative and Anti-Aging Medicine as a chapter of the CSPS. First line from the right: Mrs. Katherine Lee Tai, USA, Prof. Yilin Cao, China (President of CSPS, IPRAS Deputy General Secretary), Prof. Marita Eisenmann- Klein, Germany (IPRAS President), Prof. Chistos C. Zouboulis, Germany (ESAAM President), Prof. Zuoliang Qi, China, President-elect of CSPS. Second line from the right: Mr. TT Durai, India, Dr. Michael Klentze, Germany, Dr. Paul Ling Tai, USA, Mr. Zacharias Kaplanidis (IPRAS Executive Director), Prof. Zunli Shen, China
(EXCO member in China)
On the 25th of November, the Dutch Society for Plastic and Reconstructive Surgery (NVPC, www.nvpc.nl) organized the National Day for Plastic and Reconstructive Surgery.
As in many other countries, Dutch Plastic Surgeons struggle with an image of being solely cosmetic surgeons. Therefore, the goal of that day was to show the wide scope of our profession to the public. Special focus was set on subjects other than cosmetic surgery, such as Hand Surgery, Craniofacial and Reconstructive Surgery, illustrating and underscoring the significance of our field in modern society and the medical institutions.
The Netherlands has 17 million inhabitants and approximately 300 Plastic Surgeons. We invited all Plastic Surgery units to participate. Approximately 70% of all clinics did so. The Society supported the units by providing a central website and electronic documents to be used as banners on websites. Press release formats, to be adjusted to specific needs, werealso distributed in a ‘tool kit’. Local and national media were used, as well as social media, such as twitter (@nedverplastchir) and Facebook, to spread the word. The day was open for the general public, as well as anyone interested, such as students and local hospital staff and nurses.
Programs included lectures and live surgery through in-house TV channels or local stations. Other units organized tours through the various rooms, as well as the quite popular suturing courses on bicycle tires or bananas.
The result of the day was measured in many ways. First, the number of visitors varied between 40 and 200 per unit, adding up to approximately 1000 persons in total. Second, the number of articles and interviews in the national and local media and in the social media (twitter/facebook) was quite significant.
In conclusion; the day was a tremendous success for the Plastic and Reconstructive Surgery Society, the local organizers and our field. Next year 100% of the participants of thisedition will join, as well as a number of units that did not choose to participate this year. In addition, the number of positive news articles put our specialty in an especially positive and respectful perspective, which can only be of help for the future of our Plastic and Reconstructive Surgery.
Hinne Rakhorst MD, PhD.General Secretary Dutch Society of Plastic
and Reconstructive Surgery (NVPC)www.nvpc.nl
twitter: @nedverplastchir
The First Dutch “National Day for Plastic and Reconstructive Surgery”
successfully showed the importance and wide scope of Plastic Surgery to the general public.

58 IPRAS Journal www.ipras.org Issue 7
Hans Strömsdörfer
German Association of Plastic, Reconstructive and Aesthetic Surgeons (DGPRÄC) goes Web 2.0
Dear colleagues and friends,Having been appointed as the EURAPS local host, it is my pleasure and privilege to welcome you to the 23rd Annual EURAPS Meeting, which will be held on May 24th – 26th, 2012 in Munich, Germany. A cosmopolitan and hospitable city with excellent infrastructure, Munich offers its guests a unique atmosphere. Munich’s world-class transportation system allows visitors to easily reach the city by train, plane or car. In 2010, Monocle ranked Munich as the world’s most liveable city.The meeting venue, The Bayerischer Hof, is a leading world-class luxury hotel, ideally situated in the old town district of Munich, in direct proximity to the most important sights and shopping opportunities. The hotel maintains traditional Bavarian values (http://www.bayerischerhof.de). In addition, participants will be able to indulge in a special “Oktoberfest atmosphere” at the bavarian evening. Furthermore, a magnificent gala dinner at the BMW Weltwill be one of the social highlights of the meeting.EURAPS Meetings offer a great opportunity for all of us to update our knowledge, meet with both old and new friends and colleagues and to enjoy each other’s company. This is the best occasion to prepare the ground for fruitful scientificco-operation in the field of Plastic Surgery.The Scientific Program will focus on new developments inPlastic, Reconstructive and Aesthetic surgery, especially in the multidisciplinary setting of Regenerative Medicine. In particular, the Program will concentrate on approaches from diagnosis to state-of-the-art, less invasive treatments. This Meeting will offer new insights, which will be a platform for scientific exchange and discussion.
For the first time, all participants will have the opportunity toattend the best research paper of EURAPS Research Council Meeting on Thursday afternoon (May 24th, 2011) instead of the Refresher Course. This will be the last session of the EURAPS Research Council Meeting that will take place in Munich from May 23rd – 24th, 2012. With this idea from the new General Secretary of EURAPS Manfred Frey, we would like to emphasize the importance of research work and give the younger generation an opportunity to attend the EURAPS Meeting.Apart from the exciting scientific schedule, you willcertainly have the opportunity to sample Munich’s artistic and cultural richness. This includes splendid and exciting concerts, impressive exhibitions, culinary delights, sporting events and excellent shopping. There is more to Munich than meets the eye!For further information on the 23rd Annual EURAPS Meeting and booking details, please visit us online on WWW.EURAPS.ORG.I look forward to spending some inspiring days with you.
23rd Annual EURAPS Meeting, Munich, Germany, May 24-26, 2012
Milomir NinkovicMD, PhD, EURAPS Local Host, Munich 2012
Tweets, posts, wikis and friends – the “Web 2.0” calls for everyday interaction. Millions of users work with Facebook, Twitter and Wikipedia day by day – creating an “internet within the internet” on computers, cell phones and pads. The German Association of Plastic, Reconstructive and Aesthetic Surgeons (DGPRÄC) is now also present on these channels and welcomes you to participate:
• Facebook: www.facebook.com/dgpraec Log in and “like“ us. You will receive all new information about
DGPRÄC (in German).• Twitter: http://twitter.com/dgpraec Sign in for our Twitter account!• Wikipedia: http://de.wikipedia.org/wiki/Deutsche_Gesellschaft_der_
Plastischen,_Rekonstruktiven_und_Ästhetischen_Chirurgen

Issue 7 www.ipras.org IPRAS Journal 59
Increasing the visibility and awareness of the possibilities of Plastic Surgery remains the concern of Plastic Surgeons worldwide. To make it possible, the Association of Plastic Surgeons of India, led by its President, Dr. S. Raja Sabapathy, hit upon a novel concept of the creation of a “Plastic and Reconstructive Surgery Day”. The date was fixed as July the 15th. Though it did not commemorate abirth or signal an event in the history of Plastic Surgery, the day was chosen for logistic reasons. It was also felt that more than the date we choose, what we do with the concept will count more.
What was done on the Plastic & Reconstructive Surgery Day? A call was given by the President of the Association of Plastic Surgeons of India, Dr. S. Raja Sabapathy, requesting all their members to do at least one free surgery on that day. The day could also be utilized to conduct programs to popularize Plastic Surgery. Plastic Surgeons from all over the country responded with great enthusiasm and the concept was a phenomenal success. Activities done on that day included:
• APSI members performed free surgeries varying from free flaps to replace a giant hairy nevus on theface and reattachment of a hand in a rural setting, to the correction of post burn deformities, repair of
Plastic and Reconstructive Surgery Day 15th July, 2011
Throughout the country the media responded very well.
Replant for a poor child done in Nanded, Maharashtra State on Plastic Surgery Day
Dr. S. Raja Sabapathy, MS, M.Ch, DNB, FRCS(Ed), MAMS Director
& Head Department of Plastic Surgery, Hand Surgery, Reconstructive Microsurgery and Burns.
Ganga Hospital, INDIA

60 IPRAS Journal www.ipras.org Issue 7
cleft lip and palate and rhinoplasty. The surgeries performed covered almost the whole spectrum of Plastic Surgery.
• Press conferences were conducted by many Plastic Surgery departments. This gave Plastic Surgeons the opportunity to explain to the media the scope of Plastic Surgery. The media responded very well and carried the message to the masses.
Hon’ble Minister for Health, Government of India, Shri. Ghulam Nabi Azad, commented the Association of Plastic Surgeons of India on their innovative idea.
• Utilizing the concept of the day, Plastic Surgeons in many places met senior government officialsand ministers to describe the local needs for Plastic Surgery services. Extra funds were sanctioned for various schemes and for the creation of Plastic Surgery hospital beds exclusively for patients with Hansen’s diseases who need tendon transfers. Some young surgeons even started their practices on that day. Specialized services in hand injuries were started by some hospitals to coincide with the day.
• Taken as a whole, the concept of Plastic and Reconstructive Surgery Day provided the much needed opportunity for Plastic Surgeons to reach all sections of the society, from Government administrators to the public. Perhaps the most gratifying response was that from the President of the International Confederation for Plastic, Reconstructive & Aesthetic Surgery, Prof. Marita Eisenman-Klein, who suggested in her newsletter that July 15th, 2012 be celebrated as “World Plastic & Reconstructive Surgery Day”. Neighbouring countries like Sri Lanka have agreed to this concept. We do hope that this will help us provide yet another avenue for Plastic Surgeons worldwide to reach the masses. Since the response was overwhelming, the Association has decided to celebrate this day every year.
Surgeons conducted meetings in the hospitals to make more people aware of their department on Plastic Surgery Day.

Issue 7 www.ipras.org IPRAS Journal 61
Plastic Surgery as a professional and experiences group of scientists committed to the highest levels of service, quality and ethical values in the entire Nicaraguan medical field.
Dr. Pablo Mongalo President of the Nicaraguan Medical Association Hans in Recognition Diploma to Dra. Sandra Gutierrez President of SNCP, for its Legalization.
Early in 2010, the Nicaraguan Society of Plastic Surgery initiated the necessary procedures in order to be legally registered for the first time after almost 20years of history, according to the prerequisites of the local laws. The first legal procedure was completed in March of thesame year. The legal foundation under constitutional articles, which was then followed by the application of the Nicaraguan Society of Plastic Surgery presented to the National Assembly to possess legal status.The board of directors monitored the process until the 6th of July 2011, when the Nicaraguan National Assembly granted the Nicaraguan Society of Plastic Surgery status of a legal entity.The SNCP celebrated this important accomplishment last July, receiving recognition from the Nicaraguan Medical Association for its organizational growth. Dr. Guillermo Echeverria, President of the Ethics Committee of the FILACP was invited as a special guest and gave a speech on “Ethics and Commerce in plastic surgery” suitable for the occasion, taking into consideration that as members of the Ibero-American Federation of Plastic Surgery we all abide by our legislation and code of ethics. A fact that makes us a respected and solid Association.By being granted the long awaited legal status, our association reached a milestone in its long and successful history. We reaffirmed our position in the world of
Legalization of the Nicaraguan Society of Plastic Surgery
Founding Board of Directors. Dr. Alfonso Pares Vice President, Dra. Rossana Trejos, Secretary, Dra. Carolina Franchini Treasurer, Dra. Sandra Gutierrez President, Dr. Leandro Perez, Fiscal.
Nicaragua, election of the new board of the Nicaraguan Association of Plastic Surgery
On November 25th the Nicaraguan Association of Plastic Surgery conducted an election for the new Board of Directors which corresponds to the period of January 2012-January 2014. The event resulted in the reelection of Dr. Sandra Gutierrez as President, Dr. Alfonso Pares as Vice President and Dr. Carolina Franchini as Treasurer accompanied by Dr. Edgard Ibarra elected Secretary, Dr. Juan Carlos Arguello responsible for fiscal issues, and Dr. Dolores Brockmann asspokesperson for the Association. On December 15th 2012, the Association will be holding the inaugural ceremony for the new board, as well as the end of the year General Assembly. 2011 ends, and will remain in the Associations history as an important year, when one of the greatest achievements in our history was recorded! We obtained our official legalstatus in July 2011.
Dra Sandra Gutierrez.President. Nicaraguan Society of Plastic Surgery.
62 IPRAS Journal www.ipras.org Issue 7
Here at the Panamanian Association of Plastic, Aesthetic and Reconstructive Surgery (APCPER), having a very small number of plastic surgeons we are currently working on projects relating to academic and social fields. On November 18 and 19 we are holding a smallmeeting in Panama with the attendance of three very important international professors. We named it the “first APCPER Journeys”, where topics in aestheticsurgery will be covered with open discussions of diverse themes. Professors Celso Bohorquez, Gabriel Alvarado and Santiago Umaña from Bogota are attending after
Panamanian Association of Plastic, Aesthetic and Reconstructive Surgery (APCPER)
accepting an invitation by dr. Raul de Leon, president of APCPER. The purpose of the activity is to strengthen academic activities for the APCPER.
Also, “Operation Smile”, Panama Chapter, will be holding its annual mission at the beginning of next year, totaling 21 years of work in the country, offering surgery for the needed with birth and acquired defects.
Dr. Raul de LeonPresidentAPCPER
The Congress of the Paraguayan Society of Reconstructive and Aesthetic Plastic Surgery in Asuncion, Paraguay on September 8th to 10th, 2011.The proceedings took place in a context of warmth and friendship among all the attending local and by foreign surgeons of different nationalities. We had the joy of welcoming colleagues from France, Italy, Spain, Mexico, Brazil, and Argentina.It was nice to exchange scientific and cultural informationin parallel to the numerous scientific contributions.Some of the topics we talked about were, facial
Paraguayan Society of Reconstructive and Aesthetic Plastic Surgery
rejuvenation, rhinoplasty, breast surgery, hair implants, lip and palate surgery, burns etc.The event played a significant role to increasing theglobal knowledge on our specialties and in improving the human quality of the plastic surgeon generally.It is in our plans to continue conducting scientific eventsin partnership with countries of the region as well as the rest of the world.We sincerely thank IPRAS for the support and look forward to all our common future scientific events!
Issue 7 www.ipras.org IPRAS Journal 63
H I S T O R I C A L A C C O U N T S
History can be said to be the story of man’s advances in the world and of the contributions of individuals. Thus, the history of Plastic Surgery can be said to be based on the achievements of individuals, who have advanced their discipline, made contributions to science and, through their work, have allowed evolution to occur in this branch of Surgery. Aristotle, in his work ‘On the Parts of Animals’, said: “Art indeed consists in the conception of the result to be produced, before its realisation in the material”. How true this is of the Art and Science of Plastic Surgery, which has its foundations in the concept of repairing and changing human tissues.As in art, imaginative and creative new ways of looking at surgical problems have pushed Plastic Surgery towards the ever-advancing frontiers of surgery, resulting in “spin¬offs” that have affected many other branches of medicine. We should be grateful to all those surgeons whose innovations have made our speciality what it is today and to those whose vigilance has ensured that standards of excellence are maintained. The origins of Reconstructive Surgery procedures are to be found in Antiquity and hidden in the mists of time. Amazingly, some of the original methods remain in use today. Perhaps those surgeons who have missed out on the experience of “waltzing” a tube pedicle in multiple stages into position or the fixation of a cross-leg flap bythe use of plaster and broom sticks -along with the coating of plaster on the nurses and an irate theatre supervisor on a floor liberally coated with slippery plaster -have beendeprived of some of the joys of the “Early Days”. There were many others, but surgical advances bring changes. But one thing never changes. To produce a result that provides a reconstruction with the minimal amount of scarring in both the area of deformity and the donor site is still the ultimate aim of all Plastic Surgeons. And we can be proud that Surgeons from Australia and New Zealand have made significant contributions toPlastic Surgery, especially from the period following the First World War up until today.
The history of Plastic and Reconstructive Surgery in Australasia
Presented at the RACS AGM Plenary Session “75 Years of Surgical Progress” on the 13th of May, 2002.
Bruce Walton Taylor
In the programme of the Inaugural meeting of our College held in Canberra in March, 1928, what stands out is the number of presentations the subject of which was Plastic Surgery. The first clinical paper was entitled “The PlasticSurgery of the Human Body”. I doubt whether any of us would be so bold as to deliver such a paper today. Henry Newland (later Sir) gave papers on whole thickness skin transplants and pedicle skin grafting. There were others dealing with facial injuries, hand injuries and bums. The Royal Australasian College of Surgeons became a reality 75 years ago. It took another thirty years before the foundation of the “Section of Plastic and Reconstructive Surgeons of the RACS”. Of the 21 Foundation members of the section, 6 were from N.S.W.; 6 from Victoria; 2 from South Australia; 2 from Western Australia; 1 from Tasmania and 4 from New Zealand. Some time should be spent in reviewing some of these individuals and their contributions. However, before doing this, it would be interesting to mention three individuals who, prior to 1928, were carrying out early Plastic Surgical procedures. John Reissberg Wolfe (1823-1904) was a Hungarian Ophthalmologist, who worked in Scotland and was the first to report the repair of lower eyelid defects using fullthickness skin grafts. He practiced in Melbourne between 1889 and 1901 before returning to Glasgow. In 1899, William Moore, a Melbourne surgeon, published “Plastic Surgery”, probably the first book written inEnglish on the subject. He received the first Master ofSurgery degree from Melbourne University and worked at both Melbourne Hospital and St. Vincent’s. And thirdly, Henry P. Pickerill, was a New Zealander from Dunedin, with both Medical and Dental degrees, who had worked in England with Harold Gillies. Following his return to Wellington, he wrote a book on Facial Surgery in 1924. Later on, in 1934, he began annual visits to the Royal North Shore Hospital in Sydney, in the capacity of Plastic Surgeon, that position said to be the first PlasticSurgery post in Australia. He is remembered as the firstsurgeon to use a tube pedicle to close a palatal defect.

64 IPRAS Journal www.ipras.org Issue 7
It was, however, not until shortly after World War Two that Plastic Surgery was truly recognized as a sub-surgical speciality in Australia. At that time working in Australia were Benjamin Rank in Melbourne; David Officer Brown, Kenneth Starr and Basil Riley inSydney; Philip MacIndoe and Llewellyn Swiss Davies in Brisbane; Leslie Le Soeuf in Perth and Henry Pickerill, Bill Manchester, Frank Hutter, Joe Brownlee and Leslie Roy in New Zealand. In 1956 Sir Harold Gillies, a New Zealander by birth and then aged 74, attended the AGM in Christchurch and, believing that the time was overdue, gave great impetus for the further recognition of Plastic Surgery as a Speciality. A letter signed by David Officer Brown,Phillip Macindoe and Benjamin Rank had already been sent to the College in 1950, suggesting the formation of a Plastic Surgery Section. But it took until 1956 before the Section was founded and the inaugural meeting was held in Melbourne in 1957. The 21 Foundation members of the section were: Rank, Newing, Snell, Gunter, Hueston and Wakefieldfrom Victoria Riley, Dey, O’Mara, Gibson, Officer Brown and Starrfrom New South Wales Newland and Robinson from South Australia Le Souef and McComb from Western Australia Stephenson from Tasmania Hutter, Manchester, Brownlee and Roy from New Zealand Some of these surgeons had worked at Sidcup, England, at the Queen Mary’s Hospital, later named St. Mary’s. By 1917, this was a 600-bed hospital devoted to Maxillofacial and Plastic Surgery and was divided into British, Canadian, New Zealand and Australian sections, while later on American casualties were treated as well. Sir Henry Newland, later to become the inaugural Chairman of the newly formed Section of Plastic Surgery, was in charge of the Australian section. Born in Adelaide, be obtained his English fellowship in 1899, after which returned to practice in Adelaide. During World War One he served in the Middle East, Gallipoli and France, before his transfer to Sidcup. For his service he was awarded the DSO. He returned to Adelaide after the war, was awarded a CBE, followed by a Knighthood in 1928 and, amazingly, continued to work until the age of 78. He was the President of the Section of Surgery of the British Medical Association in Australia and of many other organisations. From 1929 to 1935 he was the President of the Royal Australasian College of Surgeons and, even more importantly for us, he was the first Chairman of theSection from 1957 to 1960. The second Chairman of the Section was David OfficerBrown, from 1960 to 1962. A graduate of Melbourne University, he also obtained his MD and MS degrees
from that University. After a period in general practice he obtained the FRACS in 1935. As was the custom, he trained further in the U.K., working with Harold Gillies, Rainsford Mowlem, Archibald McIndoe and T. P. Kilner who had joined Gillies in 1919, and on his return to Australia he confined his practice to Plastic andReconstructive Surgery. When World War Two first brokeout, he worked in the Maxillofacial and Plastic Unit at the 2nd AGH, coincidentally with Benjamin Rank. In 1940 he returned to the U.K. to work with Gillies until 1942, when he rejoined the Australian Army in Alexandria. On his return to Australia he was appointed to St. Vincent’s and RPA Hospitals in Sydney and there he trained many of the Sydney Plastic Surgeons. The third chairman of the Section, between 1962 and 1965 was Sir Benjamin. Rank, a graduate of Melbourne University who gained his English Fellowship in 1938 also came under the influence of Gillies, McIndoe andMowlem (as a matter of interest, all originally New Zealanders). When war broke out, Rank joined the Australian Armed Forces and saw action in Egypt and EI Kantara, before being transferred back to Australia to set up the Plastic and Maxillofacial Unit at Heidelberg Military Hospital in Victoria. In 1946 he took up the first Plastic Surgery postat the Royal Melbourne Hospital. Undoubtedly, Sir Benjamin helped to put Australian surgeons on the international map, being honoured in Great Britain, India, the United States and Canada. He has been a Carnegie Fellow, a Sims Professor and Moynehan Lecturer, as well as presenting the Gillies Memorial Lecture in 1973 and the Syme Oration in 1976. In 1965 he was the President of the British Association of Plastic Surgeons and Chairman of the British Surgical Colleges in 1967. From 1966 until 1968 he was the President of the Royal Australasian College of Surgeons, while in 1971 he was President of the International Confederation of Plastic and Reconstructive Surgeons at the 5th International Congress held in Melbourne, after which he was knighted. Sir Benjamin retired just a few years ago, as the President of Interplast Australia. He was the author of several books and a distinguished painter in oils. William Manchester, the fourth Chairman of the Division, was a graduate of Otago University in 1938. During his service in the New Zealand Army he was sent to England for training in Plastic Surgery under Gillies, McIndoe and Mowlem, after which he set up the Plastic and Maxillofacial Unit near Cairo. He was recalled to Christchurch in 1944 and after his discharge in 1945 he established the first Plastic Surgery Unit at Burwood.More training followed in the UK, after which he returned to Middlemore Hospital in Auckland. Amongst many honours he received a knighthood and

Issue 7 www.ipras.org IPRAS Journal 65
was, importantly, the first Professor of Plastic Surgeryin the Antipodes. In addition, he served as General Secretary of the Asian Pacific Section of the ICPRS andon the Committee of the International Confederation. He was Chairman of the Section from 1964 to 1966. Apart from the distinguished Chairmen we have just profiled, there were other surgeons who deserve mentionbecause of their efforts in establishing Plastic Surgery as a speciality in Australia and New Zealand. It is so easy to take the present status of the speciality for granted, but we owe an expression of gratitude to those who can really be termed pioneers and who worked hard to establish Plastic Surgery as a separate entity.
Kenneth Starr, an honours graduate from Sydney, worked at RPA. He too had worked with Gillies and McIndoe in England before returning to Sydney in 1942 to set up a Maxillofacial Unit at the 13th General Hospital in Concord. Starr was President of the RACS from 1964 -66 and awarded many honours, although he did not confinehis work to Plastic Surgery. He was knighted in 1971. Basil William Birkenhead Riley was born in Sydney in 1885 and served in the First World War as a Lieutenant. He graduated in Medicine from Sydney University in 1923 and trained at Royal North Shore Hospital before moving to London to work with Mowlem and Gillies. Back in Australia his return to North Shore was followed in 1937 by 18 months in Europe and the United States, studying Plastic Surgery. The Second World War saw him working in the Plastic Surgery Unit at Concord Hospital, while at the end of the war he was appointed Surgeon-in-charge at the Royal North Shore Hospital and periphery hospitals. He is remembered with affection by all who knew him. Frank Leo Hutter graduated from Otago University in 1935. He worked in Palmerston North for a while before moving to London, where he spent time in several hospitals, including Great Ormond Street Children’s Hospital, in 1938. In 1940 he joined the New Zealand Army Corps, serving in Plastic Surgery and General Surgery Units. After his discharge in 1945 he worked with Gillies, McIndoe and Mowlem at East Grinstead. On his return to New Zealand, he was appointed Plastic Surgeon to Wellington and Palmerston North Hospitals. In 1952 the unit was moved to Hutt Hospital, from which he retired in 1973 to a farming career. Leslie John Roy was also a graduate of Otago University in 1936. Having worked in Christchurch, he travelled to the U.K. and, like Hutter, he did a stint at East Grinstead, after which he was appointed as a Plastic Surgeon in the West of Scotland. When war broke out, he joined the New Zealand Army Corps, serving in Egypt and Italy. Following his discharge he returned to New Zealand to an appointment at Burwood Hospital in Christchurch.
Philip Hudson McIndoe graduated from Sydney University in 1935 and, after having obtained his fellowship in Edinburgh two years later, was appointed to Prince Henry Hospital in Sydney. During the war he served at Gaza Ridge in Palestine and later in Egypt, Greece, Crete and finally in New Guinea. In 1945 he wasappointed Officer in Charge of the Plastic Surgery Unitat Greenslopes, later working at Brisbane General as a Plastic Surgeon, before changing direction to become Medical Superintendent at Goulbourn Base Hospital in NSW. Llewellyn Swiss Davies was a Melbourne graduate who did his residency at Brisbane General Hospital. During the war he was posted to the Concord Military Hospital Plastic and Maxillofacial Unit, under Colonel K. W. Starr. Later he served in Moratai and Greenslopes in Brisbane. He remained in charge of the Greenslopes unit until after the war, when he became Senior Visiting Plastic Surgeon at the Royal Brisbane and Repatriation Hospitals, as well as the Mater and Children’s Hospitals.
We must not forget Thomas Graham Humby, a colourful and controversial character who was an English 1935 graduate. Whilst still a student at Guy’s Hospital, he modified the skin graft knife then in use, introducing hismoveable roller, which allowed more precise skin grafts. His residency at Guys was anything but dull. He was an understudy to Fred Astaire in “Funny Face”; gained the first gliding certificate in England and representedEngland in international yachting. He joined the British Navy in World War II and trained as a Fleet Air Arm pilot in Florida. The war over, he trained in Plastic Surgery and was appointed to Stoke Mandeville Hospital. Again, he did not restrict his life to surgery but started a freight carrier,”London Aeromotive Service”, using old RAF bombers. A bout of TB, farming in Dorset and a Plastic Surgery practice in the West Indies occurred before he finallycame to Sydney in 1956. He went into practice as a Plastic Surgeon in Rose Bay, concentrating on Cosmetic Surgery, one of the early surgeons to do so. There are many tales about his eccentricities but these must remain untold as it is impossible to confirm their authenticity.Ian Ross Wakefield, known to all as “The Vicar” -what else-graduated in 1941 from Melbourne University, gaining a Masters degree in 1946. During the war he was in the A1F Medical Corps. He obtained his Australian and English fellowships, then carried out Plastic Surgery training in England. Back in Melbourne he worked at The Royal Melbourne, The Royal Women’s and Royal Children’s Hospitals. With B.K. Rank he published a noted textbook on Hand Surgery. He was the first secretary of the Sectionand later its Chairman (1966-1967) Arthur Stephenson graduated from Sydney University

66 IPRAS Journal www.ipras.org Issue 7
in 1941, gaining a Masters Degree in 1949. During the war he served as a Captain in New Guinea and Tarakan. He settled in Tasmania, where he was Senior Plastic Surgeon at the Royal Hobart, as well as consultant to the Repatriation Hospital. Leslie Ernest Le Soeuf was a Melbourne graduate, 1922, obtaining a Doctorate two years later, before travelling to England to obtain his Fellowship. During the Second World War he served with the A1F in Libya, Greece and Crete, being mentioned in despatches, and was awarded the OBE as well as French decorations. He was also a prisoner of war in Germany. He held many official postsin Western Australia and served the Royal Perth and Princess Margaret Hospitals for many years. There were other dedicated surgeons who impacted on the recognition of Plastic Surgery as a separate entity. Men like Richard Newing, John Snell, George Gunter, John Heuston, David Dey, Ted Gibson, Max O’Mara, David Robinson, Harold McComb and Joe Brownlee were all Foundation members of the Section who served the speciality with dedication and enthusiasm and whose contribution is not forgotten. In 1956, following the inception of the Section of Plastic Surgery, the first College Plastic Surgery examination washeld and by 1960 a Sub-Committee on Surgical Training was founded. Due to the increase in trainee numbers in 1970, a Committee on Surgical Training was elected, the chairman being David Robinson of South Australia, Harold McComb of Western Australia and Don Marshall of Victoria. In order that there be regional representation, the Committee was enlarged to include John Williams of New Zealand, Noel Sweeney of NSW, Trevor Harris of Queensland and Arthur Stephenson of Tasmania. Later on there were two additions, Ted Gibson of Sydney and William Manchester of New Zealand. In 1977 the College determined that each speciality should have a board, in order to determine their own destiny, under directions of the College. The first Chairman wasDavid Robinson, who served until 1980. He was followed by John Hanrahan, (1980-84), who later was elected President of the College and Tony Rieger (1984-1987). Originally, most of our Plastic Surgeons received their training overseas. When Plastic Surgery residency posts first became available in our public hospitals, trainees wereselected by the hospital and normally remained in one place throughout their training. However, in 1987, it became obvious to the Board that this restriction to one hospital offered a limitation of experience. To ensure exposure to all facets of Plastic Surgery, a hospital rotation system was introduced, with the selection of the trainees being made by a sub-committee of Plastic Surgeons in each state on behalf of the Board, instead of the hospital administration. Regional sub-committees were set up, reporting to the Board. These sub-committees kept close contact with
trainees who were selected on a state-by-state basis. Since 1990, the continuation and approval by the Board in Plastic Surgery is required for each trainee. Regular inspections of hospital training posts are carried out by board members to ensure they fulfil the requirementsfor the teaching programmes. On completion of their training and the RACS exam, many go overseas for further experience in centres of excellence, chiefly inNorth America, the UK or other European destinations. In 1979 David David suggested annual week-long courses for trainees and these have been held in different centres since 1980. The late sixties and early seventies saw the beginning of many changes in the delivery of health care in Australia. Because the College of Surgeons is responsible only for training and standards and does not deal in the political and financial aspect of practice, the Australian Society ofPlastic Surgeons was incorporated in 1971 to deal with such matters, in an environment of constantly changing ground rules. A similar Society was founded in New Zealand. ASPS is open only to Fellows who fulfil thePlastic Surgery training and examination standards laid down by the College. An application was made in 1974 for establishing Armorial Bearings for the Society. In 1976 a Grant of Arms was made by the College of Heralds in London. The Kings of Arms noted that “the elements of the grant symbolise the essence of Plastic Surgery in the most pleasing and truly heraldic manner”. In 1998 the decision was made to dissolve the Division. However, while ASPS is now the sole body covering the day to day matters of the Specialty, all training and standards remain, as it always had, under the auspices of the College via the Board in Plastic Surgery. As specialisation in individual aspects of Plastic Surgery became more widely spread, the Aesthetic Society of Plastic Surgery was formed and Plastic surgeons also joined various hand, head and neck and burn societies, while small study groups continued to meet. As we have seen from the very early days of the speciality, Australasian surgeons have trained and made their mark overseas. Internationally, following the Second World War, Plastic Surgery as a speciality was gaining momentum. In 1955 the first Congress of the InternationalConfederation of Plastic and Reconstructive Surgery was held in London, coincidentally the year after two Americans from Boston, Joe Murray, a Plastic Surgeon, and Hartwell Harrison, performed the first human kidneytransplant in the world. Since that time, the Congress of the International Confederation of Plastic and Reconstructive Surgery has been held every four years. In 1971 the Meeting was held in Melbourne, under the chairmanship of B.K. Rank, while next year the Congress will again come to Australia, to

Issue 7 www.ipras.org IPRAS Journal 67
Sydney. Australian Surgeons have played an active role in the International Confederation with representatives on the central Committee and the Asia Pacific section.Over the years since the inception of the College, great advances have been made in Plastic Surgery. In Paediatric Surgery, for example, craniofacial procedures, genitalia correction, velopharyngeal procedures and improvements in cleft lip and palate offer new hope for children born with congenital abnormalities. Victims of trauma can receive replacement of severed body parts such as fingers, hands, scalps and ears, whilethe treatment of burns sees an ongoing quest for ever better methods of skin culture and grafting and post burn scar relief. Breast reconstruction, as well as reduction and augmentation, the treatment of male and female genital abnormalities and of facial palsy are only some of the areas in which plastic surgery advances provide a better and more normal life to patients. With the use of the surgical microscope, osseointegration, plate fixation,tissueandboneexpansion,musculocutaneousflaps, free flap transfers, muscle and nerve transpositionand transplantation, vascularised bone grafts and bone substitutions, we have reached results in reconstruction undreamed of 75 years ago. The elixir of eternal youth or a magic wand have not yet been developed but the subperiostal face lift, brow lift, hair micrografting, liposuction, laser surgery, implants, collagen, abdominoplasty and so on offer ways of defying the physical signs of ageing or creating a new image for the patient. Many surgeons from the Antipodes have made significantcontributions on the International scene. Moore, Pickerill, Rank, Wakefield, Hueston, Thompson, David, O’Brienand Morrison have written well known textbooks, while they and others have contributed chapters to Plastic Surgery literature worldwide. B. K. Rank, Ian Taylor, Wayne Morrison, Bernard O’Brien, to name just a few, have been major presenters at International Meetings. Some of the World’s first microsurgery procedures werecarried out and reported in Australia. Let’s look with pride at these examples. Replacement of completely severed digit (P.G.
Lendvay and E.R Owen:1970) The first Free Transfer of tissue by vascular
anastomosis (G.I.Taylor and RK. Daniel: 1973) The free vascularangeal bone graft (G.I.Taylor,
G.D.H. Miller and F.1. Ham: 1975) Replantation of an avulsed scalp by microvascular
anastonosis (G.K.H. Miller, E.1. Anstee and J.A Snell: 1976)
*The iliac crest free flap (G.I. Taylor, P. Towns and RCorlett: 1979)
Replantation of a completely avulsed ear (D.G. Pennington, M.F. Lai and AD. Pelly: 1980)
“Wrap around” toe to thumb transfer for reconstruction(W. Morrison, B. O’Brien and A MacLeod: 1984)
Since 1974 the B. K. Rank Travelling Professorship has been awarded annually, to a distinguished Plastic Surgeon from an overseas centre of excellence. The list reads like the Who is Who of the speciality. But it has not always been one sided. Australian Plastic Surgeons have been awarded Overseas Visiting Professorships and, particularly in the Asia Pacific region, have servedto benefit the hospitals in their host nations.In addition, overseas visits by groups of Plastic Surgeons from our area have been well organised and visits to centres in the United States, China, India and Russia have led to great interchange of ideas. Until recent times, there were no professorial appointments in Australia, however Wayne Morrison was the first such appointee and is now Professor ofSurgery at St. Vincent’s Hospital, Melbourne. The firstacademic Chair in Plastic and Reconstructive Surgery is held by Michael Poole in Sydney at St. George Hospital. The University of Auckland New Zealand appointed Sir William Manchester Professor of Plastic Surgery in 1977, the first such appointment in our area.It should also be noted that a federally funded Craniofacial Unit exists in Adelaide, under the Chairmanship of David David. However, there are other Craniofacial units in other Plastic Surgery departments. These all draw patients, not only from Australia, but from countries near and far. Here we must make mention of Interplast Australia, which is a medical relief organisation initiated in 1983, which sends Australian Plastic Surgery teams to some twenty different areas throughout the South Pacific. These teamsconsist of two Plastic Surgeons, an Anaesthetist and nurse, all volunteers. Procedures are carried out in the field butthere have been some forty five patients who have beenbrought to centres in Australia, while approximately forty eight doctors and nurses from eleven different areas have secured valuable experience here, which they take back to their country of origin. Since 1983, 286 teams have examined over twenty thousand patients and carried out over twelve thousand operations, assisted by local medical and nursing staff. As previously mentioned, Sir Benjamin Rank was the first President of Interplast, followed by Don Marshall.When Plastic Surgery was first officially recognised as a Surgical Speciality by the College in 1956, there were just 21 qualified Surgeons. Last year, 2001, there were 257.Like all other surgical groups, Plastic and Reconstructive Surgery has had its problems; a lack of realistic level of visiting medical officers, shortage of Hospital beds and

68 IPRAS Journal www.ipras.org Issue 7
lack of funding and facilities for research and training posts. As we look back into the history of Plastic Surgery in Australasia, we see that it is indeed an example of the participation of individuals in advancing a field ofmedical science. Time does not allow me to name all the many Fine Plastic Surgeons who have contributed to and received recognition for their part in the development of their speciality. Not all innovations have made their way into textbooks but many have been shared with students and fellow Surgeons in the operating room
SELECTION OF FOUNDATION MEMBERS OF THE PLASTIC SURGERY SECTION OF RACS
or via meetings, such as the one being held this week. There is no doubt that the advances in all branches of this Surgical Speciality have been rapid and the future is very encouraging. The progress that Plastic Surgery has made throughout the world and especially in our area during the past few decades has been remarkable. Plastic and Reconstructive Surgery is truly at the forefront of the advancing frontiers of Surgery. Just as truly, it has played an important part in the history of the development of medical care in Australasia.
I-r: J.A. Snell, B.K. Rank, G. Gunter, J.T. Hueston, A.R. Wakefield, B.W.B. Riley, D.L. Dey, M.L. O’Mara, E.W. Gibson, D. Officer Brown, K.W. Starr, H. Newland, D.N. Robinson, H.K. McComb, A. Stephenson,
W. Manchester, LJ. Roy. Not appearing: F.L. Hutter, L.E. Le Souef, R. Newing, J. Brownlee.
PLASTIC SURGEONS WHO HAVE BEEN RACS PRESIDENTS
Sir Henry Newland1929-1935
Mr Kenneth Starr1991-1993
Sir Benjamin Rank1964-1966
Mr John Hanrahan1966-1968
OTHER MEMORABLE PLASTIC SURGEONS
H.P. Pickerill, L.S. Davies, P.H. MacIndoe, T.G. Humby, J.R. Wolfe
Issue 7 www.ipras.org IPRAS Journal 69
A combined historical account of Plastic Surgery in India and the
Association of Plastic Surgeons of India
Just as the Sun rises in the East, the science of Plastic Surgery first dawned in the ancient Indian civilization. InIndia, from the beginning of recorded history, offenders or sinners were punished with mutilation or severance of the nose, ears or parts of limbs. Indian mythology and history are replete with stories of Surpanakha and Nakatapore i.e. ‘City without Nose’. Moreover, in India the nose is considered to be the organ of respect and reputation, hence plastic surgical procedures to correct these deformities were a necessity.The first detailed description of plastic surgical proceduresis found in the clinical text on Indian Surgery, the ‘Sushruta Samhita’ (circa 600 B.C.). Atharva Veda, the root of Ayurveda, the classical text of Indian medical knowledge, includes two seminal texts, Charaka Samhita, on medicinal aspects and Sushruta Samhita, which incorporates details of surgical tools and operative techniques. Sushruta wrote this treatise based on the lectures of his teacher, the famous surgeon king, Devadas (‘incarnation of Dhanwantari, the Divine Physician). In the fourth century A.D. Vagbhat, an Indian Physician, recounted the plastic surgical procedures with more details than provided in Sushruta Samhita. In his book, ‘Astanga Hridyans Samhita’ he credits the techniques to Maharishi Atreya. It is interesting to findmention of plastic surgical procedures such as rhinoplasty, otoplasty, tissue grafting, organ transplants, transfer of embryo, cross-grafting of head and reattachment of limbs etc. in these ancient Indian Medical Treatise and Puranic Literature. The gradual decline of this golden era of Hindu Surgery began at the time of Buddha (562- 472 B.C.). Buddhist scripture Mahavagga Jataka enforced strict prohibition on Surgeons and Manusmriti prescribed special rituals for their purification. Contemporary teachings, basedon Ayurveda, basically supported medicinal treatments. Ayurveda forbade surgery, as contact with blood and pus was considered polluting. Hence, during this period, these great surgical skills were delegated to lower castes like ‘Koomars’ or potters, who were known for their manual dexterity. They kept this valuable knowledge alive and passed it from father to son, as a family secret. Some of these families were identified in the latter halfof eighteenth century. Marathas of Pune, Kangharias of
Kangra (Himachal Pradesh) and some families in Nepal were practicing ancient Indian surgical skills; most notable amongst them being midline forehead rhinoplasty. In Kangra, forehead rhinoplasty had been practiced for centuries by a family of Hakim nose surgeons called ‘Kanghiaras’. They had been operating in Kangra since the time of Raja Sansar Chand (1440 A.D.) and had also obtained certification from Mughal kings. Hakim DinaNath Kanghiara was the last surviving descendent of the family, known to have performed such an operation. Details of their surgical skill appeared in Punjab Medical Journal in 1967. Later still, Dr. Tribhovandas Motichand Shah, the then CMO of Junagadh is said to have performed 400 rhinoplasties by forehead flap.In fact, India and Egypt are considered as the fountain-heads from which the stream of knowledge flowed tothe Middle East, eventually to reach the Mediterranean civilizations; the Greeks and the Romans. The ancient Indian medical knowledge was carried into Greece and Arabia by Buddhist Missionaries. Further still, avenues of trade were set up between Greece and India following the conquests of Alexander ‘The Great’. Arabs played an important role in transmitting the surgical knowledge to the West. The Persian hospital at Gandi-Sapor (6th – 10th century A.D.) was a great learning centre of that era, permitting the amalgamation of Hindu, Greek and Arab schools of thought. Here, the Sushruta Samhita was translated into Arabic and later into Latin. Arab physicians of that time, Rhazes and Aviceruna, often referred to the teachings of Sushruta and Paulus Aegina. Paulus Aegina was a 7th century physician who was responsible for the integration of Indian and Western surgical knowledge and summarized it in a seven-volume compendium. Further down the timeline, Aulus Cornelius Celsus (25 B.C.) propagated this science to Rome in his book ‘De Re Medica’. During 525 A.D. the Christian Orthodox Church started rising and the enthusiasm towards surgery declined. Surgical skills were now reared in the hands of people of lower status like barbers, a situation similar to what had happened in India centuries ago. Sushruta Samhita was translated into English by Kariraj Atrideo Gupta Vidyalankar Bishangar (1950) and Kaviraj Kunjalal Bhishagranta (1963).

70 IPRAS Journal www.ipras.org Issue 7
Despite these hurdles, reconstructive operations of the nose and face received an impetus in the European countries during the 19th century. The German, French and English Surgeons were introduced to the older Indian method. During that period, certain German scholars who studied the original text in Sanskrit, British surgeons and French travelers, who saw for themselves the rhinoplasty operations performed in India, revealed the wonders and practical possibilities of this specialty to the Western world. It was, however, the discovery of anaesthesia (Morton, Long and Wells) and anti-sepsis (Lord Lister) which revolutionized the practice of surgery and made it painless and infection-free. Modern Plastic Surgery in India started after World War II. During the war, there were a couple of British Maxillofacial Surgery Units and a special mention was made about them by Mr. Tom Gibson (Canniesburn Hospital) at Bangalore and by Mr. E.W. Peet at Pune, during their visits to India. This kindled the interest in Plastic Surgery among a few young Indian surgeons working then with the armed forces as “temporary commissioned officers”. After thewar, two of them, Dr. C. Balakrishnan and Dr. R.N.Sinha, specialized in Plastic Surgery, while Major Sukh pursued his interest in the specialty as a pioneer in the field ofPlastic Surgery at the Armed Forces Medical College and Hospital, Pune. Plastic Surgery did not exist as a recognized specialty in the country. While in training at Stoke Mandeville Hospital, U.K., Dr. C. Balakrishnan sent a memorandum to the Director General of Health Services, New Delhi, proposing the development of a Department of Plastic & Maxillofacial Surgery, because there was a crying need for at least one such department in the country. After great persuasion, he was offered the post of Lecturer and Surgeon at Medical College and Hospital, Nagpur (at that time known as the Central Provinces of Madhya Pradesh and Bihar State). He accepted the offer and started to develop a Department of Plastic and Maxillofacial Surgery. Dr. R.N. Sinha, who was trained under Prof. Kilner, on his return to Medical College, Patna (Bihar State) made pioneering efforts to educate surgical colleagues, State and Central Government and the Medical Council of India about the need to develop Plastic Surgery as a specialty. He wrote numerous articles in scientific journals and lay press to drive homethe point. This indeed was a great task, since there were no books or literature available to read, learn from and receive guidance about the new specialty. During those days, even minor progress was very difficult, because thedevelopment of specialties was generally frowned upon and frankly discouraged by General Surgeons. Slowly, even the patients started realizing that a person who concentrates in one field, does much better than one who
is a “jack of all trades and master of none”. It required all the tenacity and dedication of a handful of pioneer Indian Plastic Surgeons, who made Plastic Surgery their career, to overcomethe initial difficulties. For almost 8to 10 years, these pioneers at Nagpur, Patna, and later at Lucknow, Bombay and Calcutta, struggled hard for their existence and worked as sections in the departments of General Surgery.Dr. N.H. Antia, after his post-graduate training in Plastic Surgery in the U.K., started working in a private hospital in Pune and was also engaged in Rehabilitative Surgery at the ‘Kandhwa Leprosy Centre’ outside the city. He carried drums with sterilized linen and instruments from Pune to the leprosy centre. Dr. Antia worked here in a makeshift O.T. on absolutely voluntary and honorary basis in spite of considerable hardship. His pioneering work on leprosy was rewarded by an invitation from England to deliver the Hunterian Lecture at the Royal College of Surgeons, London in 1955.Sir B.K. Rank visited India from Australia, on a goodwill mission under the Colombo Plan to advise the Government of India and his own Government about the possibilities of developing Plastic Surgery in India. He spent two weeks in India and recommended the development of a Centre of Excellence at Nagpur, under the dynamic leadership of Dr. Balakrishnan. This was to be aided up to 50% under the Colombo Plan and the rest to be granted by Central and State Governments. Unfortunately, the plan never materialized. However, the first independentDepartment of Plastic Surgery in the country was finallycreated at the M.C. Hospital, Nagpur, in 1958.By 1955, there were about four to five Plastic Surgeons,devoting their full time to this specialty and there was a desire to form an Association. Thus, in the Annual General Body Meeting of A.S.I. (Association of Surgeons of India) held in December, 1956 at Indore, Dr. R.N.Sinha required a resolution to this effect. A sub-committee was formed with Dr. C.P.V. Menon of Madras as its Chairman and Dr. R.N. Sinha as the Convener to frame By-laws and Regulations for an Association of Plastic Surgeons of India - as a Section of Association of Surgeons of India. However, it was only in December 1987 that APSI became a Registered Society with the government.In the year 1957, considerable interest was created in Maharashtra, following the visit of Sir Harold Gillies. He was pleasantly surprised to see deformities being treated by tube pedicles and other modern techniques of Plastic Surgery. He applauded the excellent work that Major Sukh was doing in the field of Rehabilitative PlasticSurgery at the Armed Forces Medical College, Pune. It was not only an eye-opener for all, but a surprise to Dr. Gillies himself. Many war casualties needed extensive stay in his unit for such procedures of rehabilitation. Sir Harold Gillies also demonstrated various operations and

Issue 7 www.ipras.org IPRAS Journal 71
techniques at Kandhwa Leprosy Centre, where Dr.N.H. Antia was working. Dr. Gillies, as the founder of modern Plastic Surgery, was keen to propagate knowledge in this specialty in one of the most populous countries of the world. He visited and lectured at several centers in the country including Nagpur, Calcutta, Delhi, Patna and Jaipur. At Nagpur, in December 1957, he inaugurated the Association of Plastic Surgeons in India - as a section of A.S.I. The Association elected the following officebearers:
Dr.R.N.Cooper President
Dr.C.Balakrishnan First Vice-President
Dr.R.N.Sinha Founder Secretary
Dr.R.N.Sharma Founder Members
Dr.N.H.Antia Founder Member
Dr.Hirdeis Founder Member (ENT Specialist from Bangalore)
This was indeed a great historic moment and Dr. Gillies was made the first Honorary Member. Dr. Gillies stayedin India for about three months and, before leaving for England, he insisted on a token payment of Rs.100/- to Dr. Antia, as an inspiration to continue his efforts in establishing a Department of Plastic Surgery at the Government Medical College in Bombay. This proved to be a great morale booster and the first unit of PlasticSurgery started at J.J. Hospital, Bombay in December 1958 with Dr. Antia as its Head.
A Burns and Plastic Surgery Unit was established in 1961 at K.E.M. Hospital, Bombay, by Dr. Charles Pinto. Mr. E.W. Peet of Oxford was a regular visitor to this unit. The first summer conference of the Association washeld at Nagpur in 1964. The most outstanding feature of the conference was the brilliant presentation on the classification of cleft lip and palate by Prof. C.Balakrishnan; now known throughout the country as The Nagpur Classification. The first batch of post-graduatestudents trained in our country appeared for their examination from Nagpur and Patna Universities in 1962 and 1963 respectively. In 1963, the Government decided to start a Department of Burns, Plastic and Maxillofacial Surgery at Safdarjung Hospital in Delhi. Dr. J.L. Gupta had the honour of starting and developing this unit which, by sheer hard work and dedication, became a major unit of Plastic Surgery in India in a very short time. In 1964, during the first Post-graduate Medical EducationConference, convened by the Medical Council of India, under the Chairmanship of the then Union Minister of Health Dr. Sushila Nayyar at Delhi, the first curriculumand physical standards for MCh postdoctoral training in Plastic Surgery was drafted.In 1967, Dr. R. N. Sharma represented our Association at the International Meeting held in Rome, and thus, APSI joined the International Confederation of Plastic Surgeons. By December 1967, the Association had grown to about 66 members (including 37 full members). By 1968, we had 11 plastic surgery centers in the country at Nagpur,
Inaugural ceremony of IPRAS 2009 at Siri Fort Auditorium on 29th Nov 2009. (L-R Dr. G. Balakrishnan, President APSI, Dr. Suresh Gupta, President IPRAS 2009, Dr Marita Eisenmann-Klein, Secretary General IPRAS, Dr. Kiran Walia, Chief Guest and Minister of Health in
Government of Delhi, Dr. Rajeev B. Ahuja, Chairman IPRAS 2009, Dr. Rakesh Khazanchi, Secretary General IPRAS 2009).

72 IPRAS Journal www.ipras.org Issue 7
Patna, Lucknow, Bombay, Pune, Delhi, Chandigarh, Patiala, Madras, Madurai and Calcutta. In the last four decades there has been a tremendous growth of Plastic Surgery. The number of teaching centers has increased in the country and today hardly any student is going abroad for basic Plastic Surgery training. The Association has established several traveling fellowships for training within and outside the country (appendix I), as well as several Professorships (appendix II). A few specialized centers of excellence for management of burns, Hand and Micro-vascular Surgery, Craniofacial Surgery and Aesthetic Surgery also developed, in different parts of the country, by dint of hard work and special interests. The Indian Journal of Plastic Surgery started in 1981, in order to bring together all the professionals involved and to disseminate and advance their knowledge. Very proudly, IJPS (India Journal of Plastic Surgery) is now a popular journal, indexed with Medline and publishing papers from across the world.There are about 800 Full members and 150 Associate members of APSI today.
India had the privilege of hosting the IXth and the XVth Congresses of IPRAS in Delhi, in 1987 and 2009, respectively. Dr Suresh Gupta and Dr Rajeev B. Ahuja, respectively, were principally responsible for the organization of the events. Both the events were a huge success, with the delegates who enjoying the Indian hospitality. APSI also has the privilege of giving two Secretary Generals to the Asia Pacific Section of IPRAS; Dr B.M. Daver (1997-2001) and Dr Rajeev B. Ahuja (2009-2013).APSI has recently established a Humanitarian activity corpus and the interest from this will be available to any APSI member to use for a humanitarian project in the country. APSI has also leaded in proposing and observing July 15th as the Plastic Surgery Day, when all Plastic Surgeons are urged to contribute free services to the needy in their Region. IPRAS has promised to propagate this concept. APSI has also started professional development courses, which are topic-based and held three times a year, rotating across the country. They are delivered at no cost to students and APSI members, through sponsorship from Ethicon. These courses are extremely popular and have been a huge success.
Past Presidents of APSI during APSICON at Goa in 2010. (L-R Dr K.S. Sekhar, Dr N. Pandya, Dr V. Bhattacharya, Dr Suresh Gupta, Dr Mukund Thatte, Lt Gen L.P. Sadhotra, Dr Rajeev B. Ahuja, Dr K. Sridhar, Dr. Rajasabapathy)

Issue 7 www.ipras.org IPRAS Journal 73
The upcoming events of the APSI are:
20-22nd Jan 2012 ISAPS Course, Goa
19-20th Feb 2012, APSI-Ethicon accredited course on Reconstruction in Abdominal & Trunk.
27-29th April 2012, APSI-Ethicon accredited course on Basics in plastic surgery.
2-3rd Nov 2012-Preconference APSI-Ethicon accredited course in cleft surgery. Lucknow
6-8th Nov 2012 Main APSICON Conference, Lucknow
4-8th March 2013, World Congress of IFSSH
The current Executive members representing APSI:President: Dr A.K. SinghPresident Elect: Dr Ashok GuptaImmediate Past President: Dr Raja SabapathySecretary: Dr Atul ShahTreasurer: Dr Sailesh RanadeEditor: Dr Surajit BhattacharyaCouncil Members: Dr.B.G. Tilak, Dr Amresh S. Baliarsingh, Dr Nitin Mokal, Dr Ravi Mahajan, Dr Subramanian Iyer, Dr Hari VenkataramaniTrustees: Dr K.S. Sekhar, Dr J.K. Sinha, Dr K. Sridhar, Dr Suresh Gupta, Dr Rajeev B. Ahuja
Appendix I.1. Ethicon Plastic Surgery Traveling Fellowship
2. Ethicon traveling fellowship in Microsurgery
3. Ethicon cosmetic surgery traveling fellowship
4. R.G. Saraiya international fellowship –
5. Brig. Kathpalia fellowship in hand surgery
6. Myovatec fellowship for training in Plastic surgery
7. Vasudhan Arjin Fellowship in Laser Surgery
8. APSI sponsorship to attend APSICON
9. IX IPRAS Congress fund international traveling Fellowship.
10. IX IPRAS Congress fund national traveling Fellowship.
11. K.E.M. Microsurgery fellowship
Appendix II.1. Plastic Surgeon of the Year award – from DR KS
Shekar endowment
2. Honorary Membership Award
3. Ethicon Visiting Professorship in Plastic Surgery
4. Ethicon Visiting Professorship in Microsurgery
5. Ethicon Visiting Professorship in Cosmetic Surgery
6. Gen. N.C Sanyal - Armed Forces Professorship
7. Peet Prize for best presentation during Annual Congress in Award category
8. Kilner Essay Award
9. APSI Junior Best Paper Award at Annual congress.
10. McNeil audio-visual award for best presentation by a junior plastic surgeon at Annual congress.
11. Kammath Memorial prize for best poster during Annual congress.
12. N H Antia award for best publication from India.
13. Army Endowment for best report.
14. R. N. Sinha award for best paper Published in IJPS.
Contact for APSIDr. Atul Shah, Secretary APSI20, Om Park, Near Andhra Bank, Stadium Road, Akota, Baroda. Gujrat 390 020, IndiaPh: +919825033832 ; +912652321769E-mail: [email protected]; [email protected]; http://apsi.org.in
Dr Rajeev B. AhujaTrustee and Past President of APSI

74 IPRAS Journal www.ipras.org Issue 7
It is an interesting coincidence for me that this article is written just on the 50th Anniversary of the Turkish Society of Plastic Surgeons. The society was founded in 1961.The history of Turkish Plastic Surgery goes back to the 8th century. German scientists found 64 Turkish manuscripts, dated 1902 – 1914 years ago, in the Sincan region of “East Turkistan” (in present-day north-western China, where Uygur Turks live). These are the oldest documents in Turkish and Turkish Plastic Surgery 1,2,written in three different alphabets: the Uygur version of the Sogd alphabet, the Brahmi alphabet of Indian root and the Nestori/Suryani alphabet 1,2. They are kept in the Brandenburg Academy of Science in Berlin and consist of mostly traditional medical documents, dealing with subjects including nasal tumors, fascial palsy, head and neck tumors, skin lesions, wound healing and other plastic surgical problems.
At the beginning of the 13th century, the first Turkish Medical Book “Tuhfe-I Mübarizi” was written in Turkish by Hekim Bereket8.As it is known, the first University was founded in Istanbul in 1453, just after the conquest of the city by the Ottoman Turkish Empire. Şerefeddin Efendi of Amasya 3,4,5,6 was a pioneer in Turkish Plastic Surgery and he published a superb and beautifully illustrated surgical book, named “Cerrahiyyetü-l Haniyye3 in 1465, written in the Turkish language. He described many different techniques and he demonstrated these techniques with 140 diagrams in his two-volume book. Most of the cases were related to congenital problems and trauma. Additionally, gynecomastia, hermaphrodism, mandibular subluxation, and carcinoma of the lip, etc. were also described.In the 15th century, Mümin bin Mukbil16 from Sinop, described techniques for the treatment of diseases and coloured lesions on the eyelids and orbital region; in
History and present situation of Turkish Plastic Surgery
50th Anniversary of the Turkish Society of Plastic Surgeons
Prof. Ibrahim Yıldırım MDPlastic, Reconstructive and
Aesthetic Surgery Department, Cerrahpaşa Medical Faculty,
İstanbul University, İstanbul Turkey
All documents were read by Ord. Prof. Reşid Rahmeti Arat (Gabdul Raşid Rachmati Arat) in Berlin.Most of the Turkish physicians often used to work on more than one subject and the languages of the scientific arena at that time were Arabic and Persian 4. One of them was AviCenna 4 (Ibn-i Sina) (980 – 1037) from Harmaysan, near the Buhara; in his well-known book “Tıp Kanunu” (Law of the Medicine) he gave details about “Ectropion and Entropion” and the muscles of the eyelids.
addition, blepharoplasty and special surgical instruments for these procedures as well.After the “decline of the Ottoman Empire”, new understandings and modern establishments brought new horizons to medicine. The first modern school of medicine7 was established in 1827 in Istanbul by Sultan Mahmud. The Second one was a military medical school 9,10. In order to be able to relate to the Western World, the teaching language was converted to French, starting in1839 and,
TPCD
Issue 7 www.ipras.org IPRAS Journal 75
accordingly, the methodology of teaching was mostly French. This school was re-organized in 1866 – 1867, and the linguafranca was converted to the native language; the school was re-established with a civil section11. This was a very satisfactory situation; at the end of the 19th Century, there were many very well-trained phyicians.It is possible to see some plastic surgical articles17 in the of “Tıb Cemiyeti Mecmuası” journal (the Medical Journal) between 1856 and 1906, such as “Tagliocozzi Procedure for the Repair of the Nose”, “Cleft Lip and Palate repair”, “Eyelid operations”,“Indian Flap for Nasal Reconstruction (1858)”, “Partial resection of jaws (1868)”,“Epidermo-dermal Graft Application (1872), “Ollier-Thiersch Graft (1885) etc.The first modern literature in Plastic Surgery apperared during this period. Dr.Cemil Topuzlu12 presented 120 plastic surgical cases, among his series of 758 surgical cases, between 1893 and 1897. He was the first surgeon in the world to recommend “Z-Plasty” for contractures of the Achilles tendon12 and to use sutures to repair arteries.The period between the two World Wars was an excellent time for Plastic and Reconstructive Surgery, both at home and abroad. It is important to mention Dr. Cafer Tayyar Kankat, Dr. Şerif Korkut and especially Dr. Halit Ziya Konuralp, who were the pioneers of modern Plastic Surgery in the country at that time. Dr. Kankat13,14 performed many reconstructive and aesthetic operations; the first Turkish Journal of Plastic Surgery was published by him under the name of “Modern Cerrahi ve Nöroşirürji (Modern Surgery and Neurosurgery)” in three sections: General, Neuro- and Plastic Surgery, between 1936 and 1947.Dr. Kankat14 published “The First Penile Reconstruction”, “Cartilage Grafts for Impotence”, and aesthetic operations such as “Face Lifting”, “Rhinoplasty” and “Abdominoplasty” etc., in this journal. Later on, in 1953, he started publishing the first journal purely for Plastic Surgery under the title “Plastik, Reparatris ve Estetik Şirürjisi”.Dr. Konuralp15,18 performed many reconstructive surgical techniques, which he had learned from the book by Kirschner and Nordmann (1927) and published several papers in surgical journals between 1930 and 1935. Dr. Konuralp founded the first Plastic Surgical Ward in Turkey in 1938. It had 49 beds and was under the Department of General Surgery in Istanbul University Hospital. The first teaching program in Plastic Surgery was started at that time. Many very well-known Plastic Surgeons visited this clinic. They included Maliniac (USA), Rose Tilley (Canada), John Conley (USA), Heuser (Germany), Milton Freeman (USA), Griffith (USA), Polzer (USA), McDowell (USA), Schimitzu (Japan), Organe (UK), Broadbent (USA), Kilner (UK), Matthews (UK), Longacre (USA) , Skoog (Sweden), Bardach (Polonya) and others. These individuals visited at various times. In one occasion, Dr. Kilner invited Dr. Konuralp to England, where he spent time with Gillies, McIndoe, Kilner, Mowlem, Matthews, Barron, Osborne, Peet, Reidy, Dennis Brown and Sedden. His first book was published in 1952, entitled “Main Priciples in Plastic Surgery”2. He was also one of the eminent Plastic Sur geons of the fırst IPRS Congress in Stockholm, in 1955.
The second Plastic Surgery center was founded in the Military Medical Academy11in Ankara, in 1943, as “Jaw Surgery Center”, by Dr. Necdet Albay, but later, in 1958, it was changed to the “Maxillofacial and Plastic Surgery Department” by Dr.Cihat Borçbakan19. As it has been mentioned previously, the Turkish Society of Plastic Surgeons7 was founded in 1961 in Ankara. The founders were eight Plastic Surgeons, two general surgeons, and two ENT Surgeons. The first president was Dr. Konuralp from Istanbul.The first National Meeting18,19 of this society was held in Ankara and Tord Skoog from Sweden was the honorary guest and speaker. Afterwards, the first Skoog fellow was sent to Upsala. The International Association of Maxillofacial Surgeons was founded in Leipzig and Dr.Konuralp was founder and elected vice-president in 1970.Turkish Plastic Surgery Society has organized National Meetings every two years, and, in 1983, a Symposium was added to the program. Since 1988, a National Meeting and Symposium have taken place each year. Some combined meetings and courses were arranged together with other countries, such as the Turkish – French (Istanbul 1980), Turkish – Greek (Athens1988) and several Aesthetic Surgery courses of ISAPS, as well as Hand Surgery courses held in different cities of the country.The Sixth European and the Fifth Asian – Pacific Congresses were organized by the Turkish Society in Istanbul in 1989.Dr. Güler Gürsu from Turkey was the President of ISAPS between 2000 and 2002 and she was also the President of the World Congress of ISAPS, which was held in Istanbul in 2002. Over the past twenty years, new establishments like the Turkish Society of Aesthetic Plastic Surgeons, the Society of Interplast Türkiye, the Society of Hand Surgeons, the Society of Maxillo facial Surgeons, the Society of Aesthetic Face and Nasal Surgeons and the Society of Reconstructive Microsurgeons have become closely affiliated with the Turkish Society of Plastic Surgeons. Interplast Türkiye has, so far, offered its services to nearly 40 countries.There is a two-step national examination twice a year to enter the specialty training. The first step is a foreign language exam, the second part a professional exam, similar to the USMLE in the USA. This is a fairly competitive exam. After passing the exam, medical doctors earn the right to enter to the specialty programme. In Turkey, the total training time in Plastic Surgery is five years, including rotational programs in General Surgery, Pediatric Surgery, ENT, Orthopedics and traumatology, Neurosurgery, Anaesthesiology, Emergency Medicine and Anatomy.At the end of the five years residents, must have prepared a thesis, which is an experimental or a clinical research study, conducted under the instruction of a tutor. The candidate must take an examination to earn the specialty diploma, which consists of three steps: 1. Thesis must be accepted by jury members 2. An oral examination organized by jury members. 3. A practical examination in the operating room with a

76 IPRAS Journal www.ipras.org Issue 7
Halit Ziya Konuralp1903 –2005
Cihat Borçbakan1912 – 1991
Cemil Topuzlu1866 – 1958
Cafer Tayyar Kankat1895 – 1955
random choice of cases, watched by the jury members. The jury members are three lecturers from Plastic Surgery and two lecturers from any other of the close specialties like ENT, Paediatric Surgery, etc.The first specialty exam for Plastic, Reconstructive and Aesthetic Surgery took place in 1965. Training centers are allowed to conduct this exam on behalf of the Ministry of Health. Diplomas are awarded after successful examination. Any specialist with this diploma is entitled to have a practice, either in one of the official institutions or in the private sector. The public still looks at Plastic Surgery as Aesthetic Surgery. That is why this field is highly popular.Nowadays, we have 53 training centers all over the country, in University and State Hospitals. There are around 900 Plastic Surgeons and nearly 300 residents for a 75-million population. Unfortunately, some Plastic Surgeons are not members of the Society. There are “Hand Miocrosurgery Centers” in the large cities, mostly in the private sector and in University Hospitals.There are “Burn Units” in different centers, but not enough for the country.We owe thanks to Cemil Topuzlu, Cafer Tayyar Kankat, Halit Ziya Konuralp and Cihat Borçbakan who were the leading Surgeons in the development of the Modern Turkish Plastic Surgery.
References:
1. Arat, Reşid Rahmeti, Ord. Prof. Dr., Berlin Brandenburg Academy of Science, Hand- written Collection,“Zur Heilkunde der Uiguren” (SPAW, Phil. Hist. Klasse, 1930 XXIV, Berlin 1930, page(451-473)
2. Sertkaya Osman Fikri, “Kurzer Überlick Über Die Uigurischen Medizinischen Texte” Kitap: Festschrift für Arslan Terzioğlu, Prof. Dr. Ing. Dr. med. habil., zum sechzigsten Geburtstag /sahife: s. s. 125-138
3. Uzel İlter; “Şerefeddin Sabuncuoğlu; Cerrahiyetü-l Haniyye” Türk Tarih Kurumu Yayınları, III.Dizi-Sa.15,I. cilt, 495 sahife, II. cilt 98+36 fasıl, 140 minyatür, Ankara 1992
4. Ağırakça. Ahmet; Prof. Dr., “İslam Tıp Tarihi; Başlangıçtan VII./XIII. Yüzyıla Kadar, 399 sahife; FesanBasımevi, Derya Ciltevi, İstanbul, 2004
5. McDowell, Frank, MD., Sc.D., “The Source Book of Plastic Surgery”, Williams and Wilkins Company,Baltimore,1977; 509 pages
6. Horton, Charles E. MD. “Plastic and Reconstructive Surgery of the Genital Area”, 695 sahife; Little Brown and Company; Boston, 1973
7. Yıldırım İbrahim; “Plastic Surgical Training in Turkey, History, present situation and future”, EuropeanJournal of Plastic Surgery (Springer-Verlag), 16:115-117, 1993
8. Erdağı Binnur; “Anadolu’da Yazılmış İlk Türkçe Tıp Kitabı”, Türkbilig-Türkoloji Araştırmaları, 2001-2002, sahife: 46-55, TDV Matbaası, Ankara, Temmuz 2001
9. Terzioğlu Arslan Prof. Dr.; “İstanbul Tıp Fakültesi Tarihçesi 1”, Türk Dünyası Tarih Kültür Dergisi, İstanbul, Ekim 2010, s: 286, sahife 24-32
10. Terzioğlu Arslan Prof. Dr.; “İstanbul Tıp Fakültesi Tarihçesi 2”, Türk Dünyası Tarih Kültür Dergisi, İstanbul, Kasım 2010, s: 287, sahife 43-5
11. Terzioğlu Arslan, Prof. Dr., “Gülhane’nin Kuruluşunun 110. Yıld.nümü Anısına, Son Araştırmalar Işığında Gülhane ve Türk Tıbbının Gelişmesine Katkıları”, Türk Dünyası Tarih Kültür Dergisi, Ocak 2009, sayı 265, sahife 13-22, İstanbul
12. Topuzlu, Cemil; “80 Yıllık Hatıralarım, (İstibdat-Meşrutiyet-Cumhuriyet Devirlerinde) ‘Cemil Paşa’nınCerrahî Yayınları’ sahife 248-257, D.rdüncü Baskıya hazırlayan Dr. Cemalettin Topuzlu, Topuzlu Yayınları, Üniform Matbaacılık, İstanbul 2002
13. Kankat, Cafer Tayyar; “Modern Cerrahî ve N.roşirürji Mecmuası”, Ekspres Basımevi, Kader Basımevi,İstanbul 1936-1947 yılları arasında 36 sayı çıkmıştır.
14. Kankat, Cafer Tayyar; “Plâstik, Reperatris ve Estetik Şirürjisi Kitabı, 33 sahife, Kader Basımevi, İstanbul, 1946
15. Konuralp, Halit Ziya; “Plâstik Cerrahide Esas Prensipler”, 148 sahife, İsmail Akgün Matbaası, İstanbul, 1952
16. Kâhya, Esin; “Onbeşinci Yüzyılda Yaşamış Bir Bilim Adamımız, Mümin B. Mukbil”, X. Türk Tarih Kongresi, Ankara 22-26 Eylül 1986, Türk Tarih Kurumu Yayınları, IX. Dizi-Sa.10d, V. Cilt, sahife 2253- 2260, Türk Tarih Kurumu Basımevi, Ankara 1994
17. Sezer, Baha; “Plâstik Cerrahî”, Tıp Dallarındaki İlerlemelerin Tarihi (Dünyada ve Türkiye’de 1850 yılından sonra), Cerrahpaşa Tıp Fakültesi Vakfı Yayınları:4, Editör: Prof. Dr. Ekrem Kadri Unat, sahife:362-372, Gürtaş Matbaası, İstanbul 1988
18. Konuralp, Halit Ziya; Anıları “Personal Communication”, 1990-2005, İstanbul
19. Cihat Borçbakan’nın kendi sesinden Anıları, “Personal Communication”, 1986 – 1990, Ankara
The distribution of Plastic Surgeons is, unfortunately, not ideal in the country; they mostly try to stay in big cities. In our field, the number of the Plastic Surgeons in Turkey will be another problem in the near future.

Issue 7 www.ipras.org IPRAS Journal 77
The First MeetingThe inaugural meeting of the British Association of Plastic Surgeons was held at the Royal College of Surgeons of England on 20 November 1946. It was chaired by Sir Alfred Webb-Johnson (later Lord Webb-Johnson), who was then the President of the Royal College of Surgeons of England.The next day, the Association’s first President, Sir HaroldGillies, wrote the very first letter in the name of theBritish Association of Plastic Surgeons, to Sir Alfred Webb-Johnson:
Dear Alfred
I cannot let this opportunity go without putting on paper the very deep appreciation of your mostly kindly and helpful intervention last night. Your handling of the inaugural meeting, your help to me and to others in the later discussions were superb, and I can assure you and the Council of the College that our little association was happily started. We now also feel that the Royal College is our home and that the President and his team are our friends. We trust that we shall be worthy members of this surgical family.
HDG
BAPS had the objectives of relieving sickness and protecting and preserving public health by the promotion and development of Plastic Surgery. The Association also undertook to advance education in all aspects of Plastic Surgery.
The need for Plastic Surgery A Plastic Surgery Planning Committee chaired by Professor T Pomfret Kilner, and whose other members were Sir Harold Gillies, Mr Wilfred Hynes, Mr Archibald H McIndoe and Mr Rainsford Mowlem, had in fact met on five previous occasions before the inaugural meeting.They had found that the specialised war time units, which were especially equipped for treating injuries of the face and jaw, burns and soft tissues losses, had given facilities for treatment and research greatly in advance of those available in peace time. They also identifiedcivilian needs, such as some 700 cases of cleft lip and palate each year, industrial injuries and many patients for reconstruction and repair after surgery for cancer. They noted that facilities in London and in the provinces
(Stoke-on-Trent, Manchester and Birmingham) had been overwhelmed, and that even in November 1946 “the most recently established centre at Sheffield, with 40 beds, hadonly been open for five months, but already had a waitinglist of 70 cases and is compelled to refuse admission to deserving cases from surrounding towns”.The Committee was of the opinion that Plastic Surgery units should be based in general teaching hospitals and that they would function best in association with other departments, but retain their own individuality, with dedicated wards, operating theatres and offices, andwherever possible they should also support research.
The First PresidentsThe inaugural committee had faced a difficulty as towho to put forward as the first President of the BritishAssociation. The two main contenders were Sir Harold Gillies, and Professor Kilner, (who was the holder of the only chair in Plastic Surgery in the United Kingdom). The initial committee vote split, half for Professor Kilner and half for Sir Harold. A compromise solution of having two presidents was rejected by both, and Archibald McIndoe was definite in his advice that Sir Harold Gillies shouldbe put forward, and this prevailed. Sir Harold was President from 1946-47, Professor Kilner followed in 1947-48 (and was elected President again in 1955), and they were succeeded in 1949 by Archibald McIndoe.
Harold Delf GilliesHarold Gillies was born in New Zealand in 1882, the youngest of eight children. His father died when he was 4 and he was sent to boarding school in England at the age of 8. Four years later he returned to school in New Zealand, and in 1901 came back to Gonville and Caius College, Cambridge. He played the violin, developed a love of fly-fishing, he rode and played golf (reachingthe semi-finals of the amateur golf championship at StAndrews). He graduated from St Bartholomew’s Hospital, London, becoming a Fellow of the Royal College of Surgeons in 1910 and he became assistant to Sir Milsom Rees, the senior ENT surgeon at St Bartholomew’s. When war broke out in 1914, Gillies, then 32, volunteered to serve with the Red Cross and was sent to France as a General Surgeon in 1915. He was closely associated with Charles Auguste Valadier and Varaztad H Kazanjian, who
A history of the British Association of Plastic, Reconstructive and Aesthetic SurgeonsPreviously: The British Association of Plastic Surgeons

78 IPRAS Journal www.ipras.org Issue 7
stimulated his interested in maxillofacial injuries. He visited Hippolyte Morestin at the Val-de-Grâce military hospital in Paris and after watching him operate he wrote “this was the one job in the world I wanted to do”. Gillies transferred to the Royal Army Medical Corps and with the backing of Sir William Arbuthnot-Lane, set up a special unit at the Cambridge Military Hospital in Aldershot, in 1916. From the Battle of the Somme (July 1916) 2000 casualties were referred. There were only 200 beds and the facilities were overwhelmed. The Queen’s Hospital in Sidcup was established, with an additional 200 beds and when the old hospital was eventually knocked down many years later, a plaque was placed in the entrance of the new Queen Mary’s Hospital, Sidcup, to commemorate “Harold Delf Gillies, CBE, FRCS 1882-1960, whose work at this hospital attracted worldwide recognition and led to the foundation of Plastic Surgery in Great Britain”.
BAPS Between the warsAfter peace was declared in November 1918, American, Canadian, Australian and New Zealand surgeons returned to their home countries to develop Plastic Surgery and to establish new units. Most of England was covered by four Plastic Surgeons in the 1930’s – Gillies, Kilner, McIndoe and Mowlem. In 1936, Richard Battle was told “there are four Plastic Surgeons in the country and there is no room for any more”, but fortunately he was not put off. The only other surgeon in formal Plastic Surgery training at that time was David Matthews, later joined by Eric Peet and J P Reidy.The Royal Air Force was to recognise the importance of the new specialty of Plastic Surgery, setting up Plastic, Maxillofacial and Burns centres, including East Grinstead and Halton. At the Queen Victoria Hospital, East Grinstead, the Guinea Pig club was founded by surviving burnt RAF crew members. The Royal Navy and the Army also developed Plastic Surgery facilities.From 1939, the period of the “phoney war” mass casualties that had initially been expected did not materialise, but the specialty developed by accepting civilian casualties resulting from the blackouts, which increased the road and domestic accident rate, and from those injured in factories, which were depending on unskilled labour to develop munitions (for example, women whose long hair was caught in conveyor belts causing scalping injuries).The British Association of Plastic Surgeons stimulated the development of the specialty in many countries around the world. At the outbreak of the Second World War, medical officers from Australia, Canada, India,Ireland, New Zealand and South Africa were allocated to the four newly established Plastic Surgery units in the United Kingdom for training.
The Second World War and afterwardsOn December 7, 1941 the Japanese bombed Pearl Harbour and the next year large numbers of American forces began to appear in Britain, together with their surgical hospitals and field units. They brought with them specialisedMaxillofacial and Plastic Surgery teams, including pioneers such as Aufricht, Converse, Ivy, Kazanjian and Webster. The friendly co-operation during that time led to strong trans-Atlantic friendships, including the collaboration of Ralph Millard of Miami with Sir Harold Gillies, with whom he became co-author of “The Principles and Art of Plastic Surgery” (1957) being awarded an honorary FRCS(Ed).After the end of the war, Loenneken (Oslo), Olsen (Copenhagen), Ragnell (Stockholm), and Schjelderup (Bergen) were amongst those who came to Britain to train in the new specialty of Plastic Surgery, encouraged by the inauguration of the Association in 1946 and of the British Journal of Plastic Surgery in 1948.
Distinguished Visitors to Britain Many pioneers of Plastic Surgery in Europe came to train in Britain, including:
Holland: C Koch, C Honig
Belgium: J Polus, A de Coninck
France: D Morel-Fatio, C Dufourmentel, R Tubiana
Spain: B Vilar-Sancho, J Planas, L Mir y Mir, P Gabarro
Portugal: J Conde, A M Fernandes
Italy: S Rosselli, S Teich-Alasia, G Dogo
Austria: R Trauner, P Wilflingseder
Switzerland: H U Buff, H L Obwegeser
Yugoslavia: V Arneri, I Cupar, H Klemencic, M Derganc, F Zdravic
Czechoslovakia: F Burian, S Demjen
Poland: J Szlazak
Denmark: P Fogh-Andersen
Sweden: T Skoog, B Johanson
International Meetings in Plastic SurgerySurgeons from France, American and Britain, who had been engaged in treating the wounded of the First World War, attended a meeting held in Paris in June 1925. Meetings were then held in Brussels in 1936 (“Le Premier Congrès de Chirurgie Structive”) and this was followed by the “Second European Congress of Structive Surgery” in London, in October 1937. An international meeting

Issue 7 www.ipras.org IPRAS Journal 79
was planned under the presidency of Professor Sanvenero Rosselli in Milan, in September 1938 and this had to be abandoned midway, because of the Munich crisis. Dr Tord Skoog was the Organising Secretary of the Scandinavian Association of Plastic Surgeons International Congress, which was held in Stockholm in August 1955, under the presidency of Professor Erik Aschan of Finland, with Sir Harold Gillies as its Honorary President.The London International Congress was held at the Royal College of Surgeons of England, on July 13th, 1959, under Mr Rainsford Mowlem, President of the British Association of Plastic Surgeons and Professor T P Kilner, Vice-President of the Association and of the Congress. Appointed delegates of 29 national societies of Plastic Surgery attended, each seated below their national flag and receiving an address from His RoyalHighness, Prince Philip, Duke of Edinburgh, who had consented to being the Patron of the Congress (and who in November 1964 agreed to become the first patron ofthe British Association of Plastic Surgeons), a role which he continues to the present day.
BAPS Becomes BAPRASIn 2004 the majority of the members of the British Association of Plastic Surgeons (BAPS) voted to change the name of the Association to the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS), in line with many European associations of Plastic Surgery. http://www.bapras.org.ukThe Association’s new look and name came into being in July 2006. This was associated with a change of brand-identity, moving from the previous heraldic crest to a new, contemporary logo, retaining one of the key motifs, the salamander.The salamander possesses natural powers of regeneration and is able to restore lost or damaged tissue or limbs. In mythology, the salamander was believed to be capable of withstanding fire and was often depicted walkingunharmed through flames. Thus, this simple amphibianis an enduring symbol of reconstruction, protection and repair. Over the years, the salamander has also been valuable in scientific research and this new emblemprovided a vital link with history as, moving forward BAPS became BAPRAS and a new era began.The British Association of Plastic, Reconstructive and Aesthetic Surgeons is now “the voice of Plastic Surgery” in the UK, advancing education in all aspects of the specialty and promoting contemporary practice. BAPRAS sees its role as increasing understanding of the scope of the specialty of Plastic Surgery. It aims to raise the profile of Plastic Surgeons, who are a crucial elementof surgical care teams which provide specialist care to patients over a wide range of conditions. Continuing the core objective of advancing education, BAPRAS
is always looking to promote innovation within the speciality of Plastic Surgery. The President in 2011, Tim Goodacre, set out ways in which the Association looks to develop: enhancing its research profile; increasing its presence in the regionsin support of its members; and collating accurate data relating to the numbers of Plastic Surgeons, the focus of their work and the impact created.
Members and Plastic Surgery UnitsThere are currently Plastic Surgery units in 56 centres in the United Kingdom and 6 units in the Republic of Ireland. Plastic Surgery clinics, however, are held in many other hospitals throughout the country, each one linked to a regional unit. There are 892 members of the Association including honorary members, senior members, full members, trainee and junior members, and other categories of associated and overseas members.
Current Meetings, Courses, and ResearchThe Association, together with the Royal Colleges, has appointed Plastic Surgery and Cosmetic Surgery tutors. Each year, BAPRAS holds two 3- day ScientificMeetings, and two 2-day Advanced Courses, covering the spectrum of Plastic Surgery, which are open to colleagues from the UK and abroad. In addition, there are two 1- day meetings for medical students interested in Plastic Surgery, and a 1-day breast care nurses’ course. There is an active Education and Research subcommittee.The Next BAPRAS instructional Course will be held in Manchester on 18th and 19th April, 2012. Delivered by renowned international experts, this course is aimed at specialist trainees and established surgeons in Plastic Surgery, breast oncology, and applied disciplines from the UK and the wider international community and will cover the latest innovations and techniques.
Examinations and AssessmentMembers of BAPRAS have also been heavily involved in mainstream teaching, training, and examinations. The Intercollegiate Board in Plastic Surgery brings together the four Royal Colleges and the examination structure, which started with the FRCS (Plastic Surgery) in 1986 at the instigation of Mr Ian McGregor, which includes written, oral and clinical examinations. The FRCS (Plast) examination is held in different centres throughout the UK.The evolving structure of the Intercollegiate Examination has helped to shape the course of other examinations abroad, including those of the European Board, first heldin Brussels in 1994 under the encouragement of Mr Magdy Saad, then President-Elect of BAPS, and Professor John Ioannovich of Athens. The EBOPRAS European Board Examination in Plastic Surgery currently has a British Chairman, Mr John Boorman FRCS.

80 IPRAS Journal www.ipras.org Issue 7
BAPRAS and the Developing WorldBritish Plastic Surgery has a long tradition of links with the developing world. Through its Overseas Service and Training Committee, BAPRAS continues to offer support to developing countries, recognising the importance of Reconstructive Plastic Surgery in the treatment of injury and disease and helping to develop Plastic Surgery skills in these environments.BAPRAS is keen to provide sustained and effective help to colleagues abroad. Some UK Plastic Surgery units already have twinning arrangements with overseas hospitals and departments and more links can be set up through the BAPRAS Overseas Service and Training Subcommittee.BAPRAS also has links with non-governmental organisations, as well as the UK government, to provide acute help, for example following natural disasters abroad, such as earthquakes. Overseas activities include:• Funding short visits for Surgeons to learn new
techniques in the UK• Supporting Surgeons in countries as diverse as
Bangladesh, Ghana, India, Nepal, Pakistan, Sri Lanka and Uganda
• Enabling BAPRAS members to visit many of these countries to participate in meetings and to work in collaboration with overseas colleagues
• Conducting teaching and training and workshops in countries with limited plastic surgical infrastructure.
The Journal of Plastic, Reconstructive and Aesthetic SurgeryAn early proposal, after the foundation of the Association in 1946, was to start a regular scientific communication onPlastic Surgery and the British Journal of Plastic Surgery was launched in March 1948, under the editorship of Mr A B Wallace.
LecturesTHE GILLIES LECTUREIn 1961 the Council of the British Association of Plastic Surgeons instituted the Gillies Lecture as a memorial to Sir Harold Gillies. Distinguished Plastic Surgeons from within the UK and abroad, are invited to lecture to the Association and receive the Medal. The most recent Gillies Lecture was given at the BAPRAS Winter Scientific Meeting in December 2011 by Dr SamNoordhoff, a world leader in the field of cleft lip andpalate and Craniofacial Surgery, who practised for over 40 years in Taiwan and was instrumental in establishing several hospitals and Plastic Surgery Departments in Taipei, which have an international reputation.
THE McINDOE LECTUREIn 1962, the Royal College of Surgeons of England received a donation from the Royal Air Forces Association which was to cover a Lectureship, awarded by the Council of the College, on the recommendation of the President of the College and the President and Honorary Secretary of the BAPRAS, devoted to Plastic Surgery or another allied subject, in the name of Sir Archibald McIndoe, the Third President of the British Association of Plastic Surgeons.
HUNTERIAN LECTURESMany Plastic Surgeons, and members of the Association, have been awarded Hunterian Professorships by the Royal College of Surgeons, at the invitation of the Council. The most recent Hunterian lecture was given at the BAPRAS Winter Scientific Meeting in December 2011 by Mr MSchaverien whose ground-breaking work in the UK, Australia and the USA was the basis of his lecture on “The use of three-dimensional imaging for the investigation of the microvascular arterial and venous anatomies and perfusion of surgical flaps and the integument”.
The Organisation of BAPRASThe Officers of BAPRAS are its President, Vice-President, Honorary Secretary and Honorary Treasurer. The other elected members of Council and the officersare the Trustees of the Association and there has been a strong move recently towards regional representation on the Council. A number of other colleagues are invited to attend BAPRAS Council meetings, including the President of the Irish Association of Plastic Surgeons, a patient liaison representative, the editor of JPRAS, the Chairman of the Overseas Service and Training Committee, the Chairman of the Professional Standards Committee, the Communications Officer, the chairman of the SpecialistAdvisory Committee in Plastic Surgery, the President of the British Association of Aesthetic Plastic Surgeons, and the Chairman of the Education and Research Committee.From 2012 the presidency will be extended to a two year term of office. Recent Presidents:• Mr Timothy Goodacre (Oxford) 2011 • Mr Richard Milner (Newcastle) 2012• Mr Graeme Perks (Nottingham) 2013/2014
European and International RepresentationBAPRAS is proud to be represented on the European Board of Plastic, Reconstructive and Aesthetic Surgery, and the Union Européenne des Médecins Spécialistes. BAPRAS is represented on the International Confederation for Plastic, Reconstructive and Aesthetic Surgery by its President.
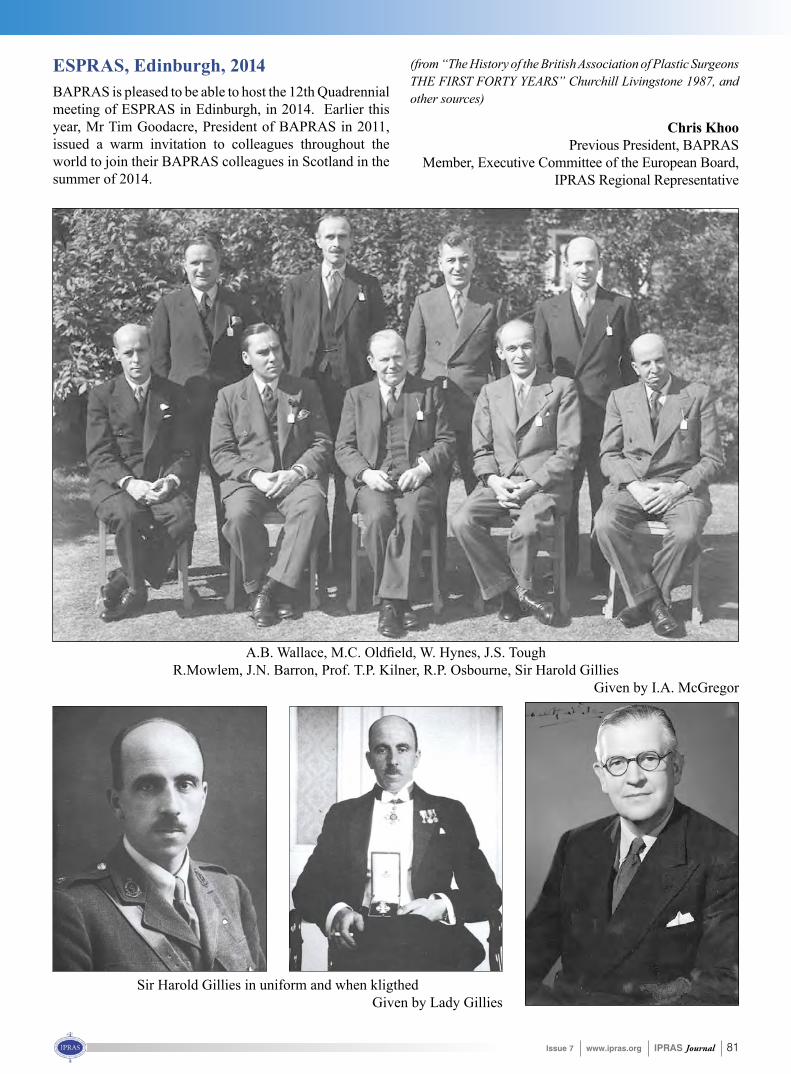
Issue 7 www.ipras.org IPRAS Journal 81
A.B. Wallace, M.C. Oldfield, W. Hynes, J.S. ToughR.Mowlem, J.N. Barron, Prof. T.P. Kilner, R.P. Osbourne, Sir Harold Gillies
Given by I.A. McGregor
Sir Harold Gillies in uniform and when kligthedGiven by Lady Gillies
ESPRAS, Edinburgh, 2014BAPRAS is pleased to be able to host the 12th Quadrennial meeting of ESPRAS in Edinburgh, in 2014. Earlier this year, Mr Tim Goodacre, President of BAPRAS in 2011, issued a warm invitation to colleagues throughout the world to join their BAPRAS colleagues in Scotland in the summer of 2014.
(from “The History of the British Association of Plastic Surgeons THE FIRST FORTY YEARS” Churchill Livingstone 1987, and other sources)
Chris KhooPrevious President, BAPRAS
Member, Executive Committee of the European Board,IPRAS Regional Representative

82 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 83
The history of Plastic Surgery in the Republic of Armenia begins in 1982. Since 1982, the “Initiative Group”, a team of young surgeons, started experimental operations. They derived from the ranks of a microsurgery fellowship in Moscow. They worked in the Armenian branch of the All-Union Scientific Center of Surgery. The firstsuccessful clinical operation, was the replantation of thumb in 1984. In 1984 a division of microsurgery in the Armenian branch of the All-Union Scientific Center of Surgerywas created by the initiative group. The first operationswere muscle, tendon, vessel and nerve reconstructions of extremities.In 1985 the first department of Microsurgery wascreated and headed by Artavazd Sahakyan. Later in 1992, a second department, the Center of Plastic and Reconstructive Surgery was organized and headed by Gagik Stamboltsyan. All surgeons of the second department completed their specialization period in Yale University. Since 1990 many aesthetic operations take place in the Republic of Armenia.In 1996 in Yerevan State Medical University and National Health Institute, two new departments of Plastic Surgery were organized. They also manage a postgraduate education program. After graduating from a 4 year residency in one of these departments you can get a Plastic Surgeon’s diploma.
The Armenian Association of Plastic Reconstructive and Aesthetic Surgeons (AAPRAS) was founded in 2005 by the main Committee (The First RPesident was Armen Hovhannisyan). The greatest part of the Armenian Plastic Surgeons have decided to create this Society, giving priority to issues like:
- coordination of the surgeons’ practical and scientific work,
- promotion of postgraduate education,
- unification of educational programs,
- organization of International Congresses.
During the last period the Association organized four International Congresses, the last of which took place under the endorsement of IPRAS and ESPRAS. Our Association is in close relationship with the Russian and Georgian Societies. Our relationship with IPRAS and ESPRAS is very productive and highly influential to ouryoung Plastic Surgeons’ education and training in famous European clinics. Nowadays, many Member Surgeons of our Association work in aesthetic and reconstructive Surgery Units worldwide. In 2013 we are planning an International Multidisciplinary Congress on Antiaging Medicine and we invite all our colleagues to participate in it.
Çistory of Plastic Surgery in the Republic of Armenia
Armenian Association of Plastic Reconstructive and Aesthetic Surgeons (ÁÁPRAS)
Dr. Armen Hovhannisyan President of AAPRAS

84 IPRAS Journal www.ipras.org Issue 7
World Health Organization
Dear colleagues,
WHO Patient Safety is pleased to share with you the results of the Latin American Study of Adverse Events (IBEAS): on a given day, 1 in 10 patients admitted to the participating hospitals were suffering from, or undergoing treatment for, a health care -related adverse event. The risk of suffering adverse events doubled if the entire hospital stay was considered. This evidence is a reflection of the reality of many other hospitals in transitional countries across the globe and it highlights the importance of addressing patient safety globally.
The result of a collaborative effort between the governments of Argentina, Colombia, Costa Rica, Mexico and Peru, as well as the Spanish Agency for Quality of the Ministry of Health, Social Policy and Equality, the Pan-American Health Organization and WHO Patient Safety, the IBEAS study is the first large scale study of this kind in Latin America.
For more information, click herehttp://www.who.int/patientsafety/research/country_studies/en/index.html
To download the study results in English, click here http://www.who.int/patientsafety/research/ibeas_report_en.pdf
To download the study results in Spanish, click here http://www.who.int/patientsafety/research/ibeas_report_es.pdf
The WHO Patient Safety team
Issue 7 www.ipras.org IPRAS Journal 85
86 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 87
88 IPRAS Journal www.ipras.org Issue 7
Issue 7 www.ipras.org IPRAS Journal 89

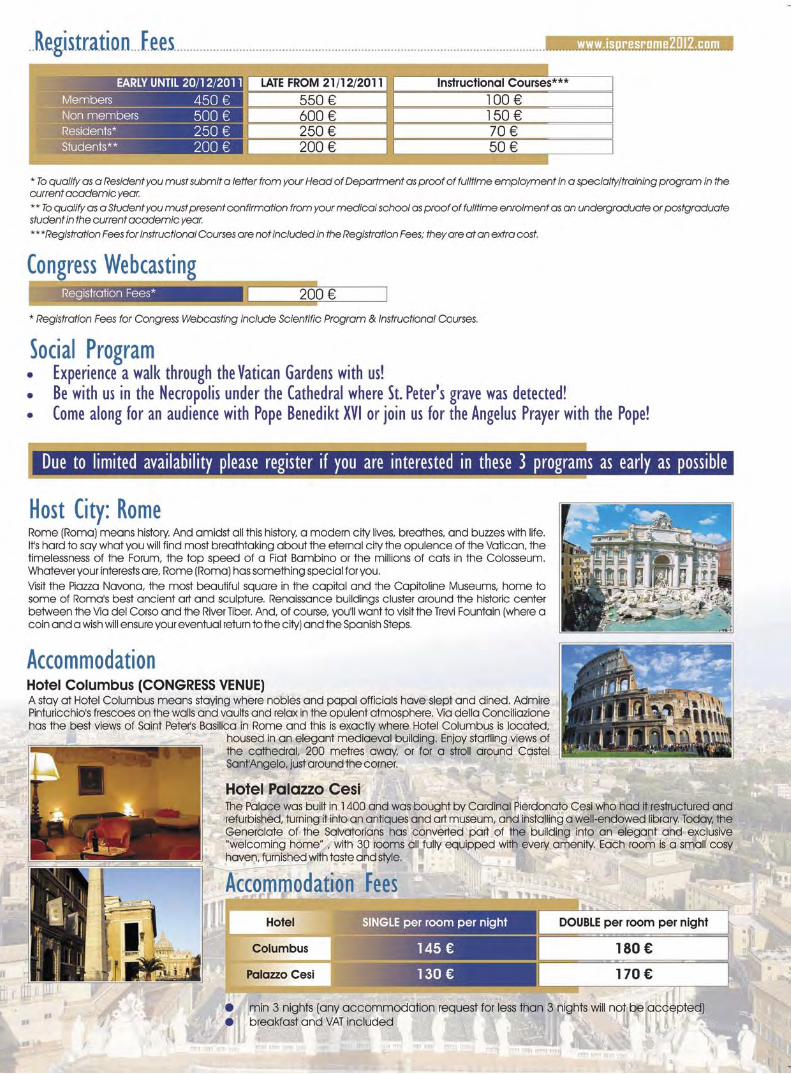

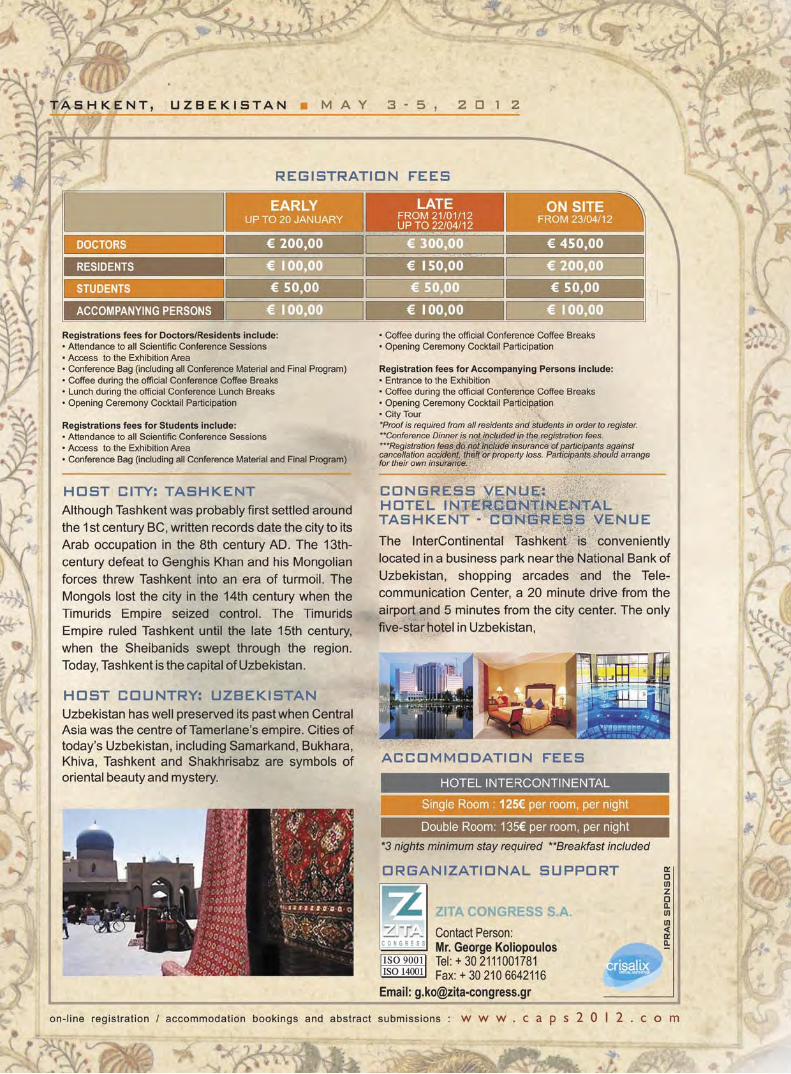





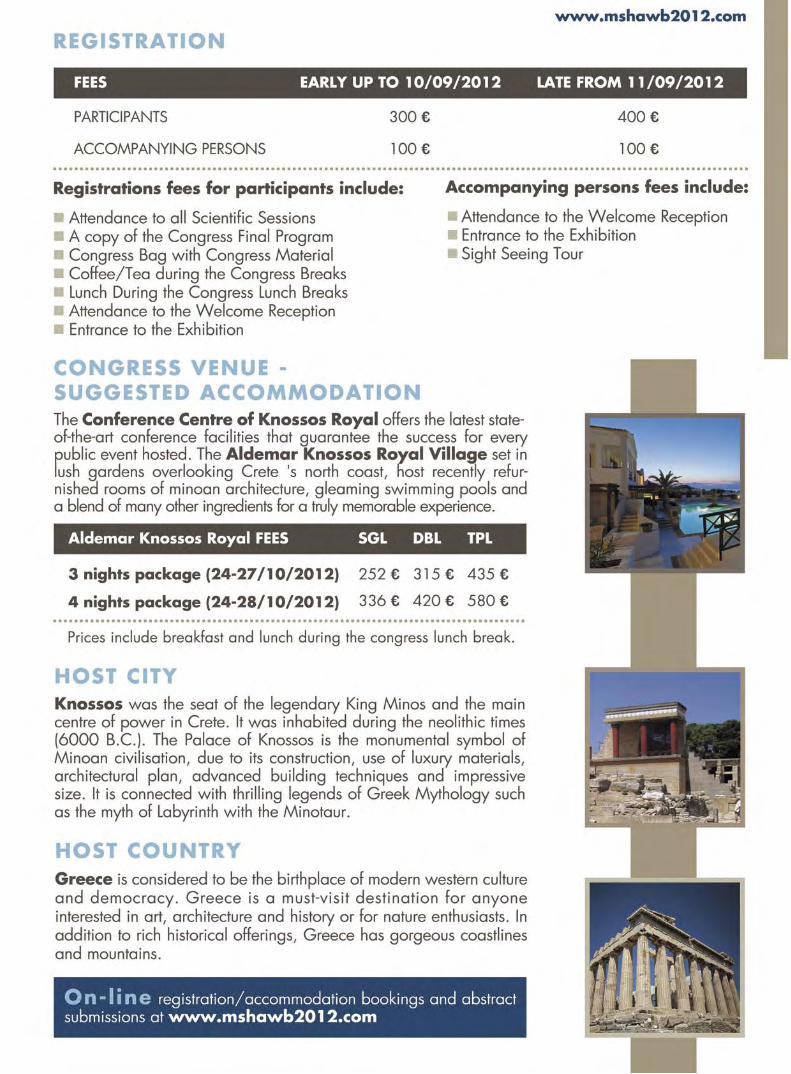
102 IPRAS Journal www.ipras.org Issue 7

Issue 7 www.ipras.org IPRAS Journal 103

104 IPRAS Journal www.ipras.org Issue 7

108 IPRAS Journal www.ipras.org Issue 7
Dear colleagues,
The IPRAS International Committee for Quality Assurance and Medical Devices in Plastic Surgery (IQUAM) celebrates the 20-year anniversary from its foundation, in 1992. This celebration will take place during the 10th Congress and Consensus Conference to be held in Athens on Nov 1st – 4th, 2012.
The organization was founded as EQUAM by a group of Plastic Surgeons from various European, Central and South American, African, Southeast Asian and Middle-Eastern countries. Representatives participating in meetings are Plastic Surgeons, scientists, manufacturers and delegates from governmental bodies involved in the development and surveillance of advanced technologies, devices and techniques in the field of Plastic Surgery.Consensus Conferences are held biennially. At the close of meetings, a Position Statement is drawn up, summarizing the conclusions of the meeting. This statement is presented to the health ministry and Plastic Surgery society of each member country, the industry and any other interested party. Over the years, these statements acquired an important significancein the practice of the Specialty and proved helpful for all.
No doubt, this type of meeting is unique in its purpose and, besides clinical practice, it also focuses on evaluating technology and methodology. Among others, topics like Fat Grafting, Stem cells and Growth Factors will be addressed, as well as results from recent and older procedures like breast augmentation and ALCL, quality of silicone implants, injectable fillers, Botulinum toxin A, suturing materials, wound dressings, medical equipment,instruments, LASER apparatuses and so many others. The recent issue regarding PIP, which alarmed Plastic Surgeons and the public worldwide, will be particularly discussed in detail.
Besides science, a rich social program is planned, including a guided evening tour at the illuminated Acropolis. Most of all please be assured that the organizing committee shall spare no effort in putting together a successful congress.
A cordial invitation to all,
C. Neuhann-Lorenz IQUAM President
Jan Poëll Congress President
Daniel Marchac Chair Organizing Co.
Andreas Yiacoumettis Chair Scientific Co.

Issue 7 www.ipras.org IPRAS Journal 109
The 1st IPRAS INTERNATIONAL TRAINEES’
MEETINGwill take place in Athens on November 1st, 2012.
This meeting will make history as the first of its kind in the world. It is expected thatTrainees from many countries will participate, as well as representatives from Trainees’ organizations.
The program will include the following:
1. Scientific Presentations
2. Training and accreditation
3. International co-operation
4. Official participation of trainees in IPRAS
The Faculty of this meeting will include respected and well known teachers, Heads of training programs, Trainees and members from the IPRAS leadership.
More information will soon be uploaded on the IPRAS website www.ipras.org
For the FIRST time…

110 IPRAS Journal www.ipras.org Issue 7
Dear colleagues and friends of IPRAS,
I have always been certain that the only way forward is to have our eyes looking to the future, confident that plastic surgery will carry on thriving, absorbing new technologies and techniques. I have accompanied our society since its first steps, and I am glad to see visions transformed to reality! It has been my hope that IPRAS and its national societies will continue to be the forums where innovation will be presented, where the inquisitive mind will find others equally curious, so that plastic surgery may evolve within the framework of two principal objectives: to generously pass on knowledge to the next generation, and to assure safety to our patients.
I am particularly happy that the upcoming IPRAS World Congress is to be held in beautiful Chile, in our continent of South America, where plastic surgery has made giant steps of development. I invite you all to add this important event to your plans for 2013 and to take advantage of the opportunity to attend one of the most important scientific gatherings for plastic surgery.
Ivo PITANGUY
Head-Professor of the Plastic Surgery Departments of the Pontifical Catholic University of Rio de Janeiro and the Carlos Chagas Institute of Post-Graduate Medical Studies
Member (and patron) of the Brazilian Society of Plastic Surgery, the National Academy of Medicine, and the Brazilian Academy of Letters
Visiting Professor, I.S.A.P.S. FICS, FACS
SUPPORT LETTER FROM BOARD OF TRUSTEES MEMBER

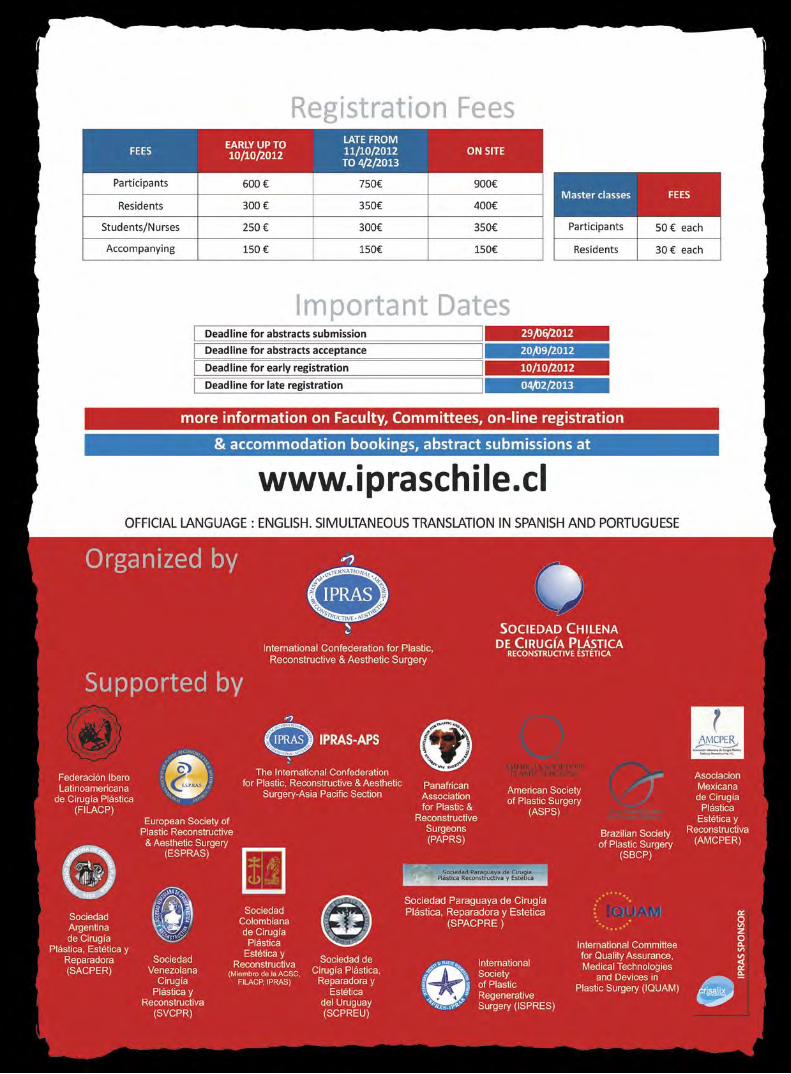
NATIONAL & CO-OPTED SOCIETIES’ FUTURE EVENTS
17 - 19 February 2012
17th Annual Pakistan Association Of Plastic Surgeon MeetingLocation: Bahawalpur, Pakistan - Venue: Quaid-e-Azam Medical College - Contact: Dr M. Mughese Amin
E-mail: [email protected] - URL: http://www.papscon2012.com
06 - 11 March 2012
XLIII National Congress of Plastic, Aesthetic and Reconstructive SurgeryLocation: Merida, Yucatan, Mexico - Venue: Convention Center Merida
URL: http://www.cirugiaplastuca.org.mx
09 - 11 March 2012
1st Congress of the International Society of Plastic Regenerative Surgery (ISPRES)Location: Rome, Italy - Venue: Hotel Columbus - Contact: Chrysa Kontololi
Telephone: +30 2111001783 - Fax: +30 2106642116E-mail: [email protected] - URL: http://www.ispresrome2012.com
11 - 14 March 2012
16th ASEAN Congress of Plastic SurgeryLocation: Boracay Island, Aklan, Philippines - Venue: Boracay Regency Beach Resort & Convention Center
URL: http://www.papras.org/
17- 20 April 2012
42º Argentine Congress of Plastic SurgeryLocation: Buenos Aires, Argentina - Venue: Sheraton Hotel - Telephone: (54) 114811-9103
E-mail: [email protected] - URL: http://www.42congresoargentino.com
03 - 05 May 2012
3rd Central Asian Plastic Surgery ConferenceLocation: Tashkent, Uzbekistan - Contact: George Koliopoulos
E-mail: [email protected] - URL: http://www.caps2012.com/
15 - 18 May 2012
11th SRBPRAS CongressLocation: Belgrade, Serbia - Venue: HYATT Regency Belgrade
E-mail: [email protected] - URL: http://www.srbpras2012.org
18 – 20 May 2012
Controversies, Art and Technology in Breast and Bodycontouring Aesthetic Surgery, CATBBAS ILocation: Ghen, Belgium - URL: www.coupureseminars.com - E-mail: [email protected]
22 - 26 May 2012
XIX International Meeting of FILACPLocation: Medellín (Colombia) - URL: http://www.filacp2012.com
29 - 31 May 2012
3rd European Congress on preventive, Regenerative & Aesthetic Medicine (ECOPRAM)Location: Istanbul, Turkey - Venue: Harbyie Military Museum - Contact: Chrysa Kontololi
Telephone: +302111001783 - Fax: +302106642116E-mail: [email protected] - URL: http://www.ecopram2012.com/
NATIONAL & CO-OPTED SOCIETIES’ FUTURE EVENTS
05 - 07 June 2012
17th Meeting of the Euro-Mediterranean Council for Burns and Fire Disasters (MBC) & 25th Anniversary Commemorative Meeting
Location: Palermo, Italy - Contact: Prof. Bishara Athiyeh - E-mail: [email protected]
16 - 17 June 2012
1st Seoul Rhinoplasty ForumLocation: Seoul, Korea - Venue: Seoul St. Mary’s Hospital
E-mail: [email protected] - URL: http://www.srf2012.or.kr/conference/1st_html/
11-12 September 2012
The XIIth Congress of the Romanian Association of Plastic Surgeons with Participation of Hungarian Association of Plastic, Reconstructive and Aesthetic Surgery Location: Sinaia, Romania - Contact: Lefteris Aivaliotis - E-mail: [email protected]
12 – 15 September 2012
LaserInnsbruck 2012Location: Innsbruck, Austria - Venue: Faculty of Catholic Theology of the University of Innsbruck
Contact: Chrysa KontololiE-mail: [email protected] - URL: http://laserinnsbruck.com/
13 - 15 September 2012
43. Jahrestagung der DGPRÄC / 17. Jahrestagung der VDÄPCLocation: Bremen, Germany - URL: http://www.dgpraec2012.de
10 - 13 October 2012
2nd World Congress of Plastic Surgeons of Lebanese DescentLocation: Cancun, Mexico - Venue: Convention Center Cancun
URL: http://www.congressmexico.com/LSPRAS2012
26 – 30 October 2012
Plastic Surgery THE MEETINGLocation: New Orleans, USA - E-mail: [email protected]
URL: http://www.plasticsurgerythemeeting.com/
1st November 2012
The 1st IPRAS International Trainees’ MeetingLocation: Athens, Greece - Venue: Royal Olympic Hotel
Contact: Mr Nikos Antonopoulos - E-mail: [email protected]
01 - 04 November 2012
10th IQUAM CONSENSUS CONFERENCELocation: Athens, Greece - Venue: Royal Olympic Hotel - Contact: Nikos Antonopoulos
Telephone: +302111001782 - Fax: +302106642116E-mail: [email protected] - URL: www.iquam2012.com
14 – 18 November 2013
49th Brazilian Congress of Plastic SurgeryLocation: Porto Alegre - URL: http://www.cirurgiaplastica.org.br/

116 IPRAS Journal www.ipras.org Issue 7
Now it is very simple to upload your scientific profile and gain the benefits of being under the IPRAS umbrella.Try it…!!Sign up on www.ipras.org and follow the following steps: 1. Create an account by clicking “Member’s
login” on the top right-hand corner and then select the “Create new account” tab.
2. Fill out your “Username”, “Email” and “Password”, as required.
3. Select the option “Doctor” and your country, under the section “If you are a doctor, complete the following”.
4. Once all account details have been added, click on “Create new account” button.
Then you click on “EDIT” and then on “DOCTOR PROFILE”.This is the section where all the information of your scientific profile can be uploaded.You may complete the fields with the information that you prefer such us: Personal Picture, Hospital Position, Affiliation, Special Field of Interest, Contact Details, Memberships, Topics of Special Interest, Publications etc.At the “EDIT” section you may proceed to the appropriate corrections at your account such us to change your password or to update personal information.When you complete the aforementioned steps there will be one last step remaining for your details to be uploaded on the IPRAS website. The application must be approved by the National Association you are a member. The application will
JOIN YOUR COLLEAGUES The first website that gives you the opportunity
to upload your scientific profile for free!!
www.ipras.org
I P R A S W E B S I T E
be sent at the Association of the country that you have declared, ensuring that only IPRAS members of good standing and high ethical principles are able to upload their personal details. As soon as your Association verifies you as a member, your profile will automatically be uploaded at the website’s, “Find a doctor” option in the “Members”section.It is also up to you to decide whether your profile will be classified as “private” or visible to all visitors of the IPRAS webpage. Our aim, besides facilitating communication among colleagues, expands to allowing patients to verify the good standing and high ethical principles of the doctors’ profiles hosted, allowing them to choose qualified IPRAS members for needed procedures.In conclusion, I want to emphasize the usefulness of the IPRAS website FORUM. A section you will gain access to, as soon as your profile has been accepted and uploaded. Only verified plastic surgeons can use it and read its contents. Therefore, you will have the opportunity to exchange ideas, news regarding plastic surgery techniques, news from your National Association, alerts and all other information you would like to share with your peers. Don’t miss the opportunity to make the IPRAS website twice as useful to you!If you face any difficulties please do not hesitate to contact me at: [email protected] . Always at your disposal!
Maria PetsaIPRAS Assistant Executive Director

Issue 7 www.ipras.org IPRAS Journal 117
Crisalix 3D simulations are now used in more than 70 countries
“Special offer for all IPRAS members and readers. See end of the article for more details.”
e-Stetix 3D
2011 has been the result of several important achievements, among them:- e-Stetix 3D progressed through versions 1 to 5, with a long
list of improvements and new functionalities. All updates were provided for free to registered users, and the service was continuously updated with the latest technology following users’ feedback.
- e-Stetix was selected by IBM for its “Smarter Planet”
I N D U S T R Y N E W S
answering the most common question from patients. Dr. Serge Lê Huu (LaClinic, Montreux) has been using e-Stetix since its first commercial release and recently announced thatin only 18 months, e-Stetix had contributed to increasing his conversion rate from 57% to over 92%. Aside from generating these impressive results, Dr Lê Huu also noted that e-Stetix has been invaluable in optimizing the relationship with patients, through educating them about their bodies, helping them to select the desired implants, and helping to understand and manage the patients’ expectations and aspirations.
Some new developments available in version 5.2: complete set of linear and surface measurements, 3D planning for implant
positioning and nipple orientation, and much more.
SHOWCASE – Serge Lê Huu – Switzerland “e-Stetix for Patient Education“
program due to its innovative cloud computing approach.- A 24/7 support desk was implemented, to train and support
every e-Stetix user whenever necessary.- A second research & development project was commissioned
by the Swiss National Fund of Research - CTI (Commission of Innovation and Technology) in Switzerland, due to the value e-Stetix unique technology brings to the field of plasticsurgery.
- e-Stetix reached the milestone of more than 1,500 active users in more than 70 countries (see map below).
- The launch of its consumer website www.sublimma.com, which today is already generating more than 30 enquiries per day in 10 different languages from people interested in
plastic surgery with certified surgeons.- Endorsements by the International confederation of Plastic
Reconstructive Aesthetic Surgery (IPRAS) and the Sociedad Española de Cirugía Plástica Reconstructiva y Estética (SECPRE). Both organizations support and share the same objective as Crisalix; increasing patient satisfaction by
Dr Lê Huu specifically refers to using e-Stetix in order tohighlight asymmetries and distance between the breasts, as well as to show how implant shapes and volumes can produce varying results on different patients’ bodies. He maintains that having this discussion prior to surgery has significantlyminimized potential disappointment, and even surgery revisions, to the extent that he has not encountered a single unsatisfied patient during these 18 months.IPRAS members and readers have a special 10% discount on e-Stetix annual subscriptions until March 15th 2011. To benefit from this offer, please visit http://www.crisalix.com/en/pricing and proceed to “sign up”. Use the following code in the “Promotional Code” field: 41f282e1d8
CrisalixPSE-A1015 [email protected]
118 IPRAS Journal www.ipras.org Issue 7
I P R A S P A S T G E N E R A L S E C R E T A R I E S
Tord Skoog (Sweden)
1955 - 1959
David N. Matthews (U.K.)
1959 - 1963
Thomas Ray Broadbent (USA)
1963 - 1967
William M. Manchester (N. Zealand) 1967 - 1971
John Watson (U.K.)
1971 - 1975
Roger Mouly (France)
1975 - 1983
Jean-Paul Bossé"(Canada)
1983 - 1992
Ulrich T. Hinderer (Spain)
1992 - 1999
James G. Hoehn (USA)
1999 - 2006
Marita Eisemann-Klein (Germany) 2006 - 2011

IPRAS BENEFITS FOR INDIVIDUAL MEMBERS
• Immediate information about safety warnings on devices, drugs and procedures
• Information regarding the proper use of all materials, substances and techniques related to Plastic, Reconstructive and Aesthetic Surgery through IQUAM (the International Committee of Quality Assurance and Medical Devices in Plastic Surgery) General Consensus statement, with an update every 2 years
• Free electronic receipt of the IPRAS JOURNAL
• Information regarding harmonization of training
• Information regarding accreditation of Plastic Surgery Units
• Promotion of Patient Safety and Quality Management (in cooperation with WHO)
• Protection of the Specialty and Promotion of its image world-wide
• Promotion of Individual Members of National Associations by uploading their scientific profile on the IPRAS website
• Exchange of ideas, views, thoughts and proposals though the IPRAS website and its FORUM section
• Certificate for Individual Members to display their IPRAS Membership
• Regular updates on necessary information and the right to participate in all events organized by National Societies and IPRAS
• Strengthening ties of professional cooperation and friendship with colleagues beyond national borders all over the world
• Information regarding the developments of plastic surgery worldwide
International Confederation for Plastic Reconstuctive and Aesthetic Surgery
IPRAS BENEFITS FOR NATIONAL ASSOCIATIONS
• Association support for educational and research purposes
• Association legal & ethical advice according to international law and practices and assistance with crisis management
• Promotion of local or regional events through the official IPRAS management office
• Promotion of local or regional news and a Historical Account for the Association through the IPRAS Journal
• Free shipment of copies and electronic receipt of the IPRAS Journal
• Immediate information and advice about safety warnings on devices, drugs and procedures
• Information regarding the proper use of all materials, substances and techniques related to Plastic, Reconstructive and Aesthetic Surgery through IQUAM (the International Committee of Quality Assurance and Medical Devices in Plastic Surgery) General Consensus statement, with an update every 2 years
• Promotion of Patient Safety and Quality Management (in cooperation with the World Health Organization - WHO)
• Information regarding harmonization of training
• Information regarding accreditation of Plastic Surgery Units
• Protection of the Specialty and Promotion of its image world-wide
• Information and reports about events organized by other National Societies and IPRAS
International Confederation for Plastic Reconstuctive and Aesthetic Surgery

IPRAS Management OfficeZITA CONGRESS SA
1st km Peanias Markopoulou AveP.O BOX 155, 190 02 Peania Attica, Greece
Tel: (+30) 211 100 1770-1, Fax: (+30) 210 664 2216URL: www.ipras.org • E-mail: [email protected]
Executive Director: Zacharias Kaplanidis E-mail: [email protected]
Assistant Executive Director: Maria Petsa E-mail: [email protected]
Accounting Director: George Panagiotou E-mail: [email protected]
Associations Management Director: Dimitris Synodinos E-mail: [email protected]
Commercial Director: Gerasimos Kouloumpis E-mail: [email protected]
Next issue: April 2012
DISCLAIMER:IPRAS journal is published by IPRAS. IPRAS and IPRAS Management Office, its staff, editors authors and contributors do not recommend, endorse or make any representation about the efficacy, appropriateness or suitability of any specific tests, products, procedures, treatments, services, opinions, health care providers or other information that may be contained on or available through this journal. The information provided on the IPRAS JOURNAL is not intended or implied to be a substitute for professional medical advice, diagnosis or treatment. All content, including text, graphics, images and information, contained on this journal is for general information purposes only. IPRAS, IPRAS Management Office and its staff, editors, contributors and authors ARE NOT RESPONSIBLE NOR LIABLE FOR ANY ADVICE, COURSE OF TREATMENT, DIAGNOSIS OR ANY OTHER INFORMATION, SERVICES OR PRODUCTS THAT YOU OBTAIN THROUGH THIS JOURNAL. NEVER DISREGARD PROFESSIONAL MEDICAL ADVICE OR DELAY SEEKING MEDICAL TREATMENT BECAUSE OF SOMETHING YOU HAVE READ ON OR ACCESSED THROUGH THIS JOURNAL.
While every effort has been made to ensure accuracy, neither the publisher, IPRAS, IPRAS Management Office and its staff, editors, authors and or contributors shall have any liability for errors and/or omissions. Readers should always consult with their doctors before any course of treatment.
©Copywright 2010 by the International Confederation of Plastic, Reconstructive and Aesthetic Surgery. All rights reserved. Contents may not be reproduced in whole or in part without written permission of IPRAS.
Not for sale. Distributed for free.
IPRAS Journal Management Editor: IPRAS Editor-in-Chief: Thomas Biggs, MD Editorial Board: Marita Eisenmann - Klein, MD Andreas Yiacoumettis, MD Christian Echinard, MD Constance Neuhann-Lorenz, MD Zacharias Kaplanidis, Economist Page Layout: Ioannis Karanasis E-mail: [email protected] Post Editing: Athena Spanou, MD Photographer: Julian Klein
7th Issue January 2012