journal of cancer policy - authentification of cancer policy 12 (2017) ... in endometrial cancer....
TRANSCRIPT

O
D
FJa
b
c
1d
Qe
f
a
ARAA
KCNDTL
1
cp
MC
(jwd
h2
Journal of Cancer Policy 12 (2017) 21–27
Contents lists available at ScienceDirect
Journal of Cancer Policy
jou rn al h om epage: www.elsev ier .com/ locate / j cpo
riginal Research
efining care trajectories: The example of endometrial cancer
ranc ois Béland a,b,c,∗, Claude Galand a, John D. Fletcher a, Walter H. Gotlieb d,eremie Abitbol d, Dominic Julien a,e,f
Solidage Research Group, CSSS de la Montagne, Site Métro, 1801, boul. de Maisonneuve Ouest, Room 600, Montréal, Québec H3H 1J9 CanadaDepartment of Health, Management, Evaluation and Policy, Université de Montréal, C.P. 6128, Succursale Centre-ville, Montréal, Québec H3C 3J7 CanadaDivision of Geriatric Medicine, McGill University, Jewish General Hospital, 3755, chemin de la Côte-Ste-Catherine, Room E-0012, Montréal, Québec H3TE2 CanadaDivision of Gynaecologic Oncology, Segal Cancer Center, Jewish General Hospital, McGill University, 3755, chemin de la Côte-Ste-Catherine, Montréal,uébec H3T 1E2 CanadaResearch Center, Institut universitaire en santé mentale de Montréal, 7331, rue Hochelaga, Montréal, Québec H1N 3V2 CanadaDepartment of Psychology, Université de Montréal, Pavillon Marie-Victorin, C. P. 6128, Succursale Centre-ville, Montréal, Québec H3C 3J7 Canada
r t i c l e i n f o
rticle history:eceived 12 July 2016ccepted 12 December 2016vailable online 16 December 2016
eywords:ancereoplasmselivery of health carerajectoriesatent class analysis
a b s t r a c t
Background: The era of patient-centered care might lead to the conclusion that there are as many configu-rations of healthcare utilization within episodes of care as there are patients. However, variability amongepisodes of care is limited by factors such as local resources or patient characteristics. As a result, thedifferences among episodes of care are reduced, and a limited number of care trajectories are expected.Objective: The aim of this study was to investigate the ability to identify clinically significant care trajec-tories using data on healthcare services used by patients with endometrial cancer.Methods: A retrospective review of sixteen healthcare services used by 394 patients newly diagnosedwith endometrial cancer was undertaken. Latent class analysis was used to investigate care trajectories.Results: The analyses segregated patients into six care trajectories: 1) surgery without hospitalizationsand emergency room [ER] visits; 2) surgery with hospitalizations and ER visits; 3) surgery, radiation therapy,and chemotherapy, without hospitalizations and ER visits; 4) surgery, radiation therapy, and chemotherapy,with hospitalizations and ER visits; 5) surgery and radiation therapy; 6) surgery and chemotherapy, with
hospitalizations and ER visits. Classification of patients in trajectories with versus without hospitalizationsand ER visits could only partially be explained by age, cancer stage, and grade.Concluding statement: Utilization of healthcare services can be grouped into a number of defined trajecto-ries in endometrial cancer. Identifying care trajectories and parameters associated with care trajectoriescould have important clinical and administrative implications.© 2016 Elsevier Ltd. All rights reserved.
. Introduction
Episodes of care are series of temporally contiguous health-are services related to treatment of an illness [1]. In the era ofatient-centered care, care services are tailored to patients’ needs
∗ Corresponding author at: Solidage Research Group, CSSS de la Montagne, Siteétro, 1801, boul. de Maisonneuve Ouest, Room 600, Montréal, Québec H3H 1J9
anada.E-mail addresses: [email protected]
F. Béland), [email protected] (C. Galand),[email protected] (J.D. Fletcher),
[email protected] (W.H. Gotlieb), [email protected] (J. Abitbol),[email protected] (D. Julien).
ttp://dx.doi.org/10.1016/j.jcpo.2016.12.001213-5383/© 2016 Elsevier Ltd. All rights reserved.
[2], which might lead to the conclusion that there are as many con-figurations of healthcare utilization within episodes of care as thereare patients. However, variability among episodes of care is lim-ited by factors such as local resources, clinical practice guidelines,patient characteristics, and severity of the condition. As a result,the differences among episodes of care are reduced, and a lim-ited number of care trajectories are expected. However, limitingan episode of care to healthcare utilization for a single health con-dition leaves out significant parts of healthcare utilization for otherhealth conditions within the same time period. Care trajectoriescan therefore be understood as the layout of a series of grouped
and contiguous healthcare services (medical visits, interventions,prescriptions, etc.) for all conditions occurring within a time periodwhereby a single health issue evolves from diagnosis to discontin-
2 Cancer Policy 12 (2017) 21–27
ue
wcn
Tcaonvc
iocma
2
2
itTtaea
2
2
aEnaad
2
ldappof
voootto
Table 1Characteristics of 394 patients newly diagnosed with endometrial cancer includedin the analyses.
Characteristics N (%) Mean (SD)
Age at inception 64.9 (12.3)Tumor histology
Endometrioid tumor and alike 341 (86.6)Clear cell and serous carcinoma 37 (9.4)Carcicosarcomas 12 (3.1)Other 4 (1.0)
Cancer stageStage I 272 (69.0)Stage II 31 (7.9)Stage III 62 (15.7)Stage IV 20 (5.1)Not determined, missing 9 (2.3)
Cancer gradeWell-differentiated 155 (39.3)Moderately differentiated 99 (25.1)Poorly differentiated 125 (31.7)Undifferentiated 5 (1.3)Not determined, missing 10 (2.5)
Healthcare servicesSurgical treatment for cancer 339 (86.0)Radiation therapy 146 (37.1)Chemotherapy 123 (31.2)Medical oncologist 66 (16.8)Oncology nurse navigator 201 (51.0)Oncology/radiation oncology nurse 167 (42.4)Oncology allied health 83 (21.1)Surgical specialist 73 (18.5)Medical specialist 145 (36.8)Nursing and allied health 121 (30.7)Obstetrics/gynecology specialist 71 (18.0)Hospitalizations 100 (25.4)ER visits 126 (32.0)Surgical oncologist 8 (2.0)Radiation oncologist 187 (47.5)
2 F. Béland et al. / Journal of
ation of treatments for this issue, and carried out in a healthcarenvironment [3].
Identifying care trajectories as well as parameters associatedith trajectories (that is, their correlates) could have important
linical and administrative implications, such as treatment plan-ing and allocation of resources.
Two studies have investigated care trajectories in cancer [4,5].he two studies, conducted among patients presenting with breastancer, identified a variety of trajectories using data miningpproaches. Healthcare services were restricted to active oncol-gy treatments or hospitalizations in those two studies, and didot include other types of services such as emergency room (ER)isits or contacts with health professionals. In addition, trajectoryorrelates were not investigated.
The aim of the current study was to investigate the abil-ty to identify clinically significant care trajectories using datan healthcare services used by patients with endometrial can-er. An operational definition of care trajectories is proposed, aethodological procedure to evaluate care trajectories is tested,
nd trajectory correlates are investigated.
. Materials and methods
.1. Data collection
The data for this study were obtained from seven databases reg-stering mandatory medical activities in a cancer center affiliatedo an academic hospital in Montreal, Canada (see Supplementaryable 1). Data pertaining to diagnosis and healthcare service utiliza-ion were collected from patients’ digital files. The study includesll consecutive patients, above the age of 18, newly diagnosed withndometrial cancer from 2008 to 2012 (N = 394). The study waspproved by the center’s research ethics committee.
.2. Measures
.2.1. CancerTumor histology was categorized into endometrioid tumor and
like, clear cell and serous carcinoma, carcinosarcomas, and other.ndometrial cancer stage (I to IV) was according to the FIGO (Inter-ational Federation of Gynecology and Obstetrics) classification [6],nd cancer grade was categorized into well-differentiated, moder-tely differentiated, poorly differentiated, undifferentiated, and notetermined/missing.
.2.2. Healthcare servicesUtilization of sixteen healthcare services (see Table 1) was col-
ected from the databases. The services were classified into fiveomains: (i) active oncology treatment (surgery, radiation ther-py, chemotherapy); (ii) outpatient contacts with a healthcarerofessional in oncology for medical exams or follow-ups; (iii) out-atient contacts with a healthcare professional in family mediciner in medical specialties other than oncology for medical exams orollow-ups; (iv) hospitalizations; and (v) ER visits.
A dummy variable was created for each of the sixteen ser-ices, representing whether or not patients used the services. Inur sample, almost every patient had visits with a gynecologicncologist (94%) and almost no patients had visits with a surgical
ncologist (2%). These variables were excluded from the analyses ashey could unlikely discriminate between trajectories. In addition,hose receiving radiation therapy were invariably seen by radiationncologists, so the latter variable was removed from the analyses.Gynecologic oncologist 371 (94.2)
NOTE: SD = Standard deviation.
2.3. Operationalization of episodes of care
In this study, the episode of care began with the diagnosis ofendometrial cancer and was deemed completed when no activecancer treatments (i.e., cancer surgery, chemotherapy, or radiationtherapy) were provided for a period of at least four months. Thistimeframe was selected as it represents the time period betweenroutine follow-up visits during the first two years following remis-sion in our institution. Care trajectories were identified using dataon all healthcare services utilized at the hospital during the firstepisode of care. Healthcare utilization was followed from the timeof diagnosis up to March 31, 2014.
2.4. Statistical analyses
To investigate individual trajectories, longitudinal calendargrids [7] were constructed using the SAS software (version 9.3).Day-to-day healthcare utilization (e.g., type of service, duration,name of the healthcare professional) was mapped in the grids.
Latent class analysis [8,9] was used to group the sample intocategories of individuals (the trajectories) who are similar within acategory but different from individuals in other categories [10]. Inlatent class analysis, competing models presenting different num-bers of trajectories are compared with fit indexes to determine themodel that best fits the data. Criteria to decide on the number of
trajectories used in this study were: (i) low Akaike’s InformationCriterion (AIC), Bayesian Information Criterion (BIC) and adjustedBIC; (ii) a significant Lo-Mendell-Rubin (LMR) test; (iii) a significantparametric bootstrapped likelihood ratio test (BLRT) [11]; and (iv)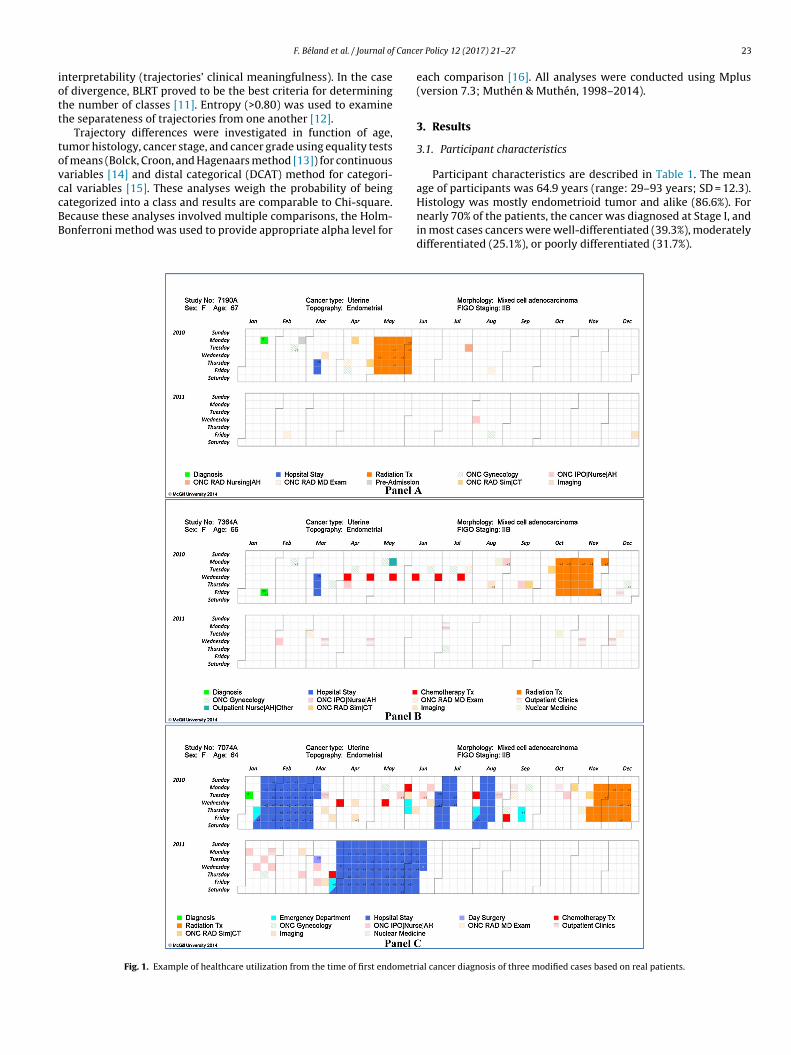
Cance
iott
tovccBB
F. Béland et al. / Journal of
nterpretability (trajectories’ clinical meaningfulness). In the casef divergence, BLRT proved to be the best criteria for determininghe number of classes [11]. Entropy (>0.80) was used to examinehe separateness of trajectories from one another [12].
Trajectory differences were investigated in function of age,umor histology, cancer stage, and cancer grade using equality testsf means (Bolck, Croon, and Hagenaars method [13]) for continuousariables [14] and distal categorical (DCAT) method for categori-al variables [15]. These analyses weigh the probability of being
ategorized into a class and results are comparable to Chi-square.ecause these analyses involved multiple comparisons, the Holm-onferroni method was used to provide appropriate alpha level forFig. 1. Example of healthcare utilization from the time of first endometr
r Policy 12 (2017) 21–27 23
each comparison [16]. All analyses were conducted using Mplus(version 7.3; Muthén & Muthén, 1998–2014).
3. Results
3.1. Participant characteristics
Participant characteristics are described in Table 1. The meanage of participants was 64.9 years (range: 29–93 years; SD = 12.3).
Histology was mostly endometrioid tumor and alike (86.6%). Fornearly 70% of the patients, the cancer was diagnosed at Stage I, andin most cases cancers were well-differentiated (39.3%), moderatelydifferentiated (25.1%), or poorly differentiated (31.7%).ial cancer diagnosis of three modified cases based on real patients.

2 Cance
3
rtwpooss
FNtR
4 F. Béland et al. / Journal of
.2. Individual care trajectories
Fig. 1 (Panels A to C) illustrates three longitudinal calendar gridsepresenting the day-to-day utilization of healthcare services ofhree patients diagnosed with endometrial cancer and presentingith the same tumor histology, stage, and grade (data modified to
reserve anonymity). In the first example (Panel A), the episode
f care was short, and comprised surgery and multiple sessionsf adjuvant radiation therapy, followed by medical visits. In theecond example (Panel B), the patient had surgery, received sixessions of chemotherapy, and then received multiple sessions ofig. 2. Relative importance of utilization of healthcare services stratified by trajectories.OTE. S: Surgery without Hospitalizations and Emergency Room [ER] visits; SCH: Surgery
alizations and ER Visits; SR: Surgery and Radiation Therapy; SRC: Surgery, Radiation Thadiation Therapy, and Chemotherapy, with Hospitalizations and ER Visits.
r Policy 12 (2017) 21–27
radiation therapy. Follow-up medical visits were recorded. Thethird example (Panel C) illustrates a more complex case with longsequences of hospitalizations and ER visits interspersed with activeoncological treatments. These examples illustrates that there aredifferences in individual care trajectories even in cases with thesame cancer site, tumor, stage, and grade.
3.3. Care trajectories
Two- to eight-class (trajectory) models were investigated usinglatent class analysis. The fit indexes of the different models did not
and Chemotherapy, with Hospitalizations and ER Visits; SH: Surgery with Hospi-erapy, and Chemotherapy, without Hospitalizations and ER Visits; SRCH: Surgery,
F. Béland et al. / Journal of Cancer Policy 12 (2017) 21–27 25
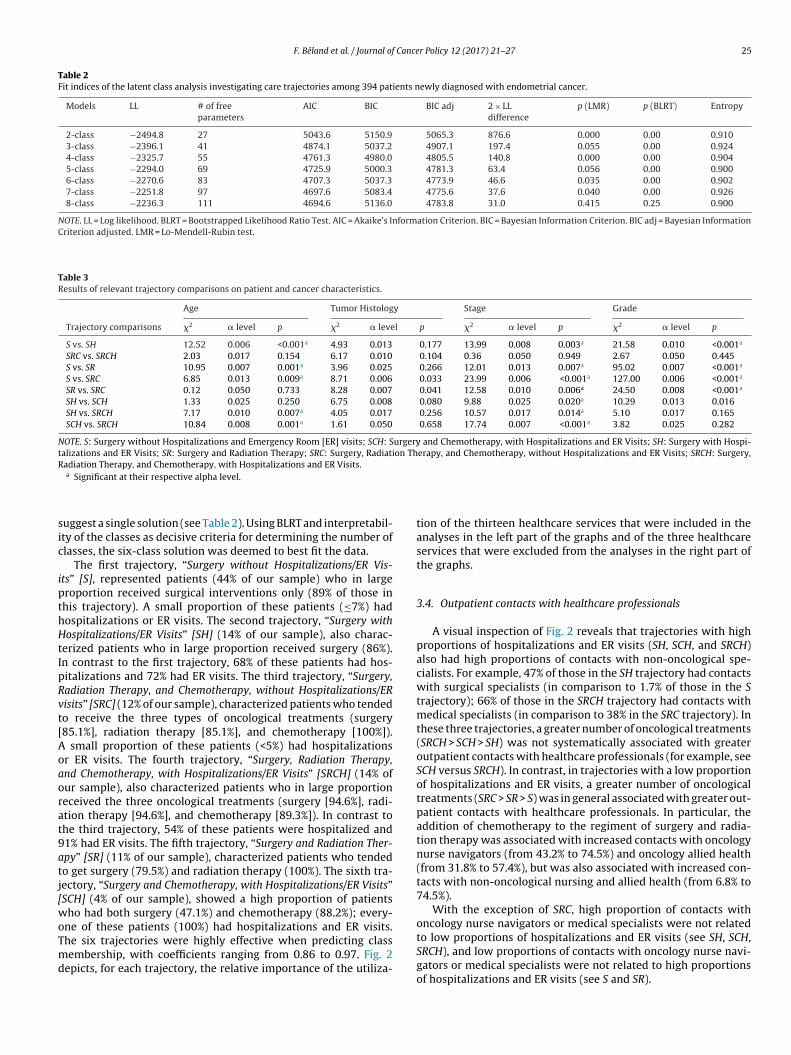
Table 2Fit indices of the latent class analysis investigating care trajectories among 394 patients newly diagnosed with endometrial cancer.
Models LL # of freeparameters
AIC BIC BIC adj 2 × LLdifference
p (LMR) p (BLRT) Entropy
2-class −2494.8 27 5043.6 5150.9 5065.3 876.6 0.000 0.00 0.9103-class −2396.1 41 4874.1 5037.2 4907.1 197.4 0.055 0.00 0.9244-class −2325.7 55 4761.3 4980.0 4805.5 140.8 0.000 0.00 0.9045-class −2294.0 69 4725.9 5000.3 4781.3 63.4 0.056 0.00 0.9006-class −2270.6 83 4707.3 5037.3 4773.9 46.6 0.035 0.00 0.9027-class −2251.8 97 4697.6 5083.4 4775.6 37.6 0.040 0.00 0.9268-class −2236.3 111 4694.6 5136.0 4783.8 31.0 0.415 0.25 0.900
NOTE. LL = Log likelihood. BLRT = Bootstrapped Likelihood Ratio Test. AIC = Akaike’s Information Criterion. BIC = Bayesian Information Criterion. BIC adj = Bayesian InformationCriterion adjusted. LMR = Lo-Mendell-Rubin test.
Table 3Results of relevant trajectory comparisons on patient and cancer characteristics.
Age Tumor Histology Stage Grade
Trajectory comparisons �2 � level p �2 � level p �2 � level p �2 � level p
S vs. SH 12.52 0.006 <0.001a 4.93 0.013 0.177 13.99 0.008 0.003a 21.58 0.010 <0.001a
SRC vs. SRCH 2.03 0.017 0.154 6.17 0.010 0.104 0.36 0.050 0.949 2.67 0.050 0.445S vs. SR 10.95 0.007 0.001a 3.96 0.025 0.266 12.01 0.013 0.007a 95.02 0.007 <0.001a
S vs. SRC 6.85 0.013 0.009a 8.71 0.006 0.033 23.99 0.006 <0.001a 127.00 0.006 <0.001a
SR vs. SRC 0.12 0.050 0.733 8.28 0.007 0.041 12.58 0.010 0.006a 24.50 0.008 <0.001a
SH vs. SCH 1.33 0.025 0.250 6.75 0.008 0.080 9.88 0.025 0.020a 10.29 0.013 0.016SH vs. SRCH 7.17 0.010 0.007a 4.05 0.017 0.256 10.57 0.017 0.014a 5.10 0.017 0.165SCH vs. SRCH 10.84 0.008 0.001a 1.61 0.050 0.658 17.74 0.007 <0.001a 3.82 0.025 0.282
NOTE. S: Surgery without Hospitalizations and Emergency Room [ER] visits; SCH: Surgery and Chemotherapy, with Hospitalizations and ER Visits; SH: Surgery with Hospi-talizations and ER Visits; SR: Surgery and Radiation Therapy; SRC: Surgery, Radiation Therapy, and Chemotherapy, without Hospitalizations and ER Visits; SRCH: Surgery,Radiation Therapy, and Chemotherapy, with Hospitalizations and ER Visits.
sic
ipthHtIpRvt[Aoaorat9atj[woTmd
a Significant at their respective alpha level.
uggest a single solution (see Table 2). Using BLRT and interpretabil-ty of the classes as decisive criteria for determining the number oflasses, the six-class solution was deemed to best fit the data.
The first trajectory, “Surgery without Hospitalizations/ER Vis-ts” [S], represented patients (44% of our sample) who in largeroportion received surgical interventions only (89% of those inhis trajectory). A small proportion of these patients (≤7%) hadospitalizations or ER visits. The second trajectory, “Surgery withospitalizations/ER Visits” [SH] (14% of our sample), also charac-
erized patients who in large proportion received surgery (86%).n contrast to the first trajectory, 68% of these patients had hos-italizations and 72% had ER visits. The third trajectory, “Surgery,adiation Therapy, and Chemotherapy, without Hospitalizations/ERisits” [SRC] (12% of our sample), characterized patients who tendedo receive the three types of oncological treatments (surgery85.1%], radiation therapy [85.1%], and chemotherapy [100%]).
small proportion of these patients (<5%) had hospitalizationsr ER visits. The fourth trajectory, “Surgery, Radiation Therapy,nd Chemotherapy, with Hospitalizations/ER Visits” [SRCH] (14% ofur sample), also characterized patients who in large proportioneceived the three oncological treatments (surgery [94.6%], radi-tion therapy [94.6%], and chemotherapy [89.3%]). In contrast tohe third trajectory, 54% of these patients were hospitalized and1% had ER visits. The fifth trajectory, “Surgery and Radiation Ther-py” [SR] (11% of our sample), characterized patients who tendedo get surgery (79.5%) and radiation therapy (100%). The sixth tra-ectory, “Surgery and Chemotherapy, with Hospitalizations/ER Visits”SCH] (4% of our sample), showed a high proportion of patients
ho had both surgery (47.1%) and chemotherapy (88.2%); every-ne of these patients (100%) had hospitalizations and ER visits.
he six trajectories were highly effective when predicting classembership, with coefficients ranging from 0.86 to 0.97. Fig. 2epicts, for each trajectory, the relative importance of the utiliza-
tion of the thirteen healthcare services that were included in theanalyses in the left part of the graphs and of the three healthcareservices that were excluded from the analyses in the right part ofthe graphs.
3.4. Outpatient contacts with healthcare professionals
A visual inspection of Fig. 2 reveals that trajectories with highproportions of hospitalizations and ER visits (SH, SCH, and SRCH)also had high proportions of contacts with non-oncological spe-cialists. For example, 47% of those in the SH trajectory had contactswith surgical specialists (in comparison to 1.7% of those in the Strajectory); 66% of those in the SRCH trajectory had contacts withmedical specialists (in comparison to 38% in the SRC trajectory). Inthese three trajectories, a greater number of oncological treatments(SRCH > SCH > SH) was not systematically associated with greateroutpatient contacts with healthcare professionals (for example, seeSCH versus SRCH). In contrast, in trajectories with a low proportionof hospitalizations and ER visits, a greater number of oncologicaltreatments (SRC > SR > S) was in general associated with greater out-patient contacts with healthcare professionals. In particular, theaddition of chemotherapy to the regiment of surgery and radia-tion therapy was associated with increased contacts with oncologynurse navigators (from 43.2% to 74.5%) and oncology allied health(from 31.8% to 57.4%), but was also associated with increased con-tacts with non-oncological nursing and allied health (from 6.8% to74.5%).
With the exception of SRC, high proportion of contacts withoncology nurse navigators or medical specialists were not related
to low proportions of hospitalizations and ER visits (see SH, SCH,SRCH), and low proportions of contacts with oncology nurse navi-gators or medical specialists were not related to high proportionsof hospitalizations and ER visits (see S and SR).
2 Cance
3c
cPiasu
tpS(p
twat
m(hdt(S
mSitt
4
ts
dsca
Ttptopttsv
rapactr
6 F. Béland et al. / Journal of
.5. Care trajectory differences in patient and cancerharacteristics
Descriptions of the six care trajectories in terms of patient andancer characteristics are presented in Supplementary Figure 1.re-planned comparisons (based on key trajectory features) were
nvestigated to examine whether trajectories differed on patientnd cancer characteristics (Table 3). (All trajectory comparisons andignificance of results are available from the corresponding authorpon request.)
Two of the trajectories were characterized by having surgery ashe sole oncological treatment but differentiated by whether or notatients were hospitalized and had ER visits (S and SH). Those in the
trajectory were significantly younger and had less advanced stagemore Stage I) and lower grade (more well-differentiated and lessoorly differentiated) than those in the SH trajectory.
Two trajectories were characterized by having received thehree types of oncological treatments, but discriminated byhether or not patients were hospitalized and had ER visits (SRC
nd SRCH). No significant differences were observed between thesewo trajectories on age, tumor histology, stage, and grade.
Three trajectories consisted of different sets of oncological treat-ents but all had a low usage of hospitalizations and ER visits
S, SR, and SRC). Those in the S trajectory were younger andad less advanced stage (mostly stage I) and grade (mostly well-ifferentiated) than those in the SR and SRC trajectories. Those inhe SR trajectory had less advanced stage (less Stage III) and grademore moderately and less poorly differentiated) than those in theRC trajectory.
Three trajectories consisted of different sets of oncological treat-ents but all had a high usage of hospitalizations and ER visits (SH,
CH, and SRCH). Those in the SH and SCH trajectories were signif-cantly older than those in the SRCH trajectory. Those in the SHrajectory had less advanced stage whereas those in the SCH trajec-ory had more advanced stage than those in the SRCH trajectory.
. Discussion
The aim of this study was to investigate the ability to iden-ify clinically relevant care trajectories using data on healthcareervices used by patients with endometrial cancer.
Computerized longitudinal calendar grids were developed toisplay a detailed history of patients’ utilization of healthcareervices (Fig. 1). This platform enables physicians to grasp theomplexity of service utilization at a glance, take critical decisionsccordingly, and assess case management efficacy.
Six care trajectories were identified using latent class analysis.wo of the trajectories were characterized by having surgery ashe sole oncological treatment but differentiated by whether or notatients were hospitalized and had ER visits (S and SH). Two otherrajectories were characterized by having received the three typesf oncological treatments, again discriminated by whether or notatients were hospitalized and had ER visits (SRC and SRCH). A fifthrajectory included patients who had surgery and received radia-ion therapy (SR). A sixth trajectory characterized patients who hadurgery, received chemotherapy, and had hospitalizations and ERisits (SCH).
Our results suggest that care trajectories in endometrial cancerevolve around two axes: specific sets of oncological treatmentsnd whether the sets of treatments were associated with hos-italizations and ER visits. The three trajectories that were not
ssociated with hospitalizations and ER visits seem to mirror clini-al pathways corresponding to straightforward endometrial cancerreatment. Trajectories associated with clinical pathways were alsoeported in breast cancer [4]. However, the three trajectories thatr Policy 12 (2017) 21–27
were associated with hospitalizations and ER visits seem to deviatefrom these pathways and they can thus be considered to be “notclassical”. These trajectories also had higher proportions of patientshaving contacts with non-oncological specialists, such as surgicalor medical specialists, suggesting that the individuals in these tra-jectories may either have comorbidities, treatment complications,or be medically more complex.
In our study, low outpatient contacts with healthcare profes-sionals such as oncology nurse navigators or medical specialists wasnot associated with high hospitalizations/ER visits. This suggeststhat low outpatient contacts with healthcare professionals wasnot the cause of increased hospitalizations/ER visits. In addition,high contacts with oncology nurse navigators or medical special-ists were not related to low hospitalizations and ER visits. Thiscould reflect the nature of the patient, their medical complexity,or perhaps that these health professionals do not have the righttools to prevent patients from being hospitalized or using the ER.Alternately, this may suggest that they refer to the ER and hospi-talizations when they deem it indicated [17].
In our study, we observed significant differences between mosttrajectory comparisons on age, stage, and grade, but, unexpect-edly, trajectories did not differ on tumor histology. In addition, age,tumor histology, stage, and grade could not explain, among thosereceiving the three types of oncological treatments, why some havehospitalizations and ER visits (SRC) while others do not (SRCH).Possible explanations are that those with hospitalizations and ERvisits have more chronic illnesses or lower social support, but thiscould not be investigated with the administrative and clinical dataat hand. Despite differences in age, stage and grade, a visual inspec-tion of Supplementary Figure 1 reveals that these variables aredistributed in almost every trajectory, suggesting that other fac-tors are involved in the making of care trajectories. Therefore, othercharacteristics must be considered to increase our understandingof care trajectories. Parameters that can be prevented or that areamenable to change (such as chronic illnesses or social support)are of special interest, in order to increase patients’ health anddecrease the proportion of patients in trajectories with high serviceutilization.
Care trajectories could be a useful, evidence-based tool for clini-cians and administrators. For clinicians, the identification of patientand disease characteristics associated with specific trajectoriesenables clinicians to identify and perhaps predict complex casesthat may require special attention or a greater use of healthcareservices. The clinician could thus take pre-emptive measures todecrease hospitalizations, tailor the management of the diseaseto the patient, and optimize treatment algorithms and time man-agement, thereby enhancing quality of care. For administrators,identifying trajectories allows for more accurate budget planningand allocation of resources based on service utilization rates. Forexample, a change in best practice guidelines towards a combi-nation of surgery, radiation therapy, and chemotherapy wouldincrease the proportion of patients in SRC and SRCH trajectories.Given these trajectories are associated with contacts with oncologynurse navigators, administrators could hire additional staff aheadof time. Identifying trajectories with particularly high resource usecould also help isolate problem areas and manage accordingly.Indeed, trajectories with high hospitalization and ER visits are likelycostly and may, in some instances, be markers of lower quality ofcare.
A limitation of the study is its retrospective design, with lim-ited information to investigate sociodemographic, psychosocial,and social differences among trajectories. Among the strengths
of this study, care trajectories were entirely delineated using sta-tistical procedures and were derived from objective rather thanself-reported data.
Cance
goteFtp
F
–JRtt
A
t
R
[
[
[
[
[
[flexible model-based approach, Struct. Equ. Model. 20 (2013) 1–26.
[16] S. Holm, A simple sequentially rejective multiple test procedure, Scand. J. Stat.6 (1979) 65–70.
F. Béland et al. / Journal of
We conclude that the utilization of healthcare services can berouped into a limited number of care trajectories. Knowledgef care trajectories and their components may be used to adjustreatment goals, enhance healthcare management, and improvefficiency and cost-effectiveness, resulting in higher value of care.urther studies in this area should actively be pursued to develophe full potential of care trajectories as an assessment tool andlanning aid for effective patient care.
unding
This work was supported by the Fonds de recherche du Québec Santé (grant number 26677). The Rossy Cancer Network and the
ewish General Hospital Foundation provided additional support.esearch in Gynaecologic Oncology is supported by grants fromhe Montreal Israel Cancer Research Fund, Gloria’s Girls Fund, andhe Levi Family Fund.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at http://dx.doi.org/10.1016/j.jcpo.2016.12.001.
eferences
[1] M.C. Hornbrook, A.V. Hurtado, R.E. Johnson, Health care episodes: definition,
measurement and use, Med. Care Res. Rev. 42 (1985) 163–218.[2] Institute of Medicine, Crossing the quality chasm: a new health system for the21st century, National Academy Press, 2001.
[3] C. Galand, D., Julien, F. Béland, Health Care Trajectories in Cancer: ASystematic and Scoping Review, Manuscript in preparation.
[
r Policy 12 (2017) 21–27 27
[4] G. Defossez, A. Rollet, O. Dameron, P. Ingrand, Temporal representation of caretrajectories of cancer patients using data from a regional information system:an application in breast cancer, BMC Med. Inform. Decis. Mak. 14 (2014) 24.
[5] N. Jay, G. Nuemi, M. Gadreau, C. Quantin, A data mining approach for groupingand analyzing trajectories of care using claim data: the example of breastcancer, BMC Med. Inform. Decis. Mak. 13 (2013) 130.
[6] S. Pecorelli, Revised FIGO staging for carcinoma of the vulva, cervix, andendometrium, Int. J. Gynecol. Obstet. 105 (2009) 103–104.
[7] M. Zdeb, R. Allison, Stretching the bounds of sas/graph software, Proceedingsof the Thirtieth Annual SAS Users Group International Conference, 2005,Paper 137–30 (2005).
[8] L.M. Collins, S.T. Lanza, The Relation Between the Latent Variable and ItsIndicators, in Latent Class and Latent Transition Analysis: With Applicationsin the Social, Behavioral, and Health Sciences, John Wiley & Sons, New Jersey,2013, pp. 49–76.
[9] B.O. Muthén, Beyond SEM: general latent variable modeling, Behaviormetrika29 (2002) 81–117.
10] B. Muthén, L.K. Muthén, Integrating person-centered and variable-centeredanalyses: growth mixture modeling with latent trajectory classes, Alcohol.Clin. Exp. Res. 24 (2000) 882–891.
11] K.L. Nylund, T. Asparouhov, B.O. Muthén, Deciding on the number of classes inlatent class analysis and growth mixture modeling: a Monte Carlo simulationstudy, Struct. Equ. Model. 14 (2007) 535–569.
12] B.O. Muthén, Entropy and interpretation. http://www.statmodel.com/discussion/messages/14/3893.html, 2009 (Accessed 24 February 2014).
13] A. Bolck, M. Croon, J. Hagenaars, Estimating latent structure models withcategorical variables: one-step versus three-step estimators, Pol. Anal. 12(2004) 3–27.
14] Z. Bakk, J.K. Vermunt, Robustness of stepwise latent class modeling withcontinuous distal outcomes, Struct. Equ. Model 23 (2016) 20–31.
15] S.T. Lanza, X. Tan, B.C. Bray, Latent class analysis with distal outcomes: a
17] C.S. Bishop, The critical role of oncology nurse practitioners in cancer care:future implications, Oncol. Nurs. Forum 36 (2009) 267–269.