lifestyle changes and cvd prevention_world-heart-day-2010-i-work-with-heart-whf
TRANSCRIPT

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
LIFESTYLE CHANGES LIFESTYLE CHANGES
AND CARDIOVASCULAR AND CARDIOVASCULAR
DISEASE PREVENTION – DISEASE PREVENTION –
FACTS AND PERSPECTIVESFACTS AND PERSPECTIVES
Author: Docent Author: Docent Simovska Vera, Simovska Vera, MD., PhD.MD., PhD. HEPA Macedonia HEPA Macedonia National organizationNational organization spec of sports medicine and public health for the promotion of Health-Enhancing spec. of hygiene nutrition for healthy and sick people Physical Activity www.cindi.makedonija.com
HEPA Makedonija WHO HEPA EuropeMacedonian Medical Society
Doctor Chamber of Macedonia
14 th SYMPOSIUM FOR SPORT AND PHYSICAL EDUCATION Professional-Scientific Conference “I WORK WITH HEARTI WORK WITH HEART” HEPA Macedonia: CME, 18 September 2010, Ohrid

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
F a c t s:F a c t s:
The greatest disease burden in Europe comes from noncommunicable diseases (NCD), especially vascular diseases in general, and coronary, cerebral and peripheral arteries diseases in particular.
Cardiovascular disease (CVD) is causing more than half of all deaths across the WHO European Region. Heart disease and stroke are the leading cause of death in all countries.
The number of deaths due to CVD reaches 4.4 million per year in Europe and 1.9 million per year in the EU.
Lifestyle risk factors (RF) and biological RF for CVD, accumulated throughout the life course have economic, social, gender, political, behavioral and environmental determinants.
From public health perspective, it is of key importance to prevent rather than treat a CVD through promoting healthy behaviors, surveillance of cases and lifestyle changes. Up to 80% of CVD are avoided in Finland from 1969-2009 (Puska P: North Karelia Project).
To reduce the prevalence of CVD, the WHO suggests an approach that emphasizes primary care, multisectoral action and community participation on a national level.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
A i m:A i m:
CVD is closely linked with style of living, genetic variants,
environmental factors and community situation: organization and
society structures.
The primary goals of lifestyle changes is to prevent and to
substantially reduce the burden of CVD. A second aim is to reduce the
risk of CVD in people who are at higher risk of Type 2 DM.
The highest priority in prevention and reduction of CVD is
addressing to common lifestyle RF for noncommunicable disease:
nutritional factors, physical inactivity, tobacco use, higher level of
alcohol consumption and a chronically stressful life and anxiety.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Common lifestyle (behavioral) RF for CVD and main NCDCommon lifestyle (behavioral) RF for CVD and main NCD
To reduce CVD mortality and morbidity, global change in lifestyle RF are needed by implementing the strategy for primary prevention and health promotion.
1. Nutritional factors involved in developing CVD: - high total caloric intake - low dietary fiber - high dietary intake of total fats (saturated and trans fatty acids) - low polyunsaturated (PUFA) to saturated fat ratio (SFA) - high atherogenic potential of diets - high glycaemic index - high sodium intake - unfiltered boiled coffee
- decreased micronutrients intake and level is new RF
The influence of micronutrients upon the risk of CVD is related to oxidative-reductive and inflammatory pathways (WCC, 2010).
2. Low level of physical activity (PALs)
3. Tobacco use
4. High alcohol consumption
5. Psycho-social stress

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Table 1. Biological RF for CVD and/or T2DM related to lifestyleTable 1. Biological RF for CVD and/or T2DM related to lifestyle
Modifiable biological RF Males Females
Raised blood pressure - HTASystolic ≥ 130 mmHg and/or
Diastolic ≥ 85 mmHg
High total cholesterol - TC ≥ 4.5 mmol/L
Reduced HDL-C < 1.03 mmol/L <1.29 mmol/L
Raised triglycerides - TG ≥ 1.7 mmol/L
Raised fasting plasma glucose - FPG ≥ 5.6 mmol/L
Overweight and obesity – BMI > 25 kg/m2; >30 kg/m2
Central obesity - waist circumference (Europids*) ≥ 94 cm* / ≥ 102 cm ≥ 80 cm* / ≥ 88 cm
Low cardiorespiratory fitness – VO2max < 20 ml/kg/min < 14.2 ml/kg/min
Europids*- European and North American cut-of-points

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Classic RF are used in clinical practice to estimate the absolute risk of CVD.
Several risk assessment algorithms have been published for estimating 10-year risk for CHD
such as Framingham score. Also, in the area of biomarkers are included genetic and
functional markers, and new technological development.
To identify genetic factors, which determine CVD risk is an innovative genetic-based health care branch. Telomere biology is relevant to understand biological mechanisms of
vascular ageing: oxidative damage and the relationship between telomere dynamics
in leukocytes and in the vessel wall.
Lifestyle RF for development of CVD might
also adversely affects genetic factors for
vascular ageing and CVD: shorter telomerase
length and low levels of telomerase activity.
Previous studies have not addressed whether
improvements in lifestyle and nutrition are
associated with increases in telomerase activity.
Biomarkers for predicting the risk of CVDBiomarkers for predicting the risk of CVD
Source: ERUSALIMSKY, J., SKENE, C.: MCHANISMS OF
ENDOTHELIAL SENESCENE. Exp.Physiology 2008.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Strategies of CVD prevention and controlStrategies of CVD prevention and control:
Integrated prevention of CVD and other main NCD is based on decrease the prevalence of biological (morph- functional) RF at population level by introducing
changes in the lifestyle (primary prevention) and early detection and treatment (secondary prevention).
The measures of CVD prevention are application of two strategies and their combination giving bigger effects:
“High risk strategy” - identification of the individuals at high risk for development of CVD - measuring level of risk and - life-style changes: weight reduction, antiatherogenic diet, increased physical activity and quit smoking.
“Population/universal strategy” – public health promotion.
Non – modifiable RF for CVDNon – modifiable RF for CVD - Age/simply getting old: Risk of cerebrovascular disease doubles every decade after the age of 55 - A positive family history (genetic predisposition) - Ethnicity: African and Asian are at higher risk of CVD - Gender: High risk for CVD in pre-menopausal women.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Familiar aggregation of CVD risk factors
Risk factors for CVD in the parents from central region of the city of Skopje
Our experiences related to multifactorial etiology of CVDOur experiences related to multifactorial etiology of CVD
Source. Simovska V.: THE PRESENCE OF RISK FACTORS FOR CARDIOVASCULAR DISEASES IN THE FAMILY AND EARLY DETECTION IN THEIR CHILDREN. Post-graduate sub specialization thesis, Medical Faculty University of Belgrade, SR Yugoslavia 1993,

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Number of risk factors for CVD in the parents and their children
INTERACTION OF FAMILY HEREDITARY AND LIFESTYLE FOR INTERACTION OF FAMILY HEREDITARY AND LIFESTYLE FOR
DEVELOPMENT OF CORONARY HEART DISEASE IN LIFE COURSEDEVELOPMENT OF CORONARY HEART DISEASE IN LIFE COURSE
Source: Simovska V., Vidin M: INTERACTION OF FAMILY HEREDITY AND OBESITY IN CHILDREN FOR DEVELOPMENT OF CORONARY HEART DISEASE IN LIFE COURSE. II-nd International Scientific Symposium for Obesity. Zlatibor 1993. The Book of Abstracts, God.IV br.1-2, Suppl. II, 1993:102.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Figure 1.Figure 1. Prevalence of risk Prevalence of risk factors for CVD in factors for CVD in adult population from the central region of Skopjeadult population from the central region of Skopje
2 4 .22 8 .2
7 5
2 .5
2 3 .41 8 .2
1 2 .5
5 8 .3
3 .7
3 5 .23 5 .9
1 8 .21 5 .8
2 8 .8
2 3 .8
1 4 .2
0
2 0
4 0
6 0
8 0
1 9 9 02 0 0 1
%
Clinical–epidemiological study “YUSAD” for research multifactor etiology of CVD (1990)We have done many research studies with aim to reduce the modifiable biological RF for CVD in adults and their children through lifestyle changes.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
The effect of systematic long term physical activity with changeable intensity on plasma lipids and lipoproteins
Figure 2.Figure 2. Lipid metabolism in untrained women Lipid metabolism in untrained women and elite female handball athletesand elite female handball athletes
Simovska V., Vidin M.: DYNAMICS OF CHANGE ON LIPOPROTEIN STATUS DURING THE PREPARATION OF SPORTS TRAINING IN PHASE OF MEZOCICLUS. In: Gruic, N. Ed. Sport and Health. Novi Sad: Medical Faculty 1999, pp. 77-85.
Wellness in the Workplace - I Work with Heart , World Heart Day 2010
75.8
14.99.3
65.5
15.9 18.6
58.8
18.6 23
41.6 41.5
16.8
0
10
20
30
40
50
60
70
80
1990 1995 1998 2001
BMI<25
BMI>25-29.9
BMI>30
%
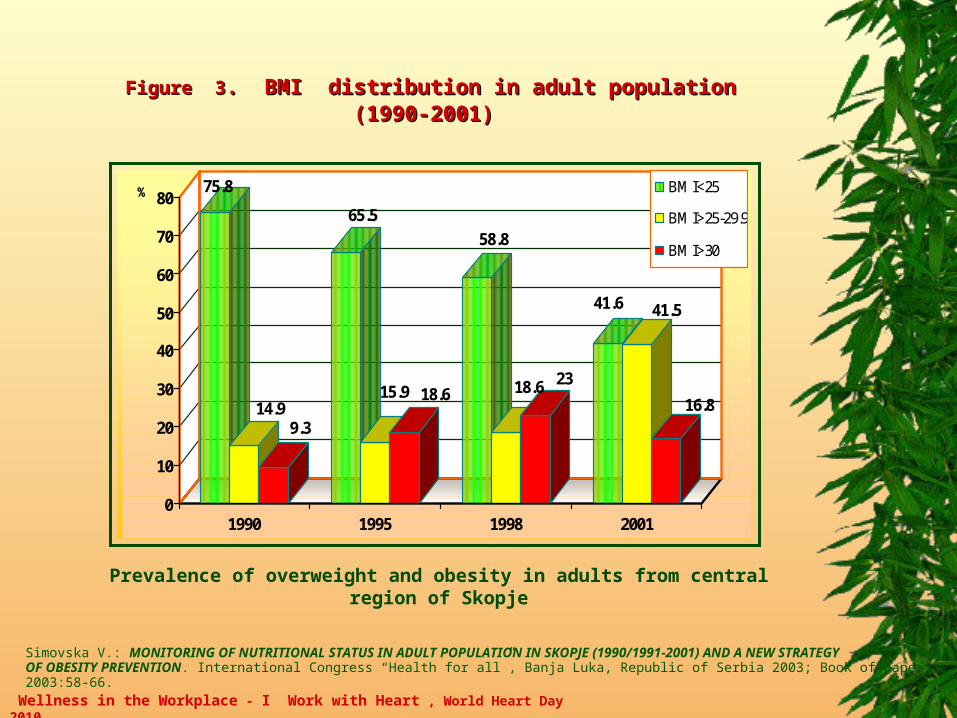
Figure Figure 33. BMI distribution in adult population. BMI distribution in adult population (1990-2001) (1990-2001)
Prevalence of overweight and obesity in adults from central region of Skopje
Simovska V.: MONITORING OF NUTRITIONAL STATUS IN ADULT POPULATION IN SKOPJE (1990/1991-2001) AND A NEW STRATEGY OF OBESITY PREVENTION. International Congress “Health for all”, Banja Luka, Republic of Serbia 2003; Book of papers 2003:58-66.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
CVD RISK REDUCTION: programmed physical activity and diet therapy CVD RISK REDUCTION: programmed physical activity and diet therapy
aimed at high risk abdominal obese individualsaimed at high risk abdominal obese individuals
Objectives:
To promote preventive-therapeutic programmes with a proposal - a measure for macronutrient content of diets and increasing cardiorespiratory fitness (VO2max) intended for abdominal obese individuals who are asymptomatic, but at high-risk for CVD.
To develop a method for prescription of programmed physical activity (PA) in accordance with individual performing the exercise and biological characteristics of individuals.
To estimate the efficiency of the method on CVD risk reduction at abdominal obese individuals included in 7wk. randomised controlled trial.
To construct a new index as mathematical model for predicting the effects of non-pharmacological therapies at obese population on average/increased and high risk for CVD and other NCD.
Source. Simovska V.: EFFECTS OF DIETOTHERAPY AND PROGRAMMED PHYSICAL ACTIVITY ON OBESITY AND IT,S COMPLICATIONS. Ed. ISBN 978-608-200-025-1, Menora, Skopje, 2008.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
41
17
5.7
14.5
1
21.4
43
16
913.7
0
18.3
30
22.5
6.8
23.1
0
17.4
0
5
10
15
20
25
30
35
40
45
1200kcal-Ist phase
1300kcal-WHO CINDI
1200kcal-Ist phase 1400kcal-IIth phase 1300kcal-WHO CINDI
Figure 4.Figure 4. BBasic food groups in daily mails asic food groups in daily mails IIst st andand II IIthth phase of diet therapyphase of diet therapy

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
MACRONUTRIENT CONTENT OF DIETS
CINDI FOOD PYRAMID (WHO)
TabTable 2le 2.. An integrated An integrated CVD CVD risk managementrisk management AntiatherogenicAntiatherogenic diets diets:: 1200 kcal/ 1200 kcal/dd in Iin Istst phase phase (a (a “temporary” diet“temporary” diet))
and 1400 kcal/d and 1400 kcal/d in II in IIndnd phase phase

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Table 3Table 3. M. Micronutrienticronutrient content of diets withcontent of diets withvitamin-minerals supplementation in the Ivitamin-minerals supplementation in the Istst phase of diet phase of diet
Wellness in the Workplace - I Work with Heart , World Heart Day 2010
17
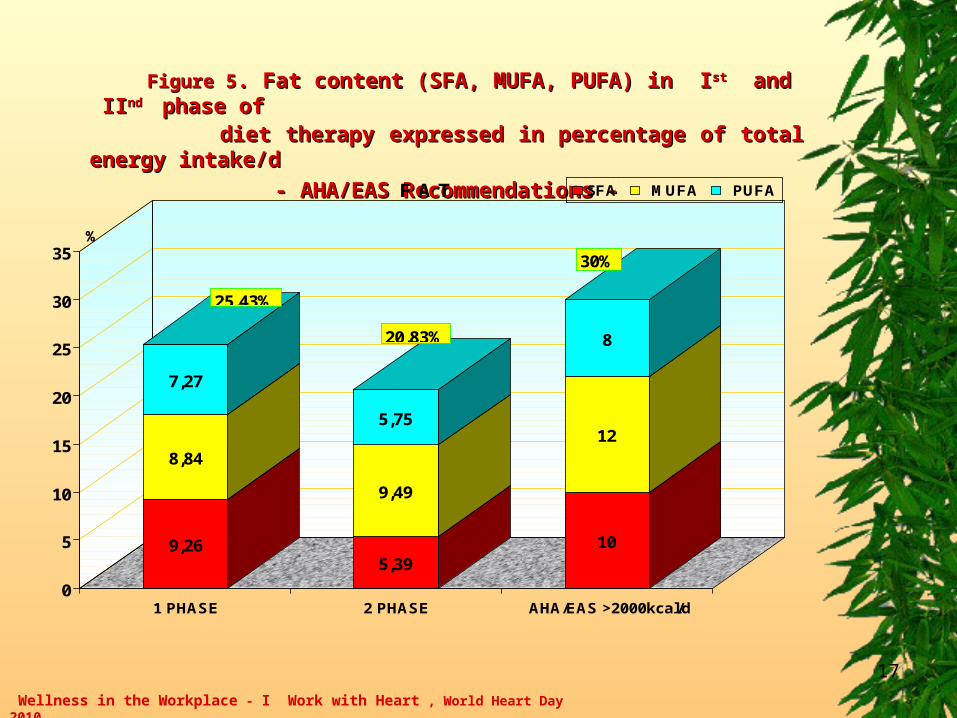
Figure 5Figure 5. Fat content (SFA, MUFA, PUFA) in. Fat content (SFA, MUFA, PUFA) in I Istst andand II IIndnd phase ofphase of diet therapy expressed in percentage of total energy intake/ddiet therapy expressed in percentage of total energy intake/d
- - AHA/EAS AHA/EAS Recommendations -Recommendations -
9,26
8,84
7,27
5,39
9,49
5,75
10
12
8
0
5
10
15
20
25
30
35%
1 PHASE 2 PHASE AHA/EAS >2000kcal/d
F A T SFA MUFA PUFA
25.43%
20.83%
30%

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
18
24.97
75.03
43.71
56.29
60
40
0
10
20
30
40
50
60
70
80
90
100%
Iphase IIphase AHA/EAS
Proteins
vegetable's protein animal's protein
25.28% 25.73% 16%
52.78
47.22
41.13
58.87
30
70
0
10
20
30
40
50
60
70
80
90
100%
Iphase IIphase AHA/EAS
merewa
Carbohydrates
mono/disaharides polysaharides
49.27 53.43% 60%
Figure 6.Figure 6. Macronutrient content inMacronutrient content in I Isst t andand II IIndnd phase of diet therapy, phase of diet therapy,
expressed in percentage of total energy intake (kcal/d)expressed in percentage of total energy intake (kcal/d)
- - AHA/EAS AHA/EAS Recommendations -Recommendations -

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
METHODS METHODS FOR FOR PRESCRIPTION PRESCRIPTION OF OF PHYSICAL PHYSICAL ACTIVITYACTIVITY
1. The basic criterion for patient selection in four groups of physical
activity levels (PALs) was initial level of VO2max expressed in terms of
metabolic equivalents (METs).
2. MET was calculated by the equation: VO2max (ml-1kg-1min-1)/3.5
3. The method for modelling of programmed PA was established using
the classification for VO2max (WHO, 1974).
4. Training pulse (% HR max reserve) was calculated using equation by Karvonen.
5. Classification for intensity of PA i.e. physical work was expressed as
energy expenditure in terms of METs.
6. Using tables for gross energy expenditure of various PA with known energy
cost (METs) were chosen different type of PA in accordance with initial level
of VO2max (METs) (Poster for Physical Activity and Health).

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Training for sport Strenuous activity
Duration and frequency according to individual fitness level
Intensity of work: male >7.0 mets; female >6.3metsRelative intensity: HRmax 80-89%; >90 %
HRmax reserve 75-84% ; >85%
Exercise for fitness and increasing performancemoderate to vigorous activity
20 minutes or more, 3 times a week.Intensity of work: male 4.5 –7.0 mets; female 4.2 - 6.3 mets
Relative intensity: HRmax 68 – 79% ; HRmax reserve 60 - 74 %
Activity for healthmoderate activity
30 minutes or more, daily Intensity of work: male 3.0-4.5 mets; female 2.1-4.2 mets
Relative intensity: HRmax 60 – 67 %; HRmax reserve 50 – 59%
Active living Light to moderate activity
10 minutes or morea few times a day, daily Intensity of work: male < 3.0 mets ; female < 2.1 mets
Relative intensity: HRmax > 35% ; 35 – 59 %; HRmax reserve > 30% ; 30 – 49 %
HRmax (heart rate max)=220-yearsHR max reserve (training puls) =0.5 (220-years-morning heart rate)+ morning heart rate

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Figure 7Figure 7. . The effects of lifestyle changes: diets and physical activity The effects of lifestyle changes: diets and physical activity in reducing CVD risk at abdominal obese individualsin reducing CVD risk at abdominal obese individuals

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Results:Results:
The efficiency of prescribed PA and/or diet therapy on CVD risk reduction was examined in abdominal obese patients included in a 7 week randomized controlled trial.
Improved VO2max at 17.16% from baseline promoted significant greater reduction on the level of risk factors for CVD in FAD than those in D group of abdominal obese individuals:
- body weight (BW kg.)
- % body fat mass (%F)
- waist circumference (WC)
- waist/hip ratio (WHR)
- systolic blood pressure (TA-S)
- index of arteriosclerosis (LDL-C/HDL-C)
- fasting plasma glucose (GLY)
- HDL was increased at 10.41% from baseline
in FAD group.
3
3,38
2,17 2,15
3,12
2,17
0
0,5
1
1,5
2
2,5
3
3,5
4
LD
LL
-C/H
DL
-C
INICIAL FINALFAD group D group K group
p<0.001p>0.05MANOVA
2.15
3.123
3.38
0
0.5
1
1.5
2
2.5
3
3.5
4
I NI CI JALNO F I NALNOmerewa
LDL-C/HDL-c
GRUPA F AD GRUPA D
p0<0.000p1<0.01
DESCRIPTIVE CHARACTERISTICS ON LDLC/HDL-C INDEX
IN INICIAL AND FINAL PHASE AND DINAMICS OF CHANGES

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Recommendation:Recommendation:
Using our method for prescription and modelling of programmed physical activity and diets we achieved:
- significant greater reduction on CVD in physical activity and diet (FAD) group
than those in D (diet) group
- enlarged types of PA
- enabled safe performance
- avoiding the risk for CVD events during the individual and group exercises.
Broader application of the method for prescription and modelling of
programmed PA is proposed to the next individuals and groups with:
- low level of cardio respiratory fitness (VO2)
- increased/high risk for CVD, T2DM and other main NCD
- insulin resistance
- FAI% and
- sport recreation.

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
Tobacco Tobacco - - Free Free MacedoniaMacedonia Statistical analisys of data obtained from cross-sectional studies and State Institute for Statistics during the period 1986-2007 years includes: cancer mortality rate in total number of dead persons and number of smokers (active and passive) among adults, school children and youth.
The following results were estimated among adults: - Increased cancer mortality rate: 13.3% (1986), 15.9% (1994) and 18.1% (2001) - Increased number of smokers: 28.2% (1990), 35.2% (1998) and 42.7% (2000). The number of smokers among school children and youth (2000): 21% of total number of school children (14-18 years old) 31% of total number of students (18-24 years old) 17.7% of all smokers (15-64 years) were older adolescents (18-24).
On the bases of these results we suggest: 1. To adopt stronger law against smoking habits. It was implemented from 1-st of January 2010 in
Macedonia. 2. To implement smoke free law in the clubs, restaurants and other public and workplaces with aim to protect
workers and other persons from the dangers of passive smoking.
2006: International “Quit & Win” campaign - http://www.nosmoking.cjb.net 2010: World/National No Tobacco Day - http://www.quit-smoking-for-a-bettre-future.cjb.net
Source: Simovska V., Popovska I, Simovski A, Panovski N, Serdjuk V.: TOBACCO FREE MACEDONIA - AN INTRODUCTORY GUIDE: TO IMPLEMENT STRONGER TOBACCO FREE LAWS. The 13th World Conference on Tobacco OR Health: Building capacity for a tobacco-free world, Washington, DC, USA 2006. URL:http://www.users.cjb.net/nosmoking/5-ctobacco%20free%20macedonia.doc

Main principles of the North Karelia ProjectMain principles of the North Karelia Project Integrated approach, targeting main risk factors linked to certain behavioural/ lifestyles: diet, physical activity and tobacco.
Chosen risk factors for CVD: smoking, elevated serum cholesterol and elevated blood pressure.
Prevention calls for simple changes in some lifestyles (individual, family, community, national and global level action)
Influencing national diets and lifestyles is a key issue
Many results of prevention occur surprisingly quickly (CVD, diabetes) and also at relatively late age
Comprehensive action, broad collaboration with dedicated leadership and strong government policy support.
Ottawa declarationOttawa declaration
Personal Responsibility: ”Nobody can take better care of your health than yourself”Public Responsibility: ”Make the healthy choices the easy ones”

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
REDUCTION OF THE HIGH CORONARY HEART DISEASE MORTALITY REDUCTION OF THE HIGH CORONARY HEART DISEASE MORTALITY IN NORTH KARELIA, FINLANDIN NORTH KARELIA, FINLAND
Principal investigator: Prof. Puska Pekka, MD., PhD.
In 35 years the annual age-adjusted CHD mortality rate among the 35-64 years old male population in North Karelia declined by 85%. The North Karelia Project, community – based CVD prevention .

Wellness in the Workplace - I Work with Heart , World Heart Day 2010
FRAMEWORK FOR PHYSICAL ACTIVITY PROMOTION WITHIN A HEALTH POLICYFRAMEWORK FOR PHYSICAL ACTIVITY PROMOTION WITHIN A HEALTH POLICY
Source: Simovska V., Panovski N., Naumovski A., Tomic-Ckalevska D.: MACEDONIAN CINDI VISION FOR A CHRONIC DISEASE STRATEGY - POLITICAL AND PRACTICAL ACHIEVEMENTS, 2001-2005. European Conference on Chronic Disease Prevention“Learning from the past-planning for the future” 2005, Helsinki, The Book of Abstracts 2005:35. www.ktl.fi/attachments/suomi/julkaisut/julkaisusarja_b/.../2005b21.pdf