low- vs. high-glycemic load diet: effects on postprandial
TRANSCRIPT

Low-vs.high-glycemicloaddiet:effectsonpostprandialplasmafreefattyacidlevels
SarahYanez
Athesis
Submittedinpartialfulfillmentofthe
requirementsforthedegreeof
MasterofScience
UniversityofWashington
2016
Committee:
MichaelRosenfeld
MichelleAverill
ProgramAuthorizedtoofferdegree:
NutritionalSciences

©Copyright2016SarahYanez

UniversityofWashington
Abstract
Low-vs.high-glycemicloaddiet:effectsonpostprandialplasmafreefattyacids
SarahMichelleYanez
Co-chairsofthesupervisorycommittee:MichaelRosenfeld,PhDSchoolofPublicHealth
MichelleAverill,PhD
NutritionalSciencesProgramandDepartmentofEnvironmentalandOccupationalHealth
Introduction:Low-glycemicloaddietsarecommonlyprescribedforbloodglucosemanagement.Currently,however,itisnotclearastowhetherthediethasanyimplications,positiveornegative,oncardiovascularhealthinhealthyindividuals.Methods:UsingdatacollectedfromtheCarbohydratesandRelatedBiomarkers(CARB)Study,conductedattheFredHutchinsonCancerResearchCenter,weanalyzedtheeffectsofahigh-vs.low-glycemicloaddietonfastinglipidsandpostprandialplasmafreefattyacidlevelsinhealthy,non-insulinresistant,adults.Participantswererandomizedtocompleteeitherahigh-orlow-glycemicloaddietfor28days,followedbyawashoutperiodof28days,andthencompletetheoppositedietfor28days.Results:Wefoundthatahigh-vs.low-glycemicloaddietdidnothaveanysignificanteffectonplasmafreefattyacidlevelsintheeighthourtimeperiodfollowingatestbreakfast.Conclusions:Glycemicloaddoesnotappeartoaffectcardiovascularhealthintheshort-term,however,furtherresearchisneededtodetermineanylong-termimplications.Basedonourfindings,wecannotsupportarecommendationthatalow-GLdietisprotectiveagainstcardiovasculardiseaseinhealthyindividuals.

INTRODUCTIONANDBACKGROUND
GLYCEMICINDEXANDGLYCEMICLOAD
GLYCEMICINDEX
Theconceptofglycemicindex(GI)wasfirstintroducedasamethodtoclassify
carbohydrate-containingfoodsbytheirabilitytoraisebloodglucoselevels.29,62GIis
calculatedasthechangeinbloodglucoseafteracarbohydrate-containingfooditem
iseaten,dividedbythechangeinbloodglucoseafteranequalmassofbreadis
eaten,multipliedby100.6,30GIhasbeenstandardizedtobethecomparisonofthe2-
hourpost-prandialglucoseresponseof50gofacarbohydratefoodwiththatof50g
ofwhitebreadorglucose,andisrepresentedbytheareaundertheglucose
responsecurve.32,53Thus,GIisanindicatoroftheintestinalabsorptionof
carbohydrates;low-GIfoodsareabsorbedmoreslowlyandinduceaslower
glycemicresponsethanhigh-GIfoods,whicharerapidlyabsorbedinthe
intestines.10,23,32Whencarbohydrate-containingfoodsofdifferingGIaremixed
togetherinameal,theGIofthemealisarelativemedianoftheindividual
carbohydratefoodGIs.65
GLYCEMICLOAD
Glycemicload,aconceptrelatedtoGI,isarepresentationofboththequantityand
thequalityofcarbohydrateconsumed.GLiscalculatedastheproductofthefood’s
carbohydratecontentanditsGIvalue.39,64GLisawaytosummarizethecombined
effectsoftotalcarbohydrateintakeandoveralldietaryGI.38Alow-GLdietdoesnot
necessarilymeanthatlow-GIfoodswereconsumed.38SinceGLisdependentupon
boththeamountofcarbohydrateandtheGIofthefoodsconsumed,either
decreasedconsumptionoftotalcarbohydrateorimprovedqualityofcarbohydrate,
GI,canlowerGLofthediet.68Thus,thelong-termhealthimplicationsofareduced
GLdietmaybedifferentdependingonwhetherthelowerGLisduetoreduced
carbohydrateintake,reducedGI,oracombinationofthetwo.
BIOLOGICALRESPONSESTOGI/GL
Traditionally,lowGIfoodsorlowGLdietshavebeenrecommendedinthesettingof
glycemiccontrol,aslowGIfoodconsumptionisthoughttoresultinlowerandmore
stablebloodglucoseandinsulinlevels.16TotalmealGLhasbeenshownto,
moderatelywell,predictserumglucoseandinsulinresponsespostprandially.24A
positiveassociationbetweenmealGLlevelsandserumglucoseandinsulin
responseshasbeendemonstrated,indicatingthat,forfoodswithequalGIs,asthe
amountofcarbohydrateincreases,therewillbeaproportionallyconstantincrease
inthebloodglucoseandinsulinresponses.24
However,currentevidencesupportingalinkbetweendyslipidemiaandGLis
lacking.SomestudieshavefoundthatGLhasnoeffectonplasmalipidlevels,16,24,32,64
somehavefoundaninverserelationshipbetweenGLandcirculatingplasma
lipids,53,60andsomehavefoundimprovedlipidstatuswithlowGLdiets.13,39,40,56

INSULIN
EFFECTSOFGI/GL
Thereisepidemiologicalandclinicalevidencesupportingthatdietsignificantly
influencesinsulinsensitivityinobeseand/orinsulinresistantindividuals;23
specifically,thatalowGLdietincreasesinsulinsensitivity.15Otherpreviousstudies
havefoundsimilarresults,andfurtherconcludedthathighGLdiets,overtime,
contributeastateofpancreaticβ-celldysfunctionandadefectiveinsulin
response.10,60,68Adietwithahighcompositionofcarbohydratefoodsinduces
compensatoryhyperinsulinemia.64,72However,ifaheightenedinsulinresponseis
requiredoveranextendedperiodoftime,theabilityofβ-cellstoproduceand
secreteinsulindeclines.Chronicallyhighglucoseintake,pairedwithdecreasing
insulinsecretion,ultimatelyresultsinβ-celldeathandreducedpancreaticcellmass.
Thelong-termconsequenceisglucoseintoleranceanddiabetes.28TheFAO/WHO
hasmadearecommendation,basedonevidencesupportingtheefficacyofalowGI
orGLdietinimprovingglycemiccontrol,10toreducedietaryGIfortheprevention
andmanagementofmetabolicdisease.19However,somestudieshavenotfound
conclusiveevidencethatdifferencesinGIconsumptionleadtodifferencesininsulin
response.16,32IthasbeensuggestedthatGI/GLmaybemostusefulinitsabilityto
regulateglucoseresponsespostprandially,notnecessarilytheassociatedinsulin
response.16

INCRETINEFFECT
Theincretineffectisaphenomenoninwhichoralglucoseadministrationhasbeen
demonstratedtoelicitagreaterinsulinresponsethanintravenousglucose
administration.48Thishasrecentlybeenexplainedbytheactivityofinsulin-
mediatingmoleculessecretedbythegut.
Incretinsarepeptidehormonesthatareproducedentero-endocrinecellsinthe
smallintestinalmucosa.48Theincretinsglucose-independentinsulinotropic
polypeptide(GIP)andglucagon-likepeptide(GLP-1)aresecretedinresponseto
nutrientingestionandactonpancreaticβ-cellsforinsulinsecretion.2,28GIPand
GLP-1havelowbasalplasmaconcentrationsandhaveaninsulinsecretoryresponse
onlyatlevelsthatcorrelatetoacertainlevelofhyperglycemia;theyarethus
ineffectiveatelicitinganinsulinresponsewithlowamountsofdietaryglucose.48
Thisultimatelyservestomaintainacertainbloodglucoseleveldespiteingestionof
awiderangeofcarbohydrateloads.2Theinsulinresponsetothesehormones
accountsforapproximately70%ofpostprandialinsulinsecretion.28Thissuggests
thattheeffectofGIoninsulinresponsesisadditionaltotheeffectofincretins;the
postprandialinsulinresponseisnotentirelydependentupontheGIofthefood
consumed.
Theincretineffecthasbeendemonstratedtobedefectorcompletelyabsentin
individualswithimpairedglucosetolerance,hyperglycemia,anddiabetes.48Inone
study,plasmalevelsofincretinsdonotappeartodifferbetweenhealthyand

diabeticpersons,implyingthatadefectorabsenceoftheincretineffectisamarker
ofbetacelldysfunctionandthereducedsecretionofinsulin.2Thishypothesishas
beenconfirmedbyotherrecentinvestigations.28,49Oneofthesestudies,however,
hasalsoconcludedthatobesesubjectswithnormalglucosetolerancealsohavean
impairedincretineffect,likelyduetoreducedGLP-1secretioninthegut.28This
supportscurrentliteraturethatobesitycontributestoinsulinresistance,butwith
additionaldataregardingthemechanisms.
SHORT-TERMBIOLOGICALEFFECTS:SERUMFREEFATTYACIDS
Itiswellknownthatinsulinhasasignificanteffectontheactivitiesoflipasesthat
regulateFFAavailability:lipoproteinlipasefoundinadiposetissue,hormone-
sensitivelipase,andadiposetriglyceridelipase.60Inthepresenceofhighlevelsof
insulin,whenlipoproteinlipaseactivityisincreasedandhormone-sensitivelipase
andadiposetriglyceridelipaseactivitiesaresuppressed,thecombinedeffectis
improvedclearanceofFFAsfromthebloodstream.31
Lipoproteinlipasehydrolyzestriglyceridesfromcirculatinglipoproteins,either
chylomicronsfromtheintestinesorverylow-densitylipoproteins(VLDL)fromthe
liver.Thisresultsintheproductionoffattyacids.Inadiposetissue,insulinincreases
lipoproteinlipaseactivityandthusincreasestheproductionoffattyacids,whichare
eitheroxidizedforenergyorrepackagedastriglyceridesforstorage.26Conversely,
insulinasaninhibitoryeffectonthelipoproteinlipasefoundinskeletalmuscle,
servingtodirectfattyacidstoadiposetissueforstorage.Thehormoneglucagon,

releasedduringtimesoflowavailablebloodglucoseforenergy,isresponsiblefor
increasinglipoproteinlipaseactivityinmuscletissue.20Theresultistheincreased
abilityofmuscletissuetomobilizefattyacidsforenergyproductionwhenthe
preferredsubstrate,glucose,isunavailable.Theultimateeffectofincreased
lipoproteinlipaseactivityisfavorableuptakeofFFAsfromthecirculation.60
Hormone-sensitivelipaseandadiposetriglyceridelipasearefoundinadiposetissue
andbothservetohydrolyzestoredtriglyceridesintoFFAforreleaseintothe
circulation.35,72Whileitwasthoughtforquitesometimethathormone-sensitive
lipasewastheprimaryenzymeinthehydrolysisoftriglyceridesinadiposetissue,it
hasbeendiscoveredthatadiposetriglyceridelipaseisinfactthecatalystforthe
reactionandhasthemoresignificanteffectontheoverallrateoffattyacid
production.65Adiposetriglyceridelipaseishighlyexpressedinadiposetissueand
highlyspecificfortriglycerides.Itremovesthefirstfattyacidfromatriglyceride
molecule,initiatingitscatabolism.73Insulinsuppressestheactivitiesofthese
molecules,althoughthroughtwodifferentmechanisms.Adiposetriglyceridelipase
isregulatedbyinsulinatthetranscriptionallevel;highlevelsofinsulinreducethe
productionofthelipase.33Insulindoesnot,however,haltproductionofhormone-
sensitivelipase,itsimplydecreasesitslevelofactivity.63Increasedlevelsofinsulin
causethecombinedeffectsofhormone-sensitivelipaseandadiposetriglyceride
lipase:reductionoftriglyceridehydrolysisanddecreasedliberationofFFAintothe
circulation.

INSULINSIGNALINGANDLIPIDMETABOLISM
Figure1.Normallipidmetabolism(black)vs.lipidmetabolisminastateofinsulinresistance(red).Insulinhasinhibitory(-)andenhancing(+)effectsonmanystagesoflipidmetabolism.Insulinplaysanimportantroleinnutrientuptakeinthepostprandialperiod.
Dietarycarbohydratesareabsorbedintheintestinesandtransportedthroughthe
bloodstreamasglucose.Whileglucoseuptakebytheliverisindependentofinsulin
action,theconversionofglucosetofattyacidsisinsulin-dependent.Glucoseis
convertedtopyruvatethroughglycolysis,andthentoacetyl-coAthroughthe
insulin-stimulatedactionofpyruvatedehydrogenase.18Acetyl-coAisthenconverted
intofattyacids,inwhichtheenzymefattyacidsynthaseisupregulatedbyinsulin.
Fattyacidsaresubsequentlyesterifiedintotriglyceridesandpackagedintovery

low-densitylipoprotein(VLDL)fortransportthroughthecirculationsystem.18VLDL
iscarriedtoadiposetissuefordepositionoffattyacidsviatheinsulin-stimulated
actionoflipoproteinlipase(LPL).6ExtractionofthefattyacidsleavesaVLDL
remnant,whichthenbecomesanintermediate-densitylipoprotein(IDL).TheseIDL
moleculeslosetriglyceridesinthebloodstreamandformlow-densitylipoproteins
(LDL).44Therate-limitingstepofLDLsynthesisisindirectlyregulatedbyinsulin.3-
hydroxy-3-methylglutaryl-coAreductaseistheresponsibleenzymeandismost
activewhenbloodglucoselevelsarehigh.48Increasedinsulinclearanceofblood
glucosedecreasestheenzyme’sactivityandthuscholesterolproduction.
Dietaryfats,ontheotherhand,areemulsifiedintheintestinesforabsorption,and
thenpackagedintochylomicronsfortransportthroughthecirculationbeforebeing
depositedinadiposetissue.AgainthroughtheactionsofLPL,stimulatedbyinsulin,
triglyceridesareextractedfromthechylomicrons.6Inadiposetissue,deposited
triglyceridesarehydrolyzedintofreefattyacids,aprocessinhibitedbytheactionof
insulin.Additionally,thefattyacid-triglyceridecycleensuresconservationof
triglyceridestorageinadiposetissuethroughtheconsistentre-esterificationoffree
fattyacidstotriglycerides.6,69
Inastateofinsulinresistance,serumlipidlevelsarenegativelyaltered.HSLactivity
isincreasedinadipocytes,increasingtriglyceridehydrolysisandbuild-upoffree
fattyacids.6Thesearethentransportedtotheliver,wheretheincreasedavailability
offattyacidsfortriglyceridesynthesisincreasestheproductionandsecretionof

VLDL.WhenthethresholdforserumVLDLisreached,formationofHDLbytheliver
decreaseswhileformationofLDLincreases.Theendresultisdyslipidemia.69
FREEFATTYACIDS
RELATIONSHIPTOGI/GL
Asdemonstratedinthefigureabove,FFAsenterthecirculationthroughthe
hydrolysisofbothtriglyceridesinadiposetissueandglucoseintheliver.However,
highcirculatinglevelsofFFAshaveyettobedefinitivelylinkedtoadiethighin
carbohydratesorglycemicload.Thecurrentevidencedescribingarelationship
betweenGIorGLandFFAlevelsvarieswidely.Somestudiesdeterminingthat
plasmaFFAlevelswereincreasedbyalowGLdiet,13,35somehavefoundnoeffectof
GIorGLonFFAlevels,16,24andstillothershavefoundthatFFAconcentrationsare
suppressedbyhighGImeals.41,53
Asdiscussedpreviously,insulinactstobothincreaselipoproteinlipaseactivityfor
theuptakeofFFAtoadiposefromthecirculationanddecreasetheactivitiesof
hormone-sensitivelipaseandadiposetriglyceridelipaseforthereductionofFFA
liberationfromadiposetissueintothecirculation.Throughtheseactions,an
increasedinsulinresponseduetoahighglycemicloadmealcouldlikelymediatethe
FFAresponsesothatthereiseithernodifferenceinplasmalevelsorverylittle
differencepostprandially.56However,inthelatepostprandialperiod
(approximatelyfourtosixhoursafterthemeal),lowbloodglucoselevelstriggera
counter-regulatoryresponseandglucagonisreleased.Glucagonstimulates

gluconeogenicandglycogenolyticpathwaysinordertoproduceglucoseandrestore
normalbloodlevels,concurrentlyelevatingFFAlevels.41Inthisway,ahigh-GLmeal
mayactuallycauseFFAlevelstoriseversusthemoreattenuatedhormoneresponse
elicitedbyalow-GLmeal.Again,thisresultwouldonlybeseeninthelaterhours
afteratestmeal.
EFFECTSONCARDIOVASCULARHEALTH
ThereareseveralmechanismsbywhichhighFFAlevelsmightimpact
cardiovascularhealth.AnincreasedamountofFFAisavailabletotheliverfor
increasedtriglycerideproductionandVLDLsecretion.39,60,70Highserumtriglyceride
levelasbeendiscoveredtobeanindependentriskfactorforcoronaryheartdisease
(CHD),afteradjustmentforLDLandHDLcholesterollevels,age,bloodpressure,
smoking,diabetes,familyhistoryofmyocardialinfarction,andanginapectoris.1,12,42
Whileitisnotnecessarilythetriglycerideitselfthatleadstoheartdisease,high
levelsoftriglyceridesindicatehighlevelsofhighcholesterol-containingremnant
lipoproteinsthatthendepositthatcholesterolintoarterialwalls.51,75
HighlevelsofFFAsarealsobelievedtocontributetoinsulinresistance.55FFAlevels
surpassingstoragecapacityinadiposetissuearedepositedinothertissues,like
skeletalmuscleandliver,35,58throughtheinhibitionofinsulinsignaling.FFAs
completewithglucoseasanenergysubstrateinskeletalmuscle,alteringthe
partitioningoffatbetweenadipocytesandmuscle.58Theexactmechanismbywhich

FFAsaffectglucosetransportandutilizationhasyettobeclearlyidentified.8Insulin
resistanceitselfisassociatedwithhighratesofcholesterolsynthesis.54
Lastly,highlevelsofFFAsmaythemselvespredictcardiovascularmortality.55The
myocardiumappearstobenegativelyaffectedbyhighlevelsofFFAs,asincreased
useasametabolicsubstrateappearstohaveunfavorablealterationsatthecellular
level,resultingininefficientglucosemetabolism.47Thishasbeendemonstratedto
haveproarrhythmiceffects,increaseischemicdamage,andcontributetothe
developmentofheartfailure.27,52
GLYCEMICLOADANDCARDIOVASCULARHEALTH
CURRENTEVIDENCE
Asofyet,theliteratureisunabletodeterminewhateffects,ifany,glycemicloadhas
oncardiovascularhealth.Whilelow-GIdietsarefrequentlyrecommendedto
diabeticpatientswiththeintentofimprovingglycemiccontrolandinsulin
sensitivity,thereislittleevidencetosupportimprovementoflipidprofiles.Thereis
evenfewerdatatodescribetheeffectsofthisdietonnon-diabeticindividuals.9
SomestudieshavefoundthatGLhasnoeffectonplasmalipidlevels,13,24,32,64some
havefoundaninverserelationshipbetweenGLandcirculatingplasmalipids,50,57
andsomehavefoundimprovedlipidstatuswithlowGLdiets.13,40,42,62
Studyresultshavevariedbasedupongender,nationality,age,andBMI
classification.Inmiddle-agedandolderSwedish,dietaryGI/GLhadnosignificant

associationwithcardiovascularillness.67AnotherstudydoneinItalywith
overweight,oldermenandwomenfoundapositiveassociationbetweendietaryGI
andincidenceofmyocardialinfarction,butnoassociationbetweendietaryGI/GL
andincidenceofcardiovasculardiseaseoritsriskfactors.37Ameta-analysis
evaluatedstudiesoftheassociationsofGIandGLwithcoronaryheartdisease
eventsandfounddiscrepanciesbetweennationalitiesandsex;DanishandBlack
AmericanmendemonstratedpositivebenefitswithconsumptionoflowerGIfoods,
andoverallonlywomen,notmen,showedanincreaseinrelativeriskofcoronary
heartdiseasewiththeconsumptionofhighGIfoods/ahighGLdiet.66
However,therehavebeenstudiesshowingasignificantpositiveassociation
betweendietaryGLandtheriskofcardiovasculardisease.Variousstudieshave
shownthatlow-GIdietsresultinlowertriglycerideandlipoproteincholesterol
levels,aswellasalowerratiooftotalcholesteroltohigh-densitylipoproteinlevels,
indicatorsofcardiovascularhealth.41OneofthefirststudiesregardingGIindicated
thatitmighthaveabeneficialimpactonbloodlipids.30IncreaseddietaryGLwas
showntobeassociatedwithandincreaseinthecardiovasculardiseaseriskfactor
high-densitylipoprotein(HDL)inBrazilianmiddle-agedmen.16InUSwomen,GI
wasfoundtobeastrongindicatorofcoronaryheartdiseaserisk,independentof
carbohydratecomplexity.40
ACochranereviewassessingtheprescriptionoflowGIdietsforcardiovascular
healthdidnotfindanyevidencefromrandomizedcontrolledtrialstoshowaneffect

oflowGIdietsoncoronaryheartdisease.Someweakevidenceforminoreffectson
someCHDriskfactorswasfound;therewassomeevidenceofareductionintotal
cholesterolwithlowGIdietsandborderlinesupportforadecreaseinLDLwithlow
GIdiets.32Obesitywasidentifiedasaknownriskfactorforcoronaryheartdisease,
thereforeenergy-restricteddietsbasedonlowGIfoodsmightproducethegreatest
weightlossandthusthegreatestcardiovascularprotection.Thesedietsalsomay
improveinsulinsensitivityinobeseindividuals,therebyimprovingcholesterol
profiles.46
Thereisaneedforwell-designed,adequatelypowered,randomizedcontrolledtrials
ofsignificantdurationtobetterunderstandthefulleffectsofGIorGLonlipid
profilesandcardiovascularhealth.Currently,thereisinsufficientevidencethat
healthcareprovidersshouldrecommendalow-GLdietoverothertherapeuticdiets
forthepreventionofheartdiseaseinhealthy,non-insulinresistantindividuals

METHODS
STUDYPOPULATION
ParticipantsintheCarbohydratesandRelatedBiomarkers(CARB)study,conducted
attheFredHutchinsonCancerResearchCenter,(FHCRC)includedhealthy,non-
smokingmenandwomenbetweentheagesof18and45yearsoldfromtheSeattle
area.SpecialrecruitmenteffortsweregivenforAfricanAmericanandHispanic
populations.Priortoenrollment,potentialparticipantsweregivenaneligibility
questionnaire,excludingthosewho:(1)hadphysician-diagnoseddiseasesrequiring
dietaryrestrictionsormodifications;(2)hadaBMIbetween25and28,inorderto
demonstrateanysignificantdifferencesinoutcomesbetweenhealthyweightand
obeseindividuals;(3)werecurrentlypregnantorlactating,orhadplanstobecome
pregnant;(4)regularlytookhormones,anti-inflammatorymedications,orother
medicationsthatmightinterferewithoutcomemeasures;(5)usedtobaccoor
consumed>2drinksperday;(6)restrictedtheireatingorhadfoodallergies;and
(7)hadimpairedfastingglucose,definedasfastingbloodglucoselevels≥5.6
mmol/L.Enrolledparticipantswerealsoaskedtodiscontinuetheuseofanydietary
supplements.ApprovalwasobtainedfromtheInstitutionalReviewBoardandthe
ClinicalTrialsOfficeoftheFHCRCandallparticipantsprovidedwritten,informed
consent.50

RESEARCHDESIGN
89participantswereenrolledinthestudybetweenJune2006andJuly2009.
ParticipantswereblockrandomizedbytheBMIgroup(18.5-24.9kg/m2or28.0-
40.0kg/m2)andsextotheorderofexperimentaldiets.61Participantswereassigned
tobothalow-andhigh-GLdiet,inacross-overdesign,for28consecutivedayseach,
witha28daywashoutperiodinbetweendietsduringwhichparticipantsconsumed
theirhabitualdiets(Figure2).62AsubsetofCARBstudyparticipantswaschosento
participateinapostprandialstudy(CARB-PPL).Thisincluded20participantswho
consumedastandardizedtestbreakfastandremainedatthefacilityforpost-
prandialtesting.61ItistheCARB-PPLsamplesthatwereusedinthisanalysis.
Participantswereinstructedtoconsumeonlythefoodandbeveragesprovided
duringthefeedingperiods;coffeeandtea(creamersandsweetenerswereprovided
bythestudy)werepermittedatstablecontinuouslevels.61Participantsateonemeal
eachday,MondaythroughFriday,attheHumanNutritionLabatFHCRCunder
supervisionbystudystaff.Aftertheeveningmeal,participantswereprovidedwith
breakfast,lunch,andsnackforthefollowingday.Followingtheeveningmealon
Friday,participantswereprovidedwithallfoodtobeconsumedovertheweekend
aswellasMonday’sbreakfastandlunch.Allfoodthatremainedunconsumedwas
returnedtothelabwherestaffweighedandrecordedit.Participantsalsocompleted
adailychecklistconfirmingconsumptionoftheday’sfoods,alongwithconsumption
ofnon-studyfoods.60

STUDYDIETS
Bothhigh-andlow-GLdietsweredesignedtobeweight-maintaining.3-daydiet
recordswereobtainedfromparticipantsinordertoestimatehabitualenergy
intake.ThisdatawasusedinconjunctionwiththeMifflinequationtoestimate
energyneeds.50A7-daymenurotationforeachdietwasgeneratedusingProNutra
(Version3.2,Viocare).Macronutrientcontentwasidenticalbetweeneachdiet,with
15%ofdailyenergycomingfromprotein,30%ofdailyenergycomingfromfat,and
55%ofdailyenergycomingfromcarbohydrates.Fibercontentdifferedbetweenthe
twodietswith55g/dayinthelowGLdietversus28g/dayinthehighGLdiet.The
lowGLdietwasdefinedatGL125,andhighwas250.61Participantweightswere
takenthreetimesperweekandenergyadjustmentsweremadein200kcal
incrementsasnecessarytomaintainbaselineweight.62Thetestbreakfastsforthe
postprandialstudywerealsodesignedtobesimilartothe28-daydietsinoverall
macronutrientcontentandmatchtheGLprofileofthediettreatment.61
Figure2.Cross-overdesignofstudydiets.

SAMPLECOLLECTIONANDANALYSIS
Samplecollectionsweredoneinthemorningsofthefirstandlastdaysofthediet
periods.50Ondayonea12-hourfastingblooddrawwastakenandonday28,from
the20postprandialstudyparticipants,apostprandialblooddrawwascollected
followingbreakfast,at0,30,60,120,180,240,270,300,330,360,420,and480
minutesafterthestartofthemeal(Figure3).Afterbeingallowedtoclotfor
approximately30-45minutes,bothserumandplasmawerespunandaliquoted.
Sampleswereimmediatelystoredat-20°C,andplacedforstorageina-80°Cfreezer
bytheendoftheday.ThesamplesprovidedbytheCARB-PPLstudyforthislipid
analysishadnotbeenpreviouslythawed.Plasmasampleswereanalyzedatthe
UniversityofWashington’sNutritionObesityResearchCenteranalyticalcoreand
lipidpanelsweregenerated.
FFAsweremeasuredonaRocheCobasMiraPlusChemistryAnalyzerusingreagent
fromGenzyme/Wako.Afterbeingallowedtothawforapproximately30minutes,
sampleswereanalyzedatroomtemperature.
Figure3.Timesofpostprandialblooddraws.

STATISTICALANALYSIS
Theoverallgoalofthisstudywastotesttheeffectsofa28-daylow-vs.high-GLdiet
interventiononthepostprandialresponsesofserumlipids,specificallyfreefatty
acids.Wecalculatedareaunderthecurve(AUC)ofpost-prandialFFA
measurementsusingtrapezoidalapproximation.In30and60minutetimeperiods,
accordingtowhenblooddrawsweretaken,wecalculatedtheAUCforthe
postprandialperiodsafterbreakfastandafterlunch.WerepeatedtheAUCanalysis
separatelyforeachthenormalweightandoverweight/obesegroupsforthetotal
timeperiod,beforelunch,andafterlunch.Apairedt-testwasdoneforeachofthe
AUCanalysesinordertodetermineifasignificantp-valueexistedbetweenthediet
sets.
Fastinglipidpanelsdrawnonthe28thdayofeachdietperiodwereanalyzedusinga
2-waypairedANOVA.

RESULTS
Table1.Characteristicsofstudyparticipantsn=20 Agerange(y) 19-44Male/Female(n) 10,10BMI(n) 18.5-24.9kg/m2
("Normal"weightgroup)10
28-40kg/m2
("Overweight/obese"weightgroup)10
Ethnicity(self-reported) Non-Hispanicwhite 8Hispanic 7AfricanAmerican 4Asian/PacificIslander/NativeAmerican 1
Blockrandomizationoftheparticipantsensuredthattheparticipantgroupwas
composedofequalpartsmalesandfemalesandnormalweightand
overweight/obeseweightgroups.Therewerefivewomenandfivemencomprising
boththenormalandoverweight/obeseweightgroups.Onaverage,the
overweight/obeseweightgroupwasslightlyolderthanthenormalweightgroup(P
<0.001).Ethnicitydidnotvaryacrossweightgroups.Baseduponself-reporteddata
fromthedailyfoodcheck-offformsandreturnedfood,itappearedthat97%of
participantsconsumedmorethan90%oftheprovidedfoods.Nosignificant
differenceinadherencebystudydietwasdetermined.

Table2.Meanenergyandmacronutrientcontentof2400kcalhigh-andlow-GLreferencedietsa
High-GLdietn=7days
Low-GLdietn=7days
Dietarydescriptor mean±SD mean±SDEnergy(kcal/day)b 2398±8 2396±6Protein(g/day) 90±1 90±0Energyfromprotein(%usingtotalcarb) 15±0.2* 14±0.4*Energyfromprotein(%usingavailablecarb)c 15±0.2 16±0.2Fat(g/day) 80±0 81±1Energyfromfat(using%totalcarb) 30±0.3* 29±0.8*Energyfromfat(using%availablecarb) 31±0.2 31±0.6Totalcarbohydrate(g/day) 341±6* 361±15*Energyfromtotalcarbohydrate(%) 56±0.5* 57±1.1*Energyfromavailablecarbohydrate(%) 54±0.8 53±0.8Dietaryfiber(g/day) 24±5* 49±8*GI/day 78±5* 34±1*GL/day 244±14* 117±3*
aDatafromProNutra:MetabolicDietStudyManagementSystem(ViocareTechnologies)and/ortheNutritionDataSystemforResearch(version2005,NutritionCoordinatingCenter,UniversityofMinnesota)bTotalenergycalculatedassumsof4kcal/gprotein,9kcal/gfat,and4kcal/gtotalcarbohydrate.cTotalenergycalculatedusingavailablecarbohydrate.Asterisk(*)nexttoP-value,0.05forpairedt-testscomparinghigh-andlow-GLdiets.
Table2showstheplanneddailymeanmacronutrientcontent,dietaryGI,dietaryGL,
anddistributionofenergyforbothhigh-andlow-GL2400-kcalreferencediets.All
dietsateachenergylevelweresimilartothereferencedietshown.Fibercontent
washigherinthelow-GLdiet.Increasedfiberintakehasbeenshowntoreducetotal
cholesterolandapoBlevelsrelativetoHDL-cholesterolandApoA1levels,thus
reducingtheriskofcoronaryheartdisease.(29)Thepercentavailablecarbohydrate
doesnotfactorthefibercontentintoenergycalculations,asfiberisonlyavailable
forenergyafterfermentation.AvailablecarbohydrateisrecommendedbytheFAO
asausefulconceptforenergyevaluation.Necessaryenergyadjustmentsforweight

maintenancethroughoutthestudydidnotsignificantlydifferbydiettypeorfeeding
period.Thetestbreakfastconsumedforpostprandialanalysiswasconstructedtobe
composedofmacronutrientratiosconsistentwiththestudydiets.
Table3.Endofdietperiodfastinglipidpanelresults(n=20)
High-GL Low-GL
mg/dL Mean±SD Mean±SDCholesterol 142±29 140±33Triglyceride 84±51 93±73HDL 41±10 40±9LDL 85±23 81±24ApoA1 130±21 130±20ApoB 73±19 73±21Fastingbloodsamplesfrom20participantsweredrawnonday28ofeachdiet
period,beforeconsumptionofthetestbreakfast.TherewasnoeffectofGLon
fastingtotalcholesterol,HDLcholesterol,LDLcholesterol,ApoA1,andApoBlevels.
Table4.Totalparticipant(n=20)areaunderthecurve,plasmafreefattyacids BeforeLunch
mEq/LAfterlunchmEq/L
TotalTimemEq/L
High-GL 1.00±0.28 1.34±0.41 2.33±0.54Low-GL 1.02±0.36 1.48±0.52* 2.53±0.79
The“beforelunch”timeperiodisdefinedastimepoints0:00through4:00,andthe
“afterlunch”timeperiodastimepoints4:00through8:00.
Atspecifictimeperiods,thehigh-vs.low-GLdietdidnothaveanysignificanteffect
onplasmaFFAlevels.

Figure1.Mean±SDFFAlevels(mEq/L)oftheCARB-PPLparticipantsatthetimeofeachblooddraw.Betweenthehigh-GL(solidblueline)andthelow-GL(solidredline)diets,thereisnotasignificancedifferenceincirculatingFFAlevelsacrosstheeighthourtimeperiod.
00.10.20.30.40.50.60.70.80.91
0:00 0:30 1:00 2:00 3:00 4:00 4:30 5:00 5:30 6:00 7:00 8:00
mEq/L
TimeofBloodDraw
Figure4.EffectsofHigh-vs.Low-GLDietonPlasmaFreeFattyAcidAverage:Total
TimePeriod
High-GL Low-GL
Lunch
Breakfast

Figure2.Mean±SDFFAlevels(mEq/L)oftheCARB-PPLparticipantsatthetimeofeachblooddrawinthetimeperiodbeforealunchmealisconsumed(0:00to4:00).TrapezoidalapproximationsdidnotdeterminesignificanceinthedifferencebetweenFFAlevelsforthetwostudydiets,high-GL(solidblueline)andlow-GL(solidredline).
00.10.20.30.40.50.60.70.80.91
0:00 0:30 1:00 2:00 3:00 4:00
mEq/L
TimeofBloodDraw
Figure5.EffectsofHigh-vs.Low-GLDietonPlasmaFreeFattyAcidAverage:Pre-
LunchTimePeriod
Low-GL High-GL
LunchBreakfast

Figure3.Mean±SDFFAlevels(mEq/L)oftheCARB-PPLparticipantsatthetimeofeachblooddrawinthetimeperiodafteralunchmealisconsumed(4:00to8:00).TrapezoidalapproximationsdidnotidentifysignificanceinthedifferencebetweenFFAlevelsforthetwostudydiets,high-GL(solidblueline)andlow-GL(solidredline)atanyoftheindividualtimepoints.
00.10.20.30.40.50.60.70.80.91
4:00 4:30 5:00 5:30 6:00 7:00 8:00
mEq/L
TimeofBloodDraw
Figure6.EffectsofHigh-vs.Low-GLDietonPlasmaFreeFattyAcidAverage:Post-
LunchTimePeriod
Low-GL High-GL
Lunch

Table5.Areaunderthecurve,FFA:normalvs.overweight/obeseparticipants
n=10 Pre-Lunch(mEq/L)
Post-Lunch(mEq/L)
TotalTimePeriod(mEq/L)
NormalWeightBMI18.5-24.9kg/m2
High-GL 1.31±0.28 2.29±0.92 3.57±1.0Low-GL 1.25±0.37 2.26±1.00 3.51±1.30Overweight/ObeseBMI25-40kg/m2
High-GL 1.40±0.50 1.98±0.50 3.38±0.78Low-GL 1.45±0.57 2.34±0.72 3.29±1.18
WeanalyzedtheFFAresponseofthetwoweightgroups,normaland
overweight/obese,forthetwostudydietsseparatelybecauseofthepotential
impactthatadiposebiologymayhaveonFFAclearance.TherewasnoeffectofGL
onpostprandialFFAlevelsbetweenthetwoweightgroups.

0
0.2
0.4
0.6
0.8
1
0:00 0:30 1:00 2:00 3:00 4:00 4:30 5:00 5:30 6:00 7:00 8:00
mEq/L
TimeofBloodDraw
Figure7.EffectsofHigh-vs.Low-GLDietonPlasmaFreeFattyAcidAverage,Normalvs.Overweight/ObeseWeight
Groups:TotalTimePeriod
Low-GL,Normalweight Low-GL,Overweight/Obese
High-GL,Normalweight High-GL,Overweight/Obese
Lunch
Breakfast
Figure4.Mean±SDFFAlevels(mEq/L)oftheCARB-PPLparticipantsatthetimeofeachblooddrawintheeight-hourperiodfollowingthetestbreakfast.
DISCUSSIONThisrandomized,cross-over,controlledfeedingstudytestedtheeffectofhigh-GLvs.
low-GLexperimentaldietsonpost-prandialplasmaFFAlevels.Theresultsofour
analysisshowedthatahigh-vs.low-GLdietdidnothaveanysignificanteffecton
fastinglipidsorpost-prandialplasmaFFAlevelsintheeighthoursfollowingatest
breakfastmeal.However,thereisacomplexrelationshipbetweendietary
carbohydratesandbloodlipidlevels.WhileGLdoesnotappeartoaffectbloodlipid
levels,andbyextensioncardiovascularhealth,intheshort-term,furtherresearchis
neededtodetermineanylong-termimplications.Thecurrentstateofresearchdoes
notsupporttherecommendationofalow-GLdietforcardiovasculardisease
preventionovertherecommendationofother,proventherapeuticdiets.
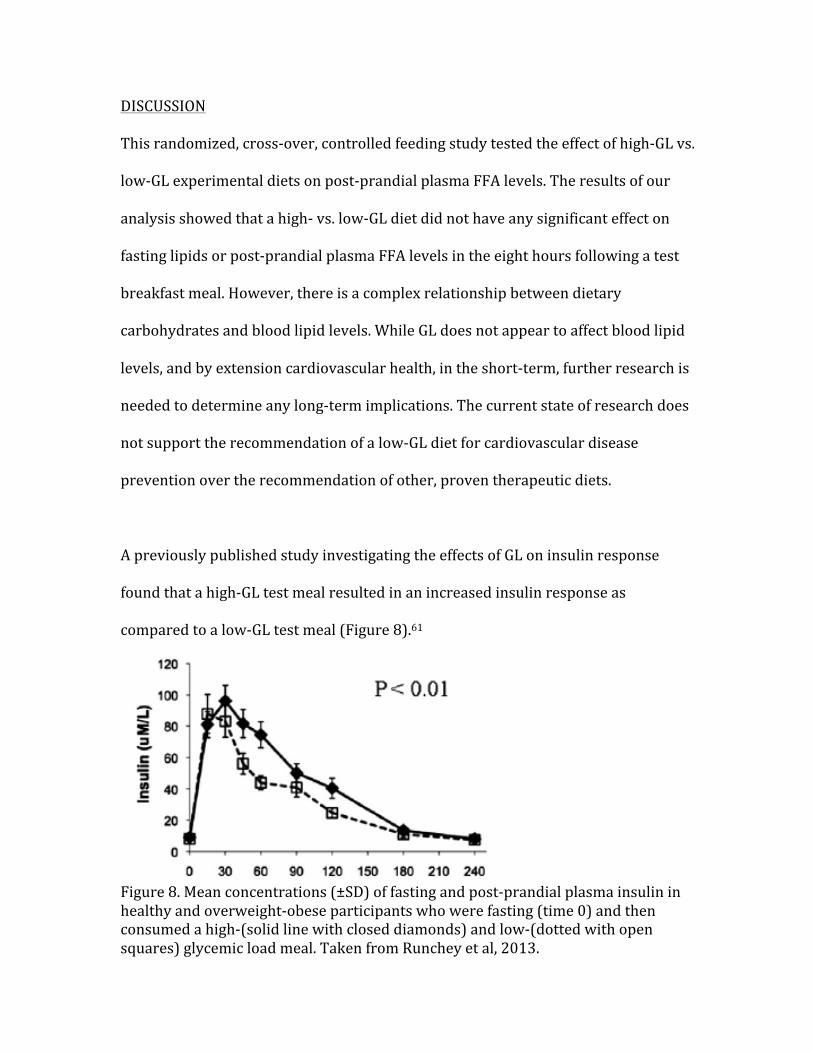
ApreviouslypublishedstudyinvestigatingtheeffectsofGLoninsulinresponse
foundthatahigh-GLtestmealresultedinanincreasedinsulinresponseas
comparedtoalow-GLtestmeal(Figure8).61
Figure8.Meanconcentrations(±SD)offastingandpost-prandialplasmainsulininhealthyandoverweight-obeseparticipantswhowerefasting(time0)andthenconsumedahigh-(solidlinewithcloseddiamonds)andlow-(dottedwithopensquares)glycemicloadmeal.TakenfromRuncheyetal,2013.

ItcouldbeexpectedthatahigherinsulinresponsewouldmediatetheFFAresponse;
theFFAresponsetoahigh-GLmealwouldthusbethesameorlowerthanthattoa
low-GLmeal.FFAuptakefromthecirculationintoadiposetissueisinsulin-
dependentthroughtheactionoflipoproteinlipase.25ThestorageofFFAinadipose
tissueastriglyceridesisalsoinsulin-dependentthroughtheactionsofhormone-
sensitivelipaseandadiposetriglyceridelipase.35,72However,whiletheactionof
insulinonhormone-sensitivelipaseisimmediate,itsactiononthemorecrucial
enzyme,adiposetriglyceridelipase,istranscriptive.33Thus,thetrueeffectsof
insulinonplasmaFFAlevelswouldnotbevisibleintheearlypostprandialperiod.
Thefourhourpostprandialtimeperiodmonitoredintheinsulinstudyisinadequate
inindetermininganycarryovereffectofGLoninsulin,alsomakingitimpossibleto
comparetheobservedpost-lunchplasmaFFAlevelsofthisstudytoaninsulin
response.
WealsoexploredthepossibledifferenceinFFAresponsebetweenthenormal
weightandoverweight/obesegroups.WedidnotfindthatGLhadadifferenteffect
onpostprandialplasmaFFAlevelsbetweenthetwoweightgroups.Wecanthen
postulatethatadiposityalonedoesnothaveaneffectonplasmaFFAlevels.The
participantsofthisstudywerenotinsulinresistant,thereforetheirinsulinresponse
wasthesameastheirnormalweightcounterparts.Theinsulinstudysimilarlydid
notobserveeffectsofadiposityoninsulinresponse.59

STRENGTHSANDLIMITATIONS
Thisstudywasacrossoverdesignwithtwo28-daycontrolleddietinterventions
differingsubstantiallyinGL.Itwasalsouniqueinthatthedietswereindividualized
toberealistic,isocaloric,andweigh-maintainingdespitebeinghigh-orlow-GL.
Therewereseveralsignificantlimitationstothisstudy.Therewasasmallsample
sizeforthepostprandialarmofthestudy;thesamplesizewasevensmallerwhen
participantsweredividedbyweightgroup.Participantswerealsosampledfroma
populationgroupthatmetveryspecificenrollmentcriteria.Allparticipantswere
healthyandinsulin-responsive,withnormalglycemiccontrol.Thiswasnota
population-basedparticipantgroup,thusresultsarelikelynotgeneralizable.
Becausevolunteerswithinsulinresistancewerenotincludedinthisstudy,wewere
unabletoexploretheeffectsofGLonbloodlipidsinthoseindividuals.Therewasno
differenceinpancreaticfunctionbetweenourweightgroups,andthereforeno
expected,orobserved,differenceininsulinresponse.Ourparticipantswerealso
limitedtothenormalandveryoverweightorobese.Beingoverweightisthoughtto
beprotectiveagainstmanychronicdiseasesandtheirriskfactors,yetwewere
unabletoexploredifferencesinFFAresponseamongtheseindividualscomparedto
theotherweightgroups.
Thedietlengthof28daysonlyallowedustointerprettheshort-termeffectsofGL
onpostprandialFFAlevels.Insulinresistancedevelopingduetoachronicallyhigh
carbohydrateintakeandstressonthepancreaticβ-cellsisnotdiscernableinafour-

weekspan.AstudyoflongerdurationwouldbeneededtodetermineifGLdirectly
contributestothedevelopmentofinsulinresistance,contributingindirectlyto
unfavorablelipidprofilesandthedevelopmentofcardiovasculardisease.
FUTUREDIRECTIONS
Thereisaneedforarandomizedcontrolledtrialofdurationlongerthan12weeks
todeterminetheeffectsofGLonbloodlipids,specificallyplasmaFFAlevels,andthe
riskofcardiovasculardisease.Thereiscurrentlylittle,ifany,evidencetosupport
thatalow-GLdietcouldbeprotectiveagainstthedevelopmentofcardiovascular
disease.
StudiesexploringtheeffectsofGLonbloodlipidprofilesbetweenindividualswith
insulinresistancearenecessarytodeterminehearthealthimplications.Wecould
thenmoreappropriatelydeterminewhetheralow-GLdietisbeneficialtoboth
insulinresistantandhealthindividuals,oronlytheformer.Wewouldalsobeable
toexploretheeffectsofGLversusanothertherapeuticdietthatperhapsprovides
protectivebenefitsinclusiveofbutnotlimitedtoGL.
CLINICALIMPLICATIONS
Basedonthisstudyandthecurrentstateoftheliterature,itcannotbe
recommendedthathealthcareproviderscounselalow-GLdietforthepreventionof
cardiovasculardiseaseinahealthypatientpopulationoverotherproven
therapeuticdiets.ThisstudydoesnotsupportarecommendationfortheuseofGL

inpreventingcardiovasculardiseaseinhealthyindividualsasneitherlow-norhigh-
GLdietswereshowntobeprotectiveagainstcoronaryheartdiseaseinregardsto
FFA.

REFERENCES
1. AssmannG,PCullen,andHSchulte.TheMunsterHeartStudy(PROCAM)–
resultsoffollow-upat8years.EurHeartJ.1998;19:A2-A11.
2. AulingerBA,TPVahl,RLPrigeon,DAD’Alessio,andDAElder.Theincretineffectinobeseadolescentswithandwithouttype2diabetes:impairedorintact?AmJPhysiol.2016;310(9):E774-E781.
3. BarclayAW,PPetocz,JMcMillan-Price,VMFlood,TPrvan,PMitchell,andJC
Brand-Miller.Glycemicindex,glycemicload,andchronicdiseaserisk–ameta-analysisofobservationalstudies.AmJClinNutr.2008;87(3):627-637.
4. BehallKM,DJScholfield,IYuhaniak,andJCanary.Dietscontaininghigh
amylosevs.amylopectinstarch:effectsonmetabolicvariablesinhumansubjects.AmJClinNutr.1989;49:337-44.
5. BeulensJWJ,LMdeBruijne,RPStolk,PHMPeeters,MLBots,DEGrobbee,and
YTvanderSchouw.Highdietaryglycemicloadandglycemicindexincreaseriskofcardiovasculardiseaseamongmiddle-agedwomen:apopulation-basedfollow-upstudy.JAmCollegeCario.2007;50(1):14-21.
6. BickertonAST,RRoberts,BAFielding,LHodson,EEBlaak,AJM
Wagenmakers,MGilbert,FKarpeandKNFrayn.Preferentialuptakeofdietaryfattyacidsinadiposetissueandmuscleinthepostprandialperiod.Diabetes.2007;56(1):168-176.
7. BjörntorpP.“Portal”adiposetissueasageneratorofriskfactorsfor
cardiovasculardiseaseanddiabetes.ArteriosclerThrombVascBiol.1990;10:493-496.
8. BodenGandGIShulman.Freefattyacidsinobesityandtype2diabetes:
definingtheirroleinthedevelopmentofinsulinresistanceandbeta-celldysfunction.EuroJClinInvestigation.2002;32(s3):14-23.
9. BouchéC,SWRizkalla,JLuo,HVidal,AVeronese,NPacher,CFouquet,V
Lang,andGSlama.Five-week,low-GIdietdecreasestotalfatmassandimprovesplasmalipidprofileinmoderatelyoverweight,non-diabeticmen.DiabetesCare.2002;25(5):822-828.
10. BrounsF,BjorckI,FraynKN,GibbsAL,LangV,SlamaG,andWoleverTMS.
Glycaemicindexmethodology.NutrResRev.2005;18(1):145-171..

11. BurgerKNJ,JWJBeulens,JMABoer,AMWSpijkerman,andDLvanderA.Dietaryglycemicloadandglycemicindexandriskofcoronaryhearddiseaseandstrokeindutchmenandwomen:theEPIC-MORGENstudy.PLOSOne.2011;6(10):e25955
12. CastelliWP.Epidemiologyoftriglycerides–aviewfromFramingham.AmJ
Cardiol.1992;70:H3-H9.
13. Castro-QuezadaI,Sanchez-VillegasA,EstruchR,Sala-SalvadoJ,CorellaD,SchroderH,Alvarez-PerezJ,Ruiz-LopezMD,ArtachoR,RosE,BulloM,CovasMI,Ruiz-GutierrezV,Ruiz-CanelaM,Buil-CosialesP,Gomez-GraciaE,LapetraJ,PintoX,ArosF,FiolM,Lamuela-RAventosRM,Martinez-GonzalezMA,Serra-MajemL,onbehalfofthePREDIMEDStudyInvestigators.AhighdietaryglycemicindexincreasestotalmortalityinaMediterraneanpopulationathighcardiovascularrisk.PLOSONE.2014;9(9).
14. ChaneyS.Overviewoflipidmetabolism.Lecture,UNCMedicalSchool.20
September2005.
15. ClappJF,LopezB.Low-versushigh-glycemicindexdietsinwomen:effectsoncaloricrequirement,substrateutilization,andinsulinsensitivity.MetabolicSyndromeandRelatedDisorders.2007;5(3):231-241.
16. CocatePG,PereiraLG,JCBMarins,PRCecon,JBressan,andRCGAlfenas.
Metabolicresponsestohighglycemicindexandlowglycemicindexmeals:acontrolledcrossoverclinicaltrial.NutrJ.2011;10:1.
17. CullenP.Evidencethattriglyceridesareanindependentcoronaryheart
diseaseriskfactor.AmJCardiol.2000;86(9):943-949.
18. DimitriadisG,PMitrou,VLambadiari,EMaratou,andSARaptis.Insulineffectsinmuscleandadiposetissue.DiabetesResearchandClinicalPractice.2011;93:S52-S59.
19. FAO.Carbohydratesinhumannutrition.ReportofaJointFAO/WHOExpert
Consultation(FAOFoodandNutritionPaper66).FoodandAgricultureOrganization:Rome.1998.
20. FareseJrRV,TJYost,andRHEckel.Tissue-specificregulationoflipoprotein
lipaseactivitybyinsulin/glucoseinnormal-weighthumans.Metabolism.1991;40(2):214-216.
21. FlemingPandMGodwin.Low-glycaemicindexdietsinthemanagementof
bloodlipids:asystematicreviewandmeta-analysis.FamilyPractice.2013;30:485-491.

22. FraynKN.Adiposetissueandtheinsulinresistancesyndrome.Proceedingsofthenutritionsociety.2001;60(3):375-380.
23. FrostG,LeedsAA,DoreCJ,MadeirosS,BradingS,andDornhorstA.
GlycaemicindexasadeterminantofserumHDL-cholesterolconcentration.Lancet.1999;353(9158):1045-1048.
24. GalganiJ,AguirreC,DiazE.Acuteeffectofmealglycemicindexandglycemic
loadonbloodglucoseandinsulinresponsesinhumans.Nutritionjournal.2006;5:22.
25. GoldbergIJ,RHEckel,andNAAbumrad.Regulationoffattyaciduptakeinto
tissues:lipoproteinlipase-andCD36-mediatedpathways.JLipidRes.2009;50:S86-S90.
26. GoldbergIJ.Lipoproteinlipaseandlipolysis:centralrolesinlipoprotein
metabolismandatherogenesis.JLipidRes.1996;37:693-707.
27. HendricksonSC,JDLouis,JELowe,andSAbdel-aleem.Freefattyacidmetabolismduringmyocardialischemiaandreperfusion.MolCellBiochem.1997;166:85-94.
28. JoãoAL,FReis,andRFernandex.TheincretinsystemABCsinobesityand
diabetes:noveltherapeuticstrategiesforweightlossandbeyond.ObesityReviews.2016;17(7):553-572.
29. JenkinsDJ,WoleverTM,KalmuskyJ,GiudiciS,GiordanoC,WongGS,BirdJN,
PattenR,HallM,BuckleyG.LowglycemicindexcarbohydratefoodsinthemanagementAmericanJournalofClinicalNutrition.1985;42:604-617.
30. JenkinsDJ,WoleverTM,TaylorRH,BarkerH,FieldenH,BaldwinJM,Bowling
AC,NewmanHC,JenkinsAL,GoffDV.Glycemicindexoffoods:Aphysiologicalbasisforcarbohydrateexchange.TheAmericanJournalofClinicalNutrition.1981;34:362-366.
31. JohnsI,LGoff,LJBluck,BAGriffin,SAJebb,JALovegrove,TASanders,G
Frost,andADornhorst.Plasmafreefattyacidsdonotprovidethelinkbetweenobesityandinsulinresistanceorbeta-cellhysfunction:resultsoftheReading,Imperial,Surrey,Cambridge,Kings(RISCK)study.DiabetMed.2014;31(11):1310-1315.
32. KellySAM,FrostG,WhittakerV,andSummerbellCD.Lowglycaemicindex
dietsforcoronaryheartdisease.CochraneDatabaseSystRev.2004;18(4):CD004467.

33. KershawEE,JKHamm,LAWVerhagen,OPeroni,MKatic,andJSFlier.Adiposetriglyceridelipase.Diabetes.2006;55(1):148-157.
34. KiensB,HLithell,KJMikines,andEARichter.Effectsofinsulinandexercise
onmusclelipoproteinlipaseactivityinmananditsrelationtoinsulinaction.JClinInvest.1989;84(4):1124-1129.
35. KiensBandEARichter.Typesofcarbohydrateinanordinarydietaffect
insulinactionandmusclesubstratesinhumans.AmJClinNutr.1996;63(1):47-53.
36. KoutsariCandMDJensen.Thematicreviewseries:patient-oriented
research:freefattyacidmetabolisminhumanobesity.JLipRes.2006;47:1643-1650.
37. LevitanEB,MAMittleman,andAWolk.Dietaryglycemicindex,dietary
glycemicloadandmortalityamongmenwithestablishedcardiovasculardisease.EurJClinNutr.2009;63(4):439.
38. LiH,LiuH,ChenJ,LiL,WansH,LiJ,andWangL.Relationshipbetween
glycemicloadandbloodlipidlevelinhospitalizedadultchinese.IranJPublicHealth.2015;44(30):318-324.
39. LiuS,MansonJE,MeirMJ,HolmesMD,HuFB,HankinsonSE,andWilletWC.
Dietaryglycemicloadassessedbyfood-frequencyquestionnaireinrelationtoplasmahigh-density-lipoproteincholesterolandfastingplasmatriacylglycerolsinpostmenopausalwomen.AmJClinNutr.2001;73(3):560-566.
40. LiuS,WilletWC,StampferMJ,HuFB,FranzM,SampsonL,HennekensCH,
andMansonJE.Aprospectivestudyofdietaryglycemicload,carbohydrateintake,andriskofcoronaryheartdiseaseinUSwomen.AmJClinNutr.2000;71(6):1455-1461.
41. LudwigDS.Theglycemicindex:physiologicalmechanismsrelatingto
obesity,diabetes,andcardiovasculardisease.JAMA.2002;287(18):2414-2423.
42. ManninenV,LTenkanen,PKoskinen,JKHuttunen,MMänttäri,OPHeinonen,
andMHFrick.JointeffectsofserumtriglycerideandLDLcholesterolandHDLcholesterolconcentrationsoncoronaryheartdiseaseriskintheHelsinkiHeartStudy.Circulation.1992;85:37-45.
43. ManzellaD,MBarbieri,MRRizzo,ERagno,NPassariello,AGambardella,R
Marfella,DGiugliano,andGPaolisso.Roleoffreefattyacidsoncardiac

autonomicnervoussysteminnoninsulin-dependentdiabeticpatients:effectsofmetaboliccontrol.JCinEndocrinolMetab.2001;86:2768-2774.
44. Martin-SanzP,JEVance,andDNBrindley.Stimulationofapoliprotein
secretioninvery-low-densityandhigh-densitylipoproteinsfromculturedrathepatocytesbydexamethasone.BiochemJ.1990;271:575-583.
45. MeadJR,SAIrvine,andDPRamji.Lipoproteinlipase:structure,function,
regulation,androleindisease.JMolMed.2002;80(12):753-769.
46. MirrahimiA,RJdeSouza,LChiavaroli,JLSievenpiper,JBeyene,AJHanley,LSAugustin,CWKendall,andDJJenkins.Associationsofglycemicindexandloadwithcoronaryheartdiseaseevents:asystematicreviewandmeta-analysisofprospectivecohorts.JAmHeartAssoc.2012;1(5):e000752.
47. MurrayAJ,REAnderson,GCWatson,GKRaddda,andKClarke.Uncoupling
proteinsinhumanheart.Lancet.2004;364:1786-1788.
48. NessGCandCMChambers.Feedbackandhormonalregulationorhepatic3-hydroxy-3-methylglutarylcoenzymeAreductase:theconceptofcholesterolbufferingcapacity.ProceedingsoftheSocietyforExperimentalBiologyandMedicine.2000;224(1):8-19.
49. NauckMAandJJMeier.Theincretineffectinhealthyindividualsandthose
withtype2diabetes:physiology,pathophysiology,andresponsetotherapeuticinterventions.LancetDiabetesandEndocrinology.2016;4(6):525-536.
50. NeuhouserML,YSchwarz,CWang,KBreymeyer,GCoronado,CYWant,K
Noar,XSong,andJWLampe.Alow-glycemicloaddietreducesserumc-reactiveproteinandmodestlyincreasesadiponectininoverweightandobeseadults.JNutr.2012;142(2):369-374.
51. NordestgaardBG,MBenn,PSchnohr,andATybærg-Hansen.Nonfasting
triglyceridesandriskofmyocardialinfarction,ischemicheartdisease,anddeathinmenandwomen.JAMA.2007;298(3):299-308.
52. OliverMFandLHOpie.Effectsofglucoseandfattyacidsonmyocardial
ischemiaandarrhythmias.Lancet.1994;343;155-158.
53. OppermanAM,VenterCS,OosthuizenW,ThompsonRL,andVorsterHH.Meta-analysisofthehealtheffectsofusingtheglycaemicindexinmeal-planning.Br.J.Nutr.2004;92:367–381.

54. PihlajamäkiJ,HGylling,TAMiettinen,andMLaakso.Insulinresistnaceisassociatedwithincreasedcholesterolsynthesisanddecreasedcholesterolabsorptioninnormoglycemicmen.JLipidRes.2004;45:507-512.
55. PilzS,JScharnagl,BTiran,USEelhorst,BWellnitz,BOBoehm,JRSchaefer,
andWMarz.Freefattyacidsareindependentlyassociatedwithall-causeandcardiovascularmortalityinsubjectswithcoronaryheartdisease.JClinEndocrinolMetab.2006;91(7).
56. RadulianG,ERusu,ADragomir,andMPosea.Metaboliceffectsoflow
glycemicindexdiets.NutrJ.2009;8(5).
57. ReshefL,RWHanson,andFJBallard.Apossiblephysiologicalroleforglyceroneogeneisinratadiposetissue.JBiolChem.1970;245(22):5970-5984.
58. ReshefL,YOlswang,HCassuto,BBlum,CMCroniger,SCKalhan,SMTilghman,andRWHanson.Glyceroneogenesisandthetriglyceride/fattyacidcycle.JBiolChem.2003;278:30413-30416.
59. RizkallaSW,TaghridL,LaromiguiereM,HuetD,BoillotJ,RigoirA,ElgrablyF,
SlamaG.Improvedplasmaglucosecontrol,whole-bodyglucoseutilization,andlipidprofileonalow-glycemicindexdietintype2diabeticmen:Arandomizedcontrolledtrial.DiabetesCare.2004;27:1866-1872.
60. RobertsonMD,HendersonRA,VistGE,RumseyRD.Extendedeffectsof
eveningmealcarbohydrate-to-fatratioonfastingandpostprandialsubstratemetabolism.AmJClinNutr.2002;75:505-510.
61. RuncheySS,PollakMN,ValstaLM,CoronadoGD,SchwarzY,BreymeyerKL,
WangC,WangCY,LampeJW,NeuhouserML.Glycemicloadeffectonfastingandpost-prandialserumglucose,insulin,igf-1andigfbp-3inarandomized,controlledfeedingstudy.Europeanjournalofclinicalnutrition.2012;66:1146-1152.
62. RuncheySS,LMValsta,YSchwarz,CWang,XSong,JWLampe,andML
Neuhouser.Effectoflow-andhigh-glycemicloadoncirculatingincretinsinarandomizedclinicaltrial.Metabolism.2013;62(2):188-195.
63. SaltielARandCRKahn.Insulinsignalingandtheregulationofglucoseand
lipidmetabolism.Nature.2001;414(6865):799-806.
64. ShikanyJM,TinkerLF,NeuhouserML,MaY,PattersonRE,PhillipsLS,LiuS,andReddenDT.Associationofglycemicloadwithcardiovasculardiseaseriskfactors:theWomen’sHealthInitiativeObservationalStudy.Nutr.2010;26(6):641-647.

65. SchweigerM,RSchreiber,GHaemmerle,ALass,CFledelius,PJacobsen,H
Tornqvist,RZechner,andRZimmermann.Adiposetriglyceridelipaseandhormone-sensitivelipasearethemajorenzymesinadiposetissuetriacylglycerolcatabolism.JBiolChem.2006;281:40236-40241.
66. ThomasDE,EJElliott,andLBaur.Lowglycemicindexorlowglycemicload
dietsforoverweightandobesity.CochraneDatabaseSyst.Rev.2007;18(3):CD0055105.
67. VanDamRM,AWVisscher,EJFeskens,PVerhoef,andDKromhout.Dietary
glycemicindexinrelationtometabolicriskfactorsandincidenceofcoronaryheartdisease:theZutphenElderlyStudy.EurJClinNutr.2000;54(9):726-731.
68. VanSchothorstEM,BunshotenA,SchrauwnP,MensinkRP,andKeijerJ.
Effectsofahigh-fat,low-versushigh-glycemicindexdiet:retardationofinsulinresistanceinvolvesadiposetissuemodulation.FASEBJ.2009;23(4):1092-1101.
69. WilcoxG.Insulinandinsulinresistance.ClinBiochemRev.2005;26(2):19-
39.
70. WoleverTMandJenkinsDJ.Theuseoftheglycemicindexinpredictingthebloodglucoseresponsetomixedmeals.AmJClinNutr.1986;43:167-172.
71. WoleverTMSandMehlingC.Long-termeffectofvaryingthesourceor
amountofdietarycarbohydrateonpostprandialplasmaglucose,insulin,triacylglycerol,andfreefattyacidconcentrationsinsubjectswithimpairedglucosetolerance.AmJClinNutr.2003;77(3):612-621.
72. ZhangZ,LanzaE,Kris-EthertonPM,ColburnNH,BagshawD,RovineMJ,
UlbrechtJS,BobeG,ChapkinRS,HartmanTJ.Ahighlegumelowglycemicindexdietimprovesserumlipidprofilesinmen.Lipids.2010;45(9):765-775.
73. ZimmermannR,JGStrauss,GHaemmerle,GShoiswohl,RBirner-
Gruenberger,MRiederer,ALass,GNeuberger,FEisenhaber,AHermetter,andRZechner.Fatmobilizationinadiposetissueispromotedbyadiposetriglyceridelipase.Science.2004;306(5700):1383-1386.
