management of ocular and orbital complications in … · and we found mucosal thickening with ......
TRANSCRIPT
Central Annals of Otolaryngology and Rhinology
Cite this article: Fadda G, Cerutti M, Crosetti E, Succo G (2016) Management of Ocular and Orbital Complications in Acute Rhinosinusitis and Skull Base Diseases. Ann Otolaryngol Rhinol 3(7): 1117.
*Corresponding author
Gianluca Fadda, ENT Department, San Luigi Gonzaga University Hospital, Regione Gonzole 10, Orbassano, 10043 Turin, Italy, Tel: 39-11-90-26-463; Fax: 39-11-90-26-583; Email:
Submitted: 02 May 2016
Accepted: 30 May 2016
Published: 31 May 2016
ISSN: 2379-948X
Copyright© 2016 Fadda et al.
OPEN ACCESS
Keywords•Acute Rhinosinusitis•Orbital cellulitis•Endoscopic sinus surgery•Ptosis•Third nerve palsy•Nasopharyngeal masses
Case Report
Management of Ocular and Orbital Complications in Acute Rhinosinusitis and Skull Base DiseasesGianluca Fadda1*, Marta Cerutti1, Erika Crosetti2, and Giovanni Succo1
1ENT Department, San Luigi Gonzaga University Hospital, Italy2I.R.C.C.S. Candiolo, Turin, Italy
Abstract
Orbital extension of acute rhinosinusitis represents a medical and surgical emergency. Radiological investigation with computed tomography (CT) and magnetic resonance imaging (MRI) is essential to distinguish different diagnosis and to evaluate the extent of disease. Endoscopic sinus surgery (ESS) is indicated any time acute sinusitis with complications is observed to reduce compression of adjacent structures, to restore sinus drainage, for bacteriological or mycotic examinations, and to provide a final histopathological examination. The clinical presentation of orbital complications of two rare cases of acute rhinosinusitis and one case of nasopharyngeal carcinoma is described in this paper and the therapeutic approaches are discussed.
ABBREVIATIONSMR: Magnetic Resonance; CT: Computed Tomography; MG:
Myasthenia Gravis; ESS: Endoscopic Sinus Surgery; WBC: White Blood Cell; CRP: C-Reactive Protein; ANA: Antinuclear Antibodies; ENA: Extractable Nuclear Antigen; TSH: Thyroid-Stimulating Hormone
INTRODUCTIONOcular and orbital symptoms (unilateral ptosis, limitation
of ocular movements, diplopia, orbital cellulitis and cranial nerve palsy) can be an expression of a variety of non-neoplastic and neoplastic diseases in the nasal cavity, paranasal sinuses and nasopharynx. Myopathies, myasthenia, viral and bacterial infection, vascular diseases, contact lens wear, head injuries, autoimmune diseases, Horner’s syndrome, infraorbital rim fracture or space occupying lesions have to be suspected in these cases [1].
We report the clinical cases of three patients, evaluated in March 2016 in the emergency ENT Department of San Luigi Gonzaga Hospital in Orbassano – Turin - Italy. They all had ocular and orbital symptoms as complications of acute rhinosinusitis and skull base diseases. Clinical presentation, radiographic findings, histopathologic evaluation, and medical and surgical management are reviewed.
CASE PRESENTATIONS
Case 1
A 29-year-old man complained of progressive left periocular pain and pressure with diplopia, unilateral proptosis, purulent rhinorrhea and fever for 7 days. Acute sinusitis and nasal obstruction were not mentioned in the patient history, but two maxillofacial traumas had occurred 3 years earlier with resulting subcutaneous emphysema of the left orbit at Valsalva maneuver.
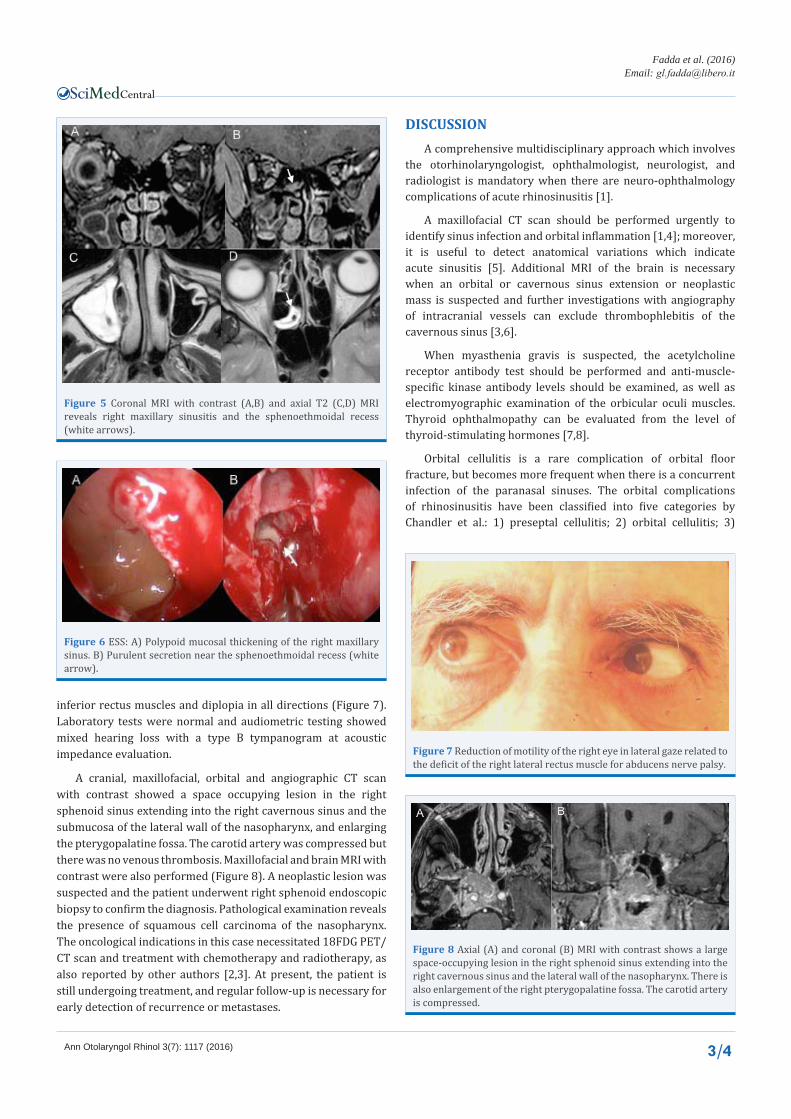
At clinical examination, we observed left proptosis with normal visual acuity and pupillary light reflex. Nasal endoscopy showed the presence of a purulent secretion in the left middle meatus (Figure 1). An increase in white blood cell (WBC) count (12.8 x 1000/µl) and C-reactive protein (CRP) (11.61 mg/L) was reported in laboratory tests. On the maxillofacial CT scan, we found soft tissue swelling with left proptosis, and involvement of the left maxillary sinus with an extended connection between the orbital floor and maxillary sinus. Furthermore, air inside the orbit compressed and relocated the inferior rectus muscle (Figure 2). Left orbital cellulitis without an orbital abscess as a result of facial trauma and maxillary sinusitis was suspected.
The patient was admitted to the ENT department and was administered intravenous antibiotic therapy including amoxicillin–clavulanate (2.2 g BID), ceftriaxone (2 g BID), methylprednisolone (40 mg BID) and pantoprazole (40 mg). On
Central
Fadda et al. (2016)Email:
Ann Otolaryngol Rhinol 3(7): 1117 (2016) 2/4
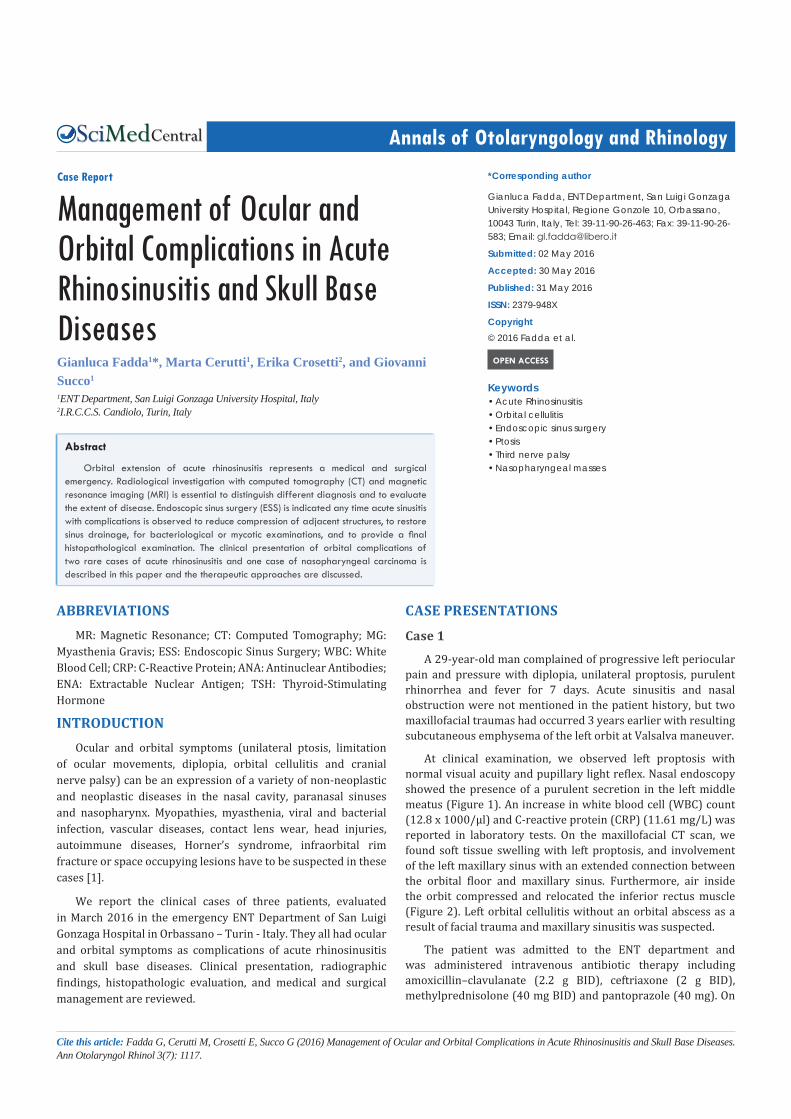
the same day, he underwent left endoscopic sinus surgery (ESS) and we found mucosal thickening with purulent secretion in the left maxillary; the maxillary roof was dehiscent with a connection with the inferior rectus muscle (Figure 3). At histological examination, a purulent inflammatory lesion was reported.
The patient was discharged 3 days after the ESS and 2 months after initial presentation, he was asymptomatic without proptosis, diplopia or orbital pain. MRI confirmed herniation of the adipose tissue and inferior rectus muscle in the maxillary sinus.
Case 2
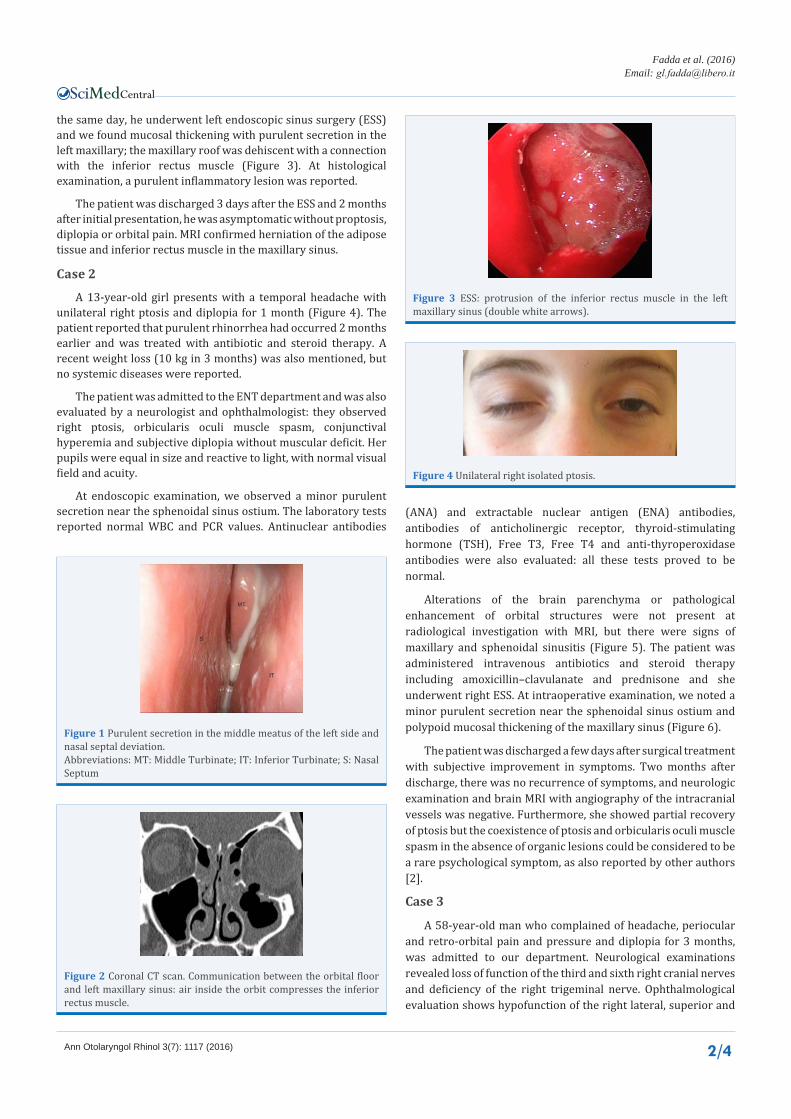
A 13-year-old girl presents with a temporal headache with unilateral right ptosis and diplopia for 1 month (Figure 4). The patient reported that purulent rhinorrhea had occurred 2 months earlier and was treated with antibiotic and steroid therapy. A recent weight loss (10 kg in 3 months) was also mentioned, but no systemic diseases were reported.
The patient was admitted to the ENT department and was also evaluated by a neurologist and ophthalmologist: they observed right ptosis, orbicularis oculi muscle spasm, conjunctival hyperemia and subjective diplopia without muscular deficit. Her pupils were equal in size and reactive to light, with normal visual field and acuity.
At endoscopic examination, we observed a minor purulent secretion near the sphenoidal sinus ostium. The laboratory tests reported normal WBC and PCR values. Antinuclear antibodies
(ANA) and extractable nuclear antigen (ENA) antibodies, antibodies of anticholinergic receptor, thyroid-stimulating hormone (TSH), Free T3, Free T4 and anti-thyroperoxidase antibodies were also evaluated: all these tests proved to be normal.
Alterations of the brain parenchyma or pathological enhancement of orbital structures were not present at radiological investigation with MRI, but there were signs of maxillary and sphenoidal sinusitis (Figure 5). The patient was administered intravenous antibiotics and steroid therapy including amoxicillin–clavulanate and prednisone and she underwent right ESS. At intraoperative examination, we noted a minor purulent secretion near the sphenoidal sinus ostium and polypoid mucosal thickening of the maxillary sinus (Figure 6).
The patient was discharged a few days after surgical treatment with subjective improvement in symptoms. Two months after discharge, there was no recurrence of symptoms, and neurologic examination and brain MRI with angiography of the intracranial vessels was negative. Furthermore, she showed partial recovery of ptosis but the coexistence of ptosis and orbicularis oculi muscle spasm in the absence of organic lesions could be considered to be a rare psychological symptom, as also reported by other authors [2].
Case 3
A 58-year-old man who complained of headache, periocular and retro-orbital pain and pressure and diplopia for 3 months, was admitted to our department. Neurological examinations revealed loss of function of the third and sixth right cranial nerves and deficiency of the right trigeminal nerve. Ophthalmological evaluation shows hypofunction of the right lateral, superior and
Figure 1 Purulent secretion in the middle meatus of the left side and nasal septal deviation. Abbreviations: MT: Middle Turbinate; IT: Inferior Turbinate; S: Nasal Septum
Figure 2 Coronal CT scan. Communication between the orbital floor and left maxillary sinus: air inside the orbit compresses the inferior rectus muscle.
Figure 3 ESS: protrusion of the inferior rectus muscle in the left maxillary sinus (double white arrows).
Figure 4 Unilateral right isolated ptosis.
Central
Fadda et al. (2016)Email:
Ann Otolaryngol Rhinol 3(7): 1117 (2016) 3/4
inferior rectus muscles and diplopia in all directions (Figure 7). Laboratory tests were normal and audiometric testing showed mixed hearing loss with a type B tympanogram at acoustic impedance evaluation.
A cranial, maxillofacial, orbital and angiographic CT scan with contrast showed a space occupying lesion in the right sphenoid sinus extending into the right cavernous sinus and the submucosa of the lateral wall of the nasopharynx, and enlarging the pterygopalatine fossa. The carotid artery was compressed but there was no venous thrombosis. Maxillofacial and brain MRI with contrast were also performed (Figure 8). A neoplastic lesion was suspected and the patient underwent right sphenoid endoscopic biopsy to confirm the diagnosis. Pathological examination reveals the presence of squamous cell carcinoma of the nasopharynx. The oncological indications in this case necessitated 18FDG PET/CT scan and treatment with chemotherapy and radiotherapy, as also reported by other authors [2,3]. At present, the patient is still undergoing treatment, and regular follow-up is necessary for early detection of recurrence or metastases.
DISCUSSIONA comprehensive multidisciplinary approach which involves
the otorhinolaryngologist, ophthalmologist, neurologist, and radiologist is mandatory when there are neuro-ophthalmology complications of acute rhinosinusitis [1].
A maxillofacial CT scan should be performed urgently to identify sinus infection and orbital inflammation [1,4]; moreover, it is useful to detect anatomical variations which indicate acute sinusitis [5]. Additional MRI of the brain is necessary when an orbital or cavernous sinus extension or neoplastic mass is suspected and further investigations with angiography of intracranial vessels can exclude thrombophlebitis of the cavernous sinus [3,6].
When myasthenia gravis is suspected, the acetylcholine receptor antibody test should be performed and anti-muscle-specific kinase antibody levels should be examined, as well as electromyographic examination of the orbicular oculi muscles. Thyroid ophthalmopathy can be evaluated from the level of thyroid-stimulating hormones [7,8].
Orbital cellulitis is a rare complication of orbital floor fracture, but becomes more frequent when there is a concurrent infection of the paranasal sinuses. The orbital complications of rhinosinusitis have been classified into five categories by Chandler et al.: 1) preseptal cellulitis; 2) orbital cellulitis; 3)
Figure 5 Coronal MRI with contrast (A,B) and axial T2 (C,D) MRI reveals right maxillary sinusitis and the sphenoethmoidal recess (white arrows).
Figure 6 ESS: A) Polypoid mucosal thickening of the right maxillary sinus. B) Purulent secretion near the sphenoethmoidal recess (white arrow).
Figure 7 Reduction of motility of the right eye in lateral gaze related to the deficit of the right lateral rectus muscle for abducens nerve palsy.
Figure 8 Axial (A) and coronal (B) MRI with contrast shows a large space-occupying lesion in the right sphenoid sinus extending into the right cavernous sinus and the lateral wall of the nasopharynx. There is also enlargement of the right pterygopalatine fossa. The carotid artery is compressed.

Central
Fadda et al. (2016)Email:
Ann Otolaryngol Rhinol 3(7): 1117 (2016) 4/4
Fadda G, Cerutti M, Crosetti E, Succo G (2016) Management of Ocular and Orbital Complications in Acute Rhinosinusitis and Skull Base Diseases. Ann Otolar-yngol Rhinol 3(7): 1117.
Cite this article
subperiosteal abscess; 4) orbital abscess; and 5) cavernous sinus thrombosis [9].
There is a high risk of cavernous sinus thrombosis, meningitis, or cerebral abscess if the patient is not promptly and adequately treated with medical and surgical therapies [10,11]. Fracture repair, if indicated, should be delayed, particularly if an alloplastic implant is used [10].
ESS is indicated any time we observe acute sinusitis with complications. The indications for ESS have been rapidly expanding since its introduction into sinus surgery. ESS has become an ideal method to manage certain orbital diseases and has the advantages of excellent visualization with minimal cosmetic and functional morbidity [12]. This procedure is needed to reduce compression of adjacent structures, to restore sinus drainage, to perform bacteriological or mycotic examinations, and also to provide a final histopathological examination [13]. In both cases 1 and 2, the results of purulent secretion culture were negative.
Specific antibiotic therapy is still being debated by several authors, whereas there is agreement about corticosteroid therapy: it is administered to reduce intracranial or intraorbital edema or when optic nerve damage is suspected [14,15]. An infectologist consultation is necessary to assess important alterations of inflammation values, or positive cultural examinations.
In conclusion, correct diagnosis, adequate antibiotic therapy, and surgical drainage are the keys to a good prognosis for ocular and orbital complications in acute rhinosinusitis and skull base disease. Delay in diagnosis can result in serious sequelae such as blindness, cavernous sinus thrombosis, meningitis, cerebral abscess, and death [16]. Postoperative management is an important procedure to control visual disturbances that frequently have a slow recovery.
REFERENCES1. Kastner J, Taudy M, Lisy J, Grabec P, Betka J. Orbital and intracranial
complications after acute rhinosinusitis. Rhinology. 2010; 48: 457-461.
2. Peer Mohamed BA, Patil SG. Psychogenic unilateral pseudoptosis. Pediatr Neurol. 2009; 41: 364-366.
3. Chahed H, Bachraoui R, Kedous S, Ghorbel H, Houcine A, Mediouni A, et al. Management of ocular and orbital complications in acute sinusitis. J Fr Ophtalmol. 2014; 37: 702-706.
4. Younis RT, Anand VK, Davidson B. The role of computed tomography and magnetic resonance imaging in patients with sinusitis with complications. Laryngoscope. 2002; 112: 224-229.
5. Fadda GL, Rosso S, Aversa S, Petrelli A, Ondolo C, Succo G. Multiparametric statistical correlations between paranasal sinus anatomic variations and chronic rhinosinusitis. Acta Otorhinolaryngol Ital. 2012; 32: 244–251.
6. Fadda GL, Gisolo M, Crosetti E, Fulcheri A, Succo G. Intracranial complication of rhinosinusitis from actinomycosis of the paranasal sinuses: a rare case of abducens nerve palsy. Case Rep Otolaryngol. 2014; 2014: 601671.
7. Piccirillo G, Trojsi F, Conforti R, Tedeschi G. Isolated unilateral ptosis due to neurovascular conflict. Neurol Sci. 2016; 37: 637-639.
8. Kiessling WR, Pflughaupt KW, Ricker K, Haubitz I, Mertens HG. Thyroid function and circulating antithyroid antibodies in myasthenia gravis. Neurology. 1981; 31: 771-774.
9. Dankbaar JW, van Bemmel AJ, Pameijer FA. Imaging findings of the orbital and intracranial complications of acute bacterial rhinosinusitis. Insights Imaging. 2015; 6: 509-518.
10. Ben Simon GJ, Bush S, Selva D, McNab AA. Orbital cellulitis: a rare complication after orbital blowout fracture. Ophthalmology. 2005; 112: 2030-2034.
11. Howe L, Jones NS. Guidelines for the management of periorbital cellulitis/abscess. Clin Otolaryngol Allied Sci. 2004; 29: 725-728.
12. Liang KL, Su MC, Shiao JY, Hsin CH, Jiang RS. Endoscopic sinus surgery for the management of orbital diseases. ORL J Otorhinolaryngol Relat Spec. 2008; 70: 134-140.
13. Mortimore S, Wormald PJ. Management of acute complicated sinusitis: a 5-year review. Otolaryngol Head Neck Surg. 1999; 121: 639-642.
14. Barry B, Ameline E, Thuong M, Brunel F, Pichelin C, Géhanno P. Orbital complications of sinusitis in adults. Ann Otolaryngol Chir Cervicofac. 2000; 117: 19-25.
15. Lee L, Huang C, Lee T. Prolonged visual disturbance secondary to isolated sphenoid sinus disease. Laryngoscope. 2004; 114: 986–990.
16. Sakamoto H, Karakida K, Otsuru M, Arai M, Shimoda M. A case of brain abscess extended from deep fascial space infection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108: 21–25.