management of pain and sublingual hematoma caused by ... · management of pain and sublingual...
TRANSCRIPT

CLINICAL REPORT
Program DireMeriden, Con
360
Management of pain and sublingual hematoma caused bysuture irritation after implant surgery: A clinical report
Avinash S. Bidra, BDS, MS
ABSTRACTHematoma in the sublingual region is an adverse consequence of implant surgery in themandibular posterior region. Improved knowledge and understanding of the anatomy as well asthe use of advanced radiographic imaging have all contributed to minimizing adverse surgicalcomplications in this region. Delayed sublingual hematoma caused by suture irritation after implantsurgery has not previously been reported. This article describes the management of a patient with adelayed sublingual hematoma after implant surgery in the posterior mandible had been performed.No evidence of encroachment of the vascular structures was noted at the time of implant surgery.However, at a 48-hour follow-up, the patient presented with severe pain and irritation of thesublingual mucosa, along with extravasation and a collection of blood in the sublingual region.Based on the patient’s symptoms and clinical signs, the source of the problem was determined tobe the stiff tags of polypropylene suture, which had been used to attain primary closure of thesurgical flaps. The situation was conservatively and successfully managed by the use of a customsoft tissue guard to protect the patient’s sublingual mucosa and the tongue from the stiff suturetags. Various suture materials and measures for preventing and managing similar situations arediscussed in this article. (J Prosthet Dent 2015;113:360-365)
Implant surgery in the outpa-tient setting as in a dentaloffice is generally considereda relatively safe procedure withminimal surgical complica-tions. Fortunately, the rateof surgical complications inimplant dentistry is lower thanthe overall rate of prostho-dontic complications.1,2 Onenoteworthy surgical complica-tion is intraoperative andpostoperative hemorrhage andits consequences. Implantplacement in the anterior orposterior mandible requires a
careful understanding of anatomy to avoid the sur-rounding vasculature and the clinical skills to manageany adverse events.3The submental artery and sublingual artery are the2 significant anatomic structures that are criticallyimportant for implant placement in the mandible. Thesubmental artery is a terminal branch of the facialartery, which originates from the external carotid ar-tery. It passes deeply into the digastric and stylohyoidmuscles and loops forward on the inferior border ofthe mandible to travel a deep groove in the sub-mandibular salivary gland.3-5 Thereafter, the sub-mental artery courses anteriorly on the surface of themylohyoid muscle and anastomoses with the mylo-hyoid branch of the inferior alveolar artery and thesublingual branch of the lingual artery.6 These ter-minal anastomosing branches may penetrate the
ctor and Maxillofacial Prosthodontist, Post-Graduate Prosthodontics, Univen.
lingual cortex of the anterior mandible by means ofthe lingual foramen or may enter through the acces-sory lingual foramina.7,8
The sublingual artery provides the majority of theblood supply to the floor of the mouth. Branches from thisartery perfuse the sublingual salivary gland, the mylohyoidand surrounding muscles, and the gingiva and mucosa ofthe mandibular anterior teeth.5,6 The sublingual artery is aterminal branch of the lingual artery, which arises from theexternal carotid artery between the facial artery and thesuperior thyroid artery. The sublingual artery travelsdeeply into the posterior belly of the digastric muscle,hypoglossal nerve, and the stylohyoid muscle. The sub-lingual branch originates at the anterior border of thehyoglossus muscle and travels forward in the anterior floorof the mouth above the mylohyoid muscle to anastomosewith the contralateral artery and with the submental
rsity of Connecticut Health Center, Farmington, Conn; Private practice,
THE JOURNAL OF PROSTHETIC DENTISTRY

May 2015 361
branch of the facial artery. These terminal branches mayresult in small alveolar branches that penetrate the lingualcortex of the mandible.4
Depending upon the amount of resorption of themandible, the ridge crest may approximate closer to thevasculature. Iatrogenic perforation of the lingual cortexcan result in damage to these arteries by the implant drilland result in massive hemorrhage. The hemorrhage canresult in the extravasation of the blood, swelling of thetongue, elevation of the floor of the mouth, and subse-quent airway compromise. Another risk with uncon-trolled bleeding is the risk of syncope and hypovolemicshock. Numerous clinical reports have described adversesurgical events related to hemorrhage and subsequenthematoma in the floor of the mouth. Dubois et al9 havesummarized more than 15 case reports with massivehemorrhage after implant placement in the mandible andhave reported that life-threatening hemorrhage afterimplant surgery mostly occurred during implant place-ment in the mandibular canine region. Almost all thesecase reports reported on hemorrhage during implantplacement due to perforation of the lingual cortex orwithin 4 to 6 hours postoperatively. In intraoperativehematomas, management of the situation mandates animmediate bimanual compression at the suspected site ofperforation and immediate transportation of the patientto the nearest hospital to secure the airway.9 In post-operative hematomas, a patient’s phone call complainingof profuse hemorrhage, protruding tongue, or respiratorydistress should alert the clinician to a possible hematoma,and the same measures should be taken as in theintraoperative situations.9 Recognizing that not all post-operative hematomas result in airway compromise orresult in life threatening situations is important.
A variety of suture materials, needles, and techniquesare available for use in implant dentistry.10 Insufficientreliable evidence is available to provide recommendationsas to which are the best incision techniques, suture tech-niques, or suture materials.11 In general, nonresorbablesutures shouldbeusedwhen tension-freeprimary closure isnecessary. The advantage of a nonresorbable suture is itspersistent strength during the contracture of thewoundandits resistant muscle pull during the remodeling of the softtissues. Typically, they are used in conjunction with guidedbone regeneration (GBR) procedures, with or withoutimplant placement, as premature inadvertent opening of aflap can compromise the success of the treatment. There-fore, these sutures are not removed until a clinician hasassessed early epithelial healing, which is usually 2 to 3weeks after surgery. The commonly used nonresorbablesutures for implant dentistry are monofilament materials,including polyamide (nylon), polypropylene, and expandedpolytetrafluoroethylene (e-PTFE).10 These polymer-basedsuture materials have the required strength to resist mus-cle pull and resist plaque accumulation.
Bidra
Polypropylene suture is a monofilament non-resorbable suture composed of an isotactic crystallinestereoisomer of polypropylene, a synthetic linear poly-olefin. It holds knots well, is biologically inert, and elicitsminimal tissue reaction.12 It is not subject to degradationor weakening and maintains tensile strength for up to 2years. However, some of the disadvantages include ma-terial memory, a kinking effect, and stiff suture tags.12
Clinicians who use polypropylene sutures value thehigh strength and the security of this suture to resistingmuscle pull and are willing to compromise on the dis-advantages of this material.
A mouthguard is defined as “a removable dentalprosthesis made of resilient material, which is useful inreducing mouth injuries and protecting the teeth andsurrounding structures from injury.”13 This definition isbroad and does not specifically address soft guards thatare meant to protect the mucosa. Such mucosal guardshave been previously described in the prosthodonticliterature as protecting against chemical burns of themouth.14,15 Essentially, the customized resilient materialcan be used to cover and protect the soft tissues againstany mechanical, chemical, or thermal injuries. The pur-pose of this clinical report is to describe the managementof a sublingual hematoma caused by polypropylene su-ture irritation after implant surgery with a soft mucosalguard.
CLINICAL REPORT
A 60-year-old, partially edentulous woman was referredto the prosthodontist by her general dentist for evalua-tion and implant placement in the left posteriormandible. The patient had been edentulous for over 40years and had been previously experienced a failed bonegraft procedure at the left posterior mandible. The pa-tient’s medical history was unremarkable. Clinical ex-amination revealed a partially edentulous mandible withmissing molar and premolar teeth. Moderate to severeresorption of the residual ridge and reduced keratinizedtissue at the ridge crest were noted (Fig. 1). The resorp-tion was largely restricted in width, and minimal loss ofheight allowed an adequate distance from the ridge crestto the mandibular canal for implant placement. Given thenature of the resorption, a cone-beam computed to-mography (CBCT) analysis was performed before thetreatment plan was finalized. Careful analysis of theCBCT confirmed the clinical findings. The CBCT alsoconfirmed the absence of any lingual undercut at theplanned osteotomy sites.
Based on the clinical and radiographic findings andthe patient’s finances and expectations, a treatment planwas developed to place a narrow diameter implant at theleft first premolar and a regular diameter implant at theleft first molar for a 3-unit partial fixed dental prosthesis.
THE JOURNAL OF PROSTHETIC DENTISTRY
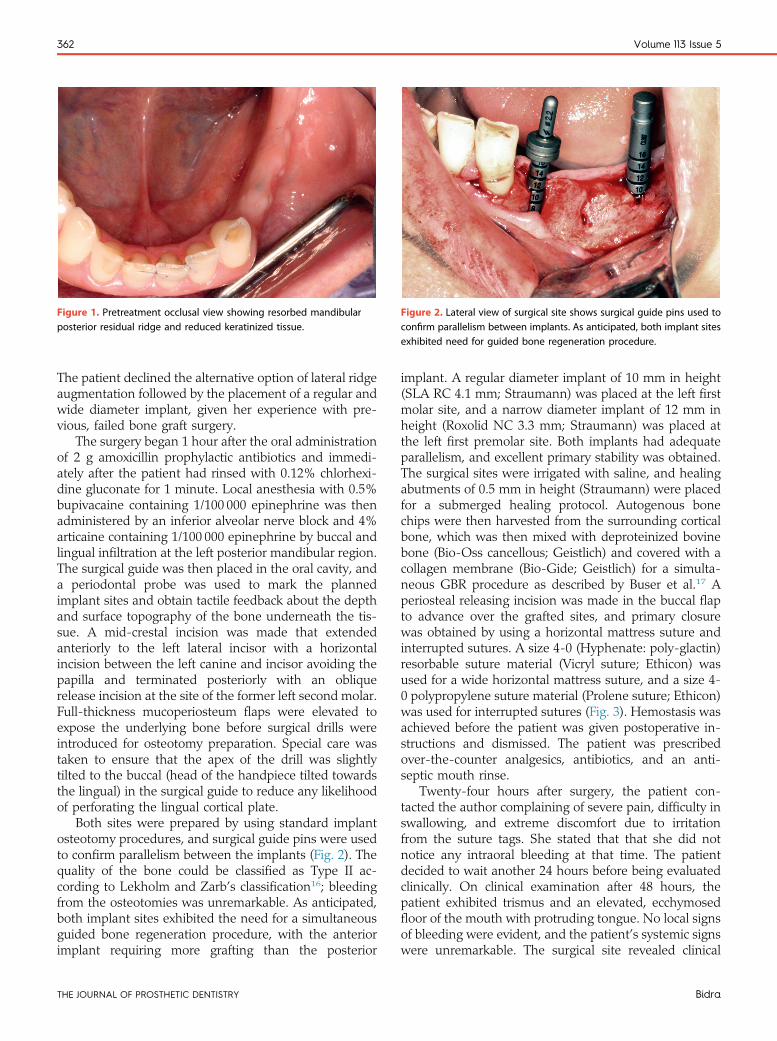
Figure 2. Lateral view of surgical site shows surgical guide pins used toconfirm parallelism between implants. As anticipated, both implant sitesexhibited need for guided bone regeneration procedure.
Figure 1. Pretreatment occlusal view showing resorbed mandibularposterior residual ridge and reduced keratinized tissue.
362 Volume 113 Issue 5
The patient declined the alternative option of lateral ridgeaugmentation followed by the placement of a regular andwide diameter implant, given her experience with pre-vious, failed bone graft surgery.
The surgery began 1 hour after the oral administrationof 2 g amoxicillin prophylactic antibiotics and immedi-ately after the patient had rinsed with 0.12% chlorhexi-dine gluconate for 1 minute. Local anesthesia with 0.5%bupivacaine containing 1/100 000 epinephrine was thenadministered by an inferior alveolar nerve block and 4%articaine containing 1/100 000 epinephrine by buccal andlingual infiltration at the left posterior mandibular region.The surgical guide was then placed in the oral cavity, anda periodontal probe was used to mark the plannedimplant sites and obtain tactile feedback about the depthand surface topography of the bone underneath the tis-sue. A mid-crestal incision was made that extendedanteriorly to the left lateral incisor with a horizontalincision between the left canine and incisor avoiding thepapilla and terminated posteriorly with an obliquerelease incision at the site of the former left second molar.Full-thickness mucoperiosteum flaps were elevated toexpose the underlying bone before surgical drills wereintroduced for osteotomy preparation. Special care wastaken to ensure that the apex of the drill was slightlytilted to the buccal (head of the handpiece tilted towardsthe lingual) in the surgical guide to reduce any likelihoodof perforating the lingual cortical plate.
Both sites were prepared by using standard implantosteotomy procedures, and surgical guide pins were usedto confirm parallelism between the implants (Fig. 2). Thequality of the bone could be classified as Type II ac-cording to Lekholm and Zarb’s classification16; bleedingfrom the osteotomies was unremarkable. As anticipated,both implant sites exhibited the need for a simultaneousguided bone regeneration procedure, with the anteriorimplant requiring more grafting than the posterior
THE JOURNAL OF PROSTHETIC DENTISTRY
implant. A regular diameter implant of 10 mm in height(SLA RC 4.1 mm; Straumann) was placed at the left firstmolar site, and a narrow diameter implant of 12 mm inheight (Roxolid NC 3.3 mm; Straumann) was placed atthe left first premolar site. Both implants had adequateparallelism, and excellent primary stability was obtained.The surgical sites were irrigated with saline, and healingabutments of 0.5 mm in height (Straumann) were placedfor a submerged healing protocol. Autogenous bonechips were then harvested from the surrounding corticalbone, which was then mixed with deproteinized bovinebone (Bio-Oss cancellous; Geistlich) and covered with acollagen membrane (Bio-Gide; Geistlich) for a simulta-neous GBR procedure as described by Buser et al.17 Aperiosteal releasing incision was made in the buccal flapto advance over the grafted sites, and primary closurewas obtained by using a horizontal mattress suture andinterrupted sutures. A size 4-0 (Hyphenate: poly-glactin)resorbable suture material (Vicryl suture; Ethicon) wasused for a wide horizontal mattress suture, and a size 4-0 polypropylene suture material (Prolene suture; Ethicon)was used for interrupted sutures (Fig. 3). Hemostasis wasachieved before the patient was given postoperative in-structions and dismissed. The patient was prescribedover-the-counter analgesics, antibiotics, and an anti-septic mouth rinse.
Twenty-four hours after surgery, the patient con-tacted the author complaining of severe pain, difficulty inswallowing, and extreme discomfort due to irritationfrom the suture tags. She stated that that she did notnotice any intraoral bleeding at that time. The patientdecided to wait another 24 hours before being evaluatedclinically. On clinical examination after 48 hours, thepatient exhibited trismus and an elevated, ecchymosedfloor of the mouth with protruding tongue. No local signsof bleeding were evident, and the patient’s systemic signswere unremarkable. The surgical site revealed clinical
Bidra
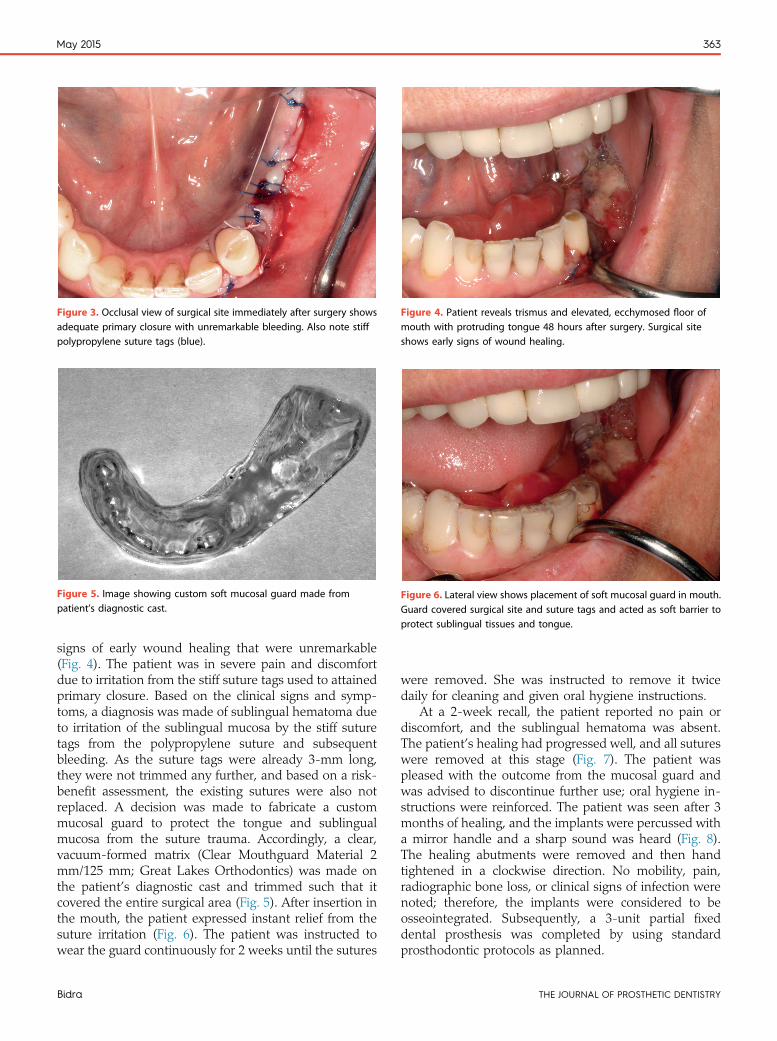
Figure 5. Image showing custom soft mucosal guard made frompatient’s diagnostic cast.
Figure 3. Occlusal view of surgical site immediately after surgery showsadequate primary closure with unremarkable bleeding. Also note stiffpolypropylene suture tags (blue).
Figure 4. Patient reveals trismus and elevated, ecchymosed floor ofmouth with protruding tongue 48 hours after surgery. Surgical siteshows early signs of wound healing.
Figure 6. Lateral view shows placement of soft mucosal guard in mouth.Guard covered surgical site and suture tags and acted as soft barrier toprotect sublingual tissues and tongue.
May 2015 363
signs of early wound healing that were unremarkable(Fig. 4). The patient was in severe pain and discomfortdue to irritation from the stiff suture tags used to attainedprimary closure. Based on the clinical signs and symp-toms, a diagnosis was made of sublingual hematoma dueto irritation of the sublingual mucosa by the stiff suturetags from the polypropylene suture and subsequentbleeding. As the suture tags were already 3-mm long,they were not trimmed any further, and based on a risk-benefit assessment, the existing sutures were also notreplaced. A decision was made to fabricate a custommucosal guard to protect the tongue and sublingualmucosa from the suture trauma. Accordingly, a clear,vacuum-formed matrix (Clear Mouthguard Material 2mm/125 mm; Great Lakes Orthodontics) was made onthe patient’s diagnostic cast and trimmed such that itcovered the entire surgical area (Fig. 5). After insertion inthe mouth, the patient expressed instant relief from thesuture irritation (Fig. 6). The patient was instructed towear the guard continuously for 2 weeks until the sutures
Bidra
were removed. She was instructed to remove it twicedaily for cleaning and given oral hygiene instructions.
At a 2-week recall, the patient reported no pain ordiscomfort, and the sublingual hematoma was absent.The patient’s healing had progressed well, and all sutureswere removed at this stage (Fig. 7). The patient waspleased with the outcome from the mucosal guard andwas advised to discontinue further use; oral hygiene in-structions were reinforced. The patient was seen after 3months of healing, and the implants were percussed witha mirror handle and a sharp sound was heard (Fig. 8).The healing abutments were removed and then handtightened in a clockwise direction. No mobility, pain,radiographic bone loss, or clinical signs of infection werenoted; therefore, the implants were considered to beosseointegrated. Subsequently, a 3-unit partial fixeddental prosthesis was completed by using standardprosthodontic protocols as planned.
THE JOURNAL OF PROSTHETIC DENTISTRY
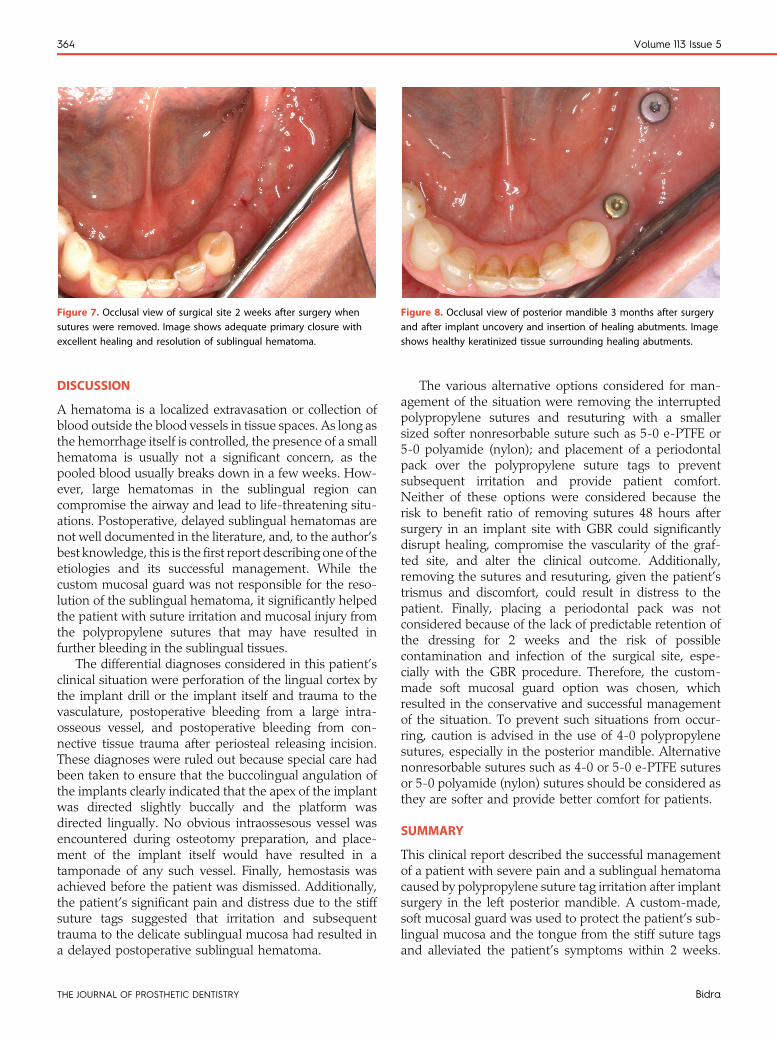
Figure 7. Occlusal view of surgical site 2 weeks after surgery whensutures were removed. Image shows adequate primary closure withexcellent healing and resolution of sublingual hematoma.
Figure 8. Occlusal view of posterior mandible 3 months after surgeryand after implant uncovery and insertion of healing abutments. Imageshows healthy keratinized tissue surrounding healing abutments.
364 Volume 113 Issue 5
DISCUSSION
A hematoma is a localized extravasation or collection ofblood outside the blood vessels in tissue spaces. As long asthe hemorrhage itself is controlled, the presence of a smallhematoma is usually not a significant concern, as thepooled blood usually breaks down in a few weeks. How-ever, large hematomas in the sublingual region cancompromise the airway and lead to life-threatening situ-ations. Postoperative, delayed sublingual hematomas arenot well documented in the literature, and, to the author’sbest knowledge, this is the first report describing one of theetiologies and its successful management. While thecustom mucosal guard was not responsible for the reso-lution of the sublingual hematoma, it significantly helpedthe patient with suture irritation and mucosal injury fromthe polypropylene sutures that may have resulted infurther bleeding in the sublingual tissues.
The differential diagnoses considered in this patient’sclinical situation were perforation of the lingual cortex bythe implant drill or the implant itself and trauma to thevasculature, postoperative bleeding from a large intra-osseous vessel, and postoperative bleeding from con-nective tissue trauma after periosteal releasing incision.These diagnoses were ruled out because special care hadbeen taken to ensure that the buccolingual angulation ofthe implants clearly indicated that the apex of the implantwas directed slightly buccally and the platform wasdirected lingually. No obvious intraossesous vessel wasencountered during osteotomy preparation, and place-ment of the implant itself would have resulted in atamponade of any such vessel. Finally, hemostasis wasachieved before the patient was dismissed. Additionally,the patient’s significant pain and distress due to the stiffsuture tags suggested that irritation and subsequenttrauma to the delicate sublingual mucosa had resulted ina delayed postoperative sublingual hematoma.
THE JOURNAL OF PROSTHETIC DENTISTRY
The various alternative options considered for man-agement of the situation were removing the interruptedpolypropylene sutures and resuturing with a smallersized softer nonresorbable suture such as 5-0 e-PTFE or5-0 polyamide (nylon); and placement of a periodontalpack over the polypropylene suture tags to preventsubsequent irritation and provide patient comfort.Neither of these options were considered because therisk to benefit ratio of removing sutures 48 hours aftersurgery in an implant site with GBR could significantlydisrupt healing, compromise the vascularity of the graf-ted site, and alter the clinical outcome. Additionally,removing the sutures and resuturing, given the patient’strismus and discomfort, could result in distress to thepatient. Finally, placing a periodontal pack was notconsidered because of the lack of predictable retention ofthe dressing for 2 weeks and the risk of possiblecontamination and infection of the surgical site, espe-cially with the GBR procedure. Therefore, the custom-made soft mucosal guard option was chosen, whichresulted in the conservative and successful managementof the situation. To prevent such situations from occur-ring, caution is advised in the use of 4-0 polypropylenesutures, especially in the posterior mandible. Alternativenonresorbable sutures such as 4-0 or 5-0 e-PTFE suturesor 5-0 polyamide (nylon) sutures should be considered asthey are softer and provide better comfort for patients.
SUMMARY
This clinical report described the successful managementof a patient with severe pain and a sublingual hematomacaused by polypropylene suture tag irritation after implantsurgery in the left posterior mandible. A custom-made,soft mucosal guard was used to protect the patient’s sub-lingual mucosa and the tongue from the stiff suture tagsand alleviated the patient’s symptoms within 2 weeks.
Bidra

May 2015 365
Prosthodontists are uniquely advantaged to manage suchpost-surgical complications, given their knowledge andunderstanding of use of a variety of biomaterials.
REFERENCES
1. Goodacre CJ, Kan JY, Rungcharassaeng K. Clinical complications ofosseointegrated implants. J Prosthet Dent 1999;81:537-52.
2. Goodacre CJ, Bernal G, Rungcharassaeng K, Kan JY. Clinical complicationswith implants and implant prostheses. J Prosthet Dent 2003;90:121-32.
3. Bidra AS. Flapless implant surgery to overcome anatomic challenges in theanterior mandible for overdenture therapy: a clinical report. J Prosthet Dent2014;111:175-80.
4. Standring S. Gray’s anatomy: The anatomical basis of clinical practice.40th ed. Spain: Churchill Livingstone/Elsevier; 2008. p. 499-506. 530-3,538-46.
5. Romanos GE, Gupta B, Crespi R. Endosseous Arteries in the anteriormandible: literature review. Int J Oral Maxillofac Implants 2012;27:90-4.
6. Moore KL, Dalley AF. Clinically oriented anatomy. 5th ed. Baltimore: Lip-pincott Williams & Wilkins; 2006. p. 886-1122. 1138-43.
7. McDonnell D, Nouri MR, Todd ME. The mandibular lingual foramen: aconsistent arterial foramen in the middle of the mandible. J Anat 1994;184:363-9.
8. Fujita S, Ide Y, Abe S. variations of vascular distribution in the mandibularanterior lingual region: a high risk of vascular injury during implant surgery.Implant Dent 2012;21:259-64.
9. Dubois L, de Lange J, Baas E, Van Ingen J. Excessive bleeding in the floor ofthe mouth after endosseous implant placement: a report of two cases. Int JOral Maxillofac Surg 2010;39:412-5.
Noteworthy Abstracts of
The influence of interimplant distance in masupported by two implants on patient satisfa
Greckili O, Cilingir A, Erdogan O, Kesoglu AC, BiInt J Prosthodont 2015;28:19-21
This study evaluates the influence of interimplant distance (Ipatients who received mandibular overdentures supported bycrest and linearly on all of the patients' mandibular casts. Thsubtracting these two values from each other. Higher IDs wehigher crestal detour values were associated with better genesthetics, pain, and QOL scores (P < .05).
Reprinted with permission of Quintessence Publishing.
Bidra
10. Silverstein LH, Shatz PC, Kurtzman D. The suture book: The definitive guideto dental suturing and surgical flap closure. Newtown: AEGIS Communi-cations 2011. p. 15-27.
11. Esposito M, Maghaireh H, Grusovin MG, Ziounas I, Worthington HV. In-terventions for replacing missing teeth: management of soft tissues for dentalimplants. Cochrane Database Syst Rev 2012;15. 2:CD006697.
12. Lai, SY, Meyers AD. Sutures and needles. Medscape Reference, November2014. Available at: http://emedicine.medscape.com/article/884838-overview.Last accessed April 6, 2015.
13. The glossary of prosthodontic terms, 8th Edition. J Prosthet Dent 2005;94:10-92.
14. Seals RR Jr, Dorrough BC. Custom mouth protectors: a review of their ap-plications. J Prosthet Dent 1984;51:238-42.
15. Seals RR Jr, Cain JR. Prosthetic treatment for chemical burns of the oralcavity. J Prosthet Dent 1985;53:688-91.
16. Lekholm U, Zarb G. Patient selection and preparation. In: Brånemark P,Zarb G, Albrektsson T. Tissue-integrated prosthesis. Chicago: QuintessencePublishing Co; 1985. p. 199-211.
17. Buser D, Chappuis V, Kuchler U, Bornstein MM, Wittneben JG, Buser R, et al.Long-term stability of early implant placement with contour augmentation.J Dent Res 2013;92(12 Suppl):176S-82S.
Corresponding author:Dr Avinash S. BidraUniversity of Connecticut Health Center263 Farmington Ave, L6078Farmington, CT 06030Email: [email protected]
Copyright © 2015 by the Editorial Council for The Journal of Prosthetic Dentistry.
the Current Literature
ndibular overdenturesction and quality of life
lmenoglu C, Ozdiler A, Bilhan H
D) on patient satisfaction and quality of life (QOL) of 55two implants. IDs were measured over the residual ridgee crestal detours of all patients were determined byre associated with better QOL scores (P < .05), whereaseral comfort, chewing, ease of hygiene maintenance,
THE JOURNAL OF PROSTHETIC DENTISTRY