management of type 2 diabetes cardiovascular outcomes ... · management of type 2 diabetes...
TRANSCRIPT

Management of Type 2 DiabetesCardiovascular Outcomes Trials
2018
Tom Blevins MDTexas Diabetes and Endocrinology
Austin, Texas

Dr. Blevins has disclosed that he has received grant support and is on the speaker’s bureau for AstraZeneca, Boehringer Ingelheim, Lilly and Sanofi, and he is on the advisory committee for Medtronic and Senseonics.
Speaker Disclosure

By the end of this activity, the participant will be better able to: Review FDA requirements for new drugs for type 2 diabetes to establish CV
safety. Describe the results of cardiovascular outcomes trials with incretin modulators
such as DPP4 inhibitors and GLP1 receptor agonists. Describe the results and clinical implications of cardiovascular outcomes trials
with SGLT2 inhibitors. Discuss the FDA indication related to cardiovascular benefits of glucose
lowering medications. Review the updates to the American Diabetes Association treatment
recommendations relating to the effect on CV outcomes of medications for treating type 2 diabetes.
Implement the clinical application of the results of cardiovascular outcomes trials in treating patients with type 2 diabetes.
Learning Objectives


FDA CVOT Guidance—2008
Timeline of Major DiabetesOutcomes Trials
5
Blue = Intensive vs standard control using same set of glucose-lowering agent(s)Purple = Intensive control with a specific agent vs standard careRed = Placebo- or active-controlled study* = FDA-mandated cardiovascular safety trial
ACCORD, Action to Control Cardiovascular Risk in Diabetes; ADVANCE, Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation; CANVAS, Canagliflozin Cardiovascular Assessment Study; DCCT, Diabetes Control and Complications Trial; DEVOTE, Trial Comparing Cardiovascular Safety of Insulin Degludec versus Insulin Glargine in Patients with Type 2 Diabetes at High Risk of Cardiovascular Events; EXAMINE, Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care; ELIXA, Evaluation of Lixisenatide in Acute Coronary Syndrome; EMPA-REG, EMPA-REG OUTCOME trial; Exenatide Study of Cardiovascular Event Lowering; LEADER, Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; ORIGIN, Outcome Reduction with an Initial Glargine Intervention; PROActive, Prospective Pioglitazone Clinical Trial in Macrovascular Events; RECORD, Rosiglitazone Evaluated for Cardiovascular Outcomes in Oral Agent Combination Therapy for Type 2 Diabetes; SAVOR-TIMI, Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus–Thrombolysis in Myocardial Infarction; STOP-NIDDM, Study to Prevent Non-Insulin-Dependent Diabetes Mellitus; SUSTAIN, Trial to Evaluate Cardiovascular and Other Long-Term Outcomes with Semaglutide in Subjects with Type 2 Diabetes; TECOS, Trial Evaluating Cardiovascular Outcomes with Sitagliptin; UKPDS, United Kingdom Prospective Diabetes Study; VADT, Veterans Affairs Diabetes Trial.
1995 2000 2005 2010 2015
Cardiovascular Outcomes Trials: A Brief History
• 2008 FDA guidance mandating assessment of CV safety of all antihyperglycemic agents in RCTs– Designed as noninferiority studies to demonstrate study drug was not
associated with more MACE than placebo• Some study designs tested for superiority if noninferiority criteria were met
– Primary endpoint: Composite of cardiovascular death, nonfatal MI, and nonfatal stroke
• Some primary endpoints included additional components
6
MACE = major adverse cardiovascular events; RCTs, randomized controlled trials.
FDA. Guidance for industry: evaluating cardiovascular risk in new antidiabetic therapies to treat type 2 diabetes. http://www.fda.gov/downloads/drugs/guidancecomplianceregulatoryinformation/guidances/ucm071627.pdf.

7

53 y/o female with Type 2 Diabetes x 6 years◦ A1c is 7.2% on metformin and DPP4◦ On ACEi and statin BP is 118/72 LDL is 69 mg/dl
Hx of MI 8 years ago What do you do?
1. Double statin to lower LDL further2. Reduce the ACEi as her BP is too low to perfuse her coronary arteries3. Discuss SGLT2 and GLP-1 CV risk reduction trials4. No changes needed since the DPP-4 is cardioprotective
Case #1 – ARS Question

9
5,380 patients with ACS
16,492 patients with CVD or CVD Risk
14,671 patients with Type 2 diabetes and CVD
10

11
12

13

14

15

66 y/o male with Type 2 Diabetes x 14 years◦ A1c is 8.2% on basal and prandial insulin and metformin◦ On BP meds and statin BP is 138/82 LDL is 55 mg/dl
Hx of CAB 12 years ago What do you do?
1. Increase BP med2. Make adjustments to the insulin and suggest another visit in 3-4
months3. Discuss SGLT2 and GLP-1 CV risk reduction trials
Case #2 – ARS Question

17
7,020 with Type 2 Diabetes and CVD (2:1 empa:placebo
10,142 with Type 2 diabetes and high CV Risk
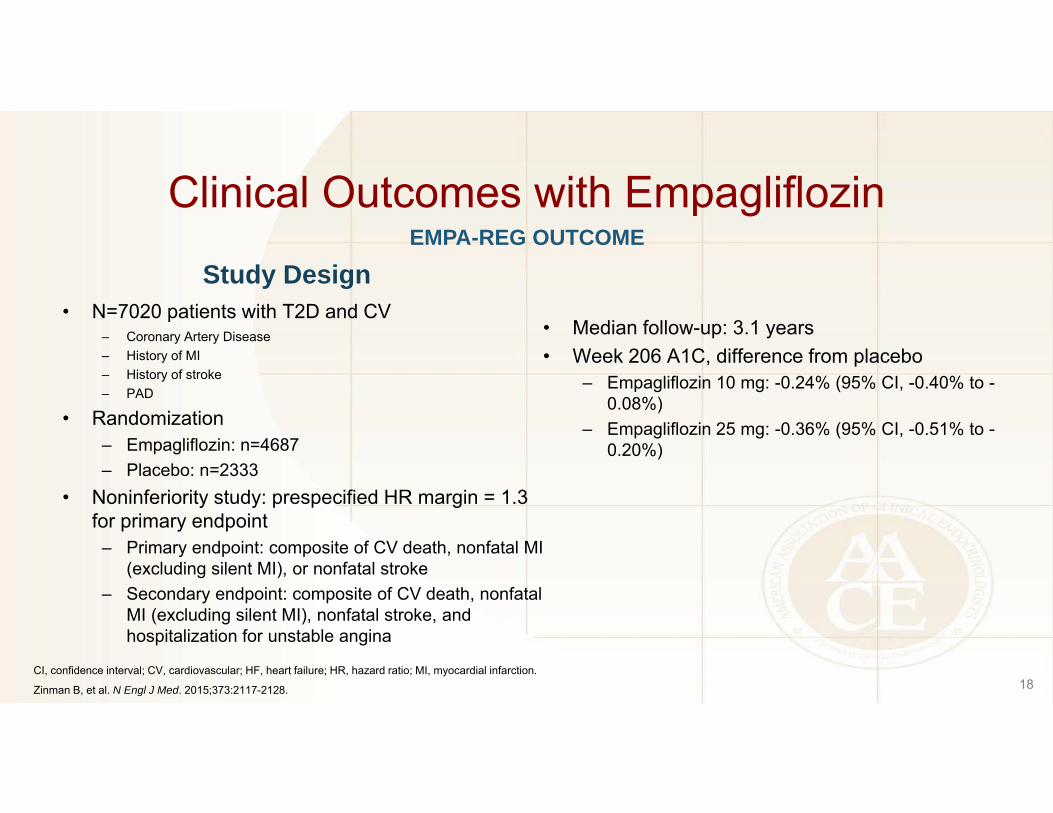
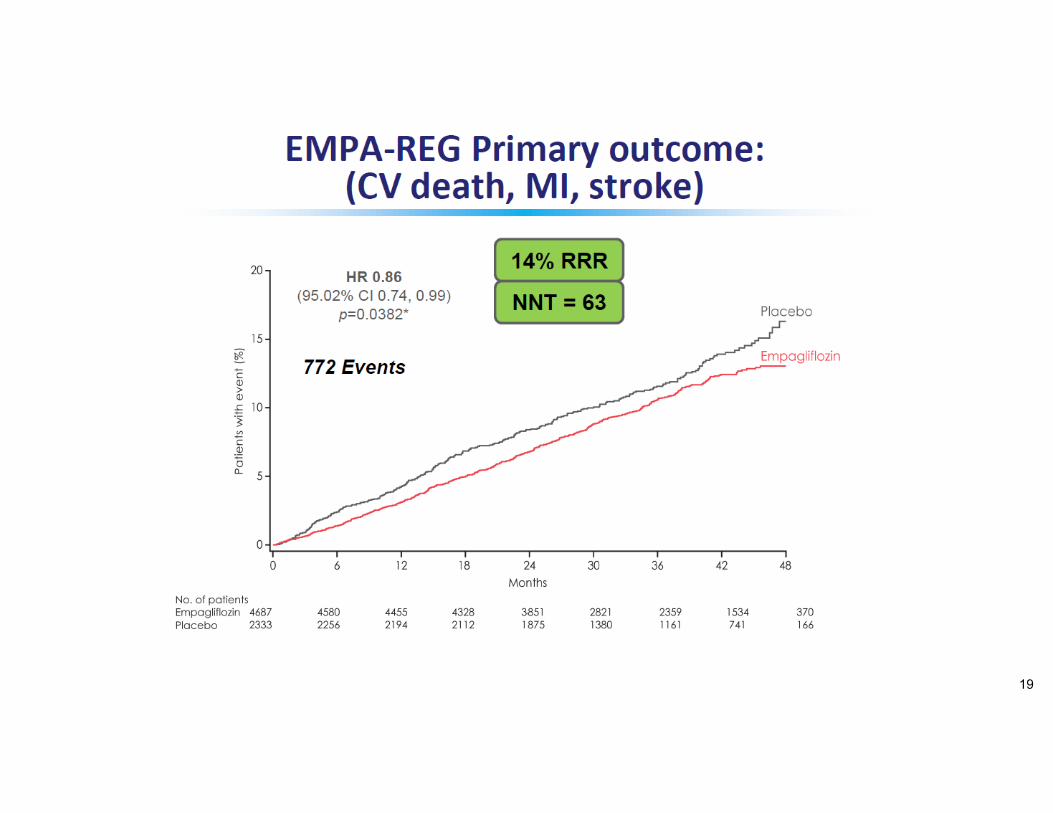
Clinical Outcomes with Empagliflozin
Study Design• N=7020 patients with T2D and CV
– Coronary Artery Disease– History of MI– History of stroke– PAD
• Randomization– Empagliflozin: n=4687– Placebo: n=2333
• Noninferiority study: prespecified HR margin = 1.3 for primary endpoint
– Primary endpoint: composite of CV death, nonfatal MI (excluding silent MI), or nonfatal stroke
– Secondary endpoint: composite of CV death, nonfatal MI (excluding silent MI), nonfatal stroke, and hospitalization for unstable angina
• Median follow-up: 3.1 years• Week 206 A1C, difference from placebo
– Empagliflozin 10 mg: -0.24% (95% CI, -0.40% to -0.08%)
– Empagliflozin 25 mg: -0.36% (95% CI, -0.51% to -0.20%)
18
EMPA-REG OUTCOME
CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Zinman B, et al. N Engl J Med. 2015;373:2117-2128.
19

20

21

23

Clinical Outcomes with Empagliflozin
24
EMPA-REG OUTCOME Safety Results
CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Zinman B, et al. N Engl J Med. 2015;373:2117-2128.
Event Pooled Empagliflozin (%) Placebo (%)
Any adverse event 90.2 91.7
Serious adverse event 38.2 42.3
Death 3.8 5.1
Any hypoglycemia 27.8 27.9
Severe hypoglycemia 1.3 1.5
Urinary tract infection Male 10.5 9.4
Female 36.4 40.6
Genital infection Male 5.0 1.5
Female 10.0 2.6
Volume depletion 5.1 4.9
Diabetic ketoacidosis 0.1 <0.1
Bone fracture 3.8 3.9

Empaglifozin Indication
25
Empaglifozin is a sodium-glucose co-transporter 2 (SGLT2) inhibitor indicated:
As an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus
To reduce the risk of cardiovascular death in adult patients with type 2 diabetes mellitus and established cardiovascular disease

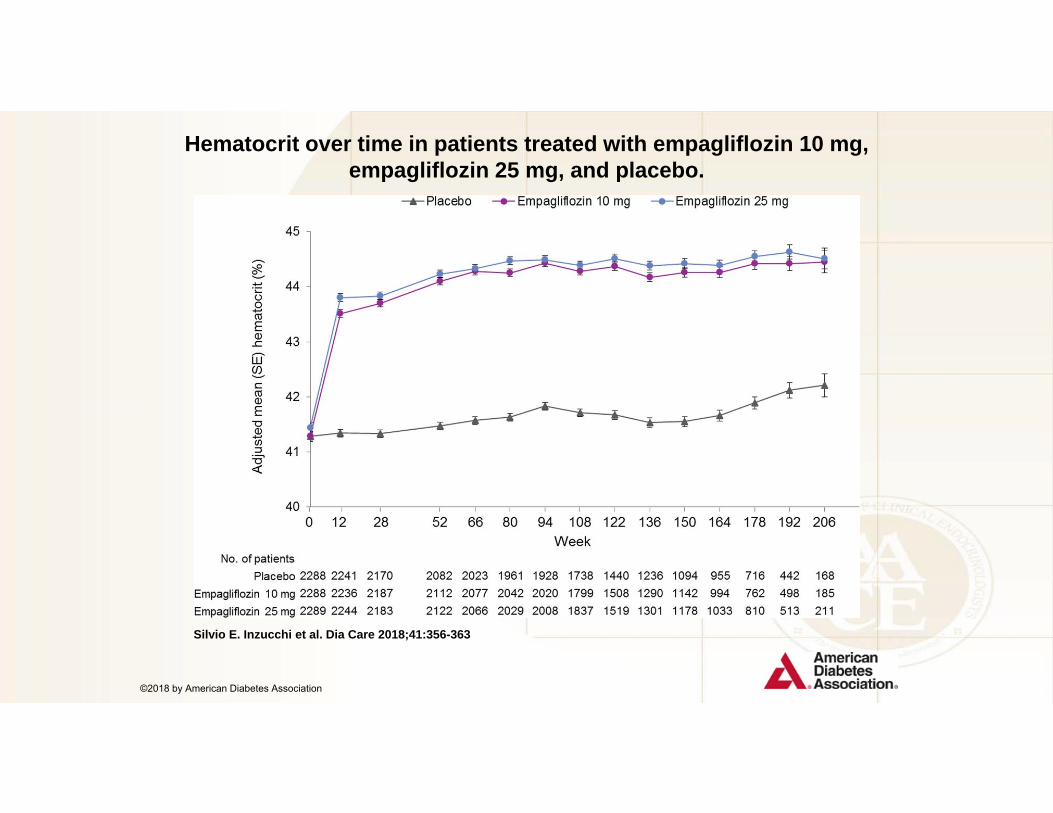
Hematocrit over time in patients treated with empagliflozin 10 mg, empagliflozin 25 mg, and placebo.
Silvio E. Inzucchi et al. Dia Care 2018;41:356-363
©2018 by American Diabetes Association

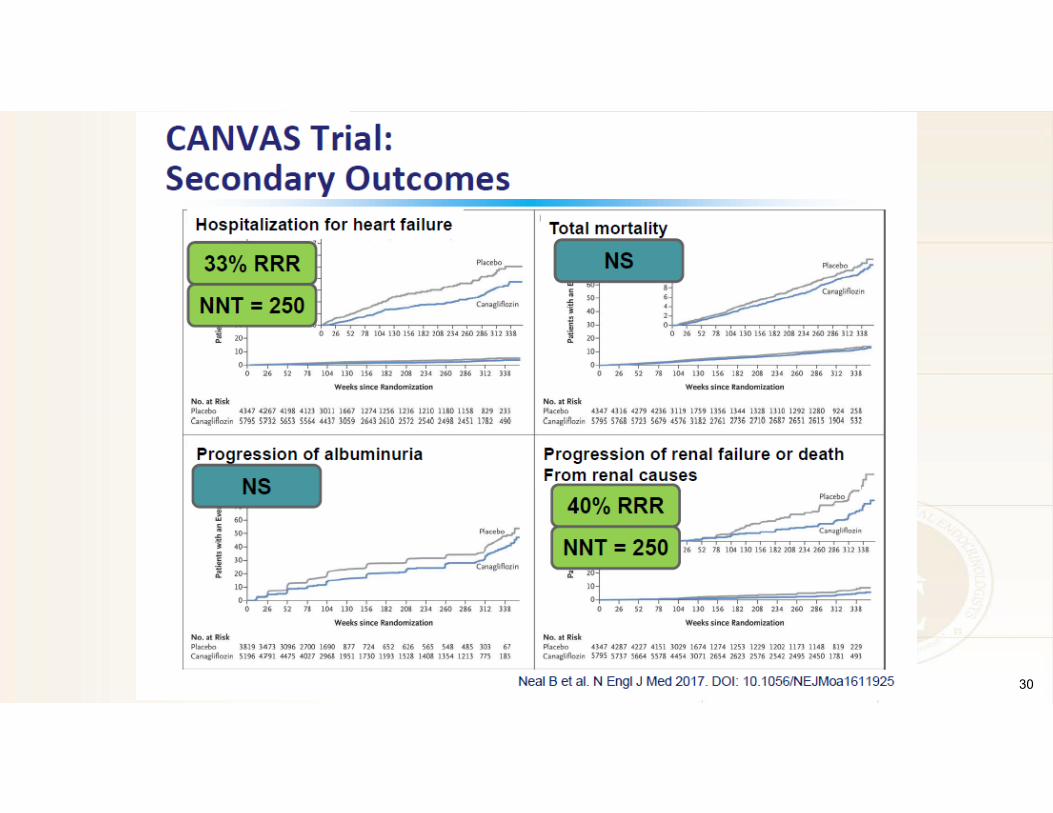
Clinical Outcomes with Canagliflozin
• N=10,142 patients with T2D and high CV risk– CANVAS: n=4330– CANVAS-R: n=5812
• Randomization (across both studies)– Canagliflozin: n=5795– Placebo: n=4347
• Endpoints– Primary endpoint: composite of CV death, nonfatal MI, or
nonfatal stroke– Secondary endpoints:
• All-cause death• CV death• Albuminuria progression• Composite of CV death and HF hospitalization
28
CANVAS Program Study Design
CANVAS, Canaglflozin Cardiovascular Assessment Study; CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Neal B, et al. N Engl J Med. 2017;377:644-657.

29
30

Adverse Events with Canagliflozin
31
CANVAS Program* Safety Results
*Includes patients from CANVAS and CANVAS-R (N=10,142). †CANVAS-only population (n=4330).
Neal B, et al. N Engl J Med. 2017 Jun 12 [epub ahead of print].
Event Canagliflozin Placebo P valueEvents per 1000-patient years
All serious adverse events 104.3 120.0 0.04
Adverse events leading to discontinuation 35.5 32.8 0.07
Diabetic ketoacidosis (adjudicated) 0.6 0.3 0.14
Events of interest occurring in significantly more canagliflozin-treated patients
Amputation 6.3 3.4 <0.001
Bone fracture (adjudicated)
All 15.4 11.9 0.02
Low trauma 11.6 9.2 0.06
Infection of male genitalia 34.9 10.8 <0.001
Osmotic diuresis† 34.5 13.3 <0.001
Volume depletion† 26.0 18.5 0.009
Mycotic genital infection in women† 68.8 17.5 <0.001

CVD-REAL Study
Study Objectives Primary Compare risk of HHF (Hospitalization for heart failure) in patients with Type 2 diabetes newly initiated on SGLT-2 inhibitors versus other glucose-lowering drugs (GLDs)
Secondary Compare risk of all-cause death between the two treatment groups Compare risk of HHF or all-cause death between the two treatment groups
Kosiborod M, et al. Lower risk of heart failure and death in patients initiated on SGLT-2 inhibitors versus other glucose-lowering drugs: The CVD-REAL Study. Circulation. 2017 May 18.




37

46 y/o male with Type 2 Diabetes x 4 years◦ A1c is 6.2% on basal insulin and metformin◦ On BP meds and statin BP is 128/82 LDL is 65 mg/dl
Hx of PAD and femoral artery stent 1 year ago What do you do?
1. Increase BP med2. No more to do. His A1c, BP, and LDL are at goal3. Discuss SGLT2 and GLP-1 CV risk reduction trials
Case #4 – ARS Question
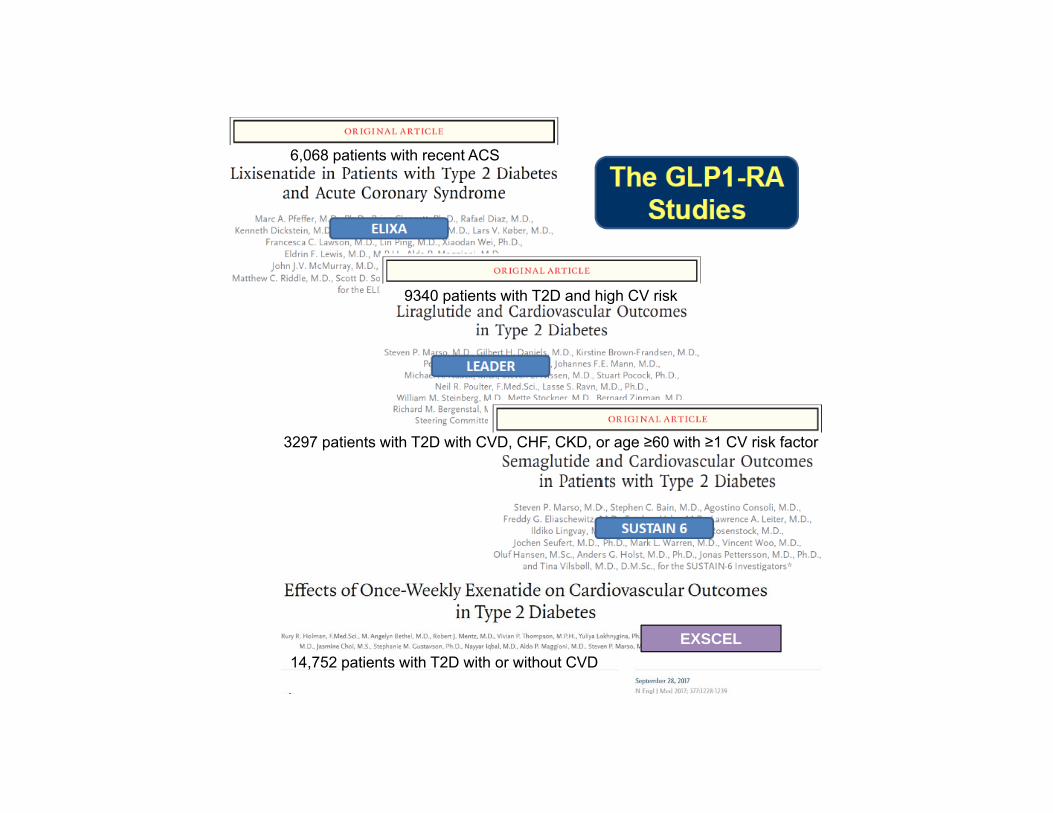
EXSCEL
6,068 patients with recent ACS
9340 patients with T2D and high CV risk
14,752 patients with T2D with or without CVD
3297 patients with T2D with CVD, CHF, CKD, or age ≥60 with ≥1 CV risk factor

Clinical Outcomes with Lixisenatide
40
ELIXA(Patients with T2D and CVD; N=6068)
*CV death, nonfatal MI, or nonfatal stroke, and hospitalization for unstable angina; †CV death, nonfatal MI, nonfatal stroke, hospitalization for unstable angina, hospitalization for HF, and coronary revascularization.
CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Pfeffer MA, et al. N Engl J Med. 2015;373:2247-2257.
0.00 1.00 2.00 3.00
Hazard ratio (95% CI) P value
Primary composite endpoint* 1.02 (0.89-1.17) 0.81
Secondary composite endpoint† 0.97 (0.85-1.10) 0.63
CV death 0.98 (0.78-1.22) 0.85
Fatal or nonfatal MI 1.03 (0.87-1.22) 0.71
Stroke 1.12 (0.79-1.58) 0.54
Unstable angina 1.11 (0.47-2.62) 0.81
Hospitalization for heart failure 0.96 (0.75-1.23) 0.75
Death from any cause 0.94 (0.78-1.13) 0.50
Favors lixisenatide

Clinical Outcomes with Liraglutide
Study Design• N=9340 patients with T2D and high CV risk• Liraglutide
– Age of >50• History of MI• Prior MI or TIA• Prior revascularization• >50% stenosis of coronary, carotid or lower extremity arteries• Symptomatic CHD• Heart failure• CKD
– CVD risk factors (age> 60)• Microalbuminuria or proteinuria• Htn and LVH• Ankle –brachial index <0.9
• Randomization– Liraglutide: n=4672– Placebo: n=4668
Key Results• Noninferiority study:
– Primary endpoint: composite of CV death, nonfatal MI (including silent MI), or nonfatal stroke
– Secondary endpoint: composite of CV death, nonfatal MI (including silent MI), nonfatal stroke, coronary revascularization, and hospitalization for unstable angina or HF
• Median follow-up: 3.5 years• Difference from placebo at 36 months
– A1C: −0.40% (95% CI, −0.45% to −0.34%)– Weight: −2.3 kg (95% CI, −2.0 to −2.5 kg)– SBP: −1.2 mm Hg (95% CI, −0.5 to −1.9 mm Hg)
• Lower numerical incidence of pancreatitis in liraglutide group (not statistically significant)
41
LEADER
CI, confidence interval; CV, cardiovascular; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Marso SP, et al. N Engl J Med. 2016:375:311-322.

42
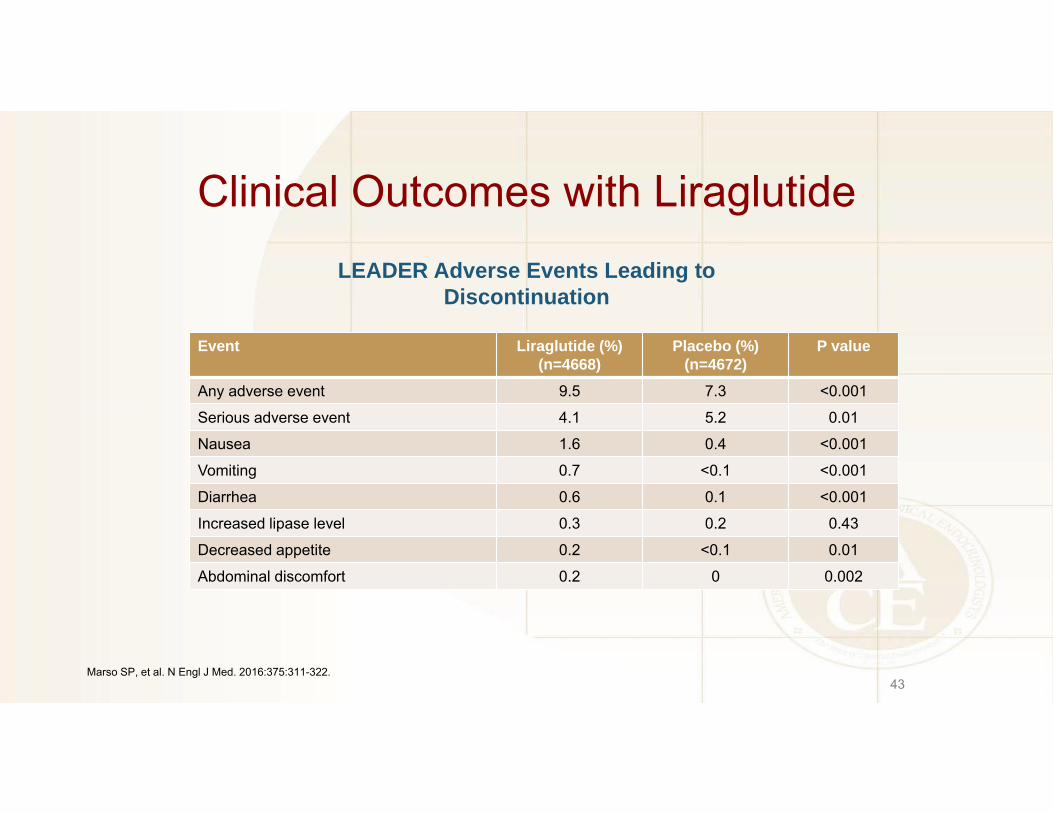
Clinical Outcomes with Liraglutide
43
LEADER Adverse Events Leading to Discontinuation
Marso SP, et al. N Engl J Med. 2016:375:311-322.
Event Liraglutide (%)(n=4668)
Placebo (%)(n=4672)
P value
Any adverse event 9.5 7.3 <0.001
Serious adverse event 4.1 5.2 0.01
Nausea 1.6 0.4 <0.001
Vomiting 0.7 <0.1 <0.001
Diarrhea 0.6 0.1 <0.001
Increased lipase level 0.3 0.2 0.43
Decreased appetite 0.2 <0.1 0.01
Abdominal discomfort 0.2 0 0.002

Liraglutide Indication
44
Liraglutide is a glucagon−like peptide−1 (GLP−1) receptor agonist indicated:
As an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus
To reduce the risk of major adverse cardiovascular events (cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke) in adults with type 2 diabetes mellitus and established cardiovascular disease
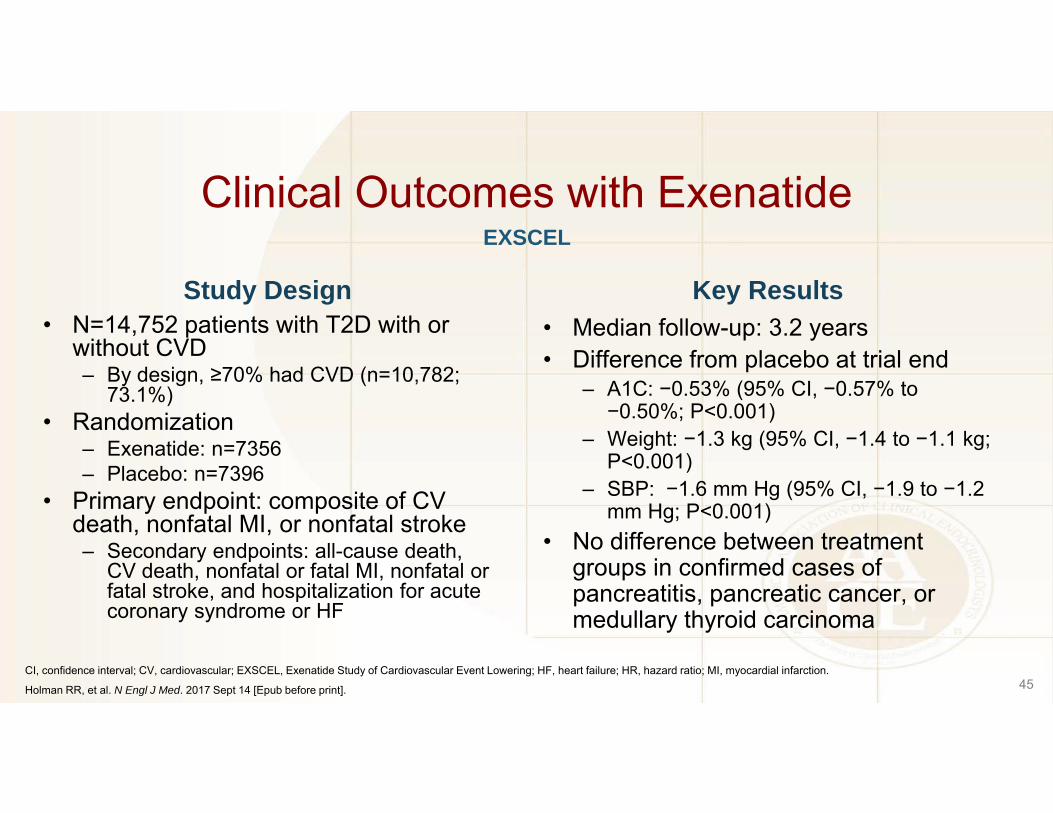
Clinical Outcomes with Exenatide
Study Design• N=14,752 patients with T2D with or
without CVD– By design, ≥70% had CVD (n=10,782;
73.1%)• Randomization
– Exenatide: n=7356– Placebo: n=7396
• Primary endpoint: composite of CV death, nonfatal MI, or nonfatal stroke– Secondary endpoints: all-cause death,
CV death, nonfatal or fatal MI, nonfatal or fatal stroke, and hospitalization for acute coronary syndrome or HF
Key Results• Median follow-up: 3.2 years• Difference from placebo at trial end
– A1C: −0.53% (95% CI, −0.57% to −0.50%; P<0.001)
– Weight: −1.3 kg (95% CI, −1.4 to −1.1 kg; P<0.001)
– SBP: −1.6 mm Hg (95% CI, −1.9 to −1.2 mm Hg; P<0.001)
• No difference between treatment groups in confirmed cases of pancreatitis, pancreatic cancer, or medullary thyroid carcinoma
45
EXSCEL
CI, confidence interval; CV, cardiovascular; EXSCEL, Exenatide Study of Cardiovascular Event Lowering; HF, heart failure; HR, hazard ratio; MI, myocardial infarction.
Holman RR, et al. N Engl J Med. 2017 Sept 14 [Epub before print].

Clinical Outcomes with Exenatide
46
EXSCE(N=14,752)
Holman RR, et al. N Engl J Med. 2017 Sept 14 [Epub before print].

New Antihyperglycaemic Medication Usage
0
2
4
6
8
10
12
14
16
Metformin Sulfonylureas Thiazolidinediones DPP-4i SGLT-2i* GLP-1 ReceptorAgonists**
Insulin
Prop
ortio
n (%
)
Exenatide Placebo
146 173
549
782
274
401
182
265
692
1021
356
450508
652
Subjects are considered to have taken a new medication if there is no indication of usage at baseline visit as well as indication of usage during at least one post-randomisation visit. Percentages presented are for available data. * Information regarding SGLT-2 inhibitor usage was added to the eCRF on 9th May, 2013. Percentages presented are for ITT population.** Includes GLP-1 receptor agonist usage other than study medication

Clinical Outcomes with Exenatide
48
Event Exenatide (%)(n=7344)
Placebo (%)(n=7372)
Any serious AE 16.8 16.6
Serious adverse treatment-related event 0.8 0.5
Serious AE leading to study withdrawal 1.5 1.4
Events of Clinical Interest
Adjudicated pancreatitis 0.4 0.3
Severe pancreatitis <0.1 <0.1
Adjudicated cancer (any) 4.8 4.9
Adjudicated medullary thyroid carcinoma <0.1 <0.1
Adjudicated pancreatic cancer 0.2 0.2
Severe hypoglycemia 3.4 3.0
Event rate 1.6 per 100 pt-years 1.8 per 100 pt-years
EXSCELSerious Adverse Events and Events of Special Interest
AE, adverse event.
Holman RR, et al. N Engl J Med. 2017 Sept 14 [Epub before print].

Clinical Outcomes with Semaglutide
• N=3297 patients with T2D with CVD, CHF, CKD, or age ≥60 with ≥1 CV risk factor
• Randomization– Semaglutide: n=1648– Placebo: n=1649
• Noninferiority study:– Primary endpoint: composite of CV death, nonfatal MI (including silent MI), or nonfatal stroke– Key secondary endpoints
• Composite of CV death, nonfatal MI, nonfatal stroke, coronary or peripheral revascularization, and hospitalization for unstable angina or HF
• Composite of all-cause death, nonfatal MI, nonfatal stroke• Retinopathy complications• New or worsening nephropathy
49
SUSTAIN 6 Study Design
CI, confidence interval; CHF, congestive heart failure; CKD, chronic kidney disease; CV, cardiovascular; CVD, cardiovascular disease; HF, heart failure; HR, hazard ratio; MI, myocardial infarction; SUSTAIN, Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes.
Marso SP, et al. N Engl J Med. 2016:375:1834-1844.
50
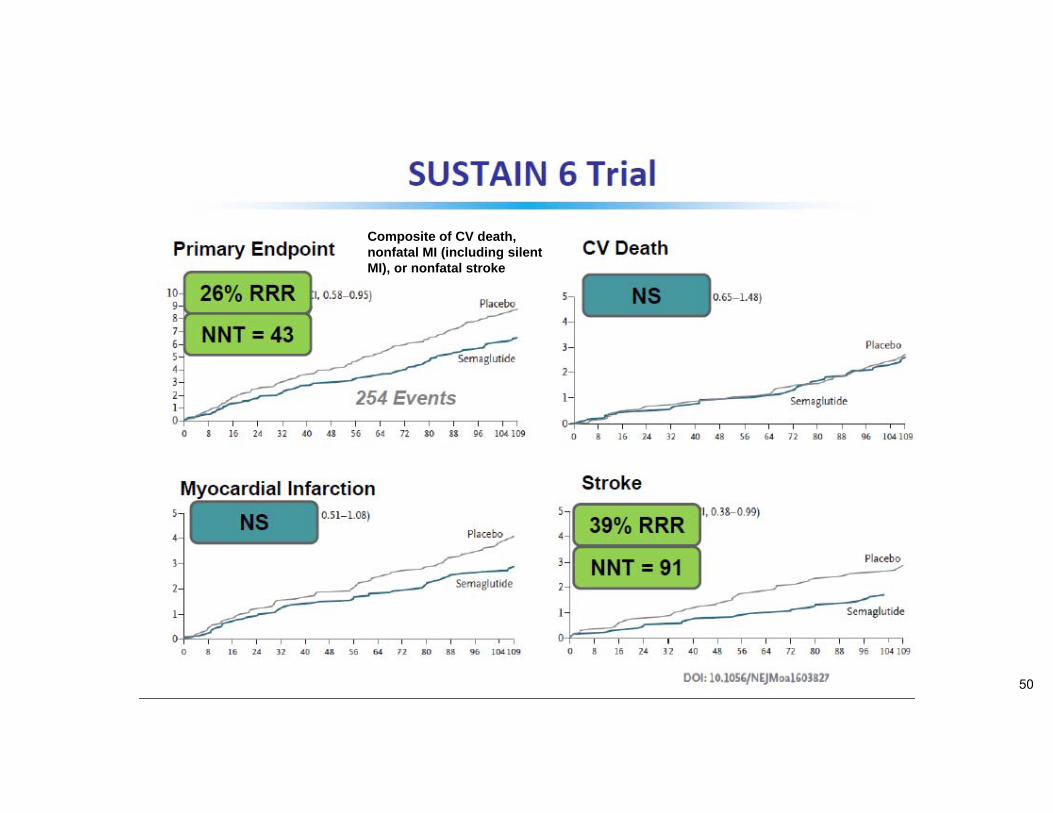
Composite of CV death, nonfatal MI (including silent MI), or nonfatal stroke

Hazard ratio (95% CI) P value
Primary composite endpoint* 0.74 (0.58-0.95) 0.02
Expanded composite endpoint† 0.88 (0.81-0.96) 0.002
All-cause death, nonfatal MI, nonfatal stroke 0.77 (0.61-0.97) 0.03
Death from any cause 1.05 (0.74-1.50) 0.79
CV death 0.98 (0.65-1.48) 0.92
Nonfatal MI 0.74 (0.51-1.08) 0.12
Nonfatal stroke 0.61 (0.38-0.99) 0.04
Revascularization 0.65 (0.50-0.86) 0.003
Retinopathy complications 1.76 (1.11-2.78) 0.02
New or worsening nephropathy 0.64 (0.46-0.88) 0.005
Clinical Outcomes with Semaglutide
51
SUSTAIN 6 Results(N=3297)
*CV death, nonfatal MI (including silent MI), or nonfatal stroke; †CV death, nonfatal MI, nonfatal stroke, coronary or peripheral revascularization, and hospitalization for unstable angina or HF.
CI, confidence interval; CV, cardiovascular; HF, heart failure; MI, myocardial infarction.
Marso SP, et al. N Engl J Med. 2016:375:1834-1844.
0.00 1.00 2.00 3.00
Favors semaglutide
Median follow-up: 2.1 years

Clinical Outcomes with Semaglutide
52
SUSTAIN 6 Selected Adverse Events
Marso SP, et al. N Engl J Med. 2016:375:1834-1844..
Event Semaglutide 1 mg (%)(n=822)
Placebo 1 mg (%)(n=825)
Any adverse event 89.1 89.2Serious adverse event 33.6 36.1Gastrointestinal disorder 52.3 35.2
Diarrhea 18.4 10.5Nausea 21.9 8.1Vomiting 14.8 4.1
Acute pancreatitis 0.4 1.1Gallbladder disorder 3.2 2.8
Cholelithiasis 2.1 1.5Acute cholecystitis 0 0.2
Severe or symptomatic hypoglycemia 21.7 21.0Injection site reaction 0.7 0.3Neoplasm (any) 10.8 8.4
Any malignant 4.9 4.2Malignant pancreatic 0.1 0.2




Baseline Patient Characteristics for CV Risk Reduction
Empaglifozin◦ Coronary Artery Disease◦ History of MI◦ History of stroke◦ PAD
Liraglutide◦ Age of >50 History of MI Prior MI or TIA Prior revascularization >50% stenosis of coronary, carotid or
lower extremity arteries Symptomatic CHD Heart failure CKD
◦ CVD risk factors (age> 60) Microalbuminuria or proteinuria Htn and LVH Ankle –brachial index <0.9

AACE
ADA
Clinical Guidelines and CVOT





Cardiovascular Risk Reduction in Diabetes
2018





47 y/o female with Type 2 Diabetes x 15 years◦ A1c is 7.8% on metformin + GLP-1 med◦ On ACEi and statin BP is controlled LDL is 60 mg/dl BMI is 32
Hx of coronary stent placed last year What do you do?
1. Add basal insulin2. Discussed exercise and weight loss3. Discuss SGLT2 CV risk reduction trials
Case #3 – ARS Question
Q and A

Before 2O15, there was limited data that showed that glucose lowering medications reduce cardiovascular disease
1. True2. False
ARS #1. True/False

1. Sitagliptin2. Empaglifozin3. Exenatide4. Liraglutide5. 2 and 4
ARS #2The following meds have been shown to reduce cardiovascular events in outcomes trials

1. Smoking2. Heart calcium (Agatson) score of >4503. Prior MI4. Prior stroke5. 3 and 46. 2 and 3
ARS #3Baseline characteristics in the Empaglifozin trial which showed reduction in CV death included the following: