medic mobile annual report 2014
DESCRIPTION
Medic Mobile builds mobile and web tools to help health workers provide better care that reaches everyone. Our annual report tells the story of our process, successes, learnings and commitment to bring health care access to everyone on the planet.TRANSCRIPT
MEDIC MOBILE TM
A N N U A L
R E P O R T
2013

In many parts of the developing world, millions of people are at risk of not receiving essential
health services. Children may not benefit from life-saving vaccinations. Women often lack care
before and after giving birth. Contagious diseases go undiagnosed and unreported. And clinics
often run out of medications.
Often, the nearest doctor or nurse is hours, or even days, away. In fact, according to the World
Health Organization (WHO), more than one billion people may never see a doctor in their lifetimes.
The people who live in these communities benefit from two powerful assets. According to
WHO, some 1.3 million community health workers, many of whom are volunteers, provide basic
healthcare to local residents and link them to the healthcare system. They are committed and
trusted members of the communities where they live and work.
In these same parts of the world, there is also reliable and nearly ubiquitous cellular phone
service. According to a United Nations agency, mobile penetration in developing nations is
around 90 percent of the population.
As a leader in the growing field of mHealth—using mobile devices to support the delivery of
healthcare—our team at Medic Mobile connects these dots.
We develop tools using cellular technology that enable community health workers, staff at
community clinics, ministers of health, and others to monitor diseases, stay in touch with families
and each other, send emergency alerts to regional hospitals, and convey critical data to key
decision makers at health ministries.
Medic Mobile enables people at all levels of the health delivery system to use simple, powerful,
flexible, and inexpensive tools to help people access care, stay in care, and receive higher
quality care—wherever it is needed.
We’re proud of our progress. At the end of 2013, our efforts covered more than five million
people in 21 countries, representing 54 projects with 39 partners.
And that’s just the beginning.
Our story

4 | 5
‘‘ ’’I met Dickson Mtanga, a community health worker, at
St. Gabriel’s Hospital in rural Malawi, where I was
volunteering. I learned more from him than anyone I’ve
ever met since, and he was a major inspiration for me to
start Medic Mobile.
This is an important moment in Medic Mobile’s journey. As we enter the next phase of our work, this
report allows us to reflect on and celebrate progress.
We have been learning and growing for years, guided by a clear mission to support community
health workers and families using mobile and web tools. The pillars of our model include our team,
technology, partnerships, and ethics, and these same components will stay with us as we scale.
One of my most important tasks has been to find and recruit smart, talented teammates as
we created our identity and strategy. My teammates at Medic Mobile spend ten hours
in vans on rough roads to visit remote clinics, code until developers in the next time
zone wake up, and work through the weekend to fine-tune models for calculating lives
saved. Their backgrounds and skills are diverse, but the commitment to our mission
is remarkably consistent across the team. They exhibit unique levels of patience,
empathy, and confidence, and they drive our work forward every day.
When we encounter gaps in the toolkit available for health workers and families,
our product team pays attention. We have a simple approach to technology
development: We only design new tools when they’re needed, and we design
for our users. We believe that the only way to unlock sustained impact is to
put users at the center of the whole process, solve real problems for people in
health systems, and create tools that people love to use.
We can only accomplish our mission at scale working with partners. Medic
Mobile is a unique organization in that we build tools but also approach
partnership discussions with a list of priority use cases. Today, we are focused
on antenatal care, postnatal care, childhood immunizations, infectious
disease surveillance, and stock monitoring for essential medicines. We are
constantly refining our answer to the question, “What’s the most important
use of mobile technology for my health system?” It is our job to proactively
find the right implementation partners.
As a focused, mission-driven, nonprofit organization, we are committed to
building the right tools and develop the right use cases for our users, partners,
and the communities we serve. Technology should be empowering rather
than intimidating. Learnings should be shared, not held tight as differentiating
business intelligence. Success and bright spots should be replicated and
scaled without unnecessary constraints. This is the Medic Mobile approach,
and we’re planning to bring it to 200,000 frontline health workers.
– Josh Nesbit
A letter from our
chief executive officer
MALAWI

6 | 7
2009
2010
2012
Our history A letter from
our boardIn every social justice organization, there is a tension between investing in long-term
change and acting on what Martin Luther King, Jr. called the fierce urgency of now. As
you read through this report, we hope it is clear that there is a profound immediacy to our
work. Spending time in the company of health workers and patients animates our team’s
urge to move quickly.
The boardroom, on the other hand, is a space to slow down, to think big, and to chart a
course for impact across a span of years and decades rather than a span of months. As
members of Medic Mobile’s board of directors, our voice is for the future.
While many charitable organizations compose large boards primarily of fundraisers,
our board is small and focused on active participation in the strategic direction of the
organization. Our expertise spans the fields of corporate law, venture capital, tech product
management, foundation-based philanthropy, and academia—all at fantastic institutions.
We meet five times a year, and individual board members often work one-on-one on
side projects with staff members. We demand that the staff run a tight ship and that many
options are on the table for every key decision. Ensuring that decisions are considered in
light of deep experience is an important part of our role. But we’re not afraid of taking risks.
At the end of the day, our work is about better decision-making, but it would be a mistake
to think of us as the sole deciders. We’re stewards of an environment where everyone can
trust that the best ideas will win.
To the staff at Medic Mobile and to our many health workers, funders, and other partners—
we’d like to congratulate you for your impressive achievements to date. We couldn’t be
more proud of you. But true to our purpose, we’d like to offer our voice for the future; the
most exciting impact is yet to come.
– Greg Ennis, Isaac Holeman, Susan Nesbitt, Amy Noris, Roni Zeiger
Josh Nesbit’s volunteer work at St. Gabriel’s Hospital in Malawi led to the
formation of Frontline SMS:Medic, which became Medic Mobile. We launched
our first project, providing mobile phones to community health workers in the
area around St. Gabriel’s. We launched Hope Phones to encourage people
to recycle their old phones, with proceeds funding the purchase of new phones
and solar chargers for community health workers.
Medic Mobile’s work expanded to ten countries in Africa,
Asia, Latin America, and the Caribbean. We also received
unrestricted grants totaling $200,000. We had a staff of four
and incorporated as a 501(c)(3) nonprofit organization.
We launched our first regional-scale programs in Africa and
received an additional $700,000 in grants. Our first SIM
application for feature phones was released, for which we
won an award from The Rockefeller Foundation. We worked
with 25 partners to serve one million people.
Medic Mobile conducted its first randomized controlled
studies. We opened a regional office in Nairobi and a
global team office in San Francisco. Our efforts covered two
million people.
2011
8 | 9
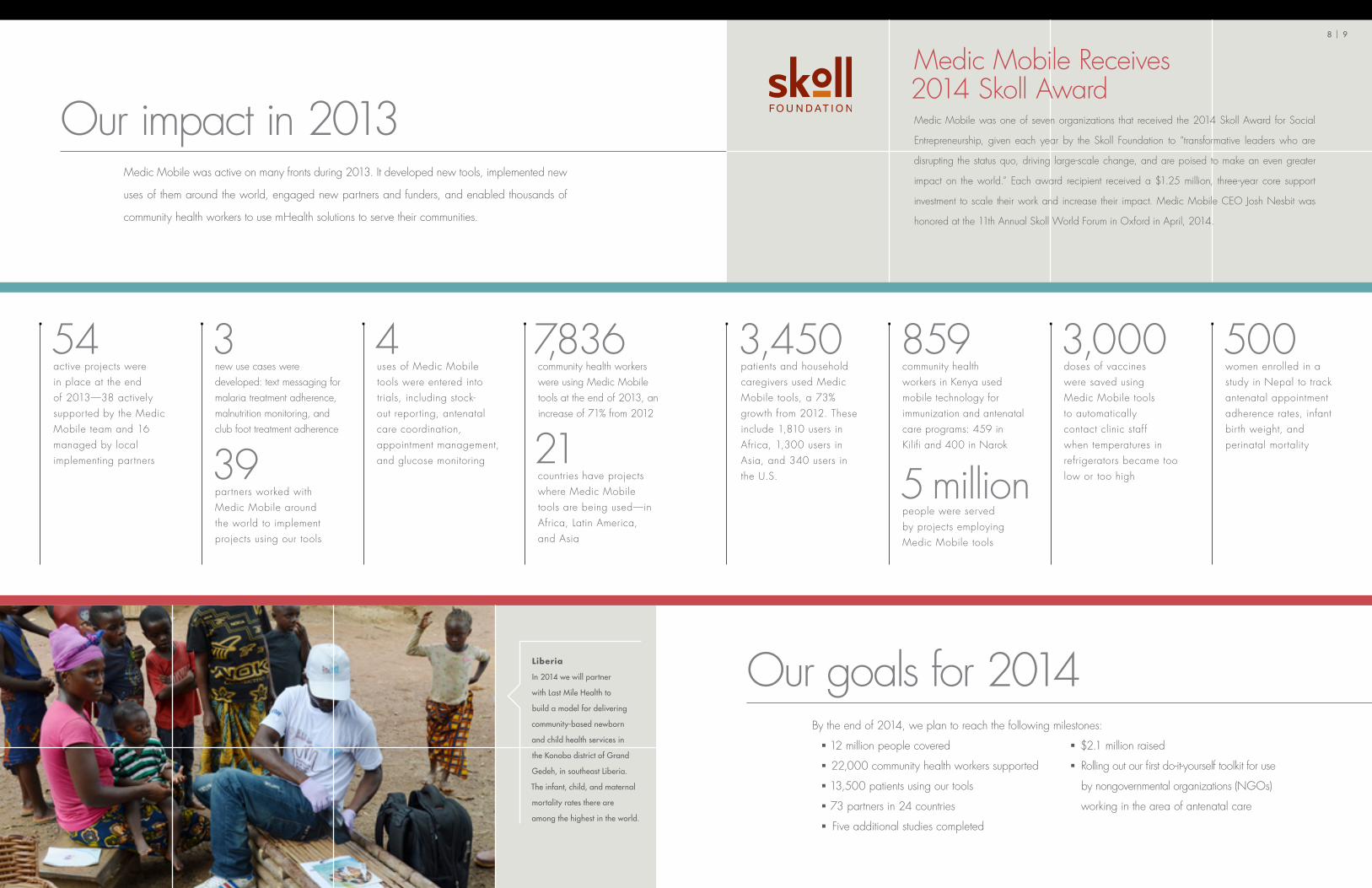
Medic Mobile Receives 2014 Skoll AwardMedic Mobile was one of seven organizations that received the 2014 Skoll Award for Social
Entrepreneurship, given each year by the Skoll Foundation to “transformative leaders who are
disrupting the status quo, driving large-scale change, and are poised to make an even greater
impact on the world.” Each award recipient received a $1.25 million, three-year core support
investment to scale their work and increase their impact. Medic Mobile CEO Josh Nesbit was
honored at the 11th Annual Skoll World Forum in Oxford in April, 2014.
Medic Mobile was active on many fronts during 2013. It developed new tools, implemented new
uses of them around the world, engaged new partners and funders, and enabled thousands of
community health workers to use mHealth solutions to serve their communities.
Our impact in 2013
54
39
3
21
4 7,836active projects were in place at the end of 2013—38 actively supported by the Medic Mobile team and 16 managed by local implementing partners
partners worked with Medic Mobile around the world to implement projects using our tools
new use cases were developed: text messaging for malaria treatment adherence, malnutrition monitoring, and club foot treatment adherence
countries have projects where Medic Mobile tools are being used—in Africa, Latin America, and Asia
uses of Medic Mobile tools were entered into trials, including stock-out reporting, antenatal care coordination, appointment management, and glucose monitoring
community health workers were using Medic Mobile tools at the end of 2013, an increase of 71% from 2012
5 million
3,450 859 3,000 500
people were served by projects employing Medic Mobile tools
patients and household caregivers used Medic Mobile tools, a 73% growth from 2012. These include 1,810 users in Africa, 1,300 users in Asia, and 340 users in the U.S.
community health workers in Kenya used mobile technology for immunization and antenatal care programs: 459 in Kilifi and 400 in Narok
doses of vaccines were saved using Medic Mobile tools to automatically contact clinic staff when temperatures in refrigerators became too low or too high
women enrolled in a study in Nepal to track antenatal appointment adherence rates, infant birth weight, and perinatal mortality
By the end of 2014, we plan to reach the following milestones:
� 12 million people covered
� 22,000 community health workers supported
� 13,500 patients using our tools
� 73 partners in 24 countries
� Five additional studies completed
� $2.1 million raised
� Rolling out our first do-it-yourself toolkit for use
by nongovernmental organizations (NGOs)
working in the area of antenatal care
Our goals for 2014Liberia
In 2014 we will partner
with Last Mile Health to
build a model for delivering
community-based newborn
and child health services in
the Konobo district of Grand
Gedeh, in southeast Liberia.
The infant, child, and maternal
mortality rates there are
among the highest in the world.

10 | 11
At Medic Mobile, we approach mHealth with the
understanding that its potential can be achieved
only when the people involved in healthcare
delivery have input at every stage of design
and implementation. They are at the center of
everything we do. Healthcare workers and others
will use our tools only if they see them as powerful
ways to improve the health of their communities.
We know that greater participation means greater
impact—and this sets the stage for greater scale.
At Medic Mobile, our work is grounded in human-
centered design. This means that our process
begins when we sit down with community health
workers, nurses, clinicians, and others who are
seeking ways to make their work more efficient,
effective, and able to reach more people.
Participants take part in role-playing and draw
sketches of current workflows. They learn about
each other’s daily lives and work, decision-making
processes, cultural traditions, experience with
technology, relationships, and what data they
collect, report, and analyze.
Everyone then brainstorms potential solutions
and new workflows, exploring ways that Medic
Mobile’s technology platform could lead to faster,
more personalized, more accurate, and often
less expensive ways of working. Additional role-
playing reveals how these tools could be used
and identifies possible barriers to implementation.
Medic Mobile developed a set of 50 “design
cards” for these sessions. They contain simple
drawings of various components of the healthcare
system: community members, healthcare workers,
places, technology, and actions involved—such
as visits to clinics. These cards are a visual and
tactile way to engage people in understanding
their work and imagining new ways of doing it.
This human-centered design approach continues
when Medic Mobile’s development team gets
involved. They work closely with people in the
field who test prototype solutions, give feedback,
and ultimately implement solutions.
While most solutions incorporate Medic Mobile’s
flexible, open-source software, we also—when
needed—develop new tools or incorporate ones
developed by others. The goal is always the right
tools for each project.
We don’t start with technology.
We start with people.
Medic Mobile’s human-
centered design process
starts with everyone
understanding each
other’s perspectives, then
goes through an iterative
process of brainstorming
possible solutions before
implementing them
and assessing their
effectiveness.
D E F I N E I D E A T E D E P L O Y M E A S U R E
O U R A P P R O A C H

12 | 13
‘‘ ’’I’m very pleased because in my heart I know that any time
I have problems, I have my community health worker, and she
can send a report to one of the proper doctors over there.
I feel looked after.
-- Janet Katana, Community Member
Maternal and infant death rates are notoriously high in many parts of the developing world. For example, in Kenya as a whole, there are 362 maternal deaths for every 100,000 births, and 72 infant deaths for every 1,000 births. In Kilifi, a farming and fishing community on the Kenyan coast, those rates are even higher.
Medic Mobile, working with Kilifi Kids and the Ministry of Health, is helping ensure the health of pregnant women and their newborns in that area with the use of mobile phones.
We worked in partnership with the Ministry of Health and Kilifi Kids to train over 450 community health workers in using cellphones to register women as soon as they became
pregnant. The goals of this effort were to encourage women to take advantage of Kilifi’s healthcare facilities and to ensure that the care they received met internationally accepted standards; these include four antenatal care (ANC) visits with a health professional and attendance at birth by a skilled professional, ideally in a clinic.
The health workers registered the expectant mother’s name, age, potential danger signs, and estimated due date and sent this information to a centralized database, hosted on computers at local clinics, using the Medic Mobile platform. Often, this visit from the health worker was the first time the family had any contact with the health system.
Medic Mobile’s system then scheduled appointments and sent automated text messages to the community health workers, prompting them to visit the homes of expectant mothers to tell them about their appointments. The health workers also used their phones to contact clinics when they observed danger signs, and the clinics informed them when someone should travel to a clinic to give birth.
These interventions had immediate benefits, including more than doubling the number of facility-based births, from 20 to 48 during the testing phase.
Studies showed that this effort also strengthened the ties, and trust, between community health workers and members of their community, improving the ways that health workers provided education and care before and after birth.
We are currently expanding our ANC work in Kilifi and in Nepal, where we are in a partnership with One Heart World-Wide.
The software package we developed for ANC will be available as a download free of charge through our website later in 2014. With this download, any health facility with some connectivity can use the Medic Mobile platform.
Taking care of
women and their babies
ANC
reminder
workflow
KEN
YAO U R I M PA C T
491,340
1,879
Bangladesh, Kenya, Nepal
Antenatal care
2014 – Q1
229
952
1879
Community health workers
2012Q4
2013Q4
2014Q1
500
1000
1500
2000
People covered
Communityhealth workers
Countries covered

‘‘ ’’The phone itself has brought big changes. Before it,
I had to write data in a book, then go by foot to the
woman in the medical clinic and speak to her.
Now I have this phone, it’s easy to do.
- Samu K Toi, Community Health Worker
It’s widely understood that the simplest and most effective way of preventing life-threatening diseases is to immunize infants against illnesses like measles, polio, diphtheria, and tuberculosis. However, according to the Centers for Disease Control, every 20 seconds, a child dies from a disease that could be prevented with a safe and effective vaccine. Millions more survive but are left severely disabled.
UNICEF reports that annually, over 22 million infants—mostly in Africa and Asia—do not receive all of their recommended vaccinations.
In Andhra Pradesh, a state in southern India, the overall rate for complete vaccination coverage was 67.1%, even though
vaccinations are provided free in public health facilities. Adherence was haphazard, people did not know about the importance of immunizations, and some believed they caused sterility.
In 2011, Medic Mobile—in partnership with DMF India, a local NGO that provides healthcare and operates an immunization center—developed a pilot project to use text messages to increase vaccination rates in Kurnool, a community in Andhra Pradesh. This intervention had the potential to send messages directly to new mothers because cellphone penetration in India is high: In 2011, over half of India’s population had a phone, with rapid growth since then.
DMF India volunteers and local nursing students visited the homes of pregnant women and recorded information—including their cellphone number and, later, the birth date of their child—and sent that to a centralized database.
The mothers then received automated text messages during their infant’s first year reminding them when their babies were due for vaccinations. These texts also contained information about caring for their newborns and the importance of immunizations.
As a result, the vaccination rate rose to 97% for the infants taking part in the trial who were eligible to receive their third dose.
The mothers also said that these messages motivated them to take greater personal responsibility for their child’s health beyond immunization—in part because they came from a local, trusted community organization.
Healthcare professionals quickly began to see other ways that SMS texting could be used, including having healthcare workers collect other data during home visits.
As a result of the success in India, Medic Mobile is expanding its immunization work into Nepal and Bangladesh.
Simple texts lead to
life-saving immunizations
Immunization
notifications
workflow
INDI
AO U R I M PA C T
140,000
1409
Bangladesh, India, Kenya,
Nepal
Childhood immunizat ions
2014 – Q1
Source: India controlled trial
67%
97%
Rate of complete vaccinations
People covered
Communityhealth workers
Countries covered
Before Medic Mobile interventions
AfterMedic Mobile interventions
14 | 15

16 | 17
‘‘ ’’You have a picture of what happened in all of the
facilities that you’re monitoring. Something that could take
you one month to analyze can actually be
done in a single day.
–Augustus Lugo, Acting District Disease Surveillance Coordinator, Kilifi County
Better reporting means better
diagnosis and treatmentIn places like rural Malawi, detecting, reporting, and treating illnesses can be daunting. In the region surrounding Namitete, in the western part of the country, 250,000 people are served by a single hospital, St. Gabriel’s, and for some it’s a 100-mile journey to get there. It’s also an area that has high rates of tuberculosis, HIV/AIDS, malaria, and a host of opportunistic infections.
Given long distances, poor roads, and paper-based and incomplete record-keeping, it can take weeks for health officials to receive information on outbreaks of disease. As a result, treatment is delayed and, in the case of contagious diseases, many others become ill.
In one of Medic Mobile’s first efforts to improve communication between community health workers and healthcare facilities, we provided mobile phones to 75 health workers in the area served by St. Gabriel’s.
The health workers used them to send and receive text messages regarding symptoms, referrals for treatment, medications and adherence, updates on patients’ health, and emergency situations.
A key outcome was that the community health workers were able to double the number of people who were found to have symptoms of tuberculosis and who were referred for treatment. In addition, traveling health specialists were able to identify
130 patients needing immediate attention for other illnesses as a result of accurate emergency calls.
Over the six months of this trial, 1,330 messages were sent, saving hospital staff over 2,048 hours of follow-up time and $3,000 in fuel.
In coastal Kenya, we worked with Kilifi Kids and the Ministry of Health to design and implement a program to improve the reporting of epidemic-prone diseases. Previously, nurses and clinic staff had traveled for many hours every week over dangerous roads in mini-buses or on the backs of motorbikes to hand-deliver paper
reports to the central referral hospital. In just the first year of this project, 97% of the required weekly reports were submitted on time, the highest rate in Kenya.
Plus, the Ministry of Health saved an estimated $56,000 and over 14,000 hours of clinical staff time.
Medic Mobile is also working on disease–reporting efforts in Senegal, in a partnership with IntraHealth, and in Nepal, where WHO, with funding from the Centers for Disease Control, is using the Medic Mobile platform to track outbreaks of disease, including polio.
Disease
tracking
workflow
MAL
AWI
O U R I M PA C T
Salima andNkhatabay districts
Kasungu district(control district)
Communication times*
300,400
2,330
9 minutesUsing mobile phones
24 hoursWithout mobile phones
28 hoursWithout mobile phones
Bangladesh, Cameroon, Kenya,
Malawi, Mali, Nepal, Senegal
Disease survei l lance
2014 – Q1
Source: K4Health Project
* Average time needed by a community health worker to submit a report and receive feedback
(includes travel time)
People covered
Communityhealth workers
Countries covered

18 | 19
A system to ensure the
availability of medications
MEX
ICO
People throughout the healthcare system are using the Medic Mobile platform to address a pressing challenge in developing countries: instances when medications are not available due to poor management of stocks.
These “stock-outs” often have life-threatening consequences. For example, a study by Oxfam found that in Malawi, only nine percent of local health facilities had a full complement of essential drugs, including antibiotics and vaccines.
Our efforts in Malawi have shown the effectiveness of tracking and maintaining inventories by having clinic staff send text messages to regional dispensaries when there are stock shortages. In a pilot study across ten districts, 80% of facilities with stock shortages
submitted reports, compared to 35% before the use of text messages. And the new system was 134 times faster and four times less expensive.
We are also working in Mexico with the Carlos Slim Health Institute and the Secretariat of Health to implement a nationwide stock monitoring program. In Mexico, there is little or no documentation of stock-outs, and patients often leave pharmacies empty-handed.
The Medic Mobile platform will be used by everyone who accesses, stocks, distributes, and monitors medications—with the overall goal of getting the right drug to the right place at the right time.
Patients can use mobile phones to notify ministries of health if local clinics have run out—ensuring greater accountability.
Clinics and pharmacies can send information to government agencies on a daily basis about dwindling supplies. This data can then be aggregated and displayed on easy-to-read dashboards, providing information that can be used to restock drugs more quickly (often from nearby clinics) and improve forecasting to avoid future stock-outs.
Improving vaccine managementVaccines must be stored at a consistent temperature in order to be effective. This requires a reliable cold chain—which includes refrigeration units at local clinics and hospitals, where power outages are common.
In Kenya, Medic Mobile partnered with Nexleaf Analytics to monitor the temperature of stored vaccines. A remote sensor, developed by Nexleaf, plugs into the headphone jack of a mobile phone. Whenever a refrigerator goes outside the required temperature range, the phone sends an SMS alert to local clinic staff so they can take immediate action.
During a one-month trial, 3,000 doses of vaccines were monitored at eight clinics. By the end of 2014, Medic Mobile’s alert system will be in place at nearly 280 additional clinics in Kenya, where vaccine supplies for two million people will be monitored.
‘‘ ’’Before this system, I would sleep very bad. Nights
I would not know if the vaccines were okay. Now,
I receive an alert, and I fly out of bed to fix the fridge.
I sleep like I know everything is okay.
–Sharlet Anzazi, a nurse at Mnarani Health Center in Kenya
This prototype dashboard shows the kind of information that will be available to state and national ministries of health in Mexico.
It includes reporting rates by clinics within each state, daily stock-out reports, the number of patients affected, and monthly
tracking by medication — which can be used to anticipate future shortages.
O U R I M PA C T
Drug stock
monitoring
workflow
902,000
80,000
3,776
3,000
10( Kenya )
Cameroon, Kenya, Malawi, Mali,
Mexico, Senegal
Drug stock monitoring
Cold chain monitoring
2014 – Q1
Partner: Nextleaf Analytics
People covered
People covered
Vaccines monitored
Communityhealth workers
Clinics covered
Countries covered

20 | 21
We’re using mobile technology to reimagine the way people receive care.
The Medic Mobile platformMedic Mobile believes that technology should increase justice and improve equity. As a result, our solutions need to work on technology that is inexpensive, easy to use, and readily available. Plus, we are committed to free, open-source platforms that can be adapted for specific uses, with—over time—no support needed from us. This means that we design solutions with scalability in mind.
The Medic Mobile platform runs on multiple devices—including feature phones, smartphones, tablets, and desktop computers—making it possible for people throughout the healthcare system to use it.
Patients and community health workers use inexpensive feature phones to collect structured data that they can submit as a simple text message (SMS) to a centralized computer or laptop at a clinic, Ministry of Health, hospital, or NGO. Healthcare workers also use their phones to place direct calls in order to receive help in caring for community members.
Data can be sent through a variety of SMS formats, including simple text messages sent from the phones community health workers already have. Users can also install Medic Mobile for feature phones via a small parallel SIM—a small wafer that slides under a phone’s existing SIM card—so that any GSM phone can run the Medic Mobile app. This makes it possible to register new pregnancies and births, schedule appointment reminders, and perform other tasks.
Medic Mobile for desktop lives on a computer or laptop in a clinic or ministry of health. In this setting, it acts as a flexible, scalable information and communication center, without requiring a connection to the Internet or remote server. Medic Mobile stores data received from community health workers, manages contacts, sends automated messages to individual or multiple recipients, and automatically schedules appointments, among other functions.
Medic Mobile for desktop provides real-time access to community data, enabling faster communication and more targeted support to patients and communities. Data can be entered via SMS, smartphones, or through a web-based interface. The platform is optimized to support a variety of uses and can easily be adapted to support other mHealth needs.
Medic Mobile also provides a powerful analytics feature that health officials can use as a dashboard to visualize their data. This feature can be used by district healthcare workers or ministries of health to track operational progress, measure impact, see trends, and make decisions based on accurate, real-time data. It can be accessed from laptops, netbooks, tablets, and smartphones. It is cloud-hosted and works seamlessly with our mobile field reporting tools.
The Mobile Medic platform
on feature phones enables
patients and community
health workers to collect
structured data and submit
it as a simple text message
to a centralized computer or
laptop at a clinic, hospital,
or NGO.
While all Medic Mobile
applications designed for
feature phones work on
smartphones, we are
exploring new ways that
smartphones can extend the
capabilities of mHealth—for
example, by using web-
based applications,
geolocation data, and photos.
Medic Mobile for desktops
lives on a computer or laptop
in a clinic or ministry of
health. It is a flexible,
scalable information and
communication center that
aggregates data, sends
messages to community
health workers and patients,
and schedules appointments.
Medic Mobile also provides
a powerful analytics feature
that analyzes data and
visualizes it in useful ways
for health officials (e.g.,
monitoring stocks of
medications, using both maps
and graphs). Shown here is a
prototype view of stock
monitoring data from Mexico.
O U R T O O L S
22 | 23
Medic Mobile collaborates with partners at all levels of the healthcare system—including community health workers, NGOs, community clinics and hospitals, ministries of health, and international agencies.
Our partners put our tools to work to enhance their ongoing programs and develop new ones, they help ensure that implementation goes to scale, they give us feedback to improve our solutions, and they evaluate the effectiveness of these interventions.
We work with partners in various ways. For example, we help NGOs that are just beginning to explore the potential of mHealth tools in their work. And we help other NGOs that are ready to partner with us on specific efforts to expand their impact.
We also partner with regional and national ministries of health, as well as international organizations like USAID, to look at overall systems of care, analyze needs and available assets, conduct human-centered design workshops, and make recommendations about bringing mHealth solutions to programs throughout the world.
As a nonprofit, Medic Mobile considers its bottom line the impact of our tools on the health of people who live in underserved communities around the world.
As a result, we take a rigorous approach to monitoring and evaluating our interventions and work closely with our partners to measure our programs’ impact. This research enables us to refine our tools and how they’re being used. It helps partners and potential partners see the impact of these solutions. And, more broadly, it helps establish models for how mHealth can radically change how healthcare is delivered in developing countries.
We measure efficiency (the time and money saved using our tools), adherence (e.g., the number of pregnant women completing all of their ANC visits, and the number of infants receiving full coverage of immunizations), reach (e.g., the number of community health workers using our tools to serve their communities, and the number of pregnant women enrolled in care), and quality of care (e.g., the reduction of stock-outs and improvements in the active management of disease).
Increasingly, we are using randomized controlled trials to assess health outcomes, comparing the impact of Medic Mobile solutions to traditional means of delivering care. The results of these trials will be available in 2014.
Core operations
Jeannette Cox, Head Accountant
Jacqueline Edwards, Director of Partnerships
Kaylor Garcia, Media Associate
Katie Kelly, Director of Communications
Josh Nesbit, Chief Executive Officer
Blair Palmer, Hope Phones Campaign
Director
Design and Products
Marc Abbyad, Product Manager
Milan Andric, Senior Web Developer
Gareth Bowen, Senior Web Developer
David Brown, Chief Technology Officer
Rowan Crawford, Senior Web Developer
Dianna Kane, Senior Designer
Caolan McMahon, Alumnus and Open-
source Contributor
Ryan Ramage, Senior Web Developer
Regional Teams
Shreya Bhatt, India Program Manager
Jay Evans, Asia Regional Director
Cheikh Tidiane Kane, Project Manager
Jane Katanu, Project Manager
Humphrey Mwaura, Project Manager
Enock Musyoka, Project Manager
Regina Mutuku, Project Manager
Maeghan Orton, Africa Regional Director
Ranju Sharma, Nepal Project Manager
Gabriela Vanegas, Project Manager
Zack Wettstein, Project Manager
Amanda Yembrick, Analytics Manager/
Regional Manager, Latin America and
the Caribbean
Research Group
Alex Harsha, Researcher
Isaac Holeman, Researcher and Board
Member
Nadim Mahmud, Researcher
Board of Directors
Amy Norris, Chief Legal Counsel,
Clif Bar & Company
Greg Ennis, Managing Director,
Peninsula Ventures
Isaac Holeman, Cofounder of Medic
Mobile, Gates Cambridge Scholar
Josh Nesbit, CEO, Medic Mobile
Roni Zeiger, CEO, Smart Patients & former
Chief Health Strategist, Google
Susan Nesbitt, Independent Consultant
& former Deputy Director,
Craigslist Foundation
Africa
African Projects Coordination Agency
(APCA), Kenya
Bushenyi Medical Center, Uganda
Children of Blessing Trust, Malawi
Christian Aid, Kenya
HealthRight International, Kenya
IntraHealth, Senegal
Johns Hopkins Bloomberg School of Public
Health Center for Communication
Programs, Malawi
Lighthouse (Kamuzu Central Hospital),
Malawi
KEMRI-Wellcome, Kenya
Kabwohe Clinical Research Center, Uganda
Kilifi Kids, Kenya
Knowledge for Health (K4Health), Malawi
Last Mile Health, Liberia
Makueni District Ministry of Health, Kenya
Mali Health Organizing Project (MHOP),
Mali
Management Sciences for Health, Malawi
and Nigeria
Marie Stopes International, Kenya
PeaceTXT, Kenya
Plan International, Kenya
Population Services International,
Cameroon and Mali
Resolve Network, Democratic Republic of
the Congo
St. Gabriel’s Hospital, Malawi
United Nations Population Fund, Mali
Asia
Centers for Disease Control and Prevention
and WHO, Nepal
DMF (Developmental Medical Foundation)
India, India
Hope Foundation, Bangladesh
miraclefeet, India
One Heart World-Wide, Nepal
Possible, Nepal
Latin America
Becton, Dickinson and Company, Panama
Carlos Slim Health Institute, Mexico
Children in Crisis (Stanford), Guatemala
Global Healing, Honduras
MASS Design, Haiti
Mission 4636, Haiti
United States
Cure Violence, IL
San Mateo Medical Center, CA
Stanford Hospital, CA
O U R P E O P L E
With Medic Mobile tools, our partners are saving time, money – and lives.
Our bottom line is making an impact.
O U R R E S E A R C HO U R PA R T N E R S

100 200 300 400 500 600 700 8000
83%
17%
82%
3%
9%
6%
2000 400 600 800 1,000
24 | 25
Medic Mobile is grateful for the generous support of our funders, whose support of our vision means that people
throughout the world can benefit from mobile technology to receive critically important medical care.
Rita Allen Foundation
Ashoka
Clif Bar & Company
Coatue Foundation
Compton Foundation
Nancy Cooley
Echoing Green
EcoPhones
The Elmo Foundation
The Greenbaum Foundation
Haas Center for Public Service
Jill Iscol
Jasmine Social Investments
McKesson Foundation
The Maternal Health Task Force
Mozilla
The Mulago Foundation
Omakase Charity
Al and Nancy Osborne
The Peery Foundation
Philanthropic Ventures Foundation
PopTech
Segal Family Foundation
Skoll Foundation
Stanford Center for Innovation in
Global Health
Donald A. Strauss Foundation
SV2
UN Foundation
The Wireless Source
Profit & loss statement
O U R F U N D E R SO U R F I N A N C I A L S
H O P E P H O N E S
Your used cellphones can help Medic Mobile earn funds to purchase new phones for community health workers in the developing world. Under our Hope Phones initiative, Medic Mobile partners with a certified recycler to ensure that data is erased and that the phones are responsibly recycled or reused. For every phone you donate, we get a payment from the recycler, which we use to purchase inexpensive feature phones that support the Medic Mobile platform.
And, we provide a tax deduction for larger donations. If Hope Phones can recycle just 1% of disposed phones each year, we can outfit one million health workers, improving the lives of 50 million people.
To learn more about donating your used phones and taking part in our corporate donation program, visit:
Hope Phones, One Heart World-Wide, and Samahope (one of the leading
suppliers of medical treatment to women and children in developing areas) are
working together to bring safe births to 11,000 women in the Dhading district
of Nepal. For every phone donated, Hope Phones equips ten female community
health volunteers with feature phones, better enabling them to care for the
pregnant women in their community.
Assets
Current Assets 321,947
Other Assets 3,805
Total Assets: 325,752
Liabilities & Net Assets
Current Liabilities 48,726
Net Assets 277,026
Total Liabilities & Net Assets 325,752
Revenue (%)
Foundations, Corporate Grants
Contracts
Government Grants
Other
Expenses (%)
Program Services
Support Services
Revenue (US$)
Foundations, Corporate Grants 799,880
Contracts 90,006
Government Grants 29,228
Other 62,615
Total 981,729
Expenses
Program Services 856,802
Support Services 178,623
Total 1,035,425
Net Income (53,696)
Medic Mobile, Inc. is a non profit 501(c)(3) company. Year ending December 31
( In thousands )
Your used phones can expand Medic Mobile’s work
2012
Balance sheet
hopephones.org

Become a partner
Recycle your used cellphoneshopephones.org
Make a donationrally.org/medic/donate
Purchase our design cardsmedicmobile.org/design-cards
Download our toolkitgithub.com/medic
Contact or follow usMedic Mobile’s mission is to improve healthcare in
under served communities using mobile technologies. [email protected]
twitter.com/medic facebook.com/MedicMobile
To help us further our mission

This annual report was made possible through a grant from the Taproot Foundation.
© 2014 Medic Mobile
Photos: Gabriel Diamond (Skoll Foundation), Lewis Feuer, Dianna Kane, Katie Kelly, Josh Nesbit, Lester Ng, Maeghan Orton
Medic Mobile36 Clyde Street San Francisco, CA 94107+1 (415) 746-9758medicmobile.org
twitter.com/medic
facebook.com/MedicMobile