mi time course of denervation of efferent sympathetic and...
TRANSCRIPT

m i
Time Course of Denervation of EfferentSympathetic and Vagal Nerves After Occlusion
of the Coronary Artery in the Canine Heart
Hiroshi Inoue and Douglas P. Zipes
To determine the time course of efferent sympathetic denervation after transmural myocardialinfarction (TMI) and of efferent vagal denervation after transmural or nontransmural myocardialinfarction (NTMI), we measured effective refractory periods (ERP) basal and apical to TMI or NTMIin secobarbital-anesthetized, open-chest dogs. In eight dogs with Latex-induced TMI, bilateral ansaesubclaviae stimulation shortened ERP at all 45 apical and basal test sites before latex injection. Afterlatex injection, ERP shortening was unchanged at all 15 basal sites but was eliminated ( s2 msecshortening) at three apical sites in 5-20 minutes and at 14 of 30 apical sites 30-180 minutes after latexinjection. At the remaining 13 apical sites, ERP shortening was not eliminated but attenuated signifi-cantly in 5-180 minutes. ERP shortening induced by infused norepinephrine (0.20-0.25 /xg/kg/min)did not differ between basal and apical test sites 3-4 hours after latex injection; that is, no supersensi-tivity occurred. Of six dogs with TMI produced by ligation of multiple coronary arteries without latexinjection, ERP shortening induced by efferent sympathetic neural stimulation was eliminated at 10apical sites in four dogs over a period of 3 hours. At 14 apical sites that did not show denervation inthese six dogs, ERP shortening was unchanged. In seven dogs with latex-induced TMI, bilateral vagalstimulation lengthened ERP at all 40 apical and basal test sites before latex injection. Vagally inducedERP lengthening was unchanged at all 13 basal sites after latex injection. ERP lengthening waseliminated (£ l msec lengthening) at four of 27 apical sites in 5-20 minutes and at 13 apical sites30-180 minutes after latex injection. At the remaining 10 apical sites, ERP lengthening was noteliminated but decreased significantly 3 hours after latex injection. Of nine dogs with ligation-inducedNTMI, five dogs showed elimination of vagal ly induced ERP lengthening at eight apical sites in 3 hoursafter ligation. ERP lengthening induced by vagal stimulation was unchanged at all 17 basal sites innine dogs with NTMI. We conclude that TMI produced by latex injection and ligation of multiplecoronary arteries produces heterogeneous loss of efferent sympathetic innervation in noninfarctedapical sites as early as 5-20 minutes after coronary occlusion with more complete denervation occur-ring over time. Loss of efferent vagal innervation also occurs heterogeneously in 5-20 minutes aftercoronary occlusion by latex injection (TMI) and by ligation of a diagonal branch (NTMI) andcontinues with more sites losing efferent responsiveness over time. (Circulation Research 1988;62:1111-1120)
Transmural myocardial infarction induced bylatex injection into a diagonal branch of theleft anterior descending coronary artery in the
dog heart interrupts efferent sympathetic fibers inner-vating the myocardium apical to the infarction by 90minutes.1 Efferent vagal fibers are also interrupted bytransmural myocardial infarction induced by latexinjection into a diagonal branch 90 minutes after emboT
lization2 and by nontransmural myocardial infarctioninduced by ligation of the left anterior descendingcoronary artery followed by reperfusion in caninehearts.3 Nontransmural myocardial infarction follow-ing ligation of a coronary artery spares the epicardium
From the Krannert Institute of Cardiology, Indiana UniversitySchool of Medicine, Indianapolis, Indiana.
Supported in part by the Herman C. Krannert Fund; by grantsHL-06308 and HL-07182 from the National Heart, Lung, andBlood Institute of the National Institutes of Health, Bethesda,Maryland; and by the American Heart Association, IndianaAffiliate.
Address for correspondence: Douglas P. Zipes, MD, KrannertInstitute of Cardiology, 1001 West 10th Street, Indianapolis, IN46202.
Received August 11, 1987; accepted January 12, 1988.
and does not result in sympathetic denervation.4 De-spite these studies, little is known about how quicklyefferent sympathetic and vagal denervation occur aftercoronary occlusion. If denervation occurred at the on-set of ischemia and was heterogeneous, it might con-tribute to the genesis of ventricular arrhythmias duringthe acute stage of myocardial infarction.
The purpose of the present study was to determinethe time course of loss of efferent sympathetic andvagal innervation in noninfarcted, normal myocardiumapical to an infarction produced by latex injection orligature occlusion of a coronary artery in the canineheart.
Materials and MethodsMongrel dogs of either sex weighing 14-29 kg were
anesthetized with sodium secobarbital (30 mg/kg i.v.).Additional amounts of secobarbital were injected asneeded to maintain anesthesia. The dog was intubatedand ventilated with room air using a volume-cycledrespirator (model 607, Harvard Apparatus, South Na-tick, Massachusetts). The chest was opened through amedian sternotomy, and the heart was suspended in apericardia! cradle. A fluid-filled cannula placed in the
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from
1112 Circulation Research Vol 62, No 6, June 1988
femoral artery was connected to a Statham P23 IDtransducer (Gould, Cleveland, Ohio) to monitor arteri-al blood pressure, and a femoral venous cannula wasused to infuse normal saline at 100-200 ml/hr to re-place spontaneous fluid losses. The dog was placed ona heating pad, and the thoracotomy was covered by aplastic sheet. An operating table lamp was used tomaintain epicardial temperature between 37° and 39°C. Arterial blood gases and pH were monitored andmaintained within the physiological range.14
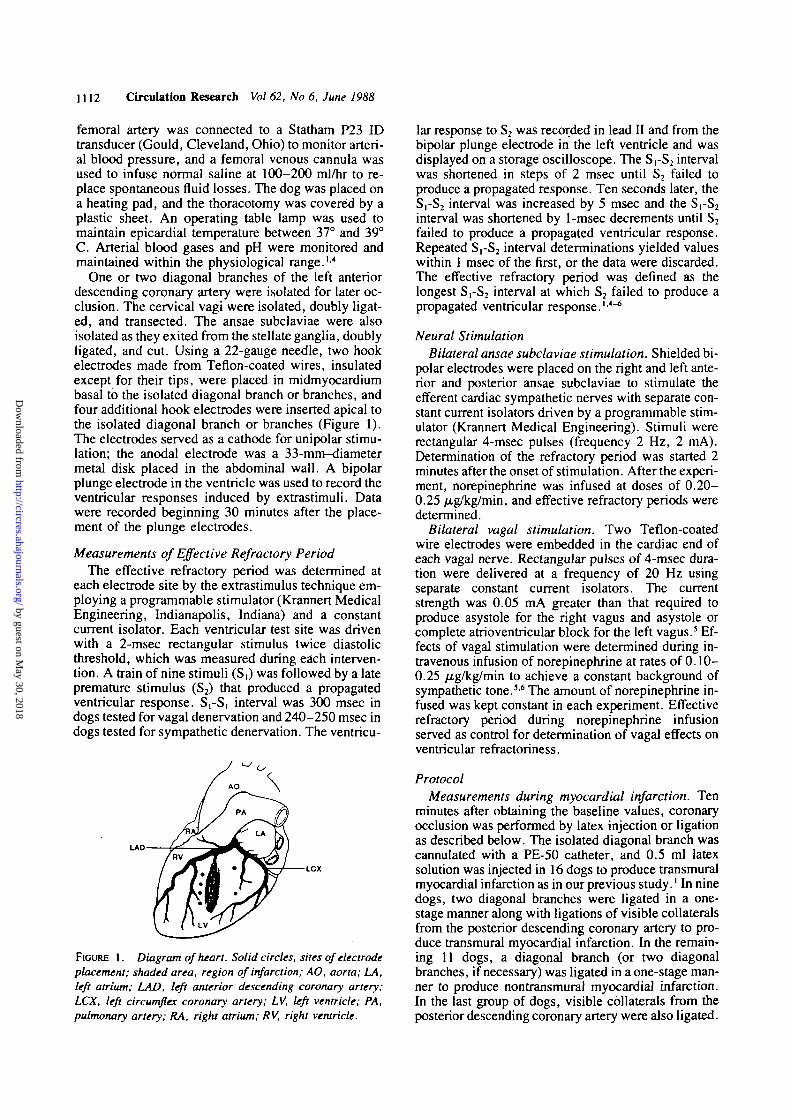
One or two diagonal branches of the left anteriordescending coronary artery were isolated for later oc-clusion. The cervical vagi were isolated, doubly ligat-ed, and transected. The ansae subclaviae were alsoisolated as they exited from the stellate ganglia, doublyligated, and cut. Using a 22-gauge needle, two hookelectrodes made from Teflon-coated wires, insulatedexcept for their tips, were placed in midmyocardiumbasal to the isolated diagonal branch or branches, andfour additional hook electrodes were inserted apical tothe isolated diagonal branch or branches (Figure 1).The electrodes served as a cathode for unipolar stimu-lation; the anodal electrode was a 33-mm-diametermetal disk placed in the abdominal wall. A bipolarplunge electrode in the ventricle was used to record theventricular responses induced by extrastimuli. Datawere recorded beginning 30 minutes after the place-ment of the plunge electrodes.
Measurements of Effective Refractory PeriodThe effective refractory period was determined at
each electrode site by the extrastimulus technique em-ploying a programmable stimulator (Krannert MedicalEngineering, Indianapolis, Indiana) and a constantcurrent isolator. Each ventricular test site was drivenwith a 2-msec rectangular stimulus twice diastolicthreshold, which was measured during each interven-tion. A train of nine stimuli (S,) was followed by a latepremature stimulus (S2) that produced a propagatedventricular response. S,-S, interval was 300 msec indogs tested for vagal denervation and 240-250 msec indogs tested for sympathetic denervation. The ventricu-
LAD
LCX
FIGURE 1. Diagram of heart. Solid circles, sites of electrodeplacement; shaded area, region of infarction; AO, aorta; LA,left atrium; LAD, left anterior descending coronary artery;LCX, left circumflex coronary artery; LV, left ventricle; PA,pulmonary artery; RA, right atrium; RV, right ventricle.
lar response to S2 was recorded in lead II and from thebipolar plunge electrode in the left ventricle and wasdisplayed on a storage oscilloscope. The S,-S2 intervalwas shortened in steps of 2 msec until S2 failed toproduce a propagated response. Ten seconds later, theS,-S2 interval was increased by 5 msec and the S,-S2interval was shortened by 1 -msec decrements until S2failed to produce a propagated ventricular response.Repeated S,-S2 interval determinations yielded valueswithin 1 msec of the first, or the data were discarded.The effective refractory period was defined as thelongest SrS2 interval at which S2 failed to produce apropagated ventricular response.14"6
Neural StimulationBilateral ansae subclaviae stimulation. Shielded bi-
polar electrodes were placed on the right and left ante-rior and posterior ansae subclaviae to stimulate theefferent cardiac sympathetic nerves with separate con-stant current isolators driven by a programmable stim-ulator (Krannert Medical Engineering). Stimuli wererectangular 4-msec pulses (frequency 2 Hz, 2 mA).Determination of the refractory period was started 2minutes after the onset of stimulation. After the experi-ment, norepinephrine was infused at doses of 0.20-0.25 /xg/kg/min, and effective refractory periods weredetermined.
Bilateral vagal stimulation. Two Teflon-coatedwire electrodes were embedded in the cardiac end ofeach vagal nerve. Rectangular pulses of 4-msec dura-tion were delivered at a frequency of 20 Hz usingseparate constant current isolators. The currentstrength was 0.05 mA greater than that required toproduce asystole for the right vagus and asystole orcomplete atrioventricular block for the left vagus.5 Ef-fects of vagal stimulation were determined during in-travenous infusion of norepinephrine at rates of 0.10-0.25 /ig/kg/min to achieve a constant background ofsympathetic tone.36 The amount of norepinephrine in-fused was kept constant in each experiment. Effectiverefractory period during norepinephrine infusionserved as control for determination of vagal effects onventricular refractoriness.
ProtocolMeasurements during myocardial infarction. Ten
minutes after obtaining the baseline values, coronaryocclusion was performed by latex injection or ligationas described below. The isolated diagonal branch wascannulated with a PE-50 catheter, and 0.5 ml latexsolution was injected in 16 dogs to produce transmuralmyocardial infarction as in our previous study.' In ninedogs, two diagonal branches were ligated in a one-stage manner along with ligations of visible collateralsfrom the posterior descending coronary artery to pro-duce transmural myocardial infarction. In the remain-ing 11 dogs, a diagonal branch (or two diagonalbranches, if necessary) was ligated in a one-stage man-ner to produce nontransmural myocardiaJ infarction.In the last group of dogs, visible collaterals from theposterior descending coronary artery were also ligated.
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from
Inoue and Zipes Time Course of Ischemia-Induced Efferent Neural Denervation 1113
Refractory periods were determined at 5, 30, 60, 120,and 180 minutes after coronary occlusion. Because ittook about 15 minutes to determine the effective re-fractory period at six test sites both before and duringneural stimulation, the data presented at 5 minutesafter coronary occlusion, for example, were collectedfrom 5 to about 20 minutes after coronary occlusion.
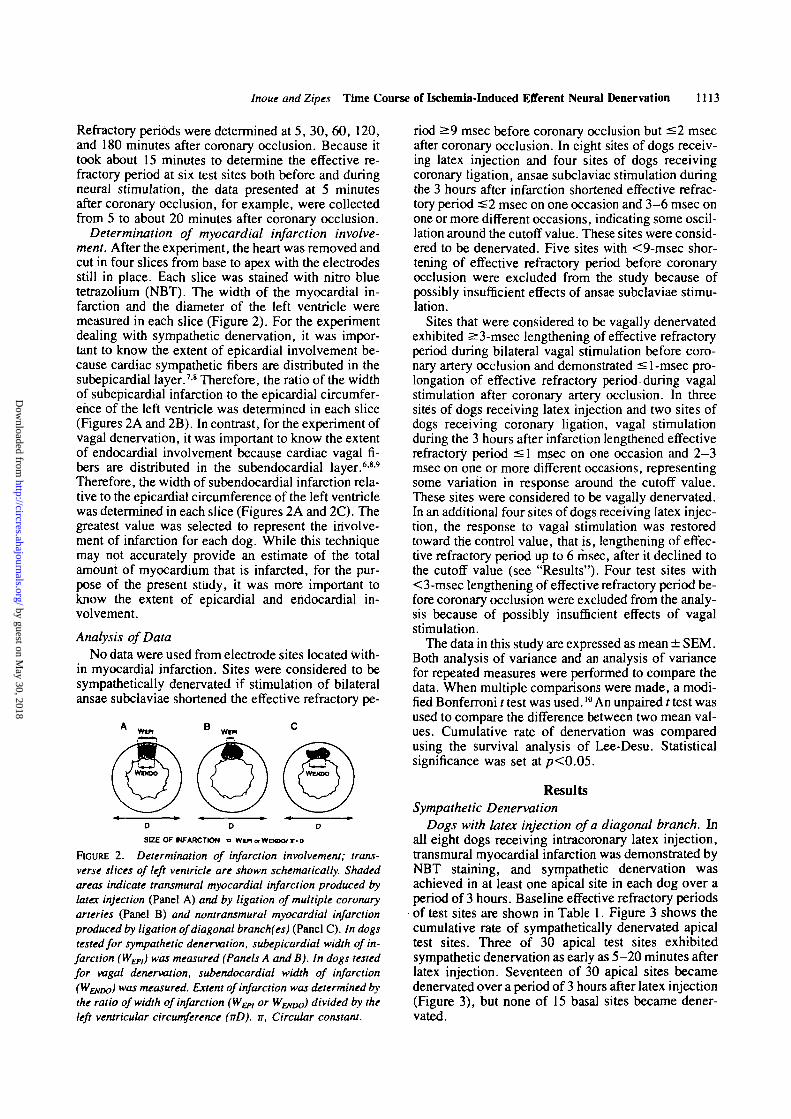
Determination of myocardial infarction involve-ment. After the experiment, the heart was removed andcut in four slices from base to apex with the electrodesstill in place. Each slice was stained with nitro bluetetrazolium (NBT). The width of the myocardial in-farction and the diameter of the left ventricle weremeasured in each slice (Figure 2). For the experimentdealing with sympathetic denervation, it was impor-tant to know the extent of epicardial involvement be-cause cardiac sympathetic fibers are distributed in thesubepicardial layer.78 Therefore, the ratio of the widthof subepicardial infarction to the epicardial circumfer-ence of the left ventricle was determined in each slice(Figures 2A and 2B). In contrast, for the experiment ofVagal denervation, it was important to know the extentof endocardial involvement because cardiac vagal fi-bers are distributed in the subendocardial layer.689
Therefore, the width of subendocardial infarction rela-tive to the epicardial circumference of the left ventriclewas determined in each slice (Figures 2A and 2C). Thegreatest value was selected to represent the involve-ment of infarction for each dog. While this techniquemay not accurately provide an estimate of the totalamount of myocardium that is infarcted, for the pur-pose of the present study, it was more important toknow the extent of epicardial and endocardial in-volvement.
Analysis of DataNo data were used from electrode sites located with-
in myocardial infarction. Sites were considered to besympathetically denervated if stimulation of bilateralansae subclaviae shortened the effective refractory pe-
D 0 O
SIZE OF NFARCTION a Wen orWEHXV r-0
FIGURE 2. Determination of infarction involvement; trans-verse slices of left ventricle are shown schematically. Shadedareas indicate transmural myocardial infarction produced bylatex injection (Panel A) and by ligation of multiple coronaryarteries (Panel B) and nontransmural myocardial infarctionproduced by ligation of diagonal branch(es) (Panel C). In dogstested for sympathetic denervation, subepicardial width of in-farction (W&,,) was measured (Panels A and B). In dogs testedfor vagal denervation, subendocardial width of infarctionV^ENDO) was measured. Extent of infarction was determined bythe ratio of width of infarction (WEPI or Wp/Do) divided by theleft ventricular circumference (nD). IT, Circular constant.
riod ̂ 9 msec before coronary occlusion but ^ 2 msecafter coronary occlusion. In eight sites of dogs receiv-ing latex injection and four sites of dogs receivingcoronary ligation, ansae subclaviae stimulation duringthe 3 hours after infarction shortened effective refrac-tory period ^2 msec on one occasion and 3-6 msec onone or more different occasions, indicating some oscil-lation around the cutoff value. These sites were consid-ered to be denervated. Five sites with <9-msec shor-tening of effective refractory period before coronaryocclusion were excluded from the study because ofpossibly insufficient effects of ansae subclaviae stimu-lation.
Sites that were considered to be vagally denervatedexhibited s3-msec lengthening of effective refractoryperiod during bilateral vagal stimulation before coro-nary artery occlusion and demonstrated <l-msec pro-longation of effective refractory period during vagalstimulation after coronary artery occlusion. In threesites of dogs receiving latex injection and two sites ofdogs receiving coronary ligation, vagal stimulationduring the 3 hours after infarction lengthened effectiverefractory period ^1 msec on one occasion and 2-3msec on one or more different occasions, representingsome variation in response around the cutoff value.These sites were considered to be vagally denervated.In an additional four sites of dogs receiving latex injec-tion, the response to vagal stimulation was restoredtoward the control value, that is, lengthening of effec-tive refractory period up to 6 msec, after it declined tothe cutoff value (see "Results")- Four test sites with< 3-msec lengthening of effective refractory period be-fore coronary occlusion were excluded from the analy-sis because of possibly insufficient effects of vagalstimulation.
The data in this study are expressed as mean ± SEM.Both analysis of variance and an analysis of variancefor repeated measures were performed to compare thedata. When multiple comparisons were made, a modi-fied Bonferroni t test was used.10 An unpaired t test wasused to compare the difference between two mean val-ues. Cumulative rate of denervation was comparedusing the survival analysis of Lee-Desu. Statisticalsignificance was set at / J < 0 . 0 5 .
ResultsSympathetic Denervation
Dogs with latex injection of a diagonal branch. Inall eight dogs receiving intracoronary latex injection,transmural myocardial infarction was demonstrated byNBT staining, and sympathetic denervation wasachieved in at least one apical site in each dog over aperiod of 3 hours. Baseline effective refractory periods
• of test sites are shown in Table 1. Figure 3 shows thecumulative rate of sympathetically denervated apicaltest sites. Three of 30 apical test sites exhibitedsympathetic denervation as early as 5-20 minutes afterlatex injection. Seventeen of 30 apical sites becamedenervated over a period of 3 hours after latex injection(Figure 3), but none of 15 basal sites became dener-vated.
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

1114 Circulation Research Vol 62, No 6, June 1988
TABLE 1. Baseline Effective Refractory Period In Dogs Tested for Sympathetic Denervation
/. Eight dogs with transmural myocardial infarction from latex injection of coronary artery
Beforecoronaryocclusion
After coronary occlusion (minutes)
30 60 120 180
Basal sites (n = 15) 169±2 173±2 173±2 174±3
Apical sites without denervation (n = 13) 172±3 172±2 172±3 171 ±3
Apical sites with denervation (n = 17) 170±2 168±2 169±2 169±2
176±2 176±3
172 + 2 173 + 3
168±2 172±2
//. Six dogs with transmural myocardial infarction from ligation of multiple coronary arteries
Beforecoronaryocclusion
After coronary occlusion (minutes)
30 60 120 180
Basal sites (n= 12) 163 + 2 162 + 3* 163±2 162 + 2
Apical sites without denervation (n= 14) 163±1 162 + 2 162±1 161 ±2
Apical sites with denervation (n= 10) 172±3 162±4t 164±2 161 ±3
163 + 2 164 + 2
164 + 1 165+1
162±3 163±3*n= 10, tn = 6 (see text for details).Values are mean±SEM in milliseconds.
When the data of these 17 denervated sites werepooled, shortening of effective refractory period de-clined progressively after latex injection (Figure 4). Atthe remaining 13 apical sites without apparent dener-vation (i.e., effective refractory period still shortened
SYMPATHETIC
00
80
60
40
20
n
5(3)
DENERVATION
7(7)'7 74)
_[1
LATEX (NLIOATION
3(11)
»30)(N.24. .20
17(12)
10 (61
C 5 30 60 120 ISOmln
FIGURE 3. Plot showing cumulative percentage of sympatheti-cally denervated apical sites divided by number of total apicaltest sites (N) is shown on ordinate as function of time. Solid line,data from dogs with latex injection; dotted line, data from dogswith coronary ligation; figures without parentheses, cumulativenumber of denervated test sites (total number of sites that hadshown shortening of effective refractory period s 2 msec at leastonce by that moment of determination); figures in parentheses,number of test sites that showed shortening of effective refrac-tory period s2 msec at that moment of determination. Presenta-tion in this fashion is necessary because some sites showedvariation in response around the cutoff value (see text). Forexample, 120-180 minutes after latex injection, four new sites(17 minus 13) became denervated, while only 12 of the 17 sitesactually still exhibited shortening of effective refractory period^ 2 msec at 180 minutes. The remaining five sites that hadshown shortening of effective refractory period £ 2 msec at leastonce by 120 minutes now exhibited refractory period shortening>2 msec at 180 minutes after infarction. Cumulative rate ofdenervated sites did not differ between dogs receiving latexinjection and coronary artery ligation (p = 0.41). C, Controlbefore coronary occlusion. * Data from one dog that developedventricular fibrillation were not included at 5 minutes afterligation.
3 msec or more during ansae subclaviae stimulation),shortening of effective refractory period became at-tenuated after latex injection, while it remained un-changed at 15 basal sites (Figure 4). The shortening ofeffective refractory period induced by norepinephrineinfusion was not different among the basal sites, theapical sites without apparent denervation, and the api-cal denervated sites (11.2 ±1.2, 10.7 ±1.6, and
SYMPATHETIC RESPONSES8 D 0 0 8 WITH LATEX
BASAL SITES ( N - 1 5 ) M±SE* p<0.005
v> C
T S. OEN(-) ( N - 1 3 )
APICAL t lTES. DEH(+) ( N - 1 7 )
nrinC S 30 6O 120 1*0 NE
mln
FIGURE 4. Bar charts. Ordinate, shortening of effective re-fractory period (AERP) induced by ansae subclaviae stimula-tion in eight dogs with transmural myocardial infarction pro-duced by latex embolization; abscissa, time after latexinjection. Top panel: Changes in ERP at basal sites. Middlepanel: Apical sites without apparent sympathetic denervation(by our definition; see text) [DEN ( — )]• Bottom panel: Apicalsites with denervation [DEN ( + )] are shown. Seventeen apicalsites, at which AERP induced by ansae subclaviae stimulationhad declined to ^2 msec on one or more occasion after latexinjection, were regarded as sympathetically denervated andwere analyzed as a group. AERP during ansae subclaviae stim-ulation were plotted over time, beginning before myocardialinfarction. Hatched bars, AERP induced by norepinephrine(NE) infusion; C, control.
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

Inoue and Zipes Time Course of Ischemia-Induced Efferent Neural Denervation 1115
8.8 ±1.1 msec, respectively; Figure 4). The subepi-cardial width of infarction relative to the left ventricu-lar circumference was 10 ± 1%.
Dogs with ligation of multiple coronary arteries. Ofnine dogs receiving ligation of multiple coronary arter-ies (4.6 ± 0.5 ligations), three dogs had nontransmuralmyocardial infarction and six dogs had transmuralmyocardial infarction as demonstrated by NBT stain-ing. The data from the six dogs with transmural myo-cardial infarction were included in the following analy-sis. Baseline effective refractory periods of test sitesare shown in Table 1. Sympathetic denervation wasachieved in at least one apical site in each of four dogsbut not at any site in the remaining two dogs withtransmural myocardial infarction. In one of the fourdogs showing sympathetic denervation, ventricular fi-brillation was induced during refractory period mea-surement 5 minutes after ligation. Ventricular defibril-lation was achieved promptly by DC shock (20 J), andall data except that collected 5-20 minutes after coro-nary ligation were obtained and included in the analy-sis. Sympathetic denervation occurred at one apicalsite 5-20 minutes after ligation and at 10 apical sites infour dogs with transmural myocardial infarction over aperiod of 3 hours (Figure 3). These 10 denervated siteshad shorter baseline effective refractory periods aftercoronary ligation than before coronary ligation (p<0.005; Table 1).
As a group, shortening of effective refractory periodinduced by ansae subclaviae stimulation declined pro-gressively at these 10 denervated apical sites (Figure5). At the remaining 14 innervated apical sites and 12basal sites, responses were not attenuated over time
SYMPATHETIC RESPONSESe DOQS WITH LIOATION OF
MULTIPLE CORONARY ARTERIES
BASAL SITES (N*12)
(10) "• 13
- 10
JL. T r JL
P I C A L S I T E S . D E N ( - ) ( N . t 4 )
i"4
'
- 10
• 3
PICAL SITES. O E N M (N -10 )
- < » r A(61
-10
-3
0C 3 30 »O 120 ISO NE
min
FIGURE 5. Bar charts. Shortening of effective refractory peri-od (AERP) induced by ansae subclaviae stimulation in six dogswith transmural myocardial infarction produced by ligation ofmultiple coronary arteries. Data in one dog that developedventricular fibrillation are not included at 5 minutes after liga-tion, and numbers of test sites analyzed at 5 minutes afterligation are indicated in parentheses. Data obtained at 5 min-utes were not included in an analysis of variance for repeatedmeasures. Format and abbreviations are as in Figure 4.
(Figure 5). Shortening of effective refractory periodinduced by norepinephrine infusion was not differentamong the basal sites, apical sites without apparentdenervation, and apical denervated sites (11.8 ±0.7,10.4± 1.3, and 9.3 ± 1.0 msec, respectively; Figure5). In four dogs with sympathetic denervation, thesubepicardial width of infarction relative to the leftventricular circumference was 7 ±4%. In the remain-ing two dogs without apparent sympathetic denerva-tion, the subepicardial width of infarction was only 1-2% of the left ventricular circumference.
In the three dogs with nontransmural myocardialinfarction, sympathetic denervation was not achieved.Shortening of effective refractory period at 10 apicalsites tended to decline over time, but the differencewas not significant in these three dogs (Table 2).
The width of subepicardial infarction relative to theleft ventricular circumference tended to be greater ineight dogs with transmural myocardial infarction pro-duced by latex embolization (10 ± 4%) than in six dogswith transmural myocardial infarction produced by li-gation of multiple coronary arteries (5 ±3%), but thedifference was not significant.
Vagal DenervationDogs with latex injection. In one of eight dogs re-
ceiving latex injection, all apical test sites were in-volved in myocardial infarction; therefore, data fromthis dog were excluded. In the remaining seven dogs,the current strength of vagal stimulation was0.55 ±0.03 mA for the right vagus and 0.48 ±0.07mA for the left vagus. Baseline effective refractoryperiods of test sites are shown in Table 3. Vagal dener-vation was achieved in at least one apical test site in sixof seven dogs and was not achieved in all 13 basal sitesin seven dogs. Cumulative rate of denervated apicalsites in seven dogs is shown in Figure 6. Seventeenapical test sites were vagally denervated over a periodof 3 hours after latex injection (Figure 6). Four testsites were denervated as early as 5-20 minutes afterlatex injection, and so were another six sites 30—45minutes after injection. The response to vagal stimula-tion, however, reappeared in four of these 10 sites at60-75 minutes after latex injection and was close to the
TABLE 2. Changes in Effective Refractory Period Induced byAnsae Subclaviae Stimulation in Three Dogs With Nontrans-mural Myocardial Infarction
coronaryocclusion
^ e r c o r o n a ry occlusion (minutes)30 60 120 180
Basal sites(n = 6)
Mean -17.0 -14.5 -16.3 -16.2 -16.7 -16.0
±SEM 1.6 1.0 0.9 0.8 0.9 0.9
Apical sites
(/i =10)
Mean -14.2 -13.1 -11.8 -12.0 -10.7 -10.6
±SEM 1.1 1.0 1.0 1.4 1.3 1.3
Values in milliseconds.
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

1116 Circulation Research Vol 62, No 6, June 1988
TABLE 3. Baseline Effective Refractory Period During Norepinephrine Infusion in Dogs Tested for VagalDenervation
/. Seven dogs with transmural myocardial ,
Basal sites (n=13)
Apical sites without denervation (n = 14)
Apical sites with denervation (n = 13)
infarction from latex injection of a coronary artery
Beforecoronary .occlusion
158±4
159±3
16O±3
5
155 + 4
157 ±3
159±4
After coronary occlusion
30
156 + 3
157±3
158±3
60
156±4
156 + 3
160±3
//. Nine dogs with nontransmural myocardial infarction from ligation of coronary artery
Basal sites (n=17)
Apical sites without denervation (n = 27)
Apical sites with denervation (n = 8)
Beforecoronary .occlusion
159±1
157±1
162 ±2
5
158±1
158+1
161 + 1
After coronary occlusion
30
158+1
158 ±1
161+2
60
158 ±1
159+1
162 ±2
(minutes)
120
157±4
159±3
160±4
(minutes)
120
159 ±2
159 ±1
163 ±3
180
158 + 4
162 ±3
161 ±4
180
158±2
160±l
164 + 2
Values are mean ± SEM in milliseconds.
baseline values at 3 hours after injection (5.8 ±0.3 vs.4.3 ±0.5 msec, p<0.02). In Figure 7, the time courseof changes in refractory period is shown. The four testsites at which vagal response recovered were excludedentirely from the analysis in Figure 7. Lengthening ofthe refractory period remained unchanged at all 13basal test sites over a period of 3 hours after latexinjection. At 13 apical sites with vagal denervation,lengthening of refractory period was significantly de-creased as early as 5-20 minutes after latex injection(Figure 7). At 10 apical sites without apparent vagaldenervation, responses were decreased 3 hours afterinjection (/><0.005).
In six dogs with vagal denervation, the subendocar-dial width of infarction relative to the left ventricularcircumference was 14 ± 3%, and in the remaining dogwithout apparent vagal denervation, the relative widthwas 10%.
Dogs with ligation of multiple coronary arteries.Diagonal branches and collaterals were ligated in 11dogs (average 2.2±0.3 ligations). Fewer coronaryarteries were ligated in this group of dogs than in thenine dogs tested for sympathetic denervation(p<0.001). In two of 11 dogs, myocardial infarctionwas not demonstrated by NBT staining, and in nine
VAQAL DENERVATION
100
8 0
60
4 0
20
LATEX (N"27)LK3ATION (N = 35>
CS 30 60 120 ISOmln
FIGURE 6. Plot showing cumulative percentage of vagaltydenervated apical sites is shown as in Figure 3 and was greaterin dogs receiving latex injection than in dogs with ligation ofcoronary arteries (p<0.002).
dogs, nontransmural myocardial infarction was pres-ent. No dog showed transmural myocardial infarction.Current strength of vagal stimulation was 0.59 ±0.09mA for the right vagus and 0.64 ± 0.11 mA for the leftvagus in these nine dogs with myocardial infarction.Baseline effective refractory periods of test sites areshown in Table 3. Vagal denervation did not occur atall 17 basal test sites in nine dogs. Four dogs did notshow vagal denervation at any apical test sites, but fivedogs showed vagal denervation in at least one apicaltest site. Eight apical sites were vagally denervated
VAQAL RESPONSES
7 D0Q8 WITH LATEX
BASAL SITES (N-13)U1SE
• p<0.0S** p<0.006
vi C
APICAL SITES. OEN(-) (N-10)
**nAPICAL SITES. DEH(+) (N-13)
C 9 v> so no iso mln
FIGURE 7. Bar charts. Lengthening of effective refractory pe-riod (LERP) induced by vagal stimulation in seven dogs withtransmural myocardial infarction produced by latex injection.Seventeen apical sites, at which bERP induced by vagal stimu-lation had declined to^l msec on one or more occasions aftercoronary occlusion with latex, were regarded as vagally dener-vated. However, response of ERP to vagal stimulation wasrestored toward the control value at four of these 17 sites (seetext). These four apical sites were excluded from the analysis.hERP during vagal stimulation were plotted over time, begin-ning before myocardial infarction. Format and abbreviationsare as in Figure 4.
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from
Inoue and Zipes Time Course of Ischemia-Induced Efferent Neural Denervation 1117
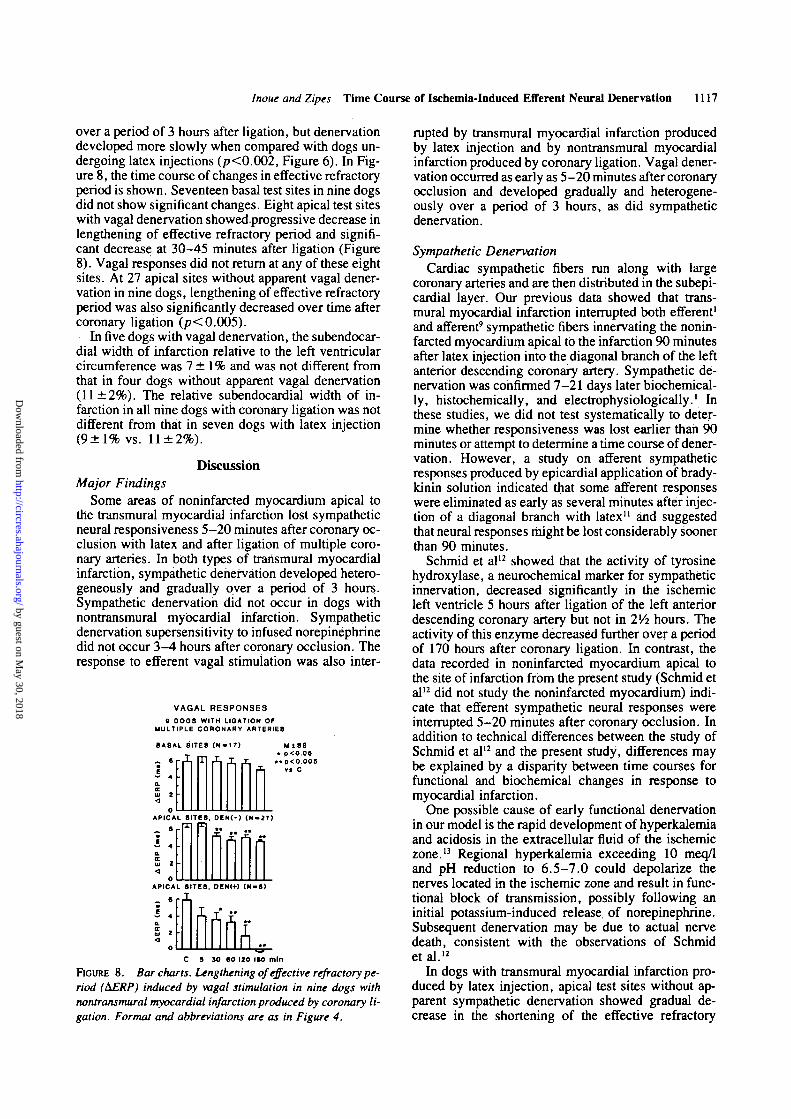
over a period of 3 hours after ligation, but denervationdeveloped more slowly when compared with dogs un-dergoing latex injections (p<0.002, Figure 6). In Fig-ure 8, the time course of changes in effective refractoryperiod is shown. Seventeen basal test sites in nine dogsdid not show significant changes. Eight apical test siteswith vagal denervation showedprogressive decrease inlengthening of effective refractory period and signifi-cant decrease at 30-45 minutes after ligation (Figure8). Vagal responses did not return at any of these eightsites. At 27 apical sites without apparent vagal dener-vation in nine dogs, lengthening of effective refractoryperiod was also significantly decreased over time aftercoronary ligation (p< 0.005).
In five dogs with vagal denervation, the subendocar-dial width of infarction relative to the left ventricularcircumference was 7 ± 1 % and was not different fromthat in four dogs without apparent vagal denervation(11 ±2%). The relative subendocardial width of in-farction in all nine dogs with coronary ligation was notdifferent from that in seven dogs with latex injection(9±1% vs. 11 ±2%).
DiscussionMajor Findings
Some areas of noninfarcted myocardium apical tothe transmural myocardial infarction lost sympatheticneural responsiveness 5-20 minutes after coronary oc-clusion with latex and after ligation of multiple coro-nary arteries. In both types of transmural myocardialinfarction, sympathetic denervation developed hetero-geneously and gradually over a period of 3 hours.Sympathetic denervation did not occur in dogs withnontransmural myocardial infarction. Sympatheticdenervation supersensitivity to infused norepinephrinedid not occur 3-4 hours after coronary occlusion. Theresponse to efferent vagal stimulation was also inter-
VAQAL RESPONSES8 DOQS WITH LIOATIOH OF
MULTIPLE CORONARY ARTERIES
BASAL SITES (N-17)
„ 6
i 4 nM 1 S B
• p<O06• * p<0.005
va C
PICAL SITES, DIN(-) (N-17)
S
4
2
PICAL SITES. DEHI+) (N-S)
C 5 JO «o no iio mln
FIGURE 8. Bar charts. Lengthening of effective refractory pe-riod (&ERP) induced by vagal stimulation in nine dogs withnontransmural myocardial infarction produced by coronary li-gation. Format and abbreviations are as in Figure 4.
rupted by transmural myocardial infarction producedby latex injection and by nontransmural myocardialinfarction produced by coronary ligation. Vagal dener-vation occurred as early as 5-20 minutes after coronaryocclusion and developed gradually and heterogene-ously over a period of 3 hours, as did sympatheticdenervation.
Sympathetic DenervationCardiac sympathetic fibers run along with large
coronary arteries and are then distributed in the subepi-cardial layer. Our previous data showed that trans-mural myocardial infarction interrupted both efferent1
and afferent9 sympathetic fibers innervating the nonin-farcted myocardium apical to the infarction 90 minutesafter latex injection into the diagonal branch of the leftanterior descending coronary artery. Sympathetic de-nervation was confirmed 7—21 days later biochemical-ly, histochemically, and electrophysiologically.1 Inthese studies, we did not test systematically to deter-mine whether responsiveness was lost earlier than 90minutes or attempt to determine a time course of dener-vation. However, a study oh afferent sympatheticresponses produced by epicardial application of brady-kinin solution indicated that some afferent responseswere eliminated as early as several minutes after injec-tion of a diagonal branch with latex" and suggestedthat neural responses might be lost considerably soonerthan 90 minutes.
Schmid et al12 showed that the activity of tyrosinehydroxylase, a neurochemical marker for sympatheticinnervation, decreased significantly in the isehemicleft ventricle 5 hours after ligation of the left anteriordescending coronary artery but not in 2Yz hours. Theactivity of this enzyme decreased further over a periodof 170 hours after coronary ligation. In contrast, thedata recorded in noninfarcted myocardium apical tothe site of infarction from the present study (Schmid etal12 did not study the noninfarcted myocardium) indi-cate that efferent sympathetic neural responses wereinterrupted 5-20 minutes after coronary occlusion. Inaddition to technical differences between the study ofSchmid et al12 and the present study, differences maybe explained by a disparity between time courses forfunctional and biochemical changes in response tomyocardial infarction.
One possible cause of early functional denervationin our model is the rapid development of hyperkalemiaand acidosis in the extracellular fluid of the isehemiczone.13 Regional hyperkalemia exceeding 10 meq/1and pH reduction to 6.5-7.0 could depolarize thenerves located in the isehemic zone and result in func-tional block of transmission, possibly following aninitial potassium-induced release, of norepinephrine.Subsequent denervation may be due to actual nervedeath, consistent with the observations of Schmidetal.12
In dogs with transmural myocardial infarction pro-duced by latex injection, apical test sites without ap-parent sympathetic denervation showed gradual de-crease in the shortening of the effective refractory
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

1118 Circulation Research Vol 62, No 6, June 1988
period induced by ansae subclaviae stimulation, sug-gesting partial denervation. This partial denervationmay have been progressive and might have becomemore complete if we had observed the dogs for a longertime period. Partial denervation in this manner is a newobservation. It is consistent with our previous observa-tion414 that, after transmural myocardial infarction pro-duced by latex injection, some dogs demonstratedshortening of refractory period in apical sites in re-sponse to ansae subclaviae stimulation (no apparentsympathetic denervation) yet showed a supersensitiveresponse of refractory period shortening to infusednorepinephrine. It is possible that these sites becamepartially denervated from the infarction (e.g., Figure 4middle panel) and that this partial denervation wassufficient to permit development of sympathetic super-sensitivity. The question of why only partial denerva-tion occurs needs to be explored in the future. Correla-tion with changes in myocardial blood flow would behelpful.
Dogs with ligation of multiple coronary arteriestended to have infarctions with less epicardial involve-ment than did dogs with latex infarction, and partialdenervation did not appear to occur. Nondenervatedapical test sites had stable shortening of effective re-fractory period induced by ansae subclaviae stimula-tion. This observation may be related to the fact thatlatex injection generally eliminates collateral flow,15
while dogs with ligation of multiple coronary arteriesstill might develop collaterals that might preserve mar-ginally ischemic areas.
In dogs with ligation of multiple coronary arteries,10 denervated apical sites had shorter baseline effec-tive refractory periods after coronary ligation than be-fore coronary ligation. Although the reason for thisshortening is not clear, it is not likely that the shorten-ing of baseline effective refractory period affected theresponse to ansae subclaviae stimulation. If shorteningof the baseline effective refractory period were thereason for the decreased response to ansae subclaviaestimulation with time, we would have expected shor-tening of the baseline effective refractory period toparallel a decrease in the response to ansae subclaviaestimulation. Instead, the baseline effective refractoryperiod remained constant.
Vagal DenervationVagal fibers appear to be located in the subendocar-
dial layer after crossing the atrioventricular groove inthe dog.6916"20 An encircling endocardial incision 2mm deep can interrupt efferent vagal fibers innervatingthe region apical to the incision." Transmural myocar-dial infarction produced by injection of latex into adiagonal branch interrupts efferent vagal fibers inner-vating the noninfarcted apical myocardium 90 minutesafter injection2 and also decreases choline acetyltrans-ferase activity, a marker for vagal innervation, in thenormal apical myocardium 7 days after myocardialinfarction." Nontransmural myocardial infarction pro-duced by ligation of the left anterior descending coro-nary artery followed by reperfusion also interrupts va-
gal innervation in the normal myocardium overlyingthe infarction 24 hours after ligation.3
Schmid et al12 found that choline acetyltransferaseactivity did not decrease significantly in the ischemiccanine left ventricle 5 hours after ligation of the leftanterior descending coronary artery, but it did decreaseat 25 and 170 hours. Data from the present study,however, demonstrate that functional efferent vagaldenervation occurs 5-20 minutes after coronary occlu-sion and develops heterogeneously and gradually overa period of 3 hours, as does sympathetic denervation.This seems compatible with our previous observationdemonstrating that the afferent vagal response to epi-cardial application of nicotine solution was significant-ly attenuated 13-15 minutes after ligation of a diagonalbranch." As we suggested above, a measurable de-crease in transmitter or enzyme activity may lag behindthe loss of functional response after coronary occlu-sion. Functional changes may be related to regionalextracellular hyperkalemia and acidosis.
Methodological ConsiderationsSecobarbital sodium414 rather than a-chloralose1
was used as an anesthetic, and the ansae subclaviaewere stimulated at a slightly lower frequency (2 vs. 3 -5 Hz) than before.' •*•14 Despite these minor differences,effective refractory period shortening induced by an-sae subclaviae stimulation in the present study wascomparable to previous results.1414
Our previous studies showed that in the canine heart4-21 days after transmural myocardial infarction ordissection of the atrioventricular groove, eliminationof responses in effective refractory period to ansaesubclaviae stimulation or vagal stimulation, respec-tively, were accompanied by the biochemical evidenceof denervation of sympathetic1 or vagal1920 fibers.Therefore, it seems reasonable to use the changes ineffective refractory period in response to stimulation ofansae subclaviae and vagi as a marker of efferent sym-pathetic and vagal innervation. However, becauseonly a limited number of sites were sampled, moreextensive denervation may exist than suggested by thedata presented.
It took about 15 minutes to determine the duration ofthe effective refractory period both in the control stateand during nerve stimulation. While it is possible thatminor spontaneous alterations in effective refractoryperiod might take place during those 15 minutes, thisdoes not appear to be an important source of error.Refractory periods in the basal sites were quite con-stant throughout the study.
The criteria of denervation were arbitrary in thepresent study as they were in our previous study.1 Indogs with latex injection, the extent of effective refrac-tory period shortening induced by stimulation of ansaesubclaviae decreased gradually after latex injection atapical test sites that were considered to be innervatedusing the present definition. This finding may be ex-plained in several ways. First, these sites may simplyhave exhibited a slower rate of denervation progres-sion. If we had waited longer, these sites might have
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

Inoue and Zipes Time Course of Ischemia-Induced Efferent Neural Denervation 1119
shown more complete loss of response to stimulation.Second, these test sites may have been partially dener-vated, consistent with data from our other studies.414
Finally, the criteria to establish the presence of dener-vation may have been too strict.
Some test sites that were designated as denervatedby the present criteria (over a 3-hour period after in-farction on one or more occasions) showed some vari-ation in responses to neural stimulation exceeding thecutoff value (Figures 3 and 6). These sites were con-sidered to be denervated and, for the group as a whole,showed a gradual decline of responses in effectiverefractory period to neural stimulation (Figures 4, 5, 7,and 8).
Restoration of vagal responses occurred at four of 17apically denervated sites in dogs receiving latex injec-tion. Although denervation tended to occur more slow-ly in dogs with coronary ligation than in dogs withlatex injection, restoration of vagal responses did notoccur in the group with coronary ligation. Collateralsdo not provide an adequate answer for restoration ofvagal responses because dogs with latex infarctionsgenerally do not develop collaterals.13 That is the rea-son for using the latex method. The effects of cavityblood may not explain the restoration of vagal re-sponses because it occurred only in dogs with latexinjection. We do not have plausible explanations forrecovery of the vagal response that occurred 60 min-utes after latex injection at the four apical test sites.
Latex was injected to embolize collaterals and toproduce a transmural myocardial infarction in the pres-ent study as in previous studies.124-915 Because of itsinert properties, it is not likely that latex itself inter-rupted both sympathetic and vagal responses. We haveshown that injection of acetone, the vehicle in whichlatex is suspended, into the diagonal branch does notinterrupt sympathetic responses.1 Of importance is thefact that myocardial infarction produced by coronaryartery ligation alone also interrupted both sympatheticand vagal responses in the present study. Therefore, itis reasonable to attribute the loss of sympathetic andvagal responses in dogs with latex injection to myocar-dial infarction, not to the latex itself. We have alsoshown that a careful dissection of the adventitia overthe left anterior descending coronary artery or its diag-onal branch does not interrupt sympathetic re-sponses,19 despite recently published observations.21
Control measurements during ansae subclaviae stimu-lation in the present study were obtained after the dis-section, indicating intact sympathetic innervation.
Myocardial blood flow was not determined in thepresent study. The site of electrode placement withrespect to the infarction was determined using NBTstaining. This determination plus the fact that infusednorepinephrine shortened effective refractory periodsequally at the basal sites and the apical denervated sitessuggest that there were still functioning adrenergic re-ceptors at the apical test sites and that there appeared tobe enough blood flow to distribute infused norepineph-rine to the apical test sites.
It has been shown that cardiac sympathetic and
vagal fibers are distributed in the subepicardial andsubendocardial layers, respectively, in the canineheart.6"81617 Based on these facts, it is reasonable toassume that the subepicardial and subendocardial ex-tent of myocardial infarction may be one of determi-nants that affect the efferent sympathetic and vagalresponses, respectively. Therefore, the subepicardialand subendocardial width relative to the left ventricu-lar circumference was used as an indicator of extent ofinfarction in dogs tested for sympathetic and vagaldenervation, respectively. While there are inherentproblems using this method as an indicator of the ex-tent of myocardial infarction, the approach seemedreasonable for the questions we wanted to answer.
Clinical ImplicationsWe showed that sympathetic denervation was ar-
rhythmogenic in dogs with myocardial infarction 4-22days after denervation.4 Although arrhythmia induc-tion was not tested in the present study, it is quitepossible that the heterogeneous development ofsympathetic and vagal denervation following myocar-dial infarction may contribute the development of ven-tricular arrhythmias that occur early after coronaryocclusion.
AcknowledgmentsWe thank Naomi S. Fineberg, PhD, for statistical
analysis and Harald P. Pride and Becky G. Davies fortheir technical assistance.
References1. Baiber MJ, Mueller TM, Henry D, Felten D, Zipes DP: Trans-
mural myocardial infarction in the dog produces sympathecto-my in noninfarcted myocardium. Circulation 1983;67:787-796
2. Browne KF, Barber MJ, Gill R, Zipes DP: Vagal denervationof noninfarcted canine myocardium produced by transmuralmyocardial infarction (abstract). Circulation 1983;68(supplin):in-247
3. Martins JB, Lewis RM, Lund DD, Schmid PG: A thin suben-docardial infarction produces cholinergic denervation of over-lying normal epicardium (abstract). J Am Coll Cardiol 1987;9:94A
4. Inoue H, Zipes DP: Results of sympathetic denervation in thecanine heart: Supersensitivity that may be arrhythmogenic.Circulation 1987;75:877-887
5. Martins JB, Zipes DP: Effects of sympathetic and vagal nerveson recovery properties of the endocardium and epicardium ofthe canine left ventricle. Circ Res 1980;46:100-110
6. Takahashi N, Barber MJ, Zipes DP: Efferent vagal innervationof canine ventricle. Am J Physiol 1985;248:H89-H97
7. Kaye MP, Brynjolfsson GG, Geis WP: Chemical epicardiec-tomy: A method of myocardial denervation. Cardiologia1968^3:139-149
8. Barber MJ, Mueller TM, Davies BG, Zipes DP: Phenol topi-cally applied to left ventricular epicardium interrupts sympa-thetic but not vagal afferents. Circ Res 1984^5:532-534
9. Barber MJ, Mueller TM, Davies BG, Gill RM, Zipes DP:Interruption of sympathetic and vagal-mediated afferent re-sponses by transmural myocardial infarction. Circulation1985;72:623-631
10. Wallenstein S, Zucker C, Fleiss J: Some statistical methodsuseful in circulation research. Circ Res 1980;47:l-9
11. Inoue H, Skale B, Zipes DP: Effects of myocardial ischemiaand infarction on cardiac afferent sympathetic and vagal re-flexes in the dog. Am J Physiol (in press)
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

1120 Circulation Research Vol 62, No 6, June 1988
12. Schmid PG, Greif BJ, Lund DD, Roskoski R Jr Tyrosinehydroxylase and choline acetyltransferase activities in ische-mic canine heart. Am J Physiol 1982;243:H788-H795
13. Hill JL, Gettes LS: Effect of acute coronary artery occlusion onlocal myocardial extracellular K+ activity in swine. Circula-tion 1980;61:768-778
14. Kammerling JJ, Green FJ, Watanabe AM, Inoue H, BarberMl, Henry DP, Zipes DP: Transmural myocardial infarctionproduces denervation supersensitivity of refractoriness in non-infarcted areas apical to the infarction. Circulation 1987;76:383-393
15. EulerDE, Prood CE, Spear JF, Moore EN: The interruption ofcollateral blood flow to the ischemic canine myocardium byembolization of a coronary artery with latex: Effects on con-duction delay and ventricular arrhythmias. Circ Res 1981;49:97-108
16. Martins JB, Zipcs DP: Epicardial phenol interrupts refractoryperiod responses to sympathetic but not vagal nerve stimulationin canine left ventricular epicardium and endocardium. CircRes 1980;47:33-40
17. Chilson DA, Peigh P, Mahomed Y, Zipes DP: Encircling en-
docardial incision interrupts efferent vagal-induced prolonga-tion of endocardial and epicardial refractoriness in the dog.J Am Coll Cardiol 1985;5:29O-296
18. Blomquist TM, Priola DV, Romero AM: Source of intrinsicinnervation of canine ventricles: A functional study. Am JPhysiol 1987;252:H638-H644
19. Kovacs RJ, Kammerling JM, Zipes DP, Bailey JC: Reductionof choline acetyltransferase activity by cardiac parasympathec-tomy and transmural myocardial infarction (abstract). Circula-tion 1985;72(suppl ni):IH-246
20. Inoue H, Zipes DP: WPW surgery interrupts vagal innervationto the left ventricle and to the AV node in the canine heart.Cardiovasc Res (in press)
21. Heusch G, Guth BD, Roth DM, Seitelberger R, Ross J JrContractile responses to sympathetic activation after coronaryinstrumentation. Am J Physiol 1987;252:H1059-H1069
KEY WORDS • denervation • efferent sympathetic nerve •efferent vagal nerve • effective refractory period • myocardialinfarction
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from

H Inoue and D P Zipescoronary artery in the canine heart.
Time course of denervation of efferent sympathetic and vagal nerves after occlusion of the
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1988 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.62.6.11111988;62:1111-1120Circ Res.
http://circres.ahajournals.org/content/62/6/1111World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 30, 2018
http://circres.ahajournals.org/D
ownloaded from