moderators: david cort, md alex denes, md panelists: stephen swisher, md, phd edward lin, md
TRANSCRIPT

Moderators:David Cort, MDAlex Denes, MD
Panelists:Stephen Swisher, MD, PhD
Edward Lin, MD

Tumor staging
T1- confined to mucosa/submucosa
T2- extends to muscularis propria
T3- extends into surrounding tissue
T4 - involves major vessels, pleura, pericardium
Nodal staging
N0 - no nodes involved
N1 - local nodes involved
N2 - distant nodes involved

Esophagectomy
Combined modality Pre-operative chemo-radiation >>> esophagectomy Esophagectomy >>>> Post-operative chemo-radiation
Non surgical Definitive chemoradiation

Surgical margins Pathology margins
R0 No tumor No tumor
R1 No tumor Microscopic tumor present
R2 Tumor present Macroscopic tumor present

What are the usual sites of recurrence Local distant
Benefits Palliative chemo ± radiation
▪ survival benefit▪ Quality of life
Treatment of recurrence in lymph node outside the initial field of initial radiotherapy
How- Physical Exam- what signs to look for CT chest/abdomen- what findings to look for EGD – what symptoms should prompt it Serum CEA levels- ? In which patients EUS - ? role
How often Suggested protocols for follow up


A 52 year old accountant with known history of Barrett’s esophagus and symptomatic reflux
surveillance endoscopy. 5 cm segment of Barrett’s esophagus proximal to the GE
junction. ▪ Biopsy - Multiple foci of HGD
1.5 cm sessile polypoid lesion at the GEJ▪ Biopsy- Invasive adenocarcinoma.

T1- confined to the mucosa and submucosa and sparing the muscularis propria.
N0 – no enlarged lymph nodes

PET/CT: No nodal or distant metastases
He undergoes esophagectomy without complications (R0 resection)
Surg path: T1, N0, (M0) moderately differentiated adenocarcinoma, No lympho-vascular infiltration multiple foci of Barrett’s all margins clear of tumor

1. CT chest and abdomen every 3 months2. CT chest and abdomen every 6 months3. CXR every 3 months4. EGD every 3 months5. All of the above6. None of the above
AQ1. Appropriate post treatment follow-up of this patient would involve

What are the chances of tumor recurrence
What are the usual sites of recurrence Local
▪ Treatment options▪ Benefits
Distant▪ Treatment options▪ Benefits
Suggested follow up after treatment
T1N0 GEJ
The cure rate 80-90%.
If EMR or radiation cure rate 60-70% (then regular EGD is indicated).
Q 6 months for the first 2 years, then annual
physical exams with routine blood work.
Imaging only when clinically indicated.

Repeat endoscopy 1 year after surgery to rule out residual Barrett’s or dysplasia
No CT Scan, CXR or PET scan unless symptoms because of low likelihood of distant mets with T1N0, LVI negative

Repeat endoscopy 1 year after surgery to rule out residual Barrett’s or dysplasia
No CT Scan, CXR or PET scan unless symptoms because of low likelihood of distant mets with T1N0, LVI negative
A 65 year old house-wife with history of GERD presents with progressive dysphagia
EGD: An irregular, non obstructing, ulcerated mass in the
distal esophagus. Biopsy: Moderately differentiated adenocarcinoma
EUS: T3 tumor (infiltrating muscularis propria) No enlarged lymph nodes
PET/CT: intense FDG uptake in the distal esophageal mass no lymph node or distant metastases



Planned treatment: Pre-operative chemoradiation followed by surgery
Patient recieves combined modality therapy with radiation and chemotherapy Follow up EGD:
▪ no residual mass and biopsy shows only radiation effect.
Patient is now reluctant about proceeding with esophagectomy

1. Convince the patient to proceed with surgery as originally planned
2. Give additional chemo-radiation to full dose
3. Can wait and see how the patient performs
4. None of the above


RTOG-Hersovic: Chemo-RT > RT: 5-year 32%, vs 12% 20% vs 0% 10 year survival. LR > 45%
Intergroup 0123: 50.4 Gy > 64.8 Gy
Phase III: Modern RT = S
CMT vs S: OR 0.53-0.86. Three Meta-analysis (Ref 1-3). (Many small studies isolated positive study mostly with 5FU/Cisplatin/50.4 cGy.
Urschel Am J Surgery 2003:6:553. 1. Surgery 2005; 137:1727 2. Gut 2004;7:925 3. Walsh et la. NEJM.1997 Kelsen DP NEJM 1998; Yu ASCO 2006 Abst 4012

Chances of tumor recurrence Sites of tumor recurrence
Local distant
Treatment options Salvage esophagectomy
Suggested follow up

CT or CT/PET and endoscopy with biopsies q 3 months x2 then 6month x 3 then yearly (RTOG 0246) Early follow/up similar survival to
trimodality

Esophagectomy R0 resection Path:
▪ No residual carcinoma in the esophagus ▪ 12 lymph nodes are clear

What are the chances of tumor recurrence
What are the usual sites of recurrence Local
▪ Treatment options▪ Benefits
Distant▪ Treatment options▪ Benefits
Suggested follow up after treatment

A 48 year old high school teacher presents with progressive dysphagia and weight loss
EGD: large ulcerated nearly circuferential mass in the lower third of
the esophagus. Biopsy: Moderate to poorly differentiated adenocarcinoma
with lymphovascular infiltration.
PET/CT: Intense FDG uptake in paraesophageal lymph nodes. No distant metastases.
EUS: T3 tumor (Nearly circumferential mass, extension into the
adventitia) N1 (multiple enlarged regional lymph nodes)
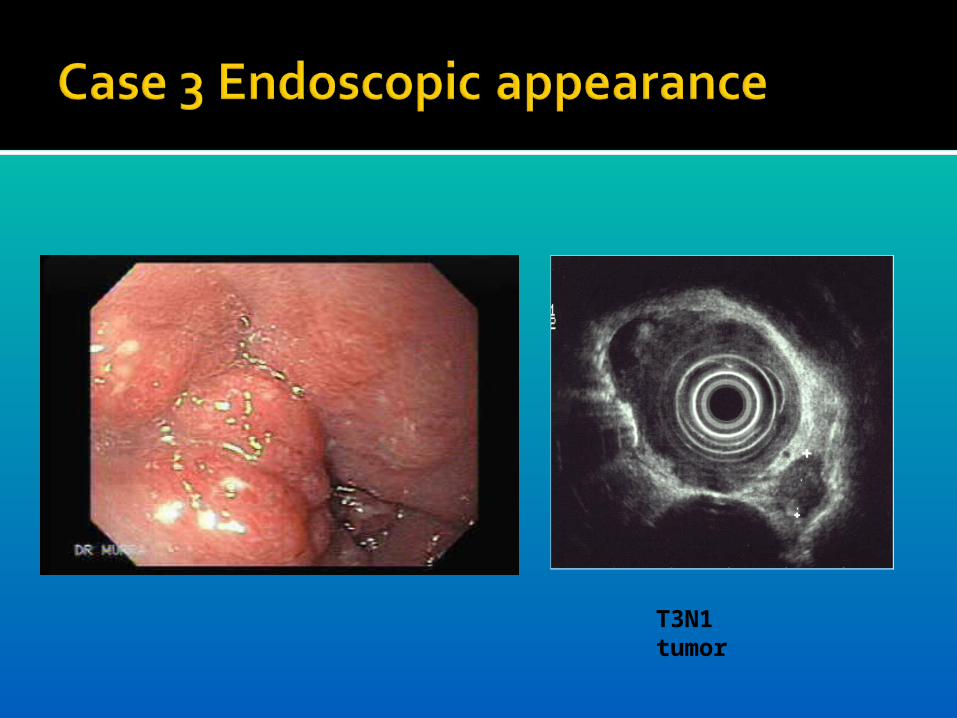
T3N1 tumor

Treatment: combined modality therapy with radiation and
chemotherapy.
Follow up EGD 75% regression of the mass. Biopsy: residual adenocarcinoma.
Esophagectomy R0 resection Path:
▪ Residual moderately differentiated adenocarcinoma, ▪ foci of carcinoma in 3 regional lymph nodes.

1. Follow up with EGD and CT scan every 3 months
2. Follow up with EGD and CT scan every 6 months
3. Additional radiation therapy to maximal dose
4. Combination salvage chemoXRT

What are the chances of tumor recurrence
What are the usual sites of recurrence Local
▪ Treatment options▪ Benefits
Distant▪ Treatment options▪ Benefits
Suggested follow up after treatment

A 68 year old retired carpenter with a history of CAD, CABG, CHF, COPD, and DM presents with progressive GERD symptoms. No dysphagia or weight loss.
EGD: distal esophagitis with an area of ulceration just proximal
to the GE junction Biopsy: Moderately differentiated adenocarcinoma.
EUS: T2 N0tumor

PET/CT: No abnormal FDG uptake in paraesophageal lymph
nodes. No distant metastases.
Surgical evaluation: Not candidate for resection due to co-morbidities
Treatment: Completes full course of combined chemotherapy and
radiation.

What are the chances of tumor recurrence
What are the usual sites of recurrence: 40% Local
▪ Treatment options: ▪ Benefits
Distant▪ Treatment options▪ Benefits
Suggested follow up after treatment