new methods to ensure target coverage - aapm
TRANSCRIPT

7/14/2015
1
New methods to ensure target
coverage 7:30: Jeffrey Siebers, Coverage evaluation and probabilistic treatment planning as a margin alternative
8:10 Jan Unkelbach, Stochastic programming methods for handling uncertainty and motion in IMRT planning
8:50 Huijun Xu, Coverage-based treatment planning to accommodate organ deformable motions and contouring uncertainties for prostate treatment
D e p a r t m e n t o f R a d i a t i o n O n c o l o g y
Objectives
• To understand – robust-planning as a clinical alternative to using margin-
based planning
– the conceptual differences between uncertainty and predictable motion
– the fundamental limitations of the PTV concept that probabilistic planning can overcome
– the major contributing factors to target and normal tissue coverage probability
– the similarities and differences of various robust planning techniques
– the benefits and limitations of robust planning techniques
Coverage evaluation and
probabilistic treatment planning as a
margin alternative
Marnix Witte
Jeffrey V Siebers
7/14/2015
2
Conflict of Interest
• JVS has received funding from
– Philips Medical Systems regarding treatment
planning
– Varian Medical Systems regarding dose delivery
verification
RT Planning Goal • Provide a tumorcidal dose while minimizing normal
tissue toxicity risk • Geometric uncertainties limit efficacy
– Image guidance reduces uncertainties • Daily on-line image alignment • Adaptive Radiation Therapy
– Planning strategies mitigate remaining errors • Margins • Probabilistic/robust planning
Effect of positioning uncertainty
• Daily random setup errors blur dose • Systematic shifts • Results
– Observed dose distribution in TPS not equal to dose received by patient
– Physician does not evaluate actual dose distribution or coverage
• Workaround – PTV coverage “representative” of CTV (Ideally)!
or or =
Planned Fractionation blurs
Systematic errors offset entire dose
distribution

7/14/2015
3
PTV - ICRU 83
Margins should ensure robustness
7/14/2015
4
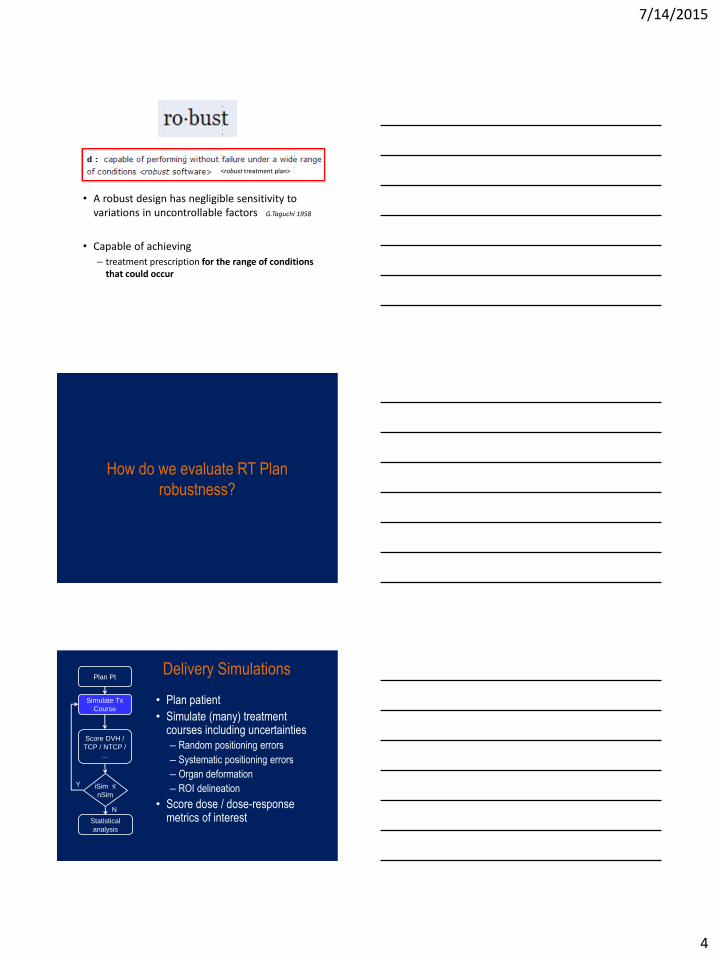
• A robust design has negligible sensitivity to variations in uncontrollable factors G.Taguchi 1958
• Capable of achieving
– treatment prescription for the range of conditions that could occur
<robust treatment plan>
How do we evaluate RT Plan
robustness?
Delivery Simulations
• Plan patient
• Simulate (many) treatment courses including uncertainties
– Random positioning errors
– Systematic positioning errors
– Organ deformation
– ROI delineation
• Score dose / dose-response metrics of interest
Plan Pt
Simulate Tx
Course
Score DVH /
TCP / NTCP /
…
iSim ≤
nSim
Statistical
analysis
Y
N

7/14/2015
5
• Include slide from CERR uncertainty inclusion
‘PlanJury’ for plan evaluation
Tomas Janssen, Román Bohoslavsky
PTV
Rectum Wall
Viewing probabilistic DVH-like metrics
dose
volu
me
dose
volu
me
dose
volu
me
Different treatments DVHs Dose-volume coverage map (DVCM)
Percentile DVH for coverage q
For (d, v, q)
Prob[Dv≥d]=q
dose
volu
me
DVCM iso-probability
= Percentile DVH

7/14/2015
6
Observations from robustness analysis
of margin-based plans
• PTVs
– Margin-formula-based PTVs are robust
(designed for p=90%, actual p>90% )
– Coverage is dictated by the treated volume
• OARs
– PRV-less plans underestimate OAR dose
– NTCP estimates generally poor
Clincal observation
Plans are not perfectly conformal
CTV
Position
Plan CTV
Position
PTVmin dose
assumed by
margin formula
Treated Volume
TV
dictates CTV dose
Typically, the TV will not conform to the PTV
In some directions there is gap between the PTV and TV,
which gives the CTV more room to move than is
assumed by the margin formulas.
PTV
CTV-to-PTV
margin
ICRU volumes deficiencies
• GTV – Tumors are heterogeneous
(ICRU assumes homogeneous)
• CTV – Subclinical disease decreases with distance
(CTV margin assumes homogeneous)
• PTV – Small errors are more likely than large ones
(PTV margin assumes equi-probable locations)
• TV (Treated Volume) – Is not perfectly conformal to PTV

7/14/2015
7
Use of fixed volumes in RT
• Does not reflect the continuous nature of
dose distributions and flexibility of IMRT
– More like a surgical margin
• Inherited from pre-IMRT era
– Easy
– Available
– But likely not optimal
Probabilistic Treatment Planning
PTP • Incorporation of mathematical models of geometric
uncertainties into the plan optimization framework with goal of creating a plan that is “robust” or tolerant to such geometric uncertainties. – Planner does NOT need to specify a fixed margin, permits more
flexibility in tradeoff (overlap or near-overlap) regions
– Creates dose distribution which ensures coverage/sparing – an implicit margin is created
– Directly optimize for desired result • dose-volume coverage probability
• TCP/NTCP
Margin based planning
CTV PTV
Optimization
Objective functions MinDose MaxDose
DVH points EUD
Dose
distribution
90% prob. of
D ≥ 95% Dprescribed
in CTV
M = 2.5Σ+0.7σ
OAR
PRV
7/14/2015
8
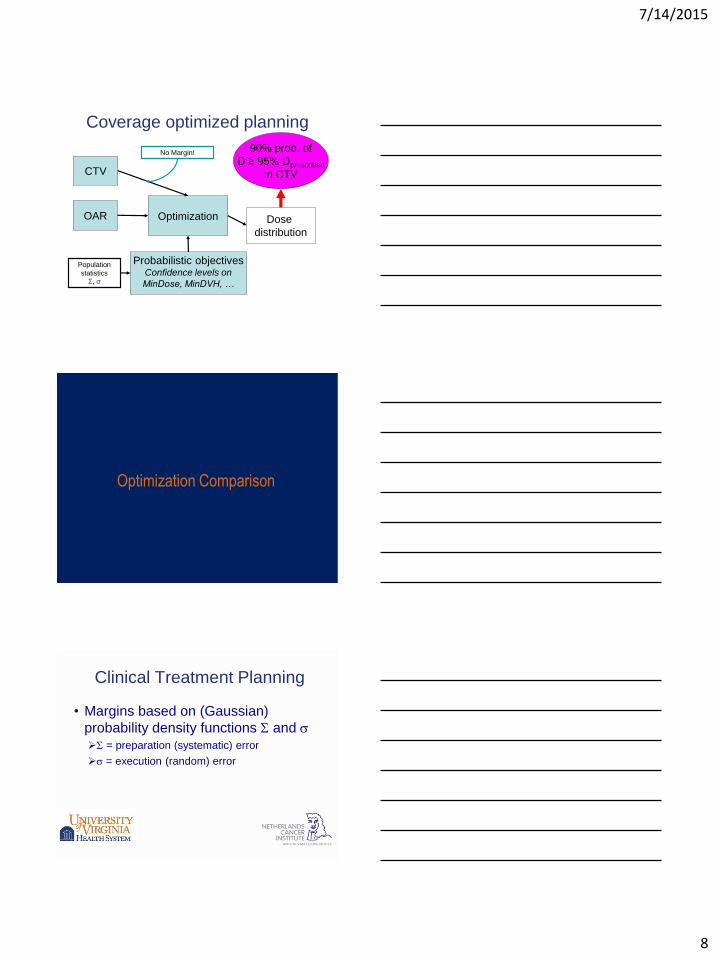
Coverage optimized planning
CTV
Optimization
Probabilistic objectives Confidence levels on
MinDose, MinDVH, …
Dose
distribution
90% prob. of
D ≥ 95% Dprescribed
in CTV
OAR
Population
statistics
Σ, σ
No Margin!
Optimization Comparison
Clinical Treatment Planning
• Margins based on (Gaussian)
probability density functions S and s
S = preparation (systematic) error
s = execution (random) error

7/14/2015
9
• Current clinical IMRT
• M = 2.5S + 0.7s
PTV
0% 0
100%
Dp Dose
Dose
Dp
0
lung CTV lung
Planned
Prescribed
PTV
Dose Profile DVH of PTV
+7%
- 5%
PTV
0% 0
100%
Dp Dose
Dose
Dp
0
lung CTV lung
PTV
Dose Profile DVH of PTV
MinDose
cost
Planned
Prescribed
- 5%
+7%
• Current clinical IMRT
• M = 2.5S + 0.7s
PTV
0% 0
100%
Dp Dose
Dose
Dp
0
lung CTV lung
PTV
Dose Profile DVH of PTV
Planned
Prescribed
- 5%
+7%
• DCTV>95% at P=90%
• Current clinical IMRT
• M = 2.5S + 0.7s

7/14/2015
10
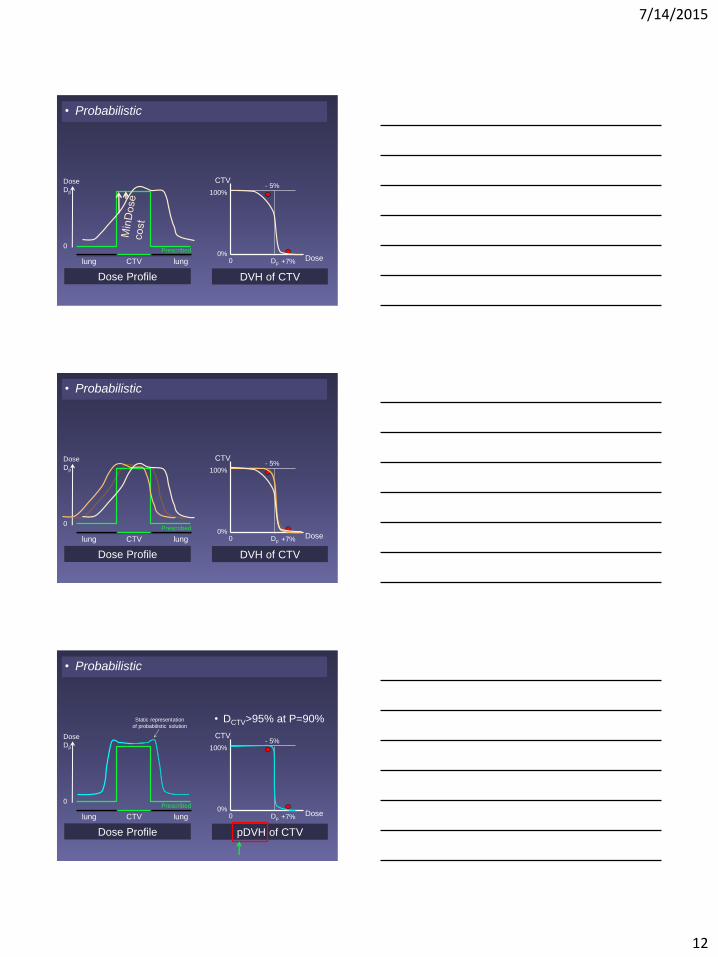
Probabilistic Treatment Planning
• Explicitly optimize using (Gaussian)
probability density functions S and s
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Static Planned
Prescribed
- 5%
+7%
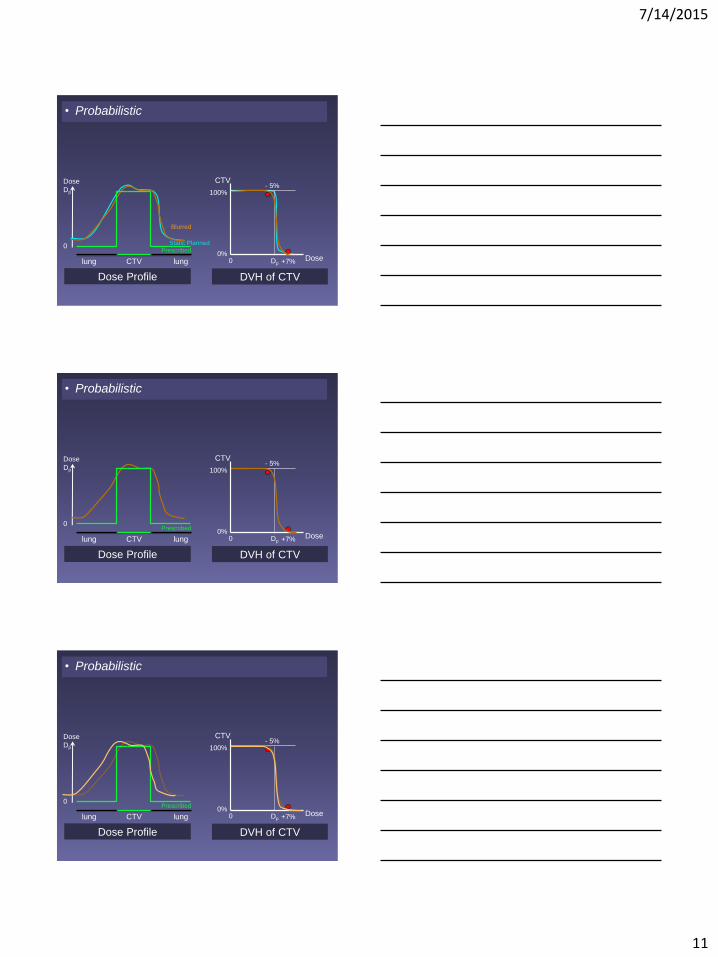
• Probabilistic
PTV
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Static Planned
Prescribed
- 5%
+7%
• Probabilistic
lung CTV lung
7/14/2015
11
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Static Planned
Prescribed
- 5%
+7%
Blurred
• Probabilistic
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Prescribed
- 5%
+7%
• Probabilistic
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Prescribed
- 5%
+7%
• Probabilistic
lung CTV lung
7/14/2015
12
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Prescribed
- 5%
+7%
• Probabilistic
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile DVH of CTV
Prescribed
- 5%
+7%
• Probabilistic
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile pDVH of CTV
Prescribed
- 5%
+7%
• Probabilistic
Static representation
of probabilistic solution
• DCTV>95% at P=90%
lung CTV lung
7/14/2015
13
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
Dose Profile pDVH of CTV
Prescribed
- 5%
+7%
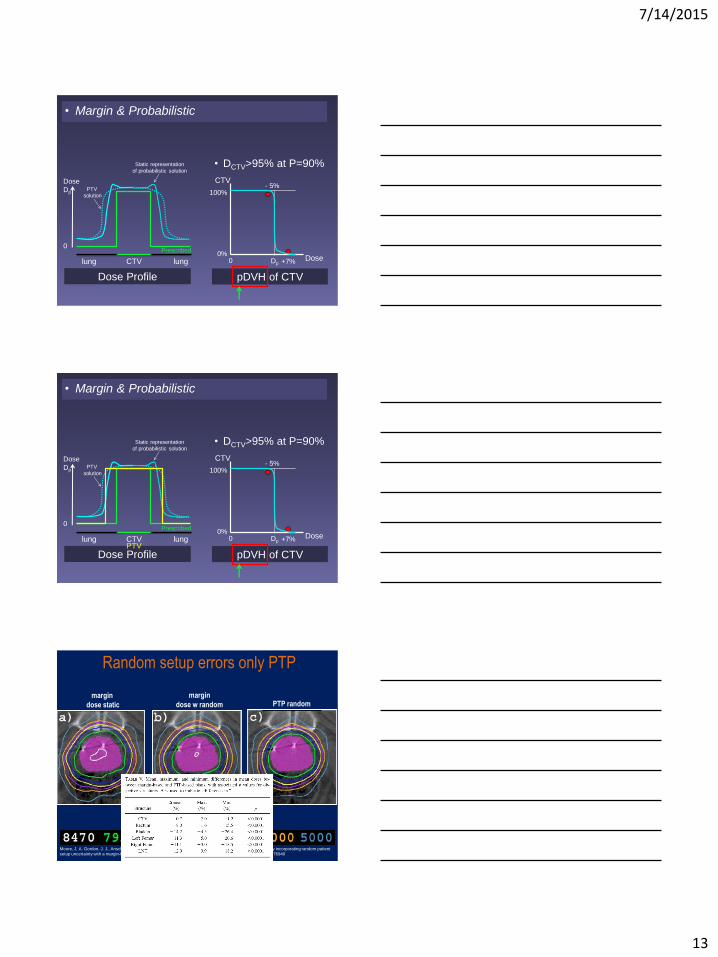
• Margin & Probabilistic
PTV
solution
Static representation
of probabilistic solution
• DCTV>95% at P=90%
lung CTV lung
CTV
0% 0
100%
Dp Dose
Dose
Dp
0
lung CTV lung
Dose Profile pDVH of CTV
Prescribed
- 5%
+7%
• Margin & Probabilistic
PTV
solution
Static representation
of probabilistic solution
• DCTV>95% at P=90%
PTV
Moore, J. A. Gordon, J. J., Anscher, M. S., & Siebers, J. V. (2009). Comparisons of treatment optimization directly incorporating random patient
setup uncertainty with a margin-based approach. Medical Physics, 36(9), 3880–3890. http://doi.org/10.1118/1.3176940
Random setup errors only PTP
margin
dose static PTP random margin
dose w random
7/14/2015
14
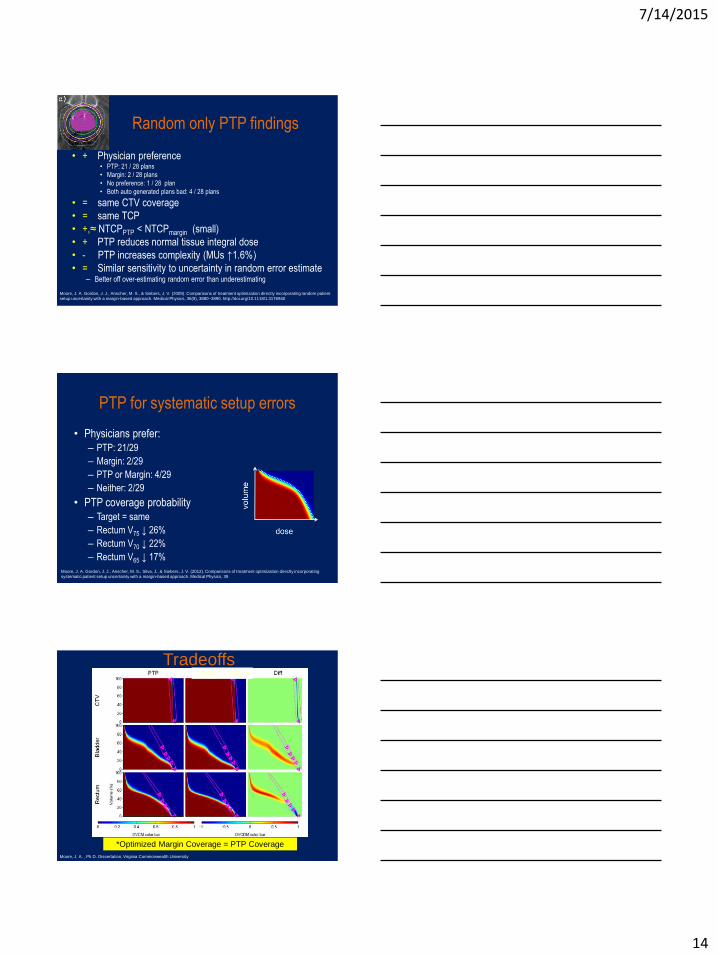
Random only PTP findings
• + Physician preference • PTP: 21 / 28 plans
• Margin: 2 / 28 plans
• No preference: 1 / 28 plan
• Both auto generated plans bad: 4 / 28 plans
• = same CTV coverage
• = same TCP
• +,≈ NTCPPTP < NTCPmargin (small)
• + PTP reduces normal tissue integral dose
• - PTP increases complexity (MUs ↑1.6%)
• = Similar sensitivity to uncertainty in random error estimate – Better off over-estimating random error than underestimating
Moore, J. A. Gordon, J. J., Anscher, M. S., & Siebers, J. V. (2009). Comparisons of treatment optimization directly incorporating random patient
setup uncertainty with a margin-based approach. Medical Physics, 36(9), 3880–3890. http://doi.org/10.1118/1.3176940
PTP for systematic setup errors
• Physicians prefer:
– PTP: 21/29
– Margin: 2/29
– PTP or Margin: 4/29
– Neither: 2/29
• PTP coverage probability
– Target = same
– Rectum V75 ↓ 26%
– Rectum V70 ↓ 22%
– Rectum V65 ↓ 17%
Moore, J. A. Gordon, J. J., Anscher, M. S., Silva, J., & Siebers, J. V. (2012). Comparisons of treatment optimization directly incorporating
systematic patient setup uncertainty with a margin-based approach. Medical Physics, 39
Tradeoffs Optimized Margin
*Optimized Margin Coverage = PTP Coverage
Moore, J. A. , Ph.D. Dissertation, Virginia Commonwealth University
7/14/2015
15
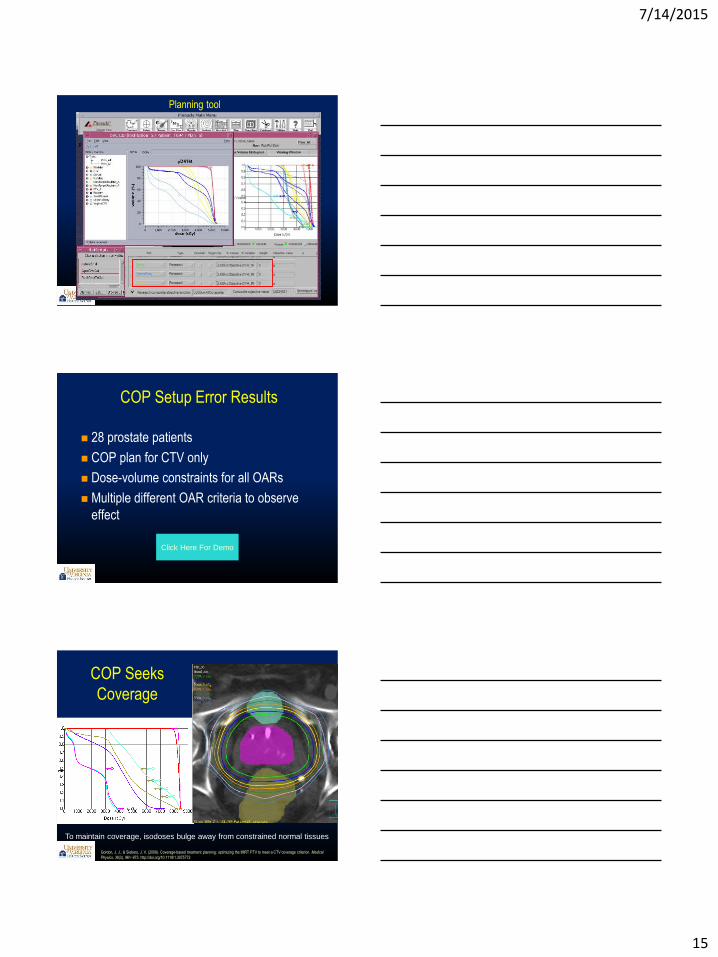
Planning tool
p
p
COP Setup Error Results
28 prostate patients
COP plan for CTV only
Dose-volume constraints for all OARs
Multiple different OAR criteria to observe
effect
Click Here For Demo
COP Seeks
Coverage
To maintain coverage, isodoses bulge away from constrained normal tissues
Gordon, J. J., & Siebers, J. V. (2009). Coverage-based treatment planning: optimizing the IMRT PTV to meet a CTV coverage criterion. Medical
Physics, 36(3), 961–973. http://doi.org/10.1118/1.3075772

7/14/2015
16
COP Seeks
Coverage
To maintain coverage, isodoses bulge away from constrained normal tissues
Gordon, J. J., & Siebers, J. V. (2009). Coverage-based treatment planning: optimizing the IMRT PTV to meet a CTV coverage criterion. Medical
Physics, 36(3), 961–973. http://doi.org/10.1118/1.3075772
COP Seeks
Coverage
To maintain coverage, isodoses bulge away from constrained normal tissues
Gordon, J. J., & Siebers, J. V. (2009). Coverage-based treatment planning: optimizing the IMRT PTV to meet a CTV coverage criterion. Medical
Physics, 36(3), 961–973. http://doi.org/10.1118/1.3075772
COP Seeks
Coverage
To maintain coverage, isodoses bulge away from constrained normal tissues
Gordon, J. J., & Siebers, J. V. (2009). Coverage-based treatment planning: optimizing the IMRT PTV to meet a CTV coverage criterion. Medical
Physics, 36(3), 961–973. http://doi.org/10.1118/1.3075772

7/14/2015
17
COP Seeks
Coverage
To maintain coverage, isodoses bulge away from constrained normal tissues
Gordon, J. J., & Siebers, J. V. (2009). Coverage-based treatment planning: optimizing the IMRT PTV to meet a CTV coverage criterion. Medical
Physics, 36(3), 961–973. http://doi.org/10.1118/1.3075772
NKI implementation
• Random errors
• Blurring of planned dose
• Voxel-specific kernel for
rotations/deformations
• Systematic errors
• ROI shift wrt dose
• Multiple ROI instances for
rotations/deformations
Margin based vs probabilistic
Cervix VMAT plan
PTV MinDose
Rotation point
90% conf CTV MinDose
Sagittal view
7/14/2015
18
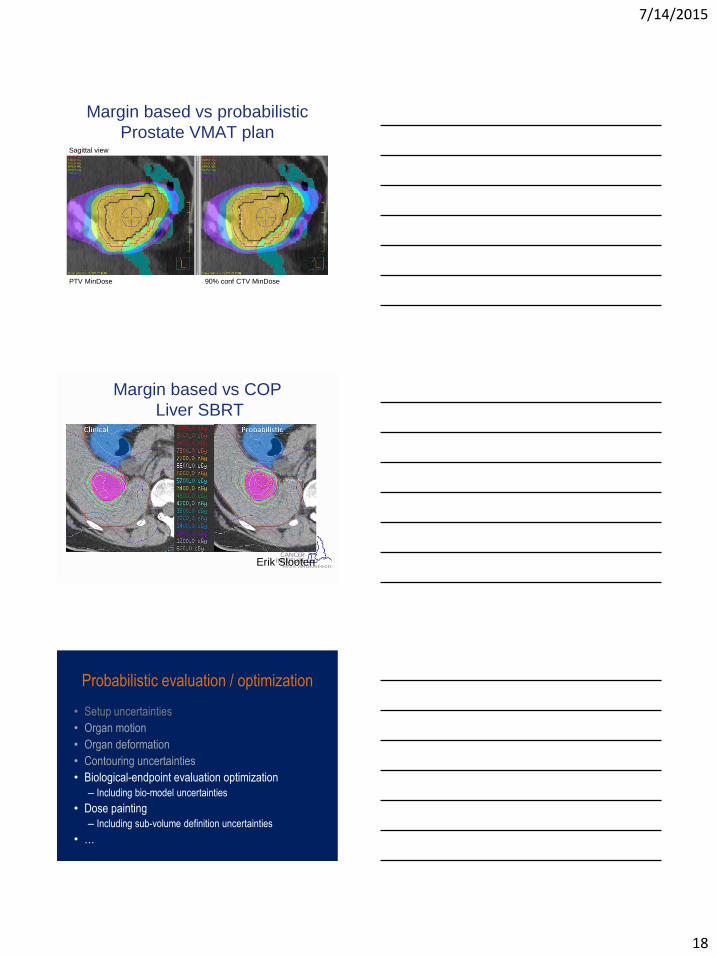
Margin based vs probabilistic
Prostate VMAT plan
Rotation point
PTV MinDose 90% conf CTV MinDose
Sagittal view
Margin based vs COP
Liver SBRT
Erik Slooten
Probabilistic evaluation / optimization
• Setup uncertainties
• Organ motion
• Organ deformation
• Contouring uncertainties
• Biological-endpoint evaluation optimization
– Including bio-model uncertainties
• Dose painting
– Including sub-volume definition uncertainties
• …
7/14/2015
19
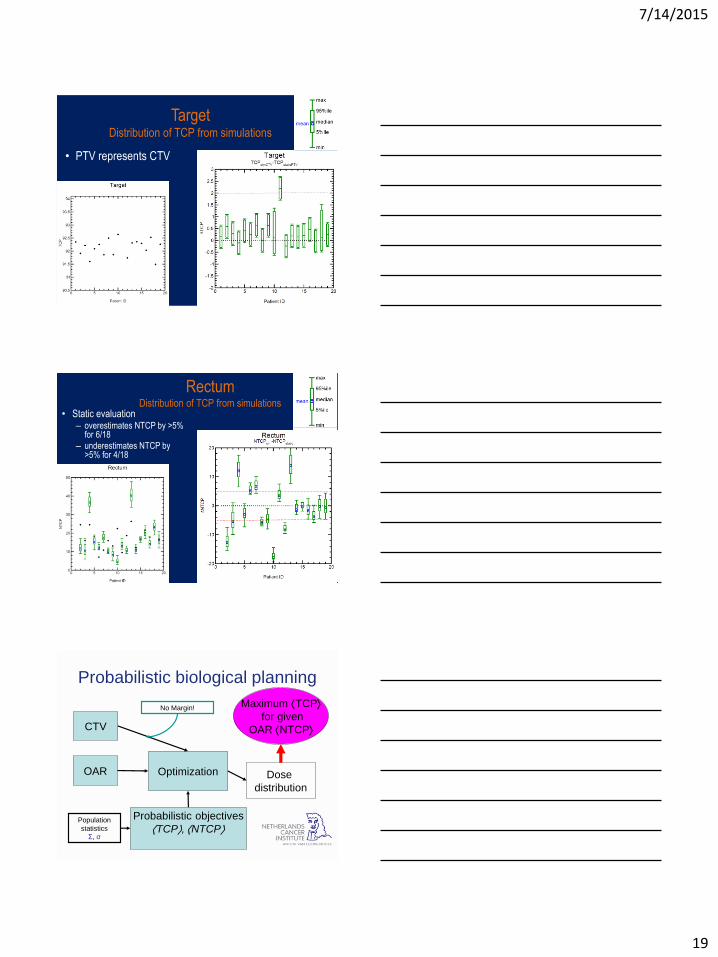
Target Distribution of TCP from simulations
• PTV represents CTV
Rectum Distribution of TCP from simulations
• Static evaluation – overestimates NTCP by >5%
for 6/18
– underestimates NTCP by >5% for 4/18
Probabilistic biological planning
CTV
Optimization
Probabilistic objectives
TCP, NTCP
Dose
distribution
Maximum TCP
for given
OAR NTCP
OAR
Population
statistics
Σ, σ
No Margin!

7/14/2015
20
Pinnacle ProbabilisticPainting Plugin
Georgy Shakirin, Matthieu Bal @Philips; Witte @NKI
Dose Level
SUV
66Gy
CTVmin
86Gy
CTVmax
Dose
Confidence Level (e.g. 0.90)
Probabilistic Dose Painting
Prostate VMAT plan
Rotation point
Tumor estimated from MRI 90% conf CTV DPBN
Sagittal view
Probabilistic biological painting NO_SUV
FDG-PET
GTV
CTV
TCP=45%
PET_SUV
GTV
CTV
TCP=64%
SUV α
α uniform
• Optimization on TCP, NTCP
– Non-uniform models: a(x), r(x), …
– Uncertainties on model parameters (sa)

7/14/2015
21
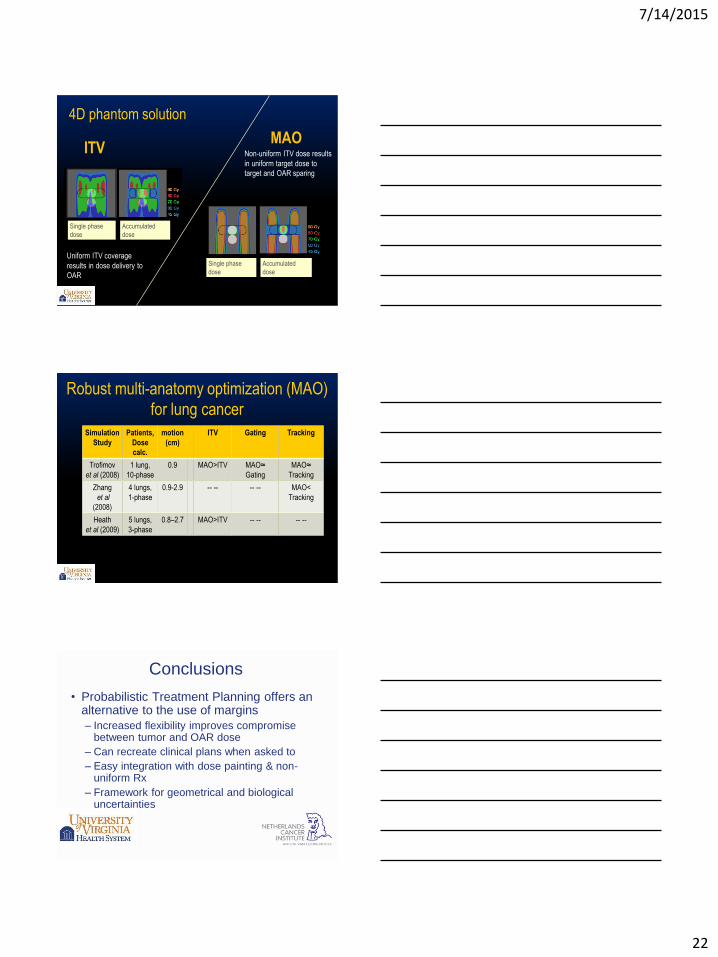
Robust lung optimization
Utilization of all 4DCT phases in plan optimization can
increase tumor dose and reduce normal tissue dose
compared with ITV method.
Multiple anatomy optimization (MAO).
MAO plan is delivered to moving anatomy
Multiple Anatomy Optimization (MAO)
Inverse planning of
dose-distributions to
treat 4D- anatomy
• Aperture does not need
to cover the entire ITV,
only needs to ensure
4D-dose is optimized
MAO aperture only needs to ensure dose to the
moving tumor, not entire ITV
MAO Flow
3-phase phantom: In phase 2, the moving target (green) is
aligned with the stationary OAR (red)
phase 1 phase 2 phase 3
7/14/2015
22
Uniform ITV coverage
results in dose delivery to
OAR
Non-uniform ITV dose results
in uniform target dose to
target and OAR sparing
MAO ITV
Single phase
dose
Accumulated
dose
Single phase
dose
Accumulated
dose
4D phantom solution
Robust multi-anatomy optimization (MAO)
for lung cancer
Simulation
Study
Patients,
Dose
calc.
motion
(cm)
ITV Gating Tracking
Trofimov
et al (2008)
1 lung,
10-phase
0.9
MAO>ITV MAO≈
Gating
MAO≈
Tracking
Zhang
et al
(2008)
4 lungs,
1-phase
0.9-2.9 -- -- -- -- MAO<
Tracking
Heath
et al (2009)
5 lungs,
3-phase
0.8–2.7 MAO>ITV -- -- -- --
Conclusions
• Probabilistic Treatment Planning offers an alternative to the use of margins
– Increased flexibility improves compromise between tumor and OAR dose
– Can recreate clinical plans when asked to
– Easy integration with dose painting & non-uniform Rx
– Framework for geometrical and biological uncertainties
7/14/2015
23
Why not in clinical use?
1. Clinical unawareness of coverage issues – Physicians believe of our plans
2. Requires change of thinking – Dose confidence level vs. DVHs
3. Requires vendor support – Vendor needs market
Acknowledgements
• Marnix Witte and NKI PTP Team
• My collaborators
– J.J. Gordon
– Joe Moore
– Huijun Xu
– …