respiratory motion aapm tg 76
TRANSCRIPT

Samir Laoui, Ph.D. UC, Irvine

Introduction
o Respiratory, cardiac and gastrointestinal
systems cause Intrafractional motion
o Respiratory motion management can improve
the treatment results of non-small-cell lung
cancer

Respiratory motion is both intra- and
inter-fraction motion
Inter-fraction motion
Intra-fraction motion

Scope
o The magnitude of respiratory motion
o Problems caused by respiratory motion
o Methods that have been used to mitigate
respiratory motion during RT

Problems associated with respiratory
motion during RT
o Image acquisition issues

Motion Induced Artifacts
o Respiratory organ motion can cause severe geometrical distortion in free breathing CT scanning
o Distortions along the axis of motion could either lengthen or shorten the target, kind of random
o In addition to shape distortion, the center of the imaged target can be displaced by as much as the amplitude of the motion

Problems associated with respiratory
motion during RT
o Image acquisition issues
George TY Chen, MGH

Problems associated with respiratory
motion during RT
o Issues during treatment planning
o Extended margins to account for motion
o Radiation delivery limitations
o Blurring of the static dose distribution over the
path of the motion
oWorse in IMRT delivery

Magnitude and measurement of
respiratory motion
o The lungs, esophagus, liver, pancreas, breast,
prostate, and kidneys, among other organs, are
known to move with breathing
Breathing pattern is never
reproducible which makes it
difficult to predict

Magnitude and measurement of
respiratory motion

Magnitude and measurement of
respiratory motion
Common issues for respiratory motion
management- Planning
o Motion artifact in the CT scan
o Daily variation of respiratory motion
o Organ volume changes
o Tumor growth and shrinkage
o Lung volume changes

Common issues for respiratory motion
management- QA
o When using gated or breath hold treatments,
the monitors have to be accurate and calibrated
o Instrument has to be calibrated routinely
o Patient training- Reproducible breath patterns
o Patient needs to be coached prior to simulation

IMRT
o Respiratory motion presents considerable
issues for IMRT delivery
o Up to 100% variation can be caused by
respiratory motion (Yu el al)
o Variation tends to average out with
fractionation
o Caution during SBRT
Methods used in the management of
respiratory motion
I. Motion-encompassing methods
II. Respiratory gated techniques
III. Breath-hold techniques
IV.Forced shallow-breathing methods
V. Real-time tumor-tracking methods
15

I. Motion encompassing methods
o During imaging, respiratory motion can be
accounted for by:
o Slow CT
o Inhale-Exhale breath-hold CT
o 4D CT
o It should be noted that extra dose comes with
the use of the above techniques

I. Motion encompassing methods: Slow
CT scanning
o The CT scanner is operated very slowly, and/or
multiple CT scans are averaged such that
multiple respiration phases are recorded per
slice
o Most available
o Loss of resolution due to motion blurring
o Increased dose

I. Motion encompassing methods:
Inhale and exhale breath-hold CT
o Acquire both inhale and exhale gated or
breath-hold CT scans
o Relies on the patient’s ability to hold his/her
breath reproducibly
o Maximum intensity projection (MIP) is
generated from the 2 individual scans for
planning purposes

I. Motion encompassing methods:
4DCT
o acquisition of a sequence of CT image sets over consecutive segments of breathing cycle
o Concept:
oAcquire CT images at all phases in a series of respiratory cycles
o Each image is tagged with breathing signal(time stamp)
owhen the scan is done, all the images of the selected phase are retrospectively organized to form 4D video images(3D+time).

I. Motion-encompassing methods:
4DCT
20

II. Respiratory gating methods
o Administration of radiation within a portion of
the patient’s breathing cycle “gate”
o The position and width of the “gate” is
determined using external respiration signal or
internal fiducial markers
o Can result in a decrease of margins
o There are 2 types: displacement and phase
gating

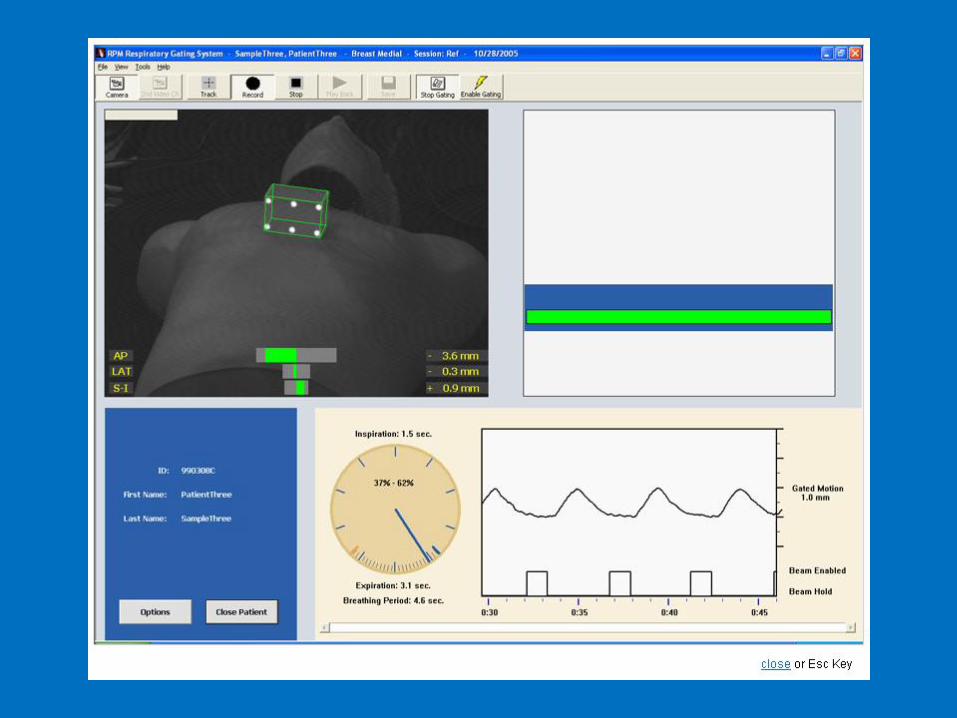
II. Respiratory gating methods
o Most widely used solution developed by
Varian is the RPM (real time position
management) system.
o An infrared reflective plastic box is placed on
the patient’s anterior abdominal surface,
typically midway between the xyphoid process
and the umbilicus.

II. Gating using an external respiration signal
o Patient related quality assurance o Time-dependent internal target position will not match the
respiration monitoring.
Comparison of external marker block motion with internal motion of the clinical target
volume (CTV) for a patient with (a) no phase shift and (b) a patient with significant
phase shift. The respiratory gating thresholds are set using the external marker block
motion. The beam-on pulses are highlighted in red over the internal CTV position. 24

II. Gating using internal fiducial
markers
o Invasive
o Implanted fiducial markers in or near the
tumor for real time tracking
o Fiducial position is tracked in all 3D several
times a second using a pair of stereotactic KV
–x-rays
25

II. Gating using internal fiducial
markers

III. Breath hold methods
o Used primarily for lung treatment
o Breath hold techniques
oDeep-inspiration breath hold
oActive breathing control
o Self-held breath hold without monitoring
o Self-held breath hold with monitoring

III. Breath hold methods: Deep-Inspiration
Breath-Hold (DIBH)
o For thoracic tumors, DIBH helps in
reproducing a state of maximum breath hold
oMinimize dose to OAR
o Involves spirometer
oWas developed by MSKCC in late 90’s
o Limited by patient compliance
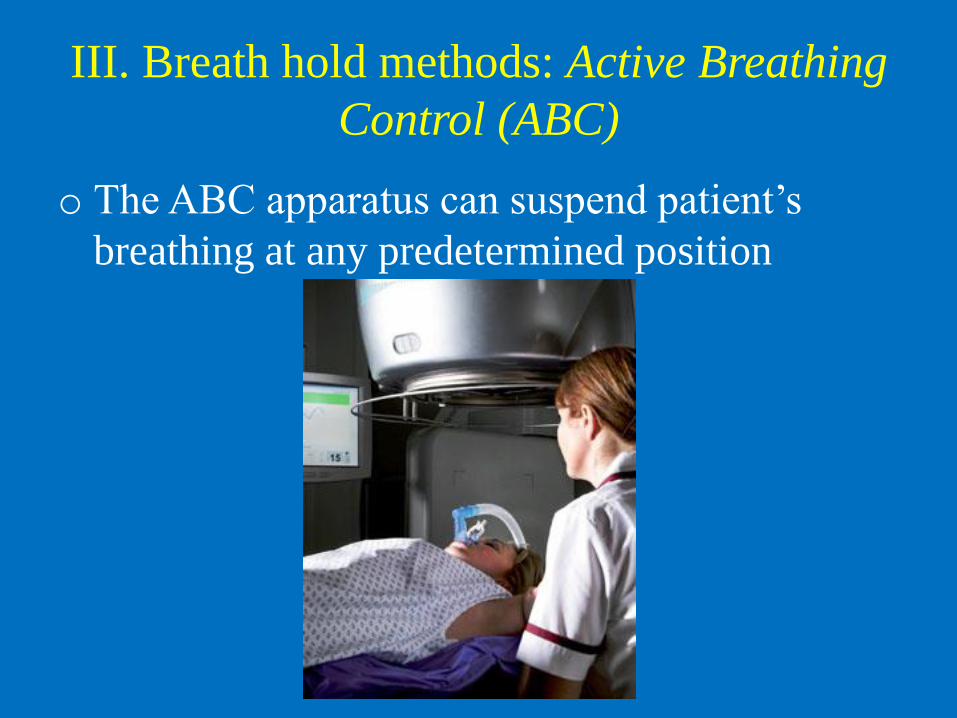
III. Breath hold methods: Active Breathing
Control (ABC)
o The ABC apparatus can suspend patient’s
breathing at any predetermined position

III. Breath hold methods: Active
Breathing Control (ABC)
o Moderate deep inspiration breath-hold (DIBH)
at 75% to 80% of maximum inspiration
capacity to displace of thoracic contents and
avoid tiring the patient
o Patient selection; long breath-hold (>15 sec) is
desirable
o Therapists involve in verbal coaching

III. Breath hold methods: Self-held breath
hold without external monitoring
o Although only the therapist is allowed to turn
the beam on, the patient is given the ability to
release a treatment interlock
o Depends highly on patient compliance

III. Breath hold methods: Self-held breath
hold with external respiratory monitoring
o It is RPM based technique
o Patient is coached to hold breath at a specified
part of the respiratory cycle
o Depends highly on patient compliance
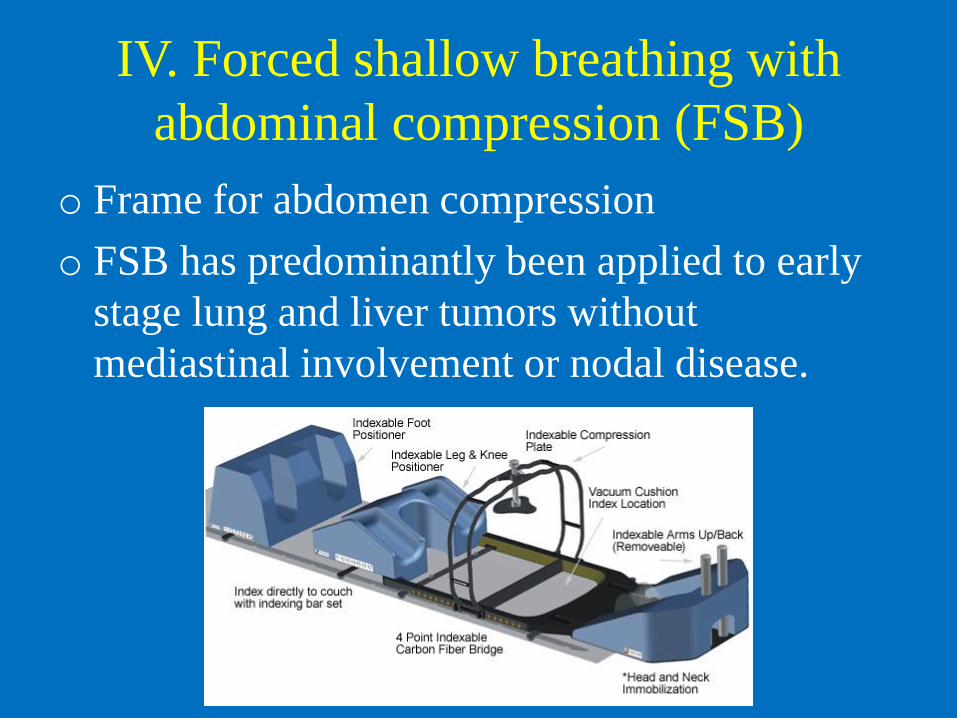
IV. Forced shallow breathing with
abdominal compression (FSB)
o Frame for abdomen compression
o FSB has predominantly been applied to early
stage lung and liver tumors without
mediastinal involvement or nodal disease.

V. Real time tracking methods
o Reposition the radiation beam dynamically so
as to follow the tumor’s changing position
o Identify tumor position in real time
oAnticipate tumor motion
o Reposition the beam
oAccount for lung volume changes and OAR
location

V. Real time tracking methods
o Tumor position
o Real time imaging of tumor itself (Fluoroscopy)
o Fiducials (High Z)
o Surrogate breathing signal
oNon-radiographic tumor tracking (Calypso)
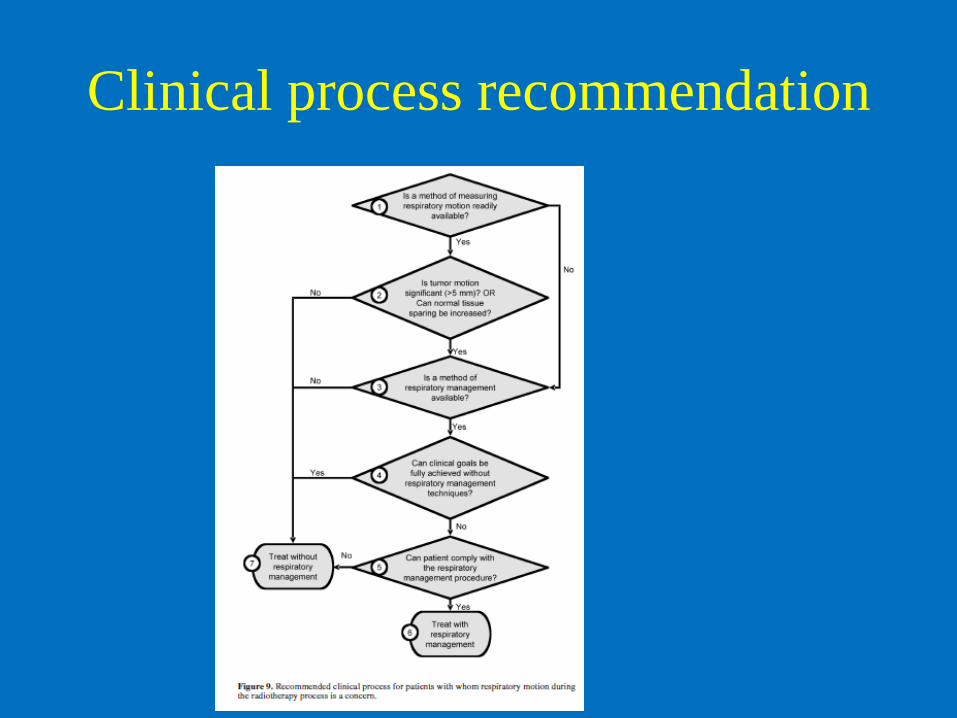
Clinical process recommendation

Treatment planning recommendation
oWhen deriving CTV/PTV:
oAccount for image distortion due to respiratory motion
o If a structure is used as a surrogate, the displacement
and phase relationship between structure and tumor can
have uncertainties which have to be accounted for
o Irregularities in breathing cycles have to be accounted
for
oMargins have to be increased in the absence of a
respiratory motion device

Other recommendations
oWhen a respiratory management device is used, a
qualified medical physicist has to be present
o Strict QA procedures for the imaging, planning,
and delivery of radiotherapy using respiratory
management devices are required to ensure the
safe and effective use of these devices

The end