nicola taddio arezzo nicolas foundation 2011 shoulder cadaver lab
TRANSCRIPT

Nicola Taddio, Physical Therapist, BPT, OMTP, ATCMasters Degree in Science of Health and Rehabilitation Professions
First Level Master IFOMT in Manual Therapy and Musculo-Skeletal Rehabilitation, University of Padua, ItalyLecturer a.c. Master in “Sports Physioterapy”, University of Siena, Italy
Lecturer a.c. Master in “Sports Physiotherapy and Performing Arts”, University of Genoa, Savona pole, Italy
www.fisioterapiafkt.com [email protected]

Acknowledgements

The interpretation of diagnostic test: a primer for physiotherapists.Davidson M.
Aust J Physiother. 2002;48(3):227-32. Review.
Shoulder girdle:physical examination of
passive structures

Introduction

• Gleno-humeral• Acromion-clavicular• Sterno-clavicular
• Scapulo-toracic• Sub-acromion deltoid
“SHOULDER COMPLEX”
complex of 5 joints
Anatomicaljoints(properlydefined)
Muscletendonsfasciae slide one eachother, on the toraxand ribs

Kinetic Chain Role
John McMullen, MS, ATC*; Timothy L. Uhl, Phd, ATC, PT A Kinetic Chain Approach for Shoulder Rehabilitation
Journal of Athletic Training 2000:35(3):329-337
1. Any movement of upper limbs generate a “PRE-ACTIVATION” (anticipatory contraction) of
deep lumbo-pelvic muscle
2. Therefore, the sequence of muscular activation
begin from “CORE” to periferic joint (proximal to
distal)
3. The rationale in shoulder rehabilitation is
“INTEGRATE, FROM THE BEGINNING”, the exercises of trunk and lower
limbs in the exercise of upper limb and shouldercomplex

Mobility with Stability

Stability and instabilityClinical spinal instability and low back pain.
Panjabi MM.J Electromyogr Kinesiol. 2003 Aug;13(4):371-9.
ActiveSystem
• Musculoskeletal
• Stiffness
• Force/resistence/power
Passive System
• Bone surfaces
• Ligaments
• Labrum
ControlSystem
• Nervous System
• Central and Peripheral

Lee SB, Kim KJ, O'Driscoll SW, Morrey BF, An KN.Dynamic glenohumeral stability provided by the rotator cuff muscles in the mid-range and
end-range of motion. A study in cadavera.J Bone Joint Surg Am. 2000 Jun;82(6):849-57.
Curl LA, Warren RF.Glenohumeral joint stability. Selective cutting studies on the static capsular restraints.
Clin Orthop Relat Res. 1996 Sep;(330):54-65. Review.
The glenohumeraljoint relies on static
and dynamic contributions of the local soft tissues
to maintain joint stability.Dynamic stabilizers consist of the local
musculature (the rotator cuff and periscapular
muscles), whereas static stabilizers include the glenoid labrum and associated capsulo
ligamentous components.

1. Ligaments [CHL, SGHL, MGHL, IGHL (AB, PB, AP)]
2. Capsule (AX.P, P)
3. Labrum
4. Gleno-humeralcongruency
5. Concavity compression
6. Adhesion-cohesionmechanism
7. Neuromuscular balance
8. Proprioception and neuromuscular control
MOBILITY with STABILITY

Why and How instability
LAXITY
INSTABILITYIPER-LAXITY
SIGNS SIMPTOMS
NORMAL
PATHOLOGICAL

History and clinical picture
TRAUMA OVERUSELAXITY

Unstable Shoulder Picture
T.U.B.S.
OVERUSELAXITYT.RAUMATIC A.TRAUMATIC A.CQUIRED
U.NIDIRECTIONAL M.ULTIDIRECTIONAL I.NSTABILITY
B.ANKART B.ILATERAL O.VERSTRESSED
S.URGERY R.EHABILITATION S.HOULDER
R.EPAIR S.URGERY
I.NTERVAL
TRAUMA
A.M.B.R.R.I A.I.O.S.S.

Burkart AC, Debski RE.Anatomy and function of the glenohumeral ligaments in anterior shoulder instability.
Clin Orthop Relat Res. 2002 Jul;(400):32-9. Review.
1. The function of glenohumeral ligaments is highly dependent on the position of the humerus with respect to the glenoid.
2. The coracohumeral ligament with superior glenohumeral ligament the was shown to be an important stabilizer in the inferior direction.
3. The middle glenohumeral ligament provides anterior stability at 45 degrees and 60 degrees abduction whereas
4. The inferior glenohumeral ligament complex is the most important stabilizer against antero-inferior shoulder dislocation.
5. Therefore, this component of the capsule is the most frequently injured structure.
6. In addition, a detached labrum can lead to recurrent anterior instability and a compromised inferior glenohumeral ligament complex.
Bankart
SLAP
PB AP AB

Wang VM, Flatow EL.Pathomechanics of acquired shoulder instability: a basic science perspective.
J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):2S-11S. Review.
1. Normal asymptomatic glenohumeral motion is dependent on the coordinated function of dynamic and static stabilizers.
2. Data from both selective sectioning studies of the capsuloligamentouscomponents and tensile testing of the inferior glenohumeral ligament have provided important insights into the in situ function of these structures.
3. However, little is known regarding the mechanism of microdamageaccumulation in acquired shoulder instability.
4. Recent findings suggest that cyclic subfailure loading of the inferior glenohumeral ligament may induce gradual stretching of the anteroinferior capsule, compromising its capacity to restrain excessive humeral translations.

The interpretation of diagnostic test: a primer for physiotherapists.Davidson M.
Aust J Physiother. 2002;48(3):227-32. Review.
Shoulder girdle:physical examination of
passive structures

E.B.M. approach to orthopaedicclinical examination
Reliability [true and error about test or measure (intra and
inter examiner) acceptable reliability] = affidabilità, attendibilità
Diagnostic accuracy (comparison between golden
standard to clinical test) = accuratezza, esattezza, precisione diagnostica2x2 Contingency TableOverall AccuracyPos. and Neg. Predictive Value
Sensitivity = detect people have disorder or tear
Specificity = detect people don’ t have disorder or tear
Likelihood RatioConfidence IntervalPre-Test and Post-Test ProbabilityCalculating Post-Test ProbabilityAssessment of Study Quality

Clinicalexamination to
assess the baselinefunction and
the rehabilitativeprogram progresses
or outcome
Physical Therapist Orthopaedic Surgeon
Clinicalexamination to
assess if the patientand lesion need the
surgical or conservative
approach

Labrum and Biceps Anchor
Definition• The labrum is a firm ring of fibro-
cartilage that surrounds the edge ofglenoid
• It serves two pupose: 1. it increase the depth and size of
glenoid fossa, giving the joint greaterstability and surface area;
2. it acts a “chock block” to stop the humeral head from translating off the glenoid
• The term labral tear is used to classifyseveral types of labral injury, the mostcommon is Bankart lesion and SLAPlesion

Suspected injuries
• Labral tear (traumatic)
• Labral lesion (degenerative)
• Bankart lesion (in which the antero-inferior labrum is torn)
• SLAP lesion (in which the superioranterior or posterior or both may havebeen injuried)

Labrum tearsBANKART SLAP TYPE 2°
BONY BANKART

Epidemiology and demographics
• The most common cause of labral tear istrauma from a dislocation
• In addition, younger individuals are prone tolabral injury with repetitive overhead motion, such as swimming, tennis or throwing
• Older people are more prone to degenerative lesions, which often are associated with poorvascular supply to the labral tissue

Relevant special tests• Active compression test of O’Brien• Anterior slide test• Biceps tension test• Clunk test• Biceps load test• Labral crank test• SLAP prehension test
Note: no one test can provide a definite diagnosis of labral lesion
Parentis MA, Glousman RE, Mohr KS, Yocum LA.An evaluation of the provocative tests for superior labral anterior posterior lesions.
Am J Sports Med. 2006 Feb;34(2):265-8.

Active compression test of O’Brien• Purpose = assess the integrity of superior aspect of the shoulder labrum
• Patient position = standing, arm forward flexed to 90° and the elbowfully extended
• Examiner position = stands slightly behind and adjacent to the test shoulder
• Test procedure = the examiner puts one hand on the patient’s shoulderto stabilize the scapula and clavicle and the other hand on the forearmof the affected arm. The arm is horizintally adducted 10° to 15° (startingposition) and intrarotated with the thumb faces downward (pronated). The examiner applies a downward eccentric force to the arm. The arm isreturned to the starting position, the thumb is upward (supination) and the downward eccentric load is repeated.
• Indication of a positive test = if pain or painful clicking is producedinside the shoulder(not over the A/C joint) in the first part of the test (intrarotation) and eliminated or decreased in the second part (extrarotation), the trest is considered positive for labral abnormalities
• Clinical note/caution = the test also “locks and loads” the A/C joint in I/R
• Reliability/Specificity/Sensitivity =
Specificity: 31% to 99% Sensitivity: 54% to 00%

Anterior Slide Test• Purpose = assess the integrity of anterior shoulder
labrum
• Patient position = sitting or standing, with the hands on the waist, thumbs posterior
• Examiner position = standing behind, stabilizescapula and clavicle and with the samehand/fingers palpate the humeral head. The otherhand on the posterior aspect of elbow
• Test procedure = the examiner applies ananterosuperior force at the patient’s elbow
• Indication of a positive test = if labrum is torn(SLAP lesion) the humeral head slides over the labrum with a pop or crack and with pain or painfulclicking. Sometimes is possible to palpate anteriorsuperiorly the pop or click/crack
• Reliability/Specificity/Sensitivity = Specificityrange: 85% to 91,5% Sensitivity range: 8% to 78%

Biceps Tension Test• Purpose = to assess for a lesion of the superior
shoulder labrum
• Patient position = the patient standing, abduct
and externally rotates the shoulder, the elbow
fully extended, the forearm supinated
• Examiner position = standing behind, stabilizescapula and clavicle and with the samehand/fingers palpate the humeral head. The otherhand grasp the wrist and forearm
• Test procedure = the examiner applies an eccentric adduction force tothe straightened and supineted arm
• Indication of a positive test = the test is positive if labrum is torn (SLAP lesion) and we see a reproduction of patient’ s symptoms
• Clinical note/caution = the test stress also the biceps tendon and thenSpeed test should be done di differential diagnosis
• Reliability/Specificity/Sensitivity = Unknown

Clunk Test• Purpose = to assess the integrty
of anterior shoulder labrum
• Patient position = the patientlies supine
• Examiner position = standing adjacent and superior to the shoulder to be tested
• Test procedure = the examiner places one hand under the posterior aspect ofthe shoulder so that it lies under the humeral head; the other holds the humerus above the elbow. The examiner fully abducts the arm over the patients head and push anteriorly the hand or the fist while the other handexternally rotates the humerus at the shoulder level
• Indication of a positive test = a clunk or grinding sound indicates both a positive test result and a labral tear. The test also may cause apprehension ifanterior instability is present
• Clinical note/caution = the test stress different parts of labrum if arm ispositioned in different amount o abduction (if done in adduction relocation)
• Reliability/Specificity/Sensitivity = Unknown

Biceps Load Test
• Purpose = to assess for a lesion of the superior
shoulder labrum
• Patient position = the patient lies supine, with the shoulderabducted 90° and externally rotates, the elbow 90° flexed, the forearm supinated
• Examiner position = the examiner stands slightlysuperiorly and adjacent to the test shoulder
• Test procedure = the examiner holds the patient’s elbow for support with onehand and grasp the wrist with the other hand, perform an apprehension test by a fully external rotoation. If apprension appears the examiner stops the E/R and hold the position and ask the patient flex the elbow against the examinerresistence
• Indication of a positive test = the test is positive if elbow flexion reproduce the patient’ s symptoms (pain and apprension) and negative if decreaseapprension and pain
• Reliability/Specificity/Sensitivity = Specificity 96,6% Sensitivity 89%
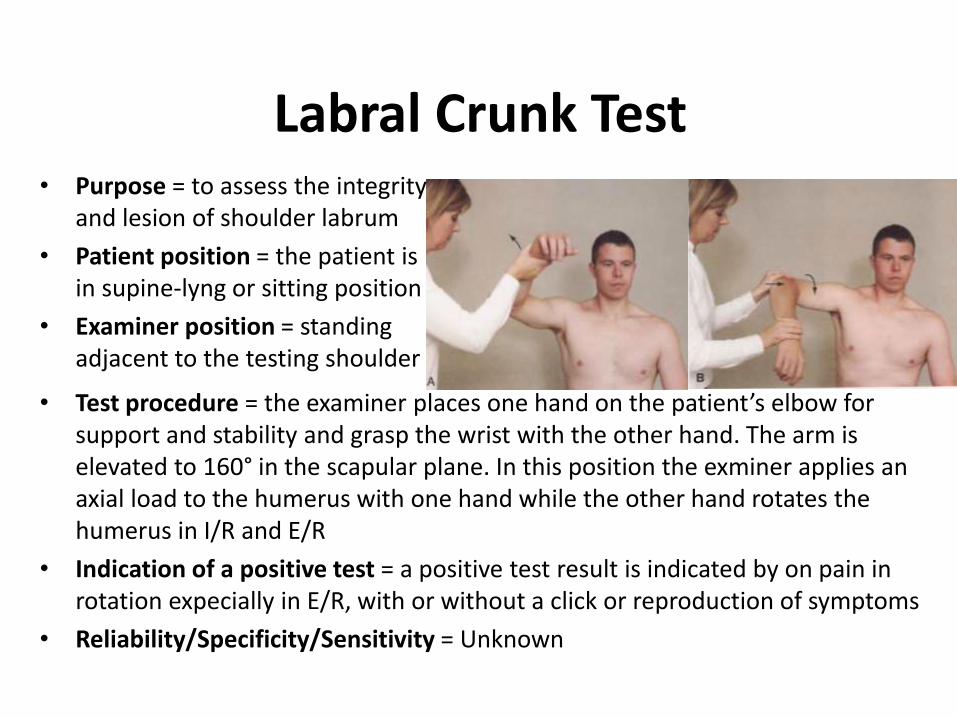
Labral Crunk Test• Purpose = to assess the integrity
and lesion of shoulder labrum
• Patient position = the patient isin supine-lyng or sitting position
• Examiner position = standing adjacent to the testing shoulder
• Test procedure = the examiner places one hand on the patient’s elbow for support and stability and grasp the wrist with the other hand. The arm iselevated to 160° in the scapular plane. In this position the exminer applies anaxial load to the humerus with one hand while the other hand rotates the humerus in I/R and E/R
• Indication of a positive test = a positive test result is indicated by on pain in rotation expecially in E/R, with or without a click or reproduction of symptoms
• Reliability/Specificity/Sensitivity = Unknown

SLAP Prehension Test
• Purpose = to assess for a lesion of shouldersuperior labrum
• Patient position = the patient is in standing or sitting position
• Examiner position = standing behind and adjacent to the testing shoulder
• Test procedure = the examiner places one hand on the patient’s shoulder tostabilize scapula and clavicle and holds the wrist with the other hand. The examiner abduct the arm to 90° in the scapular plane with the elbowextended and yhe forearm pronated (thumb down and shoulder in I/R). The patient then, is asked to adduct the arm orizzontally. The movement isrepeated with the forearm supinated (the thumb up and the shoulder in E/R)
• Indication of a positive test = if patients feel pain in the bicipital groove withpronation and lessens or absent with supination, the test is positive for SLAP
• Reliability/Specificity/Sensitivity = Unknown

Inferior Gleno HumeralLigament (IGHL)

Curl LA, Warren RF.Glenohumeral joint stability. Selective cutting studies on the static capsular restraints.
Clin Orthop Relat Res. 1996 Sep;(330):54-65. Review.
The function of the capsuloligamentous restraints is highly
dependent on arm position

Debski RE, Weiss JA, Newman WJ, Moore SM, McMahon PJ.Stress and strain in the anterior band of the inferior glenohumeral ligament during a
simulated clinical examination.J Shoulder Elbow Surg. 2005 Jan-Feb;14(1 Suppl S):24S-31S.

Relevant special tests
Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests.
Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT 3rd, Cook C.Br J Sports Med. 2008 Feb;42(2):80-92; discussion 92. Epub 2007 Aug 24. Review.
•Load and Shift Test (Anterior)•Crank Apprehension Test (Relocation Test)•Rockwood Test (Modification of Crank Test)•Fulcrum Test (Modification of Crank Test) •Load and Shift Test (Posterior)•Norwood Stress Test•Posterior Apprehension or Stress Test•Sulcus Sign•Feagin Test
AnteriorInstability
PosteriorInstability
Inferior and/or Multidirectional
Note: no one test can provide a definite diagnosis of capsulo-ligamentous lesion
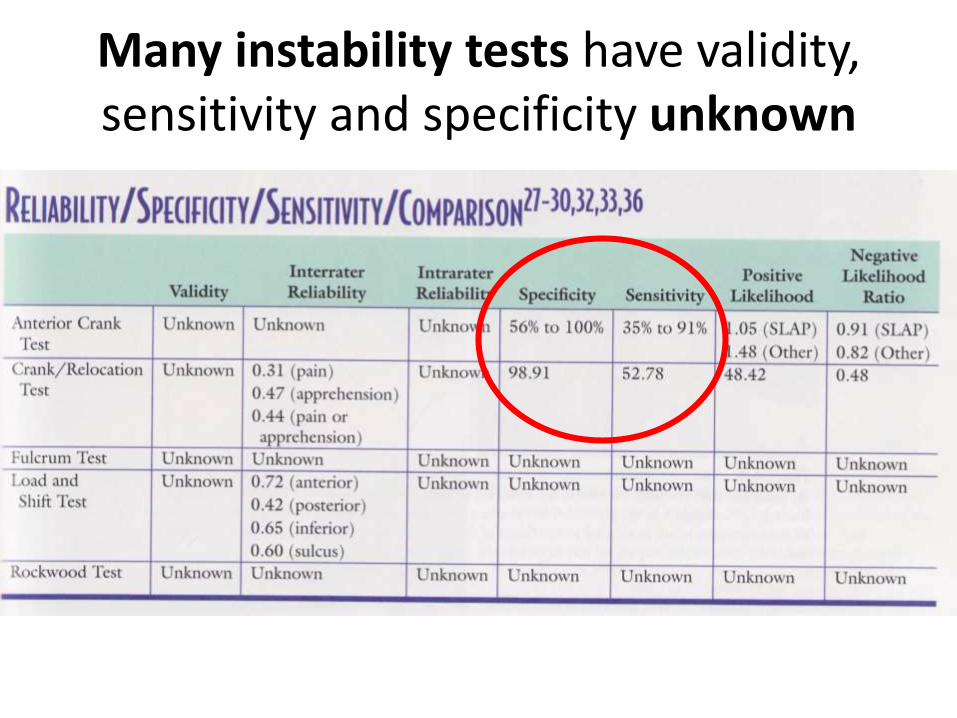
Many instability tests have validity, sensitivity and specificity unknown

Crank Apprehension Test (Relocation Test)
• Purpose 1 = to determine whether the humerus will sublux or dislocate anteriorly out of the glenoid
• Purpose 2 = to differentiate between dislocation/subluxation(apprehension) and impingement (pain)
• Purpose 3 = to differentiate between instability and impingement(relocation part of the test)

Crank Apprehension Test (Relocation Test)
• Patient position = the patient lies supine, with the shoulderabducted 90° and externally rotates, the elbow 90° flexed, the forearm pronated. The test arm is close to the edge ofthe couch
• Examiner position = the examiner stands at the patient’s side facing to the test shoulder

Crank Apprehension Test (Relocation Test)
• Test Procedure
• Step 1 The Crank Test
• Step 2 The Relocation test

Crank Apprehension Test (Relocation Test)
• Specificity Range: 56% to 100%
• Sensitivity Range: 35% to 91%

Medium Gleno HumeralLigament (MGHL)

Relevant special tests
The middle glenohumeral
ligament provides anterior stability at 45 degrees
and 60 degrees abduction whereas
Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests.
Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT 3rd, Cook C.Br J Sports Med. 2008 Feb;42(2):80-92; discussion 92. Epub 2007 Aug 24. Review.
Note: no one test can provide a definite diagnosis of capsulo-ligamentous lesion
?

Superior Gleno HumeralLigament (SGHL)

Relevant special tests
?Physical examination tests of the shoulder:
a systematic review with meta-analysis of individual tests.Hegedus EJ, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman CT 3rd, Cook C.
Br J Sports Med. 2008 Feb;42(2):80-92; discussion 92. Epub 2007 Aug 24. Review.
Note: no one test can provide a definite diagnosis of capsulo-ligamentous lesion
Coraco Humeral Ligament (CHL)

Relevant special tests
?The coracohumeral ligament with superior glenohumeral ligament the was shown to be an important stabilizer in the inferior direction.
Anatomy of the superior glenohumeral ligament.Kask K, Põldoja E, Lont T, Norit R, Merila M, Busch LC, Kolts I.
J Shoulder Elbow Surg. 2010 Sep;19(6):908-16.

Rotator Interval

Relevant special tests

SURGICAL FINDINGSThe addition of an arthroscopic rotator interval closure after posterior
capsulolabral repair did not improve posterior stability; however, anterior stability was improved further after a rotator interval closure.
Inferior stability was not improved. Arthroscopic rotator interval closure significantly decreased external rotation at both neutral and
abducted arm positions.
CLINICAL RELEVANCEArthroscopic closure may be beneficial in certain cases of
anterior shoulder instability; however, posterior instability was not improved. Predictable losses of external rotation after rotator interval
closure are of concern.
Mologne TS, Zhao K, Hongo M, Romeo AA, An KN, Provencher MT.The addition of rotator interval closure after arthroscopic repair of either anterior or
posterior shoulder instability: effect on glenohumeraltranslation and range of motion.
Am J Sports Med. 2008 Jun;36(6):1123-31. Epub 2008 Mar 4.

Posterior Capsule(PC)

Posterior capsular contracture of the shoulder.Bach HG, Goldberg BA.
J Am Acad Orthop Surg. 2006 May;14(5):265-77. Review.
• Common cause of shoulder pain in which the patient presents with restricted internal rotation and reproduction of pain.
• Increased anterosuperior translation of the humeral head occurs with forward flexion and can mimic the pain reported with impingement syndrome; however, the patient with impingement syndrome presents with normal range of motion.
• In the throwing athlete, repetitive forces on the posteroinferior capsule may cause posteroinferior capsular hypertrophy and limited internal rotation.
• This may be the initial pathologic event in the so-called dead arm syndrome, leading to a superior labrum anteroposterior lesion and, possibly, rotator cuff tear.
Posterior Capsular Contracture

Relevant special tests
Note: no one test can provide a definite diagnosis of labral lesion
Parentis MA, Glousman RE, Mohr KS, Yocum LA.An evaluation of the provocative tests for superior labral anterior posterior lesions.
Am J Sports Med. 2006 Feb;34(2):265-8.

Thanks for yourkind attention
science explain what is possible to make
ethics tell us what is right (Socrates)la scienza spiega cio’ che e’ possibile fare,
l’etica dice cio’ che e’ giusto fare (Socrate)