o ne ropuiation rrogram of tne government of...
TRANSCRIPT

Report No. PP-13a I1; L.lln;s W J u
o ne ropuiation rrogram of tneGovernment of MalaysiaA Sector Rev@ewSeptember 6, 1974
rPopulation andU NOutritionProjects Department
Nolt for Public Use
Document of the International Bank for Reconstruction and Developmentinternational DeveLopment Association
This report; was prepared for official use only by the Bank Group. It may notbe published. quoted or cited without Bank Group authorization. The Bank Croup doesnot accept: responsibility for the accuracy or completeness of the report.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized


T-n POP-U-LATION PKOGKAM OF T-HE GuVEIRN'NL OF M¶ALAXYSIA
A SECTOR REVIEW
Table of Contents
Page No.
PREFACE ..... .......................................... i-ii
I. DEMOGRAPHIC TRENDS . ................................... i
II. ORGANIZATION OF THE NATIONAL FAMILY PLANNING PROGRAM .. 4
A. Existing Situation ............................... 4
B. Limitations of the Existing Organization .... ..... 6
C. Recommendations . . ................................ 7
III. ACHIEVEMENT OF THE PROGRAM ........................... 8
A. New Acceptors .................................... 8
B. Impact of Knowledge, Attitude and Practice ... .... 9
C. Births Averted ....... ............................ 10
IV. DELIVERY SYSTEM OF SERVICE ........... .. ............... 15
A. Existing Situation ................................ 15
Be Limitations of the Delivery System .... ........... 22
C. Recommendations .................................. 24
V. AVAILABILITY AND TRAINING OF HEALTH PERSONNEL ......... 27
A. Existing Situation ............................... 27Be Limitations - .... ................. 31
C. Recommendations ................. 33
VI. INFORMATION, EDUCATION AND COMMUNICATIONS . .36
A. Review of Existing Program and Facilities .36Be Limitations of the Co mmrications Program .37C. Recommendations .. 38De Renuired Inuts ....................... 41
This report is based on the findings of the preappraisal and appraisal missionS
which visited Malaysia from November 1-22, 1971 and February 21 to March 21,
1972. The preappraisal mission consisted of Miss I. Z. Husain, Dr. T. I. Kim,
Mr. Robert Blake (consultant), Mr. Roger Mellem (consultant), Dr. J. Y. Perng
(consultant), and Miss S. Piso Joo. The appraisal mission was comprised oi
Miss I. Z. Husain, Dr. T. I. Kim, Mr. J. Burfield, Dr. Leslie Corsa (WHO),
Miss Verderese (WHO), and Messrs. Royal Colle (consultant), J. Y. TakeshitaL(consultant) and M. Milo (consultant). This report was prepared by Miss Husain
and Dr. Kim.

TABLE OF CONTENTS (Cont'd)
VII. EVALUATION OF THE PROGRAM ............... .. ............ 44
A. Existing Situation ............................... 44B. Limitations of the Existing E-va-uatioL System .... 46C. Recommendations for Improving the Evaluation
System ......................................... 47
VIII. PPULATIOUN RESER FACILITIES ........................ 51
A. Tne Need for Population Studies Capabilities inMalaysia .................. ..................... 51
B. Existing Facilities ...... ................ 53C. Recommendations ................ .............. 53
IX. FINANCES .......... .................................... 56
ANNEXES
1. Population Size and Growth Rate, 1911-732. Population Projections with Constant Fertility, 1975-19993. Area, Population and Density by States, 19704. Percentage of Rural Population by State, 19705. Distribution of Population by Ethnic Group and by Urban and
Rural Areas, 1957, 1967, and 19706. Age Structure of Population, 1957-19697. Fertility Rates, 1957-728. Age-Specific Fertility Rates, 1957-699. Percentage of Women Currently Married by Age, 1957, 1962, and 1967
10. Rural-Urban Age-Specific Fertility Rates and Total FertilityRates, 1962 and 1967
11. Age-Specific Fertility Rates by Ethnic Group, 1957-6912. Live Birth Order by Ethnic Group, 196913. Socio-Economic Variable and Fertility by States, 196914. Mortality Rates, 1951-7215. Mortality Rates by Ethnic Group, 196916. Targets and Achievements of Family Planning Program, 1967-7517. Regional Differentials in Acceptability, 196918. Acceptors by Agency, 1967-197319. Monthly Acceptor Rates in Integration Areas, 197220. Number and Proportion of Acceptors by Method, 1967-7321. The Age-Specific Continuation Rates for Oral Contraceptives! 196922. Family Planning Acceptors by Age Group, 1967-7221 Mnnt-hlv Tnrome Level of Hl1sbands of Arrentor-.. 1967-7224. Level of Education of Acceptors, 1967-7225. rmitive Winmher nf Aptpnt-nrs hv b thnir' Crniin. 1967-7226. Knowledge, Attitude, and Desired No. of Children, 1966/67 and 197027. Ucse of Family Plan.ning Methods 1966/67 and 1970

-3-
TABLE OF CONTENTS (Cont'd)
28. Mean Live Births; Desired Number of Children; Proportion EverUsed Contraception and Currently Using ConLracepLLon -
1966/67 and 197029. Mean Live Births, Mean Desired Ntmber or Cnildren and Use of
Contraceptives in Metropolitan, Urban and Rural Areas, 197030. Births Averted in Malaysia, i967-7031. Annual Births Averted According to Characteristics of
Acceptors and Program, 1968-7132. Age of Women Practicing Contraception Within and Without the
Program, April 1968 - March 196933. Target Number and Proportion of Married Women (15-49) to be
Reached by National Family Planning Program, 1971-7534. Rural Clinic Facilities Compared with Target of New Acceptors
Set for 1971-7535. Existing Government Family Planning Service Facilities36. Categories of Staff by State Under the NFPB, November, 197137. Average Deliveries per Government Hospital Bed by State, 196838. Staffing Pattern of a Rural Health Unit, 197139. Population Coverage of Health Facilities Under the Second
Malaysia Plan - 1971 and 197540. Outpatient Attendance at Health Centers, 197041. Maternal and Child Health Clinic Attendances, 197042. Stages of Family Planning Integration into Rural Health
Services, 1971-7643. Number of Clinics Operated by the Federation of Family
Planning Association, 197144. Distance Between Main Health Center Sub-Health Center and Between
Sub-Health Center and Midwife Clinic-cum-Quarters in theIntegration Area
45. Health Manpower in Government Health Services46. Estimated Shortage of Nursing Personnel, 1971-7547. Public Health Personnel Trained at Rural Health Center,
Jitra, 1956-7148. Public Health Personnel Trained at Rural Health Center,
Rembau, 1966-7149. Family Planning Syllabus for Auxiliary Course at Rural Health
Training Centers50. National Family Planning Board Training Courses51. Number of Nursing Personnel, 1966-75


THE POPULATION PROGRAM OF THE GOVERNMENT OF MALAYSIA
A CIIWA 0VVT?7VR
A% GEV V A.QVA.!!Lff
PREFACE
:.Thi report providd a broad re-iew of Malaysia's populatlonproblem, of the Government's population policy, and of the national familyplanning program. Tho materia;l was collected by member of two W'orld Ba kmissions which visited Malaysia from November 1-22, 1971, and February 21to Hirch 21, 1972. it im hoped that the report wiii oe useful to anyonewho has an interest in the Malayaian program, and especially to thoseMalaysians who are concerned with their country's population problem andwith the devolopment of effective measures for dealing with it.
Ii. Thn Government of Malaysia adopted family planning as a nationalpolicy in 1964, and a National Family Planning Board was established in 1966to prepare and carry out a program. Although the program has not receivedthe deoired political support, a 1970 survey indicated that about 78% of tCecurrently married women in the childbearing age group approved of familyplanning in concept, indicating strong private support. The same surveyshowed that only 16% of these women were current users of modern contracep-tives. It seems clear that if information and education activities arestrongthened, and if the availability of services is increased, many morecoupleo will become acceptors.
Wii. The sector study identified a number of high-priority needs forfurther development of the program, including several suitable for Bankassistance, The project oubequently developed is intended to help thenational family planning program reduce fertility faster than would other-wise occur, mainly by stepping up education and training activities and byextendins the network of health facilities, particularly in the rural areasiwhere the Governmont hao recently decided to extend family planning serv-ices through its regular maternal and child health program. Judging onpost and present Inputs to the family planning program, it may not be pos-sible to reduce tho birth rate from 37 in 1966 to 26 in 1985. AdditionalInputs by the project will assist the national family planning program toreach the above tarnet, takina into consideration that the duration of theproject is five years. The project Is also intended to qualitatively im-prove the services. The proJect will cost an estimated US$14.5 million,and will be financed cooperatively by the Bank, the United Nations Fund forPopulation Activities. and the Government. The Bank will provide a 25-yearloan of $5.0 million, UNFPA will provide grant assistance of $4.3 million,and the Gavernment will orovide the largest share. S5.2 million in localcurrency, (See the Bank Appraisal Report No. PP-12a, dated 21 December,1972.k A Plan of Aetion waa preparAd bv the Covernmant in 1973 that con-taie the detailed schedule of implementation of the project. (Plan ofAction. of Family PlnI""ng ProgrAm nf Palfnnlar Malavtia 1973-75).

-- I -
lv. The bsetor rport fista issued in December, 1972 has been subse-quelntlyrevised 'to "ineerrate cement. of -the National 1Fly Plamingboard ad Ut latbe t e at-iavailable.

T rD -OPDADUTr MDVMT%C
Population Size and Growth Rate
1.01 In the 1970 census, the population of Malaysia was estimated atIV.O ULULiLo.u. About 85/ oL the populatioU, or 9.2 mill..Ln, was reported
in West Malaysia and the rest 1.6 million in the states of Sabah andSarawa&k, WLhiCh constitute East Malaysia.
1.02 hne natural rate of population growth in West Malaysia was 2.5Zin 1972, resulting from a birth rate of 32 and a death rate of 6.8 perthousand; there was little international migration. In the 1920s -he rateof population growth, perhaps after accounting for migration, averaged 3%.During the Depression and the Second World War it fell to an average ofless than 2%, but regained the level of 3% in the late fifties and remainedthere until the early sixties (Annex 1). Since that time the rate of growthof population has slowed somewhat. However, the postwar baby boom willsharply reverse this trend during the next few years unless there is a su)-stantial further decline in fertility or net out migration (Annex 2).
Population Distribution
1.03 The density of population per mile2 was 84 in 1970 for the coun-try as a whole; however, the density of West Malaysia (181) was severaltimes higher than that of East Malaysia (21). About 62% of the populationof West Malaysia resides in the four states of Selangor, Perak, Johor andKedah. There has not been a substantial internal migration since 1957 tochange the regional balance of population (Annex 3).
1.04 According to the 1970 census, 71% of the population was rural, aslight increase from the 68% reported in the 1957 census. The percentage ofpopulation living in rural areas varies considerably from state to state.For example, in Penang only 49% of the population is rural, in Kedah thecorresponding proportion is 87, and in the small state of Perlis all of thepopulation is rural (Annex 4).
1.05 The 1957 census reported 49.7% of the population as Malay, 37.2%Chinese, and 11.3% Indian and 1.8% others. The 1970 census reported aslight change in ethnic composition: 53.4% Malay, 35.4% Chinese, and 10.6%Indian and 0.6% others (Annex 5).
1.06 As a result of high birth rates in the post-World War II period,about 19% of the population was under five years of age in 1957. Conse-quently, in 1969 about 487,000 females were 15-19 years of age as comparedwith 300,000 in 1957 (Annex 6). These figures represent an increase of62.3% in females in the early stages of the reproductive period between1957-69 as compared with the increase in total female ponulation of 45.5%.

-2-
Fertility Decline
1.07 The crude birth rate, that was reported at 46.2 in 1957, declinedto 33.0 in 1969 and to 32.2 in 1970. The total fertility rate declined from6.7 in 1957 to 4.8 in 1969. The corresponding declines in general tertilityrates were 229 and 163 respectively (Annex 7). However, if current fertil-ity rates continue, the birth rate is expected to increase to 35.3 In 1975and to 37.1 in 1985 because of the larger number of persons entering thereproductive ages due to the postwar baby boom as mentioned in para 1.02.
1.08 The history of fertility decline in Malaysia can be divided intothree phases. The first phase was the decline during 1957-62 before theFederation of Family Planning Association (FFPA), the voluntary organiza-tion, started its activities. The second phase covered the period 1962-67when the FFPA was actively involved in the program. The third and contin-uing phase is the post-1967 period when the Government program was initiated.Total fertility (the number of births per woman) declined by about 12% during1957-62 and by 11% during 1962-67. During the period 1957-67 as a whole, thedecline in total fertility was around 21%. Between 1967-69, total fertilitydeclined by about 6%. The age pattern of decline in fertility indicated thatduring 1957-67 the decline was sharp at ages 15-19 and 20-24 years, decliningby about 42% for females aged 15-19 years and 30% for those aged 20-24 years.A considerable proportion of the fertility decline during 1957-67 could havebeen due to a substantial fall in the percentage of married women in the re-productive ages. The proportion of married women between the ages of 15-19years declined by about 49% and between 20-24 years by more than 20% during1957-67. In the subsequent period (1967-69), fertility decline acceleratedfor females of all ages in the reproductive period except for those aged20-24 and 30-34 years (Annexes 8 and 9).
Differential Fertility
1.09 The fertility rates in the metropolitan and urban areas were al-ready lower than in rural areas in 1962. Again, during 1962-67 (the periodfor which data are available), fertility declined faster in urban areasthan in rural or metropolitan areas (Annex 10). The difference betweenrural and urban fertility can be explained by variations in family planningpractices in addition to the difference in Dronortion married. Estimatesfrom the West Malaysian Family Survey in 1966-67 showed that 39% of marriedwomen 15-44 vyars in metronolitan arean uised fnmilv nlAnnina at sonme. t-imP-
with 31% currently using it. In urban areas the corresponding figures were27Z nnd 917 while in t-hp ru1ral rq5 t-hp figu'iresa wa-er onlyT 6% e"A TY The.
proportion of married females at all ages was highest in rural areas andlowest in town.
1.10 Tn 10r,7, tbe total f:ertilit4+y rat-e was hi-.1est 'or the Tndi,- asI S'S ~ ~.Lft SJ.J , bLC 5.S.O.*UhAJ Iy Ua1 khrl LU U_ LUC A.U.LdJ
followed by the Chinese and the Malays. But the position was reversed by' nt '7 _ _ _ ._ _1 C , ,_ _,_ .. __ 1 XC 7 47 I- .3 L 1 JL. _e _ - - E__ CI , V ±LXII Lllt LULd± LLeL.rt'i L eLty UUra1t6 1 7JI-U/ II^U IUJn b y JR
for the Malays, 36% for the Chinese and 33% for the Indians. In 1967-69,however, the decline in fertility among the Malays was highest at 8%,

- 3 -
followed by the Indians at 7%, and the Chinese at 5% (Annex 11). Yet thetotal fertility rate in 1969 was lowest at 4.4 for the Chinese and highestfor the Malays at 5.2. While about 20% of total births were first order inWest Malaysia, the highest proportions of first and second order births wereamong the Chinese, indicating the use of contraceptives for spacing (Annex 12).
1.11 The birth rate, as usual, varied considerably from state to state.It was low in Penang and Perlis and highest in Trengganu, followed by Pahangand Kelantan. These wide differences could not be due to variations in agestructure alone and simple observation of data indicates that these werenot related to levels of development, reflected by the per capita income orpercentage of urban population in different states. The decline in birthrate by state also did not seem to be related to these variables. It was,to some extent, related to the ethnic composition. A positive association,however, is indicated between birthrate and infant mortality rate among dif-ferent states. Trengganu, Kelantan and Pahang had high infant and maternalmortality rates as well as high birth rates in 1969. On the other hand,Penang had the lowest birtn rate and maternal mortality rate, as well asone of the lowest infant mortality rates (Annex 13).
Mortality Decline
1.12 The death rate declined from more than 15 per 1,000 in 1951 to6.8 per 1,000 in 1972. At the same time, infant mortality declined from97 per 1,000 in 1951 to 43 per 1,000 in 1969 (Annex 14). In Malaysia.the toddler mortality rate 1 / (which is internationally accepted as anindex of the nutritional status of a community) declined from 11 per 1,00Cin 1957 to 5 per 1,000 ir. 1969. Yet, whereas the infant mortality ratein Malaysia was only twice that of developed countries. the toddler mor-tality rate was 5-6 times as high. Although the 0.4 year age group com-prised 16% of the population, it contributed almost 31% of the total numberof deaths. While death and infant maortality rates were highest for theIndians and lowest for the Chinese, the toddler mortality rate was highest:among the Malays (Annex 15).
1/ Defined as the ntumber of deaths per 1,000 children between the agesof 1-4 years.

-4-
II. ORGANIZATION OF THE NATIONAL FAMILY PLANNING PROGRAM
A. Existing Situation
2.01 Malaysia's National Family Planning Program is administered bythe National Family Planning Board (NFPB), an autonomous statutory bodyhaving inter-ministrial functions. The Board was established by the Actof Parliament on June 10, 1966. The NFPB is under the Prime Minister'sDepartment. According to the functions of the NFPB, it directs and coor-dinates the national family planning activities with all the relevantministries and organization. At present, the family planning servicesare provided mainly by the NFPB, the Rural Health Services of the Ministryof Health, the Family Planning Associations, and other private organizationssuch as estates and private practitioners.
2.02 In 1965, population and family planning were first announced aspublic policy in the First Malaysia Plan (1965-70). The Plan specified asa major objective "to lay the groundwork for less rapid population growthby instituting an effective program of family planning". It further spec]i-fied, among its long-term goals for 1985, a reduction of the birth rate inorder to reduce the population growth rate from 3 to 2% to help achieve theper capita income target of M$ 1,500 per year.
2.03 Specific objectives of the family planning program in the SecondMalaysia Plan (1971-75) are: "(a) to extend family planning services tothe rural areas; and (b) to bring the birth rate down to 32-per thousandpopulation", by reaching 600,000 new acceptors and increasing current usersfrom the present level of 105,000 to about 267,000 by 1975. 1/
Family Planning Association
2.04 The first organized family planning activity actually began inJuly 1953 with the formation of the FPA of Selangor. followed by three otherstates -- Johor, Perak, and Malacca. In 1958, these four states formed theFederation of Family Planning Associations, with gradually increasing finan-cial assistance from the Social Welfare Lotteries Board, IPPF, Ford Founda-tion, nnd the Pathfinder Fund. It then became possible for the F-FPA topromote organized family planning activities in other states. By July 1962,family planning associations had been formed in all eleven states.
2.05 By the end of 1971, the FFPA wa-s delivering services through 169
clinics and 116 estates. With the official program expanding at a rapidpace, the FDA's role a-d 4uncti4O hava habecme mn unvaieA. Thaw,s ar
summarized as follows:
1/ The Government's new targets now call for a reduction in birth rateL~. ie-i 1- ~ap LAA 1-e4.., 1P1.-- wq.m-- OfMa a.(e" 4 a-
by 19-75 to, 30 pe-r .housand populatio-. (The ro-r.sent f kPlan of Action of Family Planning Program of Peninsular Malaysia,4fl7'_ rw
- 5 -
a. To provide, on nongovernment premises, at least in the maintowns of each state, a greater range of methods and a morecomprehensive type of family planning service than is pos-sible in a mass family planning program, e.g., a higherratio of medical coverage, PAP smears, pregnancy tests,treatment of sub-fertility, etc.;
b. To provide family planning information service, which couldconcentrate upon collection, collation, and circulation ofinformation and material relating to various aspects offamily planning programs, particularly for the higher pro-fessional groups and appropriate social organizations; and
c. To gradually extend FFPA activity into new fields, e.g.,family life education, marriage guidance, etc.
National Familv Planning Board and the Ministrv of Health
2.06 Under the statute, the NFPB should comprise a Chairman, a Direct:or-General, and twenty members -- ten representing relevant ministries and tenothers representing various public groups. The Board functions through it:sfive divisions, each of which is headed by a chief. In 1972, the total stafffor all divisions numbered 400. The NFPB has recently appointed as DeputyrDirector a former civil servant for strengthening its administration.
2.07 In the years 1967 and 1968, the NFPB concentrated its efforts,mainlv through epnarate clinnis, tn rparh the turban onnulation through anextension of family planning services, and family planning. Later theRoard sought- ton fuii-t-her Yt-rA sa1-iri ce a the ruval sarena but 1 eck-ed the
health personnel to establish separate clinics. Thus, a program was devisedin consnction w4t-h 4.the Health Se-vce (Rural) of the Ministry of Heal hto integrate family planning services with Maternal and Child Health (MCH).Lfl...4 4 *&UU LfL -. EL CA 1 ----- C CkC. .A.. *fSU-- %.&,_ ..A. U -. ~ Ow*SIrse -ce ir. the rural areas bysae.Src hr,teN-Bhbe.wrc
ing out the details of integration with the MH. The day-to-day supervi-sions of this integrated progr-am has A dl1-te-A the State DirectAr
of Medical and Health Services who is in charge of health services both inpreventive an,d curative aspects. Y.e 'Ls h-eaA of the State Healt.h Depart nlt'
which consists of a staff of about 40 to 50. The Senior Health Officer,,-A..o isusual t-rainetd ir. publD"ic I&hCeAAL.&A, is reso.sbl for U -r, Y4eti
with support from the State Matron, who is head of nursing affairs. So far,there is no full=tim=e me%dicaal offficer to tak-e c.z1krge of -A-4nlstratl re andtechnical supervision for NCH service at the state level.
2.08 To assist both the NFPB and MOH in implementing, coordinating,and evaluating the integration of family plarninug serv`ces -with tbhe ruralhealth services, the Central Coordinating Committee (CCC) was formed.This CCC is assisted by four Sub-Committees for Service, Evaluation,Training and Information. The function of the CCC is to set up guide-lines for hLe integratLon program in accordance WiLt Lth pUoLiEcy of thenational family planning program and at the same time to help State

-6-
uooraiUatiug UatW UCL.m-1t tUteL-esI woU-rlLk Lout detaills f0r OiL i of thef plan
drawn up by the CCC. However, the Director-General of NFPB exercises thesame power in the integration areas as Chief Executive Officer as laiddown in the Family Planning Act No. 42, 1966 for planning, directing,coordinating and continuence of family planning activities in PeninsularMalaysia. The CCC is comprised of 16 members representing the NFPB, MOH,FFPA and others and is chaired by the Director of Health, MOH and cochairedby the Director General of the NFPB. The State Coordinating Committee (SCC)of each state is comprised of 12 members representing the NFPB, the officeof the State Director of Medical and Health Services, the FPA and otherco-opted members, and is chaired by the State Director of Medical and HealthServices. The SCC is responsible for the implementation of the integrationprogram in rural areas but not for the family planning program outside ofthe integration areas administered directly by the NFPB and the FPAs.
B. Limitations of the Existing Organization
2.09 The present level of political commitment is insufficient for theexpansion and extension of services according to the goals specified in theSecond Malaysian Plan. This limitation is not specific to organizationalproblems, but is a basic underlying constraint for the progress of allfamily planning activities. Because of increased ethnic sensitivities,since May 1969, Government policy has been to move forward with the familyplanning targets with little publicity. However, the political commitmentof continuing with a high level semi-autonomous agency (NFPB) identifiedfor the family planning program has not been affected so far.
2.10 Periodic consideration of other population growth rate alterna-tives in terms of both developmental gains and costs needs more attentionby the Economic Planning Unit itself than it has received in recent years.Discussions and agreements at cabinet level also appear necessary at thistime, particularly on policy agreements that will determine the NFPB andthe MOH responsibilities for family planning services, family planning in-formation and education during the present plan period.
2.11 In the demarcation of the responsibilities of different aaenciesfor working purposes it is stated that the program in the urban areas willcontinue to be the resnonsibilitv of the NFPB with the FPA playing bothcomplimentary and supplementary roles. The private practitioners willalso comnpement the nrnoram- The family nlanning nrnorami in rural Arpna
are divided into an integrated program and a non-integrated program. Theintegrated program will hb imnlemonted vy the MinistrY of Health as a partof Rural Health Services and the non-integrated program by the NFPB and otherconcerned organizations identified by the NFPB.
2.12 in smmmary, the specific problems which hInder the rap-4,d p-roresss w- -r,~~ r---, - - .~^ ^~^~ ^ -_ - 1-45-~
of integration efforts are: (a) inadequate coordination between the NFPBand. m the *O; (b) i.s4nufficier -4.t co tment ar,d availabi,ity of: f-tie

persons for MCH and family planning services at the state levels; (c) in-adequate facilities and manpower under the health infrastructure; and (d)the absence of a five-vear familv planning plan.
C. Recommendations
2.13 The di visinn8 nf the N'PR shnuld not be guii4ied hv acting chiefstoo long if the healthy operation of the organization is to be maintained.Furthermnrre; reasonable degree of authority should be given tn the divi-sion chiefs which would allow them to carry out daily work more efficientlywitho.t unneressary delAy.
2-14 The NFPB should prepa-e a comprehenrsive fam-ily plalnnin.g pla.nl con-taining a detailed plan of action for five years which defines the role ofeach ministry and agency. The plan would t-hen lbecme a commItmeint for theorganizations, involved in the program, such as Ministries of Health, Educa-tion, NatIonal n"A Pural -Ae TnfommatIon And Education, inaddition to the FFPA.
2.15 Effective administrative offices need to be established in eachstate with specified W-atIhority for servi supplies, ir.fLor-t4r. tr4.i.
of personnel, and finances, and with maximum opportunity for coordinationwith the state healt-h adu.ir.isration..
.... ..1.. 1qLL A~a.. LII LLUL.LLL.LCbLLG.CL.ALII
2.1 The~ Mw. ULI LoLf thLeLL iL the adUiLLLuni'striat ive n.ucle-us L Lof C t LMJ.L.Ly
planning service throughout the nationwide health infrastructure. This unitsho-uld 'e strenLgtleneu by upgrading the position of tne CChie'f and by 'UdiIIgmore manpower.
2.17 A post of MCH/FP officer in each state should be created tostrengthen coordination with the State NFPB officers. The MCiHFP officerwill provide proper supervision for integrated family planning servicesi.n the rural areas at state level.
2.18 A management adviser, possibly a professional firm of consultants,should assist the NFPB in examining existing NFPB and MOH systems of manage-ment and administration.

-8-
III. ACHIEVEMENT OF THE PROGRAM
3.01 This chapter attempts to evaluate the program in terms of (a)recruitment of new acceptors in relation to the target; (b) impact on know-ledge, attitude, and practice of family planning; and (c) births averted bythe program. Some recommendations for improvement in setting up the targetsand their evaluation are also given.
A. New Acceptors
3=02 The NFPB had set yearly targets to reach 3%, 5%. 8%; and 10% ofthe married women between the ages of 15 and 44 as new acceptors during1967, 1968, 1969, and 1970= The targets for 1971 rn 1973 rall fnr noering
5.4%, 6.7% and 7.8% of married women within the fertile ages as new acceptors.These lo whih totala nout a -ua rter of all marriedA wmnm within the re-
*-- - tt -- _ o
productive ages were set without direct reference to the desired reductionin birth rate. During 1967 sd 1968, the achievements e.ceeded the targets.Since 1969, the number of new acceptors started declining. In 1970, thenr,,mber of accepton.rsa wna A nn o an6,0nnr*A ton mor thi f An ?0,00 4in 16.Q TIn
1971, the number declined further to about 55,000 and did not exceed 56,5004.. 1072 rh. TM.e present trend iS r.no btter o the number of acceptors for 1073was reported to be 38,443,1/ (Annex 16). The main reasons for the shortfallwere stated to be the diffi4culties i:: (z) reachin.g thbe 1hard core of elig-Uibl
couples in urban areas where the program has been confined so far; and (b)extendir.g 1the services to rural areas bwecause of the shortage of parameAdiclstaff trained in family planning. However, in 1971, the MOH integrated theAeli1very of services with m-te..al zr.d -1hild lea`t in a few rura'l areas onu J.LVA L LJ. A. V±L , W LAI W 6~ L. A. %AI %.IL.LJ.LU LI d..L&L J.L A.LW LUaL a~. J
a pilot basis.
3.03 No clear statement of targets by state was available to programworkers. Thie NFrPB sets the targets biy states fLor iLts UwnL eva'LuatLon, bJutthere was no feedback to the officers at the state level. According to NFPBdata, there were marked different'ials 'n regional performance. Acceptors aspercentage of eligible women were highest in Perlis and lowest in Kelantan.Performance was also high in Negri Sembilan and low in Kedah and Trengganu.Such differential performances did not seem to be related either to percapita income or to the percentage of rural population in different states.A closer association of such differential performances seems to exist withthe availability of facilities for the delivery ot services or the popula-tion density per clinic. For example, Kelantan had the largest number ofeligible women per facility and the lowest percentage of eligible women asacceptors while Negri Sembilan had one of the highest performance rates andthe smallest number of eligible women to be covered by NFPB facilities(Annex 17). No evaluation has been made so far of such differential per-formances and their reasons.
1 / C,,m.il a4~.-o 4 ~.wvotKrniigh Jul._

- 9 -
3.04 In 1967, a little less than half of the acceptors were recruitedby the FFPA_ and a little less than 40% by the NFPR. In 1973; however.about 63% of the acceptors were recruited by the NFPB and only one-fifthby the FFPA. Alsn in 1473; the MON reported ahn,it R8 nf the ArepntorRfrom its integrated areas (Annex 18). With the expansion of facilitiesin the ruianl Arn t-ho MnH ia going to play an TTir.crenaiiy imrnrtnnt rnlein recruiting new acceptors. In the districts where the MOH started thedelivery of ln.tegrated servlces, a sousta4tial increase in 4h r..r ofnew acceptors has been reported for 1971 (Annex 19).
3.05 About 87% of the acceptors were reported to be on pill by 1973,a compFaredu to 972%1 ir, 191681. T"here hL_ benalitl hftt triiaiU1j)L~U U ~L. ~L1 I UU * .LLL=L"- LLftZ U--CL&L J L.LLL.LC aLLLJ. L LU -V.J.~0J~l
and other methods in recent years. The proportion of sterilization cases4 J ~~~ ~ ./ Z.. 1f~~~~O I £0, j 4 17 - 2 __ increased Alrom o-ver 3L%o iLn 19768L to mo1,Ire than L6% Jn 173 LLU Uo other -tholds
from .5% in 1968 to about 5% in 1973. The proportion of IUD users is more orless the s-ame since 197600 (AUnex 20%). Ihe CUonLtLiUnLLULI ILto LUL LLI th piJ..L.
users were quite high as compared to other countries. About 66% of thewomen on, p'"" ils were- repOrtled to oe continuing after 12 monLns anlU J55% 4aLtLt18 months (Annex 21).
3.06 The age composition of acceptors was also quite favorable. In1972, about 64% of the acceptors were less than 30 years of age (Annex 22L.The acceptors were largely drawn from the relatively lower income groups,wLtn 17% of them having husbands earning less than M$ 100 per month and61% with less than M$ 300 per month (Annex 23). A little more than one-fifth of the acceptors had no schooling while about one-half had a primary-level education; only 13% had a secondary or higher education (Annex 24).In 1971 a larger percentage of acceptors was Malay (46.3%) than Chinese(42.1%) or Indian (10.5%) (Annex 25). But in relation to their proportionto the population, the Chinese contributed a greater proportion of acceptorsthan the Malays.
B. Impact of Knowledge- Attitude, and Practice
3.07 Results of KAP surveys at two points of time, i.e., 1966-67 and1970, are available. The changes in knowledge, attitude, and practicebetween 1966-70 could be in part the result of the national program. Theimpact of the family planning program seems to have been favorable both ornthe desired size of family and the use of contraceptives by females of all.ages within the reproductive ages. The knowledge of family planning in-creased substantially during the period. In 1966-67, only 44% of the eli-gible respondents knew about family planning while in 1970 as many as 85%knew about it. The change in attitude has also been more favorable; theproportion of those disapproving of family planning declined from 21% in1966-67 to 13% in 1970. The proportion of eligible women desiring 7 ormore children declined from 16% to 8% and those desiring two or lesschildren increased from 5% to almost 9% during the same period. Stillthe program has to go a long way in inculcating two-or-three-child familynorms as about 45% of the eligible women desired three-to-four children andanother 38% desired more than four (Annex 26).

- 10 -
3.08 The proportion of females who ever used contraceptive methods in-creased from 14% in 1966-67 to 27% in 1970. Similarly, the proportion ofthose currently using a method increased from 8% to about 16% during theperiod (Annex 27). The proportion of females who ever used a method, orthose currently using one in 1970, was twice that reported in 1966-67 formothers below the age of 34 years (Annex 28). Efforts to increase familyplanning practices should be concentrated largely in rural areas since notonly the nronortion of those desiring a larger number of children was hieherthere, but also the proportion of current users was about half of that inmetronolitan areas at almost all aaes. The Dronortion of current contra-ceptive users or those who ever used a method for females in all the re-nroAtirtive age-ornunp was also lower in rural areas as nompared to tons(Annex 29).
C.B irths Averted -
Method g
3.09 An attempt is made here to evaluate the impact of the program intermA of (a) births averted by acceptnrs in the program _A comnared Atn thneaverted in the country as a whole as a result of general socio-economic de-v1e mennt-a (b h) whther g _en whon usaed f m4ly n1nvnn4ineg aa,-,4r-ic A-4A add8because of the existence of the program or for other reasons. The methodo-J.J5 AU Ur SA v v iO UO O A SAiA* *- A_C b AS A A. *J*>__i Q A .J a, OJ _P Ut C A_ c;; *t L.logy} tV -e use 4s 1ae4on the^*$ V Av s wors oc Potr Bea an Wee s zer el ^oZ
Lee and Isbister, Mauldin, and Wishik. Basically it uses the concept ofcoup'le years ofl protection, li-fe +---le contlis-atlorn rates, aud 4ertilltyI..Li)J~ 7~L U.. JLJL~LJLiL~ .LJ.J.L LUAL 0" .L LLL.n.uat.iJln A es O.LL LCL L.LJ.J.tY
differentials by age. The data available for this analysis consist ofclassLLLcatLonb o,L the nuUJLL-er o, acceptors b'y quarter o,L acceptarLce be-tween July 1967 and December 1970 according to various characteristics ofthe acceptors and continuation rates. On the basis of this informationand using the decay function R = ae-rt where "a" is the proportion ofacceptors who effectively begin contraceptive use, -r" is tne rate ofacceptors who drop out each period, and "t" is the number of periods afteracceptance, the values or "a" and 'r" can be estimated, and from this Rcan be estimated for different values of t. By integrating the functionR = ae-rt between the moment t1 and the moment t2, it is possible to deter-mine the number of couple months of protection given to a cohort of womenbetween t 1 and t2 when they have joined in the period "0". The number ofcouple-months of protection multiplied by the age specific fertility of thewomen in that cohort gives an estimate of the number of births that the co-hort of women would have had nine months later if they had not been protectedin that particular time period. When this is done for each age group and foreach time period, the result is the number of children which a woman wouldpossibly have had in different time periods if she had not practiced birthcontrol.
1/ The discussion is based on the work of Roberto Cuca, Population andHuman Resources Division, IBPDT.

= 11 -
3.10 Estimates of the number of actual births in Malaysia can be ob-tained from the Vital Statistics Registration System. The number of birthsthat were averted in the country as a whole are estimated as the differencebetween actual births and the estimated number of births that would haveoccurred if the married women in the years 1967-1970 had had the fertilityof 1957. The calculation indicates that the decline in fertility between1957 and 1969 has meant about 37,000 less births in 1967, 39,000 less birithsin 1968, 59,000 less births in 1969, and 71,000 in 1970. The important faictis, of course, the increase in births averted between 1968 and 1969 whichreached a peak of 20,600 declined to less than 12,000 between 1969 and 1970.The births averted by the program, however, in 1968 were 3,300 and increasedto 17,300 in 1969, and to 26,700 in 1970 (Annex 30).
3.11 If the program had not been in existence, some women who joinedthe program would possibly have practiced birth control. On the other hand.some women, who started practicing contraception after the inception of theprogram but who did not obtain supplies from the clinics. could have beeninfluenced by the program. Assuming then that these two factors cancel ouit,the increase in births averted in the country of 20,700 between 1968-69 canbe divided between an increase of 14,000 within the program and an increaseoutside the program of 6.700. Similarly, for 1969-7Q; out of the 12 000births averted, about 9,400 are estimated to have been averted through theprogram and 2.300 outside the proeram. In this case, the contribution ofthe program would have been higher than that revealed by the services ren-dered. Of the total births averted, 29% were averted due to the servicesof the program in 1969, and 38% in 1970.
3.12 Births averted according to various characteristics of acceptorsappear in Annex 31. They are classified first by year in which the birthwas averted and also by agency supplying the services and by method. Itis assinu-ed that the gge distribution of the acceptors has been tbhe samefor these classifications as the age distribution of all acceptors in eachperiod of acceptance. The bias introduced by this assumption is that if,for example, the pill users were younger than the users of other methodsthen the pihl would have provided a somewhat larger number of births avertedthan the one appearing in the table. The same situation would occur withthe agencies providing the services, and al'th.oug the relative distribution.could have some changes this obviously would not affect the totals.
3.13 With respect to age distribution it seems to indicate that theprogram was m-ore effective for younger women "15=34 years of age'. A prob-=able explanation is that the initiation of the program by expanding infor-ntion. induced a larger number of yotinger wo-,Len to practLice contraception.
These women, in the absence of a Government policy, may not have heard offamil planning. A1so, the women practicing contraceptiorA outsiUe the pro--
gram could be women who had been controlling their fertility for some yearsbefore the program was est"abllshed and consequently were, on tle average,older than the women in the program. Thirdly, it is possible that olderwomen not in the progra,u had adopted a permanent method or birth controlbefore the program came into existence so that when the program was initi-atea they were already covered for the rest of their childbearing years.

- 12 -
3.14 If it were assumed that a given proportion of births averted inan age group corresponds to the same proportion of women in that age prac-ticing contraception, then a comparison of numbers of women controllingthIeir fertlity wtlh aid without the services o' the program would be asshown in Annex 32. The conclusion here would be that in the program 3.0women practiLcing contraceptiLon for one year wouLUd avert one birth, wnilethe average for the country is 3.9 women practicing contraception for eachuirth averted. Outside the program then there would have to be 4.3 womenpracticing contraception in order to avert a birth. These figures may beonly approximations and need not hold in the future, but the implicationis that by concentrating on the young age groups the program is, on theaverage, more effective than the over-all practice of family planning inthe whole country. This of course, does not imply that the cost per birthaverted in the program is lower than the cost outside the program. ifwomen outside the program were having sterilizations as the major methodof family planning while women in the program used the pill, the cost perbirth averted in the program could be higher in the long run.
3.15 The results of this evaluation indicate that the family planningprogram of the Government implemented througn the NFPB is really increasingthe number of births averted. It seems that the initial reaction was ashift of private family planning users to the official program followed bya large increase of users both within and outside the program. However, thegreater increase was in the Government program. So it may be said that theofficial program provided an outlet for new users and consequently preventedadditional births rather than providing only an alternative institution forcurrent users.
3.16 The program seems to be more effective in its results than theprivate services due to the younger age distribution of its clients. Thenumber of new acceptors has declined somewhat and this could be due to limi-tations for the provision of services or to a decreased demand because themost eager family planners are already in the program, making it necessaryto attract new and less-convinced persons. What is encouraging is that thesenew acceptors, who have been drawn from groups with less education and pos-sibly with less income, would not be practicing birth control in the absenceof the program because of the high expenses involved.
3.17 With a birth rate of 33 per thousand in 1969 there is still roomfor a further substantial decline in fertility. The slackening in the num-ber of acceptors in the program in 1970 implies that the program has to beimproved in order to obtain an increasing number of new acceptors. Theactual users will grow older as time passes so the program should continueto concentrate on the young women in order to obtain a balance of ages.
3.18 The concentration on young women in the past could have a greaterimpact in the future course of fertility than is visible from the eva1ua-tion. Women who had decided to adopt birth control at an early age, evenif they dropned out because of contracentive failure or because the- wantedto have more children, will possibly go back to the use of contraception in

- 13 -
~ n..n-4,,~a.-.. .,.n -~4 - 14-*A +1-n4. An ,, -4 ~ 1ir a4va -U~h.a9 effective fo.._ after havirg .o.leted their desired flysize. Wh.ether
they use the services of the program in the future is of no consequence since,4n a..y case, ...ey wil b cor,tolingj their fertilit.aJLy .aD ,LAMY3 WJ..LA. U= 6ULLL.L.L.LLL6 61M.L& LCL L.L.L.L6Y
Fu7txure Targets
3.19 Tze ar,Luai targets 'Lo 1971-75 envisage ar, Jncre=e of 600,000
new acceptors based on estimates of contraceptive coverage which would re-duce the cruue Dirt'f rate from 32.2 in 19710 to .30 in- 1975 Ln kLUCLUL -with
the long-term goal of a reduction in crude birth rate to 26 in 1985.1/ Theannual distribution is given in Annex 33. It is estimated by tne NrrD LlthLit would not be possible to achieve the existing targets without an intensiveeffort both by the MOn and the NFPB. The targets ot recruitment or acceptorsby different agencies are given in Annex 34. From the 600,000 new acceptorsrequired to achieve the desired reduction in the birth rate, 450,000 are tobe recruited from rural areas and 150,000 from urban areas. From the 450,000new rural acceptors, only 54.1% are estimated to be reached by the Mwd throughthe integrated program. The remaining 46% (207,000 rural acceptors) cannotbe achieved unless MOH facilities are strengthened further. Some of theseacceptors are expected to be recruited by other agencies. The NFPB proposesto reach 150,000 acceptors.
Recommendations
3.20 a. The target of reducing the birth rate to 26 by 1985is modest. The rate of population growth would stillbe around 2% in 1985. Existing targets should, there-fore, be carefully re-evaluated in terms of their impacton basic economic variables by the Economic Unit (EPU).These should then be revised upwards taking into accountthe proposed expansion of facilities.
b. The targets for the country as a whole should be allo-cated officially to each state and possibly to eachhealth district and health center. The review ofachievements and analysis of differential performanceshould be fed back to state officials periodically.
c. Periodic surveys should be undertaken in the countryas a whole to monitor the acceptors and users not usingthe clinic facilities.
1/ The target of reduction in birth rate by 1975 is revised to 30 perthousand from 32 per thousand in the Government's Plan of Action forfamily planning for 1973-75. However, the estimated required numberof acceptors has nnt ben changed.

- 14 -
d. Service statistics should be analyzed regularly withrespect to the characteristics of acceptors and impacton fertility.
e. Coverage of the rural population by the programshould be improved as expeditiously as possible.

- 15 -
IV. DELIVERY SYSTEM OF SERVICE
A. Existing Situation
Policy
4.01 One of the major policies of the Government concerning family plan-ning service was set by the NFPB in August 1966, as tollows: "!It is theultimate aim of the Board to incorporate family planning into the healthservice to make it a complete health packet for the people. This is vitalto the interest of mothers and their babies and the family as a whole."After four years of providing family planning service under the NFPBs olwnservice system, the Board is now reconfirming its policy to encourage theintegration of family planning with the health service system.
Potentiality and Demand
4.02 Malaysia is one of the nations which has a well-established nationalhealth service system as compared with other countries in the region. Unlderthe Ministry of Health and 11 state medical departments, there are 61 Govern-ment hospitals (with more than 27,000 beds) and 44 functioning rural healthunits. Various categories of medical and health personnel are reasonablywell-trained locally and work under the Government health services. A surveyconducted in 1970 indicated that about 78% of the currently married women inthe childbearing age group approved of family planning. Thus, there is clearevidence that, if services are provided, a large proportion of the coupleswill accept family planning.
Proeram Particination
4.03 While the NPPB is mainlv rpqnonsible for the nrovision of serv:Lcethroughout the country, the Federation of Family Planning Association (FFPA)and some private doctors also partircpate in the national nrogram. Veryrecentlv, the Ministry of Health (MOH) and the NFPB started integration offamily planning with the Rural HMalth Servisa in a limit-A numnhr of healthdistricts. So far, the national program, which is medically oriented andIreliep heavily on oral contrapentives, has reached approximately 21% of thetarget women for the period 1967-70.
NFPB Service
4.04 General Set-up of Clinics: The NFPB was to implement its program,*.-'.~ AL L I UI JI I ~ ~ O LL~.L Lt U ai ~ 0 .L Twhich begar. ir -uy 19167 ir, phaases, starting ir, th ra reas 4n phae
and II and gradually extending it to rural areas in phases III and IV. E,ythIe endu ofI Q97A a total0 of 77 ticcr.can41moleuishdbe.estb lIsdL I / L I Isying t pLlanni lar±L c s a p[rt f1 r J l.L UJi t hae d IGverJnnLestablished, thereby identifying family planning as a part of the Governmient

- 16 -
health services, such as Government hospitals, rural health centers, and mid-
wifery clinics-cum-quarters (MCQs)(Annex 35). For various reasons, suchas a shortage of manpower, less than 30% of the original plan for clinic es-
tablishment has been achieved as indicated in the table given below. Theinvolvement of the NFPB in rural areas is, therefore, limited. The Ministry
of Health would be mainly responsible for extension of service in rural areas
as a part of its maternal and child health program. The MIOH has already in-
troduced family planning services in some of the rural areas (details in
next section).
Year Phase Clinics Scheduled Clinics Established
1967 I 7 16 static clinicsUrban 37 mobile units
1968 II 38 40 static clinics150 mobile units
1969 III 44 NIHC 17 static clinics143 mobile units
Rural 1970 IV 180 SHC 4 static clinics950 MCO 88 mobile units
4=05 Cnntracentive services are available through NFPB clinics daily or
periodically at 95% of the Government hospitals, 40% of the health centers,and 10% of the MGQ9. A field staff- which numbered 286 as of November 1971,
delivers services through three types of clinic operations: main clinics,substations, and mohile clinies (Annex 36).
a. The main rlinir. eRtablihed at the statp lpvsel ron-sists of all categories of staff, such as a medicalofficer, supervi.onr_ staff niirse- trained assiQtantnurses (TANs), family planning workers, and a regional1nfor.matlon of ficer. Services are offered daily inthese clinics and IUD insertions and vasectomy operationsare a'-so performed.
b. f'..e su.bstation 4s maned by two or. th-ree persons, eiath4-Aer
a staff nurse or TAN and one or two family planningwrkers. r s YLhese stations, Wi4ch are usually locael -indistrict hospitals, offer services daily.
c. The mobile clinic is run by main clinic and substationpersonnel either weekly or fortnightly 'Ln places wherethere is a need. These clinics usually coincide with
MCH clinics conducted by Ministry of Health personnelat rural health units.
4.06 NFPB Clinics in Government Hospitals: Since 1967, 44 of the 77NFPB static clinics were established on Government hospital campuses. Thefamily planning service is not integrated with hospital services, but ser-vice is offered by NFPB s own staff under its own administrative set-up,

- 17 -
utilizing hospital physical facilities such as a part of a main buildingor a small oILd iLLLUnUdependent buiUldLLng within the hIlosp'ita'L campus. In somecases, hospital corridors or garages are utilized for family planningactivities. In short, so far, family planning services in tnese centershave not enjoyed the status and privileges of other health programs.
4.07 During the three-year period from 1968-70, the Malaysian familypla.nning program succeedeu in recruiLting 201,465 new acceptors. About
130,643 new acceptors, or 64.8% of the total new acceptors, were recruitedby the NFPB and 41./8% of NFPB achievement was contributed by 44 NFPB clinicsattached to Government hospitals during this period as shown in the follow-ing table:
1968 1969 1970 Total
Total National Program Clinics 74,935 70,575 55,955 201,465Total NFPB Acceptors:Total Numfber 43,058 48,140 38,441 130,64RPercentage 57.4 68.2 70.4 64.8
NFPB Acceptors from Government Hospitals 21,761 19,523 13,452 54,736Percentage 50.5 40.5 34.1 41.1,
4.08 There were about 2,200 maternity beds in 53 Government hospitalsas of January 1971. The number of beds in each hospital range from lessthan 10 to more than 200. In 1968, 29.8% of the total registered births, or89,230 deliveries, occurred in these hospitals. This was equivalent to 45deliveries per maternity bed (Annex 37). In the same year there were 21,761new acceptors recruited in these hospitals. If we assume that about 50% ofthe new acceptors in these hospitals were "direct acceptors" or recruited.from obstetrical patients, "direct acceptors" in 1968 can be estimatedat 10,000.
4.09 Approaches Through Other Various Channels: Since the fall of 1970,family planning services have been extended to about 81 Federal Land Develop-ment Authority (FLDA) Schemes from a total of 91 FLDA Schemes in the country.All eligible couples are advised to obtain pills from MCQ stations within.the FLDA Scheme. Oral contraceptives are dispensed by the Government midwifeand M$.50 is deducted from the individual settler's account by the FLDAmanagement. The money collected by the management is supposed to be utilizedby the FLDA for the benefit of the settlers and reported to the NFPB. TheNFPB is taking on the responsibilities of supplying pills and field supervi-sion. 'The Ministry of Health approved the utilization of the Governmentmidwife at FLDA Schemes with the condition that she would not be involved, inthe collection of money for pills.
4.10 The Board plans to extend family planning services to the Low CostHousing Schemes in the urban area on a pilot basis. The Sungei Besi Flatwas chosen for study to determine whether the residents in the flat wouldutilize the opportunity if family planning services were offered at the door-step. The response was not encouraging. The impression is that women prefer

- 18 -
to go to the hospital clinic; they hesitate to request services within the flatmiinly because they are quiteP shy bout being recognized by neighbors as con-traceptive acceptors.
4.11 So far, the Board has not introduced family planning services inthe snAstraln cnmnlex. Thcre 4is howeveror a prelmnary plan to IAdntf4y-the feasible industrial complex and develop a service scheme jointly withthe welfare service and manaoers of the industr4es.
4.12 Utilization of Traditional Midwives for Family Planning: Tradi-tional midwives (kampong bidans) still attend about 40% of the total deliv-eries ifln M-lO,ays4a anA are re.ognized as one of the co L..unuity influentialsin rural areas. Although an accruate number is not definitely known, theremay be as many as 6,000 bldans. *The MOH requested kampong bidans to reg'sterby July 1, 1972. The main bidan registration objective is to control themby law anrd at the sa-M time stop the influx of new bida,s by c-urbin regis-tration. On the other hand, the NFPB was planning to utilize bidans forfamily plann'ng arid started their trainirng 'n 1969 with the support of UAICEF.The NFPB and the MOH are now conducting an action research study to assessthe utilization of bidans for family planning with a grant from the uSAIDthrough the University of Michigan. The bidans are paid M$ 30 per month for:(a) recruiting acceptors aa bringing them to tne neaitn centers for initiaiacceptance; and (b) monitoring the use of contraceptives by supplying pillsor condoms at village level after initial acceptance at the health center.A special bonus payment is given to each bidan if a six month assessmentreveals that the quantity of her performance is above average.
4.13 Contraceptive Methods: Pills and conventional methods are pre-scribed by medical, paramedical, and auxiliary personnel. While pills areprescribed without a pelvic examination, a thorough medical history in rela-tion to contraindications is taken. No more than three cycles of pills areprescribed at one visit. Insertion of IUDs, vasectomy operations, and tuballigations are performed by medical personnel, free of charge. Pills are dis-tributed to acceptors at a cost of M$ 1 per cycle and condoms are sold at acost of M$ 1 per dozen; both are distributed free of charge to those unableto pay. One cycle of pills is distributed to postpartum women who want topractice contraception; then these provisional acceptors are given an appoint-ment for a clinic of their choice. The NFPB policy did not permit home visitsby the field staff until recently, prior to that time the mailing system wasthe only means utilized for follow-up of dropouts.
4.14 The number of cycles of oral contraceptives distributed throughthe NFPB is as follows:

- 19 -
Number of Pill Cycles PercentageAcceptors Distributed Sold
1967 18,541 160,000 65.01968 69,337 689,000 78.01969 65,572 979,189 76.01970 49,564 1,068,978 79.01971 47,790 1,162,563 72.01972 48,924 1,154,728 64.0
The mission could not specifically study the distribution of contraceptivessince a commercial system for the national program has not been organized.However, considerable supplies of pills have been sold in wholesale markets --
522,000 cycles in 1967, 758,000 cycles in 1968, and 300,000 cycles in 1969.
Extension of Service by the Ministry of Health Throughthe Rural Health Scheme
4.15 Or2anization of Rural Health Scheme: Since Independence in 1957,emphasis has been given to the development of a network of rural health unitsto provide medical and health services to the rural areas where about 702 ofthe total population resides. The aim is to establish one rural health unitfor everv 50.000 rural nopulation. Each unit comnrises one main healthcenter, 4 subhealth centers, and 20 midwifery-clinic-cum-quarters; theirchaarrtPrist:les are depctrihpri hblow.
a. M:ailn Heal th eanter - nloated 4in ,irnl aar i with A fulll-
time doctor. Usually there is one MHC in each healthdistrict.
b. Sub Health Cernter - lopated in a rural area with a doctorvisiting on certain days from the MHC. Usually four SHCsare supe.nvised by or.e MaC.
c. Midwife clinic-cum quarters - serves as a station fordomiciliary midwifery services in rural areas. Usuallyfour MCQ's are suprised by onn
4.1 f, 're relatl-onshi4ps among the unit com.por.er.ts and tsrgeOt coverageaAof population in the long run are shown in Chart 6483R. Also, a standardst af f -AIng patterLL, WhLiA.1. ch consists of -a total of4 93 heal.t p--- - i. 17
categories, has been established for the rural health unit (Annex 38).Materr,al an.u chi.L.Lu hleaL.Lh serv'ces are being contin-all.y strr.thed g
well as the seven other basic services provided by the unit. There were'44+ rnaiLn hneaLtn centers `'rS)J 1780 subhDeaLth centers (SHnCs) andu 94-3midwifery-clinics-cum-quarters (MCQs) in West Malaysia at the end of 1970.T'ne plan is to establish 22 rinCs, 69 SHCs, and 401 MCQs during the SecondMalaysia Plan (1971-75). The population coverage is still far from the idealtarget of 50,000 per unit set by the Government, but it nas improvedu rapdly
since 1960 when coverage was 638,000 population per unit (Annex 39).

4.17 Effort for Introducing a New Rural Health Scheme: Due to the needto integrate various vertical health proiects into the rural health servicesand as a result of findings of the operational research on local health ser-vice, which was carried out by the MOH in collaboration with WHO in 1969-1971,the MOH is planning to change the existing three-tier rural health scheme toa two-tier scheme, to provide more effective coverage of the rural nonulation.Each scheme will consist of one health center headed by a medical officer and4-5 Kelinik DePsa (rural health clinics) staffed by two multinurnose workers ineach. The population coverage of each scheme will be 15,000-20,000 insteadnf the Pexistina sOn0no. Such a change will he romnlrted bv 19959 The Rrhemewill be implemented by: (a) constructing new clinic buildings following thenew design, t'h' gradually ulpgrading health subcenters to mai-n healt-h renters,
and (c) enlarging the clinic space of existing health centers and midwiferyclinics.
4.18 Clinic Attendance at the !Ural Health Centers: In the year 1970,a total of 2,043,098 outpatient attendances was reported from 37 MHCs and166 SHCs. Based on 272 working doayso per year, average daily attendanceswere 65 at MHCs and 31 at SHCs, or an average of 37 at all health centers.Al,out .'- 40% of te 7,.Cs ,- had 20 A ao4 attenAances andi 51%. of the AmfCs h-ad3 50ftuJUUL 9tu/. U LLII EAL%0L. LC.U ~W LU ~tJ 01 . LCLLU L C 0LU .J I/. Ut L.LL ±MJtA. iLLU .IU
to 199 attendances daily. About 54% of the SHCs had 20 to 49 attendancesandu 15%- of the SHCs had 50 to 1 a9 attenAances Aaily. Average timle spent or, ir.-OUU I.Jt UtI LIUC .JiLL LLCAS -J I LU I I7. I a Cu Lit.C tS LJ.. flV C rC LrC 0C U ndividual attendance was about 10 minutes, assuming that each clinic session1Lastedl U [Lours daiL'Ly. So.ome LLCeaLt Lth centers, Lowe-ver, provdUeu onLy J Lo J
minutes per individual attendance. The work load at some health centers wasso heavy thLat, '±n all probability, onUl±y iorIi.LlJal care could be provided(Annex 40). Each main health center and subhealth center conducts threer-aternal and chilu health (MCHn) cluLic sessionU a Week In Lhe sLanUaam pat-tern. There were 1,353,807 MCH clinic attendances at health centers in 1970;a-verage attendance per session was 49 at i-inCs and 38 at SHCs (Annex 41).
4.. J integration or ramily rlanning bervice wifn Null Service: ine ex-tension of service to rural areas by the NFPB in the fourth phase was impededby the shortage of staff. Having recognized these difficulties, the DirectorGeneral of the NFPB agreed, in principle, that family planning services shouldbe functionally integrated with the rural health services of the MOH. Thepurpose of integration was to extend and maximize family planning servicesin rural areas by utilizing the rural health personnel. The integrated pro-gram is again divided into stages.
4.20 In 1970, in the first phase of stage I, reportedly eight healthdistricts in seven states were selected to cover about 800,000 people. Twoof the areas -- Tanjong Karang of Selangor and Parit Jawa of Johor -- werechosen to determine the extent and level best for integrating family planningwith rural health services.
Achievement of the Integrated Program
4.21 It is now planned to expand the program to the second phase ofstage I to include at least one focus in the remaining four states of WestMalaysia. In all, there will be 14 health districts with a population of

- 21 -
1.82 million to be covered by 1973. This will involve 19 MHCs, 73 SHCs,and iAs MCrQs. ExPnninn tn othpr nrpas wil1 hp in 9tAap TT of the programn.In the first phase of stage II, the campaign will be expanded to the sevenstates which1l are involverd i*n t-he first nhnse of qstag T, for the neriod oi-
1974-75. The last phase of stage II of the integration program will beexpansion to the rest of the states. Accordi4ng t t t-he latPest nian- integra-
tion of the whole rural area will be completed by 1976 (Annex 42).
4.22 Role of Paramedical Personnel Under the Rural Health Scheme:Trained assistant nurses (ITA?J.A a-n m-4ves ---- rise the majior nArt of tlipwork force of the Malaysian Health Services. No less than 4,300 staff memi-bers or .63.5%. of the total nursing personnel (4ncl-in midwi4-- _Jves4 ) wLithin the
services are paramedical personnel. The paramedical personnel under therv -11U-1.. a e- u vu 1 annn w n/ sFIIULra LCteL.,L OcL.e.ne CaUjove aree aIOuL I , - .LnI niLuLer or nearV Of tor taeLnursing personnel under the scheme. In 1970, there were about 6.9 million.atten.Udances at hIealth centers andU a-IbJout 1 .7 m.illion hLome V4silts were made
by health workers. These figures are equivalent to about 14,000 attendancesp r MASI nin 1 ~ v.J-.4 -- rrA.1 42.J_ ..... r. A-.14-..4 - ~-.,,4AWifd.
per~ 1ttN, 91U Liumie LVb.LLs L L per T Lr ULLUW.LLt, andU 5J4 Udie.LpLVer.mdwfe
.js Coverage Of RuLXU.L TargetL rOpU1dlaUtin 1Il #stL.LLIUIzLU LdLL poCLp Ju,.a=
tion of married females, aged 15 to 49, in the rural area was 1 million in1971. Target population coverage per paramedical personnel was 528 on theaverage, and considering TANs and midwives separately, coverage per TAN was2,037 and coverage per midwife was 714. If the Government were able to fillthe posts, the population coverage would drop to 1,180 per TAN, 588 per mid-wife, and 392 per paramedical personnel. It does compare favorably witnother countries: for instance, a full-time family planning worker in Koreacovers 1,600 eligible couples in a rural area and 2,300 eligible couples inan urban area, and in Taiwan a worker is responsible for 5,000 eligiblecouples.
4.24 Performance of Paramedical Personnel: Data from six months' expe-rience in the integrated demonstration area of Alor Gajah are available.During the period from January to June 1971, with 37 TANs and midwives inthe Alor Gajah area, average monthly achievements were 91 new acceptors, 16provisional acceptors, and 640 revisits. These achievements were equivalentto an average of 2.5 new acceptors, 4 provisional acceptors, and 11.6 re-visits per TAN or midwife per month during the period.
Clinic Service by Federation ofFamily Planning Association (FFPA) Clinics
4.25 Recognizing that no voluntary association can hope to provide anationwide family planning service, the FFPA had to be comparatively modest:in regard to both the potential target and the opportunity which exists forfamily planning development in Malaysia. Although a certain amount offamily planning work is carried out in the rural areas by means of motorizedtransport, the service has been confined to large towns and other concentratedareas of population.

- 22 -
4.26 Various contraceDtive services are available in a variety of placessuch as Government and municipal MiCH centers, rented accommodations, estate -disnpnsaripe and hospitals; armed forces medical insnertion rooms, and mn-hileclinics at some rural health centers. By the end of 1971, the FFPA deliveredqPrirPc thrnough 169 uirhnn flini;c and 116 PtAtP rlinicr~ Ahbolt 15% of l1leligible women, aged 15-49, were reached by FFPA clinics during the periodfrom 1962 to 1970. There is an agrpempnt hetween the FFPA and the NFPB forthe NFPB to gradually accept the responsibility of operating some of the FFPAclinics. Hnoweavr mnot rlinir .servir'e nn m,nnagempnt nremiseq will bhe main-
tained by the FFPA in the future (Annex 43).
4.27 All categories of personnel are participating in the service --dortors_i niirses istocial workers, and lav twnrkerQ At- nprscnt, nuor 5T of
those actively engaged in the service are on a voluntary basis. Insufficientresou-frces to attract an naenuate nucleus of -aid full-time professional stsff
-- particularly doctors and social workers -- remain a major problem.
4.28 A choice of medically-approved methods -- pills, diaphragms,condo.ms, foam. tablets, etc., are offered, -bu4.t the ntajJJ. of tJ-r
choose pills. The FFPA is making an attempt to provide, at least in the..nin to-.ns of ecOh state, an alternative form,V of m.ore special4zed tamu.lyplanning services than is possible in a mass family planning program. Forex-ample, the specialized program UAgh inc,4 z ihe atoofmdiaa ~ j.~ A~5L U& . L L .JUU LAILrLL& I. .LJ JL WUL_ J.
coverage, pap smears, pregnancy tests, treatment of subfertility, etc.
B. Limi<LdtatlUons oL thie Delivery System
4.29 Existing capacities of the rural health unit, facility-wise andmanpower-wise, are not sufficient to accommodate additional functions, suchas family planning and applied nutrition because the standard size of theclinic facility in tne health center was designed more than 10 years agowhen the Rural Health Scheme was dealing mainly with the traditional typeof MCIi service. Without expanding facilities and manpower, integration offamily planning will be limited in quality and quantity.
4.30 There has been a trend in increasing vasectomy acceptance in thepast few years. It is not certain whether this is due to increased avail-ability of service or increase in demand, or both. While the Governmentmedical otficers are not officially allowed to perform vasectomies at Gov-ernment hospitals, NFPB clinics are still considered one of the best servicepoints. Most of the NFPB clinics located in the Government hospitals aresuffering from lack of space and equipment. Operation theaters in the Govern-ment hospitals are heavily scheduled and therefore not readily available to eheclient when needed.

4.31 Face-to-face contact is one of the most effecitve methods, notonly i"n = tivating people, but in keeping a close follou of acreptonrin order to improve the continuation rate of contraceptive practice. Un-fortunatelyS ,NPB field workers uptil .ow were not making home visits. Thispolicy has adversely reduced the effectiveness of the delivery system. How-
CL I.L LILC IN LI 1 VJ, v-f.CA LOV L. L .l IUJtL SCA L&lf5
UASeve r, now +4: -NFPB1 worker hlave started hom,e v4siti-ng m-ainly forM lo-! ofdrop outs.
4.32 In the past, over 90% of total acceptors of family planning weret a1,4 ng ora conracep-ve. "I .1 __ :_*4s resu e' rom af cobnto of ace
l. a& VL CX UL.LL .L.VII A. . L. L. L a UL A.II %_I L, -- -L'
choice and the lack of information and education on other contraceptive methods.HIIowever, -iLthe trend 'Ls changing andU the acceptanceterae of vasectuomy is in-creasing. The number of sterilizations increased from 627 in 1967 to 3,477i.L 197 andU thle LNPrrBi andi the 01'1 are quite prepared to emUphasize vasectoml.esand IUDs in the future. If family planning programs are integrated withthLe eruraL LheaLthil servce riatLonwide, all I-lbs ano Srl-s should ue equippedwith clinical services such as the vasectomy and IUD. Equipment for pelvicexarmilnations, surgical instruments for vasectomies, and some simple audio-visual equipment are needed to carry out family planning programs at hea:Lthcenters.
4.33 The standard health center's clinic building consists of four workrooms, a toilet, a room for storage and record filing, and a hall. The sizeof each work room is about 100 square feet and the size of the hall is about200 square feet. Four work rooms have space for dental care, dispensary,maternal and child health services, and a staff office. Clinic buildings inMHCs and SHCs are identical. To extend family planning services, the NFI'Bstaff carry out family planning activities in a corner of the hall or evenon the porch because of lack of space. Usually, the hall is so crowded thatNFPB or health center staff cannot conduct group talks with patients whilethey are waiting for medical care or MCH services. During the clinic session,the limited staff time per patient and lack of privacy make discussion offamily planning services difficult if not impossible.
4.34 Health center workers usually make field trips twice a week, oneday for home visiting and another day for visiting MCQs. Via field trips,health workers provide health education through group teaching and person-to-person contact, conduct follow-up of cases, and provide technical assis-tance and supervision at MCOs. Therefore, an attempt was made to estimatethe traveling distance of health center workers from a NHC to a SHC to aMCQ. While information was available only from 8 health districts (familyplanning integration areas), covering 29 SHCs and 94 MCQs, it was determinedthat the average distance from a MIC to a SHC was 20.5 miles and the averagedistance from a SHC to a MCQ was 10.5 miles. About 7% of the SHCs were morethan 50 miles from MHCs and about 3% of the MCQs were more than 30 milesfrom SHCs (Annex 44). There is a definite need for means of transportationfor health workers, such as a motorized bicycle for supervision.

- 24 -
C. Recommendations
Acceleration of Integration Program
4.35 In order to make family planning services available to the entirepopulation as soon as possible, the implementation schedule of the presentlyplanned integration program with rural health services should be shortenedas much as possible. The Government should correct the situation in whichalmost 90% of the midwifery clinics under rural health still remain unex-posed to family planning activities.
4.36 The Ministry of Health should send out clear instructions to thelocal health authorities that family planning service is one of the majorcomponents of MCH services, even before additional inputs are added to theexisting health service resources. Then each health unit could take a stepforward to start providing family planning services promptly. The existingconcept borne by officials of the MOH and the NFPB is that the familyplanning program is entirely the NFPB's responsibility and that MOH or localhealth authority support to the NFPB's program must be eliminated. If thisis to be the case, all personnel who are responsible for MCH services shouldrealize that family planning services are their obligation and not someoneelse's.
4.37 Recruitment of TANs and midwives in rural health units is urgent.As of October 1971, 42% of TAN posts and about 21% of midwife posts in ruralhealth units were vacant. The MOH should put top priority on recruitment ofthese personnel and minimize transferring them from one place to anotheruntil all rural health units reach an initial level of family planning ser-vices. An additional TAN should be posted in each health center and a newclerical worker's post in each MHC should be created in order to strengthenMCH/FP services in rural areas.
Dece-itralization of Activities to State Level
4.38 The National Family Planning Program in Malaysia is now enteringa new staap nf PxpQnsion. The NFPR Qhnold take steps grandully to decern-tralize some of the activities to the state level officers as far as possiblein order ton pvnna and Petpeni seruirc tn grass roots level nationrally, 4withmulti-disciplinary approaches. Up to now, the NFPB has taken full responsi-bility for every aspect of the program, with direct control over fieldactivities. Such a direct control was feasible during the pioneering stageto creante th*e foundat4n- of various comnponents onf program. activii4--es w..4 .ha short period of time. Now the time has come to organize a body in eachstate to create a locally-oriLertedu program to utilize local resources aUndto facilitate integration with rural health services and hospital serviceswith a reasonUble degree of authority. It is recommenaed that sucn a bodybe organized under the direction of the State Coordinating Committees.

Availability of Family Planning Servicesat Government Hospital Services
4.39 NFPB clinics were responsible for the target population mainly inurban and semi-urban areas because of the location of hospitals. But, Ihospitalfamily planning activities should be extended to rural areas to providesurgical contraceptive methods with a hieher degree of professional skil.l.Rural health service and hospital services should be more closely coordinatedto provide comnrehensive family nlannina services to the target population inboth urban and rural areas. For example, rural health services refer tub-ectomv natients to the hosnital and the hosnital extends clinic service tohealth centers to provide vasectomy operations convenient to the patients'residein e
4.40- Th.n phyTsician sig.nDA tn fnmily planning ap vires- especially to
full-time clinic service, may lose interest after several years because dailyrout.ne sevices are 14m4ted n sT tesgated ser%irp can
eliminate such a problem because more than one physician will rotate familyplanni clinic ass ignmetsaA canpa C4pte 4 oe 4c l t.nial activities
of the hospital.
Role of FFPA Clinic Services Should be Encouraged
4.41 Even after the Government sector is able to provide family plan-niLng serviLces through a'll h elhfclte tther _ill stlll be some of~~LV ~tZ~ IiLUUI1 d~L± LiL LLCU.L1LI LUdL_L.L~L.L=.2, LIICLC W.LJ.L. 0 L.LJ..L --
the population that could be reached more effectively through the privatesector, suc'L; - - - Ar a- fa-L,wLl y- ' plani.g -associatior,._j_ TLhe -private sector is a-'le~ LU ~ ~LLL ~ d dILL.LYP±dLCLiLL.LLV CI:.Jt _kL.LOLL. IzIe jJL.LVC*L= OCL.LL'L.
to select more freely clinic locations and hours of service (including even-JiLgs) dIU LaII prUvidU broadeUr scope OL srLViCe '(to UincL-JUe subfertil llity
cancer detection, etc.).
4.42 The Government should support the FFPA by assisting it financially,if necessary. It should encourage the FrPA to develop its activitles in
areas where there is no duplication with Government efforts. The followingfaciLLties would be neededU to uvercoriie thle ex-st'Lrig LHLmLtatcLons anU i.,.ple.,.ent
the recommendations stated above.
Suggested Additional Inputs
4.43 The following items would be needed to overcome the existing limi-tations and implement the recommendations stated above;
a. Establishment of a state MCH/Fp center in each state tostrengthen administration and service for MCH and familyplanning under a unified effort.
b. Provision of additional clinic facilities for MCH/FP ser-vices in the rural health centers to improve privacy forconsultation and to introduce clinical contraceptivemethods and nutrition education.

- 26 -
c. Upgrading of MCQ facilities and provision of a more com-prehensive service both in curative and preventive aspectsat the MCQ level, to improve the coverage of the targetpopulation.
d. Equipment for vasectomy operation and IUD insertion at allhealth centers where physical facilities would be availablefor the purpose.
e. Provision of a new family planning clinic facility in Gov-ernment hospitals to increase work efficiency and to improvethe identity of the clinic to the public.

- 27 -
V. AVAILABILITY AND TRAINING OF HEALTH PERSONNEL
A Aon4,~.c4-..44..In. Existir.g Situati-r
brief Review of Health Manpower
5.01 Medical Doctors: At present more than 90% of the authorized postsfor medical doctors are filled throughout the medical servlce systemi in WlestMalaysia. The Ministry of Health employs 1,028 Government doctors -- about96 of them (9%) are from such countries as Egypt, Indonesia, Korea, Pakistan,and the Philippines. In addition, there are about 1,500 doctors in the pri-vate sector. During the Second Malaysia Plan period it is estimated thatanother 140 doctors will be required for the health services. Since 1969,the Faculty of Medicine at the University of Malay, which has an annual irn-take capacity of 100 to 120 students, has been graduating medical doctors.
5.02 Nursing Personnel: The nursing service system in this country isreasonably well established. About 6,000 posts have been established infour major categories: matron, nursing sister, staff nurse, and assistantnurse (TAN). About one-half of these posts are for assistant nurses. Ingeneral, the vacancy rate is 20%; however, it is higher in the Rural HealthScheme than in the hospital service. In the rural health units, about 42%of the assistant nurse posts are not filled. According to Ministry of Healthestimates, an additional 1,000 staff nurses and 900 assistant nurses will berequired during 1971-75 (Annexes 45 and 46).
5.03 Midwives: Midwife posts in the Government medical services numbermore than 2,500, with over 80% of them filled. More than 70% of the totalposts are located in the Rural Health Scheme where midwives (together withassistant nurses) are key MCH personnel. About 150 midwives graduate annuallyand as no provision has been made to increase this training capacity, a shDrt-age of 400 midwives is estimated for the 1971-75 period (Annexes 45 and 46).
5.04 Other Paramedical Personnel: In addition to nursing personnel,paramedical personnel, who are related to family planning and who playan important role in the health service system, are public health inspectors,public health overseers and hospital assistants. The first two are engagedin environmental health and the latter in outpatient care. There are about1,900 posts for these three categories of personnel (Annex 45). Previously,hospital assistants were trained at nursing schools until a new school,attached to the General Hospital at Seremban, was started early in 1971.Training courses for health inspectors are conducted by the Public HealthInstitute: beginning in 1973 the duration of these courses will be increasedfrom one to three years.
Education and Training of Nursing-Midwifery Personnel
5.05 Registered Nurses: The education of registered nurses is providedby three Ministry of Health schools of nursina which graduate a total of

- 28 -
about 260 nurses annually. There are, in addition, two other schools ofnursing in West Mzalaysia -- one within the Medical Center at the Uniiversityof Malaya, and one private school connected with Assunta Hospital. The annualoutput of these two schools is limited and their graduates are mainiy aDsorDedby the hospitals with which the schools are connected.
5.06 The Health Ministry is planning to open two new schools of nursing:one in Kota Bharu in mid-1972 and the other in Ipoh by 1974 or 1975. Thismeasure seems justifiable since the annual increase in student intake -- from900 to 1,051 in 1971 and to 1,350 in 1972 -- will not be sufficient to fillthe gap between available resources and projected requirements for the nextdecade.
5.07 A comprehensive four-year basic nursing education curricula isbeing designed to prepare students in the field of nursing and midwifery,including public health nursing. This new curricula was to replace thethree-year and four-month program which, although it included experiencein public health nursing, was mainly hospital-centered with reliance on spe-cialized post-basic programs to prepare nurses for special fields. In actualpractice, the time required for the preparation of a public health nurse-midwife is a minimum of 5 years and 4 months with emphasis on three separatecurricula:
Basic Nursing 3 years and 4 monthsNursing-Midwifery (Division I) 1 yearPublic Health Nursing 1 year
5.08 The implementation of a four-year basic nursing program which in-cludes midwifery and public health would speed up the preparation of nursesfor rural health work.
5.09 Assistant Nurses and Midwives: The training of assistant nursesis provided in 17 schools including 2 special project schools -- the mentalhospital and the leprosarium. It is a two-year course for candidates whohave completed 9 years of general education. Midwives are trained in 13hospital schools supplemented by domiciliary midwife training centers forfield training in home deliveries. The course is a two-year one for candi-dates with six years of general education as a minimum requirement.
5.10 The physical facilities for teaching assistant nurses and midwivesneed much improvement. The capacity of these schools is, in general, limitedto 20 to 40 students. The hostel facilities in the health centers wherethe students stay during their period of Dractice in rural areas (RiX monthsfor midwifery pupils and one month for assistant nurses) need also to beexpanded anndpniqatp tranSport (bicyrles nr unn) needs to be provided.
5.11 The impression gained on, a field visit to midwife clinlcs-cum-quarters was that midwives working in isolated communities are likely to be.ndere.mployed. 'Their functions are limited to .mternal care (pre.natal, n l.-aa,and postnatal). The question naturally arises whether the midwife could be

- 9Q -
trained as a multipurpose health worker who would exercise broader functLonsthan she does now.
5.12 Community Nurse Program: The Ministry of Health is developing aprogram for training community nurses (multipurpose auxiliary health workers).The present role of midwives in the rural community does not adequately sa-tisfy the needs and demands of the population. It was proposed that theassistant nurse and non-nurse midwifery training be combined to create the"community nurse." The objective of this program is to train only one cate-gory of auxiliary nurse to function both in hospitals and in the healthservice. The community nurse will be more acceptable to the community ifher scope is broadened to include preventive and curative services.
5.13 Community nurse training is preferable to the existing assistantnurse and non-nurse midwifery training for the following reasons:
a. the comprehensive training would prepare the pupil to beboth an assistant nurse and a midwife who could performmultipurpose functions at an auxiliarv level:
bI thp rtirriel iium wouil d redrie to twxo years the time requiredfor the preparation of assistant nurses and midwives;
c. through regionalization of schools greater economy in theuse of teaching staoff would be achieved annd quanlifiPed tuitorsfor the program would be provided;
d. and also, through regionalization of schools, more uniformityanid. better coorA4natlon of the total trair.ing progr a m, intheory and practice, could be developed; and
e. regional facilities for training would be more economicalariAU efficiert.
5.14 This plan would increase the health se.c d T.Trn,1 nachieve a better utilization of the qualified tutors to be provided for the
-program.. Xs ThsLsuV; inov sv ar, u Lcores 'L s'Lz :: asU we'L' s renoLBlvaCl 4on and rei,- -irsG
of the present assistant nurse training schools, which are to serve asregional training cent-ers fLor a 'larger num,ber oil students, and/or construction4_of new school buildings. The first regional assistant nurse training schoolin 1--antan -will lbe establ3ished in 1Q972-73, -with a caact ofaout 200.L.4 iui L\U I L..L. U~ Ld.I.LLI~ 1.1 u in I9 2 I WI. LII a #C&jJFaU. L L, S CU& Jau .S"
trainees.
5.15 Family Planning Content in Training Curricula: The inclusion ofcomprehensive family planning training in basic nursing program-s L8 esseatalso that the graduate nurse of tomorrow will be prepared to support familyplanning as an integral part of nursing practice. At present, some instruc-tion in family planning -- in the form of three 45-minute lectures and someobservations on family planning activities in health centers and familyplanning clinics -- is included in the third year of the basic curriculafor nurse students.

- 30 -
5.16 Most, if not all, qualified tutors in the nursing schools haveattended short courses in family planning at the National Family PlanningBoard. However, the schools of nursing lack the necessary commitment topush ahead with the integration of family planning into the curriculum andare therefore, failing to give the students a sound education in the broadaspects of family planning, its philosophy, theory, and practice. Adequatelibrary resources for reference and additional readings in family planningand related subjects are also lacking for the proper implementation of familyplanning teaching.
Rural Health Training Centers
5.17 Since the inception of the rural health service scheme in 1956, oneof the main health centers in Jitra has been functioning as a demonstrationhealth center for inservice training of health personnel. Additional facili-ties, such as classroom, demonstration room, library, and dormitories havebeen added to the main health center. In 1966, another main health centerin Rembau began providing inservice training similar to the Jitra center.
5.18 Both centers have trained about 2,500 health personnel throughvarious inservice training courses during the last 15 years. Major 10 to16-week training courses consisting of theoretical and practical training.with special emphasis on rural health services, are conducted for auxiliarypersonnel such as assistant nurses, midwives, and public health overseers.In addition to these regular courses, the centers also provide field trainingfor the trainee from the Public Health Institute, Kuala Lumpur. The centersserve so-called "accredited training centers," for the Public Health Institute(PHI). While public health nurses or public health inspectors are receivingbasic public health training at the PHI, they attend three field trainingsessions (3-4 weeks duration each) within a one-vear period.
5.19 The centers also provide a three-week orientation course for medicalstudents and a four-week inservice training courses for supervisory staff.Mnst of the courses introduce family Dlanning subierts during theoretical
and practical training. During the training of the assistant nurse and themidwife, a one-week session on family nlannino is inluded (Annexes 47, 48and 49).
Training Activities of the Public Health Institute
5.20 The Institute conducts about 25 different types of courses forabout 500 to 600 students a year. In most of these courses, elements offamily planning are incorporated to varying extents. There is also pro-vision for special seminars to be held in various public health projectswhich could include family planning information.
5.21 The Public Health Institute plays a part in offering advice tovarious agencies on public health matters, e.g., the Public Health Instituteis a member of the Central Coordinating Committee dealing with the integra-tion of family planning with the rural health services. The Director of

- 31 -
the Institute is also Chairman of the Training Subcommittee of the aboveCommittee.
5.22 The staff of this Institute also provides various agencies in-cluding the National Family Planning Board and the voluntary tamily planningassociations with lecturers in health education and rural health servicesfor the various family planning courses that these agencies conduct. TheInstitute also has the capacity to prepare and pretest some audiovisual aidswhich could include family planning material.
Activities of the National Family Planning Board
5.23 The Training Division of the NFPB had trained a staff of over2,900 in family planning ranging from NFPB medical officers and familyplanning workers to other personnel which the Board felt could be utilizedto extend family planning concepts and services to the general populationby the end of 1971. About 164 courses of different types were offered,ranging from orientation to specific projects, and lasting from one day t:ofour weeks. Training and Medical Research Center at the Government MateimityHospital in Kuala Lumpur serves as a training demonstration center forthe practical aspects of family planning training. Programs are arrangedin such a way that when trainees are scheduled at a time when the stafffrom the Center are present to demonstrate the practical aspects of famiLyplanning training. At the same time, the staff provides field servicesfor patients residing within a radius of 10 miles of the Training andMedical Research Center (Annex 50).
5.24 Since the integration program started, the NFPB has engaged intraining of trainers, e.g., training doctors and professional nursing staffs;they, in turn, will train subprofessional nursing and midwiferv staff atthe local level. This training program, therefore, is the key factor inexpediting the integration program to cover the whole countrv.
B. Limitations
Programming of Trainine
5.25 Much has heen done to prepare nursing midwiferv personnel forfamily planning activities in West Malaysia. However, there is still a longwav tn gon as oC rAl n,ir-ino-miit.wife-rv rtaffR in hnanif-nla nnti henlth
centers do not consider family planning an integral and essential part coftheir !dail, work. In the dvlopment of an adequate family plar.r.ing programas an integral part of nursing-midwifery practice, priority should be givento the training of teachers, supervision, and co4tiruing inservice edution.
Preparation of "u-tors
5.26 The: prVparato.L of tutors 'as not beer. abLle oke-aewtthe expansion of~ the L traini s ouL .LiA pUr sent LU avai-l WqaLfiL
the expansion of the training schools. At present, most available qualified

- 32 -
tutors (a total of 34 for West Malaysia, as of February 1972) are in schoolsof nursing and post-basic -roranms for nurses arnd m4dwives.
5 NY,,,one of the teachers in traingn- schools for asslstant nrseand -
midwives (Division II) has received formal preparation for teaching. Effortsto coApn sat e * the _orta g S ofA tu t rs. . fhrog- _ ot J p rovsion tf inse4 Av 4i
education for nursing sisters have helped to implement orientation and otherstaff. dAevelopmentu programs for auxiliaries.
Upgrading of Nurses TrainingAr
,.28 Specifc plans have been made ly -le ,Nursir.g Div'sion of the Min's-J *0. ~p c..iL JLLO LL~V U~L IU~ ULi Ltl l UL~± L.V.L X LU U LiA 11±.L S
try of Health to implement a four-year basic nursing education curriculum,WhICh LncluUes Ll.,LU ICLfy adLU pUU.L.L hLeta.LL Ltrainirg, aiiu Lo inLLcreasCe Lte
student capacities of the schools. An effort to develop a community nursetraining program through combining the assistant nurse and midwifery trainingand regionalizing the training both fit in with the policy to broaden thefunctions of the MCQs, and increasing therefore, service coverage. Tnesemodifications involve expansion of the present physical facilities for teach-ing, practical experience in rural areas, and nostei accommodations.
5.29 There are, however, some important problems to be solved duringthe implementation period. For example, (a) adjustment of the nursing staffpattern when cheap student iabor is no longer available; (b) retraining TANsand midwives in order to upgrade them as community nurses; and (c) coordina-tion for discontinuation of existing training courses and setting up retrain-ing courses with minimal interruption to the health services.
5.30 The teaching of family planning in the nursing schools and in thetraining courses for assistant nurses and midwives is inadequate to preparethe students to function as family planning workers in a variety of settingswhere family planning needs are present. Adequate library resources forreference and additional readings in family planning are also lacking forthe proper implementation of family planning teaching.
Shortages of Nursing Personnel
5.31 If we assume that the additional manpower requirement for nursingpersonnel would increase by 50% during the period of the Second MalaysianPlan, shortages of 1,081 nurses and 935 assistant nurses will exist duringthat period. Even the requirements for nursing personnel will increase by47% for nurses and 137% for assistant nurses during the same period (Annex51). Establishment of the two nursing schools in Kotabaru and Ipoh wouldnot affect production of nurses before 1975 because of the long duration ofthe training courses. The gap between present number and future demandof nursing personnel is one of the most serious problems to the healthservices and to the national family planning program. However, both quanti-tative and qualitative aspects of the problem can be solved by rapid regiona-lization of the schools for assistant nurses.

Inservice Training Backlog
5.32 Due to limited training capacities and a large training target,only 40% of the existing assistant nurses (TANs) and 15% of the midwiveshave received inservice training up to June 1971. The number of TANs andmidwives to be trained at RHTCs is estimated at about 2,500 for the perio&Lof 1972-75. Thus, it will take 17 years to complete inservice training ofTANs and midwives if RHTCs continue to maintain an annual training capacit:yof 144 students.
Under Rural Health Scheme TANs Midwives Total
Existing number of staff 491 1.403 1,894Number of staff trained at RHTCs 197 239 436Expected number of staff by 1975 1,161 1,767 2,928Number of staff to be
trained at RHTCs 964 1.528 2,492
Weaknesses of the NFPB Training
5.33 Training at the NFPB level suffers from several shortcomings:
a. thp exiRtfna nhvysnal factlititR rectriet trainina activitiesto about 30 students per course;
b. textbooks and manuals are in short supply, and in somecases, oultd-ated; and
c. both admin4strative and financial respo.sibilit4es fortraining health personnel at the local level are not^learly Aef 4nred... LO L J. C A~l I 4 .6* 1.VJ J CL .*L 9- u
5, 34V 1 JL ~JOf A -M,.IZ '972, the I £1 LC G. ha .zlrady exhiauste the trair.in
budget, as only M$ 25,000 had been approved against M$ 231,510 requestedby the Trainin.g Dii.sion of tb.e Nf.. Furt1be-re, I . thr ls 4 -r
that the NFPB will get additional funds for training through the supplementLary
that the NFPB budget allocation is adequate to support family planningLraLILng aL Loca'L levels as well as at tiLe centraLl. leveL.
C. Recommendations
c r ,r mu . _ _ _ , ,__ .u _ * . _ ___ ____J. JJ I e runistry oL nea±Ln in conjunction witn irrrn is planuiLng oorganize four regional centers for short-term training of paramedical staff,assistant nurses, and midwives in order to expedite the integration offamily planning with rural health services. About 12 courses, each witha three-week duration and accommodating 25 students, wiil be scheduled byeach center annually to complete the family planning orientation course

- 34 -
for the existing 2,500 paramedical staff in rural health services. AccordingL. the1 ti,utale the training ---- ---- several years to complete andan attempt should be made to shorten this schedule.
5.36 All tutors in schools for nurses, assistant nurses, and midwivessh o[uldU receiLve orien.tation to the aims, Uetho ds, nru. organization of t.he
rural health services in order that teaching in all subjects and trainingat every stage will 1 .Le directeud toward coordinatLing prL=V-=en.'Ve -Ad cu-ative
nursing services in both rural and urban areas. The teaching staff shouldalso master tEne LacLual Juater'La'L anu uasic coUmUIUnicLatioUnL skis LLn hL eLreL-LLt
in family planning in order to effectively conduct orientation and trainingof other nursing teaching staff. international assistance may be needed toassist the schools with the introduction of family planning in the nursingcurricula.
5.37 High-quality supervision, sufficient in quantity, is perhaps themost effective means of raising the standard of MCH/FP services. Shortageof staff transport and appropriate utilization of senior staff time havesometimes reduced supervisory activities. There is a great need, especiallyamong state, district, and field staff for more close contact, guidance, andopportunity for discussion and exchange of experience with senior staff.
5.38 The Public Health Institute should be able to meet the requirementfor quality supervision. The opportunity tor face-to-face contact to enableguidance, service demonstration, review of records, etc., involves adequatemeans of transport, and a reallocation ot supervisory statt activities toenable the staff to devote more time to technical supervision. Continuinginservice education for all staff in hospitals and extra hospital servicesand regular contact between hospital and health unit staff are essentialfor coordination and high quality MCH/FP services.
Additional Inputs Required
5.39 In developing family planning as an essential component of varioustraining courses for nursing-midwifery personnel, nursing advisory servicesshould be available to the MOH. However, this assistance has already beenincluded in the WHO-assisted project "Development of Health Services," inwhich provision is made for a public health nurse educator starting in mid-1972.
5.40 Fellowships should be offered to prepare nurses for leading rolesin teaching, administration, and implementation of nursing components ofMCH-FP services.
5.41 Materials for the library in nursing schools and assistant nurse-midwifery schools are needed.
5.42 Construction of one new rural health training school with atraining capacity of 60 students on the East Coast sqhnouldl hp tmnernrtak-ln.
- 35 -
5.43 Construction of an extension to the rural health train.ing schoolat Rembau should be undertaken to increase the training capacity to 60
students.
5.44 Vehicles are required for transporting rural trainees and auudo-visual laboratory sets are needed for three rural health training schools.

- 36 -
VI. INFORMATION, EDUCATION AND COMJMNICATIONS
A. Review of Existing Program and Facilities
6.01 Since its inception in mid-1966 the family planning program inMalaysia has been successful in attracting a substantial percentagee ofacceptors among eligible women in urban areas. Program strategy to establisha large core of acceptors among those women most likely to accept is verysound. Urban people are better educated, more innovative, and are easier toreach than rural dwellers. The information effort to support this initialphase of the program required only making people aware of Government servicesand announcing location of services. These obiectives have been largelyaccomplished.
6.02 But now the program is entering a much more difficult stage. FamilynlAnnino srvi1r.9 arp being integrated with MCH activities in a phased fashionin rural areas. The communications task, while much more difficult, will bevital to the success of the National Family Planning Program effort. The
communications effort must be directed towards convincing potential acceptorsthat contrarpntion is a socially accentable nractice; that smaller size
families of two and three children are desirable, and that the Governmentfam41ir plannInc progcrszm ic aloa rq 1 frnTm ti Pi 71d4y4rIii1n fnmiIv und rtmmutnInt
point of view.
6.03 A wide variety of Government mechanisms exist for carrying outinfo.m.ational, motivational and educational family planning activities.Major responsibility for energizing this system has been given to the In-fPorma-ton Division of the National Family 'Planning Board4. Thec Info=mationLUL hid L. L jJ.. V± UL L it ~ L 11 IN .. LJLC I CII.L .
7i a *.1
6it a h 1 U I LhtII L
Division consists of a headquarters in Kuala Lumpur and ten regional in-formation offices located throughout TWest Malasia The-~ hedqatesstfiLl LL~±L U. L £ 1 ±LaL U LI LJU i'L V~ L. rLJ-..LCtYZ.LC. II h aU.UL L -1i-CX4AC L.AZ *LdCI
includes the Head of the Division and three other professionals, two tech-nicians, anu a clerical stafL. ihe IleadquartLers unit supervLses andU coorudi-nates the information work of the regional units, develops and producesprinted and auULo-vLsual miaterials ilor use iin group sessions by the 'UiloUL-La-tion Division and other Government organizations, and prepares publicity andprograms for the mass media. The unit also maintains liaison with Governmentand political agencies, and provides information to opinion leaders.
6.04 Since its inception in 1967, the Information Division has producedone 16 mm motivational film, a number of booklets and leaflets, and a set ofposters. These materials are available in all languages and are providedfree of charge to all N FPB clinics, FPA clinics and Ministrv of Health serviceclinics as required. They are also available to extension personnel of otherministries on request. In 1970, over 800,000 copies of booklets and leafletswere distributed through these channels. A monthly radio program in Tamil,Chinese and Malay is prepared by the Information Division and broadcast by

Radio Malaysia. The program is originally heard during the early eveninghours n'nd is later rebroadcast in tne afternoon hours. Tlle LoLiiiaL varles,but generally consists of a panel discussion about population problems fromthe point of view of the nation, the community and the family. Lne Informa-tion Division also prepares and distributes a Population Nexwsletter in bothMalsy and English which is distributed to over 7,000 people monthly. hLleDivision arranges for television coverage of newsworthy population eventsand handles press relations for the N FPB. A wide variety of news and featurestories appear in both the English and vernacular presses.
6.05 At the regional level, all the information units have been suppliedwith an audiovisual van. Regional Information Officers are obliged to planfor at least 21 public address cum film shows each month, 14 group talks and.at least 3 days for exhibitions. These activities are frequently held inconjunction with extension officers from other ministries, but are alsoarranged in collaboration with NFPB cinics, Family Planning Association'sactivities and health subcenter programs. Typically, two or three developmentfilms are shown, including a family planning film which is introduced by ashort talk. Booklets and leaflets on family planning are available on request.
6.06 The Regional Information Officers also spend a good deal of timein working with extension officers from other ministries to encourage themto include references about family planning in their educational programs.They also work closely with Ministry of Information and Broadcasting Informa-tion Officers in the regions who are much better equipped to reach rural areas.Some of the NFPB Regional Information Officers have been asked to talk tosecondary school children about population dynamics and effects of populationgrowth. Another important function of the regional staff is to sample theclimate of opinion concerning family planning so that it can be used indevising communication plans and strategy.
6.07 Supervision and coordination of the regional units come from Informa-tion Division headquarters, but the regional units have close association withMinistry of Health personnel in the region.
B. Limitations of the Communications Program
6.08 The communications program of the Information Division adequatelysupported the services component of family planning in the 1960s. However,it does not appear to be able to meet current challenges and opportunities,nor those which will be presented in the near future. This is not a resultof poor leadership. Limitations of the present program stem primarily fromthe shortage of funds,, shortage nf trained personnel;- and nolicy restrictions.It should be noted that in the following paragraphs the limitations apply tothe total family planning information system, not only those over which NFP3has immediate control.

6.09 The Government at present has a low-key family planning program,thus compromising the possibility of a forceful campaign by the InformationDivision. The role of radio and television is illustrative. These media,which undoubtedly have great potential in the family planning communicationscheme, are being used sparingly if at all. The Information Division's op-tions have been further reduced by the Government's decision to use only the"health" theme in promoting family planning.
6.10 Any family planning education program has limited chances of successif it has to operate under these restrictions. The use of mass media to"legitimize" public discussion and to "surface" population issues can becrucial in achieving program goals. Further, all available evidence indicatesthat most couples become family planning acceptors for economic rather thanhealth reasons.
C. Recommendations
Communications Strategy
6.11 The communications program should be directed not only to eligiblewomen but should also focus on husbands (who are a very important factor inmany women's decision about contraception), conmunity leaders, religiousleaders and health personnel charged with the responsibility of deliveringfamily planning services. A continuing effort should be made nationally,among elite groups, to interpret program objectives so that public supnortof the program will be strengthened. This new and enlarged communicationsprogram must reach a constantly expanding number of rural couples with con-vincing messages, utilizing a variety of media, with appropriate frequencyover a period of time. A vastly expanded information effort at the NFPB-and including regional information units, will be required.
taterials Development
6.12 A second need is the development of a wide variety of new, innova-tive educational and informational materials. Such materials should bedeveloped for specific target groups, which are now to be approached withserviCe s i.e., proorly-educated rural groups in integrated areas, inustriLaLworkers, and inhabitants in low-cost housing schemes. These materials might
inclue sl rated booklets, sound/film.strips, 2 x 2 olidesets, radio dramas, films, newspaper releases, and feature stories. Thegeneral theme of these material's should popularize the two- anid three-childfamily and should emphasize the purpose of the national family planning pro-gram which is to assist eachi fami [y to have thet numuer of children tnat itdesires. These two educational objectives may seem to be at odds since mostevidueice Lnduicates thLat ,lalaysian couples want large fami'ies; but they arehaving more children than they want. A campaign which will depict the Govern-menE family planning program as one giving couples the freedom to choose the
- 39 -
time of the next pregnancy and assisting couples to have only those pregnanciesthat they desire should prove effective in the rural areas. Rural people LnMalaysia, like rural people everywhere, are conservative in their outlookand resist change until it has been demonstrated that change is advantageols.Any communications program should be directed towards designated targetgroups and should include individual, group and mass media. Examples ofsuch media are:
a. Individual: Booklets, pamphlets and leaflets listing reasonsfor family planning should be developed and distributed bv allGovernment personnel contracting rural couples in integratedareas, industrial workers, and dwellers in low-cost housingschemes. Other booklets on human reproduction and birth con-trol methods are needed for distribution by health nersonnel;
b. Group: Flinhooksj sound/filmstrips, charts and transnarencieslist:ing reasons for having onlv those children desired bycouples are needed for use by all G-overnment extension personnelwho contact groups in integrated areas. Other group mediacovering human reproduction and family planning methods arerequired for use by health personnel with groups of acceptors;and
c. Mass Media: Radio listeg..ig ls very common among all classesof Malaysians, therefore, this medium should be used much moreextensively. Apparently, dramas and casual 'talk sh-ows very popular and it is suggested that these formats be used.BecaVuse urbaL. andu rural areas are coveredeU extensively uyaudiovisual vans from various ministries, additional familypla,n'nig fl±ms woulU receive wiCe circuLatiLonL. These Lil±Lms
should attempt to shift family size, attitudes and normsthlrougn carefully thought-out themes, but they snoulu notdiscuss contraceptive methods. Newspapers can be utilized forcirculating both eUucat'Lo.aL andU pubLiLc informational materials.A weekly question and answer column on human reproduction andsimple contraceptive advice can be easily ueveloped and dIstri-buted. Such a column can be "regionalized," in that prospectiveclients can be directed to specific district and generalhospitals. Such columns, appearing in both English andvernacular presses can attract a very substantial readershlpin a short time, with a minimal effort. Television, as wellas the press, should be utilized to mobilize puDlic supportfor Government family planning activities. Panel discussionswith leading medical authorities, religious leaders and aspoliticians about the necessity for limiting populationgrowth, as well as the reporting of program success storiescan be useful if participants are selected on the basis oftheir ability to communicate freely and openly. At times,sports figures, movie stars and other popular figures mightbe willing to participate and endorse family planning.

- 40 -
Population Education in the School System
6.13 Any program to develop communications materials for family planningshould not neglect the area of1 population ed'ucatiLon 'ln thLe school system.There is an increasing awareness among educators of the important role theycan play in assisting the nation to solve its mOSt perplexing proDlem. Educa-tors are understandabiy cautious of "Sex Education," or even "Family LifeEducation." But tnere appears to be no reluctanlce to include populationdynamics, and the effects of population growth in school curricula. TheInformation Division of the NFPB should increas? its capacity to developcurriculum materials for use in public schools and to collaborate with theDepartment of Education in developing teacher training programs. The Ministryof Education has recently drawn up a detailed scheme for the introduction ofpopulation education.
Training Materials and Programs
6.14 A wide variety of training materials, particularly sets of overheadtransparencies, 2 x 2 slide sets, and sound filmstrips should be produced bythe Information Division and reproduced for distribution to training centersresponsible for providing family planning content to field personnel. Suchmaterials should be planned in collaboration with the NFPB Training Division,Ministry of Health training people and the Public Health Institute. Examplesof materials that would be extremely useful is a series of transparencies onpopulation growth of Malaysia, contrasted with population growth in France,India and Ghana. Other transparencies could be produced on the organizationof the NFPB, the integrated MCH/family planning program, and illustrationsof various growth rates on the age composition of populations. Sound filmu-strips and 2 x 2 slide sets can be produced covering human reproduction,contraceptive methods, community organization, interviewing techniques, clinicorganization and record keeping, as well as other instructiona] areas coveredin training courses.
Research and Testing
6.15 The Information Division does not have the expertise and manpowerto carry out even moderately sophisticated communication research prolects.A vast amount of client time is wasted during periods when women must waitfor a doctor or a nurse in a clinic. Since nurses are generally too busyto carry out "motivation" during these periods (especially in subhealthclinics), efforts could be made to utilize that time for motivation andinformation via self-instructional materials. Other kinds of communication".svqtpms" lay equallv unexnlored.
6, 16 At the cent-ral I eupel, a greatPr rnrdination bet.wveen all the agenciesthat can be used for family planning information has to be brought about bythe iTFP Tn Tnfnryst-4n T,r, tr4c4n4 t ton nimprove the popula-tin --ea-
6.17 Assist-Nt nurses, staff nurses, and other staff in the rural healthcenters should be trained in the use of audiovisual equipment and motivationaltechniques t1o reachO thLe eligible mothers. Such training can fo', . part of theMOH training program in family planning.
6.18 Face-to-face motivation and follow up of dropouts should be encouragedUy iL OVL sLtaff £ t hrough th L'Le I' oiLie viLsi'LtiLng program.
D. Required Inputs
6.19 To develop the NFPB communications program described above, it willbe necessary to strengthen the Inrormation Division or tne NFPB and its fieldunits along with the health education program of the Ministry of Health whlchmay also focus on this probiem because or present sensitivities. Tne follow-ing activities would be required for the expansion of information activitiesof the NFPB.
Educational Material Production
6.20 The production capabilities of the Intormation Division should bestrengthened by providing equipment for the establishment of an EducationaLMaterial Production Center. A broad variety of information, education andcommunications materials should be created and developed for use by the NFPIBand for distribution to its regional offices, the Ministry of Health (includingthe Public Health Institute), the Ministry of Education (population educat-Lon),and other components of the Government information system. These materialswill allow the NFPB to develop booklets, brochures, flipbooks, sound/film-strips, radio tapes, and other kinds of audiovisual aids for use in trainingprograms and population education programs. The educational materialslibrary, a resource center stocked with films, slides, and audiovisualmaterials from around the world would be useful in providing ideas for thecreation of Malaysia-oriented materials. Similar capability should be devel-oped at the Ministry of Health for producing material for the health educa--tion program including the family planning content.
Strengthening the Regional Units
6.21 It is proposed that each regional MCH/FP administrative unit bestrengthened by the additional audiovisual van unit in each of the elevenregions. In addition, each regional unit would be supplied with equipmentto establish a small educational materials laboratory. It will expand thecapacity of regional MCH/FP units to penetrate rural areas and to experimentwith developing localized audiovisual materials and techniques. Each regionalunit should be supplied with an additional mobile van to increase its ruralarea coverage. In addition, the regional units should be provided with suchstandard equipment as projectors and audio tape recorders.

- 42 -
6.22 The Regional Infonnation Offices, of wqhich there are at presentten, should be increased to correspond to the eleven MCH/FP AdministrativeUnits at the state level. Each of these offices at each unit should be fullyequipped to meet the local requirements and provide logistic support to theproposed Health Education Officer to be appointed for each state.
Educational Program for Rural Health Centers
6.23 All rural health centers should have audiovisual equipment. Thisequipment should be designated explicitly (but not exclusively) for use infamily planning information work with clinic "clients' and would be intendedto help medical staffs carry out informational and motivational work bothby providing them with communication tools and by allowing them to "automate"some of the information work. This equipment, along with "software" materialsnroduced by the NFPB_ should dramaticallv improve educational programs inrural areas. Family planning instruction can be carried on in a systematicfashinn w7ithin rlinir settings Training mater4als for rural hpaltlh personnelcan be utilized at the main health centers for staff development.
Technical Assistance
6.24 Advisory Services: UNESCO in 1971 posted a short-term mass communi-rations spetrialist to work with the NFPB Information nivisionn This speialistshould provide much needed assistance in planning the utilization of massmedia. Another adv4s-er fncr oQtahlichinS thq- FAitu-nt1nnnl Material ProAdution
Center would be needed for two years at the NFPB. He would also help inmaterial development, particularly for the demonstration pro4ect. H.e wod1Aalso assist the Ministry of Health in the production of health educationmaterial.
62 55 The c.mm.un i cati o n s progrwnm in Mala-sa,- 141- family p1lnn 4 -- pro=
grams elsewhere, requires a research and evaluation component to ensure that.le progra..m is properly focuseA ar,d i8 achi&eving itLs obJectives. AVos
nothing is known, for instance, about which messages are most likely to inducech'an-ges 'n contraceptive behavior. Studies on effects of: various "mi'xes" ofL~~IL~~1I~C~~ LU ~~UL&LL JL.LVC U~~~~LL~~V1UL. .)LUU.L~~~~~ IJLL CLLCLLb UL VdLLOU=11 L D LU.LALL L OL
media on attitudes and behavior are also required. The communicatons researcha(lviser should be assigned to the Research Unit of the Evaluation Division,NFPB, but will work closely with the Information Division in developing,pretesting and evaluating tecnniques for information, education and communi-cations materials and programs. He will also be involved in the demonstrationproject in estaDiisning research projects to determine the most effectiveappeals to various audiences, and differential effects of media on specificaudiences.
6.26 The third area requiring attention is population education. Acarefully outlined program, including seminars and conferences, as well asthe development of audiovisual curricula materials as prototypes for evalua-tion might provide an entrance into the formal education system. An adviserfor this purpose would be needed in the Ministry of Education.
- 43 -
6.27 Fellowships: Long-term and short-term fellowships are needed toprovide adequately trained manpower immediately for the .N1F.PB informationunit and for the Ministry of Health education unit.

- 44 -
VII. E UVALATION OF THE PROGRAM
A. Existing Situation
Obiective
7.01 The stated obtectives of the evaluation proRram of the NationalFamily Planning Board are:
a. assessment of program effectiveness and progresstowards the attainment of national obiectives; and
hb nrnmotion of stndfes and research on: (i) inter-relationship between social, cultural, and economicfacrtnrs nnd nnni,l,tlnn rhnngpes and (ii) fprtil1 tvand mortality patterns in the country.
Agencies
7.02 The evaluation activities of Malaysia's National Family PlanningProgram are undertaken ai.o-st e-cu-si-vely bDy the Evaluationn Dtricin of theNFPB, with some involvement of the Training, Education, and Research Divisionon a proJect basis, and witAh substantial technical support by the Give-.ment'sDepartment of Statistics. In the past, there has been technical back-stoppingprovidL'ed unduer FlordU Founation- ausice by the, Unierit ofichigafsou
J. ivJ.Cu ILUC5. < itU .Li -LA,AL. t.-L -t oJ ...- LI Y tA I .- , .I CL lyt Lit L L..LL.L5
aLL a £ LVPU-
lation Studies Center (1966-69) and by the Center for Population Planning
Facilities
7.03 The Evaluatlon Divisio n of the Frl-B is staffed currently by 1'members under the supervision of its Acting Chief, a trained statisticianand evaluation specialist (i.S. degree in Population Planning, university ofMichigan, 1970). He is assisted by one Assistant Planning Officer (with oneyear of training, iiniversity of icnigan, equivalent to M.S. degree), andtwo Pesearch Assistants having formal training in evaluation-related subjectmatters (6 months of training at TJS Census Bureau). There is one researchassistant with some local training in statistics. The others have been trainedon the Job to code and tabulate data and to do simple calculations. A coupleof these have had short-term training in key-punching and sorter operationsat the local IBM Office. The Division relies exclusively Of1 computer facilitieswhich are operated by the Department of Statistics and which are quite heavilyutilized by the Department itself.

- 45 -
'!FPE. F7A uati-on Ac-tivities-
7 .04 Mo4r fnocus of he- NTT7PF t- A<t- h, han aTn
AJl 4 ~ An* F- - 4- _.,-n t-it _f nfni . .__ ._.
a.* Analysis of data fro an. input/output efficiency andeffectiveness study by district and/or state conductedin 1071.
b. Mnthl taultation of th_e n.bIer ofacetr in tIheU .lUtLLULLY L.IU .L~ L.LUL Xl LitI I"IUtI C L U -aLCJL)I L .AIL
national program by method and by clinic. Monthly andquarterly reportLs on hILIe acceptors are received rom theclinics by the end of the first or second week followingth'e endu ofL the m,on,th iLn which, acceptanice occurs. Thl'e itemtsare coded at headquarters and sent for key-punching to theDepartument of Statistics by thle endu oLi the Umonth 'U n -whI ich
the records are received from the clinics. Key-punching andtabulation at the Departuriient of Statistics take aDout amonth. The monthly report is then prepared within twoweeks of the return of the tabulations from the Departmentof Statistics. Thus, the monthly report becomes availableusually about two to two-and-a-half months after acceptancerecords are received at the NFPB headquarters. Acceptorsare also tabulated by social and demographic characteristics.
c. Estimation of continuation rates through the missed appoint-ment records and an acceptors' survey (1969). The missedappointment reports which are received from the clinics atthe time the acceptance records are filed and coded; thenthe coded items are key-punched and a tape is prepared foranalysis at the University of Michigan. An effort is beingmade there to determine whether the missed appointmentreport gives reasonable estimates of continuation rates forthose accepting pills at the NFPB clinics.
d. Processing of various evaluation records from the integrationproject study areas and preparation of biannual reports. Theseare required by the NFPB Central Coordinating Committee.
e. Assessment of changes in knowledge, attitude, and contraceptivepractices since the start of the national program through 1970.The post-enumeration survey, (PES), which included questions onknowledge, attitude, and practice (KAP), can be compared withthe Malaysian family survey, which was conducted as a benchmarkbefore the start of the program in 1966-67 to assess the impactof the program.
f. Assessment of the impact of the program on fertility.
g. Target-setting for the national program in terms of the numberof acceptors required for achievement of targets.

- 46 -
h. Evaluation of contraceptive methods.
i. Evaluation of the kampong bidan (traditional midwife) projectsin Perlis and Malacca under supervision of the 11niversity ofMlichigan's Center for Population Planning financed by USAID.The aim of this study is to assess the feasibilitv of bringingMalaysia's traditional midwives in rural communities into thenational pamily planning program to recruit acceptors.
Other Evaluation Activities
7.05 Department of Statistics:
a. Further analysis of the PES/KAP survey is planned incollaboration with the NFPB. A copy of the tape of therelevant data is deposited with the Acting Chief of theEvaluation Division, NFPB, who is responsible for furtheranalvsis from it.
b. Computation of age-specific fertility rates by race andstate based on 1970 census data.
7.06 Center for Population Planning, University of Mfichigan:
a. Further analysis of the 1969 Acceptor Follow-up Survey.
b. Measurement of program impact on fertility through matchingproject-linked identification card numbers from acceptorand birth records.
c. Assessment of continuation rates based on the missed appoint-ment reports for pill acceptors in the NFPB clinics.
d. Preparation of basic tabulation for the compilation ofservice statistics on an annual basis (to be published by theNFPB as a data source for further trend analysis of acceptorcharacteristics. etc.).
e. Further analysis of data from a clinic-level input studyconducted in 1969-70.
E. Limitations of the Existing Evaluation Svstem
Svstem Limitations
7.07 The evaluation activities described above are all useful and relevantfor the 'ational Family Pthenenf , howeeris and mre shd towanrrdiagden t lngthese lines. None of the efforts, hawever, is directed towards identifying

- 47 -
operat ional problemsI andu finding ways to improve specic Coperations. kost:
of the activities undertaken so far are concerned with the impact of theprogrmi on thile clienLtee an' on thLe fertility level of te populatin as whole. If evaluation efforts are to extend beyond the usual impact studies:anu incluude rilonLtorLng of the ongoing program fr ior Lmprovem,ent of prograL,I1management, at least two conditions must be created:
a. Mechanisrn must be developed to bring the program administratorsand tne evaluation orficers routinely together to identiry thepoints in the system where information might be gathered formonitoring operation of the program;
b. The service statistics system should help to identify problemsby producing operationally adequate data for meaningful feedbackto the delivery system (i.e., the clinics).
7.08 Technical Limitations
a. The NFPB is totally dependent on the data processingfacilities of the Department of Statistics for prepara-tion of the monthly and quarterly reports and for tabula-tion of research data and computerized statistical analysis.This means that for some time to come NFPB requests willhave very low priority in that they must compete with the1970 census tabulations that the Department of Statisticsis under pressure to produce. The monthly and quarterlyreports are delayed beyond the usual 2 to 2-1/2 monthsperiod and, therefore, their usefulness is severelv curtailed.Analysis of research data too must be postponed. IJnfortunately,the data processing capabilities in terms of both equipmentand technical skills in the NFPB are very weak and cannot beexpected to meet the needs of the program;
b. The Evaluation Division is short of trained personnel.The Division requires addition of high caliber people whocan be trained in necessary skills.
C. Recommendations for Improving the Evaluation System
Target Setting
7.09 ITp to now, the targets have been set quite independently of theeconomic goals and of the impact of varying rates of population growth onthe economic and social development of the countrv. To a certain extent theEconomic Planning Unit is developing capability to develop models for sucha fuinction The lFu2iFtion UTnit nf the MFPR shoun1d translate the desired

= 48.=
goals of fertility decline in terms of the number of acceptors. These targetacceptors sloulU 'ILten Ue allocated as perfoi.ance guidelines to eac stateand preferably to the health district and checked periodically against theaci-nieveritents andU actua'l i,It-Lpact on fertility rates.
r.valuatiorl Ut PLUroglr .0peraLt ion
7/. I Thne Evaluati'on j lvsiuxsuo j Chief, 'in consultation with Ihe ii'reCLOrand the other Division Chief, should come up with a model that describes theprogram operations identifying the specific points at which data should begathered. The model would necessarily have to reflect any changes that areintroduced in the delivery systemr (such as the introduction of health/familyplanning integration). Then, the entire senior staff (Director and thePivision Chiefs) should meet at least once a month to discuss program pro-gress with particular emphasis on identifying operational problems and defin-ing procedures by which some of the problems might be solved. The evaluationsystem must be flexible and responsive to the needs of the program administrat-ors. Setting up this kind of mechanism for interaction would provide thelink between the evaluation system and the administrators needed to keep theformer flexible and responsive to the latter. For example, the EvaluationUnit has to work very closely with the Ministry of Health to evaluate theprogram as it is being integrated with MCH services. While some of the eva-luation efforts currently undenray are focused on input/output analysis underthe various conditions of the study design, there is basically a lack ofclear-cut criteria to judge whether a given appraisal is effective and/orefficient so that realistic recommendations can ultimately be made with regardto going ahead with one or more of the alternative schemes. The responsibilitymay have to be placed on the Evaluation Chief to develop these criteria andprepare his report in those terms when he meets with the Central CoordinatingCommittee which is charged with directing project operations.
Evaluation of the Program Inputs
7.11 The Evaluation UJnit should be in charge of evaluating all programinputs and should work in close liaison with other units of the NFPB andother organizations engaged in the program to discuss the results for con-tinuous improvement.
a. Training programs can be evaluated in terms of (i) number oftrainees completing the programs; (ii) placement of traineesin appropriate posts; (iii) performance of the placed traineesvis-a-vis family planning service activities; (iv) perceptionof the clientele with respect to the performance of thetrainees in their posts; and (v) cost-effectiveness in termsof expenditures for traininR, man-years of family planningservices rendered, acceptances, and births averted.

- L9 -
b1. Ino.ato/ed4ucatio ipu can be evaluatedl in -erm.s of~' k J. aaL 4CI L. I( ~_UU L.IAJL ±LL ULVLL La V .LUa U L L I~U
(i) type of information/education input per month translatedJILU ::iiUHtf WtIKILt:!U IIIUa5ULtb UI et4U1Vd-LLIL klIdL-11UUL b, dIllU
(ii) cost-effectiveness in terms of expenditures for con-UuctiLng the actiLvities, mIan-ihLours Ue-voteU to the activities,
acceptances, and births averted.
Improvements in Service Statistics System
7.12 First of all, for supply purposes the client intake record shouldindiccate tne date or next appointment made by the client and then filed accord-ing to the next due date.
7.13 Ideallv, a month after the appointment date, an effort should bemade to follow up everv ciient who has missed an appointment to make furthermotivational input. This is not possible in the Malaysian program unless ahome-visiting svstem is made an integral part of the program both in urbanand rural areas. At present, a reminder is sent by mail but the responsehas been virtually nil.
7.14 Copies of the intake records and the missed appointment reportsshould be sent to the NFPB headquarters and filed there as at present. Animproved copying system should be incorporated, however. Copying currentlyis done in most places by hand by the family planning workers.
7.15 The monthly report should list not only the number of apparentlynew acceptors for each clinic, hut also the number of "active users" definedas those whose appointments are not due in the month and/or those who havemissed their appointments (one month beyond the date of appointment), plusthose who did return for additional supplies on or within the one-month periodshould be reported.
7.16 The highest and lowest proportions of those returning for supplieswithin the one-month period of their appointment date should be reported forthe country as a whole, for the state, and for the district; and the per-centile or rank position of the state, the districts and the clinics shouldbe given. These figures will allow the identification of problem areas muchmore systematically than at present.
7.17 The report showing the analysis should be discussed with the Directorand the Division Chief of the NFPB at the monthly meetings and an effort shouldbe made to identify problem areas and explain the cause of these problems.
7.18 The regional medical officers, information officers, and clinicsshould be alerted to the problem areas and directed to ascertain the natureand possible causes of the problems and make whatever input is deemed neces-sary to improve the situation. Their diagnosis and suggestions for improve-ment should be reported back to headquarters. There should be a follow-upon the added effort even though the changes will be detected through thesubsequent monthly output in acceptance and "active users."
- 50 -
7.19 Eventually a system (possibly computerized) might be developed tocross-check all the intake record files to identify transfer cases (thosewho show up at another clinic without notifying the original place of accep-tance and thus without generating a "transfer record"j. Such a cross-checkwill improve the missed appointment record system as a quick means to esti-mate the continuation rates for pill acceptors.
7.20 At each visit, the client record should be updated for any changein status including changes in name, address, living children, fetal loss,etc. Such changes should be reported to the NFPB through a change-of-statusreporting system so that the central file can routinely be updated. Again,the ideal procedure would be to aim for computerization of the system.
7.21 These modifications are not meant to discontinue the current systemof reporting the cumulative numbers of acceptors by various social and demo-graphic characteristics. The system should continue to generate data use-ful for impact analysis and to improve the operation by helping the adminis-trators identify problem areas fairly quickly.
Additional Facilities Needed
7.22 To strengthen the evaluation activities at the state level:
a. A clerical person should be added to the staff of each mainhealth center to relieve the family planning workers fromhaving to engage in data tabulation, etc. Data tabulationprocedures at the local level must be kept simple to assuremaximum reliability when used by these clerks.
b. The summary reports that are currently being prepared bythe clinics on a monthly basis should be sent to familyplanning administrators at the state level with copiessimultaneously forwarded to NFPB headquarters.
7.23 To facilitate data processing and feedback of relevant information.a small computer for installation at the NFPB is recommended. Greater dataprocessing capability at the NFPB becomes imperative if the above recoummenda-tions that evaluation activities be made more responsive to program needs areaccepted. This would. of course, entail the additional need to hire ortrain persons to effectively utilize the computer.
- 51 -
VIII. POPULATION RESEARCHI FACILITIES
A. The Need for Population Studies Capabilities in Malaysia
b.U1Q For a country that officially recognizes the role of population.growth in economic development, the paucity of research and research capabi-lities dealing with the population phenomenon is striking. What researchthere is has been undertaken primarily by outside investigators with onlytoken collaboration, if at all, with local researchers. Where there have beencollaborators, the latter for the most part were junior partners and/or pro-viders of facilities, manpower, or data. It is high time that some systematiceffort be made to develop internal capabilities for independent populationresearch with emphasis on operational aspects that may help in improvingtezhniques of program evaluation and continuous program developments.
8.02 The Department of Statistics takes the census and undertakes surveysthat often include items of demographic relevance, but no independent studiesbased on data that are collected by the Department have been made. TheNational Family Planning Board has a capable evaluation officer but againhe alone cannot take care of the immense work that needs to be done. Heshould, of course, concentrate his effort on current evaluation activitiesanyway. None of the universities have any faculty members whose concern inteaching and research can be identified as being in population even whenbroadly7 defined. This means that there is at present no agency outside theNFPD that can undertake any major evaluation of the National Family PlanningProgram apart from the routine evaluation activities within the NFPB thatare necessary to guide its operations. What is more, the lack of teachingand research capabilities at the universities means that Malaysia willcontinue to be incapable of producing any specialists in this area.
cuggested Research Topics
8.03 Nunerous research topics require attention. The following listincludes only a few suggestions:
a. Analysis of the interrelationship between the inputsbeing made by the national family planning program andthe diffusion of knowledge and practice of family planningamong different sections of society. How much changeis there and how much of the chanee is due to secular forcesand how much to program input? How much impact does thenational nrogram have on the fertility of the peonle itis trying to reach?
b. Analysis of the interrelationship between the efforts ini-formation dissamination and education pertaining to
population and/or family planning and popular responsesboth Lii i n thiu'e short=ru an.d in the long-rur..

c. Analysis of the mechanisms by which findings frompopulation research of the sort listed above aretranslated into policy alternatives and operationalprocedures and effectively fed back into the decision-making system of the Government and variousagencies concerned with these matters.
d. Analysis and developmernt of evaluation techniques forall program inputs, continuous baseline surveys, andstudies.
e. Analysis of the interrelationship between the social,political, and economic goals of Malaysia and the goalsof the national family planning program, with specialfocus on the implications pertaining to target-settingfor the program. One of the important questions requiringinvestigation is: How adequate is the target of thenational family planning program for Malaysia's economicdevelopmental goals, and what are the implications ofvarious targets on the economic developmental goals?
f. Systematic analysis of the vital statistics (birth anddeath data), including an objective assessment of theirreliability, the ethnic group by residence, etc., develop-ment of life tables. and proiections of population growth.
g. Analysis of the interrelationship between differentialpopulation growth and socio-political forces in theMalavyian snoiety.
h. Analys4s nf thp interrelt4inship between populatiorgrowth, age composition, school population, laborforce, emploYment, and economic developm.ent.
i. A,-.lyi,vi of sociali economicr,icutu,ral, an poiArl4tlcal.o
factors affecting fertility and mortality in Malaysia.
4. Systematic analysis of the census data to determine them--- rr1 -nrQ-4nI a or-I i t ,, 4In t-ha c1nr h-cteG_4. t c 0 4_
the ialaysian population (number, age-sex comiposit'on, racialcomposition, residential distribution, educational coILUposi-tiont, income distribution, occupational compositfon, laborfoar._e _OmIPOSitiun, etc.. Thue 1970- census art' the post-LJL WIp L.W_ J. Li : I 2 v 1U C1LU -LE pO t
enumeration survey recertly completed and currenUty undertabJuation should be a particularly rLichi source for detailedanalysis of the population situation in Malaysia today.
k. Analysis of the internal migration patterns (includingurbanization) and their implications for developmental plansin the areas of industrialization, rural and agriculturaldevelopment, urban development, employment, etc.

- 53 -
B. Existing Facilities
8.04 Tne following research activities have been planned and/or under-taken:
a. The Ford Foundation has been trying in recent years togenerate interest in population studies among universitypeople -- at the University of Malaya in particular.
b. The Department of Statistics has a UNDP-funded program toimprove their data-gathering and analytical capabilitiesover the next 5 years or so with the assistance of 9specialist/advisers and 20 overseas fellowships for theirtechnical staff. The Chief Statistician has also invitedoutside assistance to undertake analytical studies of the1970 census returns. So far he has had moderate to enthu-siastic responses from the University of Penang, theUniversity of Michigan, and the University of Chicago.
c. The Economic Planning Unit, under its Output and EmploymentDivision, is planning to undertake some research on theinteraction of demographic and economic variables. Dr. L.Saunders of the Ford Foundation has been advising them onthis aspect. The Head of the Unit, who is a competentresearcher, has plans to have an elaborate model on alterna-tive patterns of economic growth with different assumptionsof population increase. But, so far no systematic planninghas been made of the type of studies to be undertaken by thisUnit which may be helpful in laying down the relevant targetsof fertilitv decline. If the family nlannine Droeram is tosucceed in Malaysia the administrators must realize theimplications of DoDulation growth for economic development.In providing such education, as well as in giving the requiredtarget-s to t-hp N_FFPB; t-his UTnit will nlav a crurcial rnle.
d. The NFPB's Evaluation Unit of the Denartment of Statistics haveconducted various surveys with technical assistance from thellnivpr.citv of MichiGan inclluding a nost-eniumration surveVy
There are, however, no research facilities in terms of manpower,eqitinment Or rpnonsihilitv-
C. Recommendations
A8.0 TlkxxThe T,iu-raitu nf Malnyn has reuest-ed t-he TThFPA t-n nrnuvide edvicnryservices, fellowships and material support to develop a population studiesprogram in the Faculty of Economics a.d AAm4in 4etratin at the Urniversity ofMalaya. The primary concern of the program is to ensure continuity in teach-i.ng anA. research ir. thepplto f4eld with a long-term v ofe

- 54 -
establishing a broader-based population center. First priority will be givento strengthening the undergraduate teaching program in demography as demo-graphic research is supposed to be an important component of the program. Itis stated that: starting from the first year of the program emphasis wouldbe Dlaced on research studies which have practical relevance to problems ofeconomic and social development. The long-range plan for expanded programswill incluide collaboration with anDroDriate agencies and organizations out-side the University in areas of population research and information consideredmiitiuallv henefirial. Although the TJniversitv's research studies program hasnot been elaborated as yet, it seems that the concentration will be more onteachina AnA on general sQf-ijesf of populat4in growth=
8.06 The Census office and University of Mnlaau and the EPTJ may cover
some of the studies enumerated earlier. But other research studies of amore operational nature, particularly the first four listed in para 8.03,should be conducted by a Population Research Unit to be set up separatelyat the NPB. Th..e main function of the Research Ur.it should be to developthe internal capability of the NFPB to undertake baseline surveys and studiesfor evaluation of all program inputs and to develop methodology The Unitwould, of course, have to work closely with the Evaluation Unit because insome stud4es the line 14 o f Admn,ti4" wu nlA d, we , -ut unclear.
Personr.el and Fciliti -Required for the NFPB Resea-rch Unit
8. 07 rhe 7NFPBJ woulA require:a. A qualified serior specialist 4. population studies for a
Im 'j~L.LL J.L U OC1. L J. L.L&.F .~ .LJl L~tO AU
period of 3 man-years to establish the Unit and enhanceresearch1 IHLntrsLs~ aniU capabilitie at the
b. One junior specialist to ass'st the senior rLsULr for atleast 2 years. This junior person will work closely withthe senior specialists in identifying topics for study anddesigning and implementing them. He should be a demographer,a specialists in fertility studies with competence in surveyresearch techniques.
8.08 Meanwhile, one senior social scientist would have to be sent abroadfor a Ph.D. in demography. As this academic training represents about a3-year investment, the person selected should eventually take over the roleof senior consultant.
8.09 Three junior social scientists should be sent abroad for one-yearMA programs in population studies: one in social demography, another ineconomic demography, and another in family planning communication. Thesefellowships can be obtained from the Population Council or other similarorganizations.

8.10 Funds for reference collection, whose items might be selected bythe consultants together with the local faculty, should be provided.
8.11 The Research Unit should utilize the computer facilities to beprovided at the NFPB.

- 56 -
IX. FINANCES
Family Planning Budget
9.01 Budget allocation approved by the Treasury for operating expensesamounted to M$ 2,100,000 in 1972. This amount was short of the request madeby the Board in order to carry out program implementation for the year. Asupplementary allocation was made later in the year providing a total amountof M$ 2,300,000 for the whole year. This amount was only sufficient to meetthe needs for payment of salaries and other recurrent expenditures during theyear resulting in the slow down on recruitment of personnel. For the firsttime, in 1972 the MIOH made provision of M$ 70,415 for the family planningprogram in budget. For 1973 the budget was M$ 2,692,701. The allocations ofthe NFPB budgets are given in the following table:
Program 1972 1973
Technical and Planning 37 48Administration, Finance, and Supply 518 646Service 1,173 1,315Training and Education 76 197Research, Evaluation, and Planning 80 100Information and Publication 216 387All Programs 2,100 2,693
Foreign Assistance
9.02 The amount of foreign assistance received by the NFPB during 1968-70has been US$ 1,142,745. The Ford Foundation approved an initial grant in1966 of US$ 189.000 to the University of Michigan to provide advisoryassistance and material to the Government of Malaysia. An additional grantof USS124.000 was approved to cover until 1970. The assistance was furtherextended to the end of 1971. The Swedish International Development Association(STDA) has supplied t-he NFPR wlth I millinn cyvles nf nral nillqs as wall as
vehicles, equipment and material required in the training and informationprogram. In 1969, TNICEF nllocated "S$1?,500 for trainin. of tradtionalmidwives.
9.03 In 1973, the Government signed two agreements, one with the InternationalBank for Reconstruction -and DevelA op4.ent* ahon-Fund for Population Activities for support of a project to strengthen thenatior.al family p.Lannng program. * The tL o t aL proJect cost estimated at
US$14.5 million is to be financed as follows:
1/ DIBRu Appraisal of' a PopuLat'or, Project, Malaysia, LICUe...L 1, 1972.

M$ .......... millions . US$..... US$Local Foreign Total Local Foreign Total %
Bank loan - 12.69 12.69 - 4.50 4.50 33.14UNFPA 5.80 6.81 12.61 2.07 2.41 4.48 32.92GOM 13.00 - 13.00 4.60 - 4.60 33.94Total 18.80 19.50 38.30 6.67 6.91 13.58 100.00


8+Jrc;9Ts UOtxSYLtt 9.Th eqeP £L-TL6T-n•tTIA:1 /TY n nAnjodPLT n'Trn I9 A-) rT_ JOT vitlar
'OS *d g5Z-IL61TteTrT TTSe FA-|TT puOnnC C1T e Te TTT.T TA nT1IffTrnAArl
'e *d 'TL61 jaqo,oo pUB TFlJidV ' sSS4% I ____
.,% r -r n -Bone -rn AT7nl§T TVrQr v-c iw =T W,Tn n nM 4TZ9 A (In vl-TA lIfY-TCC~T C1 JTW TA WireM-9-0,AAf C .. L-
-Y n-~~~7 C1Lzr Z-
5JU 7 u ZCS r9. -£L
S- Z9-~ Z 656 ZL6T*, U W H Q O,tO LJ,O L
Z9Z16 OL619-Z 9 6106 6961
6-z 6,z ~~~~~69L9 996T6-z L Z 6 -961
Zoe V t 996_6- Z 6- Z 6609 596TL Z 1- tr (L L8L '1961LZ£ 0.~ £119L £961tr c I*T LLF L Z961
£ £ t-t Lt 1L 1961T'e £ 1 f6069 0961
Tc £ tc 9699 65615 C Z*? 66tT9 95618- g 5' t 6LZ9 L561
91 906' L?610. f _ 8L£ 1f6T
_ _ 6ffZ 1161
uO&o|tiid (%) 48~eJioU ( spuBSnotr) waJo tnAO.xp jTo fV-fl4x JO uoTIwndodaTH TenTuuy ase- jenuuy
T JO T advd
T'XglNN
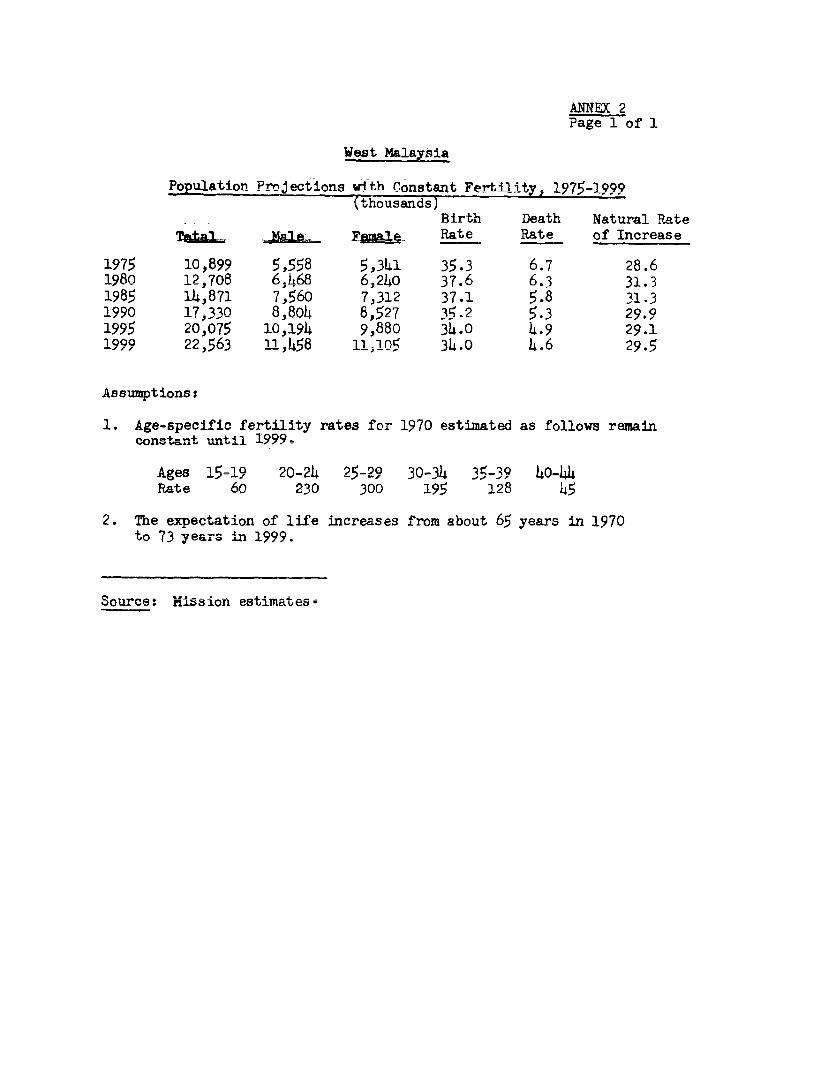
ANNEX 2Page 1 of 1
West Malaysia
Population Projfctionn with Constant Fertility - 1975-1999(thousands)
Birth Death Natural Rate
TaUl. 1A6l9 E@&I-e Rate Rate of Increase
1975 10,899 5,558 5,341 35.3 6.7 28.61980 12j708 6;468 6,24O 3?.6 6.3 31.31985 14,871 7,560 7,312 37.1 5.8 31.31990 17-330 8I804 8f527 35.2 5.3 29.91995 20,075 10,194 9,880 34.° 4.9 29.11999 22,563 11 ,k51R 11j05 34.0 k.6 29.5
Assumptions:
1. Age-specific fertility rates for 1970 estimated as follows remainconst.ant unil 1999,.
Rate 60 230 300 195 128 45
2. The expectation of life increases from about 65 years in 1970to 73 years in 1999 .
Source: Mission estiImatese

ANNEX 3De 1 of :1
,est Malaysia
Area, Population and Density by States, 1970
Percentage ofArea in Population :Ln
States Square Miles Population Density Different States
1957 L970
Johor 7,360 1,330,426 181 14.8 1L4.5Kedah 3,660 995,291 272 11.7 :L0.8Kelantan 5,780 715,253 124 8.1 7.8Malacca 640 421,440 659 4.6 4.6Negri Sembilan 2,590 502,240 194 5.8 5.5Pahang 13,920 526,107 38 5.0 5.7Penang 390 807,987 2,072 9.1 8.8Perak 7,980 1,635,255 205 19.5 17.8Perlis 310 125,791 406 1.4 1.4Selaiigor 3j160 1;699;527 538 16.1 1L8.5Trengganu 5,050 422,357 84 4.4 4.6
West Malaysia 50,840 9,181,674 181 100 1(0Fst. Malavsia 77;640 1.632,635 21 -
Tontl MnIaysr.ia 128)4R80 10,814309 8i -
SLrcesa: pDnraila Fnrwn wrmol4ner r,.nnQiC nf, MnInv.cti; 1Q70_
1957 Cansus of Population.
Note: 1970 Census Population adjusted for the b>

ANNE 4n. -- -I ,a 1-
W~~~~~~~~~~~~~~~~~L. ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
vi D.Ui~J. rvpu±.I --i UI--A 4- 'L~ n±7nL
PercentPage ofUrEJd.LI nurdJ. UV ILLU.
State Population Population
johor 9oi 73.7
Kedah 870 87.4
Kelantan 607 84.8
Malacca 317 75.1
Negri Senbilan 395 78.6
Pahang 426 81.0
Penang 396 49.0
Perak 1184 72.4
Perlis 126 100.0
Selangor 935 55.0
Trengganu 308 73.0
Total 6543 71.3
Source: The Urban population is derived from the percentage ofurban population given in the Field Count Summary, Populationand Housing Census of Malaysia, 1970.

ANNEX 5Page 1 of 1
West Malaysia
Distribution of Ponpulation by Ethnic Groupan and Rural Areas. 1957, 1967 and 1970
Ethnic Percentage Total Urban-Rural Percentage (1957)Group_ 1957 1970 Urban Rural Tot;Tl
Malay 49.7 .53j4 17.6 82.4 100.0
Chinese 37.2 35.4 51.8 48.2 100.0
Indian 11.3 10.6 35.1 64.9 100.0
Other 1.8 o.6 44.1 55.9 100.0
Total 100.0 100.0 32.3 67.7 100.0
Sources: Census and Lim Lin-Lean - Some Aspects of Income Differentials inWest Malaysia, Kuala Lunmpur, September 1971'-

ANNEX 6Page 1 of I
West Malaysia
Age Structure of Population. 1957-1969(thousands)
_ _~~~~1957- 1969 ~to_
ARo Persons Males Females Zot&l Persons Males Females to Total
Under 5 1,196 607 589 19.0 1,406 716 690 15.6
5-9 945 481 464 15.0' 1,323 671 652 14.7
10-14 671 348 323 10.7 1,177 599 578 13.0
15-19 603 303 300 9.6 991 504 h87 11.0
20-24 514 254 260 8.2 721 370 351 8.0
25-29 435 213 222 6.9 619 312 307 6.9
30-34 367 185 182 5.8 516 251 265 5.7
35-39 335 17l 164 5.3 -39 209 230 b 9
40-44 2_9 15_ 13h h.6 363 176 187 4e.O
45-49 268 150 118 4t -3 334 167 167 3.7
5° -5 220 127 93 3-5 290 152 138 3_2
55-59~Q 162 97 65 2.6 285 152 133 3.2
60-614 13 64 1. 1.a o1r 90 2.3Ac~~~Ao l.~~~ -i ') ~~~~ RA
65-69 174. 41f s1271 66 .(44-. .'.J.7 Le.
- -~~~~~~~~~~~~~ 70 ar.d over_ 9 6 5 .'LI -101 9 .
Total 6,289 3,242 3,047 100.0 9,019 4,585 4,,434 100.0
sources: Government of Malaysia. Department of Statistics, Vital Statietics,West Malaysia, 1969. Tan Boo Ann, NFPB, General Consequencesand Implication of Rapid West Malayrsia,Population Gn,wth.

ANNEX 7Page- 1 of 1
r erti'i'ty Rates , lz957- I 2
Year Birth Rate Total Fertility Fertility Rate
1957 46.2 6.7 229
1958 43.3 6.1 _
1959 42.2 6.1 -
1960 40.9 6.1 -
1961 41.9 6.2 -
1962 40.4 5.9 -
1963 39.4 5.9
1964 39.1 6.0 -
1965 36.7 5.5 -
1966 37.3 5.2 -
1967 35.3 5.2 _
1968 35.2 _ _
1969 33.0 4.8 163
1970 32.2 - 157
1971 32.6 158
1972 32.0
Sourcest Government of Malavsia. Department of Statistics. VitalStatistics, West Malaysia, 1969 and October 1971General Fertility Rates are NFPB estimates.Data for 1971 and 1972 are mission estimates.

ANNEX 8Poe f 1.
West MalayBia
Age-Specific Fertility Rates, 1957-69
Year Percentage Change
Age Group 1957 1962 2 1969 1957-1962 1962-1967 1957-1967 1967-1969
15 - 19 123 103 71 59 - 16 - 31 - 42 - 21
20 - 24 329 277 231 238 - i6 - 17 - 30 + 3
25 -29 314 333 289 257 _ 4 - 13 - 17 - 12
30 - 314 272 237 221 23 -13 - 7 - 9 + 6
35 - 39 182 154 166 133 - 15 + 8 - 9 - 25
40 - 44 79 68 68 58 - 14 0 - 17
To t '. Il LDJ.rt it -U
Rate 6,660 5,860 5,230 4,900 - 12 -11 -21 - 6
Sources: "Estimates of Fertility for West Malaysia (1957-67)," June 1969.kuuver.Sm=u.t of ry. La , parUWU.J of SaiL-t4oLcs, Vtal vt&tlst.cs,
West Malaysia, 1969 and October 1971.

ANNEX 9PIage l Of l
West Malaysia
Percentage Of Women Currently Married by Age19572 1962 and 1967 _
Percentage Change inPercent Married Percent Married
Age of Women 1957 1962 1967 1957-62 1962-67 1957-67
15-19 34.7 26.3 17.9 - 24 - 32 - 49
20-24 74.7 67.0 59.3 - 10 - 12 - 21
25-29 89.6 87.2 84.8 - 3 - 3 - 5
30-34 90.9 91.0 91.2 + 0 + 0 + 0
35-39 87.6 88.6 89.6 + 1 + 1 + 2
40-44 80.6 83.0 85.4 + 3 + 3 + 6
Source: R. Chander,Fam!U ?lamin Fertility Trends in WestMala2y-sia,i L)ena-q-rtm-e-nt- of Statistinns Gonvernment of KA-lay-si

ANNEX 10oage 1 1
rWest riav-L"Ls'L UcL-4 - Lt.J....I I .la
iaaua±-u vruai
Age-Specific Fertility Rates andl& tv....&aJ r jit.. -Re n-- - 9at an l /
IPb± tWbL±b~ V-LU~ 1 yoc 8110 1iD(
er cu a'Ltage fuafngeAges 1962 1967 1962-67
IN-4- n 4.-
,r1uLv- PO 6LIU
AreasIr' In I L I I 0I_-1 44 44020-24 245 195 - 2025-29 271 210 - 2330-35 204 196 - 43-5-39 140 113 - 2440-44 72 36 - 50
TFR 4,920 3,970 - 19
ur*utln Areas
43 - 4920-24 290 141 - 5125-29 376 259 - 3130-34 243 196 - 1935-39 121 125 + 340-44 77 49 - 36
TFR 5_5960 4,065 - - 32
Rural Areas
15-19 123 82 - 3320-24 286 253 - 1225-29 344 314 - 930-34 243 230 -535-39 159 183 + 1540-44 66 77 + 17
TFP 65105 5,695 - 7
l- "Hetropolitan Areas" include towns having a nnnulation of moethan 75,000 in the 1957 Census and the State Capitals;'Urban Areas" are nlace-s with pnpulation of 7,670-75,00nin the 1957 Census, and "Rural Areas" are all others.
Source: "Estimates of Fertility for West Malaysia (1957-67)'," June 1969.Government of Malaysia, Departmet of Statistics, Vital Statistics,West Malaysia, 1969 and October 1971.

ANNEX 11Pare 1 of 1
West Malaysia
Age-Specific
Fertilitv Rates bv Ethic Group
Percentage Change1957 1962 1967 1969 1957-62 J962-67 1557-67 1267-69
Malay
15-19 163 144 97 80 - 12 - 33 - 40 - 1820-24 342 287 260 262 - 16 - 9 - 24 + 125-29 279 306 296 242 + 10 - 3 + 6 - 1830-34 208 219 224 261 + 5 + 2 + 8 + 1435-39 146 153 170 134 + 5 + 11 + 16 - 2140-44 55 51 81 60 - 7 + 59 + 47 - 26
TFR 5,967 5,800 5,640 5,195 - 3 - 3 - 5 - 8
Chinese
1'-19 38 37 25 24 - 3 - 32 - 34 - 420-24 280 245 177 181 - 13 - 28 - 37 + 225-29 1h12 378 288 270 - 8 - 2h - 30 - 630-34 355 268 228 209 - 25 - 15 - 36 - 835-39 235 1fl9 *I53 130 - 29 - 9 - 36 - 1540-44 117 111 51 61 - 5 -54 - 56 + 16
TFR 7,209 6,040 4,610 4,375 - 16 - 24 - 36 - 5
Indian
15-19 209 126 100 69 - 40 - 21 - 52 - 3120-2I 4 1429 361 270 307 - 1I - 25 - 37 + 1225-29 441 353 250 259 - 20 - 29 - 43 + 330-31423 23 9 20nn 198 - 21 - 10 - 29 - 1
35-39 159 128 193 124 - 19 + 51 + 21 - 3640-1414 60 38 53 37 -37 +39 -12 -30
Ts 7 a Al. A 7)c0C 61 5 ,330 le70 - 22 -0- 33
-JJ4. it, ~ l IL . Lfla.I. . 4 1y '- LCtSL1 AA4f 4 4. ' - . 4 * P
Soures R. Chade Fa-..m Iy Pan -ng andq Frnt;li+y Trendsq i *.n Wes
Malaysia, Government of Malaysia, Department of Statistics,Pape.r 6. Goveiirnment of Yialaysia, DRpartmint Of StttCs,Vital Statistics, West Malaysia, 1969 and October 1971.

ANNEX 12Page 1 of 1
West Malaysia
Live Birth Order by Ethnic Group, 1969
AllLive Birth Indian and Ethnic
Order MalaY Chinese Pakistani Others Groups
1st 18.8 21.5 18.7 31.7 19.8
2nd 17.5 18.1 16.3 27.0 17.8
3rd 2.5.1 15.3 14.3 16.0 15.1
4th 13.0 11.7 11.6 9.3 12.4
5th 10.9 9.1 9.9 5.7 10 1
6th + 24.7 2h.2 29.2 10.3 24.8
Total 100.0 99.9 100.0 100.0 100.0
Source: Government of Malaysia, Department of Statistics, Vital+asi tC8sU West w-7now40 I O A nc+VYber 1071.

West Malaysia
Socio-Economic Variable and Fertility by States(1969)
Crude Birth Rate by Ethnic Compos ition (7 .Crude Birth Percentage Decline Ethnic Group Indian Percent of Per
Rate in Crude Birth Rate Indiarn & Pakistani Population - MortalitL CapitaStates 1958 1968 1969 1958-68 1968-69 1958-69 Malay Chinese Pakistani Malay Chinese Other Rural Maternal Infant Income
(1968 M$)Johor 47.0 34.0 32.5 27.7 4.4 30.8 36,5 29.6 28.7 50.1 40.2 9.7 73.7 1.39 39.7 766Kedah 34.2 36.3 32.5 6.1 10.5 4.9 35.1 26.9 29.2 68.1 20.0 11.9 87.4 2.08 51.1 656Kelantan 44.2 36.7 35.8 17.0 2.5 19.0 36.9 25.7 23.1 91.6 5.5 2.9 84.8 2.74 51.8 420Malacca 48.5 34.8 32.9 28.2 5.5 28.4 34.8 2'9.8 34.2 50.7 39.2 10.1 75.1 0.63 47.0 580Negri Sembilan 48.0 32.6 31.6 32.1 3.1 32.0 33.6 29.7 34.4 42.6 39.9 17.5 78.6 0.82 42.2 934Pahang 41.8 39.1 37.3 6.5 4.6 10.7 40.9 32.1 38.9 57.3 3/..1 8.6 81.0 2.25 43.7 1,091Penang 40.2 31.0 29.1 22.9 6.1 27.6 30.3 27.8 31.3 29.0 56.9 14.1 49.0 0.66 36.9 777Perak 44.0 34.5 31.8 21.6 7.8 27.7 36.1 29.2 30.2 40.5 43.4 16.1 72.4 1.90 44,8 834Pierlis 38.7 31.9 30.2 17.6 5.3 21.9 30.1 29.7 42.0 77.1 17.9 5.0 100.0 1.61 44.3 555Selangor 43.2 36.4 34.2 15.7 6.0 20.8 40.9 32.5 31.4 30.2 47.2 22.6 55.0 1.07 33.6 1,537Trengganu 47.8 41.5 38.1 13.2 8.2 20.2 39.5 19.6 30.0 92.6 5.9 1.5 73.0 1.96 55.0 580West Malaysia 43.3 35.2 33.0 18.7 6.2 23.7 36.5 29.7 31.2 50.3 36.9 12.8 71.3 1.57 43.2 874
Scources: Government of Malaysia, Oepartment of Statistics, Vital Statistics, West Malaysia, 1968 and 1969.Rural Population, Field Count Summary 1971) Census.NFPB Bulletin, January/February 1972Lim Uhe Lean, jme Ag ;ects of T im nifftrpntalj tn j, lt. . aa Kuala Lumpur, September 1971.
dLeM
t b

ANNEX I L'agsi1T 1
West malaYsia
Mo rtality Rates, 1951- 72
Year Infant Mortality Toddler Mortalty Death Rate
1951 97 - 15.1l1952 90 - 13.81953 83 - 12.61954 83 - 12.l1955 78 _ 11.7
1956 75 - 11.61957 76 11 12.1958 80 9 11.01959 66 8 9.71960 69 8 9.5
1961 60 8 9.21962 60 8 9.t1963 57 7 9.0196U 48 6 8.11965 50 6 7.9
1966 48 5 7.61967 hU 5 7.51968 42 5 7.619iQ9 )"3 5 7.21970 6.9I Q71 6 8
1972 6.8
Source=: Governrnent of MalaysAi DeparLtwat of Statistics, Vital Statistics,West Nalaysia, 1969. Mlni-trv af salthL. -A1-t'h in Malaviain 1971.
19-(U72 - NrPB estimates.

ANN EX 15
Page 1 of 1
West Malaysia
Mortality Rates by Ethnic Group v 1969
Ethnic Infant Neonatal ToddlerGroup eTath Rate Hortali+vy Mortalit .-.rt-t1+
All 7.2 -4 _2 _23. L4 .4.9 02
MMaIlayr 7.' A 2.A.A 1I.7 61.42J m~~~~~~IL4 ' L-4. I '.J L4L
C; n ese a6. 4 31.1 2.0 2.4
~~~ D ~~~~~ A~% r'0 A. o'- % o r' tL
J. dA. u & Pais-Li U. d.52.D4 279 .3
O >hier 3.3 , 2 1
Source: Government of Malaysia, Department of Statistics, VitalStatistics, West Malaysia, 1969.

ANNEX 16Page 1 of 1
Mest Malaysia
Targets and Achievements of Family Planning Program(1967 - 1975)
Acceptors asPercentage of
No. of Women No. of Acceptors Married Women Percentage ofYear Marield( 4 Actual Target Actual Target Achievement(2 to 3)
()2) (37 7h) (5) (6) '"
1967-70 1,320,582 222,217 343,351 17.0 26.0 64.8
1971 442,570 54,769 80,000 4.5 5.4 68.5
1972 1,491,363 56,417 100,000 3.8 6.7 56.4
1973 1,548,108 38,443* 120,000 - 7.8 -
1974 1,604,852 - 140.,000 - 8.7 -
1975 1,661,597 - 160,000 - 9.6
* Up to August 1973.
Sources: NFPB. Annual Report. 1970.Government of Malaysia, Plan of Action of Family Planning
Program 1973-75.

West MaLasiLa
Regional Differentials in Ac eptability
Total.Acceptors Eligib:Le
Crude as Porcerit Womaen Etlhnic Conrposi'tion(%)BiLrth of Eligible per NFPB 'ndian Percent of' PeirRate Wiomen Clinic Pakistani Rctral poDf- CELpitP15169 :L967-197() 19i70 Malay Chinese Other Rul Pou CaitaStates Oerlaktionl Irncome)
Johor 32.5 21.4s9 2,732 50.1 40.2 9.7 73.7 766Keidah 32.5 13.36 3 ,250 68.1 20.0 11.9 87.lA 656Kelantan 35'.8 8.554 4,833 91.6 5.5 2.9 84.8E 420MaLlacc:a 32 .9 21.35 1,857 50.7 39.2 10.1 75.1 580Neigri Sembilan 3]L.6 27.81 1,225 42.6 39.9 17.5 78.6 931aPahang 37 .3 16.27 1,,748 57.3 34.1 8.6 81.0CI 1,091Penang 29.1 24.22 2,256 29.0 56.9 14.1 49.Cl 777Peirak 3]L.8 16.55 1,,751 40.5 43.4 16.1 72..4 8314Perlis 30.2 28.12 1.,796 77.1 17.9 5.0 1.00.0C 55'>Selangor 3,,.2 21.94 3,999 30.2 147.2 22.6 55.0 1L,537Trenggaanu 38.1 13.25 2,i486 92.6 5.9 1.5 73 . 580)West Malaysia 3'3.0 18.78 2,390 50.3 36.9 12.8 71.3 87l4
Sources: Government of Malaysia, Department of Statistics, Vital Statistics, West Malaysaia,1968 and 1969. NFPB Bulletine, January/February 1972.Rural Population , Field Co-nt Suimary 197CI Census .Lim Lir L ean, Some Aspects of Incone Differentials in West Malaysia, Kuala Lurpur,Septenber 1971.

ANNEX 18Page 1 of 1
West Malaysia
Acceptors by Agency, May 1967 to August 1973
Inte-NFPB % FPA % Others % !Ixtkxi% Estate % FLDA % Total
1967(May-Dec) 8,247 39.8 10,132 48.9 552 2.7 _ - 1,795 8.6 _ - 20,726
1968(Jan-Dec) h3,058 57.4i 25,158 33.6 4,189 5.6 - - 2,530 3L - - 74,935
I1969(Jan-Dec) 48,140 68.2 16,695 23.7 3,596 5.1 - - 2,14h 3.0 - - 70,575
197G 39,441 70.4 13,995 25.0 1,568 2.8 - - 830 1.5 147 G.3 55,981
1971 36,157 66.o 13,212 24.1 701 1.3 2,963 5.4 642 1.2 1,094! 2.0 54.769
1972 35,015 62.1 12,957 23.0 807 1.4 4,904 8.7 390 0.7 1,347 2.4 56,417
107-41973itug) 24,134 62.7 7,998 20.8 1,691 4.4 3,135 8.2 425 2.5 1,060 2.7 38,443
Total 234,192 63.0 100,144 27.0 13,10h 3.6 11,001 3.0 8,756 2.4 3,648 1.0 371,846
1/ The Service Program of the NFPB started in May 1967.
Sources: NFPB Annual Report, 1972 and Monthly Acceptocrs Report, August 1973.

iWest Mtalaysia
Monthly Aoceptor Rates in Integration Areas, 1972'
-Pl revious , - 1972Clinic Monthly verale Integration Areas Monthly Acceptor Rates 1971 A/and 15972 2/ Month19 7otal
1969 - 70 1971 Jan Fieb Mar Apr May Jun Jul Aug Sept, Oct Nov Dec _ No. Ave.
Alor GaJah 16 54 48 31 40 29 49 60 49 SO 62 59 577Malacce. 45.4s 43.'2 79.0 (88)21(67) (111) (103) (82) (95) (73) (72) (63) (97) (38) (57) (946) 48.1
Penrlis 39..1 40.9 81.0 86 96 94 120 120 75 96 100 69 72 72 70 1,070 89.1(45) - (53) (108) (110) (88) (98) (133) (101) ( 70) (71) (67) (976)
4'Parit Jawa 49 91-' 33 37 28 37 33 26 38 24 32 428Johor 13.4 13.5 49.5 (15) (10) ( 7) ( 8) (119)2110) (83) (71) (4:L) (51) (45) (34) (594) 35.7
Pasir Has 46 44 4L9 33 34 33 40 30 26 143 21 29 428KelantaLn 13. 6 10.9 35.0 - - - - - - (51)2/(68) (56) (60) '(35) (37) (421) 35.7
Negri Sembilan 82 59W 89 82 145: 84 94 102 108 115 82 77 1,119Area 83.4i 59.3 72.0 - _ _ _ _ _ _ _ (91)2(95) (117) (867) 93.3
1/ Figures in parent'heses are 1971 data.2/ Month integration started in 1971.3/j Because of the slow transition from NFPB to integration, these statistics are a combination of NFPB acceptors and 0
integration acceptors.4/ Cornbined for February and March. H
J/ Excludes data for Rembau and Taspin which is being includled irn March data.
Source: National Family Planning Board.

West Malaysia
Number and Proportion of AcceptcErsb Meth 2 dj 196773
]967 % 19 68 A 1969 % 1970 % 1971 X 1972 _ % 1973 _ _%__
Pill 18,541 899.4 69,337 92.5 65,572 92.9 49,564 86.6 47,790 87.3 148,921 86.7 33,442 86.9
IUD 724 3-5 1,173 1.6 1,127 1.6 797 1.4 925 1.7 1,137 2.0 646 1.7
Sterilization 627 3.0 2,609 3.5 2,689 3-8 3,477 6.2 3,979 7.3 3,883 6.9 2,531 6.6
Condom - - 889 1.2 753 1.1 1,470 2.6 1,735 3.2 2,149 3.8 - -
Injectable - _ 562 0.7 260 0.4 4i91 0.9 197 0.3 159 0.3 - -
Others 4 4.o _365 _ 0.2 0-3 _J Ml 0.2 16. 0.3 1.82b k.
Totals 20,726 100.0 74,935 200.0 70,575 1()0.0 55,055 1/ 100.0 54$ 767 100.0 56,417 100.0 38,4h3 100.0
1/ 26 cELses unclassified.
Sources: NFPB Annual Report for 1972 and Monthly Acceptor Report, Augus1 1973.
H

ANNEX 217PagFc1 o1 '
West Malaysia
The Age-Specific Continuation Ratesfor Oral Contraceptive-s 1962
First Serent All SegmentsAges Sa!uplA Size 12 month 1 V., OL9 ,month ld month
i5-19 91 "I. - 2,.L nL .; C. I 27.20-24 495 h6.0 30.7 57.1 44.425-29 600 514.1 L-L.b 68.2 18.830-34 549 59.3 46.6 71.7 39.9
2AR ~~~~-7nI-,L L..e LL35c-39Q 308 57.2 147 67.9 w.l.O -44 121 57.9 52.2 67.9 61.2/45 10 79.3! 4 79.3?- 79.-3? 79.3?!
A IL ua 2 -1 53.8 41.7 66.o 55.5
1/ Hounded f2igure of a weighted sample.2/ Unreliable due to small sample size.
Source: Takeshita J. and Tan Boo Ann ,- Acceptors Survey, NFPB 1969.

Famil]y PlanningLAcce orsbyAge Group, 1967-72
19>67- % 19_68 % 19,9 19 1971 % 31972 _
15-19 935 4.5 3,283 4.4 3,423 4.8 3,115 5.6 3,557 6.5 3,801 6.7
20-24 4h,429 21.4 16,664 22.2 16,770 23.8 1L5,077 26.9 1/5,o54 29.3 17,156 30.4
25-29 6,261 30.2 22,013 29.4 19,703 27.9 1L4,928 26.7 114,173 25.9 15,178 26.9
30-34 5,094 :24.6 18,380 24 .5 17,060 24.2 :12,615 22.5 1L,643 21.3 11,101 19.7
35-39 2,880 :13.9 10,098 13.5 9,43t4 13 .4 6,98:3 12.,5 6,583 12.0 6,564 11.6
,40-44 995 4.6 3,740 5.0 3,4814 14.9 2,68 7 14.13 2,368 14.3 2,253 4.0
45-49 172 0.8 749 1.0 703 1.0 51:1 0.9 388 0.7 364 0.7
:Not reported - _-_ 8 - 8 _ - 39 0.1 1 0.0 -
rotal 20,726 100.0 74,935 100.0 70,575 10(.0 55,9515 100.() 514,767 100.0 56,417 .00.0
1/ May - Decemiber 1967. N
2/ 26 cases urLclassIified.
Source: NFPB Annual Report, 1972.

West MaLaysia
Monthly Income Level of Husbands of Acmtozrs, 1967-72
M[S$ 1967- % 1968 % 1969 ,_ 1970 , 197:L % 1972' %
Under 100 606 8.5' 8,197 11.0 8,060 11.4 6,651 11.9 9,038 16.5 9,731 17.2
100-2599 2,342 32.8 25,020 33.4 23,3L4 33.:L :21,017 37.6, 23,35 1 4 42.6 24,503 43.4
300-1499 280 3.9 2,991 14.0 2,958 4.3 2,900 5.2 3,407 6.2 3,538 6.3
500-699 57 0. 8 528 0.7 513 0.7 498 0.51 63( 1.2 1,070 1.9
700-9599 18 0.3 226 0.3 247 0.3 296 0.5 38:L 0.7 452 0.8
1,000 8 abore 15 0.2 1156 0.2 1514 0.2 203 0.14 339 o.6 362' 0.6
Unapprop. 169 2. 4 1,522 2.0 1,311 1.'3 1,028 1.8 1,0o45 1.9 880 1.6
Nlot Reported 3,647 51.1 36,295 48.14 23t 8 148.:L 23.362 41.7 ]6.573 30.3 1 28.2
I'otal 7,134 100.0 74,935 100.0 70,575 100.0 2/56,41 ]L00 0
1/ November and December figures only.2/ 26 cases unclassified.
Source!: NFPB Ainual Report, 1972.
HIro
F0

West Malaysia
Level of Education of Acceptors, 1967 72
196- 1/ 1968 % 1969 1% 970 _ _ 19171 , 1972 _ _
No Schooling 2,029 28.4 14,658 19.6 16,577 23.5 12,,804 22.9 13,226 214.2 12,571 22.3
Primary 1,886 26.4 22,053 29.L 25,602 36.3 27,230 48.7 28,325 5:L.7 29,6:33 52.5
Seicondary 1,302 18.3 15,620 20.8 13,073 18.5 5,683 10.2 6,625 12.1 7,2133 12.9
Upper Seconclary 9( 1.3 662 0.9 313 0.4 119 0.2 72 (.1 60 0.1
College/Universit;y 16 0.2 74 0.1 112 0.2 131 0.2 115 0.2 1137 0.2
Not Reported 1,81L 25.-! 21,868 29.2 14,898 21.1 9,988 ] 78 6,404 1L.7 6,6;6 11.8
Total 7,134 100.0 74,935 100.0 70,575 100.0 55,955#- 100.0 54,767 100(.0 56,310 100.0
V1 November and December figures only.7/ 26 cases unclassified.
Source: NFl'B Arunual Report, 1972
tIq X (D
O3 r-

ANN EX 25Page 1 of 1
West Malaysia
Cumu1ative Number of Acceptors by Ethnic GroUp v 1967-71
Year Mala % Chinese % Indian % Others % Total
1967 1/ 8,583 41.14 8,895 42.9 3,060 14.7 188 0.9 20,726
1968 33,903 45.2 32,206 42.9 7,885 10.5 941 1.2 774,935
1969 31,691 44.9 30,773 43.6 7,119 10.2 912 1.2 70,575
1970 26,862 47.9 22,921 40.9 5,606 10.0 592 0.9 55,981
1971 2/ 21,037 50.7 16,159 38.9 3,941 9.5 391 0.5 41,52 8
TOtal 122,07A 46-3 11095)l 4i21 27)691 10.5 2,711 1.0 263,7145
_/ MYv - Decelmben r 16Q72/ January September 1971.
Source: NFPB unpublished data.

ANNEX 26Page i of 1
W'est Mialay-sia -
Knowieage Attitude, & Desired No. of unildren 7 and 1970(Respondents Sample of Currently Married Women 15-4 years
West MalaysiaKnowledge of Family Survey PES-KAP
1. Family Planning 1966/67 Surve
Total: %: 100.0 100.0No: (5,457) (17,365)
Yes 44.O 84.5No 57.0 14.2
2. Attitude
Total: %: 100.0 100.0No: (5,457) (17,365)
Approves 70.0 77.9Depends 2.0 4.3Disapproves 21.0 13.2Do not Care 6.0 3.1
3. Desired Number of Children
Total: %: 100.0 100.0No: (5,457) (17,365)
0-2 5.0 8.73-4 31.0 44.75-6 27.0 29.47 and Above 16.0 8.3Do not Care 19.0 7.6
PES - Post-Enumeration Survey.KAP - Knowledge, Attitude and Practice.
1/ Totals may not add up to 100 because of a proportion of nonresponse.
Source: Government of Malaysia, Department of Statistics, Post-Enumeration Survey Report, KAP Section. 1970.

ANNEX 27West. MalayRSi PageZ 1 ofW 1
Use of Family Planning Methods 1966/67 and 1970 -/
(R espondenits Sample of C-rren'Ly IMVriedL fUJI1 LDL4L4 years)
West MalaysiaFamily Survey PES.q-KaP
1. Ever Used 1966/67 Survey 1970
Total: %: 100.0 100.0No: (5,457) (17,365)
Pill No Data 19.8Other Methods No Data 4.7Pill and Other Methods No Data 2.4SubtotEal 14.0 26.9Never 86.o 71.3
2. Current Use
Tntal l: 10 0 100.0No: (5,457) (17,365)
Pill 4.0 11.90ther MPfthAds !j.. 3.9None 91.0 82.4
3. First Use
Total %: 100.0 100.0,'o: f(5,hc5) (I 7,36A
fl eVnva 'I c+ P--r.van Vflrn
after 1st pregnancy 4.0 5.4After 2nd or 3rd p- -. 8.1After 4th or 5th pregnancy 2.0 6.4A4J-a-L U .i-i V, F L C 6.o"L1'A. Ute 6t prg.ac 4I .0 6~L~ .8
Inappropriate (never usedrf-41- pl&u--ig or wh.en
used is unknown 86.o 71.4Not- A-ailale 1.X.
PES - Post-rEnumeration Survey-.
KAP - Knowledge, Attitude and Practice.
1/ Totals may not add up to 100 because of a proportion of nonresponse,
Source: Government of Malsysia, Department of Statistics, Post-EnumerationSurvey Report, KAP Section, 1970.

ANNEX 28Page 1 of 1
-West Malaysi.a
Mean Live Births; Desired Numberof' (1hlre- Proporuion Ever 'U'se Coo .tra 1 I
And Currently Using Contraception-1966/67 & 1970knespondents Sample olf Currently Married women l5-h4 years)
West Malaysia Family SurveyKAP PES-KAP
Wives 15 - 24 Years Old 1966/67 Survev 1970
Mean number of live births 1.9 1.6
Mean number of children wife wants 4.4 4.1
Percent who have ever used contraception 10.0 19.6
Percent who are currently usingcontraception 5.0 11.7
Wives 25 - 34 Years Old
Mean number of live births 4.3 4.1
Mean number of children wife wants 5.3 4.5
Percent who have ever used contraception 16.0 33.0
Percent who are currently usingcontraception 11.0 19.8
Wives 35 - 44 Years Old
Mean number of live births 5.8 6.0
Mean number of children wife wants 5.3 4.5
Percent who have ever used contraception 14.0 25.5
Percent who are currently usingcontraception 9.0 14.4
PES - Post-Enumeration Survey.KAP - Knowledge. Attitude and Practice.
l/ Totals may not add up to 100 because oI a proportion of nonresponse.
Source: Government of Malaysia, Department of Statistics, Post-Enumeration Survey Report, KAP Section, 1970.

ANNEX 29Page 1 of 1
West Malaysia
Mean Live Births, Mean DesiredNumber of Chiidren and Use of Contraceptives in
Metropolitan, Urban and Rural Areas, 1970(Respondents Sample of Currently Married Women 15-L4 years)
Metro-politan - RuralAreas _' Towns Areas
15-24
Mean number of live births 1.4 1.5 1.6Mean number of children wife wants 3.6 4.0 4.1Percent who have ever usedcontraception 35.1 27.7 16.2
Percent who are currently usingcontraception 19.1 16.3 10.1
25-34
Mean number of live births 3.h 3.7 4.4Mean number of children wife wants 3.9 4.3 4.8Percent who have ever usedcontraception 51.3 40.5 27.4
Percent who are currently usingcontraception 32.0 24.9 16.1
35-44
Mean number of live births 5.3 6.o 6.2Mean number of children wife wants 4.3 4.8 5.1Percent who have ever used
contraception 37.2 34.1 21.3Percent who are currently usingcontraception 20.4 19.0 12.2
"Metropolitan Areas" are towns having population of more than 75,000in the 1957 Census, and the State Capitals.
1/ Totals may not add up to 100 because of a proportion of nonresponse.
Source: Government of Malaysia, Department of Statistics, Post-Enumeration Survev Report, KAP Section, 1970.
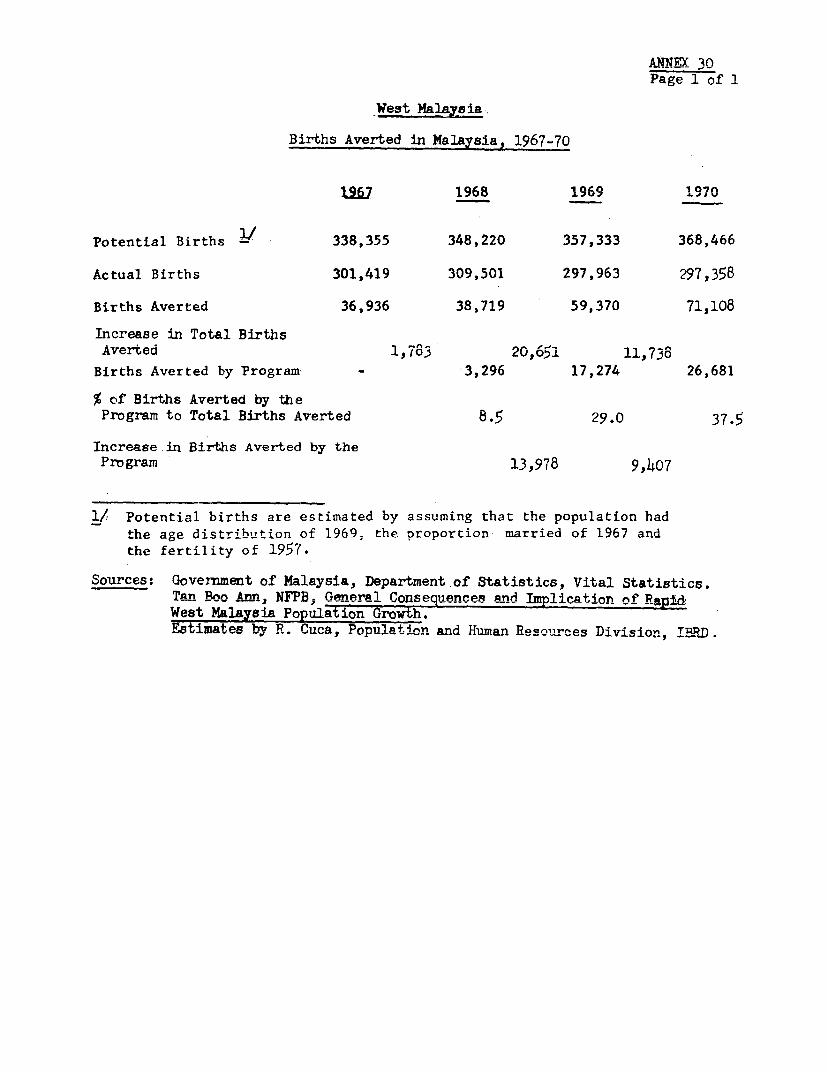
AONNX 30Page 1 of 1
Births Averted in Malaysia, 1967-70
A..R 17UO J
Potential Births 338,355 348,220 357,333 368,466
Actual Births 301,419 309,501 297,963 297,358
Births Averted 36,936 38,719 59,370 71,108
Increase in Total BirthsAverted 1,783 20,651 l,738
Births Averted by Program - 3,296 17,274 26,681
% of Births Averted by theProgram to Total Births Averted 8.5 29.0 37.5
Increase in Births Averted by theProgram 13,978 9,407
1/ Potential births are estimated by assuming that the population hadthe age distribution nf 1969; the proportion married of 1967 and
the fertility of 1957.
Sources: Government of Malaysia, Department of Statistics, Vital Statistics.Tarn Boo Annn N'PRB. RGe1ne Consen ences and Tmrypliration of RApi
West Malay8ia Population Growth.Estimates by R. Cuca, Population and Hinman Resou-ces Division, IERD.

ANNEX 31West Malaysia Page 1 o:f 1
Annual Births Averted According toCharacteristics of Acceptors and Program,
1968-71
Births Averted
1968 1969 1970 1971 Total
Year ofAcceptance 1967 2,756 3,794 1,736 780 9;066
1968 540 12,720 11,480 4,256 28,996
1969 - 752 12,912 8s734 22j398
1970 - - 553 7,093 7,646
3.296 17,266 26,681 20,863 68,106
Agnryv Pro-viding theSeruires NFPB 1,407.43 9.330.54 16,487.62 13,713.66 40,937
FPA 1,529 6,303 7,897 5,650 21,379FLDA )Estates) 360 1,631 2,301 1,503 5,795
Others )
3,296 17,264 26,685 20,866 68,111
Age 15-19 183 907 1,238 863 3,191
20-24 963 4,987 7,056 4,963 17,969
25-29 1,067 5,831 8,680 6,376 21,954
30-34 767 3,842 6,448 5,660 16,717
35-39 273 1,459 2,663 2,418 6,813
40-44 40 233 513 576 1.362
45-49 2 14 42 57 115
3,295 17,273 26,640 20,913 68,121
Method Fill 2,965.90 15,861.92 24,667.92 19,033.91 62,526
Other 331 1,403 2,018 1,833 5,585
Source: Estimates by R. Cuca, Population and Human Resources Division, IBhTj.

AwwwY 3Page 1 of 1
Vme+ Mnl n',y4 9
A ge Of Wo,e eOC+ i4-- *gXr^cpion
Within and Without the Program, April 1965 - March 1969
Womter-, Practicing Corttr-Lce-pt'on
Age tv.LuluWik rrogram W.ithOUt Program L
15-19 2,565 3,443 6,00820-24 11,334 6,605 17,93925-29 15,067 42,171 57,23830-34 12,849 20,873 33,72235-39 7,014 51,212 58,22640-44 2,378 45,622 48,00045-49 538 11,039 11,577
TOTAL 51,745 180,965 232,710
Births Averted 17,274 42,096 59,370
Women Practicing Contra-ceDtion per BirthsAverted 3.00 4.30 3.92
Source: Estimates by R. Cuca, Population and Human Resources Division, IBRD.

rU,1Vs 22
Pa,ge 1of 1
West Malaysia
Taget Number and Proportion of Married Women (15 -J49)to be Reached by National Family Planning Program . 127175U
Target NewEst. Mid-Year , No.of Marripd Program Acceptors
Year Population - Women _/ No.
1971 9,853,247 1,442,570 80,000 5.54
1972 10.120.153 1.491,363 100,000 6.70
1973 0.445.o06 4 1,548,108 120,000 7.75
197T 10,769,973 1,604,852 140,000 8.72
1975 11,094,886 1,661,597 16.QDQ.Q 9.62Total 600,000
I/ Mid-vyFar rpnnulatinn estimates based nn Pnnpuls&tinn Prn1aetinnby Age, RAce, and Sex for West Malaysia 1967-1997" ResearchPaper* l4, rlnvArnment of Malaysia, Department of Statintics,November, 1969 p. 26-27. Population estimates interpolated,where n sanaAA-v- byv linear interp1t,olein ThaaCtA IntiRMates aresomewhat higher than those based on the preliminary figures from+t.he 1970 canzsusr and wa1l behad4unted to ,v^nfo,n to the cavirnie
when final official figures are released. Population figuresfor period 1967=1970 i8a the ^ti+.ated population at the mld=pointof this four year period, i.e., beginning of 1969.
2/ Number of mnrried women aged 1 -'a i8 based or. the assump2tIonthat the same proportion of this age group will remain married
nu4,% loA7-.2O#. 4 a AC94 -E ~4 I1 I nnea, 1E:fJ.o
as ir. -,R i.e.m 65.5- Of- 107 .r. sged ar. .
Sorce' P A,ip3in1 Repor't for~ 1970.

Wesit Malaysia
RuLral Clinic Facilities Compared withTarget of New Acceptors Set for 1971-75
Estimate 'Total Clinic Facilities 1971-75 Targets of New Acceptors ____IntegrationRural Total Population Percentage RuralPopulation Faci.lities Coverage Coverage of Total Clinics Population (B) as
Year (millions) KHC SHC MCQ (A) (millions) I/ Population Total Rural 'Integrated Others / Total Coverage Percentage- _ _ _ - _C(mulative) Urban (Cumulat:ive) Areas - _ (B) milionst of (A)
1971 6.4 47 200 988 1235 4.056 63.2 40,000 40,000 40,000 9,000 31,000 230 0).71 17
1972 6.6 57 220 1174, 1451 4.359 65.9 180,1000 80,000 100,0(0 25.000 75,00)0 400 11.2 27.6(+100,000)
I )I ) . I
1973 6.8 62 236 1250 1548 4.644 67.6 300,000 120,000 180, 0O 61,000 119,000 800 2.4 51.7(+120,000)
1974 7.0 65 246 13031 1t614 4.842 68.6 440,1000 140,000 300,000 122,000 175,000 1,200 :3.6 74.3(+140,000)
1975 7.246 66 252 1344 16562 4.974 68.6 600,000 150,COO 4 50Q,0O 207,CO0 243,0c0 1,658 4. 9 100(+160,000) (100lQ ) (4t5 ) (5 I%)
MiC - Main Health Center.SHC - Sub Health Center.MCQ - Midwife Clinic-cum-Quarter..1/ Coverage based on an average of 3,000 per faciLlity.2/ National Fanily Planning Board, Family Planning AsODciation, etc.NOTE: Figures in parenthesis indicate. additional number of acceptors to be
recruited each year..
Soulrces: NFPB and Hinistry of Ma.ltb.

UNEX1 35Page 1 or l
West Ma4ysia
Existing Government Family PlaningService Facilities
NM FacilitiesStatic Slobile
Johor 10 52Kedah 5Kelantanr 1XMalacca 25Negri SbiehIlan 9 hhPahang 7 29
Perlis 1 8Pe*ok ~~16 10,
Selangor 9 44
All States 1j
Source: NFPB unpublished data.

2ategnri!3 of Staff by State Under the NFPB, November, 19,71
RegionaLl FamiLlyTrained Fanily CLerk Infor- Plann:Lng
Med:Lcal Statr sasistant Plaundig Recep-- Clinical mation Field DriverState Officer Sister Nurse Nurse WoDrker tionist Servant Officer Assistant. Operator Total
Johor 1 3 1]. 15 1 2 1 2 1 37
Kadah - 1 4 6 8 - - 1 1 1 22
Kelantan :1 1 - 2 8 1 1 1 1 1 17
Malacca - 1 2 3 4 1 1 1 2 1 16
NegriSembilan IL 1 1 so 8 1 1 1 1 1 25
Pahang 1L 1 1 8 8 1 1 1 1 1 241
Penang 3 4 6 8 2 2 1 1 1 29
Perlis - - ]L 1 - - - - - 2
Perak 1 2 6 1l; 21 2 2 1 2 2 54
Selangor 1. 2 6 13 12 2 3 1 1 2 43
Trengganu 1 2 2 7 1 1 1 1 1 17
rotal 65 14 29 76 l0O 12. 14 10 13 12 286
Source: NFP.B unpublished data. 0 a

ANNEX 37Page 1 of 1
West Malaysia
Average Deliveries per Government HospitalBed by State, 1968
Number of Average
Number Deliveries Deliveries
State of Beds per Bed per Bed
Johor 335 16,120 48
Kedah 110 6,307 571 10t7
Kelantan 49 24
Malacca 134 39
Negri Sembilan 171 6,542 38
Pahang 97 4,832 50
Penang 193 12,494 65
Perak 366 17,187 47
Perlis 36 751 20
Selangor 438 17,700 40
Trengganu 65 893 14
Total 1,994 89,230 45
Source: Ministry of Health.

ANNEX 38Page I ofP
West Malaysia
Staffing Pattern of a Rural Health Unit, 1971
A. in Genter
1. .,44c al n, Und HntI+h nffierA
2. Dental Officer
4. Public Health Nurse5 Dn ent. **urme6. Clerical Assistant7. UW pial A"4s+.t+
8. DispenserO A44 . _4. U.,_ f'N7* LC%LLuu L1UAW %C
10. MidwifellJ. b' 4&.4 C oa.&M, ners ov
12. Dental Surgery Assistant.L3. SOni ati.LW Laborrs(214. Attendants (2).J.. Dent,al Att'Lendarit16. Drivers (2)
17. ardener
B. Subeenter
1. Public Health 'Nurse2. Hospital Assistant3. Clerical Assistant4. Assistant Nurses (2)5. Midwife6. Public Health Overseer7. Sanitation Laborers (2)5. Attendants (2)9. Driver
10. Gardener
C. Midwife Clinic-cum-Quarters
1. Midwife
Source: Ministry of Health.
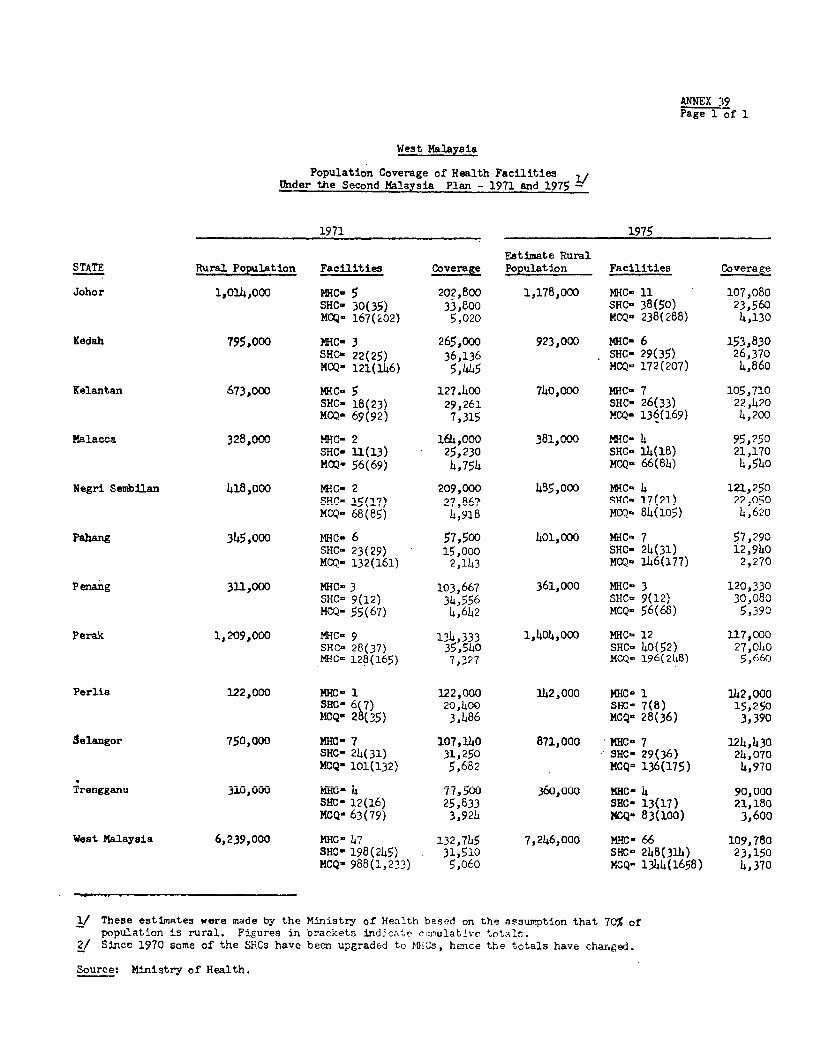
ANNEX 39Page 1 of 1
West Malaysia
Population Coverage of Health Facilitiestnder the Sennei Malavia Plrn, - 1971 And 1975-
1971 1975
Estimate RuralSTATE Rural Population Facilities Coverage Population Facilities Coverage
Johor 1,014,000 MHC- 5 202,800 1,178,000 MHC- 11 107,080SHC- 30(35) 33,800 SHC- 38(50) 23,560MCQ- 167(02> 5,020 MCQ- 238(288) 4,130
Kedah 795.000 MRC- 3 265.000 923.000 MHc- 6 153.830SHC- 22(25) 36,136 SHC- 29(35) 26,370MCQ- 121(146) 5,445 MCQ- 172(207) 4,860
Kelantan 673,000 MHC° 5 127.400 740,000 MHC- 7 105,710SHC- 18(23) 29.261 SHC- 26(33) 22,420MCQ- 69(92) 7,315 MCQ- 136(169) 4,200
Yalacca 3228,000 wc- 2 a1Alo. nr310 NM Mr.- 4 cc 95,20SHC- 11(13) 25,230 SHC- 14(18) 21,170MOQ- 56(69) 4,754 MCQ- 66(84) 4,540
Negri Sembilan 418,000 MHC- 2 209,000 485,000 NMHC 4 121,250SHC- 1I(17) 7,RA87 SHC- 17(21) 22,050MCQ- 68(85) 4,918 MCQ- 84(105) 4,620
Pahang 3345,ow NmC- 6 57,500 401,000 MC- 7 57,290SHC- 23(29) 15,000 8HCm 24(31) 12,940MCO- 132(161) 27143 MCQ- 146(177) 2,270
Penang 311,000 MRC- 3 103,667 361,000 MHC' 3 120,330S'nC= 9(i2') 34,556' Mvc 9(\-3008MCQ- 55(67) 4,642 MCQ- 56(68) 5,390
Perak 1,209,000 MHC- 9 134,333 1,404,000 MNC 12 117,000SHC- 28(37) 35,540 SHC- 40(52) 27,040NRC- 128(165) 7,327 MCO- 196(2h8! 5;660
100 Ann' 2,0.. 1 122,000 nn-L0 VWL nn C= r. 1 142,000SHC- 6(7) 20,400 SHC- 7(8) 15,250MCQ- 28(35) 3,486 MCQ- 28(36) 3,390
aelangor 750,000 MHC- 7 107,140 871,000 MHCO 7 124,430SHr- 21(,A1i) 32 RHO -o 9QU(.S 21.,n7n
MCQ- 101(132) 5,682 MCQ= 136(175) 4,970
Trengganu 310,000 MRC- 4 77,500 360,000 aHC- 4 90,000SHC- 12(16) 25,833 SHC- 13(17) 21,180MCQ- 63(79) 3,921 MmO- 8(lo00o) 3600
West Malaysia 6,239,000 MHC- 47 132,745 7,246,000 HXC- 66 109,780S'nZ= 198(2245) 31,510 SHCuo 240(3ih) 23,150MCQ- 988(1,233) 5,o60 MCQ- 1344(1658) 4,370
1/ These estimates were made by the Ministiy of Health based on the assumption that 70% ofpopulation is rural. Figures in brackets indicate rui.ulatlvc totals.
2./ S4-Ce 1970 som..e of the SYL.Cs have becr. upgraded to IL'1I-, he.ce the totals have changed.
Source: Ministry of Health.

ANNEX 40PAge 1 of 1
TJW+ U.,-e 4n
Ntpati4ent Atter.d.lace a+ He 'th Cer.ters, 1970
Size of Daily MHC. SHIC TotalAtter.d -- c- Nu.,.er Percen' Nuruber Ine0rcen 0I- t wnu-,lber PeIrcent&ILU UWALLUM.L1 )q1 UIII J L Zi .Kw .- UI, a UIULJVL rtiii 1 LAJL ZL 1
-1 A ' 7 I,7 in q I Q n.L - 7 L r .f Li .L'o.C i.vV .7
10 - 19 1 2.7 34 20.5 35 17.220 - 7 X 8.L .7 ?V 2.L.( 4.2
30 - 39 6 16.2 33 19.9 39 19.2L40 - L47 C2 .4 C. .v C22 1U.8
50 - 99 11 29.8 22 13.3 33 16.3II^ 9a.^^ 0 e z ,0 IlUU - 1o7 U C.L. 3 11 i4
200 and over 1 2.7 1 0.6 2 1.0
Total 37 100.0 166 100.0 203 100.0
Sources: Data from Ministry of Health and computations by the mission.

A V-.Y Ii I
Page 1 of a
Wmst Mal1avsia
Maternal and Child Health Clinic Attendances, 1970 2/
New and New andReturn Average Return AverageAtten- Atten- Atten- Atten-
No. dance dance per No= dance dance perState MHCa Per MCH Session SHC3 Per SHC Session
Johor 5 777 52 28 8,113 54Kedah 3 9,3914 63 20 4j,31h 29Kelantan 5 11,690 78 16 7,120 47Malacca 2 8,506 57 11 J.,166 29Negri Sembilan 2 24,065 160 15 3,654 24Pahanr 6 5,14914 37 20 5,LR68 36Penang 2 11,918 80 6 17,918 119Peal i 1 15,306nA In10 If 4 20
Perak 7 6,065 40 28 4,993 33~~nl~r~~ '7 1. 71 3 001 L A 1 I 0Sel^anor 7 ,232 21L L4,0,32 27
Trengganu 4 5,776 39 10 3,336 22Nvational
Average 44 7,346 49 180 5,725 38
l/ Based on 150 clinic sessions per year in each health center.
Sources: Data from Ministry of Health and computations by thejnission.
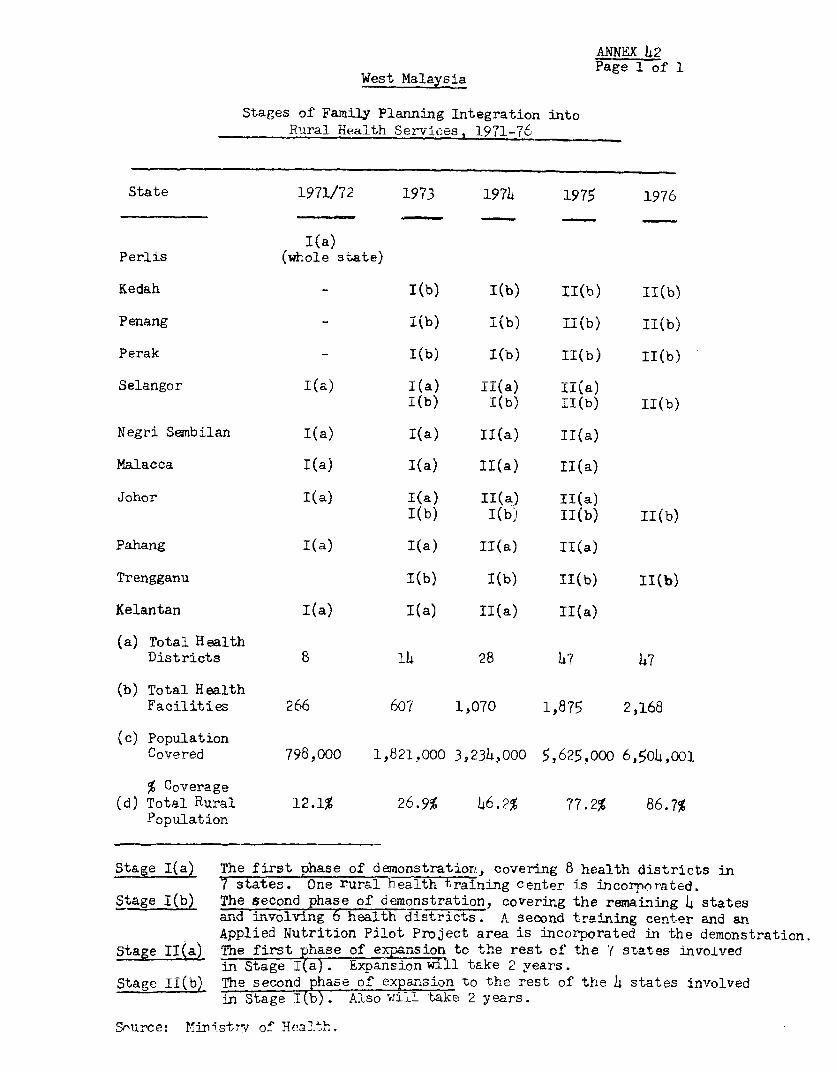
ANNEX 42
West Malaysia Page 1 of 1
Stages of Family Planning Integration intoRural Health Ser-v-ices. 1971-76
State 1971/72 1973 1974 1975 176r
I(a)Perlis (whole state)
Kedah I(b) I(D) II(b) b i(b)
Penang - I(b) I(b) II(b) II(b)
Perak l(b) 1(b) II(b) 1I(b)
Selangor I(a) !(a) !!(a) !!(a)I(b) I(b) II(b) II(b)
Negri Sembilan I(a) !(a) II(a) II(a)
Malacca I(a) I(a) II(a) II(a)
Johor I(a) I(a) II(a) II(a)I(b) I(b) II(b) II(b)
Pahang I(a) I(a) II(a) II(a)
Trengganu 1(b) I(b) II(b) II(b)
Kelantan I(a) I(a) II(a) II(a)
(a) Total HealthDistricts 8 14 28 47 47
(b) Total HealthFacilities 266 607 1,070 1,875 2,168
(c) PopulationCovered 798,000 1,821,000 3,234,000 5,625,000 6,504,001
(d) Total Rural 12.1% 26.9% 46.2% 77.2% 86.7%Populat ion
Stage I(a) The first phase of demonstration, covering 8 health districts in
7 sttes. One rural health training center is incornorated.
Stage I(b) The second phase of demonstration, covering the remaining 4 statesand iunvolving 6 health districts. A second traiinnng center and an
Applied Nutrition Pilot Project area is incorporated in the demonstration.
Stage 11(a) Tne first phase of expansion to the rest of the ( states involved
in Stage I(a). Expansion will take 2 years.
Stage II(b) Tne second a oI exp arsion to the rest of the 14 states inv olvedin Stage I(b). Also will take 2 years.
Snurce: Minrst-v of Healt)h.

ANNEX 43Page 1 of 1
West Malavsia
Nuniber of Clinics OperatedFeder-ation of Family Planning Association, 1971
State Urba5 Estate 2/ Total
Johor 23 20 43Kedah 11 11Kelantan 9 9Malacca 17 17Negri Sembilan 12 12Pahang 6 6Penang 14 14 28Perlis 4 4Perak 39 82 121Selangor 26 26Trengganu 8 _8
Total 169 116 285
1/ End of year figures.2'/ Rubber estates and tin mines.
Source: Federation of Family Planning Association.
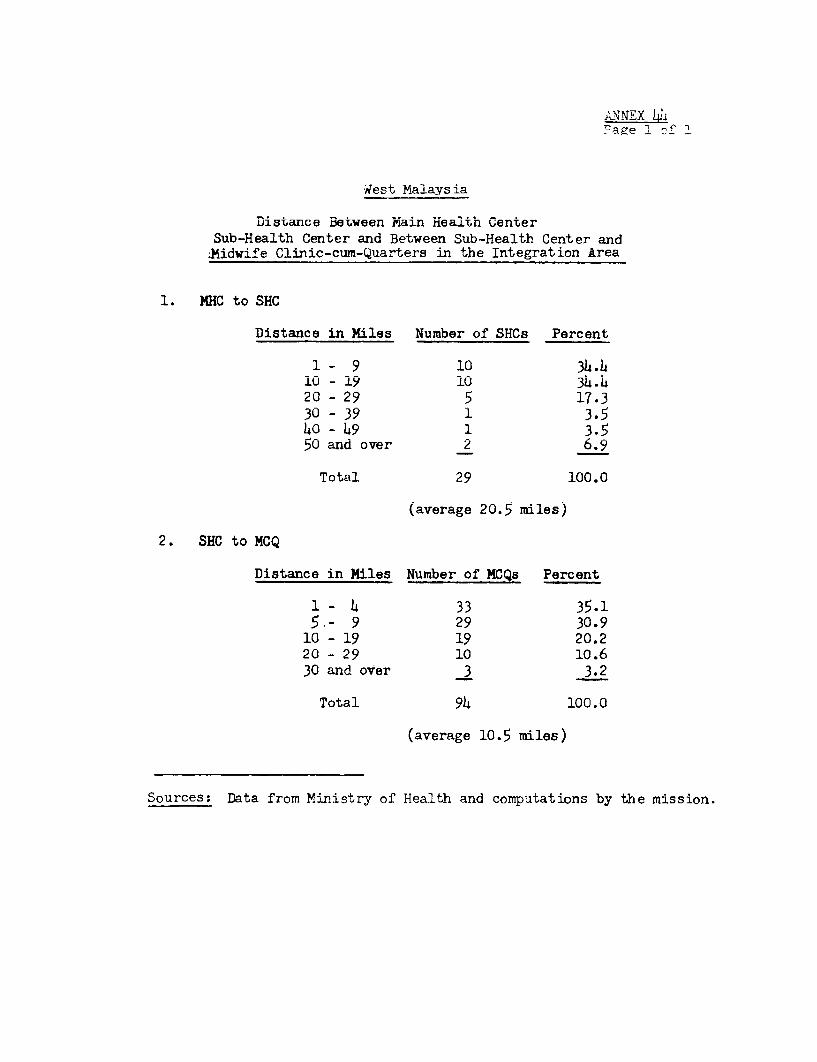
ANNEX 1ELPage 1 -: '
w'es t Malaysia
Distance Between Main Health CenterSub-Health Center and Between Sub-Health Center and
;Midwife Clinic-cum-Quarters in the Integration Ar-ea
1. MHC to SHC
Distance in Miles Number of SHCs Percent
1- 9 10 34.410 - 19 10 34.420 - 29 5 17.330 - 39 1 3.540 - 49 1 3.550 and over 2 6.9
Total 29 100.0
(average 20.5 miles)
2. SHC to MCQ
Distance in Miles Number of MCQs Percent
1 - 4 33 35.15,- 9 29 30.9
10 - 19 19 20.220 - 29 10 10.630 and over 3 3.2
Total 94 100.0
(average 10.5 miles)
Sources: Data from Ministry of Health and computations by the mission.

ANNEX 45Page 1 of 1.
West Malaysia
Health Manpowrer in Government Health Services
Posts VacanciesCategories Authorized Filled No. d
Medical Doctors 1,117 1,028 89 7.9
Nursing Personnel 5,966 4,749 1,217 20.3
Matrons (all categories) 75 71 4 5.3
Nursing Sisters h9l 40h 87 17.7
,in AospitaLs) (L08) (326) (82) (20.0)(ln lue a-l th)1 (83 -7Q ) (f) (,
-L A U gnf, 1.7~~~~~~~~~~( r
Staff N'iu±rses 2,7 147 L78 19.3
(in Hospitals) (1,926) (1,585) (3-I) (L7.7)(in Health) (5L7) (L10) (137) (25.()
Assistant Nurses 2,927 2,279 6h8 22.1
(in losPI ti ss (2,080) (1,791) (289) (13.8)(in Health) (8M7) (488) (359)
Midwives 2,545 2,023 522
(in Hospitals) (756) (608) (148) (19.5)(in Health) (1,789) (1,415) (371) (20.9)
Public Health Inspectors L0L 33h 70 17.3
Public Health Overseers 410 402 8 1.)
Hospital Assistants 1,067 867 200 18.7
1/ Includes only categnries relevant to the family planning program,as of October 1971.
Source: Ministry of Health.

ANNEX 46Pag 1 of' 1
West Malaysia
F'StAmTelCi Shrta rf Ntlrming PpynrnnnP1 197-1-75
TrainedRegistered AssistantNurses Nurses Midwives
A. Number of PostsAuthorized in 1971 2,473 2,927 2,545
B. Number of PostsEstimated for 1975 Y 3,568 4,405 3,054
C. Number of Personnelin Service in 1971 1,995 2,279 2,023
D. Additional Requirement(B-C) 2,573 2,126 1,031
E. Estimaijed Graduates withExisting Plan 2/ 1,492 1,191 627
F. Remaining Shortage(D-E) 1,081 935 404
1/ Assuming 50% increases in authorized posts fOr registered nurses andTANs and a 20% increase for midwives during the period Of 1971-75,based on MWl manpower projections.
2/ Graduates in 1971 are not included, assuming that they were alreadyengaged in the service.
Sources: Ministry of Health and computations by the mission.

West Malayeia
Publ:Lc Health Personnel Trained at Rural Health Center, Jitra. 3956-.71
Auxdli<iry Staf f Supervisory Staff
10-16 Week Course 2-3 Week Course Field Traininfrom PHI Super- TotalTotal Medical viLsorr Super-
Student/ Auxi- PHU Students Course visory GrarldPHO TAIN MiLdwife Others lir. (9L iks) PHI (3 'WsL (4, _Wke Others Staff Total
1956 12 13 13 38 - - 3819.57 7 18 11 36, - - 3619.58 9 10 10 259 - 2 22 - 22 511959 13 12 10 35 - - - 35196S0 19 13 45 - - - 451961 24 12 12 148 - 214 22 - 46 941962 19 13 12 17 61. 1.1 22 - 23 21 77 13819653 22 13 13 48, 1]6 214 *- 23 37 100 14819654 23 13 13 449 114 121 . L6 - 42 9119655 32 114 114 60 20 2 3 20 - 63 1231956 17 9 9 35 - ' *- - 10 15 50196,7 11 6 6 24 47 - 12 -21 5 38 851968 6 12 9 26, 53 12 21 52 - 10 94 1 471969 - 27 32 59' ] 2 30 1,7 - - 89 1481970 8 49 88 145 1]0 42 1 48 - 25 125 2701971 - 23 66 89, 1.0 33 37 - 80 169
:222 254 331 67 874 105 214E 181, 1148 108 792 1,666
Sources: Ministry of HIeal-th.P'ubliLc Health Institute.

Weest Malaysia
Public Health Personnel Trained at Rural Health Center, ReRbLu 1 66
Auxil.iary Staff SurviStory Stalf
10-16 lieek Course 2-3 Week Course FIiQel Tx4kining f,Q.yM.PI Super- Total
…… ~ Total Medical visory Sulper-
Student/ Auxi- PHN Students Course visory Grand
PE) TAN Mdiwife Others _ _lia_ SESkZ) (L3LWk) (h i k2 Others Staff Total
1 966 17 7 -1 -15 51 - :
1L967 23 8 6 4 41 8 63 19 3 93 124
1968 2'5 L 12 30 78 9 25 - 13 4t7 125
:L969 43 - - 43 10 31 - 41 84
:L970 82 - - 68 150 10 35 - 10 55 205
:L971 - 29. 37 91 157 10 35 _ 17 62 219
Total 190 57 65 208 5'20 47 189 43 43 322 8142
Sources: Ministry of Health.PuLblic Health Institute.

ANNEX49Page 1 of 1
West Malaysia
Family Planning Syllabus for Auxiliary Courseat Rural Health Training Centers
Theory
1. Why Family Planning? Demographic, Economic, Social,and Health Aspects 1 hr.
2. Policies of the National Family Planning Board ½ hr.
3. Anatorly and Physiology of the Female/MaleReproductive Systems 1 hr.
4. Methods of Family Planning:
Conventional Methods 1 hr.
Pill 1 hr.
Intrauterine Contracentive navice 1 hr.
Tn ine ti on 1 hr-.
Surgery 1 hr,
5. N+inal mily Plnina B Program forService, Training, Information, Evaluation,and S u p pf 2hr
6. Evaluation ni.d qupp1rr (>ractical) 1¼ or
7. T ofNationa. .- a. of1 atio.ar Fa* * .Lain6 Boardwith the Rural and Medical Health Services ½ hr.
8. Methods of Family Planning (Practical) 1 hr.
9. Beliefs and Taboos in Relation to Family Planning 1 hr.
Sources: Ministry of Health.rublic Health Instuitute.

ANNEX 50Page 1 of 1
West Malaysia
National Family Planning Board Training Courses
-. ------ , / 1/~~~~~. r---'- A 2 TNo. Category of Personnel/ No*. of Personnel Trained aL d NO . of CouJrsesType of Course Duration 1967 1968 1969 1970 1971 Total
1. NFPB Staff - Initial 4 weeks 77/4 90/5 52/4 33/3 29/2 281/18
2. NFPB Staff - Refresher 3 days- 13/2 25/2 58/4 35/2 64/3 195/131 week
39-Seminar3. NFPB Staff - integration 4 days 35-Course/- 75/-
4. Ministry of Healthl - 2 weeks 57/4 212jl2 3U06i/7 2f/1U0 9/lU0 9fL/53
Orientation
5. Ministry of Health - 3 Weeks 238/15 79/5 317/20Integration
6. Ministry of Health - 4 days 78/5 78/5Seminar on Integration
7. Special Course for Mini- 2 days 24/2 25/1 49/3stry of Health Staff M.O.
8. Ministry of Information 2 days 17/1 3/- 20/1& Broadcasting-Orientation
9. Ministry of Social 3 days 19/1 13/1- 32/2Welfare - Orientation
10. Private Practitioners 1 day 39/3 39/3
11. Peace Corps Volunteers- 10 days 13/1 13/1Initial
3-Integration12. Peace Corps Volunteers- 2 days 12/1 15/1
Refresher
13. Traditional Midwives 3 weeks 213/12 149/9 353/16 715/37
14. Estates 2 weeks 7/- 26/- 2/- 3/- 27/2 65/2
15. Other Related Services - 8/- 2/- 15/1 13/4 38/5
Total 198/12 416/24 646/38 870/46 772/44 2,902/164
1/ Fisrt figure in column indicates number of personnel trained; second figureSu dicNat.m inalm i1vr of cour esnndc-terd=
Source: Natinnal Familv P1lanning, Rnard=-

ANNEX 51Page 1 of 1
West Malaysia
Number of Nursing Personnel, 1966-75
Actual Number
Year Nurses Assistant Nurses Midwives
1966 217 .17 146
1967 203 279 139
1968 133 172 128
1969 332 62 81
1970 225 93 li
Subtotal A 1,110 623 608
Expected Graduates
1971 23h 297 107
1972 2)17 159
1973 3°5 5h8 158
1071 hn3 95 152
1 07 C
Subtotal B 1,726 1 J17R 73L
Percentage inc rease
from A to B 47.0 137.0 20.0
Source: Ministry of Health