ob/gyn for ems providers
DESCRIPTION
Prehospital care for Obstetrical patients with A&P.TRANSCRIPT

Obstetrics - EmergenciesObstetrics - Emergencies
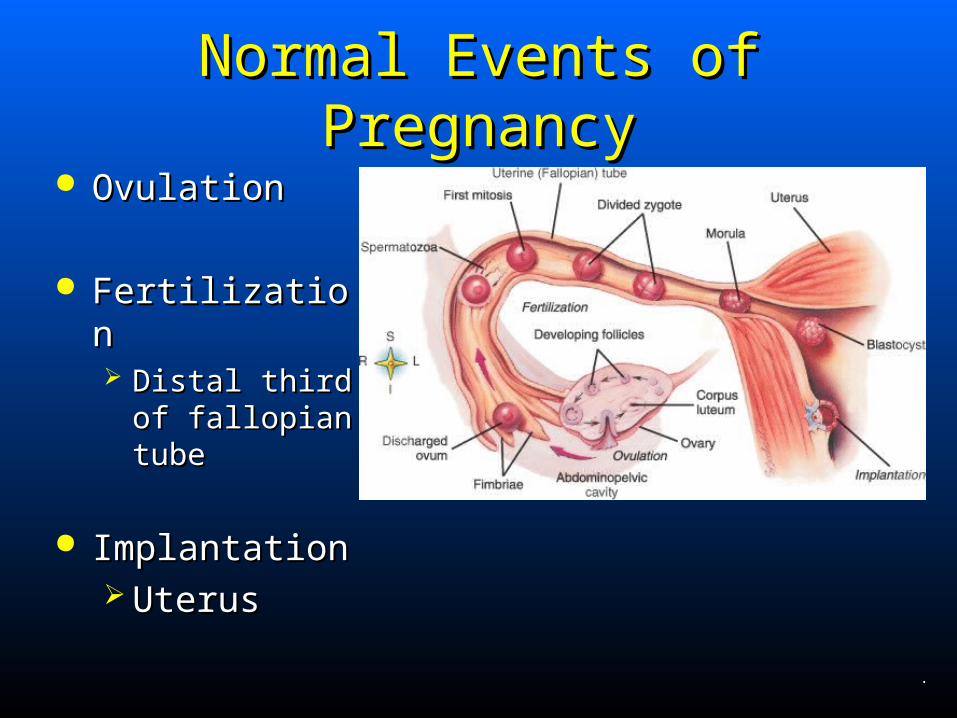
Normal Events of PregnancyNormal Events of Pregnancy OvulationOvulation
FertilizationFertilization Distal third of Distal third of
fallopian tubefallopian tube
ImplantationImplantation UterusUterus
.
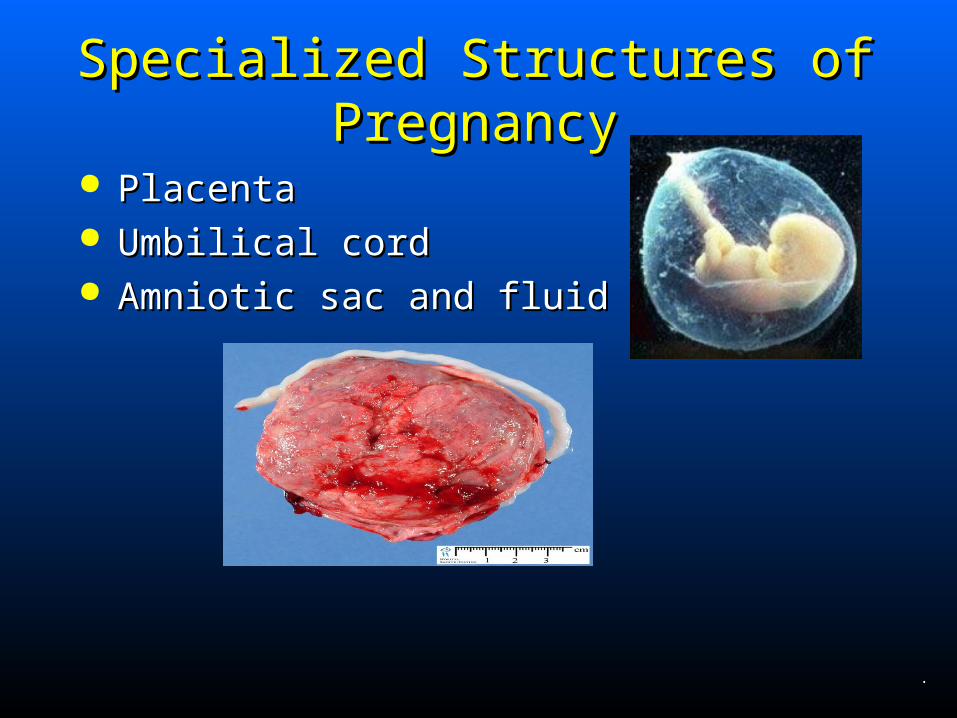
Specialized Structures of PregnancySpecialized Structures of Pregnancy
PlacentaPlacenta Umbilical cordUmbilical cord Amniotic sac and fluidAmniotic sac and fluid
.
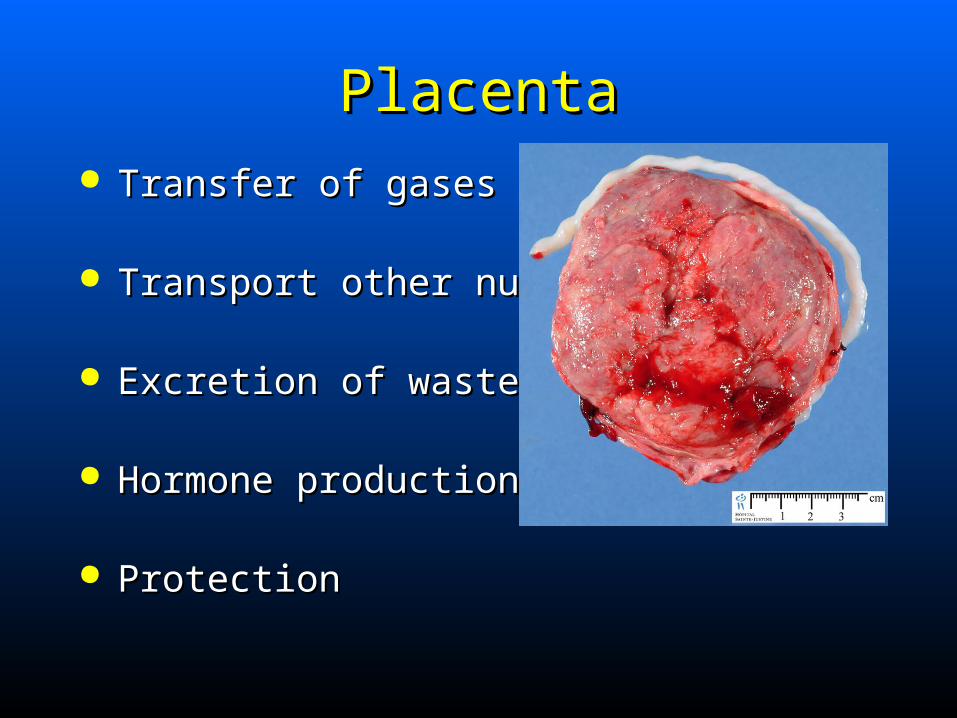
PlacentaPlacenta Transfer of gasesTransfer of gases
Transport other nutrientsTransport other nutrients
Excretion of wastesExcretion of wastes
Hormone productionHormone production
ProtectionProtection
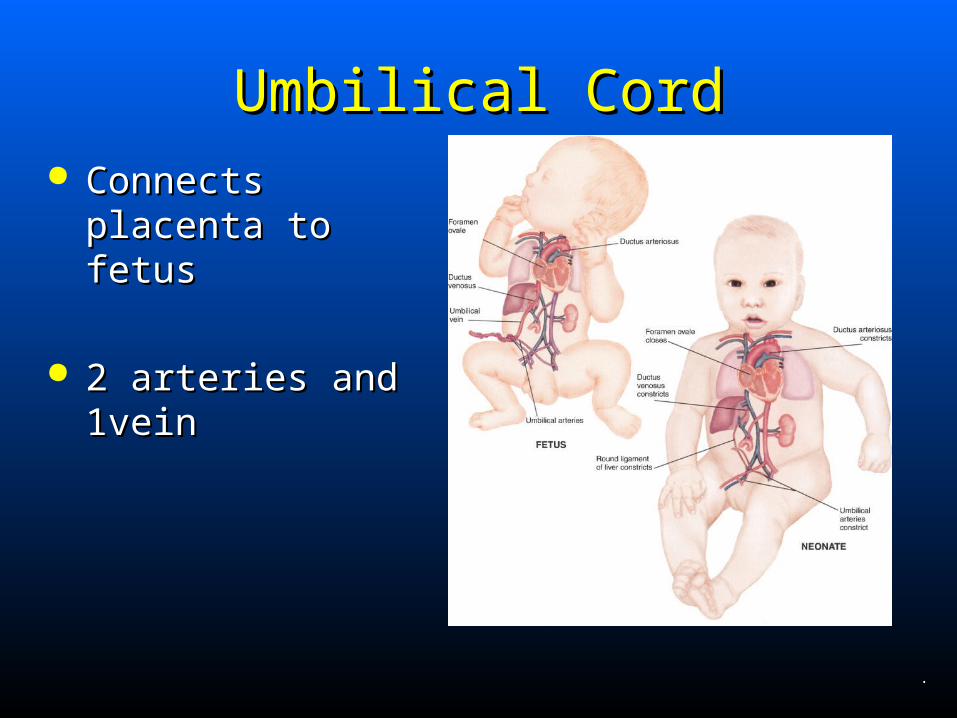
Umbilical CordUmbilical Cord Connects placenta Connects placenta
to fetusto fetus
2 arteries and 1vein2 arteries and 1vein
.
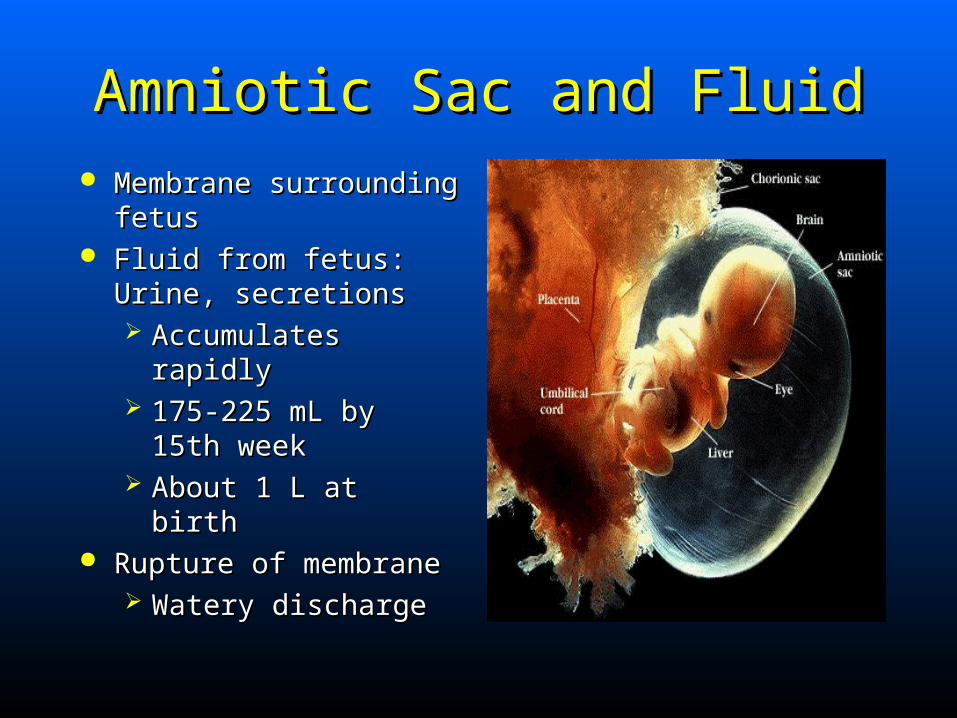
Amniotic Sac and FluidAmniotic Sac and Fluid Membrane surrounding Membrane surrounding
fetusfetus Fluid from fetus: Urine, Fluid from fetus: Urine,
secretionssecretions Accumulates rapidlyAccumulates rapidly 175-225 mL by 15th 175-225 mL by 15th
weekweek About 1 L at birth About 1 L at birth
Rupture of membraneRupture of membrane Watery dischargeWatery discharge

Fetal Growth and DevelopmentFetal Growth and Development
First 8 weeks of pregnancyFirst 8 weeks of pregnancy EmbryoEmbryo
After that and until birthAfter that and until birth FetusFetus
Fetal Growth and DevelopmentFetal Growth and Development
Term InfantTerm Infant
Anytime after 37 but before 42 weeksAnytime after 37 but before 42 weeks
Most weigh 6.6 to 7.9 poundsMost weigh 6.6 to 7.9 pounds Average 40 wks from fertilization to deliveryAverage 40 wks from fertilization to delivery 90-day periods (trimesters)90-day periods (trimesters) Gestation – time from fertilization until birth (avg. Gestation – time from fertilization until birth (avg.
is 266 days or 8.86 mos)is 266 days or 8.86 mos)
.
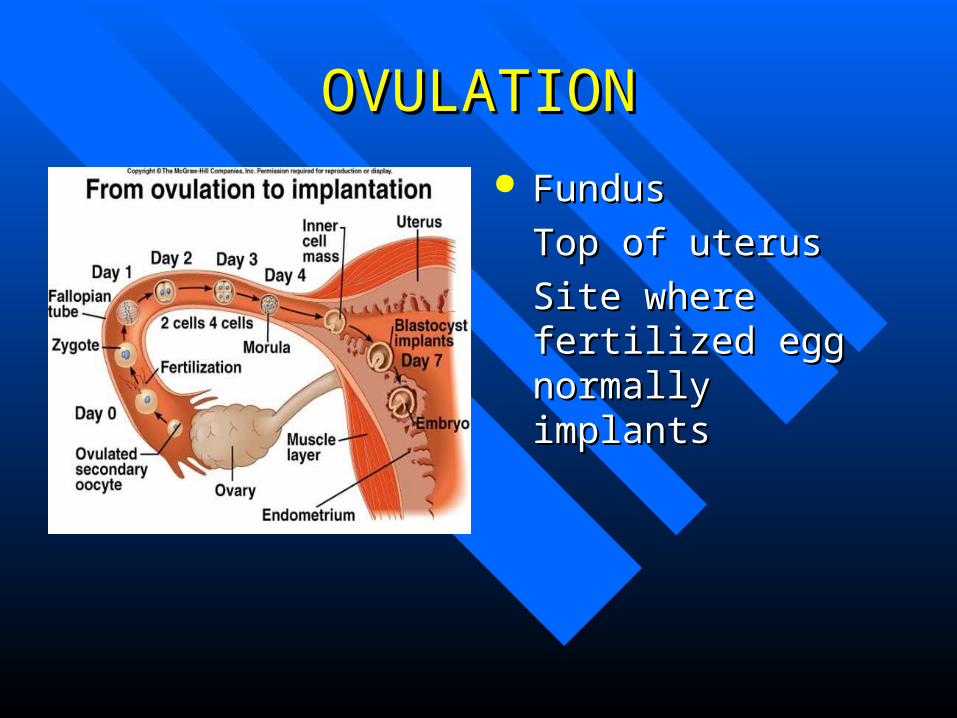
OVULATIONOVULATION FundusFundus
Top of uterusTop of uterus
Site where fertilized Site where fertilized egg normally egg normally implantsimplants
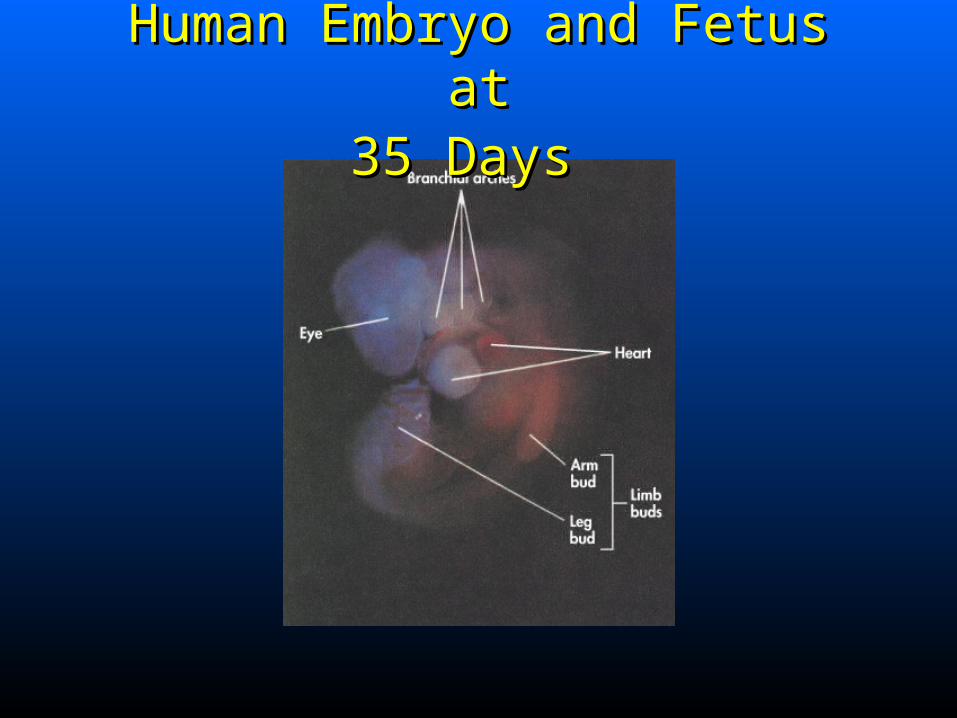
Human Embryo and Fetus atHuman Embryo and Fetus at35 Days35 Days
Human Embryo and Fetus atHuman Embryo and Fetus at49 Days49 Days
Human Embryo and FetusHuman Embryo and Fetusat End of 1st Trimester at End of 1st Trimester
Human Embryo and Fetus atHuman Embryo and Fetus at4 Months 4 Months
.
PregnancyPregnancy Term Infant
Anytime after 37 but before 42 weeksMost weigh 6.6 to 7.9 pounds
Obstetrical TerminologyObstetrical Terminology GravidaGravida
All current and past pregnanciesAll current and past pregnancies
Para Para Number of past pregnancies viable to deliveryNumber of past pregnancies viable to delivery
AntepartumAntepartum Period before deliveryPeriod before delivery
GestationGestation Period of intrauterine fetal developmentPeriod of intrauterine fetal development
Grand multiparaGrand multipara Seven deliveries or moreSeven deliveries or more
Obstetrical TerminologyObstetrical Terminology MultiparaMultipara
Two or more deliveriesTwo or more deliveries
NatalNatal Connected with birthConnected with birth
NulliparaNullipara Has never deliveredHas never delivered
PerinatalPerinatal——occurring occurring At or near time of birthAt or near time of birth
PostpartumPostpartum Period after deliveryPeriod after delivery
Obstetrical TerminologyObstetrical Terminology Prenatal Prenatal
Before birthBefore birth
PrimigravidaPrimigravida Pregnant for first timePregnant for first time
PrimiparaPrimipara Gave birth onceGave birth once
TermTerm Pregnancy at 40 weeks’ gestationPregnancy at 40 weeks’ gestation
.
Maternal Changes During PregnancyMaternal Changes During Pregnancy
Cessation of menstruationCessation of menstruation
Enlargement of uterusEnlargement of uterus
Other changes affect: Other changes affect: Genital tractGenital tract BreastsBreasts Gastrointestinal systemGastrointestinal system Cardiovascular systemCardiovascular system Respiratory systemRespiratory system MetabolismMetabolism
Obstetrical History Obstetrical History Length of gestationLength of gestation Parity and gravidityParity and gravidity Previous cesarean delivery Previous cesarean delivery Maternal lifestyle Maternal lifestyle Infectious disease statusInfectious disease status Previous gynecological or obstetrical Previous gynecological or obstetrical
complications complications PainPain
Obstetrical HistoryObstetrical History Quantity, character of vaginal bleedingQuantity, character of vaginal bleeding
Abnormal vaginal dischargeAbnormal vaginal discharge
““Show” Show” Expulsion of mucous plug in early laborExpulsion of mucous plug in early labor
Rupture of membranesRupture of membranes
General health and prenatal careGeneral health and prenatal care
.
Obstetric HistoryObstetric History Allergies, medications takenAllergies, medications taken
Use of narcotics within 4 hrsUse of narcotics within 4 hrs
Urge to bear down Urge to bear down
Sensation of imminent bowel movement Sensation of imminent bowel movement
.
Physical ExaminationPhysical Examination Chief complaint determines examChief complaint determines exam
Rapidly identify acute surgical or life-threatening Rapidly identify acute surgical or life-threatening conditions or imminent deliveryconditions or imminent delivery
Take appropriate management stepsTake appropriate management steps
Physical ExaminationPhysical Examination Evaluate general appearance and skin colorEvaluate general appearance and skin color
Assess vital signs and reassess Assess vital signs and reassess
Examine abdomen for previous scars and Examine abdomen for previous scars and any gross deformityany gross deformity
.
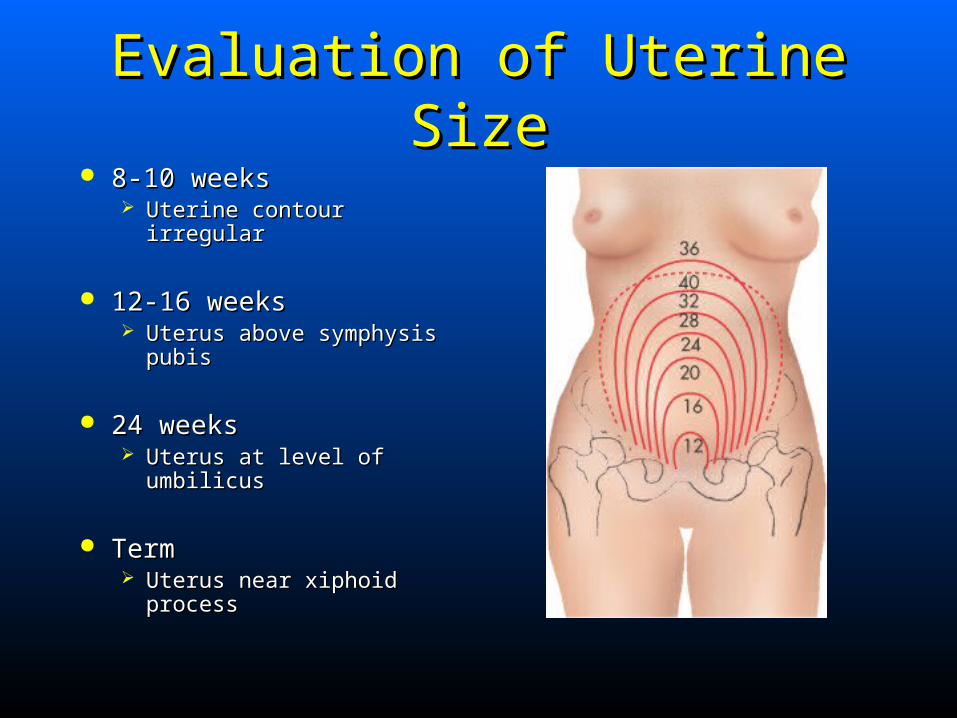
Evaluation of Uterine SizeEvaluation of Uterine Size 8-10 weeks8-10 weeks
Uterine contour irregular Uterine contour irregular
12-16 weeks12-16 weeks Uterus above symphysis Uterus above symphysis
pubispubis
24 weeks24 weeks Uterus at level of umbilicusUterus at level of umbilicus
TermTerm Uterus near xiphoid Uterus near xiphoid
processprocess

Fetal MonitoringFetal Monitoring Fetal heart soundsFetal heart sounds
Auscultate between 16 and 40 wks by Auscultate between 16 and 40 wks by stethoscope, fetoscope, or Dopplerstethoscope, fetoscope, or Doppler
Benefits of fetal monitoringBenefits of fetal monitoring ProcedureProcedure Normal fetal heart rate: 120-160 bpmNormal fetal heart rate: 120-160 bpm
Fetoscope Fetoscope
Doppler Doppler
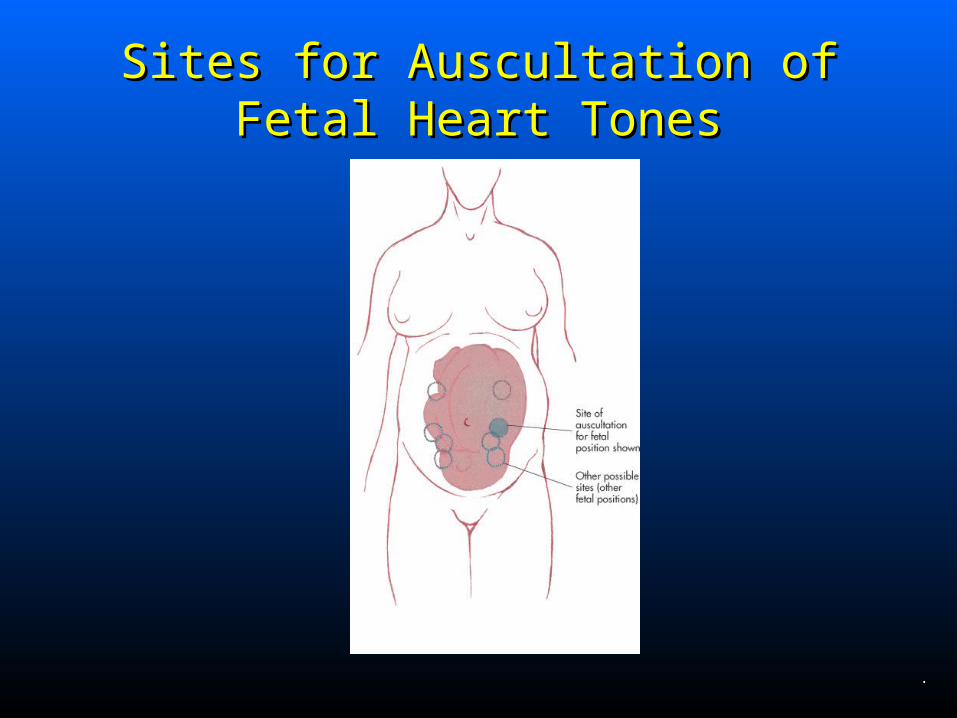
Sites for Auscultation ofSites for Auscultation ofFetal Heart TonesFetal Heart Tones
.

General Management of OB PatientGeneral Management of OB Patient
If birth not imminent, care for healthy patient often If birth not imminent, care for healthy patient often can be limited to basic treatment modalitiescan be limited to basic treatment modalities
In absence of distress or injury, transport in position In absence of distress or injury, transport in position of comfort:of comfort:
Usually left lateral recumbentUsually left lateral recumbent ECG monitoring, oxygen, and fetal monitoring may be ECG monitoring, oxygen, and fetal monitoring may be
indicatedindicated Based on assessment Based on assessment IV access in some patientsIV access in some patients
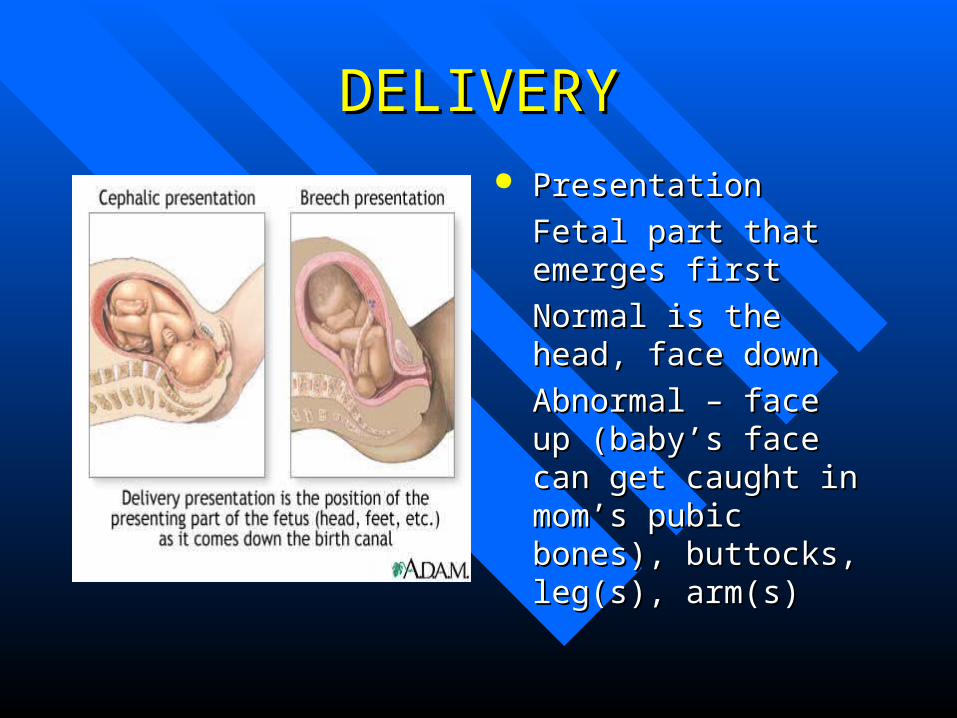
DELIVERYDELIVERY PresentationPresentation
Fetal part that emerges Fetal part that emerges firstfirst
Normal is the head, Normal is the head, face downface down
Abnormal – face up Abnormal – face up (baby’s face can get (baby’s face can get caught in mom’s pubic caught in mom’s pubic bones), buttocks, leg(s), bones), buttocks, leg(s), arm(s)arm(s)
Cesarean SectionCesarean Section
Performed when Performed when mom or fetus in mom or fetus in dangerdanger
If in mom’s history, If in mom’s history, ask why section ask why section done.done.
May give you clues May give you clues as to past delivery as to past delivery complicationscomplications
Cesarean SectionCesarean SectionCommon causesCommon causes
Placenta previaPlacenta previaAbruptio placentaAbruptio placentaLabor that didn’t Labor that didn’t progressprogressEclampsiaEclampsiaFetal distressFetal distressBreech presentationBreech presentationProlapsed cordProlapsed cord
Cephalopelvic Cephalopelvic disproportion – baby disproportion – baby too large for mom’s too large for mom’s pelvic openingpelvic openingActive herpes lesionsActive herpes lesionsRarely, old C-section Rarely, old C-section scar can weakenscar can weaken

Complications of PregnancyComplications of Pregnancy TraumaTrauma
Medical conditionsMedical conditions
Pregnancy itselfPregnancy itself
Prior disease processesPrior disease processes Aggravated by pregnancyAggravated by pregnancy
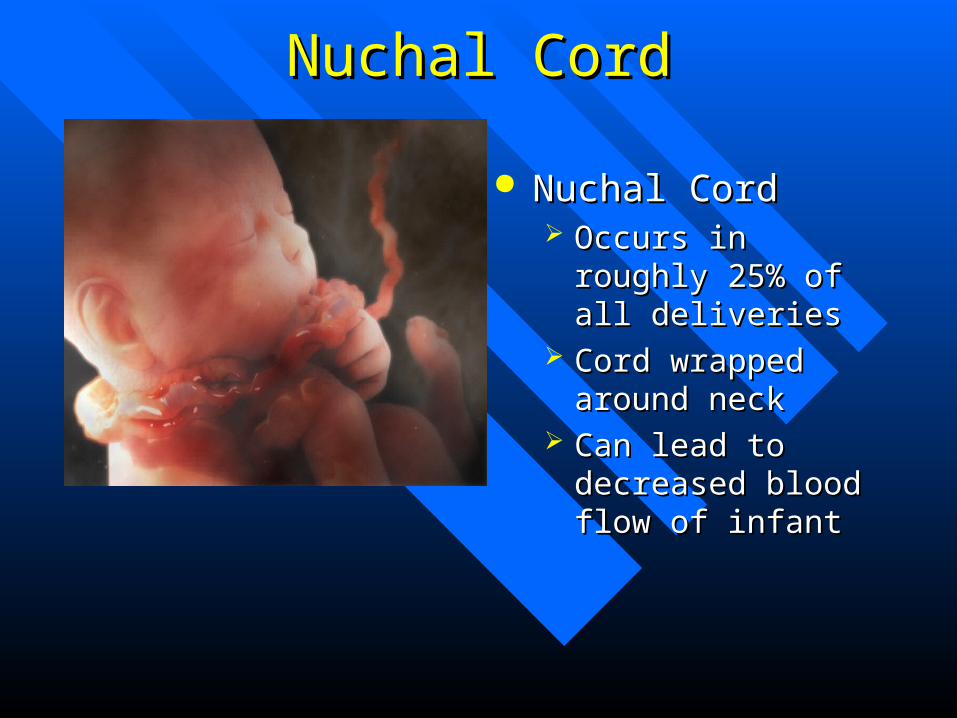
Nuchal CordNuchal Cord
Nuchal CordNuchal Cord Occurs in roughly Occurs in roughly
25% of all deliveries25% of all deliveries Cord wrapped Cord wrapped
around neckaround neck Can lead to Can lead to
decreased blood flow decreased blood flow of infantof infant
Trauma in PregnancyTrauma in Pregnancy Causes of maternal injuryCauses of maternal injury
Vehicular crashesVehicular crashes FallsFalls Penetrating objectsPenetrating objects
Greatest risk of fetal deathGreatest risk of fetal death Fetal distress and intrauterine demise caused by Fetal distress and intrauterine demise caused by
trauma to mother or her deathtrauma to mother or her death
Trauma in PregnancyTrauma in Pregnancy Assess and intervene for motherAssess and intervene for mother
Fetal death from maternal traumaFetal death from maternal trauma
Pregnant trauma patient needs physician Pregnant trauma patient needs physician evaluationevaluation
AssessmentAssessment Signs of shock can be slow to developSigns of shock can be slow to develop Decreased fetal movement/HR may indicate shockDecreased fetal movement/HR may indicate shock
.
Trauma in PregnancyTrauma in Pregnancy ManagementManagement
OxygenateOxygenate Prepare for laborPrepare for labor Aggressive resuscitation if arrestAggressive resuscitation if arrest Immobilize and transport Immobilize and transport
• Left lateral recumbant positionLeft lateral recumbant position
• Manual uterine displacementManual uterine displacement
Medical Conditions Medical Conditions Pregnancy can mask or aggravate:Pregnancy can mask or aggravate:
AppendicitisAppendicitis CholecystitisCholecystitis HypertensionHypertension DiabetesDiabetes InfectionInfection Neuromuscular disordersNeuromuscular disorders Cardiovascular diseaseCardiovascular disease
PreeclampsiaPreeclampsia Unknown causeUnknown cause
Often healthy, normotensive primigravidaOften healthy, normotensive primigravida• After twentieth week, often near termAfter twentieth week, often near term
Preeclampsia and EclampsiaPreeclampsia and Eclampsia Diagnosis of preeclampsiaDiagnosis of preeclampsia
HypertensionHypertension• Blood pressure >140/90 mm HgBlood pressure >140/90 mm Hg• Acute rise of 20 mm Hg in systolic pressureAcute rise of 20 mm Hg in systolic pressure
OROR• 10 mm Hg rise in diastolic pressure over prepregnancy 10 mm Hg rise in diastolic pressure over prepregnancy
levelslevels ProteinuriaProteinuria Excessive weight gain with edemaExcessive weight gain with edema
Treat hypertension, prevent seizuresTreat hypertension, prevent seizures

EclampsiaEclampsia Same signs and symptoms plus seizures or comaSame signs and symptoms plus seizures or coma
Tonic-clonic activityTonic-clonic activity
Often begins as oral twitchingOften begins as oral twitching
Often apnea during seizureOften apnea during seizure
Can initiate laborCan initiate labor
EclampsiaEclampsia——ManagementManagement Left lateral recumbent positionLeft lateral recumbent position
Minimize stimulationMinimize stimulation
Oxygen and ventilation assistanceOxygen and ventilation assistance
If seizures:If seizures: Monitor vital signsMonitor vital signs
Gestational Diabetes MellitusGestational Diabetes Mellitus Mother can’t metabolize carbohydratesMother can’t metabolize carbohydrates
Excess glucose goes to fetusExcess glucose goes to fetus Stored as fatStored as fat
TreatmentTreatment Glucose monitoringGlucose monitoring DietDiet ExerciseExercise InsulinInsulin
Vaginal BleedingVaginal Bleeding Abortion (miscarriage)Abortion (miscarriage)
Ectopic pregnancyEctopic pregnancy
Abruptio placentaeAbruptio placentae
Placenta previaPlacenta previa
Uterine ruptureUterine rupture
Postpartum hemorrhagePostpartum hemorrhage
AbortionAbortion Termination of pregnancy from any cause before 20Termination of pregnancy from any cause before 20thth
week of gestationweek of gestation Later is known as Later is known as preterm birthpreterm birth
Common classifications of abortionCommon classifications of abortion
Determine:Determine: Onset of pain and bleedingOnset of pain and bleeding Amount of blood lossAmount of blood loss If any tissue passed with bloodIf any tissue passed with blood
ManagementManagement
Ectopic PregnancyEctopic Pregnancy Ovum implants outside uterusOvum implants outside uterus
CommonCommon
Predisposing factors Predisposing factors
Classic triad of symptomsClassic triad of symptoms Abdominal painAbdominal pain
• Shoulder painShoulder pain Vaginal bleedingVaginal bleeding AmenorrheaAmenorrhea
• May not be presentMay not be present
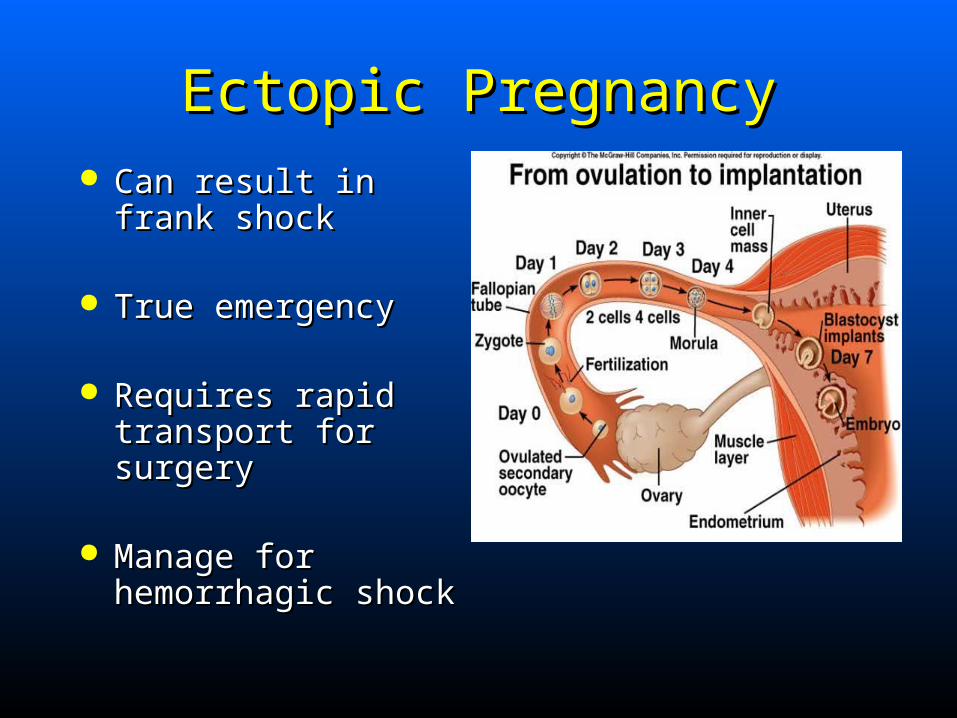
Ectopic PregnancyEctopic Pregnancy Can result in frank Can result in frank
shockshock
True emergencyTrue emergency
Requires rapid Requires rapid transport for surgerytransport for surgery
Manage for Manage for hemorrhagic shockhemorrhagic shock
Third-Trimester BleedingThird-Trimester Bleeding 3% of pregnancies3% of pregnancies
Never normalNever normal
Most often due to:Most often due to: Abruptio placentaeAbruptio placentae Placenta previaPlacenta previa Uterine ruptureUterine rupture
Abruptio PlacentaeAbruptio Placentae Partial or complete detachment of normally Partial or complete detachment of normally
implanted placenta at more than 20 weeks’ implanted placenta at more than 20 weeks’ gestationgestation
Predisposing factorsPredisposing factors TraumaTrauma Maternal hypertensionMaternal hypertension PreeclampsiaPreeclampsia MultiparityMultiparity Previous abruptionPrevious abruption

Abruptio PlacentaeAbruptio Placentae Sudden vaginal bleeding in 3Sudden vaginal bleeding in 3rdrd trimester trimester
PainPain Abdomen may be tender or rigidAbdomen may be tender or rigid
May be minimal bleeding with shockMay be minimal bleeding with shock Most of hemorrhage may be hiddenMost of hemorrhage may be hidden
Contractions may be presentContractions may be present
If fetal heart tones absent, fetal death is likelyIf fetal heart tones absent, fetal death is likely

Placenta PreviaPlacenta Previa Placental implantation in lower uterine Placental implantation in lower uterine
segment, encroaching on or covering cervical segment, encroaching on or covering cervical osos
1 in 300 deliveries1 in 300 deliveries More common in preterm birthMore common in preterm birth
Painless, bright red bleedingPainless, bright red bleeding Increases if labor beginsIncreases if labor begins Fetal compromiseFetal compromise
Placenta PreviaPlacenta Previa More common with:More common with:
Increased maternal ageIncreased maternal age MultiparityMultiparity Previous cesarean sectionPrevious cesarean section Previous placenta previaPrevious placenta previa
.
Uterine RuptureUterine Rupture Spontaneous or traumatic rupture of uterine wallSpontaneous or traumatic rupture of uterine wall
CausesCauses Previous scar opensPrevious scar opens TraumaTrauma Prolonged or obstructed laborProlonged or obstructed labor
Rare but accounts for 5%-15% maternal deathsRare but accounts for 5%-15% maternal deaths 50% of fetal deaths50% of fetal deaths
Uterine RuptureUterine Rupture Sudden abdominal painSudden abdominal pain
““Tearing”Tearing”
Active laborActive labor
Early signs of shockEarly signs of shock
Vaginal bleedingVaginal bleeding May be hiddenMay be hidden
Management of 3Management of 3rdrd Trimester Bleeding Trimester Bleeding Prevent shockPrevent shock
Do not examine patient vaginallyDo not examine patient vaginally May increase bleeding and start laborMay increase bleeding and start labor
Emergency care Emergency care ABCsABCs Left lateral recumbent positionLeft lateral recumbent position Check fundal heightCheck fundal height
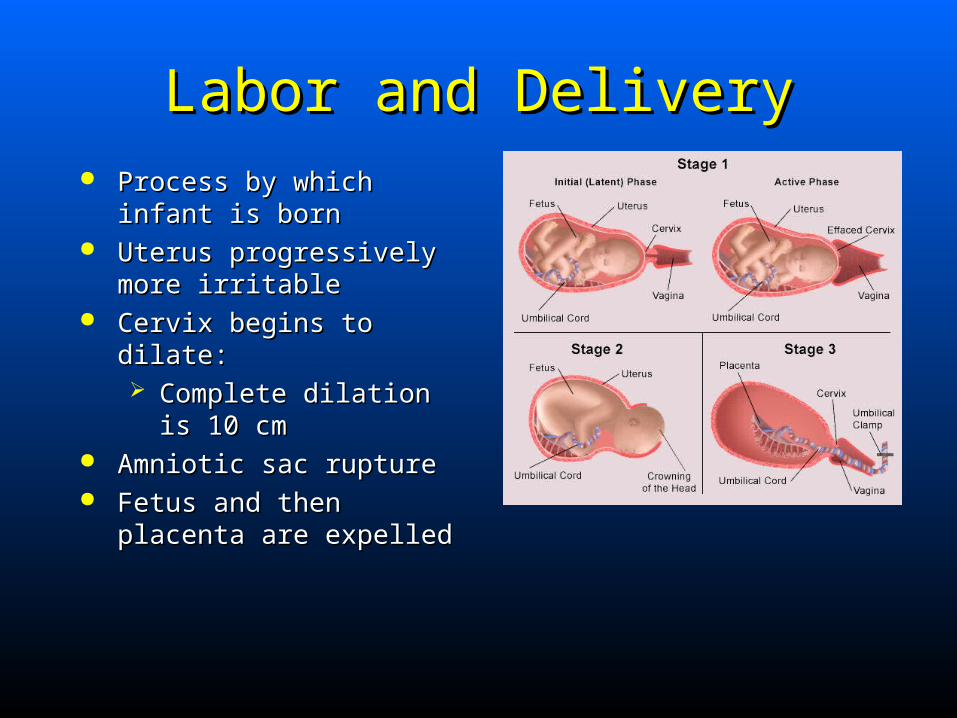
Labor and DeliveryLabor and Delivery Process by which infant is Process by which infant is
bornborn Uterus progressively more Uterus progressively more
irritableirritable Cervix begins to dilate:Cervix begins to dilate:
Complete dilation is 10 Complete dilation is 10 cmcm
Amniotic sac ruptureAmniotic sac rupture Fetus and then placenta are Fetus and then placenta are
expelledexpelled
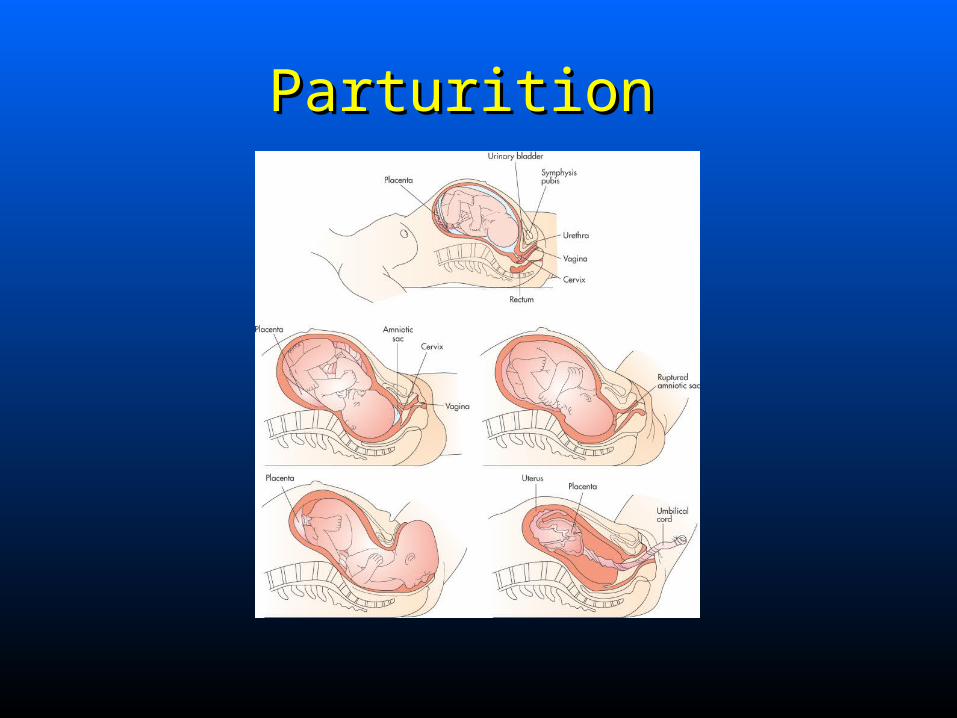
Parturition Parturition
Stages of LaborStages of Labor 11stst Stage: Stage: Onset of contractions Onset of contractions
to full dilation of to full dilation of cervix(10cm)cervix(10cm)
Usually 8-12hrs, prior Usually 8-12hrs, prior 6-8hrs6-8hrs
Amniotic sac usually Amniotic sac usually ruptures toward endruptures toward end
Stages of LaborStages of Labor
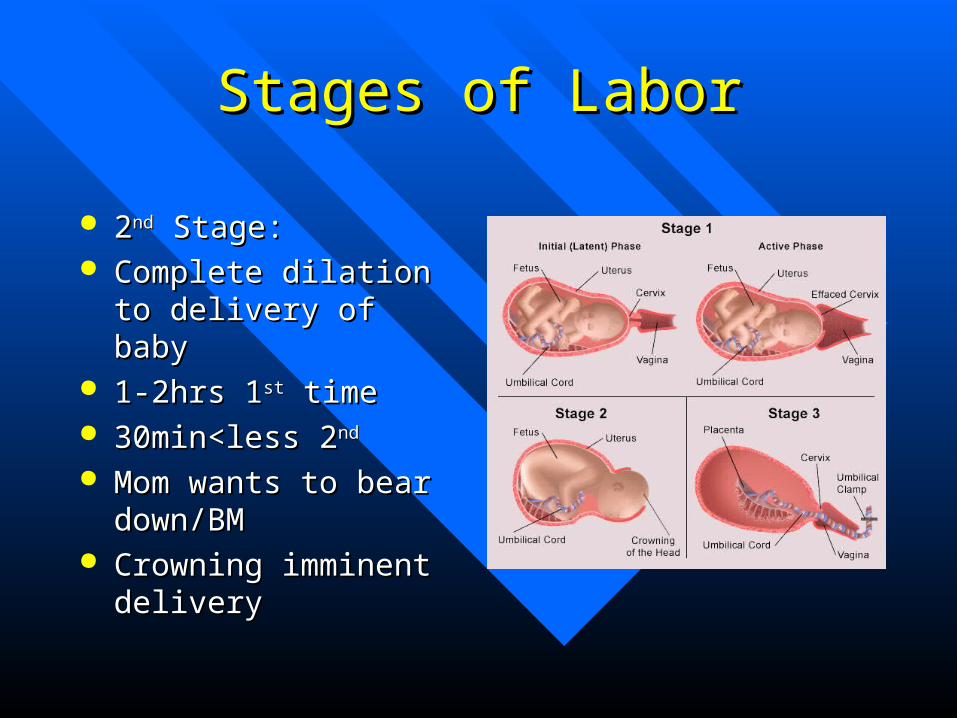
22ndnd Stage: Stage: Complete dilation to Complete dilation to
delivery of babydelivery of baby 1-2hrs 11-2hrs 1stst time time 30min<less 230min<less 2ndnd
Mom wants to bear Mom wants to bear down/BMdown/BM
Crowning imminent Crowning imminent deliverydelivery
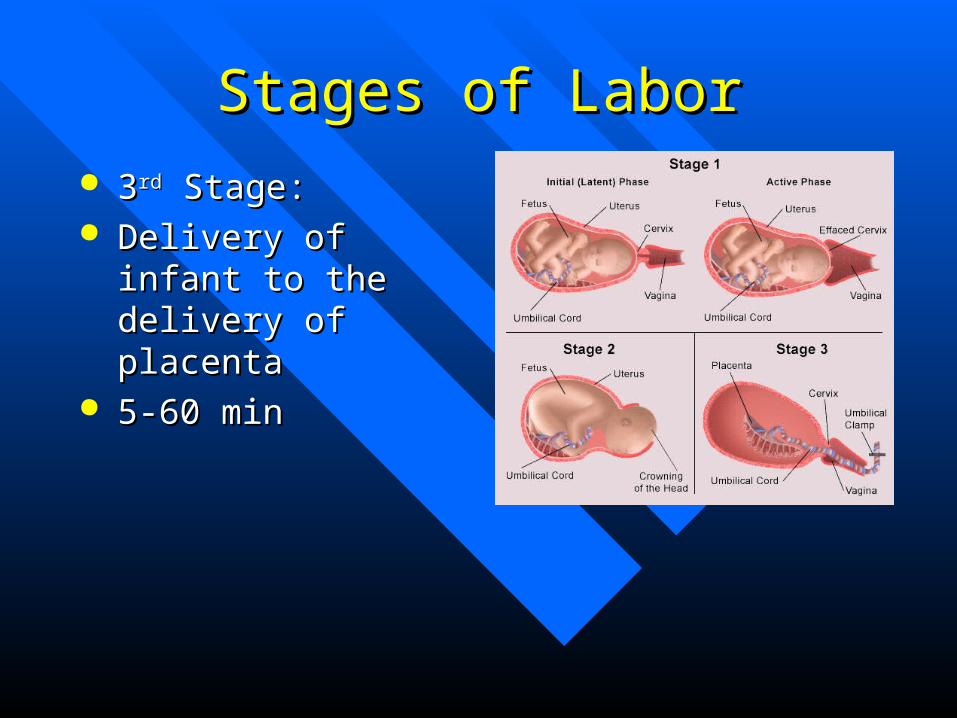
Stages of LaborStages of Labor 33rdrd Stage: Stage: Delivery of infant to Delivery of infant to
the delivery of the delivery of placentaplacenta
5-60 min5-60 min
Signs and Symptoms ofSigns and Symptoms ofImminent DeliveryImminent Delivery
Prepare for delivery if:Prepare for delivery if: Regular contractions lasting 45-60 sec at 1-2 min Regular contractions lasting 45-60 sec at 1-2 min
intervalsintervals Urge to bear down or sensation of bowel movementUrge to bear down or sensation of bowel movement Large amount of bloody showLarge amount of bloody show Crowning occursCrowning occurs Mother believes delivery is imminentMother believes delivery is imminent
Signs and Symptoms ofSigns and Symptoms ofImminent DeliveryImminent Delivery
Do not delay or restrain delivery except for cord Do not delay or restrain delivery except for cord presentationpresentation
If complications are anticipated or abnormal delivery If complications are anticipated or abnormal delivery occurs, medical direction may recommend expedited occurs, medical direction may recommend expedited transport to a medical facilitytransport to a medical facility
Preparing for deliveryPreparing for delivery
Delivery equipmentDelivery equipment
.
Prehospital Delivery EquipmentPrehospital Delivery Equipment
.
Assisting with DeliveryAssisting with Delivery Assist in natural events of childbirthAssist in natural events of childbirth
Responsibilities of EMS crew:Responsibilities of EMS crew: Prevent uncontrolled deliveryPrevent uncontrolled delivery Protect infant from cold stress after birthProtect infant from cold stress after birth
Assisting with a Normal DeliveryAssisting with a Normal Delivery
Delivery procedureDelivery procedure
Evaluating infantEvaluating infant
Cutting umbilical cordCutting umbilical cord
Delivery of placentaDelivery of placenta
Fundal massage to promote uterine contractionFundal massage to promote uterine contraction
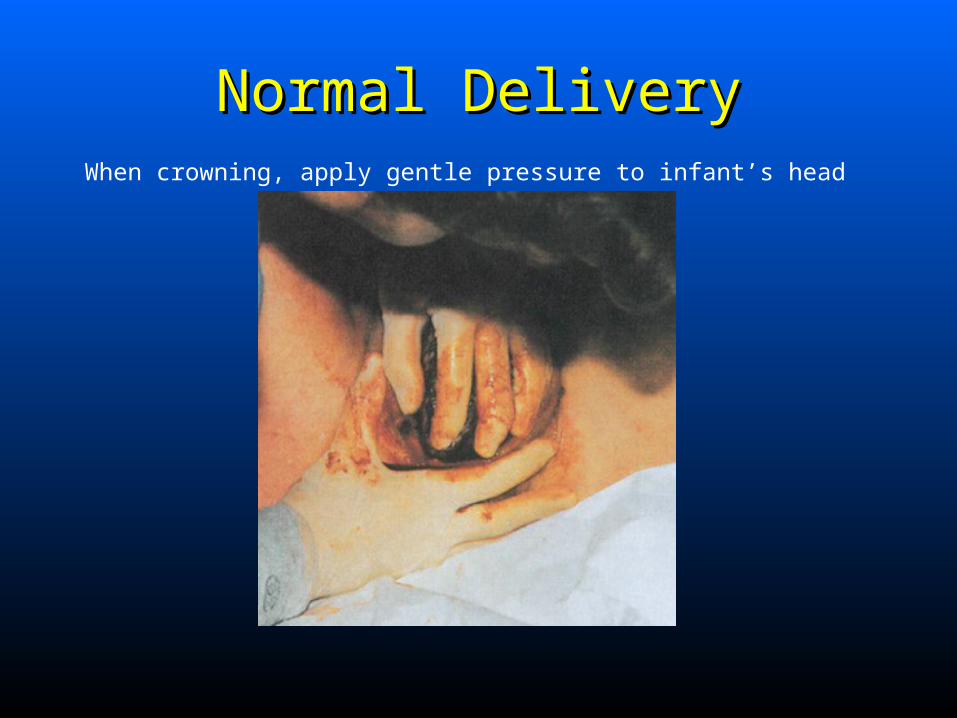
Normal DeliveryNormal DeliveryWhen crowning, apply gentle pressure to infant’s head
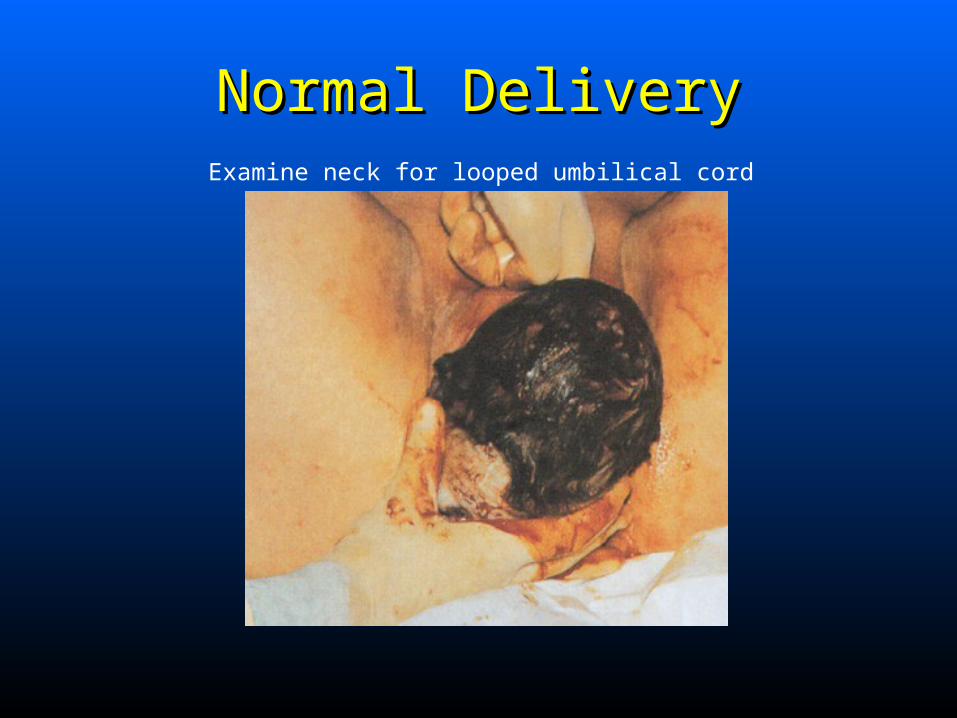
Normal DeliveryNormal DeliveryExamine neck for looped umbilical cord
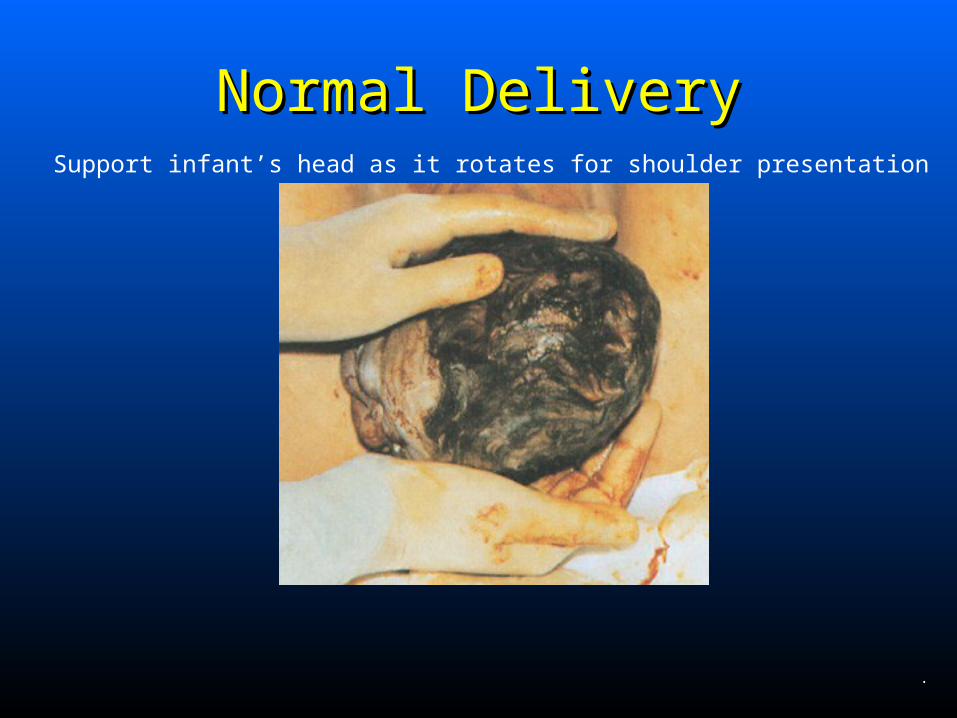
Normal DeliveryNormal DeliverySupport infant’s head as it rotates for shoulder presentation
.
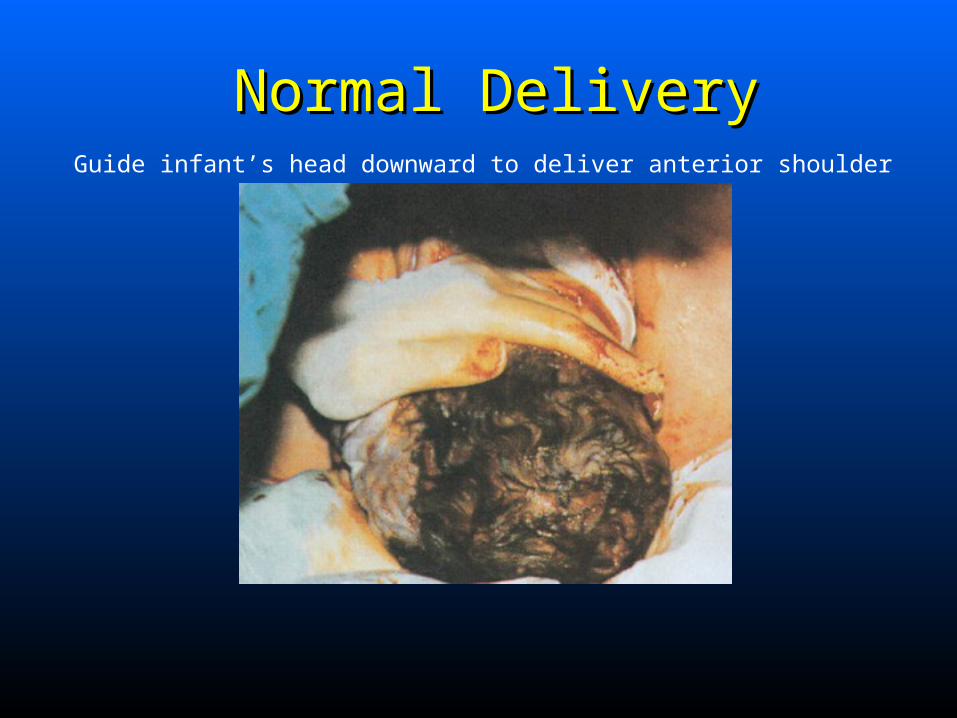
Normal DeliveryNormal DeliveryGuide infant’s head downward to deliver anterior shoulder
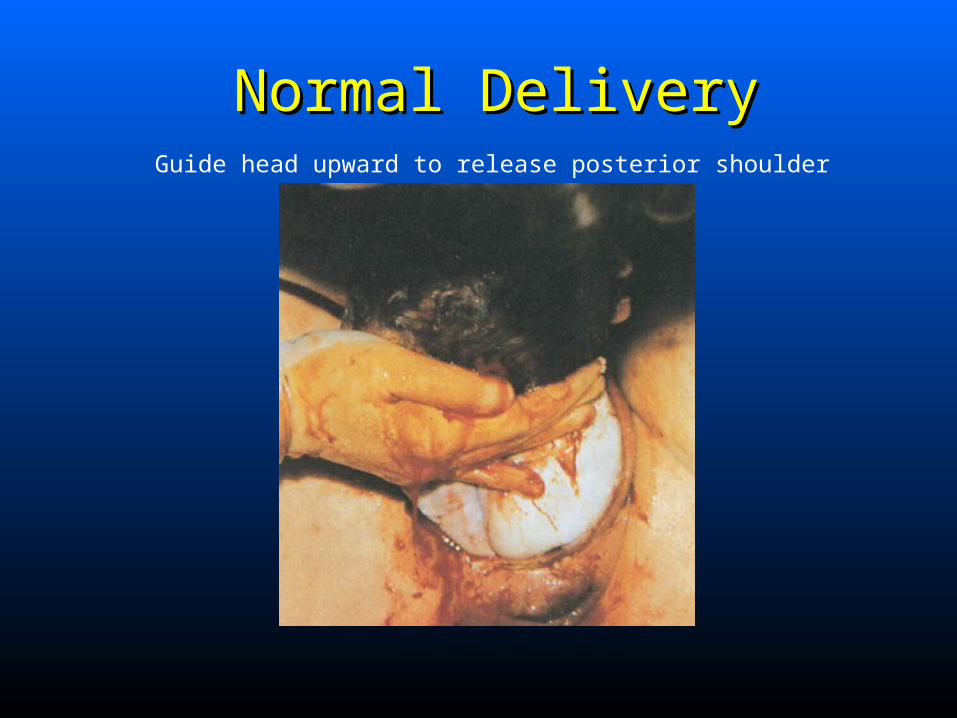
Normal DeliveryNormal DeliveryGuide head upward to release posterior shoulder
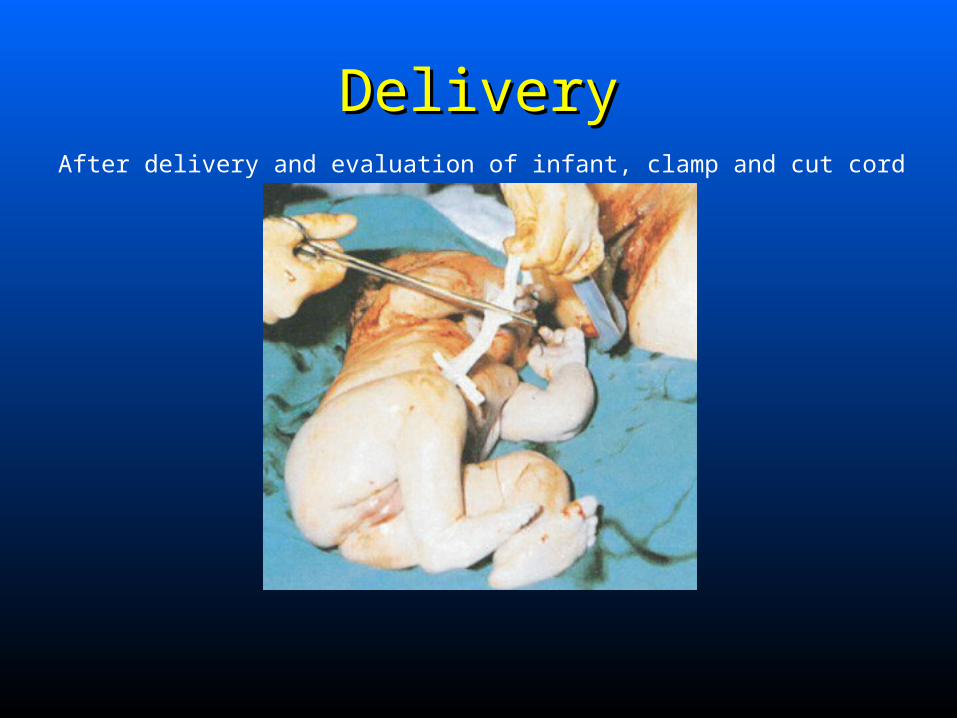
DeliveryDeliveryAfter delivery and evaluation of infant, clamp and cut cord
Postpartum HemorrhagePostpartum Hemorrhage >500 mL of blood loss after delivery >500 mL of blood loss after delivery
Immediate or delayed 24 hrsImmediate or delayed 24 hrs
Risk factorsRisk factors Uterine atony from laborUterine atony from labor Grand multiparityGrand multiparity TwinsTwins Placenta previaPlacenta previa Full bladderFull bladder
.
Postpartum HemorrhagePostpartum Hemorrhage Control external hemorrhageControl external hemorrhage
Massage uterusMassage uterus
Encourage infant to breast feedEncourage infant to breast feed
Administer oxytocinAdminister oxytocin
Don’t attempt vaginal examDon’t attempt vaginal exam
Rapid transportRapid transport
Delivery ComplicationsDelivery Complications Maternal factorsMaternal factors
AgeAge No prenatal careNo prenatal care LifestyleLifestyle Preexisting illnessPreexisting illness Previous OB historyPrevious OB history Intrapartum disordersIntrapartum disorders
Delivery ComplicationsDelivery Complications Fetal factorsFetal factors
Lack of fetal well-beingLack of fetal well-being Decreased fetal movementDecreased fetal movement History of heart rate abnormalitiesHistory of heart rate abnormalities Fetal immaturityFetal immaturity Fetal growthFetal growth
Cephalopelvic Disproportion Cephalopelvic Disproportion Difficult labor because of:Difficult labor because of:
Small pelvisSmall pelvis Oversized fetusOversized fetus Fetal abnormalitiesFetal abnormalities
• Hydrocephalus, conjoined twins, fetal tumorsHydrocephalus, conjoined twins, fetal tumors
Often primigravida experiencing strong, frequent Often primigravida experiencing strong, frequent contractions for long periodcontractions for long period

Cephalopelvic Disproportion Cephalopelvic Disproportion Prehospital carePrehospital care
Maternal oxygen administrationMaternal oxygen administration IV access for fluid resuscitation if neededIV access for fluid resuscitation if needed Rapid transport to receiving hospitalRapid transport to receiving hospital
Abnormal PresentationAbnormal Presentation Most infants born head firstMost infants born head first
Cephalic or vertex presentationCephalic or vertex presentation Rarely abnormal presentationRarely abnormal presentation
Breech presentationBreech presentation ManagementManagement
Shoulder dystociaShoulder dystocia ManagementManagement
Shoulder presentation (transverse presentation)Shoulder presentation (transverse presentation) ManagementManagement
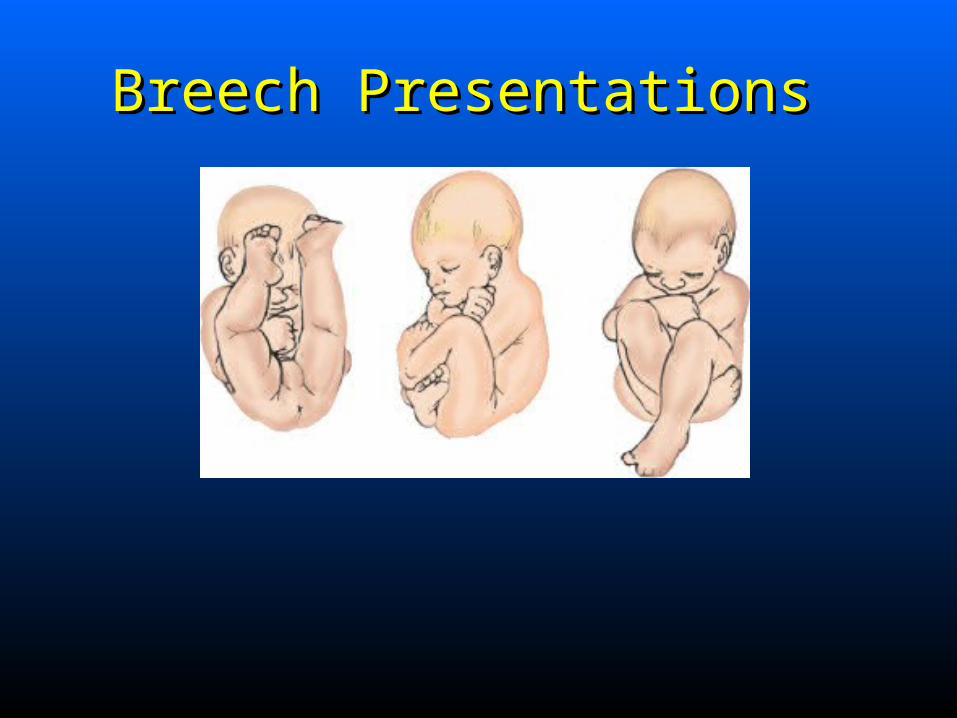
Breech Presentations Breech Presentations
Abnormal PresentationAbnormal Presentation Cord presentation (prolapsed cord)Cord presentation (prolapsed cord)
Elevate mother’s hipsElevate mother’s hips Maternal oxygenMaternal oxygen Have mother pant with contractionsHave mother pant with contractions Apply moist, sterile dressing to cordApply moist, sterile dressing to cord Gently push infant back into vaginaGently push infant back into vagina
• Elevate presenting partElevate presenting part
• Maintain during transportMaintain during transport
Other Abnormal PresentationsOther Abnormal Presentations Face or browFace or brow
Occiput posterior presentationOcciput posterior presentation Face upFace up
Increased perinatal morbidity and mortalityIncreased perinatal morbidity and mortality
Early recognition criticalEarly recognition critical
Abnormal PresentationAbnormal Presentation Prehospital managementPrehospital management
Recognition of potential complicationsRecognition of potential complications Maternal support and reassuranceMaternal support and reassurance Rapid transport for definitive careRapid transport for definitive care

Premature Birth Premature Birth Birth at <37 weeks of gestationBirth at <37 weeks of gestation
Care of premature infantCare of premature infant Keep warmKeep warm Suction mouth and nares oftenSuction mouth and nares often Monitor cord for oozingMonitor cord for oozing Administer oxygenAdminister oxygen
• Monitor for need to assist ventilationsMonitor for need to assist ventilations Gently transportGently transport
Multiple GestationMultiple Gestation More than one fetusMore than one fetus
Associated complicationsAssociated complications Premature labor and deliveryPremature labor and delivery Premature rupture of membranesPremature rupture of membranes Abruptio placentaeAbruptio placentae Postpartum hemorrhagePostpartum hemorrhage Abnormal presentationAbnormal presentation
Delivery procedureDelivery procedure
Multiple GestationMultiple Gestation Delivery procedureDelivery procedure
Deliver first twin as normal birthDeliver first twin as normal birth Cut and clamp cordCut and clamp cord Second twin delivery within 30-45 minSecond twin delivery within 30-45 min
• Medical direction may recommend transportMedical direction may recommend transport
Keep warmKeep warm Monitor for severe postpartum hemorrhageMonitor for severe postpartum hemorrhage
.
Precipitous DeliveryPrecipitous Delivery Rapid spontaneous deliveryRapid spontaneous delivery
Less than 3 hrs from onset of labor to birthLess than 3 hrs from onset of labor to birth
Overactive uterine contractions and little Overactive uterine contractions and little maternal soft tissue or bony resistancematernal soft tissue or bony resistance
Apply gentle counterpressure to headApply gentle counterpressure to head
Uterine InversionUterine Inversion Rare serious complication of childbirthRare serious complication of childbirth
Uterus turns inside outUterus turns inside out After contraction, sneezing, coughingAfter contraction, sneezing, coughing IatrogenicIatrogenic
Signs and symptomsSigns and symptoms Profuse postpartum hemorrhageProfuse postpartum hemorrhage Severe lower abdominal painSevere lower abdominal pain
Uterine InversionUterine Inversion ManagementManagement
Position patient supinePosition patient supine Push fundus up through cervical canal orPush fundus up through cervical canal or Cover with moist sterile dressingsCover with moist sterile dressings Rapid transportRapid transport Medical direction may advise use of analgesicsMedical direction may advise use of analgesics
Pulmonary EmbolismPulmonary Embolism Pregnancy, labor, or postpartum periodPregnancy, labor, or postpartum period
Common cause of maternal deathCommon cause of maternal death
Often blood clot from pelvisOften blood clot from pelvis
More common with cesarean deliveryMore common with cesarean delivery
Pulmonary EmbolismPulmonary Embolism Signs and symptomsSigns and symptoms
DyspneaDyspnea Sharp chest paiinSharp chest paiin Tachycardia, tachypneaTachycardia, tachypnea Hypotension possibleHypotension possible
ManagementManagement ABCsABCs ECG and IVECG and IV TransportTransport
Fetal Membrane Disorders Fetal Membrane Disorders Premature rupture of membranesPremature rupture of membranes
Amniotic sac rupture before laborAmniotic sac rupture before labor ““Trickle” or sudden gush of fluid from vaginaTrickle” or sudden gush of fluid from vagina Infection possible if delivery delayedInfection possible if delivery delayed Transport Transport
Fetal Membrane Disorders Fetal Membrane Disorders Amniotic fluid embolismAmniotic fluid embolism
Amniotic fluid gains access to maternal circulation:Amniotic fluid gains access to maternal circulation:• During labor or deliveryDuring labor or delivery• Immediately after deliveryImmediately after delivery
Signs and symptomsSigns and symptoms Same as for pulmonary embolismSame as for pulmonary embolism High mortality High mortality
ManagementManagement As for pulmonary embolismAs for pulmonary embolism
ConclusionConclusionObstetrical emergencies can develop Obstetrical emergencies can develop
suddenly and become life threatening. The suddenly and become life threatening. The paramedic must be prepared to recognize paramedic must be prepared to recognize
and manage these events.and manage these events.

Questions?Questions?