on school based health care at fairview elementary school
TRANSCRIPT
From Paper to Policy: On Proposing School-Based Health Care at Fairview Elementary School
A Needs Assessment Featuring the PRECEDE/PROCEED Model
CATHOLIC CHARITIES BLOOMINGTON & INDIANA UNIVERSITY SCHOOL OF PUBLIC HEALTH
Spring 2015
Authored by: Julius Lee

Spring 2015 From Paper to Policy
1

Spring 2015 From Paper to Policy
2
TABLE OF CONTENTS
EXECUTIVE SUMMARY 4
PRECEDE/PROCEED MODEL 5
PRECEDE
PHASE 1: SOCIAL ASSESSMENT 6-8
PHASE 2: EPIDEMIOLOGICAL, BEHAVIORAL,
AND ENVIRONMENTAL ASSESSMENT 9-12
PHASE 3: EDUCATIONAL AND ECOLOGICAL ASSESSMENT 13-16
PHASE 4: ADMINISTRATIVE AND POLICY ASSESSMENT
AND INTERVENTION ALIGNMENT 17-23
Spring 2015 From Paper to Policy
3
TABLE OF CONTENTS
PROCEED
PHASE 5: IMPLEMENTATION 24-32
PHASE 6: PROCESS EVALUATION 33-35
PHASE 7: IMPACT EVALUATION 35-36
PHASE 8: OUTCOME EVALUATION 36-37
CONFOUNDING ISSUES/VARIABLES 38-39
BIBLIOGRAPHY 40-44

Spring 2015 From Paper to Policy
4
APPENDICES 45
APPENDIX A: GEOGRAPHICAL MAPS
FAIRVIEW GEOGRAPHICAL GRID
MONROE COUNTY COMMUNITY SCHOOL CORPORATION FEEDER SCHOOLS FLOW CHART
BLOOMINGTON TOWNSHIP EDUCATIONAL AND CULTURAL ASSETS
BLOOMINGTON TOWNSHIP TRANSPORTATION ASSETS
BLOOMINGTON TOWNSHIP FOOD AND GAS FACILITIES
BLOOMINGTON TOWNSHIP PARKS AND RECREATIONAL ASSETS
APPENDIX B: GRANTS AND FUNDING OPPORTUNITIES
PERSONAL RESPONSIBILITY EDUCATION PROGRAM (PREP) COMPETITIVE GRANTS UNDER
THE AFFORDABLE CARE ACT
AFFORDABLE CARE ACT (ACA) GRANTS FOR SCHOOL-BASED HEALTH CENTER CAPITAL
EXPENDITURES
USDA TEAM NUTRITION TRAINING GRANTS
HEALTHY TOMORROWS PARTNERSHIP FOR CHILDREN PROGRAM
MONROE COUNTY HEALTH DEPARTMENT
CITY OF BLOOMINGTON, INDIANA HOUSING AND NEIGHBORHOOD DEVELOPMENT
DEPARTMENT: COMMUNITY DEVELOPMENT BLOCK GRANT (CDBG)
INDIANA HOUSING AND COMMUNITY DEVELOPMENT AUTHORITY: NEIGHBORHOOD
ASSISTANCE PROGRAM
FUNDS FOR SUPPORT FOR EXPECTANT AND PARENTING TEENS, WOMEN, FATHERS AND THEIR
FAMILIES
JACK HOPKINS SOCIAL SERVICES FUNDING COMMITTEE
TITLE V MATERNAL AND CHILD HEALTH SERVICES BLOCK GRANT PROGRAM
MATERNAL AND CHILD HEALTH PUBLIC HEALTH CATALYST PROGRAM
R40 MATERNAL AND CHILD HEALTH RESEARCH PROGRAM (MCHR)
COMMUNITY ACCESS TO CHILD HEALTH (CATCH) PLANNING GRANTS
NATIONAL INSTITUTE OF HEALTH (NIH) RESEARCH GRANT PROGRAM (PARENT R03)
COMMUNITY FOUNDATION
o PRECISION HEALTH NETWORK FUNDING INITIATIVE
o COMMUNITY IMPACT FUNDING INITIATIVE
o MATCHSTICK
PARTNERSHIPS WITH STATE MEDICAID AND CHILDREN’S HEALTH INSURANCE
PROGRAM (CHIP)
APPENDIX C: SUPPLEMENTAL RESEARCH: ON SCHOOL-BASED HEALTH CARE AT A LOCAL TITLE I
ELEMENTARY SCHOOL—A FEASIBILITY STUDY

Spring 2015 From Paper to Policy
5
Executive Summary
For the third consecutive year, students at Fairview Elementary School have failed the
Indiana State Test of Educational Progress, a benchmark exam mandated by the department of
Education to measure their reading, writing, comprehension, and mathematical skills. Upon
revealing the test scores last year, the Fairview community met to define and discuss why the
children are faltering the exam. Suggestions such as afterschool tutoring, mental health services,
and a revamp of the Coordinated School Health Program were implemented, but it is too soon to
evaluate their success.
Catholic Charities Bloomington and the Indiana University School of Public Health
proposes the Fairview Health Care Center, a School-Based Health Care (SBHC) that would
provide on-site acute and preventive care to children and their families. Based on prior research
found in the supplementary section, students who attend a school with a SBHC have reported a
greater rapport with their teachers, reduced absenteeism, and stronger academic achievement as
compared to schools without said facility.
This Needs-Based Assessment maximizes the PRECEDE/PROCEED Model to identify
the social, ecological, and epidemiological factors affecting the students, supportive policy on
their behalf, and our premise on why the facility should be available to this vulnerable
population. Supplemental information includes geographical descriptions of boundaries,
community assets or social capital, funding opportunities, and a Feasibility Study conducted
prior to this assessment.
Spring 2015 From Paper to Policy
6
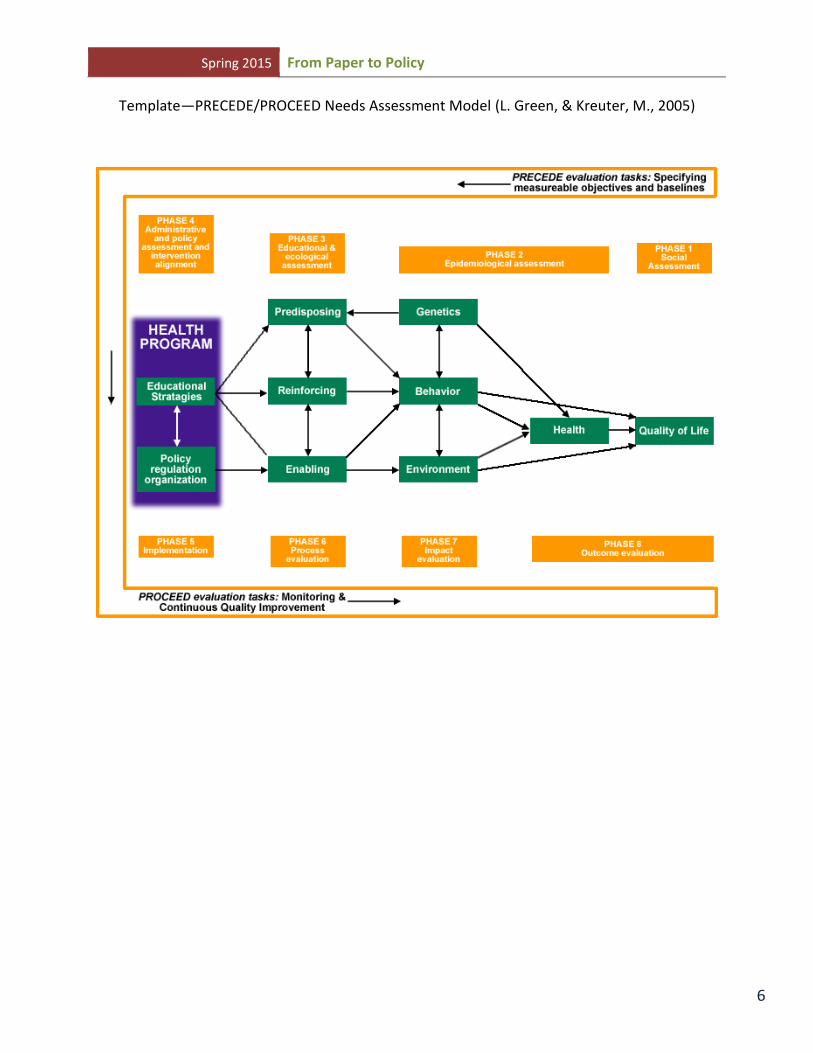
Template—PRECEDE/PROCEED Needs Assessment Model (L. Green, & Kreuter, M., 2005)

Spring 2015 From Paper to Policy
7
PRECEDE
Phase 1: Social Assessment
For the third consecutive year, Fairview Elementary School’s students have faltered on
their mandated exams by the Indiana Department of Education (IDOE) and consequently earned
an F as an accountability grade. This is in accordance with the House Enrolled Act 1750 which
produced Public Law 221 (PL221). To measure progress, P.L. 221 places Indiana schools into
one of the five categories based upon student performance and improvement data from the state’s
ISTEP+ assessments in Grades 3-8 and End Course Assessments in Algebra I and English 10(I.
D. o. Education, 2011). The five categories correspond with the letters A through F, with the
following descriptions:
A (Exemplary Progress)
B (Commendable Progress
C (Academic Progress)
D (Academic Watch)
F (Academic Probation—High Priority) (I. D. o. Education, 2011)
Schools in the lowest P.L. 221 category (Academic Probation) face a series of interventions
that are designed to provide the additional support needed to improve student achievement.
These consequences become more serious the longer schools remain in the bottom category(I. D.
o. Education, 2011).

Spring 2015 From Paper to Policy
8
Similarly, federal school accountability, known as Adequate Yearly Progress (AYP), was
first established in 2001 with the passage of the federal No Child Left Behind (NCLB) Act(I. f.
Q. o. Education, 2013). Although the NCLB has expired in 2007, the Indiana House of
Representatives are now implementing legislation to take over schools suffering from six
consecutive years of academic failure to four. This bill contains two major components:
Accelerate school takeover by “special management teams” through contracts with the
State Board.
Creates transformation zones—a model currently used in Evansville and IPS
(Indianapolis Public Schools) that allows outside entities to operate schools
(Association, 2015)
Concern has not been raised on the personal health of each student, whether their
socioeconomic conditions enable or inhibit their health, thereby adversely affecting their
academic achievement. Given that an estimated 88% of students qualify for free or reduced
lunch, students qualify for Healthy Indiana Plan- also known as Medicaid. Study after study
shows that they are more likely to report poor health, to see doctors less often (even when they
are sick), to go without preventive care, and to turn to emergency room when in need of
treatment(J. F. McKenzie, Pinger, R.R., & Kotecki, J.E., 2012). Apparently, school health is a
complex issue plagued by lack of resources, ambiguity of who should be in charge of children’s
health (community vs school) and ultimately who should pay for school health efforts(L. M.
Vaughn, Jacquez, F., Zhao, J., & Lang, M., 2011). Questions should be raised if an onsite
preventive health care facility, known as School Based Health Care (SBHC), would improve the
health status of children. For example, if acute care is required, what are the parent’s preferences

Spring 2015 From Paper to Policy
9
in terms of healthcare services for their child? Should a SBHC be operated beyond the academic
school year? What funding is available for an SBHC? These concerns should be addressed to
implementing a school-based healthcare facility at Fairview, because it could positively affect
the academic outcomes and health behaviors of the students, thereby improving their success rate
in passing state mandated exams. Further, it could improve their overall quality of life.
Catholic Charities Bloomington and the Indiana University School of Public Health will
facilitate a needs assessment to evaluate the health of Fairview students. A needs assessment is
used to create and promote change by engaging the community to identify priorities, to use and
build on strength already present, and to give power to the community participants (Hancock,
2008; L. M. Vaughn, Jacquez, F., Zhao, J., & Lang, M., 2011). Furthermore, involving
community members to explore the meaning and reason for change can lead to increased
commitment and ownership in the action for change (Hobbs, 1987; L. M. Vaughn, Jacquez, F.,
Zhao, J., & Lang, M., 2011). The goal of this PRECEDE/PROCEED needs assessment is to
facilitate a school-based healthcare program that maximizes local and state resources for
preventive and/or urgent care onsite during the academic school year.
Spring 2015 From Paper to Policy
10
Phase 2: Epidemiological, Behavioral, and Environmental
Assessment
In 2014, Bloomington ranks 8th
in the state in terms of health outcomes, quality and
length of life. (R. W. J. Foundation, 2014) An estimated 88% has graduated from high school,
while 78% of the populations have completed some college. There is an estimated 20% of
children living in poverty and 31% in single-parent households. 13% of the population became
pregnant during their teens, and 7.1% are reported as low birth rate. Although 18% were reported
as uninsured in 2014, Indiana has recently expanded Medicaid to cover the adults who cannot
qualify for Universal health coverage.
In 2010, census data reports there were 141,210 citizens in Bloomington,, Indiana(U. C.
Bureau, 2009). The majority of the population is comprised of Caucasian American Non-
Hispanic (87.8%), with Asians (6.0%), African American Non-Hispanic (3.5%),and persons of
Latino or Hispanic Origin (3.2%) composing much of the rest of the population. American-
Indian and Alaska Native persons comprised of 0.3% of Monroe County(U. S. C. Bureau, 2013).
Indiana Health Indicators from 2011 indicated the infant mortality rate for Bloomington,
Indiana is 5.5 per 1,000 live births. Teen births, ages 15 to 19 years is estimated as 14.9 per
1,000 females, while premature births are 9.6 per 1,000 females. These infants are characterized
as babies who were born premature before 37 weeks gestation. Low birth weight is characterized
as newborns born weighing 5.5 lbs or less, and Bloomington’s rate is 7.4 per 1,000 live births.
Additionally, mothers who smoke during pregnancy is rated at 15.3 per 1,000 live births(Health,
2011).
Spring 2015 From Paper to Policy
11
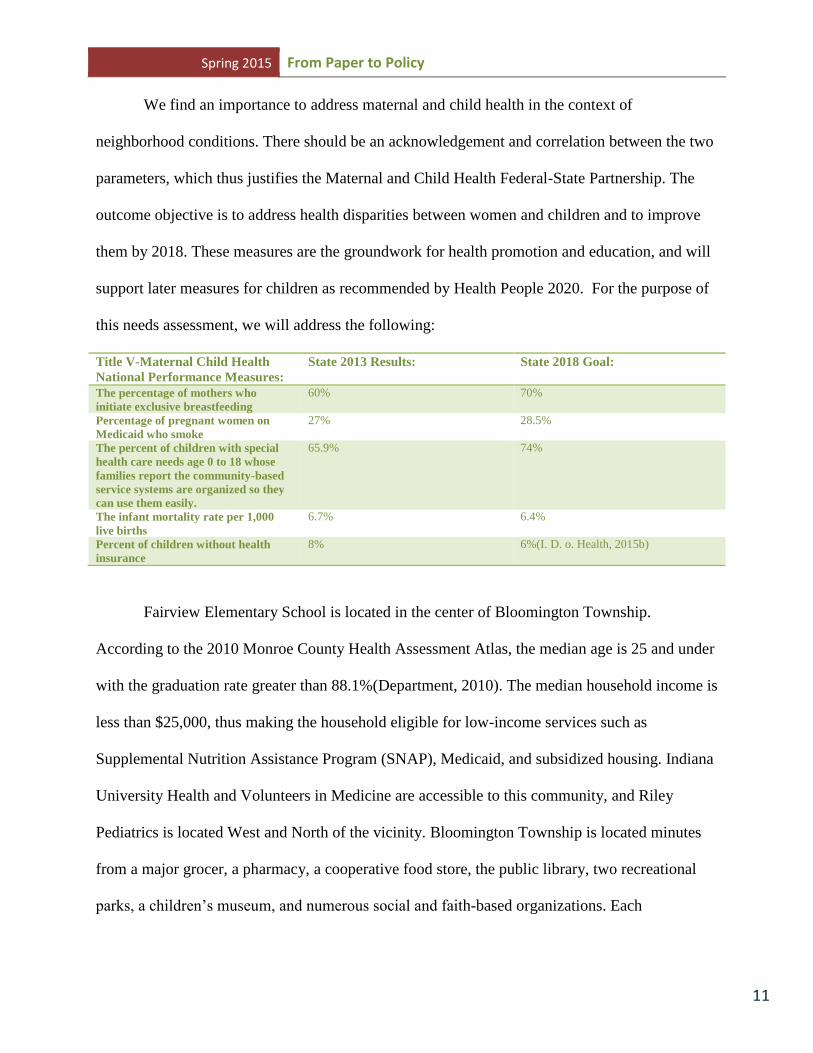
We find an importance to address maternal and child health in the context of
neighborhood conditions. There should be an acknowledgement and correlation between the two
parameters, which thus justifies the Maternal and Child Health Federal-State Partnership. The
outcome objective is to address health disparities between women and children and to improve
them by 2018. These measures are the groundwork for health promotion and education, and will
support later measures for children as recommended by Health People 2020. For the purpose of
this needs assessment, we will address the following:
Title V-Maternal Child Health
National Performance Measures:
State 2013 Results: State 2018 Goal:
The percentage of mothers who
initiate exclusive breastfeeding
60% 70%
Percentage of pregnant women on
Medicaid who smoke
27% 28.5%
The percent of children with special
health care needs age 0 to 18 whose
families report the community-based
service systems are organized so they
can use them easily.
65.9% 74%
The infant mortality rate per 1,000
live births
6.7% 6.4%
Percent of children without health
insurance
8% 6%(I. D. o. Health, 2015b)
Fairview Elementary School is located in the center of Bloomington Township.
According to the 2010 Monroe County Health Assessment Atlas, the median age is 25 and under
with the graduation rate greater than 88.1%(Department, 2010). The median household income is
less than $25,000, thus making the household eligible for low-income services such as
Supplemental Nutrition Assistance Program (SNAP), Medicaid, and subsidized housing. Indiana
University Health and Volunteers in Medicine are accessible to this community, and Riley
Pediatrics is located West and North of the vicinity. Bloomington Township is located minutes
from a major grocer, a pharmacy, a cooperative food store, the public library, two recreational
parks, a children’s museum, and numerous social and faith-based organizations. Each

Spring 2015 From Paper to Policy
12
Wednesday, the public library’s Bookmobile visits the Crestmont community (part of
Bloomington township) from 4:45-5:30. From March through November, the Farmer’s Market
operates every Saturday at City Hall; here, patrons can purchase fresh fruits and vegetables,
eggs, poultry and other items using cash or their SNAP Card. A point-of-sale (POS) machine
exchanges the participant’s monetary value for tokens which allows them to make a purchase.
Additionally, the Community Garden project is North of the campus where participants can
purchase a plot for a nominal fee. The Bloomington “B-line” walking trail also connects most of
these facilities running North to South of the community. Bloomington and Rural Transit bus
services operate throughout the community Monday through Saturday. Finally, Ivy Tech
Community College and Indiana University are both accessible to residents in this community.
At Fairview Elementary School, the 2013-14 academic year indicated a total enrollment
of 385 students; with 183 females and 202 males enrolled from the Head start Program to Grade
Six. Overall, 253 are White or Caucasian, 56 are African American Non-Hispanic, 24 are
Hispanic, 3 are Asian, and 1 is American Indian. There are 48 students who list themselves as
multiracial. Out of this population, 316 are eligible for free lunch and 23 qualify for a reduced
lunch(I. D. o. Education, 2015). For three consecutive years, their attendance rate has remained
constant at an estimated 94%, a slight increase from 93% during the 2010-11 academic year.(I.
D. o. Education, 2014d). Currently, as part of their improvement plan, their student faculty ratio
is 1:17 in Kindergarten and first grade, 1:20 in second grade, and 1:22 in grades three through
six(Lane, 2015).
Onsite, students receive healthcare provided by a nurse and licensed psychologist.
According to the Monroe County Community School Corporation (2015), School nursing
interventions with students who have acute and/or chronic health concerns improve student

Spring 2015 From Paper to Policy
13
health and provide a positive impact on school achievement and success. School nurses assist
students to develop the skills necessary for successful self-management. School nurses provide
health promotion, disease prevention education and activities for students, staff and families.
While supporting goals to maintain optimal health and encouraging attitudes conducive to
lifelong positive health practices, school nurses effectively impact the community as a
whole(Schilling, 2015).
The school nurse and psychologist are part of the coordinated school health program
(CSHP), which is an organized set of policies, procedures, and activities designed to protect,
promote, and improve the health and well-being of students and staff, thus improving a student’s
ability to learn(J. F. McKenzie, Pinger, R.R., & Kotecki , J.E., 2012). Despite the CSHP,
students are faltering the Indiana Test for Educational Progress (ISTEP). ISTEP test scores from
2014 indicate failure for Fairview students from grades three through six. The following table
illustrates the number that passed and failed the English Language Acquisition (ELA) and the
Math portion of the state exam, and the total number of students per grade level(I. D. o.
Education, 2014c).

Spring 2015 From Paper to Policy
14
Grade ELA Pass
N=
ELA
Percent
Pass
Math Pass
N=
Math
Percent
Pass
Both Math
and ELA
Percent
Pass
Total
Number of
Students
Per Grade
Level
3 29 63.0% 26 55.3% 54.3% 58
4 20 51.3% 18 45.0% 35.9% 42
5 12 46.2% 15 57.7% 40.0% 31
6 26 56.5% 32 63.6% 45.7% 51

Spring 2015 From Paper to Policy
15
Phase 3: Educational and Ecological Assessment
Eighty-eight percent of Bloomington students graduate with a high school diploma or
equivalent. Students who continuously attend Fairview progress to Tri-North, Bloomington High
School North, or alternate schools such as the Academy of Science and Entrepreneurship, or the
Bloomington Graduate School. Conversely, twelve percent of Bloomington’s students are not
graduating from high school. Questions should be raised to address predisposing factors that
inhibits their achievement.
The personal health of each student and their family’s Socioeconomic Status (SES) may
affect their academic capabilities; in particular, they may experience illness more than their
counterparts. SES is important to health at all levels of status an in general, the more advantage
individuals are, the better their health, and the more disadvantaged individuals are, the greater
their chances of increased morbidity and mortality(Alder, 1997; Kidder, 2007; Sanders
Thompson, 2012; Zlotnick, 2009).
Maladaptive neurological development may affect children’s cognitive development—
specifically their ability to read. Reading Disability (RD) is a brain-based developmental
disorder associated with deficits in phonological processing, especially phonological awareness,
the metalinguistic understanding that spoken words are made of smaller units(Bradley, 1978;
Lyon, 2003; Pugh, 2014; Snowling, 1981). In a research study with 75 children ages six through
ten, the Yale University Reading Center examined the effects of various tests on a child’s neuro-
metabolites. This study examines neurochemistry early in the process of learning to read, which
is critical for understanding the functional significance of neuro-metabolite-reading
relations(Pugh, 2014).Through the use of several tests and Magnetic Resonance Spectroscopy,
they found a correlation between neutron-metabolites and reading performance. Analyses

Spring 2015 From Paper to Policy
16
showed that Cho and Glu concentrations were inversely correlated with reading and related
linguistic measures such that high concentrations were associated with poorer
performance(Pugh, 2014). Generally, this pre-disposing factor may justify the faltering of the
ISTEP exam among Fairview students.
Whereupon it was learned that 70 percent of Fairview’s student were not reading at grade
level, the school administration decided to take steps to help move the school forward(Murray,
2014b). Last year, the Herbert Presidential Scholars facilitated a literacy program to improve the
children’s reading capabilities. According to the Indiana Daily Student, the students who will
participate in the program are ones the Fairview community believes will benefit from the
program the most..” (Murray, 2014a)
Abby Englert, coordinator for the Herbert Scholars, says Indiana University students
volunteer for ten weeks to work selected students. The students are taught reading pedagogy
from an instructor, then works closely with an estimated 22% of the student body four days. The
Herbert Presidential Scholars collaborates with Cox Scholars, and the Banneker Center to
provide assistance after school and four days a week. Students are arranged in a classroom by
grade level, with fifth and six grade students working together. Given the pending acquisition of
Fairview by the state government, Abby says that mathematics is also included in tutorial
services. She added that if the acquisition happens, her hope is to continue the program as a
means to providing academic improvement.
Abby mentions that sometimes the children need help beyond the academic ambits, and
will converse with the students on personal matters that are occasionally intervened by the social
worker. Hearing this suggest a need for health services that enables the children to address and
resolve their problems. In doing so, the children are enabled to focus on their academics.

Spring 2015 From Paper to Policy
17
Although a social worker and psychologist are available on-site, Abby says that the children
connect with the mentors—perhaps feeling comfortable to disclose their problems. Abby says as
children, the mentors have also faced adversity and can empathize with their mentees.
Presumably, the Fairview Literacy Program’s mentors are both a reinforcing factor in terms of
moral support and education, and likewise aiding the children in becoming resilient.
Resilience can be categorized among education and health; educational resilience has
been defined as “the heightened likelihood of success in school and other life accomplishments
despite environmental adversities brought about by early traits, conditions, and
experiences(Reiss, 2005; J. E. Richardson, 2008). Considering health, resilience is a function of
culturally sensitive, integrated structural and programmatic processes for children(Mykota, 2005;
J. E. Richardson, 2008). Whereas the Fairview Literacy Program directs their efforts towards
educational resilience, Catholic Charities Bloomington strives to improve their mental health.
Last year, Catholic Charities was concerned with the mental stability of the students
following the news of their faltering on the ISTEP. According to Marsha McCartney, the
partnership between Fairview and Catholic Charities is we (Catholic Charities) have seen
children at Fairview for a number of years. She says:
We’ve had a relationship with Fairview in that way; and two of our employees were at
Fairview. I’m unsure who talked with us, but initially, Tammy Miller (then Interim
Principal) suggested how great it would be to have services at Fariview- including
medication supervision and pediatric assessment by Mary Balle. Mary and I started to
talk with Tammy, and if Mary is do the medicine distribution, then we would want others
to screen the best referrals, and would we do that. Mary and I started to talk with Tammy
and the social workers who were there at the time. So we developed this plan to see how
it might work even though we were at the end of the school year. We got a list of students
who were referred, and of course Tammy left, Dr Hunter (principal) came, and we re-
vamped it once school started.

Spring 2015 From Paper to Policy
18
Promoting tutorial services through collaboration with outside agencies, a quality
education both during and after school, personal health and mental health to selected students,
and overall moral support all serves as constructs for Social Cognitive Theory (SCT). Social
cognitive theory specifies a core set of determinants, the mechanism through which they work,
and the optimal ways of translating this knowledge into effective health practices(A. Bandura,
2004). In relation to promoting health in schools, Social Cognitive Theory considers the macro
and micro factorials of the individual, as they are equally relevant to health promotion. In this
model of reciprocal causality, behavioral patterns, and environmental influences all operate an
interacting determinants that influence one another bi-directionally(Bandura, 2001; J. F.
McKenzie, Neiger, B.L., Thackeray, R., 2013b). Once these factors are evaluated, health
promotion and education are effective with the supportive framework of the family and
community. Comprehensive approaches that integrate master health programs with family and
community efforts are more successful in promoting health and in preventing detrimental habits
than are programs in which the schools try to do it alone(A. Bandura, 2004; Perry, 1992).
Self-efficacy in children is an important factor of Social Cognitive Theory, because it is
the beliefs about personal ability to perform behaviors that bring desired outcomes(McAlister,
2008). Seemingly, there is an uncertainty among the Fairview students’ self-efficacy: this focal
belief is the foundation of human motivation and action. Unless people believe they can produce
desired effects by their actions, they have little incentive to act or to persevere in the face of
difficulties(A. Bandura, 2004).

Spring 2015 From Paper to Policy
19
Phase 4: Administrative and Policy Assessment, and Intervention
Alignment
In spite of the individual challenges that inhibit cognitive development among students at
Fairview Elementary School, domestic policy such as Healthy People 2020 attempts to mitigate
them by health education and promotion. Healthy People 2020 provide objectives for healthcare
providers and communities to improve health outcomes and decrease health disparities(Inman,
2011). These objectives are variable in that they are designed to complement the mission
statement and goals set forth by the health care provider. According to their website, this
framework includes a new component specific to early and middle childhood (EMC)
development, and the educational and community-based objectives (ECBP). This needs
assessment will focus on the following objectives in the context of Coordinated School Health:
EMC-1: (Development) Increases the proportion of children who are ready for school in
all five domains of healthy development, physical development, social-emotional
development, approaches to learning, language, and cognitive development(Promotion,
2015).
ECBP-2 Increase the proportion of elementary, middle, and senior high schools that
provide comprehensive school health education to prevent health problems in the
following areas: unintentional injury; violence; suicide; tobacco use and addiction;
alcohol or other drug use; unintended pregnancy, HIV/AIDS, and STD infection;
unhealthy dietary patterns; and inadequate physical activity(Promotion, 2015).

Spring 2015 From Paper to Policy
20
The Monroe County Community School Corporation promotes these objectives in the
Coordinated School Health Program. According to the CDC (2015), the eight components of
Coordinated School Health are: Health Education; Physical Education; Health Services;
Nutrition Services; Counseling, Psychological and Social Services; Health and Safe School
Environment; Health Promotion for Staff; and Family/Community Involvement. Together, these
components guide people involved in school health planning to think broadly about how to
prevent health related barriers to learning, and promote health for the entire school
community(Authority, 2015).
At the beginning of 2015, Lisa Petscher was appointed health manager over the
Coordinated School Health. In a phone interview, she says:
“Indiana University Health Bloomington, Indiana University School of Public Health,
Premier Health Care, Bloomington Hospital Foundation, Community Foundation of Monroe
County, and MCCSC, all of these sectors came together and decided to bring back this position
that was cut due to the budget problems prior to 2008. This is where I am come in, my title is
manager of Coordinated Health, in addition to helping the schools start health initiatives , find
funding for them to make them sustainable, I will also as a district and as a whole that we are
meeting state mandates concerning health. A lot of times health gets put aside, all because
pressures regarding standardized testing. So making sure somebody- which is myself- that health
is in the conversation and that schools are being held accountable for that. Anything under the
health umbrella falls under my realm: the health education, physical activity, school health
services including the nurses and health aids, school nutrition services including what food is
served during the day the vending machines and afterschool programming, school
counselling/social services, over-arching culture/environment of the schools, to make sure the
school presents itself in a manner that is welcoming and safe and the staff making sure they have
health promotion and services as needed. Every school has a health wellness coordinator that
works at the individual building level. In addition to that, there is family and community
involvement and I think this position is fortunate to be funded through all of these different sectors
because we can then have a two-way relationship where I can call on them as needed for
resources, and then this gives them an opportunity to be engaged for extend their outreach in the
schools, their families, and the communities.”
Due to the nascent of Coordinated School Health in Monroe County Community School
Corporation, it is too soon to implement an outcome evaluation. For instance, the health and
wellness coordinator is voluntary at each school and the proxy meets with Lisa twice a year. Yet
Freddie Holmgren, Wellness and Fitness specialist from the MCCSC Health and Wellness
Spring 2015 From Paper to Policy
21
Center, corresponds with the teachers via email with quarterly challenges. These challenges
“trickle down” from the teachers to their students. Specifically, Lisa says: “Freddie sent out a
challenge such as a 10,000 steps challenge, and one of the teachers at the elementary school got
her students involved, and they were trying to reach that goal as well.” In a phone conversation,
we notified Freddie to inquire the success rate of her quarterly challenges, and discovered she is
new to her position.
Without specifying which Health People 2020 objective, we have asked Lisa how the
Healthy People 2020 objectives support the vision of Coordinated School Health. She answers
in the context of formative evaluation:
“most of the people who funded this collaboration.. it is their work, and that they look to
them to see where they should set their goals and how high to reach, and knowing what’s
important globally as well as in the community while keeping this an eye on the big picture. This
program is very new, so we’re still working on which indicators do we measure to see how
effective this program was, and we’ve look to a number of different programs that has something
similar and organizations such as the World Health Organization, and to see what’s important
here.”
Overall, the Coordinated School Health program shows promise in reducing health
behaviors and increasing health education among students. However, unless objectives are
specific, measurable, achievable, realistic and relevant, and time-bound, formative evaluation on
the effectiveness of this program may not occur. This may result in continued academic failure
among the students, and health behaviors that will continue into adulthood. Given the effort
required to make school policy changes to influence health, research is needed to test the premise
that promoting student health will also support academic achievement(Ickrovics, 2014). This
research is evident in the School-Based Health Care (SBHC) program.

Spring 2015 From Paper to Policy
22
The SBHC is a model of pediatric primary care delivery that offers a comprehensive
services provided by a multidisciplinary team on school grounds(Brindis, 2003; Care, 2010;
Juszczak, 2003; Keeton, 2012; Larson, 2014). The SBHC’s integration within the school
community has allowed for increased access to health and mental health care, especially for the
hard-to-reach and high-risk adolescent population, as well as minority and lower socioeconomic
pediatric populations (Allison, 2007; Brindis, 2003; Care, 2010; Keeton, 2012; Larson, 2014;
Soleimanpour, 2010; Wade, 2008). Currently, there are 1,900 SBHC’s nationwide located in
urban, rural, and suburban communities(Care, 2010; Larson, 2014). In Indiana, there are 87
SBHC facilities, but there is a dearth of research (Care, 2015).
Given SBHC is mandated throughout Illinois, we have examined the impact of this public
policy on its constituents. In corresponding with proxies from the Illinois Department of Human
Services, we have learned that specified services are sponsored by the Illinois Department of
Education and considered School-Based Linked Health Care. Apparently, there is an association
between Medicaid and Education due to the implementation of the Medicare Catastrophic
Coverage Act (Public Law 100-360); Illinois has actively supported this relationship since 1992,
through the School-Based Linked Health Services program, (S. Illinois, 2015). School-Based
Linked Health Centers (SBLHC) are underwritten by the Illinois Department of Healthcare and
Family Services (IDHS). To become certified, each agency must meet the standards established
by IDHS in 77 IL. Adm. Code, Part 2200(Services, 2002). Each child is also assigned an
Individualized Education Program (IEP) which thereby approves specific services. Covered
services include: audiology, developmental assessments, medical equipment, medical services,
medical supplies, nursing services, occupational therapy, physical therapy, psychological

Spring 2015 From Paper to Policy
23
services, school health aide, social work, speech/language pathology, and transportation(S.
Illinois, 2015).
In contrast, School-based Healthcare centers are not sponsored by the Illinois Department
of Education. However, they provide similar services with the premise “every child deserves a
medical home.” The goals are:
Improve the quality of health care and child health outcomes
Assure appropriate utilization of health care services
Reduce the usage of the emergency room for routine medical care
Improve access to care through the availability of a provider network and
expansion of providers
Provide the most appropriate and cost-effect level of care(ILHS, 2008).
Maternal health is afforded to mothers for 60 days and after a baby is born. “Mom and
Babies” offers inpatient and outpatient care including delivery(I. D. o. H. a. F. Services, 2015).
Further, perinatal depression screening is available. It is estimated that 10-20 percent of women
in the United States who give birth experience a major depression during pregnancy or within a
year after delivery; the prevalence may be higher in women with low socioeconomic
status(ILHS, 2008). Further, providing this service has been mandated as Public Act 95-0469(I.
D. o. H. Services, 2015). After the child is born, single mothers/ parents have the option of
enrolling their child/children into the “All Kids” health insurance. “All Kids” is Illinois’ program
for children who need comprehensive, affordable health insurance, regardless of family income,
immigration status or health condition(S. o. Illinois, 2015). Further, children who qualify will
receive coverage up until 18 years of age.

Spring 2015 From Paper to Policy
24
Our research has found that the EverThrive Illinois Coalition for School Based Health
Care (ICSHC) is an advocacy group in support of health care for both pregnant mothers and
children through the school setting. According to their website, ICSHC’s goal is to represent
institutions and individuals who support, receive, and provide health care in schools and school-
linked programs((ICSHC), 2015). Additionally, their mission is to provide leadership, resources,
training and technical assistance to enable school health centers to deliver high quality services,
become financially stable and play an active role in public policy. Further, they advocate for
local, state and national policies and funding to integrate school health centers into health and
education systems((ICSHC), 2015).
Through EverThrive’s 2015 policy, they explain the predisposing, enabling and
reinforcing factors affecting their clientele and how their mission and goals are supportive of
existing services. This includes SNAP (Supplemental Nutrition Assistance Program), the
Affordable Care Act, and immunizations. EverThrive Illinois envisions an Illinois that works
toward equity and social justice, fosters the development of healthy families and provides fair
access to quality health care(E. Illinois, 2015). Furthermore, EverThrive addresses income
inequality as a construct of health disparities among their target population. This includes:
Support policies and programs that lessen the economic disparities that exist for
women, children and families.
Advocate for policies and programs that improve educational opportunities for
lower income families.
Support a fair tax structure and adequate revenue for Illinois, advocating for no
harmful or inequitable cuts to vital programs and services for families.
Support policies to raise the minimum wage (E. Illinois, 2015)
Spring 2015 From Paper to Policy
25
We found it important to examine the total Medicaid spending during fiscal year 2012,
monthly enrollment for children in both Illinois and Indiana, and the overall infant mortality rate
in both Illinois and Indiana. In Illinois, total Medicaid spending was $13,392,553,588, whereas
in Indiana, it was an estimated $7,486,196,206(K. F. Foundation, 2015b). This funds the monthly
enrollment of 1,573.8 children in Illinois, and 570.5 in Indiana(K. F. Foundation, 2015a). We
also evaluated the infant mortality rate from 2011, which is 6.6 per 1,000 live births in Illinois(I.
D. o. P. Health, 2015), and 7.7 per 1,000 live births in Indiana(I. D. o. Health, 2015a).
Coincidentally, both rates exceed the Health People 2020 infant mortality goal- which is 6.0 per
1,000 live births(I. D. o. Health, 2015a).
Spring 2015 From Paper to Policy
26
PROCEED
Phase 5—Implementation
Given our target population—children—is a vulnerable population, we believe this is an
intervention in the community. These interventions seek more intensive or profound change in a
subpopulation, usually within or from a specific community site such as a workplace, hospital or
clinic, nursing home, or school; this approach is targeted and setting specific(L. W. K. Green,
M.W., 2004). On a macro level, the Bloomington community (e.g., Indiana University’s
Fairview Literacy Program, Catholic Charities Bloomington) is interested in helping Fairview
students academically by providing a literacy program, mental health services, and the eight
components of the Coordinated School Health Program. On a micro level, however, Fairview’s
attempt to promote the “Artful Learning” curriculum is not working to the advantage of
academic achievement, especially with regards to the Indiana State Test of Educational Progress
(ISTEP). Additionally, Fairview Elementary risk government takeover should the majority of
students fail the ISTEP exam this school year. We believe the children’s health status is in direct
proportion of their academic success; therefore, a school-based health care facility would
mitigate their health disparities, reduce absenteeism, and elevate their academic achievement.
To better understand the socio-environmental conditions that affect this target population we
suggest applying this needs assessment and facilitating a steering committee. This volunteer-
based committee would consist of an external evaluation team consisting of: two pediatricians,
one attorney, two parents, two educators (a primary and intermediate grade-level educator), one
interpreter, the health educator from Monroe County Community School Corporation, one proxy
from the Monroe County Health Department, and two professors from Indiana University (one

Spring 2015 From Paper to Policy
27
professor from the School of Public Health, one professor from the Department of Medical
Sciences). These partnerships not only enhance the health of the populations they serve, but they
benefit their academic health institutions by educating health professionals for the future(Smego,
1996). The advantages to an external committee are:
Known expertise.
The responsibility for conducting the program becomes the work of another.
Sometimes external personnel are more respected than internal personnel simple because
they are from the outside.
Bring global knowledge to the program because they have worked with a variety of
entities and cultures(Harris, 2001; J. F. McKenzie, Neiger, B.L., Thackeray, R., 2013a).
The creation of an external group is the starting point of MAP-IT (Mobilize, Assess, Plan,
Implement and Track), a framework promoted by the US Department of Health and Human
Services. MAP-IT: A Guide to Using Healthy People 2020 in Your Community offers guidance
on mobilizing partners, assessing the needs of your community, and creating and implementing a
plan to reach Health People 2020 objectives, and guidance to track your community’s progress
(Hatcher, 2014; U. S. D. o. H. a. H. Services, 2015). We have selected MAP-IT because of the
Healthy People 2020 objectives mentioned earlier in phase four, and the overall format will
further progress the PROCEED section of the needs assessment model.
We will conduct our assessment within the context of research, to ascertain valuable data
from previous studies, to facilitate our research under guidance from our professors from Indiana
University, and to promote further research in School-Based Health Care among marginalized
communities. We will use focus groups or community forums to facilitate a discussion;
according to Krueger and Casey (2000), focus groups are carefully planned series of discussion
where participants usually are selected on the basis of a shared set of attributes. They are
Spring 2015 From Paper to Policy
28
designed to obtain thoughts, feelings, opinions, insights, attitudes, misconceptions, and/or beliefs
about a defined area of interest(Kreuger, 2008). Our participants are parents/guardians and other
stakeholders who are relevant to the Fairview community. To obtain their support, we will gather
a convenience sample of informants that will consist of a minimum of 12 adults age 18 or older.
Our moderator will ask questions that are pre-approved from the Institutional Review Board at
Indiana University, and each participant will receive a gift card from Kroger.
Our external committee will then analyze the responses for emergent themes from our
participants. This information will be applied to further developing the SBHC under constructs
that are recommended by our external group and the Centers for Disease Control and Prevention.
Before the 2016-17 school year, we will collaborate with both the MCCSC School Board and
Fairview’s Administration to identify an area specific to SBHC. If feasible, we will facilitate a
pilot study with the assistance from our external committee to assess the usage of the health care
medium. If impractical, we will suggest the Ronald McDonald Care Mobile, a fleet of state-of-
the-art mobile healthcare vehicles that deliver cost-effective medical, dental, and health
education services directly to vulnerable youth in six countries(M. s. Corporation, 2015).
We will establish a Board of Directors who will oversee operations and facilitate
activities on behalf of the health care center. This includes establishing bylaws, becoming
incorporated, applying for 501c status, and selecting personnel(Smego, 1996). Concurrently, we
will begin fundraising by facilitating a Capital Campaign and seeking local, state, and national
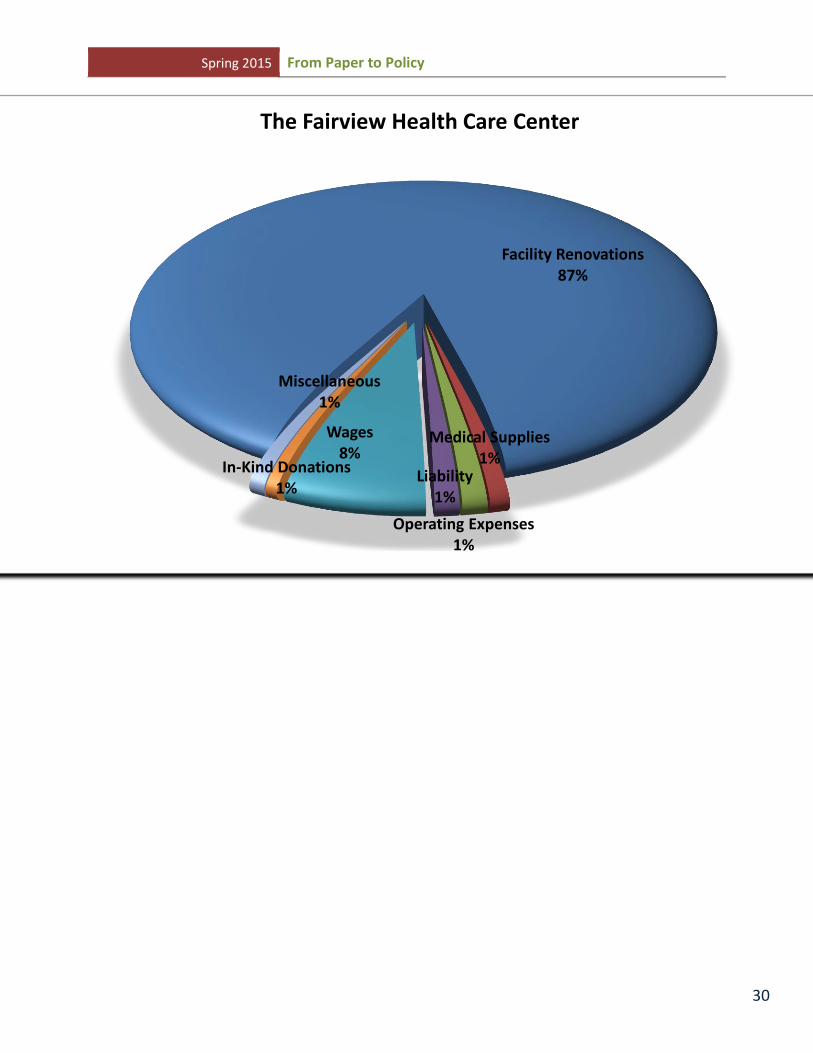
resources. Based on the cost of medical supplies, facility renovations, operating costs, wages,
and liability insurance, we will set our funding floor at $2 million. The following illustrates our
fiscal spending:

Spring 2015 From Paper to Policy
29
Spring 2015 From Paper to Policy
30
Facility Renovations 87%
Medical Supplies 1%
Operating Expenses 1%
Liability 1%
Wages 8%
Miscellaneous 1%
In-Kind Donations 1%
The Fairview Health Care Center
Spring 2015 From Paper to Policy
31
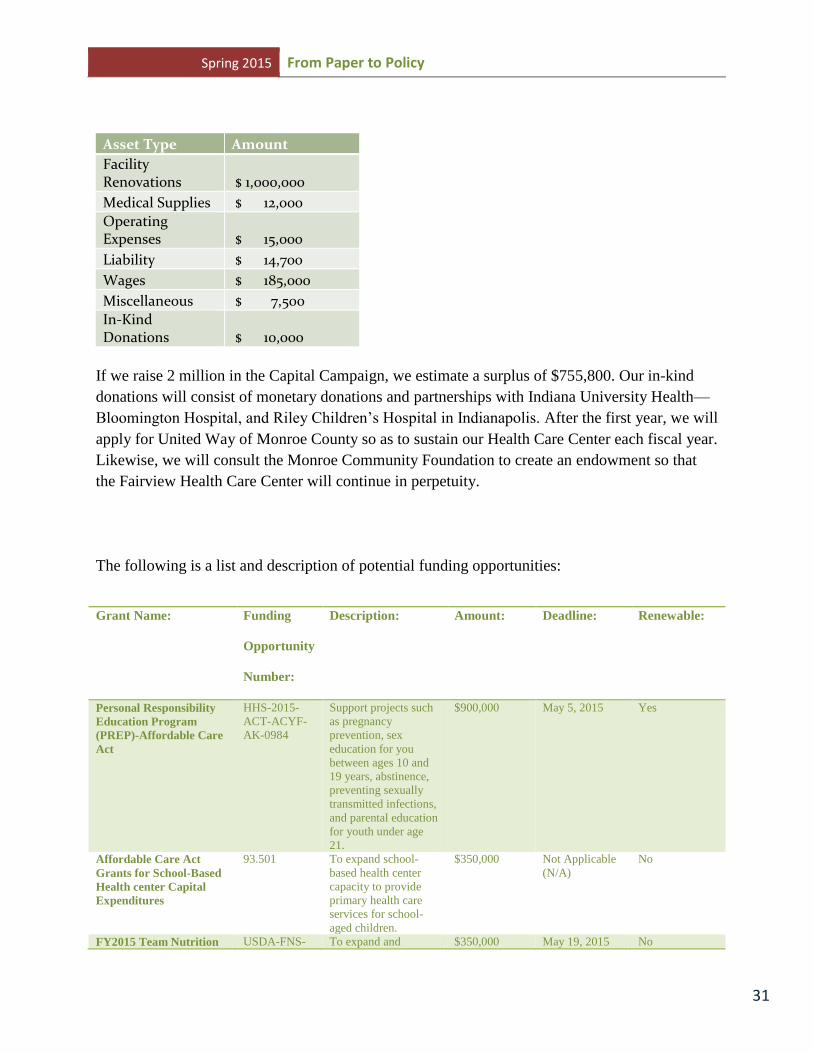
Asset Type Amount
Facility
Renovations $ 1,000,000
Medical Supplies $ 12,000
Operating Expenses $ 15,000
Liability $ 14,700 Wages $ 185,000 Miscellaneous $ 7,500 In-Kind
Donations $ 10,000
If we raise 2 million in the Capital Campaign, we estimate a surplus of $755,800. Our in-kind
donations will consist of monetary donations and partnerships with Indiana University Health—
Bloomington Hospital, and Riley Children’s Hospital in Indianapolis. After the first year, we will
apply for United Way of Monroe County so as to sustain our Health Care Center each fiscal year.
Likewise, we will consult the Monroe Community Foundation to create an endowment so that
the Fairview Health Care Center will continue in perpetuity.
The following is a list and description of potential funding opportunities:
Grant Name: Funding
Opportunity
Number:
Description: Amount: Deadline: Renewable:
Personal Responsibility
Education Program
(PREP)-Affordable Care
Act
HHS-2015-
ACT-ACYF-
AK-0984
Support projects such
as pregnancy
prevention, sex
education for you
between ages 10 and
19 years, abstinence,
preventing sexually
transmitted infections,
and parental education
for youth under age
21.
$900,000 May 5, 2015 Yes
Affordable Care Act
Grants for School-Based
Health center Capital
Expenditures
93.501 To expand school-
based health center
capacity to provide
primary health care
services for school-
aged children.
$350,000 Not Applicable
(N/A)
No
FY2015 Team Nutrition USDA-FNS- To expand and $350,000 May 19, 2015 No
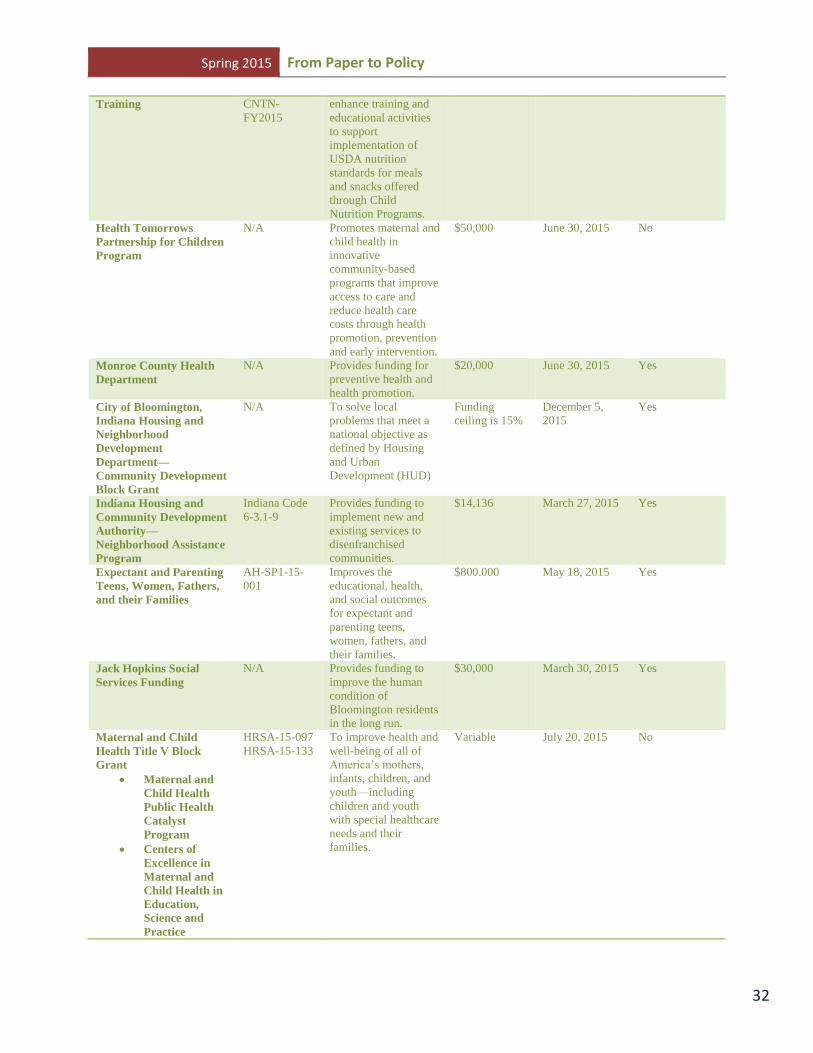
Spring 2015 From Paper to Policy
32
Training CNTN-
FY2015
enhance training and
educational activities
to support
implementation of
USDA nutrition
standards for meals
and snacks offered
through Child
Nutrition Programs.
Health Tomorrows
Partnership for Children
Program
N/A Promotes maternal and
child health in
innovative
community-based
programs that improve
access to care and
reduce health care
costs through health
promotion, prevention
and early intervention.
$50,000 June 30, 2015 No
Monroe County Health
Department
N/A Provides funding for
preventive health and
health promotion.
$20,000 June 30, 2015 Yes
City of Bloomington,
Indiana Housing and
Neighborhood
Development
Department—
Community Development
Block Grant
N/A To solve local
problems that meet a
national objective as
defined by Housing
and Urban
Development (HUD)
Funding
ceiling is 15%
December 5,
2015
Yes
Indiana Housing and
Community Development
Authority—
Neighborhood Assistance
Program
Indiana Code
6-3.1-9
Provides funding to
implement new and
existing services to
disenfranchised
communities.
$14,136 March 27, 2015 Yes
Expectant and Parenting
Teens, Women, Fathers,
and their Families
AH-SP1-15-
001
Improves the
educational, health,
and social outcomes
for expectant and
parenting teens,
women, fathers, and
their families.
$800.000 May 18, 2015 Yes
Jack Hopkins Social
Services Funding
N/A Provides funding to
improve the human
condition of
Bloomington residents
in the long run.
$30,000 March 30, 2015 Yes
Maternal and Child
Health Title V Block
Grant
Maternal and
Child Health
Public Health
Catalyst
Program
Centers of
Excellence in
Maternal and
Child Health in
Education,
Science and
Practice
HRSA-15-097
HRSA-15-133
To improve health and
well-being of all of
America’s mothers,
infants, children, and
youth—including
children and youth
with special healthcare
needs and their
families.
Variable July 20, 2015 No
Spring 2015 From Paper to Policy
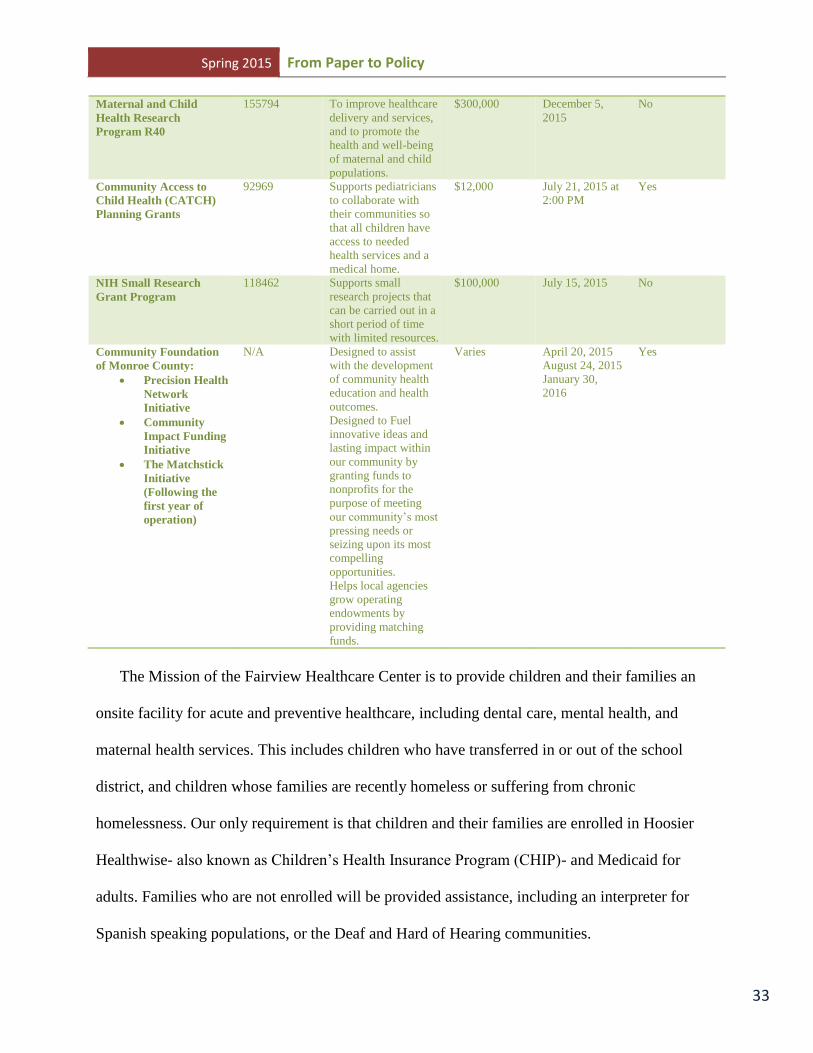
33
Maternal and Child
Health Research
Program R40
155794 To improve healthcare
delivery and services,
and to promote the
health and well-being
of maternal and child
populations.
$300,000 December 5,
2015
No
Community Access to
Child Health (CATCH)
Planning Grants
92969 Supports pediatricians
to collaborate with
their communities so
that all children have
access to needed
health services and a
medical home.
$12,000 July 21, 2015 at
2:00 PM
Yes
NIH Small Research
Grant Program
118462 Supports small
research projects that
can be carried out in a
short period of time
with limited resources.
$100,000 July 15, 2015 No
Community Foundation
of Monroe County:
Precision Health
Network
Initiative
Community
Impact Funding
Initiative
The Matchstick
Initiative
(Following the
first year of
operation)
N/A Designed to assist
with the development
of community health
education and health
outcomes.
Designed to Fuel
innovative ideas and
lasting impact within
our community by
granting funds to
nonprofits for the
purpose of meeting
our community’s most
pressing needs or
seizing upon its most
compelling
opportunities.
Helps local agencies
grow operating
endowments by
providing matching
funds.
Varies April 20, 2015
August 24, 2015
January 30,
2016
Yes
The Mission of the Fairview Healthcare Center is to provide children and their families an
onsite facility for acute and preventive healthcare, including dental care, mental health, and
maternal health services. This includes children who have transferred in or out of the school
district, and children whose families are recently homeless or suffering from chronic
homelessness. Our only requirement is that children and their families are enrolled in Hoosier
Healthwise- also known as Children’s Health Insurance Program (CHIP)- and Medicaid for
adults. Families who are not enrolled will be provided assistance, including an interpreter for
Spanish speaking populations, or the Deaf and Hard of Hearing communities.
Spring 2015 From Paper to Policy
34
We will evaluate or track our program’s success with the use of goals and SMART
Objectives. Our goals are as follows:
To reduce chronic absenteeism among our target population
To promote preventive healthcare
To provide prenatal, perinatal, and post-partum care to mothers, including
perinatal depression screening.
To create a liaison between Fairview Elementary School, the Parents or
Guardians, and Riley Pediatrics
To provide mental health services.
To provide pregnancy and sexually transmitted infection prevention, promote
abstinence, and provide resources to teens who become parents.
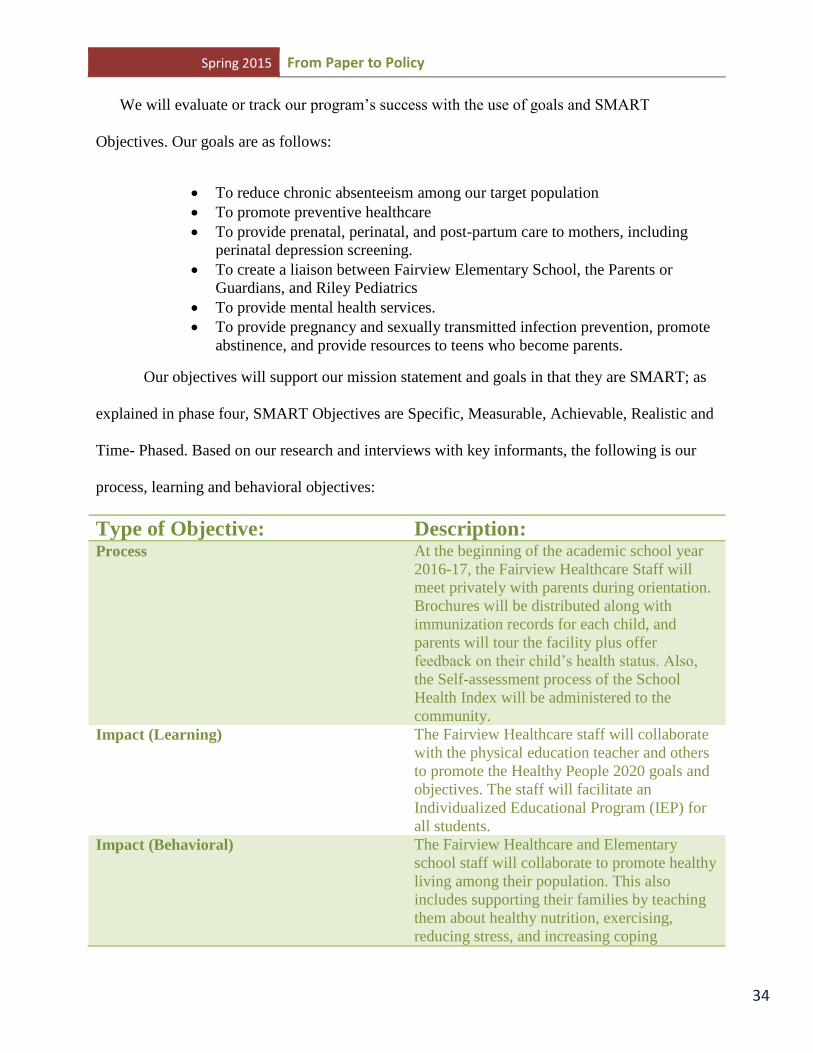
Our objectives will support our mission statement and goals in that they are SMART; as
explained in phase four, SMART Objectives are Specific, Measurable, Achievable, Realistic and
Time- Phased. Based on our research and interviews with key informants, the following is our
process, learning and behavioral objectives:
Type of Objective: Description: Process At the beginning of the academic school year
2016-17, the Fairview Healthcare Staff will
meet privately with parents during orientation.
Brochures will be distributed along with
immunization records for each child, and
parents will tour the facility plus offer
feedback on their child’s health status. Also,
the Self-assessment process of the School
Health Index will be administered to the
community.
Impact (Learning) The Fairview Healthcare staff will collaborate
with the physical education teacher and others
to promote the Healthy People 2020 goals and
objectives. The staff will facilitate an
Individualized Educational Program (IEP) for
all students.
Impact (Behavioral) The Fairview Healthcare and Elementary
school staff will collaborate to promote healthy
living among their population. This also
includes supporting their families by teaching
them about healthy nutrition, exercising,
reducing stress, and increasing coping

Spring 2015 From Paper to Policy
35
mechanisms.
Impact (Environmental) By the end of 2017, the parents will learn
sustainability opportunities such as gardening
and recycling in their community. Based on
each student’s IEP, students will be
coordinated with services specific to their
learning and personal interests. This outcome
is due to the collaboration of the Fairview
Healthcare Center and supportive services that
foster sustainable living.
Outcome Objective At the end of 2017, the success of the Fairview
Healthcare Center will be determined by the
School Health Index (Planning for
improvement process), test scores from the
Indiana State Test of Educational Progress
(ISTEP), and the grades of all students. For
each grade level, our target is at least 65% of
the students should successfully pass the
ISTEP after 2017, and 70% after Year 2018.
We believe our mission statement, goals and objectives will all support the Indiana State
Board of Education’s Title 511 Article 7—Special Education. Accordingly, Article 7 specifies a
protocol should be met by a school or school system that will positively affect the student’s
academic pursuits. Similar to Illinois’ Department of Education, it recognizes the Individualized
Education Program (IEP) in the context of accomplishments known as benchmarks. An
Individualized Education Program, or “IEP” means a written document, developed, reviewed,
and revised by the CCC in accordance with 511 IAC 7-42, that describes the following: 1) how a
student will access the general education curriculum, if appropriate, and 2) the special education
and related services needed to participate in the educational environment(I. D. o. Education,
2014b). Benchmarks establish expected performance levels for students assessed against
alternative achievement standards that allow for regular checks of progress that coincide with the
reporting period for informing parents of the student’s progress toward achieving the annual
goals delineated in a student’s IEP(I. D. o. Education, 2014a).
Spring 2015 From Paper to Policy
36
Phase 6- Process Evaluation
We want to ensure the Fairview Healthcare Center is meeting its objectives and goals.
We desire accountability to our stakeholders and subsequent sponsors so that it will continue in
perpetuity. To ensure assurance, we will facilitate a process evaluation, which investigates how a
program is executed in order to assess and improve implementation(Golden, 2014). Process
evaluations should be embedded in trial evaluations to use consistent measures to assess
implementation fidelity, acceptance, and reach. However, they also need to go beyond these by
collecting qualitative contextual data, which will help answer the questions: what works, for
whom, in what circumstances, and why(Bonell, 2012; Langford, 2014). We will address the
following questions:
1. What features of the Fairview Healthcare are not meeting the goals and objectives set
forth by the external group? Why not?
Reasoning: Underserved populations also disproportionately rely on schools to meet
child-health needs because they are less likely to have family-level health resources such
as a regular source of care, health insurance, and access to quality health care.(Smedley,
2008; L. M. Vaughn, Jacquez, F., & Zhao, J., 2011). To address health disparities in
underserved populations, health intervention and prevention programs must capitalize on
the opportunities available in the school setting(L. M. Vaughn, Jacquez, F., & Zhao, J.,
2011).
Reasoning: Health habits are rooted in familial practices. But schools have an important
role to play in promoting the health of a nation. This is the only place where all children
can be easily reached (Al. Bandura, 2004)
2. What percentage of students suffer from chronic absenteeism? Why?
Reasoning: Low income increases the likelihood that youth will not be insured, see a
dentist, and have to use emergency rooms as treatment sites. These same health issues
trickle into school and so manifest themselves in learning disabilities, short attention
spans, poor attendance, and academic performance(J. W. Richardson, 2008).
Reasoning: Regular school attendance and educational attainment are known to predict
later health in adulthood(Cann, 2014; Kuh, 1993; Wadsworth, 1997).
3. How much staff time and SBHC resources did intervention implementation require
(Golden, 2014)?

Spring 2015 From Paper to Policy
37
4. What percentage of students has transferred in/out of Fairview Elementary School?
Choose one of the two questions- or both- for follow up
5. With students who have transferred in: what percentage of medical records arrive within
days of their admittance?
6. With students who have transferred out: what percentage of medical records were sent to
their elementary school nurse or pediatrician?
Reasoning: Medical Records Verification using PowerSchool
PowerSchool is a widely used web-based student information system, supporting 10
million students in all 50 states and over 65 countries. PowerSchool enables educators to
make data-driven decisions that impact student performance while creating a
collaborative environment for parents, teachers and students to work together.
Because students’ health data….are entered into the students’ records, they are portable-
if a student starts at one elementary school and moves to another mid-year or in/out of the
district, all of the health data moves with the child’s academic record and is fully
available at the new school immediately. Data are also retained over time for all children;
if a student drops out or moves out of the district and returns, for example, his or her data
is re-activated(Project, 2013).
The process evaluation provides data on the quality and fidelity of delivering the
interventions. Such data can help develop corrective actions(Issel, 2014). These questions
incorporate quantitative and qualitative data collection, thereby providing both objective and
subjective data. Additionally, it will answer any concerns addressed in the self-assessment
process of the School Health Index—particularly the weaknesses of previous health services
provided to the children.
Spring 2015 From Paper to Policy
38
Phase 7: Impact Evaluation
At the end of the first year, we recommend planning for improvement process: the second
assessment of School Health Index to determine the effectiveness of the Fairview Healthcare
Center. Whereas the self-assessment process provided insight in terms of the strengths and
weaknesses of the health program, this can provide feedback to facilitate an impact evaluation,
an evaluation that focus on the immediate observable effects of a program (e.g., awareness,
knowledge, attitudes, skills, environment, and behaviors) leading to the intended outcomes of a
program(L. W. Green, & Lewis, F.M., 1986; J. F. McKenzie, Neiger, B.L., & Thackeray, R.,
2013). According to the CDC (2015), using the School Health Index will:
Enable schools to identify strengths and weaknesses of health and safety policies and
programs.
Enable schools to develop an action plan for improving student health, which can be
incorporated into the School Improvement Plan.
Engage teachers, parents, students, and the community in promoting health-enhancing
behaviors and better health(Prevention, 2015).
Promoting the School Health Index at Fairview Elementary would provide the external
committee, the administration, and stakeholders a response as to whether the healthcare center
has provided effective improvement since the beginning to the school year. Particularly, the
planning for improvement process:
Enables you to identify recommended actions your school can take to improve its
performance in areas that received low scores. It guides you through a simple process for
prioritizing the various recommendations. This step will help you decide on a handful of
actions to implement this year. Finally, you will complete a School health Improvement
Plan to list the steps you will take to implement your actions(Prenvetion, 2015).
Spring 2015 From Paper to Policy
39
Promoting the School Health Index’s “planning for improvement” section would describe
the success of the Fairview Healthcare program, and similarly areas where improvement is
needed. This feedback is critical for subsequent funding, community and stakeholder support,
and the overall longevity of the school-based health care center. Further, this information can be
disseminated to our funding partners and Indiana University who may desire feedback for
subsequent research.
Phase 8: Outcome Evaluation
Throughout the intervention, we utilized formative evaluation to ensure that goals and
objectives, and social cognitive theory are salient and efficacious. Similarly, we would calculate
an outcome evaluation over a longer period of time. An outcome evaluation is long-term in
nature and generally takes more time and resources to conduct than impact evaluation(J. F.
McKenzie, Neiger, B.L., & Thacckeray, R., 2013). As mentioned in phase five, we will evaluate
each student and create an IEP that’s specific to their cognition. Shared characteristics among the
students will result in similar control groups, and we will monitor the effectiveness of health care
on their progress. We will also evaluate the students who matriculate at kindergarten and remain
at six grades. Students who transfer from Fairview Elementary School will no longer qualify for
the Fairview Healthcare Center. Rather, their records will be sent to the school via the
PowerSchool database, which was described earlier. New students or transfer will receive
placement into a controlled group that’s specific their transference into the school, but will also
receive an IEP. We believe their academic progress would compromise the internal validity of
the controlled groups who attended Fairview since their matriculation in kindergarten.

Spring 2015 From Paper to Policy
40
In addition to an IEP, each student will receive a pre-test and post-test to quantify school-
readiness and academic progress. These scores, their academic progress, and the passing of
standardized tests will provide substantial evidence regarding the Healthcare center’s
effectiveness. Additionally, this feedback is instrumental in implementing additional goals, and
enhancing or modifying services to meet the student’s needs.
Notably, Fairview Elementary School will become the first Title I Elementary School in
Bloomington to facilitate a School-based Health Care program. As a result, we consider external
validity as the number of parents who opt out of services provided at the Fairview Healthcare
facility. In an interview with one parent regarding her child’s pediatrician, the mother strongly
feels that only Dr. Debra K. McDaniel of Riley Pediatrics is the best and only pediatrician for her
child. Thus, we will not undermine the parent’s choice, but would enroll their children into a
specific control group when they feel otherwise about our program.

Spring 2015 From Paper to Policy
41
Confounding Issues/Variables
Throughout this assessment, a few confounding issues developed that ultimately was not
included. In terms of correspondence, we made every effort to notify parents, key informants and
many organizations to support our research, but did not receive the response we were hoping for.
Had answers been provided, it would alter the calculus of this assessment.
Regarding the Fairview Literacy Program, we were concerned about impact evaluations.
Our follow-up questions included:
o Are there goals set for the children with a specific time frame?
o Is there subsequent correspondence between the mentors and teachers to discuss
the outcomes after each class, including where improvement is needed?
o In spite of the children’s challenges, what keeps them motivated to keep trying?
o What percentage of students improved academically because of the program?
We reviewed the local newspaper regarding the parent’s frustration with the ISTEP
test(Carlton, 2015). Apparently, parents are temporarily withdrawing their children and opting
for homeschooling during the said exam. If the parent “opt out” for the child taking the test,
he/she will earn a failing grade, but it will not affect Fairview Elementary School in terms of the
number of students failing the exam overall. We were concerned about this issue, but found it
could not be addressed in our assessment due its complexity.
Recently, Dr. Judith DeMunth, Superintendent with the Monroe County Community
School Corporation, suggested to Governor Mike Pence of Indiana that the ISTEP should be
administered to students at the end of the school year, as the current date does not account for
missed school days due to the winter break or during severe winter weather. Dr. DeMunth
further suggests that the current assessment procedure is not working to the benefit of both the
Spring 2015 From Paper to Policy
42
student and teachers. Feedback however, has not been provided from Governor Pence, which is
why this was not addressed I our assessment.
Due to budgetary constraints, we were only able to interview three parents and two key
informants. Although we attempted to notify the parents who collaborate with both Fairview
Elementary School and Catholic Charities, this sampling pool resulted in two interviews.
Despite this, we collaborated with other agencies including the Monroe County Community
School Corporation, the Monroe County Health Department, Riley Pediatrics, the Indiana
Department of Health, the Illinois Department of Human Service, the Illinois Department of
Education, Indiana University, and Whitney Thomas at Fairview Elementary School.

Spring 2015 From Paper to Policy
43
Bibliography
(ICSHC), I. C. f. S. H. C. (2015). Mission & Overview. ICSHC Mission & Overview. http://www.ilmaternal.org/icshc/mission.html
Alder, N. E., Boyce, T., Chesney, M., Cohen, S., Folkman, S. Kahn, R., & Syme, S.L. (1997). Socioeconomic status and health: The challenge of the gradient. American Psychologist, 49, 15-24.
Allison, M. A., Crane, L. A., Beaty, B.L., Davidson, A.J., Melinkovich, P., & Kempe, A. (2007). School-based health centers: improving access and quality of care for low-income adolecents. Pediatrics, 120(4), e887-894.
Association, I. S. T. (2015). The House Education Committee Indianapolis ISTA Headquarters. Authority, O. H. (Producer). (2015). Coordinated School Health Approach. Oregon Health Authority.
Retrieved from http://www.public.health.oregon.gov/HealthPeopleFamilies/Youth/HealthSchool/HKLB/Pages/model.aspx
Bandura, A. (2001). Social Cognitive Theory: An Agentic Perspective. Annual Review of Psychology, 32, 1-26.
Bandura, A. (2004). Health Promotion by Social Cognitive Means. Health Education & Behavior, 31(2), 143-164.
Bandura, A. (2004). Health Promotion by Social Cognitive Means. Health Education and Behavior, 31(2), 143-164.
Bonell, C., Fletcher, A., Morton, M., Lorenc, T., & Moore, L. (2012). Realist randomized controlled trials: a new approach to evaluating complex public health interventions. Social Science Medicine and Research, 75(12), 2299-2306.
Bradley, L. B. P. E. (1978). Difficulties in auditory organization as a possible cause of reading backwardness. Naure, 271, 746-747.
Brindis, C. D., Klein, J., Schlitt, J., Santelli, J., Juszczak, L., & Nystrom, R. J. (2003). School-based health centers: accessibility and accountability. Journal of Adolescent Health, 32(6), 98-107.
Bureau, U. C. (2009). Total Population. Washington DC: United States Census Bureau. Bureau, U. S. C. (Producer). (2013). State and County Quick Facts. United States Governent. Retrieved
from http://quickfacts.census.gov/qfd/states/18/18105.html Cann, W., Cassidy, J., Coverdale, G., Ha, M.A., Nicholson, W., & Rao, M. (2014). The value of using
schools as community assets for health London: Royal Society for Public Health Care, N. A. o. S.-B. H. (Producer). (2010). School-based health centers: national census school year 2007-
2008. National Assembly on School-Based Health Care. Retrieved from http:// ww2.nasbhc.org/NASHBCCensusReport07-08.pdf
Care, N. A. o. S.-B. H. (Producer). (2015). The Facts: Funding for School-Based Health Care Centers under the Affordable Care Act. NASBHC. Retrieved from http://www.nasbhc.org/atf/cf/%7BCD9949F2-2761-42FB-BC7A-CEE165C701D9%7D/SBHC%20PPACA%20FACT%20SHEET%203.8.11.PDF
Carlton, K. (2015). Frustrated MCCSC parents opt children out of ISTEP test. Bloomington: Heral-Times Newspaper.

Spring 2015 From Paper to Policy
44
Corporation, M. C. C. S. (2013). MCCSC Feeder Schools Flow Chart. MCCSC. http://www.mccsc.edu/cms/lib07/IN01906545/Centricity/Domain/69/High%20School%20Flow%20Chart.pdf
Corporation, M. C. C. S. (2015). Fairview Elementary School Boundary Map. Monroe County Community School Corporation. http://mccsc.schoolwires.net/cms/lib07/IN01906545/Centricity/Domain/393/FAI.pdf
Corporation, M. s. (Producer). (2015, March 5). Legacy on Wheels. Ronald McDonald Care Mobile Open doors for Children. Retrieved from http://www.aboutmcdonalds.com/mcd/our_company/amazing_stories/serving_our_community/legacy_on_wheels.html
Department, T. M. C. H. (2010). Monroe County Health Assessment Atlas. Bloomington: Monroe County Health Department.
Education, I. D. o. (2011). Indiana Department of Education Supporting Success Public Law 221 Overview. http://www.doe.in.gov/sites/default/files/accountability/2011-pl-221-fact-sheet.pdf
Education, I. D. o. (2014a). 511 IAC 7-32-11. Indianapolis: Indiana Department of Education. Education, I. D. o. (2014b). 511 IAC 7-32-48 "Individualized education program" or "IEP" defined.
Indianapolis Indiana Department of Education. Education, I. D. o. (Producer). (2014c). Historical 2014 ISTEP Schools. IDOE. Retrieved from
http://www.doe.in.gov/accountability/find-school-and-corporation-data-reports Education, I. D. o. (2014d). IDOE Data. Indiana Department of Education.
http://www.doe.in.gov/idoe/idoe-data Education, I. D. o. (2015). School Enrollment, Ethnicity, and Free, Reduced Price Meal Status. Indiana
Department of Education. http://www.doe.in.gov/idoe/idoe-data Education, I. f. Q. o. (2013). Strong Accountability that is Fair and Transparent Institute for Quality of
Education http://www.i4qed.org/policies/strong-accountability-that-is-fair-and-transparent Foundation, K. F. (Producer). (2015a). State Health Facts: Monthly Medicaid Enrollment for Adults and
Children (in thousands). Kaiser Family Foundation Retrieved from http://kff.org/medicaid/state-indicator/monthly-medicaid-enrollment-for-adults-and-children-in-thousands/
Foundation, K. F. (Producer). (2015b). Total Medicaid Spending. Kaiser Family Foundation. Retrieved from http://kff.org/medicaid/state-indicator/total-medicaid-spending/?state=IL
Foundation, R. W. J. (2014). Country Health Rankings and Roadmaps. Indiana 2014 Rankings. http://www.countyhealthrankings.org/app/indiana/2014/rankings/monroe/county/outcomes/overall/snapshot
Golden, S. D., Moracco, K.E., Feld, A.L., Turner, K.L., DeFrank, J.T., & Brewer, N.T. (2014). Process Evaluation of an Intervention to Increase Provision of Adolescent Vaccines at School Health Centers. Health Education & Behavior, 41(6), 625-632.
Green, L., & Kreuter, M. (2005). Community Tool Box: Section 2 PRECEDE/PROCEED. Community Tool Box. http://ctb.ku.edu/en/table-contents/overview/other-models-promoting-community-health-and-development/preceder-proceder/main
Green, L. W., & Lewis, F.M. (1986). Measurement and evaluation in health education and health promotion Palo Alto: Mayfield.
Green, L. W. K., M.W. (2004). Applications in Communities Health Program Planning: An Educational and Ecological Approach (pp. 255-311). Boston: McGraw Hill.
Hancock, T. M., M. (2008). Community health assessment or health community assessment: whose assessment? Community Organizing and Community Building for Health New Brunswick: Rutgers University Press.
Spring 2015 From Paper to Policy
45
Harris, J. H. (2001). Selecting the right vendor for your health promotion program. Absolute Advantage, 1(4), 4-5.
Hatcher, M. T. N., R.M. (2014). Engaging Communities and Building Constituencies for Public Health Novick & Morrow's Public Health Administration (pp. 391-413). Burlington: Jones and Bartlett.
Health, I. D. o. (Producer). (2015a). Infant Mortality. Indiana Department of Health Retrieved from http://www.in.gov/isdh/26283.htm
Health, I. D. o. (2015b). The Maternal and Child Health Federal-State Partnership. Maternal & Child Health (MCH) Measures. https://mchdata.hrsa.gov/TVISReports/Snapshot/SnapShot.aspx?statecode=IN
Health, I. D. o. P. (Producer). (2015). Infant Mortality Statistics. Illinois Department of Public Health. Retrieved from http://www.dph.illinois.gov/data-statistics/vital-statistics/infant-mortality-statistics
Health, I. S. D. o. (Producer). (2011). Public Health Geographics Maps Viewer. Indiana State Department of Health. Retrieved from https://gis.in.gov/apps/ISDH/MapView/index.htm
Hobbs, D. (1987). Strategy for needs assessment Needs Assessment: Theory and Methods. Ames: Iowa State University Press.
Ickrovics, J. E., Carroll-Scott, A., Peters, S.M., Schwartz, M., Gilstad-Hayden, K.,& McCaslin. C. (2014). Health and Academic Achievment: Cumulative Effects of Health Assets on Standardized Test Scores Among Urban You in the United States. Journal of School Health, 84(1), 40-48.
ILHS. (2008). Handbook for providers of healthy kids services. ILHS. http://www.hfs.illinois.gov/assets/hk200.pdf
Illinois, E. (2015). 2015 EverThrive Illinois 2015 Policy Priorities EverThrive Illinois. http://www.ilmaternal.org/docs/EverThrive-Illinois-2015-Policy-Priorities.pdf
Illinois, S. (Producer). (2015, March 2). School Based Health Services. SBHS Illinois. Retrieved from http://www.sbhsillinois.com/
Illinois, S. o. (2015). Department of Healthcare and Family Services. All Kids: Answers to Your Questions about All Kids. www.allkids.com
Inman, D. D., Van Bakergem, K.M., LaRosa, A.C., & Garr, D.R. (2011). Evidence-based health promotion programs for schools and communities. American Journal of Preventive Medicine, 40(2), 207-219.
Issel, L. M., & Fagen, M.C. (2014). Evaluation of Public Health Programs Novick and Morrow's Public Health Administration (pp. 413-430). Burlington: Jones and Bartlett Learning.
Juszczak, L., Melinkovich, P., & Kaplan, D. (2003). Use of health and mental health services by adolescents across multiple delivery sites. Journal of Adolescent Health, 32(6), 108-118.
Keeton, V., Soleimanapour, S., & Brandis, C.D. (2012). School-based health care centers in an era of health care reform: building on history. Current Problems in Pediatric and Adolescent Health Care, 42(6), 132-156.
Kidder, D. P., Wolitskim R. J., Campsmith, M.L., & Nakamura, G.V. (2007). Health status, health care, health use, medication use, and medication adherence among homeless and housed people living with HIV/AIDS. American Journal of Public Health, 97(12), 2238-2245.
Kreuger, R. A., & Casey, M. A. (2008). Focus groups. A practical guide for applied research. Thousand Oaks: Sage Publications.
Kuh, D. J., Wadsworth, M.E. (1993). Physical health status of 36 years in a British national birth cohort. Social Science Medicine, 37, 905-916.
Lane, L. (2015, February 24). MCCSC board to consider class size ratios Tuesday Night.

Spring 2015 From Paper to Policy
46
Langford, R., Bonell, C.P., Jones, H.E., Pouliou, T., Murphy, S.M., Waters, E., Komro, K.A., Gibbs, L.E., Magnus, D., & Campbell, R. (2014). The WHO Health Pormoting School framework for Improving the health and well-being of students and their academic achievement (Review). UK: Wiley.
Larson, S. A., & Chapman, S.A. (2014). Patient-centered medical home model: do school-based health centers fit the model. Policy, Politics & Nursing Practice, 1-12.
Lyon, G. R., Shaywitz, S.E., & Shaywitz, B.A. (2003). A Definition of Dyslexia. Annual Dyslexia, 53, 1-14. McAlister, A. L., Perry, C.L., & Parcel, G.S. (2008). How individuals, environments, and health behaviors
interact: Social Cognitive Theory Health Behavior and Health Education: Theory, Research, and Practice (pp. 169-188). San Francisco: Jossey- Bass.
McKenzie, J. F., Neiger, B.L., & Thacckeray, R. (2013). Evaluation: An Overview Planning, Implementing, & Evaluating Health Promotion Programs: a Primer (pp. 372-386). Boston: Pearson Education Inc.
McKenzie, J. F., Neiger, B.L., & Thackeray, R. (2013). Glossary of Terms Planning, Implementing, & Evaluating: Health promotions programs a primer (pp. 435-450). Boston: Pearson Education.
McKenzie, J. F., Neiger, B.L., Thackeray, R. (2013a). Identification and Allocation of Resources Planning, implementing & evaluating Health promotion programs: a primer (pp. 280-310). Boston: Pearson Education Inc.
McKenzie, J. F., Neiger, B.L., Thackeray, R. (2013b). Theory and Models Commonly Used for Health Promotion Interventions Planning, Implementing & Evaluating: Health Promotion Programs, a primer (pp. 162-204). Boston: Pearson Education.
McKenzie, J. F., Pinger, R.R., & Kotecki , J.E. (2012). The School Health Program: A Component of Community Health An Introduction to Community Health (pp. 145-172). Sudbury: Jones and Bartlett.
McKenzie, J. F., Pinger, R.R., & Kotecki, J.E. (2012). Health Care Delivery in the United States Community Health (pp. 369-427). Sudbury: Jones and Bartlett.
Murray, S. (Producer). (2014a, April 02). Education: Fairview Begins Literacy Program. Indiana Daily Student. Retrieved from http://www.idsnews.com/article/2014/04/fairview-begins-literacy-program
Murray, S. (Producer). (2014b, January 14). Education: Parents talk Fairview's future. Indiana Daily Student. Retrieved from http://www.idsnews.com/article/2014/01/parents-talk-fairviews-future
Mykota, D. B., & Muhajarine, N. (2005). Community resilience impact on child and youth health outcomes: a neighborhood case study. Canadian Journal of School Psychology, 20(5), 5-20.
Perry, C. L., Kelder, S.H., Murray, D.M. Klepp, K. (1992). Communitywide smoking prevention: Long-term outcomes of the Minnesota heart health program and the class of 1989 study. American Journal of Public Health, 82(1992), 1210-1216.
Prevention, C. f. D. C. a. (Producer). (2015). Adolescent and School Health: Using the School Health Index. CDC. Retrieved from http://www.cdc.gov/healthyyouth/shi/introduction.htm
Project, N. S.-B. H. C. B. a. R. (2013). At the intersection: connecting health and education data in school-based health centers. School-Community Health Alliance of Michigan. http://scha-mi.org/wp-content/uploads/2013/07/KresgeCaseStudies-FINAL.pdf
Promotion, O. o. D. P. a. H. (Producer). (2015). Healthy People 2020. Early and Middle Childhood. Retrieved from http://www.healthypeople.gov/2020/topicsobjectives2020/default
Pugh, K. R., Frost, S.J., Rothman, D.L., Hoeft, F., Del Tufo, S.N., Mason, G.F., Molfese, P.J., Mencl, W.E., Grigorenko, E.L., Landi, N., Preston, J.L., Jacobsen, L., Seidenberg, M.S., & Fullbright, R.K. (2014). Gluamate and Choline Levels Predice Individual Difference in Reading Ability in Emergent Readers. The Journal of Neuroscience, 34(11), 4082-4089.
Spring 2015 From Paper to Policy
47
Reiss, S. M., Colbert, R.D., & Herbert, T.P. (2005). Understanding resilience in diverse, talented students in an urban high chool. Roeper Review, 27(2), 110-120.
Richardson, J. E. (2008). From risk to resilience: promoting school-health partnerships for children. International Journal of Educational Reform, 17(1), 19-33.
Richardson, J. W. (2008). From Risk to Resilience: promoting school-health partnerships for children. International Journal of Educational Reform, 17(1), 19-46.
Sanders Thompson, V., Wells, A., & Coats, J. (2012). Dare to be sick: poverty and health among vulnerable populations. Advances in Education in Diverse Communities: Research, Policy and Praxis, 8, 23-47.
Schilling, T. (Producer). (2015, February 13). Monroe County Community School Corporation Health Services. Retrieved from http://www.mccsc.edu/domain/61
Services, I. D. o. H. (Producer). (2015, March 2). Public Act 95-0469. Illinois Department of Human Services. Retrieved from http://www.dhs.state.il.us/page.aspx?item=35251
Services, I. D. o. H. a. F. (2002). Handbook for providers of school based/linked health center services. Illinois Department of Hlealthcare and Family Services. http://www.allkidscovered.com/assets/102102sblhc.pdf
Services, I. D. o. H. a. F. (Producer). (2015, March 2). Mom and Babies Program for Pregnant Women. All Kids. Retrieved from http://www.allkids.com/pregnant.html
Services, U. S. D. o. H. a. H. (Producer). (2015). Healthy People 2020 MAP-IT. Program Planning: MAP-IT. Retrieved from http://www.healthypeople.gov/2020/tools-and-resources/Program-Planning
Smedley, B. D. (2008). Moving beyond access: achieving equity in state health care reform. Health Affairs, 27(2), 447-455.
Smego, R. A., & Costame, J. (1996). An academic health center--community partnership: the Morgantown health right free clinic. Academic Medicine, 71(6), 613-622.
Snowling, M. J. (1981). Phonemic deficits in developmental dyslexia. Psychological Research, 43, 219-234.
Soleimanpour, S., Geierstanger, S.P., Kaller, S., McCarter, V., & Brindis, C.D. (2010). The role of school health centers in health care access and client outcomes. American Journal of Public Health, 100(9), 1597-1603.
University, I. (2010). Monroe County Health Assessment Atlas. Health and Community Assets of Monroe County, IN. http://www.indiana.edu/~sphgis/mocha/mocha/
Vaughn, L. M., Jacquez, F., & Zhao, J. (2011). Partnering with Students to Explore the Health Needs of an Ethnically Diverse Low-Resource School. Family Community Health, 34(1), 72-84.
Vaughn, L. M., Jacquez, F., Zhao, J., & Lang, M. (2011). Partnering with students to explore the health needs of an ethnically diverse, low-resource school. Family Community Health, 34(1), 72-84.
Wade, T. J., Mansour, M.E., Guo, J.J., Huntelman, T., Line, K., & Keller, K.N. (2008). Access and utilization patterns of school-based health centers at urban and rural elmentary and middle schools. Public Health Reports, 123, 739-750.
Wadsworth, M. E. (1997). Health Inqualities in the life course perspective. Social Science Medicine, 44, 858-869.
Zlotnick, C., & Zeerger, S. (2009). Survey finding on characteristics and health status of clients treated by federally funded (US) health care for the homeless programs. Health & Social Care in the Community, 17(1), 18-26.

Spring 2015 From Paper to Policy
48
Appendix A—Geographical Maps
This study includes geographical maps to indicate the boundaries of the Bloomington
Township District(University, 2010), and Fairview Elementary School(M. C. C. S. Corporation,
2015), assets or social capital(University, 2010), and the recommended trajectory for middle and
high school(Corporation, 2013). We believe this information is critical to stakeholders in
identifying the services afforded to the community, and the need for additional services to
improve their living standards.
Appendix B
We believe these funding opportunities are best representations of our mission, goals and
objectives. They are taken from local, state and national resources and offers suggestions for
further information.

Spring 2015 From Paper to Policy
49

Spring 2015 From Paper to Policy
50
qwertyuiopasdfghjklzxcvbnmqw
ertyuiopasdfghjklzxcvbnmqwert
yuiopasdfghjklzxcvbnmqwertyui
opasdfghjklzxcvbnmqwertyuiopa
sdfghjklzxcvbnmqwertyuiopasdf
ghjklzxcvbnmqwertyuiopasdfghj
klzxcvbnmqwertyuiopasdfghjklz
xcvbnmqwertyuiopasdfghjklzxcv
bnmqwertyuiopasdfghjklzxcvbn
mqwertyuiopasdfghjklzxcvbnmq
wertyuiopasdfghjklzxcvbnmqwe
rtyuiopasdfghjklzxcvbnmqwerty
uiopasdfghjklzxcvbnmqwertyuio
pasdfghjklzxcvbnmqwertyuiopas
dfghjklzxcvbnmqwertyuiopasdfg
hjklzxcvbnmqwertyuiopasdfghjk
Appendix C—Supplemental Section
From Paper to Policy: On Proposing School-Based Health Care at Fairview
Elementary School
A Needs Assessment Featuring the PRECEDE/PROCEED Model
Spring 2015
Julius Lee

Spring 2015 From Paper to Policy
51

Spring 2015 From Paper to Policy
52
TABLE OF CONTENTS
INTRODUCTION 50-51
LITERATURE REVIEW 52-62
METHODOLOGY 63-65
DISCUSSION 66-70
LIMITATIONS 71
BIBLIOGRAPHY 72-73
TIMELINE 74-75
BUDGET 76-77
APPENDIX A—STUDY INFORMATION SHEET 78-79
APPENDIX B—FOCUS GROUP QUESTIONNAIRE 80-85
APPENDIX C—DEMOGRAPHIC QUESTIONNAIRE 86-87
APPENDIX D—RECRUITMENT LITERATURE 88-91
APPENDIX E—PAYMENT FORM 92-93

Spring 2015 From Paper to Policy
53
Introduction
School-based health centers (SBHCs) operate in nearly 2,000 schools in the United
States{Healthcare, 2009 #1;Walker, 2010 #2}.Typically providing some combination of primary
health, immunization, reproductive, and mental health services, SBHCs are intended to improve
availability of these services to children and youth who are traditionally underserved within
community health and mental health settings{Brown, 2003 #3;Walker, 2010 #2}. SBHCs have
been shown to increase access to care for high-risk groups, such as those living in high-poverty
communities, those with no health insurance, and ethnic minority youth{Allison, 2007
#4;Gance-Cleveland, 2005, Benefits of a School-based Health Center in Preschool; Juszczack,
2003, Use of Health and Mental Health Services in a Large`, Urban School District; Kaplan,
1996, Elementary School-based Health Center Use; Wade, 2008, Access and Utilization Patterns
of School-based Health Centers at Urban and Rural Elementary and Middle Schools; Silberberg,
2009, Making the Case for School-based Health: Where do We Stand?;Wade, 2008,
Improvements in Health-related Quality of Life Among School-based Health Center Users in
Elementary and Middle School; Walker, 2010, Impact of School-Based Health Center Use on
Academic Outcomes}. In partnership with schools, SBHCs could have a profound effect on
learning outcomes, which include but are not limited to poor concentration in school, attendance,
and disturbances of normal sequential cognitive development if SBHCs could build a bridge
between the health and the educational lexicon{Richardson, 2007, Building Bridges Between
School-Based Health Clinics and Schools}.
In a report from 2010-2011, there is an estimated 31 SBHCs in Indiana that receives
$2,444,594{Alliance, 2010-2011, Key SBHC Data by State}. These 31 SBHCs only represent
one-third of Indiana’s 92 counties- with some cities or towns consisting of several SBHC.

Spring 2015 From Paper to Policy
54
Further research is needed to evaluate the benefits of SBHCs particularly in Title I Elementary
Schools, because there is in addition a preponderance of evidence that academic performance is
related to health issues such as absenteeism (particularly with asthmatic youth) and conditions
such as attention deficit hyperactivity disorder, attention deficit disorder, and lead poisoning (all
of which are associated with disruptive behavior, shortened attention spans, and participation in
extracurricular activities {Guo, 2000, The Mechanisms Mediating the Effects of Poverty on
Children's Intellectual Development; Fletcher, 2004, Children's Lack of Access to Health Care as
a Barrier to Academic Performance: a Brief Summary of Issues; Geierstanger, 2004, School-
Based Health Centers and Academic Performance: Research`, Challenges`, and
Recommendations ;Raphael, 2005, Poverty and Children are a Lethal Combination; Schettler,
2000, In Harm's Way: Toxic Threats to Child Development; Richardson, 2007, Building Bridges
Between School-Based Health Clinics and Schools}). Interestingly, research is limited regarding
the parent’s perspective on the value of SBHCs and the reduction of the aforementioned health
inequities. Past studies examining preventive care from the parent perspective have been largely
quantitative and focused on information needs, satisfaction with care, and provision of services
(Radecki, 2009). Through the use of focus groups, the goal of this research is to determine their
viewpoint in terms of quality health care for their child, and answer the following research
questions:
1. What benefits would the SBHC provide parents during the school year?
2. Do parents believe a SBHC improve their child’s academic outcome?
3. In what way does a school-based health care program foster community
participation and thus support health and wellness in their students?
Spring 2015 From Paper to Policy
55
Literature Review
Physiological Development and Probable Causation
Neurological development is significant during in-utero development because it
determines physiological and cognitive development, adaptability or maladaptive behavior.
Shonkoff (2010) suggests that illnesses such as rubella or fetal alcohol syndrome can disrupt
neurological development and result in subsequent cognitive impairment during early childhood.
When early influences have been positive, physiological systems are typically healthy and
adaptive. When influences have been adverse, systems may be dysfunctional and lead to
impaired learning, maladaptive behavior, illness, disability, and a shortened lifespan {Shonkoff,
2010, Building a New Biodevelopmental Framework to Guide the Future of Early Childhood
Policy} By comparison, Duncan et.al (2010) proposes neurological development to be critical
during these years, yet associates social conditions to developmental determinants. First, family
income had consistently larger associations with measures of children’s cognitive ability and
achievement than with measures of behavior, mental health, and physical health. Second, family
economic conditions in early childhood appeared to be more important for shaping ability and
achievement than did family economic conditions during adolescence. And third, the association
between income and achievement appeared to be nonlinear, with the biggest impacts at the
lowest levels of income {Duncan, 1997, Consequences of Growing Up Poor; Duncan, 2010,
Early-Childhood Poverty and Adult Attainment`, Behavior`, and Health}. Economic deprivation
in early childhood could create disparities in school readiness and early academic success that
persist or widen over the course of childhood{Cunha, 2005, Interpreting the Evidence on Life

Spring 2015 From Paper to Policy
56
Cycle Skill Formation; Duncan, 2010, Early-Childhood Poverty and Adult Attainment`,
Behavior`, and Health}. Moreover, this adversity, also known as toxic stress, can result in further
academic impairment beyond the early childhood parameter.
Toxic stress is defined as the excessive or prolonged activation of the physiologic stress
response systems in the absence of the buffering protection afforded by stable, responsive
relationships{, 2011, Harvard University ;Garner, 2012, Early Childhood Adversity`, Toxic
Stress`, and the Role of the Pediatrician: Translating Developmental Science into Lifelong
Health}. Garner continues by describing the three tiers of toxic stress and how they can disrupt
the fluidity of neurological development and result in pathology, thereby implying a strong need
for pediatric primary care. Given the extent to which costly health disparities in adults are rooted
in these same unhealthy lifestyles and persistent inequalities, the reduction of toxic stress in
young children ought to be a high priority for medicine as a whole and for pediatrics in particular
{Shonkoff, 2009, Neuroscience`, Molecular Biology. and the Childhood Root of Health
Disparities: Building a New Framework for Health Promotion and Disease Prevention;
Braverman, 2009, Health Disparities Beginning in Childhood: a Life-Course Perspective;
Garner, 2012, Early Childhood Adversity`, Toxic Stress`, and the Role of the Pediatrician:
Translating Developmental Science into Lifelong Health}
Theoretical Lens: Eco-bio-developmental Framework
To counter toxic stress, Garner suggests applying an eco-bio-developmental (EBD)
framework. Applying the EBD framework to the challenges posed by significant childhood
adversity reveals the powerful role that toxic stress can play in disrupting the architecture of the

Spring 2015 From Paper to Policy
57
developing brain, thereby influencing behavioral, education, economic, and health outcomes
decades and generations later{Shonkoff, 2010, Building a New Biodevelopmental Framework to
Guide the Future of Early Childhood Policy;Garner, 2012, Early Childhood Adversity`, Toxic
Stress`, and the Role of the Pediatrician: Translating Developmental Science into Lifelong
Health}.
When stress is not countered, the effects can last through adulthood. Duncan et. al (2010)
describes the effects in the context of economics, morbidity, attainment, and health behavior.
Throughout their longitudinal study from birth through age 37, adults who suffer from toxic
stress during childhood did not complete their high school education, may have been
incarcerated, and have a lower income than their counterparts. In contrast to children whose
families had incomes of at least twice the poverty line during their early childhood, poor children
complete 2 fewer years of schooling, work 451 fewer hours per year, earn less than half as much,
received $826 per year more in food stamps as adults, and are more than twice as likely to report
poor overall health or high levels of psychological distress. Further, poor children have BMIs
(Body Mass Index) that are 4 points higher than those well above the poverty line, and are almost
50% more likely to be overweight as adults {Duncan, 2010, Early-Childhood Poverty and Adult
Attainment`, Behavior`, and Health}. Similarly, Shonkoff and Garner (2012) discuss these
disparities in an effort to justify early intervention—namely with pediatric health care. The
pediatric medical home of the future could offer more than the early identification of concerns
and timely referral to available programs, as enhanced collaboration between pediatricians and
community-based agencies could be views as a vehicle for testing promising new intervention
strategies rather than simply improving coordination among existing services{Shonkoff, 2012,
The Lifelong Effects of Early Childhood Adversity and Toxic Stress}.
Spring 2015 From Paper to Policy
58
Shonkoff acknowledges the challenges pediatricians face amid promoting children’s
health in the context of public policy. Although chronic difficulty in securing access to indicated
services is an important problem facing most practicing pediatricians, the limited evidence of
effectiveness for many of the options that are available (particularly in rural areas and many
states in which public investment in such services is limited) presents a serious problems that
must be acknowledged and afforded greater attention . Moreover, at this point in time, the design
and successful implementation of more effective models of health promotion and disease
prevention for children experiencing significant adversity will require more than advocacy for
increased funding. It will require a deep investment in the development, testing, continuous
improvement, and broad replication if innovating models of cross-disciplinary policy and
programmatic interventions that are guided by scientific knowledge and led by practitioners in
the medical, educational, and socials services worlds who are truly ready to work together (and
to train the next generation of practitioners) in new ways {Leslie, 2010, Members of Vision of
Pediatrics 2020 Task Force. Peering into the Future: Pediatrics in a Changing World; Starmer,
2010, Members of Vision of Pediatrics 2020 Task Force. Pediatrics in the Year 2020 and
Beyond: Preparing for Plausible Futures; Shonkoff, 2012, The Lifelong Effects of Early
Childhood Adversity and Toxic Stress}

Spring 2015 From Paper to Policy
59
Well-Child Care and School-Based Health Care Models
Nationwide, well-child care (WCC) services are available to support pediatric growth and
development. These services are available to all families but are specifically directed towards
marginalized communities who live at or below the poverty level. Well-child care includes an
array of services ranging from developmental screening to physical exams. Many parents,
however, do not have their psychosocial, developmental, and behavioral concerns
addressed{Schuster, 2000, Anticipatory Guidance: What Information do Parents Receive? What
Information Do They Want? ;Trigg, 1989, Listening Carefully. Improving Communication
About Behavior and Development; Bethell, 2004, Measuring the Quality of Preventive and
Developmental Services for Young Children: National Estimates and Patterns of Clinicians'
Performance; Coker, 2009, Low Income Parents' View on the Redesign of Well-Child Care},
many children do not receive screening for developmental delay, and many pediatricians do not
have the time, training, or financial incentives to provide recommended preventive
services{O'Conner, 2005, What to Say and When? Prioritizing and Prompting Preventive
Services (abstract);Hochstein, 2001, A Comparison of Barriers to the Provision of
Developmental Assessments and Psychosocial Screenings During Pediatric Supervision
(abstract);Coker, 2009, Low Income Parents' View on the Redesign of Well-Child Care}. As a
result, two focus groups were conducted both locally and nationally to evaluate the benefits of
well-child care from the parent’s perspective.
Coker et al. (2009) uses a convenience sample for Los Angeles residents in both the
clinical setting and through the use of mail. Potential participants were encouraged to contact the

Spring 2015 From Paper to Policy
60
study coordinator or participating pediatric center. To gain a variance in perspective, certain
conditions were needed to be fulfilled. Eligible parents spoke English or Spanish and had a child
6 months to 5 years of age. This age range was chosen to capture perspectives of a variety of
parents, from those just beginning WCC for children 0 to 3 years of age to those who had
completed it{Coker, 2009, Low Income Parents' View on the Redesign of Well-Child Care}.
Similarly, Radecki et al. (2009) facilitated recruitment in Chicago, Albuquerque and San Diego
to gain a diverse variety of perspectives. We recruited parents by flyers distributed in local
schools, libraries, health centers, churches, and day care centers rather than through physician
offices to ensure participants with a broad range of pediatric providers{Radecki, 2009, What Do
Families Want from Well-Child Care? Including Parents in the Rethinking Discussion}. Both
studies overlapped in the same objective: if we consider changes in the content and delivery of
preventive health care to better meet the needs of families, it is imperative to include the
consumers of that care, namely parents, in the conversation{Radecki, 2009, What Do Families
Want from Well-Child Care? Including Parents in the Rethinking Discussion}. Further, unlike
the local focus group who gained 56 participants, the national focus group received 101
participants. Both however, were supported by mothers. Additionally, both asked open-ended
questions to gain feedback on pediatric services. In contrast, Coker et al. itemizes the concerns of
the parents and include key directives for the moderator to further the discussion. The following
are a list of questions from the local focus group:
Topic One: Understanding/Knowledge of Well-Child Visits
Who has recently gone for one of these well-child visits? What are some of the
different things that happened during these visits? (Write down these items that
the group gives on a dry erase board or large piece of paper taped to the wall)
(If the group does not have any nonmedical items such as checking for
development, helping with parenting issues, etc. ask) What about other things like

Spring 2015 From Paper to Policy
61
checking to make sure your infant is developing normally or helping with
parenting issues like [age-appropriate topics: feeding, dealing with tantrums, toilet
training]? [Probe] Are there more examples of these types of services that your
[baby/child] might get at these visits?
Topic Three: Alternative Systems of Care—Timing and Locations
Do you know how often doctors want you to bring your infant or child in for a
well visit? (Get Response before Going On) Right now, parents go to the doctor
for visits at 2 months of age, 4 months, 6 months, 8 months, 12 months, 24
months, and 36 months (Write on Board) Do you think this is too often, not often
enough, or just right? (Probe) Why not more/less often? (Probe) Which categories
do you think that your children should not receive more or less often?
Are there other places that you can think of where you might like these well-child
care services to be given? [Probe if few responses] What about grocery stores or
discount superstores like Target or Walmart? What about at daycare centers of
schools? At home visits? At places in your neighborhoods, like community
centers or churches. [Probe} There are some clinics in stores across the country
like Wal-Mart and Target where you can use a nurse for regular healthcare things
like getting shorts or blood tests for your child. You could even get a physical
exam there. These are usually just walk-in clinics, or places where you don’t need
an appointment. You are even seen by nurses or doctor assistants, but if needed,
they can give prescriptions too. Have you heard of these clinics? Have you seen
them at your local store? Some names are Redi-Clinic, Minute Clinic, and Take
Care Clinic. Would you be interested in using these clinics for your child? Why or
Why Not? [Probe} Can you think of any reasons why you would not want to use
these clinics for your child? [Probe] What sounds good to you about these clinics?
What about them does not sound good? {If someone has gone to one of these
retail-based clinics, they can share their experience}
Are there some types of services that are better at locations outside of the doctor’s
office or clinic? What are these and why? (Probe) How would you feel about
getting some of these services in places outside of the doctor’s office or a clinic?
(If it hasn’t come up in earlier discussion, then ask Why?) What would be some of
the problems of having some of these types of services given to you at these other
places? What are some of the good things about doing things this way? {Coker,
2009, Low Income Parents' View on the Redesign of Well-Child Care}
In contrast, although Radecki’s questions fostered an active discussion, critical thinking
questions were utilized towards the parent so that s/he could reflect on her/his needs as well.
They are as follows:
Spring 2015 From Paper to Policy
62
Theme: Current Well-Child Care Experiences
What do you wish your doctor/health care provider had talked to you about at
what point in your child’s life but hasn’t? Have you tried to find information from
other sources?
Describe what a “perfect” well-child visit would be like for you and your family.
Theme: New Ways to Think About Well-Child Care
What do you think about getting information about your child’s growth and
development in other than a personal visit with your pediatrician (e.g. pediatric
nurses and nurse practitioners, social service providers, educators)? Are there
ways that you would like to get information about your child’s development and
behavior using technology such as the telephone, e-mail, or the Internet?
How can your child’s doctor best help you do a good job as a parent? {Radecki,
2009, What Do Families Want from Well-Child Care? Including Parents in the
Rethinking Discussion}
Moreover, these focus groups facilitate critical thinking in terms of providing the best
service for the child without sacrificing the parent’s needs overall. This includes communication,
awareness of appointments, and options for health care delivery that could be easier for the
parent in terms of transportation. These questions will also serve as a framework for focus
groups that will be conducted locally, which will be discussed later in the methodology section.
Although a dichotomy exists between school-based health care and the school structure,
Strolin-Goltzman (2010) suggests they are complimentary and not independent of each other.
This includes a rapport between the students and staff of the SBHCs, the high value in academia
as a result of a health facility in the school, and the SBHCs overall service to the community at
large. In summary, SBHCs are not only involved in the provision of health-related services, but
often also provide other services to the larger school community that may enhance the overall
learning environment{Strorlin-Goltzman, 2010, The Relationship Between School-Based Health
Centers and the Learning Environment}.

Spring 2015 From Paper to Policy
63
In contrast to Strolin-Goltzman’s belief that there’s a codependency between both,
Richardson (2010) believes their objectives are distinguishing determinants which therefore
results in their independence. Though it seems clear that SBHCs and schools could be partners,
the challenge lies in convincing educational leaders that time spent collaborating, space
allocation, and funding of SBHCs will not detract from student-related compliance dictated by
mandates such as No Child Left Behind (2001){Richardson, 2007, Building Bridges Between
School-Based Health Clinics and Schools}. Moreover, funding could be the reason why there are
only thirty-one SBHCs in Indiana.
Despite this dilemma, the World Health Organization (WHO, 2014) believes that school
should serve the child holistically through parameters that are tantamount to their development.
The Health Promotion Schools framework is based on an eco-holistic model, recognizing the
physical, social, mental, emotional and environmental dimensions of health and well-being
(Parsons, 1996) {Langford, 2014, The WHO health Promoting School Framework for Improving
the Health and Well-Being of Students and Their Academic Achievement (Review)}Moreover,
these values should be articulated throughout the school curriculum and the child’s community,
because otherwise they will lose credibility. To achieve this, schools should take into account the
views and opinions of the families and communities they serve, and encourage their support and
participation in health promoting activities {Langford, 2014, The WHO health Promoting School
Framework for Improving the Health and Well-Being of Students and Their Academic
Achievement (Review)}
There is a unique difference between a SBHC in a rural community compared to an urban
community. Wade et al. (2008) provides quantitative data to support the use in both communities
during a three year school period. Examples used were ethnicity, morbidity, and the use of public

Spring 2015 From Paper to Policy
64
or private health insurance. In this study, students with public health insurance or no health
insurance were more likely to utilize SBHC and had significantly higher rates of utilization
compared with students who had private insurance, suggesting improved access for these
disadvantaged groups{Wade, 2008, Access and Utilization Patterns of School-based Health
Centers at Urban and Rural Elementary and Middle Schools}. And, among social and
economically disadvantaged families, parents who are likely in lower-paying jobs with less
freedom and autonomy would not have the ability or flexibility in their work schedule to take
time off to bring their child to the doctor for health problems{Wade, 2008, Access and
Utilization Patterns of School-based Health Centers at Urban and Rural Elementary and Middle
Schools}.
By comparison, a four year longitudinal study discussed the residual benefits of SBHC on
academia—notwithstanding funding. Walker, et al. (2010) acknowledges a student’s morbidity,
but also how the SBHC’s service provides acute and immediate care to resolve it and therefore
reduce absenteeism. The results indicate that, with low to moderate effect sizes, SBHC use is
significantly associated with GPA (grade point average) and attendance gains, and that these
effects are moderated by type of use. We found that medical use was most strongly associated
with increases in attendance and mental health use was more strongly associated with increases
in GPA{Walker, 2010, Impact of School-Based Health Center Use on Academic Outcomes}.
Parental involvement is also a significant determinant in a child’s health and
consequently their academic achievement. This includes their support during the school day,
after school activities such as the PTA (Parent Teacher’s Association) and even during
homework. Bartel (2010) supports her premise through the context of the Title I Elementary
School. Whether construed as home-based behaviors (e.g., helping with homework), school-

Spring 2015 From Paper to Policy
65
based activities (e.g., attending school events), or parent-teacher communication (e.g., talking
with the teacher about homework), parental involvement has been positively linked to indicators
of student achievement, including teacher ratings of student competence, student grades, and
achievement test scores{Hoover-Dempsey, 1997, Why Do Parents Become Involved in their
Children's Education?;Bartel, 2010, Home and School Factors Impacting Parental Involvement
in a Title I Elementary School}. Parental support may facilitate success or failure of a school-
based health care center—of which will be determined in this research.
Spring 2015 From Paper to Policy
66
Conclusion
Health and education are strongly connected: healthy children achieve better results at
school, which in turn are associated with improved health later in life(Langford, 2014).
Therefore, determining a health intervention model for a child will be significant to their
development. The World Health Organization (WHO) suggests that children spend a large
proportion of their time at school and thus schools have the potential to be a powerful domain of
influence on children’s health(Langford, 2014). However, further research is needed to
determine if the school structure is ideal or impractical to providing acute care in direct
comparison to the pediatric clinic or health care center. These concerns would be best addressed
in qualitative research designs that include focus groups and are comprised of adults with
children from birth to age 12. Although this age group respectfully excludes adolescents,
research suggests that these critical years determine subsequent development in terms of
cognition and adaptive behaviors.
Spring 2015 From Paper to Policy
67
Methodology
School-based health care programs should be fundamental to all schools based on children
attending school nearly eight hours daily. Likewise, the parents of attending children would
value the use of on-site primary care facility for existing and/or sudden illnesses. Based on the
conducted literature review, focus groups should be facilitated at the local Title I Elementary
School to identify the parent’s response and evaluate its success if implemented.
In conducting this research, focus groups are optimal because they will provide parental
insight regarding the personal health of their child and options on how appropriate healthcare.
According to Krueger and Casey (2000), focus groups are carefully planned series of discussions
where participants usually are selected on the basis of a shared set of attributes. They are
designed to obtain thoughts, feelings, opinions, insights, attitudes, misconceptions, and/or beliefs
about a defined area of interest. Additionally, they take place in an informal, permissive,
nonthreatening environment, and each group conducted with a small number of people by a
skilled moderator who uses a detailed protocol{Krueger, 2000, Focus Groups: A Practical Guide
for Applied Research}.
At most, sixty participants will be recruited for the focus groups conducted at the local
elementary school. Materials such as the demographic questionnaire, focus group questions, and
recruitment literature were evaluated and approved at the Institutional Review Board (IRB) at the
Midwestern University. Following said approbation, these materials and the IRB protocol
number were disseminated to the principal and administrators at the school corporation. Focus
groups will be scheduled at the convenience of the administration, and the co-investigator will
regularly meet with the principal investigator and elementary school principal to discuss all
work.

Spring 2015 From Paper to Policy
68
At the beginning of each meeting, the moderator will read my narrative on why I am
conducting the research. He/she will then begin distributing the consent form and demographic
questionnaire to evaluate gender, race, highest education obtained, the number years their child
has attend the local elementary school, and age of child/children. In lieu of the person’s name, a
pseudonym—or number—will be used for identification. Participants at any time during the
discussion may opt out of questions or refuse to participate entirely.
After this data is collected, the moderator will inform the participants the interview will be
recorded. Before beginning the interview the moderator will ask if there are any questions the
participants have of the researcher. If there are none, they will continue with the opening general
question. The moderator will then summarize the points of the focus group and close the
discussion by asking if there are any questions. A final information sheet will be distributed to
acquire the mailing information for the participant’s address for the Kroger gift card.
The principal investigator and co-principal investigator will code all responses for emerging
themes and outliers. A code in qualitative inquiry is most often a word or short phrase that
symbolically assigns a summative, salient, essence-capturing, and/or evocative attribute for a
portion of language-based or visual data{Saldana, 2013, The Coding Manual for Qualitative
Researchers}. This information will then be analyzed with the socio-ecological framework.
According to Sallis et al. (2008), the core concept of an ecological model is that behavior has
multiple levels of influences, often including intrapersonal (biological psychological),
interpersonal (social, cultural), organizational, community, physical, environmental, and policy.
Ecological models are believed to provide comprehensive frameworks for understanding the
multiple and interacting determinants of health behaviors{Sallis, 2008, Ecological Models of
Health Behavior}. After a meticulous analysis, the information will be presented to the
Spring 2015 From Paper to Policy
69
elementary school principal and administrators for further discussion and potential
implementation.

Spring 2015 From Paper to Policy
70
Discussion
To date, four interviews were completed: two parents at said elementary school (please
see the appendix for the questions), one parent at Catholic Charities Bloomington, and a mental
health counselor between Riley Pediatrics, Catholic Charities Bloomington, and said elementary
school. No demographic information was gathered for the mental health counselor. Regarding
the parents, all three interviews were married women who had an associate’s degree or higher,
were Caucasian, one aged between 35 and 39, and the others age 40 or above. Two have children
who were in primary (defined as kindergarten to grade three) while the other was in intermediate
elementary school (defined as grades four through six). One parent was un-employed, self-
employed, and employed. Furthermore, two of the parents lived in the Bloomington Township
district, and the other parent lived outside of the district. One parent would drive her child to
school, while the other two would walk or bike via the Bloomington-line Trail (B-line Trail).
The general consensus is these parents are pleased with the local elementary school due to its
diversity and the artful learning program. When asked to define the artful learning program, the
parent says:
Artful Learning Program (A curriculum designed by Leonard Bernstein that incorporates Art
and Music in reading, writing, and mathematics. Each semester, the students have a theme that
discusses an artist. This program progresses through each grade. It aids also in diversity.
The mental health counselor also applauded the diversity at the elementary school in that the
staff supported both her transgender and foster child. Although the children are no longer
students, she says:
the social worker, nurse, and staff was very supportive in terms of mental and behavioral components of my children. As a foster parent, I experienced the behaviorisms of the child prior to adoption, and then the psychosomatic responses following adoption. I also have a child that is transgender, and was transitioning during
Spring 2015 From Paper to Policy
71
her tenure. Thanks to the staff, they would support both children and provide interventions whenever there were substitute teachers, and overall keeping them safe.
When asked whether the parents drive to the pediatrician, all three parents said yes. Two of
the parents visit Riley Pediatrics, which is within proximity of the neighborhood, while the third
mother drives to another pediatrician. Appointments generally last an hour, and longer should
further tests are necessary.
It is important to note that two interviews were conducted within two weeks of the
commencement of school. In contrast, the third interview was conducted the last week in
February. That said, only one child has been sick at school and missed school once, whereas the
other child was absent for over twenty days due to a kidney aliment. Because the child missed
over twenty days of school, the parent was referred to the social worker and warned that
subsequent absences without valid reasoning will result in referral to the Department of Family
and Child Services (DCFS). Despite said notice from the pediatrician, the parent was
reprimanded.
The mental health counselor commented on the lack of communication between Riley
Pediatrics, the local elementary school, and sometimes the parent(s). She explained that both
Riley Pediatrics and the local elementary school work independently of each other, but
the correspondence is limited. If you have a kid that comes in and they’re ill (e.g., ear infection),
they may send them to Riley Pediatrics and them a note is written to excuse them from school.
Chronic conditions are not conversed between them and the school nurse. The doctors are
saying, “here’s what we need medically and here’s a doctor’s note for the kid to be out twelve
until he gets better,” while the teachers and school nurse are saying “here’s what we need
academically.” And oftentimes there isn’t a release note indicating they need to be given the
medication three times a day, which can put a stress on a school being responsible to give the
medication. The school can call and say “here’s an issue we want you to look at without a
release of information, and most of the times there isn’t a release of information between the
two, unless the parent intervenes. For instance, if the child is ADHD and needs medication, but
the parent doesn’t know or does not want the school to know much about the child’s
medication. And the school may not know about the side effects until they reveal themselves at

Spring 2015 From Paper to Policy
72
the start of school. There isn’t a continuous line of communication between the staff,
pediatricians, and the parent.
All three parents mentioned they pick their children up from school when sick, with two
mentioning they leave work upon notice. Two parents would appreciate a pediatrician on site.
One parent says:
If the pediatrician was communicate with me via telephone, I could hear his voice and talk
with my son to detect what’s wrong, that’s different. “Is it a wet cough?” He would know what
that meant, and then monitor and get back with me in an hour.
The third parent praised her pediatrician in terms of her care when her daughter had a kidney
ailment; it’s for this reason she prefers her pediatrician at the pediatric center.
It was asked what type of care would they prefer for their child and why? One parent
described:
“I like the idea of getting the opportunity to receive the vaccinations. Because last year, son was
in fifth grade and the community health nurse came and gave all vaccinations to everyone. I loved it
because it saved time, and the $85.00 when it was state mandated unless you had religious objections.
They all got Bat-man ban-aids and it was done. I would love that option It also taught the child that
“shots are not a big deal” and it lessens the anxiety with their child. That would be great if there were
wellness checks made available at the school.”
In contrast, one parent commented on what doesn’t want for her child; she says:
“If they are stable and don’t require an epinephrine pen. I want to be called no matter what,
but broken bones should be cared for by the emergency room or urgent care facility. I wouldn’t
leave that to the pediatrician because even when I have been to the pediatrician they would send
me to the orthopedist for an X-ray.”
Finally, we asked about mental health care provisions to their child, and one parent
summarized it in the context of the Indiana State Test of Educational Progress, and the departure
of principal Tommy Richardson.
I would like to be able to participate in that service. If there was a death of a student or faculty
member here, I really believe that in part of growing a community is that grieving together and
solving a problem together , but I wouldn’t want to be subjugated to just a student with an adult. I
would like for it to be integrated in those types of settings. Like if we had a vigil, we had sessions,
and we can all grieve together and then we can all hear the same information together. So that as a
parent, I could help support with the counselors and they would give me tools to deal with it at

Spring 2015 From Paper to Policy
73
home, because grieving doesn’t just stop within the walls here, it goes wherever you are. So I
would appreciate to be a part of that. And there’s a heads up from the teachers and “I referred your
child, he’s having issues with this, I have referred him to a counselor, would you like to come
meet?” I would be okay for him to meet separately for a set week because he’s almost twelve, so
he can speak his mind and he has good boundaries but then I would want to meet with both of
them and she can say “look these are the issues and I talked to him to here’s what he said to me,
let’s meet together.” I would like to be as integrated as possible and not an in-school setting. It
should be a community outreach, because sometimes the kids will tell what’s really bothering
them before they tell their parents—say bullying-- because they’re afraid…..
The mental health counselor also alluded to the use of a case manager at the elementary
school so as to serve as a liaison between the pediatric center, elementary school and parent. She
believes that a health counselor would build trust between the parent, the elementary school, and
Riley Pediatrics, and override any extenuating circumstances- such as when there was a
tremendous turnover of staff.
Yes, considering the collaborative health care model, the case manager would keep the
school and pediatric health care abreast of the child’s health care needs. If we could have
someone to go back and forward, their very basics could be met rather than the parents
visiting the emergency room for urgent and primary care. If you have a kid going to the
emergency room for multiple breaks, MCCSC and Riley Pediatrics won’t know the
problems due to lack of communication, thus being unable to intervene.
She continues:
There has been a tremendous turnover in the staff, thus affecting the relationship between
the parents and teachers and staff. If the parent has suffered adversity, they may not wish
to discuss their challenges with the new teacher or staff member. With the turnover, the
respect isn’t there because they don’t know the staff. These staff has to “relearn” all of
these things.
The parent discusses a mental health counselor in relation to the principal’s resignation. She says:
As long as there’s communication going back and forth for like there’s an in-school- but if there’s
a big school issue…..like we should have counseling when Tommy Richardson our principal left
abruptly. And at that point we really could have used some mental health (counseling) because the
kids were just really getting attached, and then he left….And nobody really knew why. And then
the Blonde-haired lady (as described by the son) (Interim Principal Tammy Miller) who yells at
him all the time showed up and tried to change everything they have been doing. And then the
parents were getting upset.
My son has two parents who are totally involved, who makes the time, I mean we didn’t have our
kids until later on purpose, but what about the kids where that is not the construct. That is what I
Spring 2015 From Paper to Policy
74
worry about; they don’t even have the words to talk about it, and that’s why we need a mental
health professional here.
Conclusion/ Limitations
Since this feasibility was conducted, we attempted a convenience sample at our elementary
school by attending the open house and parent/teachers association meeting. Our response rate
was two parents, which resulted in further advertisement of our study. Leaflets were distributed
in newsletters to parents, indirect communication through other social service agencies, and
through direct communication. Other options included notifying other social service agencies to
encourage collaboration, but their response was less than favorable.
On January 12, 2015, the co-investigator began his internship with Catholic Charities
Bloomington, a social service agency who collaborates with the Title I Elementary School. Their
provisions include counseling, therapy, diagnostic mental exams, and other services. The co-
investigator agreed to facilitate interviews with the school’s parents who collaborate with
Catholic Charities, and the interviews would be presumably successful. Further, an amendment
was sent to the Institutional Review Board to include Catholic Charities, and to modify the
interview protocol from focus groups to a single interview. In doing so, privacy was ensured to
each participant.
Our interview goal became a limitation due to budgetary constraints and the response rate.
Notwithstanding, the women whose children attend the elementary school are concerned about
their child’s health- regardless if care is provided at a pediatric center or on-site. Similarly, the
mental health counselor provided a lens from whence her children attended, to providing health
services to the attending children. Further research is needed to promote SBHC in any—or all—
Title I Elementary Schools in marginalized communities.

Spring 2015 From Paper to Policy
75
Bibliography
Harvard University (2011, 03 08). Center on the Developing Child. Retrieved from
www.developingchild.harvard.edu
Alliance, S.-B. H. (2010-2011). Key SBHC Data by State. Washington D.C.: School-Based
Health Alliance.
Allison, M. A., Crane, L.A., Beaty, B.L. et al. (2007). School-based Health Centers: Improving
Access and Quality of Care for Low-income Adolescents. Pediatrics, 120, 887-894.
Bonell, C., Fletcher, A., Morton, M., Lorenc, T., & Moore, L. (2012). Realist randomized
controlled trials: a new approach to evaluating complex public health interventions. Soc
Sci Med, 75(12), 2299-2306. doi: 10.1016/j.socscimed.2012.08.032
Braverman, P., Barclay, C. (2009). Health Disparities Beginning in Childhood: a Life-Course
Perspective. Pediatrics, 124(Suppl 3), S163- S175.
Brown, M. B., Bolen, L.M. (2003). School-based Health Centers: Strategies for Meeting the
Physical and Mental Health Needs of Children and Families. Psychology School, 40, 279-
287.
Cunha, F., Heckman, J., J., Lochner, L., & Masterov, D. (2005). Interpreting the Evidence on
Life Cycle Skill Formation Handbook of the Economics of Education (pp. 697-812).
Amsterdam: North Holland: Elsevier B.V.
Duncan, G., J.,& Brooks-Gunn, J. (Eds.). (1997). Consequences of Growing Up Poor. New
York: Russell Sage Foundation.
Duncan, G., J., Ziol-Guest, K., M., Kalil, A. (2010). Early-Childhood Poverty and Adult
Attainment, Behavior, and Health. Child Development, 81(1), 306-325.
Fletcher, J. S. (2004). Children's Lack of Access to Health Cre as a Barrier to Academic
Performance: a Brief Summary of Issues. American Journal of Health Education, 35,
234-237.
Gance-Cleveland, B., Yousey, Y., (2005). Benefits of a School-based Health Center in
Preschool. Clinical Nursing Research, 14, 327-342.
Garner, A., S., Shonkoff, J., P., Siegel, B., S., Dobbins, M., I., Earls, M.,F., McGuinn, L.,
Pascoe, J., Wood, D. L. (2012). Early Childhood Adversity, Toxic Stress, and the Role of
the Pediatrician: Translating Developmental Science into Lifelong Health. Pediatrics,
e224- e232.
Geierstanger, S. P., Amaral, G. Mansour, M., Walters, S.R. (2004). School-Based Health Centers
and Academic Performance: Research, Challenges, and Recommendations. Journal of
School Health, 35, 36-38.
Guo, G., Harris, K.M. (2000). The Mechanisms Mediating the Effects of Poverty on Children's
Intellectual Development. Demography, 37, 431-448.
Healthcare, N. A. o. S. B. (2009). School-based health centers: national census school year 2007-
08. Washington D.C.: National Association of School Based Health Care.
Juszczack, L., Melinkovich, P., Kaplan D. (2003). Use of Health and Mental Health Services in a
Large, Urban School District. Journal of Adolescent Health, 32, 109-118.
Kaplan, D. W., Brindis, C.D., Naylor, K.E., et al. (1996). Elementary School-based Health
Center Use. Pediatrics, 6, 1-7.

Spring 2015 From Paper to Policy
76
Leslie, L., K., Slaw, K., M., Edwards, A., Starmer, A., J., &Duby, J., C. (2010). Members of
Vision of Pediatrics 2020 Task Force. Peering into the Future: Pediatrics in a Changing
World. Pediatrics, 982-988.
Raphael, S. (2005). Poverty and Children are a Lethal Combination. Journal of Child and
Adolescent Psychiatric Nursing, 18, 36-38.
Richardson, J. W. (2007). Building Bridges Between School-Based Health Clinics and Schools.
Journal of School Health, 77(7), 337-344.
Schettler, T., Stein, J., Reich, R., Valenti, M., Wallings, D. (2000). In Harm's Way: Toxic
Threats to Child Development. Boston: Greater Boston Physicians for Social
Responsibility
Shonkoff, J., P., Boyce, W., T., McEven, B., S. (2009). Neuroscience, Molecular Biology. and
the Childhood Root of Health Disparities: Building a New Framework for Health
Promotion and Disease Prevention. JAMA, 301(21), 2252-2259.
Shonkoff, J., P., & Garner, A., S. (2012). The Lifelong Effects of Early Childhood Adversity and
Toxic Stress. Pediatrics, 129, e232- e246.
Shonkoff, J. P. (2010). Building a New Biodevelopmental Framework to Guide the Future of
Early Childhood Policy. Child Development, 81(1), 357-367.
Silberberg, M., Cantor, J.C. (2009). Making the Case for School-based Health: Where do We
Stand? Journal of Health Politics and Policy Law, 33(1), 3-37.
Wade, T. J., Mansour M.E., Guo, J.J., et al. (2008). Access and Utilization Patterns of School-
based Health Centers at Urban and Rural Elementary and Middle Schools. Public Health
Report, 123, 739-750.
Wade, T. J., Mansour, M.E., Guo, J.J., et al. (2008). Improvements in Health-related Quality of
Life Among School-based Health Center Users in Elementary and Middle School.
Ambulatory Pediatrics, 8(4), 241-249.
Walker, S. C., Kerns, S.E.U.. Lyon, A.R., Bruns, E.J., & Cosgrove, T.J. (2010). Impact of
School-Based Health Center Use on Academic Outcomes. Journal of Adolescent Health,
46, 251-257.
Spring 2015 From Paper to Policy
77
Timeline
May 20, 2014: Submit proposal to Dr. Obeng
June 2, 2014: If approved, notify Monroe County Community School Corporation to
present research. If approved, commence IRB application.
June 9th
, 2014. Upon IRB approval, begin correspondence with Fairview Elementary
School to draft plan for notifying parents or guardians.
June 16th
, 2014 through August 6, 2014: Continue reviewing literature to add to existing
research. Build on Introduction and Methodology sections.
Consult Dr. Obeng for additional instruction.
August 8th
, 2014: Present research at McNair Symposium.
August 11th
: Attend PTA Meeting to Introduce my Research and the Purpose of the
Focus Groups. Further, inquire about suggested recruitment at local social service
agencies.
September, 2014: Present Preliminary research at the National McNair Research
Conference (Unless Instructed Otherwise)
October 1, 2014: Complete Focus Groups and commence analysis and coding. Complete
the last section of the research paper.
November 21, 2014: Present Research at the Indiana University Undergraduate Research
Conference
January, 2015: Continue research with Needs Assessment with Catholic Charities
Bloomington and the Indiana University School of Public Health

Spring 2015 From Paper to Policy
78
January 2015: Submit an Amendment to the Institutional Review Board to change the
interview protocol and to include Catholic Charities as an interview site.
February 8-10th
, 2015 If approved, present research at the Ethnographic and Qualitative
Research Conference
March 2015: Interpolate Feasibility Study as Supplementary Material for Needs
Assessment

Spring 2015 From Paper to Policy
79
Budget
Purchase 60 gift cards in the amount of $5.00 from Kroger. This will equal $300.00
Revision: 10 gift cards in the amount of $5.00 from Kroger; This will equal $50.00

Spring 2015 From Paper to Policy
80
Study Information Sheet
IRB STUDY #1405047790
INDIANA UNIVERSITY STUDY INFORMATION SHEET FOR
On the Value of Acute Primary Care at Title I Elementary Schools
You are invited to participate in a research study of the need for a school-based health care center at Fairview Elementary School. You were selected as a possible subject because your child or children is/are enrolled . We ask that you read this form and ask any questions you may have before agreeing to be in the study.
The study is being conducted by Julius Lee and Cecelia S. Obeng PhD from the Department of Applied Health Sciences at Indiana University. It is funded by the Ronald McNair Scholars Program.
STUDY PURPOSE
The purpose of this study is to learn more about your child or children’s health care needs and if they can be provided with an on-site pediatrician here at Fairview Elementary School. We want to know if a school-based health care center is created, what would you want and not want provided to your child.
PROCEDURES FOR THE STUDY:
If you agree to be in the study, you will do the following things:
You will participate in a focus group of five or more adults aged 18 or older. This focus group will be held at Fairview Elementary and will last thirty minutes. Participation is voluntary.
CONFIDENTIALITY
Efforts will be made to keep your personal information confidential. We cannot guarantee absolute confidentiality. Your personal information may be disclosed if required by law. Your identity will be held in confidence in reports in which the study may be published. All focus groups will be recorded and data will be saved at Indiana University Department of Applied Health Science. Once the data has been analyzed, all materials will be destroyed.
Organizations that may inspect and/or copy your research records for quality assurance and data analysis include groups such as the study investigator and his/her research associates, the Indiana University Institutional Review Board or its designees, the study sponsor, the Ronald McNair Scholars Program and the Department of Applied Health Sciences, and (as allowed by law) state or federal agencies, specifically the Office for Human Research Protections (OHRP) and the Food and Drug Administration (FDA) [for FDA-regulated research and research involving positron-emission scanning], the National Cancer Institute (NCI) [for research funded or supported by NCI], the National Institutes of Health (NIH) [for research funded or supported by NIH], etc., who may need to access your medical and/or research records.
Spring 2015 From Paper to Policy
81
PAYMENT
You will receive a $5 payment for taking part in this study in the form of a gift card from Kroger. Upon participating in the focus group, your name and address will be collected and a gift card will be mailed to you. Please allow four to six weeks for delivery.
CONTACTS FOR QUESTIONS OR PROBLEMS
For questions about the study, contact the researcher Julius Lee or Cecelia S. Obeng at 812-856-0502.
For questions about your rights as a research participant or to discuss problems, complaints or concerns about a research study, or to obtain information, or offer input, contact the IU Human Subjects Office at (317) 278-3458 or [for Indianapolis] or (812) 856-4242 [for Bloomington] or (800) 696-2949.
VOLUNTARY NATURE OF STUDY
Taking part in this study is voluntary. You may choose not to take part or may leave the study at any time. Leaving the study will not result in any penalty or loss of benefits to which you are entitled. Your decision whether or not to participate in this study will not affect your current or future relations with Fairview Elementary School, the Monroe County Community School Corporation, or Indiana University and the Department of Applied Health Science.
Spring 2015 From Paper to Policy
82
Demographic Questionnaire
Anonymous

Spring 2015 From Paper to Policy
83
Demographic Questionnaire
Appendix B
Please answer each question.
1) Gender
a) Female
b) Male
c) Transgender
2) Race or Ethnic Origin
a) Caucasion American, White—Non Hispanic
b) African American, Black—Non Hispanic
c) Hispanic or Latino American
d) Asian American
e) Other
3) Age
a) 18-21
b) 22-25
c) 26-29
d) 30-33
e) 34-37
f) 38 and older
4) Marital Status
a) Single
b) Married
c) Divorced
d) Widowed

Spring 2015 From Paper to Policy
84
5) Smoker
a) Yes
b) No
6) What best describes your current living situation?
a) Living with parents
b) Living alone
c) Living with a roommate
d) Living with a spouse and children
e) Living with a domestic partner and her/his children from a previous
relationship.
7) What is the highest level of Education you have completed?
a) Less than high school
b) Graduated high school
c) GED degree
d) Some vocational or technical school
e) Completed vocation or technical school certificate
f) Some college
g) AA degree (two year college degree)
h) BA or BS (four year college degree)
i) Some graduate school
j) Completed graduate degree

Spring 2015 From Paper to Policy
85
8) Employment
a) Unemployed
b) Employed
c) Self-Employed
9) Considering all of your employment, how many hours per week do you usually
work?
a) I am not currently employed
b) Less than 10 hours
c) 10-20 hours
d) 21-30 hours
e) 31-40 hours
f) More than 40
10) How many children do you have?
a) One child
b) Two
c) Three
d) Four

Spring 2015 From Paper to Policy
86
11) Are you a step-parent?
a) Yes
b) No
12) Are you a foster parent?
a) Yes
b) No
13) Do You have Health Insurance
a) Yes
b) No

Spring 2015 From Paper to Policy
87
Appendix C—Focus Group Questions
Theme: General Questions Concerning Fairview School
1. What do you like most about Fairview Elementary School?
2. What does your child like most about Fairview?
3. How far do you live from Fairview?
(Probe: If they live far, ask how their child travels to school)
Theme: General Child Wellness
4. How often does your child visit your pediatrician?
5. How far do you live from the pediatrician?
6. Do you drive to the office? (Probe: Ask if any get the bus, cab or walk)
7. How long are the appointments? (Probe: Ask if walk-in hours are available)
8. If your child needs a prescription, where do you go? (Probe: Offer CVS or
Kroger as examples)
Theme: Child Illness and School
9. In the past two weeks, how often was your child sick at school? (Correlated with
Question 10)
10. In the past two weeks, how many days was your child absent from school?
11. When your child is sick is at school, do you immediately take him/her to the
pediatrician? Probe: Why or Why not?
12. If your child is sick at school, do you leave work to pick him/her up?
Spring 2015 From Paper to Policy
88
13. If there was a pediatrician at Fairview, what care would you want for your child?
14. Why?
15. In terms of pediatric care at Fairview, is there anything you do not want for your
child?
16. Why Not?
Follow Up Questions:
If necessary, return to questions that generated a follow up question.

Spring 2015 From Paper to Policy
89
Appendix D—Recruitment Literature
Parent and Teacher Association—Recruitment Letter
Hello, my name is Julius Lee and I am a senior majoring in Community Health at Indiana
University. I am also an undergraduate researcher with the Ronald E. McNair Scholars Program.
I am working on a feasibility study concerning a preventive health care program here at Fairview
in that it would provide health care to your children. Specifically, if your child gets sick in class,
or at home, would an onsite pediatrician in addition to the school nurse be ideal.
My research project requires the participation of parents or guardians of children only attending
Fairview School, who will participate in a focus group. This group will answer questions
concerning preventive health care for their child or children. Also, you will answer questions on
what type of care would you want provided to your child. Lastly, you will answer questions
concerning your satisfaction with Fairview Elementary School.
As a thank you, you will receive a $5 gift card from Kroger.
Do you have any questions?

Spring 2015 From Paper to Policy
90
School-Based Health Care at Fairview
Join Us for a Discussion on: Place: For More Information, Contact Julius Lee at 812-856-0502 or [email protected]
Spring 2015 From Paper to Policy
91
YOUR OPINION MATTERS:
JOIN US FOR A DISCUSSION ON SCHOOL-BASED HEALTH CARE HERE AT FAIRVIEW ELEMENTARY SCHOOL Date and Time: Place: For More Information, contact Julius Lee at 812-856-0502 or [email protected]
Spring 2015 From Paper to Policy
92
Join Us for a Discussion on Health Care and Your Child When: Time: Place: For More Information, Contact Julius Lee at the Department of Applied Health Science 812-856-0502 or [email protected]

Spring 2015 From Paper to Policy
93
Appendix E—Payment Form
A FEASIBILITY STUDY ON THE USE OF SCHOOL-BASED HEALTH CARE AT FAIRVIEW ELEMENTARY SCHOOL
PAYMENT AND LOCATING INFORMATION FORM
PLEASE COMPLETE AND RETURN THIS FORM
PART A: PAYMENT FORM
We want to be sure you receive your payments promptly! Please complete the section below with the
mailing address where you would like us to send your payments, and your most current email address.
Print Name: ___________________________________________________
Address: ______________________________________________________
City: ______________________ State: __________ Zip Code: _________
Home Phone: (____) ____________ Cell Phone: (____) ____________
Email Address: _________________________________________________
Signature: ____________________ Date: _______________
PART B: ALTERNATE CONTACT INFORMATION
Spring 2015 From Paper to Policy
94
Just in case we lose touch with you before the study is complete, please provide the name and phone
number of a significant person in your life who does not live with you and will know how to reach you if
you move or change phone numbers.
Name of Family Member or Close Relation/Friend (who does not live with you):
________________________________________________________________ Phone Number: (_____) _______________
Thank you very much for your help! IRB Protocol Number 1405047790