open enrollment 2012. health care commission (hcc) approved employee & employer rates – agency...
Post on 21-Dec-2015
213 views
TRANSCRIPT

Open Enrollment 2012

Health Care Commission (HCC) • Approved employee & employer rates
– Agency composite rates increases • 12.5% on 7/1/10• 15% on 7/1/11• 7.5% on 7/1/12
– Return to the 95/55 employer contribution• Coverage cost for employee-only will increase
– Actual increase depends upon plan, tier and coverage level
• Continue to provide a 55% contribution toward dependent coverage
Other HCC Action• No plan design changes for Plans A and B• Plan design changes for Plan C pharmacy
benefit• Added Stormont-Vail HealthCare as a regional
preferred lab vendor • Quest will continue to offer a statewide
preferred lab option• Added the HealthQuest Rewards Program

Legislative Changes• Autism Spectrum Disorder Pilot
– Benefit will be continued for 2012
• Limits placed on SEHP coverage for abortions– Only covered to protect life of the mother

2012 SEHP Medical Plans• All plans are Preferred Provider Organizations
(PPO)– Claims paid based on the network status– Network providers accept the plan allowance as
payment in full– Non Network Providers can balance bill– All plans include preventive care
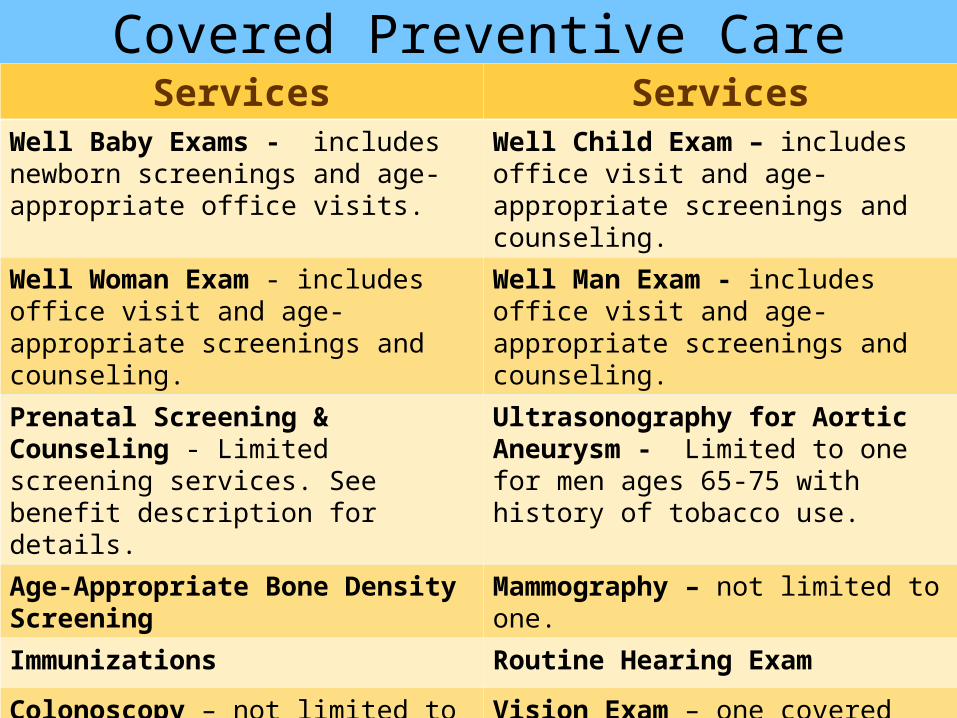
Covered Preventive CareServices Services
Well Baby Exams - includes newborn screenings and age-appropriate office visits.
Well Child Exam – includes office visit and age-appropriate screenings and counseling.
Well Woman Exam - includes office visit and age-appropriate screenings and counseling.
Well Man Exam - includes office visit and age-appropriate screenings and counseling.
Prenatal Screening & Counseling - Limited screening services. See benefit description for details.
Ultrasonography for Aortic Aneurysm - Limited to one for men ages 65-75 with history of tobacco use.
Age-Appropriate Bone Density Screening Mammography – not limited to one.
Immunizations Routine Hearing Exam
Colonoscopy – not limited to one. Vision Exam – one covered per person per year
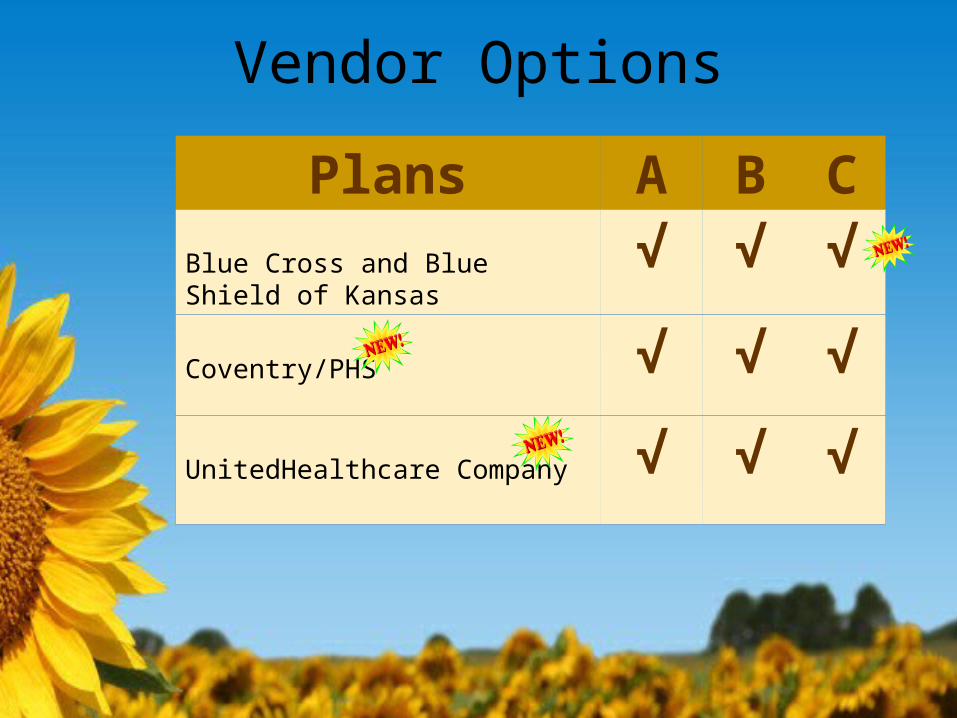
Vendor Options
Plans A B CBlue Cross and Blue Shield of Kansas √ √ √
Coventry/PHS √ √ √
UnitedHealthcare Company √ √ √
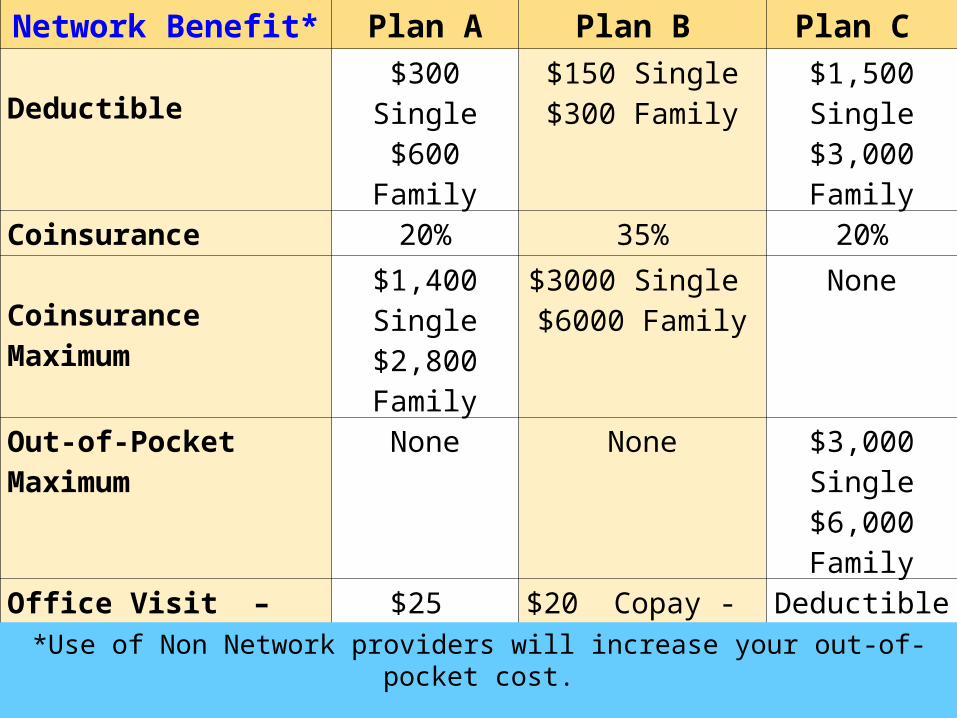
Network Benefit* Plan A Plan B Plan C
Deductible$300 Single$600 Family
$150 Single$300 Family
$1,500 Single$3,000 Family
Coinsurance 20% 35% 20%
Coinsurance Maximum$1,400 Single$2,800 Family
$3000 Single $6000 Family
None
Out-of-Pocket Maximum None None $3,000 Single$6,000 Family
Office Visit – Primary Care Providers
$25 Copay $20 Copay - Adult$10 Copay - children < age 19
Deductible & Coinsurance
Office Visit - Specialist $45 Copay $40 Copay - Adult $25 Copay - Children < age 19
Deductible & Coinsurance
Preferred Lab Benefit Yes Yes No
*Use of Non Network providers will increase your out-of-pocket cost.

Selecting a Medical Plan1. Pick a plan design (A, B or C)
– Which plan design provides the coverage you and your family need?
2. Review the Provider Networks – Each of the medical plans uses a different provider
network
3. Review the other services each medical plan offers
4. Review the premiums
Quest Diagnostics
www.labcard.com
Stormont-Vail HealthCare• Stormont-Vail HealthCare is a new regional
preferred lab vendor in NE Kansas.• 100% coverage for eligible outpatient lab tests • All Plan A and B members may use the
Stormont-Vail draw site locations.• Labs drawn at other Cotton-O’Neil locations
may be included if by network providers.• Covered lab procedures are covered at 100%.
– Show your medical ID card to access benefit.
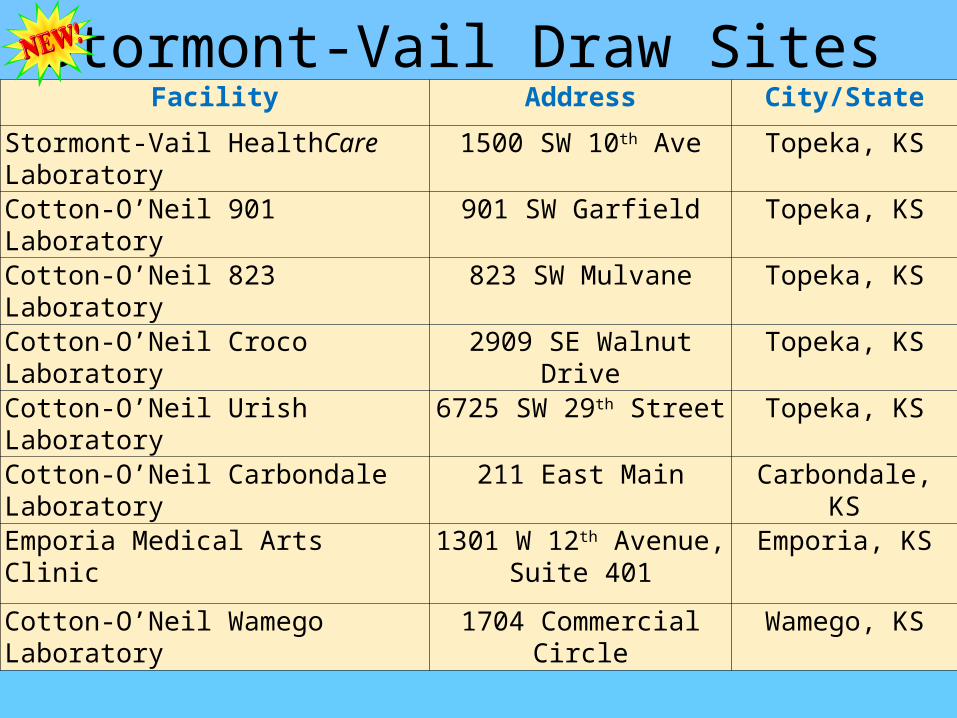
Stormont-Vail Draw Sites Facility Address City/State
Stormont-Vail HealthCare Laboratory 1500 SW 10th Ave Topeka, KS
Cotton-O’Neil 901 Laboratory 901 SW Garfield Topeka, KS
Cotton-O’Neil 823 Laboratory 823 SW Mulvane Topeka, KS
Cotton-O’Neil Croco Laboratory 2909 SE Walnut Drive Topeka, KS
Cotton-O’Neil Urish Laboratory 6725 SW 29th Street Topeka, KS
Cotton-O’Neil Carbondale Laboratory 211 East Main Carbondale, KS
Emporia Medical Arts Clinic 1301 W 12th Avenue, Suite 401
Emporia, KS
Cotton-O’Neil Wamego Laboratory 1704 Commercial Circle Wamego, KS
Plans A & B Drug BenefitGeneric Drugs
– 20% CoinsurancePreferred Brand
– 35% CoinsuranceNon Preferred Brand
– 60% CoinsuranceSpecial Case Medications
– 25% to a max of $75 per 30-day supply
www2.caremark.com/kseUp to a sixty (60) day supply of most drugs available
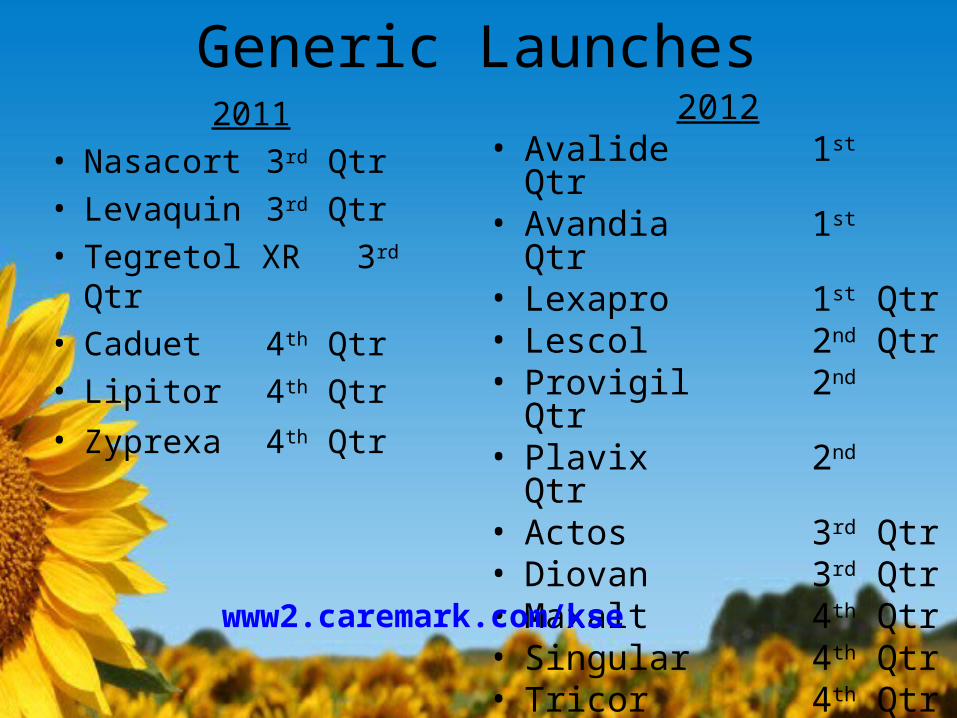
Generic Launches 2011
• Nasacort 3rd Qtr
• Levaquin 3rd Qtr
• Tegretol XR 3rd Qtr• Caduet 4th
Qtr• Lipitor 4th Qtr• Zyprexa 4th
Qtr
2012• Avalide 1st Qtr• Avandia 1st Qtr• Lexapro 1st Qtr• Lescol 2nd Qtr• Provigil 2nd Qtr• Plavix 2nd Qtr• Actos 3rd Qtr• Diovan 3rd Qtr• Maxalt 4th Qtr• Singular 4th Qtr• Tricor 4th Qtr
www2.caremark.com/kse
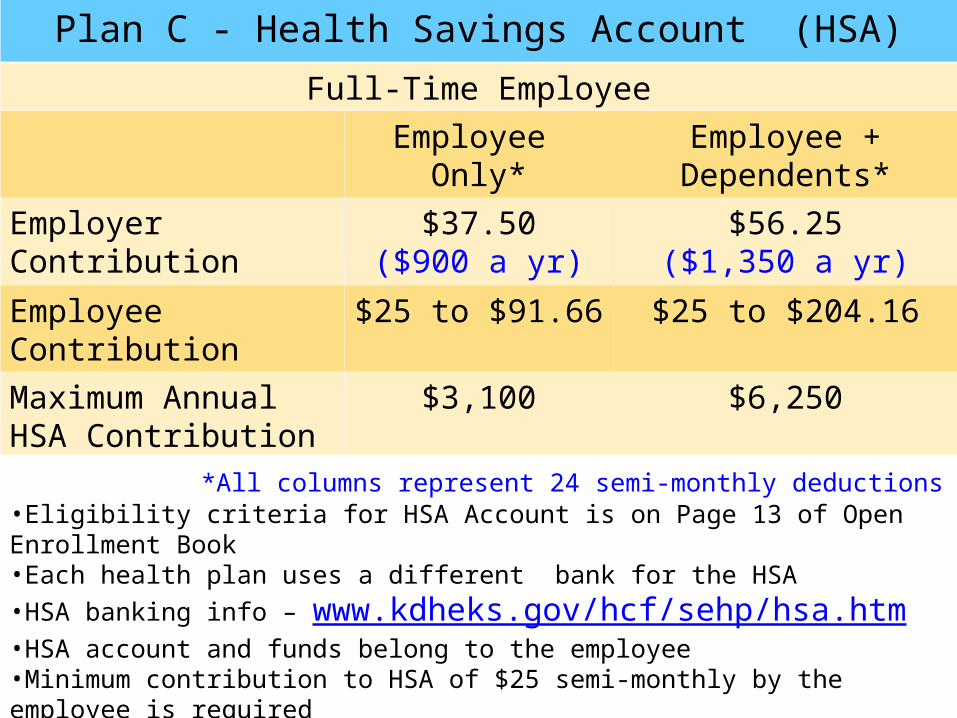
Plan C - Health Savings Account (HSA)
Full-Time EmployeeEmployee
Only*Employee +
Dependents*Employer Contribution $37.50
($900 a yr)$56.25
($1,350 a yr)
EmployeeContribution
$25 to $91.66 $25 to $204.16
Maximum Annual HSA Contribution
$3,100 $6,250
*All columns represent 24 semi-monthly deductions •Eligibility criteria for HSA Account is on Page 13 of Open Enrollment Book•Each health plan uses a different bank for the HSA •HSA banking info – www.kdheks.gov/hcf/sehp/hsa.htm•HSA account and funds belong to the employee•Minimum contribution to HSA of $25 semi-monthly by the employee is required

Plan C Drug Plan• Plan C now has a Coinsurance Drug Plan• Drugs are subject to the Deductible, then:
– Generic 20% Coinsurance– Preferred Brand 35% Coinsurance– Non Preferred Brand 60% Coinsurance– Special Case Drugs 25% Coinsurance to a
max of $75
• Generic Incentive Provision• Not creditable coverage

Plan C Chronic Care BenefitPrescription Drugs for:
Prescription Drug Product
Member ResponsibilityPer 30-Day Supply
Diabetes
Generic Drug Deductible and then 10%to a maximum of $10
Preferred Brand Drug
Deductible and then 20% to a maximum of $20
Asthma
Generic Drug Deductible and then 10% to a maximum of $10
Preferred Brand Drug
Deductible and then 20% to a maximum of $20

Dental Coverage• Plan pays in full for two exams & cleanings
per person per year • Plan Deductible
– Applies to Basic & Major Restorative Care– $50 per person, maximum of 3 per family
• Orthodontic benefit – $1,000 per person per lifetime
• Annual benefit maximum– $1,700 per person per year
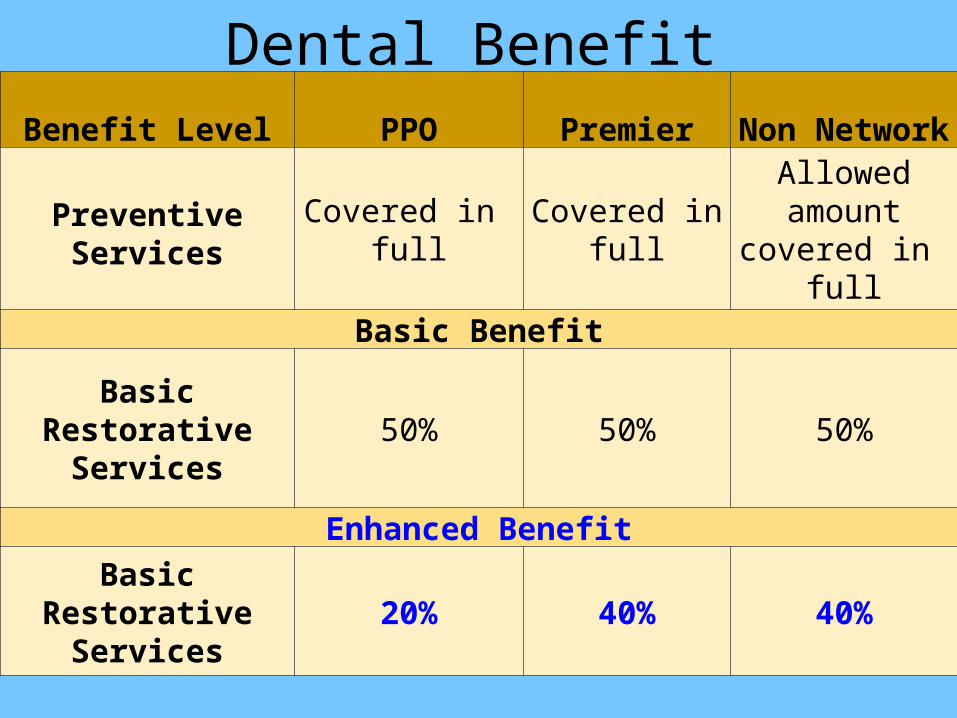
Dental BenefitBenefit Level PPO Premier
Non Network
Preventive Services
Covered in full
Covered in full
Allowed amount
covered in full
Basic Benefit
Basic Restorative
Services50% 50% 50%
Enhanced BenefitBasic
Restorative Services
20% 40% 40%
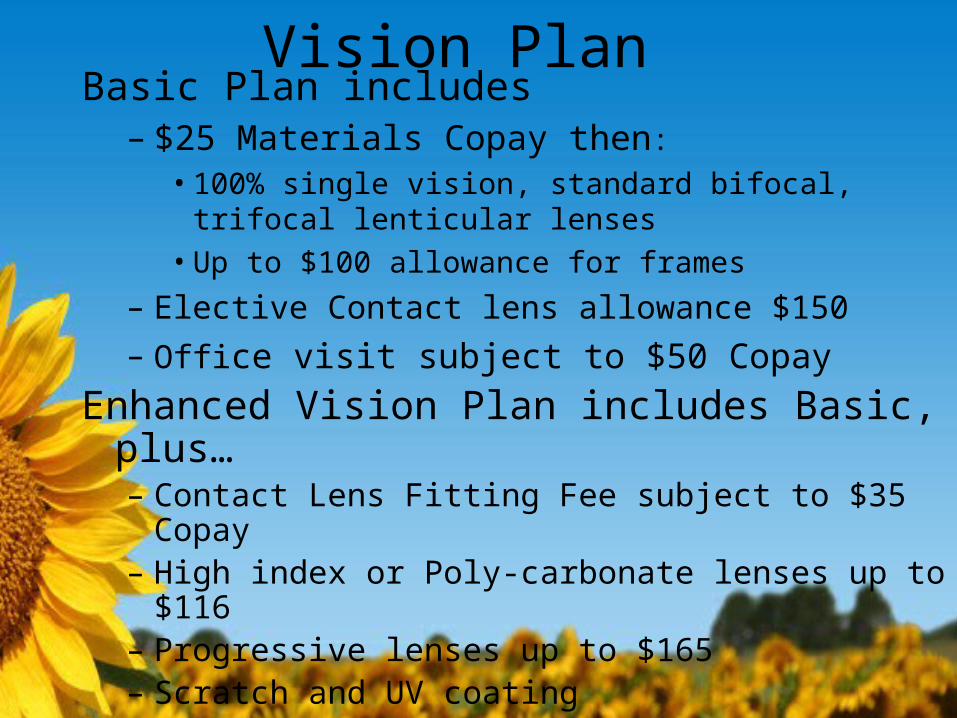
Vision PlanBasic Plan includes
– $25 Materials Copay then:• 100% single vision, standard bifocal, trifocal lenticular
lenses• Up to $100 allowance for frames
– Elective Contact lens allowance $150– Office visit subject to $50 Copay
Enhanced Vision Plan includes Basic, plus…– Contact Lens Fitting Fee subject to $35 Copay– High index or Poly-carbonate lenses up to $116– Progressive lenses up to $165 – Scratch and UV coating

Flexible Spending Accounts• Health Care Flexible Spending Account
– For Plan A and B members only – Grace period for Health Care FSA– Debt Card available
• Dependent Care Flexible Spending Account– For Child care expenses
• Pre-tax contributions– Up to $5,000 per account per year
• Details on eligible expenses available at:www.asiflex.com

Optional HCFSA Debit Card• Visa card to access funds
– Documentation may still be required by ASI
• Debit card election form is mailed to you– You pay a $12 nonrefundable service fee per
year
• Debit card enrollment rolls from year to year– Current debit card users must contact ASI to
cancel debit card enrollmentwww.asiflex.com

Limited FSA for Plan C• Can set aside funds for dental and vision
expenses only• Cannot be used for medical expenses
– HSA account is designed for that purpose
• Debt card not available • “Use it or lose it” applies to this account
– Funds must be used by December 31 each year
Open Enrollment• Enroll online:
– Make health plan selections– Add/drop dependents– Declare tobacco status – Enroll in Flexible Spending Accounts– Enroll in HealthyKIDS
• Families at 250% of poverty level• State pays 90% of children’s premium• Enroll at: https://khap.kdhe.state.ks.us/hkapplication/
– Coverage effective January 1, 2012

Required Documentation• If you are adding a dependent, documentation
of eligibility is required. Provide copies of:– Birth certificates – Marriage licenses– Affidavit of common law marriage– Social Security numbers required
• Document due by 10/31/11 to HR office
Defaults• Members currently enrolled in UMR who do not
make an enrollment election will have United HealthCare for 2012.
• Members currently enrolled in Preferred Health Systems who do not make an enrollment election will have Coventry/PHS for 2012.
• If you fail to make a tobacco use election you will be defaulted to paying the base rates in 2012.
Identification Cards• All medical plans are issuing new ID cards.• Delta Dental is issuing new ID cards. • Lab, Vision and Drug are not issuing new cards

Resources• Review the Open Enrollment (OE) booklet• ?’s: Call the health plan customer service
– Phone numbers in the front of the OE booklet
• Visit the website: www.kdheks.gov/hcf/sehp.htm– Benefit descriptions available– Provider directory listings– Preferred drug list– Information on the HSA and FSA accounts
• Email ?’s to SEHP: [email protected]

Questions?

Option Slides
Primary Care Providers (PCPs)• General practice• Family practice• Geriatrics
• Internal medicine• Physician extenders• Pediatrics
• Plans A & B only• PCPs have lower office visit copays • Member may have more than one PCP• No referrals required

Network vs. Non NetworkPlan A - Non Network Provider
Service on 1/2/2011Plan Pays
Member Pays
Provider Write-Off
Billed Charge $1,500
Allowed Charge $1,400 $100 $0
$500Deductible ($500) $500
50% Coinsurance $900 $ 450 $450
Total $450 $1,050 $0
Plan A - Network Provider
Service on 1/2/2011 Plan PaysMember
PaysProvider Write-Off
Billed Charge $1,500
Allowed Charge $1,400 $100
$300 Deductible ($300) $300
20% Coinsurance $1,100 $880 $220
Total $880 $520 $100

Plan A – Network Providers• Office Visit Copays
– $25 for Primary Care Office Visits– $45 for Specialist Office Visits
• $300/$600 Deductible • 20% Coinsurance• Coinsurance Max $1,400/$2,800
• Preventive Care Services paid at 100%
• Lab Card Benefit

Plan B – Network Providers• Primary Care Office Visits
– $20 Copay for Adults – $10 Copay for Children <age 18
• Specialist Office Visits– $40 Copay for Adults– $25 Copay for Children <age 18
• $150/$300 Deductible• 35% Coinsurance• Coinsurance max $3,000/$6,000
• Preventive Care Services paid at 100%
• Lab Card benefit
Plans A & B Non Network Providers• $500/$1,500 Deductible• 50% Coinsurance• Coinsurance Max $3,650/$7,300• Non Network Providers can balance bill• Preventive care not covered

Preferred Lab Benefit Expanded
• Available on Plans A and B only• 100% coverage for eligible outpatient lab tests •Two vendors participating in the program
– Quest Diagnostics -- Statewide/Nationwide access– Stormont Vail Healthcare -- Regional access
Stormont-Vail HealthCare• Stormont-Vail HealthCare is a new regional
preferred lab vendor in NE Kansas.• Cotton O’Neil patients will automatically
participate • Non Cotton O’Neil patients in Plans A or B may
visit one of the 8 draw site locations– Take your Medical ID card– Photo ID– Doctor’s Lab orders
• Covered lab procedures are covered at 100%.
Plan C w/ Health Savings Account• Network Provider Coverage
– $1,500/$3,000 Deductible– 20% Coinsurance– $3,000/$6,000 Out-of-Pocket Maximum– Preventive Care Services paid at 100%
• Non Network Provider Coverage– $2,000/$4,000 Deductible – 50% Coinsurance– $3,650/$7,300 OOP Maximum – Preventive Care is not covered

Dental Preventive Care• Covered in full:
– Prophylaxis/cleanings – twice per year.– Oral examinations – twice per year.– Bitewing x-rays –
• adults – 1 x a year • children under 18 - 2 x a year
– Full mouth x-rays – once each five (5) years.– Limited coverage for children only:
• Sealants• Space maintainers• Topical fluoride
– Ancillary – emergency relief of pain.

Dental Restorative Services• Basic Restorative
– Regular restorative dentistry – fillings– Oral surgery– Endodontics – root canals – Periodontics – treatment of gum & bone disease– Additional diagnostic X-Rays
• Major Restorative– Special restorative dentistry – crowns– Prosthodontics – bridges, implants, dentures– TMJ Treatment – Requires prior authorization
Restorative care is subject to a $50 deductible

Dependent Eligibility Change• Effective 1/1/11, dependents are eligible to
be covered on the plan to age 26 even if:– they do not live with you– they are not a student– they are not dependent on you for support, or– are married
• Spouses of dependents are not eligible.• Grandchildren are only eligible under limited
circumstances.
• You can add coverage for your eligible dependents during this Open Enrollment.