oral final 16
TRANSCRIPT

RADS – 216 Image Evaluation:
Radiograph Oral Presentation
Image Evaluation of the Hand, AP External
Oblique 45°By: Melissa Krezel

Is the Image HIPAA Compliant?
The image is HIPAA compliant.
All patients health information is
properly protected while allowing
the flow of health information
needed to provide and promote
high quality health care and to
protect the patients health and
well being.
The image does NOT violate
patient confidentially.

Marker & Patient ID
A right anatomical side marker is
visible in the image.
The marker is positioned so it is on
the viewers left side.
The technologists ID is included but
covered for confidential reasons.
The marker does NOT superimpose
any pertinent anatomy.
“A best practice on digital
radiography is the consistent use of
lead anatomic side markers
captured on the original image
during the x-ray exposure.”
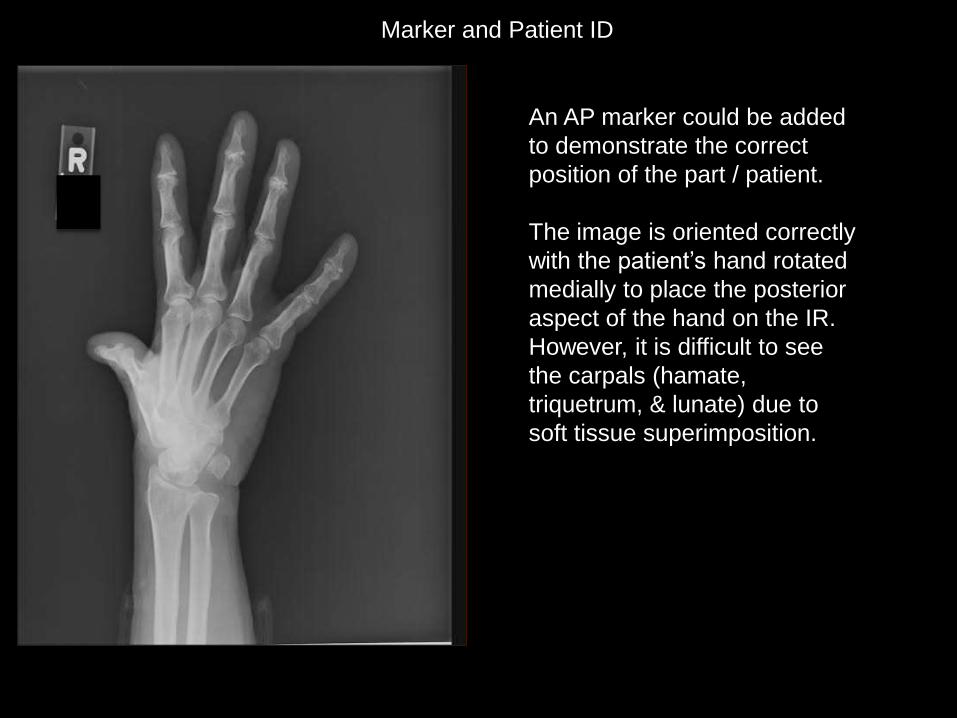
Marker and Patient ID
An AP marker could be added
to demonstrate the correct
position of the part / patient.
The image is oriented correctly
with the patient’s hand rotated
medially to place the posterior
aspect of the hand on the IR.
However, it is difficult to see
the carpals (hamate,
triquetrum, & lunate) due to
soft tissue superimposition.

Radiation Hygiene Masking, shuttering, or cropping should NOT be
used as replacements for beam restriction
achieved through physical collimation of the x-
ray field size.
Beam restriction rule: Three sides of beam
restriction MUST be visible.
This image DOES have adequate three sided
beam restriction /collimation. The superior,
medial, and inferior aspect of the image displays
appropriate collimation.
“A best practice in digital radiography is the use
of secondary lead shielding for anatomic parts
that are adjacent to the x-ray field.”
Gonadal shielding rule: Shielding must be
provided if the gonads are within 5 cm of the
primary beam.
The image does in fact display evidence of
appropriate use of shielding because beam
restriction is visible on the medial, superior, &
lateral side of the IR, but should also have
included lateral aspect too.
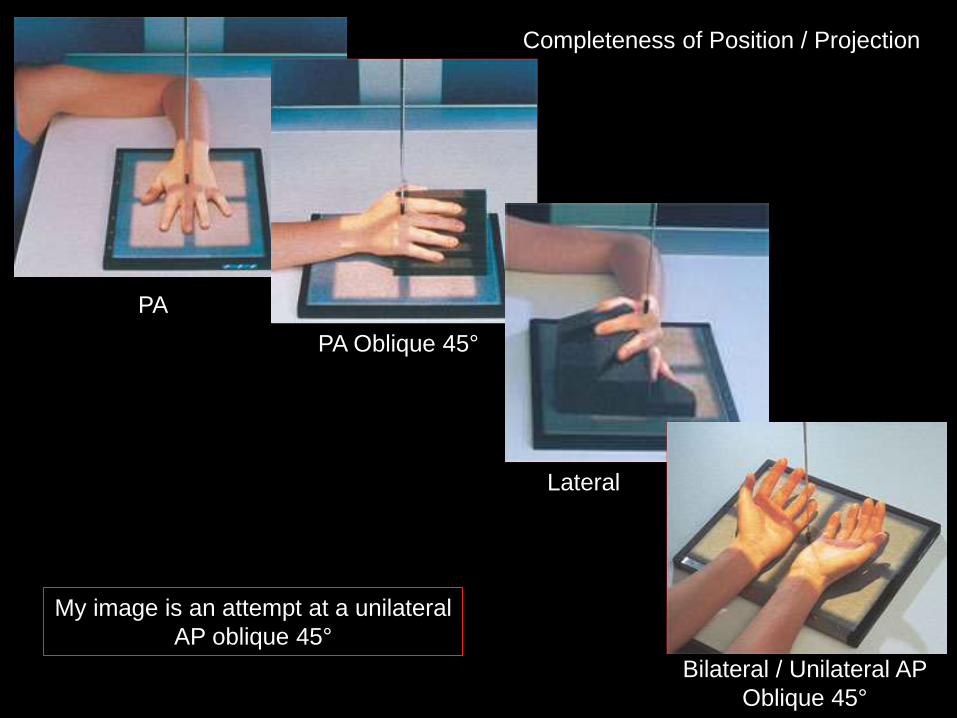
Completeness of Position / Projection
PA
PA Oblique 45°
Lateral
Bilateral / Unilateral AP
Oblique 45°
My image is an attempt at a unilateral
AP oblique 45°
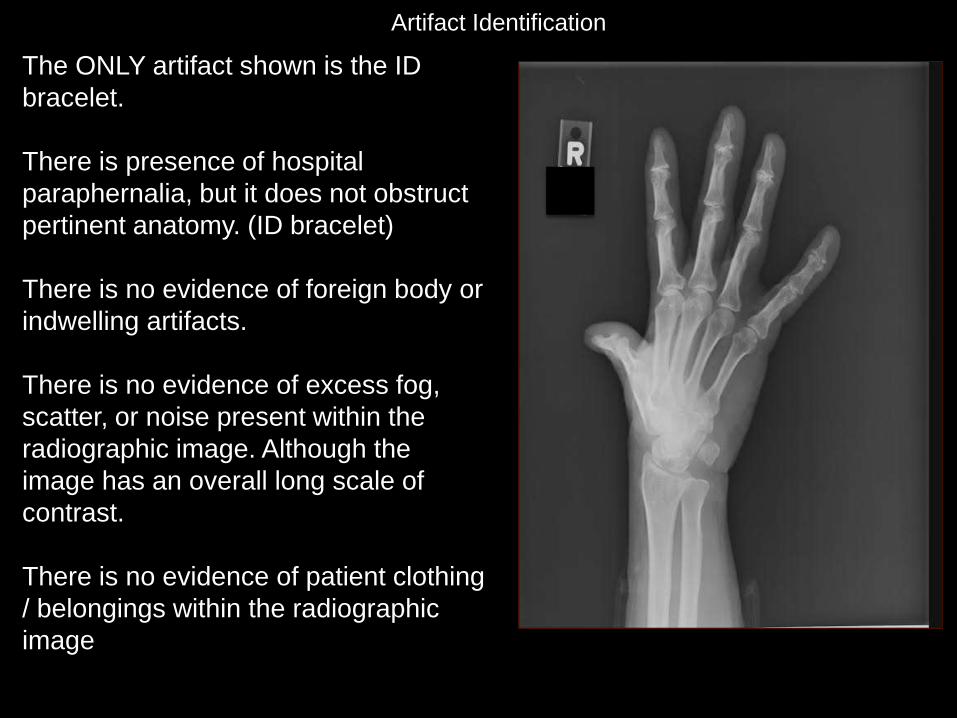
Artifact Identification
The ONLY artifact shown is the ID
bracelet.
There is presence of hospital
paraphernalia, but it does not obstruct
pertinent anatomy. (ID bracelet)
There is no evidence of foreign body or
indwelling artifacts.
There is no evidence of excess fog,
scatter, or noise present within the
radiographic image. Although the
image has an overall long scale of
contrast.
There is no evidence of patient clothing
/ belongings within the radiographic
image

Image Sharpness
There is NO gross voluntary motion visible
on the image.
There is NO excessive quantum mottle
present within the image, although the
image lacks overall spatial resolution.
There is NO evidence of double or
previous/ ghosted exposure.
No evidence of CR/DR artifacts.
Grid lines, grid artifact, or grid cut-off are
NOT visible in the image. A grid is NOT
used when imaging an oblique hand.
Size distortion does NOT appear to be
greater then expected.
There is NO evidence of shape distortion.

Accurate Part Positioning The part is not adequately centered to the
IR’s longitudinal axis. (white line)
The part is off centered to the IR (red lines)
The CR is centered to the IR (red lines)
The CR is NOT correctly centered over the
base of the 3rd metacarpal. (red lines)
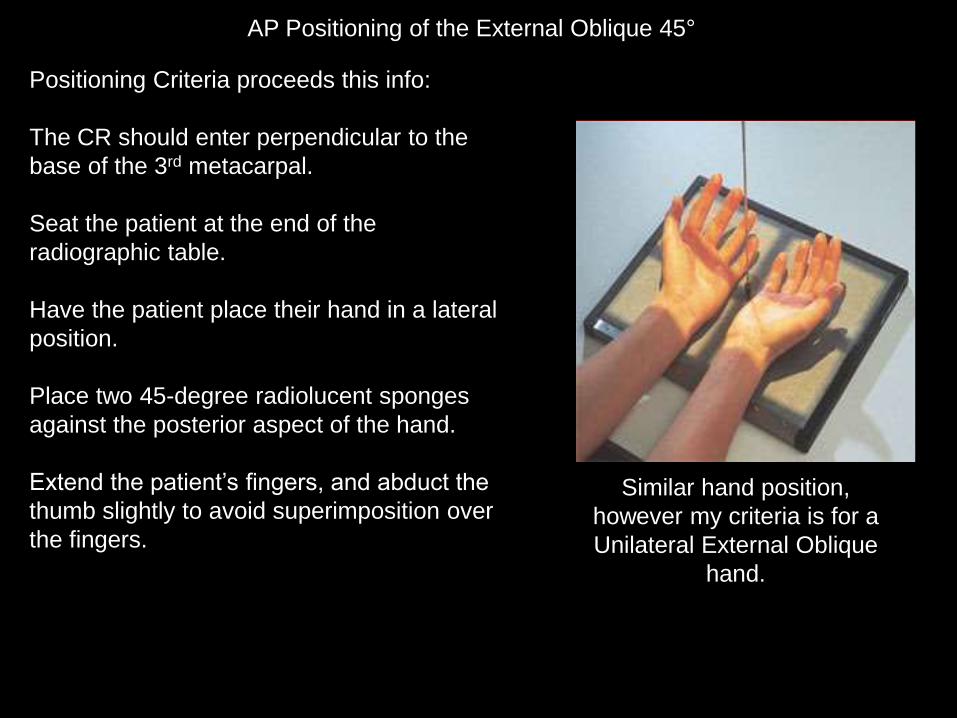
AP Positioning of the External Oblique 45°
Positioning Criteria proceeds this info:
The CR should enter perpendicular to the
base of the 3rd metacarpal.
Seat the patient at the end of the
radiographic table.
Have the patient place their hand in a lateral
position.
Place two 45-degree radiolucent sponges
against the posterior aspect of the hand.
Extend the patient’s fingers, and abduct the
thumb slightly to avoid superimposition over
the fingers.
Similar hand position,
however my criteria is for a
Unilateral External Oblique
hand.

Accurate Part Positioning
Is the part accurately positioned based on this criteria?
The part is NOT correctly positioned
based on criteria listed on the previous
slides.
The CR needs to be centered over the
base of the 3rd metacarpal.

Does the CR’s Alignment Conform to an Accepted IR Exposure Field
Recognition Template / Field?
Yes, the image displays (3) sides of
beam restriction, However, the
medial side is not parallel to the
adjacent IR edge. The side closest
to the gonads has proper beam
restriction.
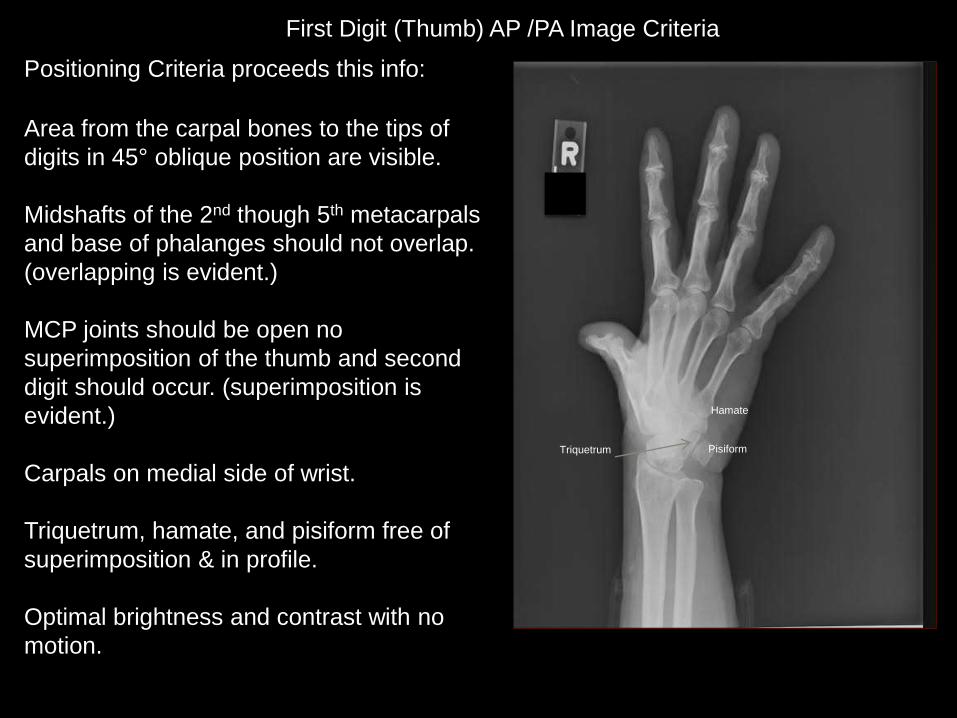
First Digit (Thumb) AP /PA Image Criteria
Positioning Criteria proceeds this info:
Area from the carpal bones to the tips of
digits in 45° oblique position are visible.
Midshafts of the 2nd though 5th metacarpals
and base of phalanges should not overlap.
(overlapping is evident.)
MCP joints should be open no
superimposition of the thumb and second
digit should occur. (superimposition is
evident.)
Carpals on medial side of wrist.
Triquetrum, hamate, and pisiform free of
superimposition & in profile.
Optimal brightness and contrast with no
motion.
Pisiform
Hamate
Triquetrum

Judicious Exposure Technique
Most Radiolucent structure: soft
tissue and the joint spaces.
Most Radiopaque structure: bony
cortex– but the image lacks overall
contrast and the cortex is not visible.
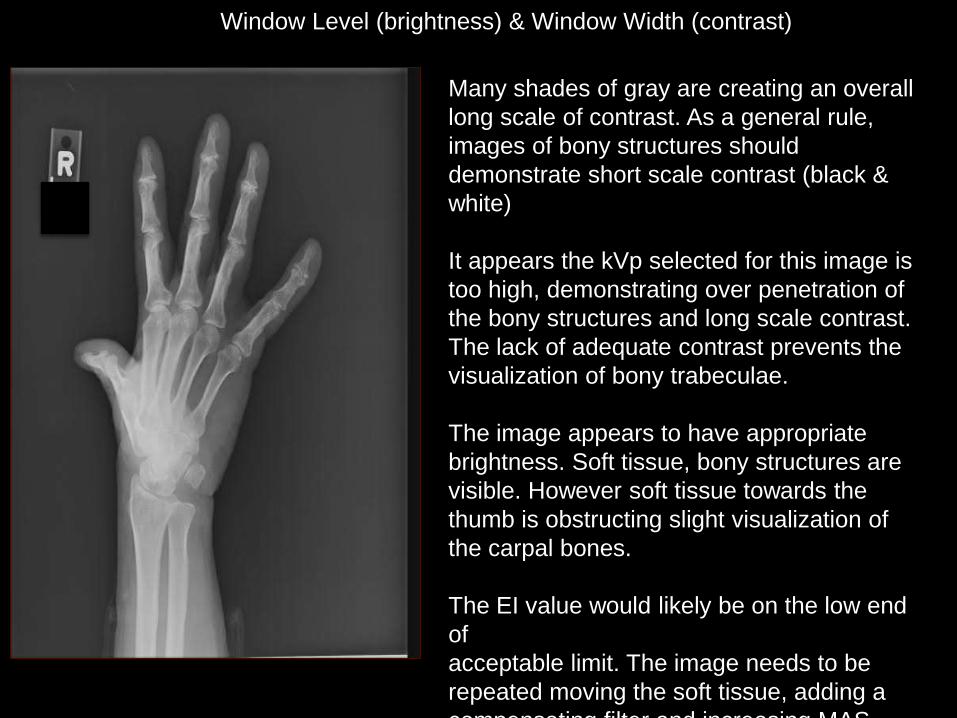
Window Level (brightness) & Window Width (contrast)
Many shades of gray are creating an overall
long scale of contrast. As a general rule,
images of bony structures should
demonstrate short scale contrast (black &
white)
It appears the kVp selected for this image is
too high, demonstrating over penetration of
the bony structures and long scale contrast.
The lack of adequate contrast prevents the
visualization of bony trabeculae.
The image appears to have appropriate
brightness. Soft tissue, bony structures are
visible. However soft tissue towards the
thumb is obstructing slight visualization of
the carpal bones.
The EI value would likely be on the low end
of
acceptable limit. The image needs to be
repeated moving the soft tissue, adding a
compensating filter and increasing MAS
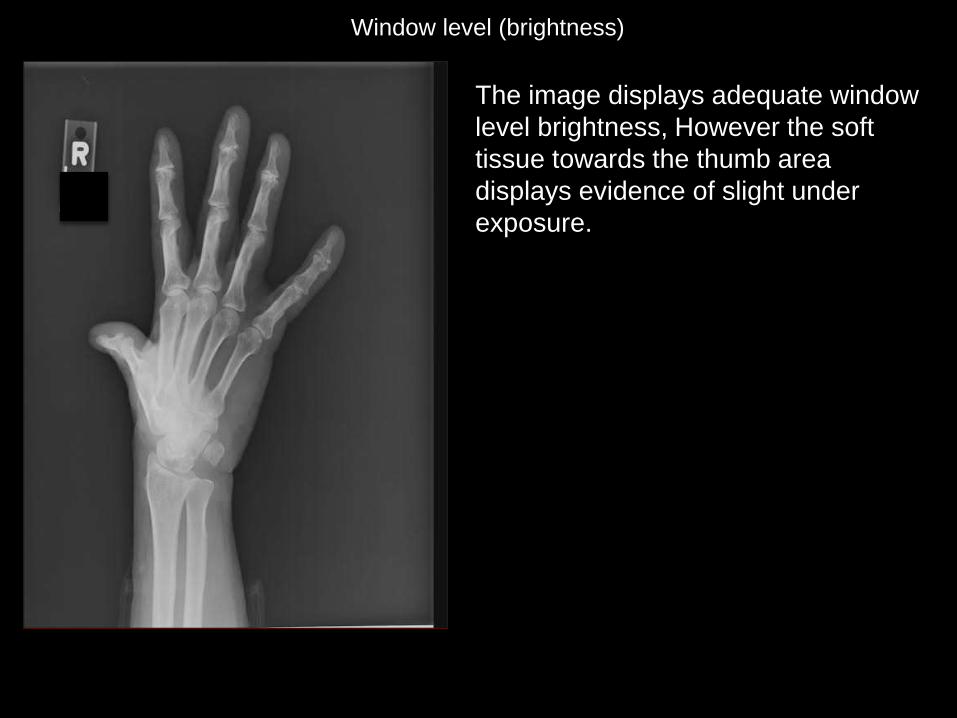
Window level (brightness)
The image displays adequate window
level brightness, However the soft
tissue towards the thumb area
displays evidence of slight under
exposure.

Window width (contrast)
The many shades of grey (long scale
contrast) do differentiate soft tissue from
bone, but the bony structures lack
appropriate short scale contrast to
adequately demonstrate trabeculae and
cortex. The image lacks appropriate
contrast resolution, likely due to over
penetration.
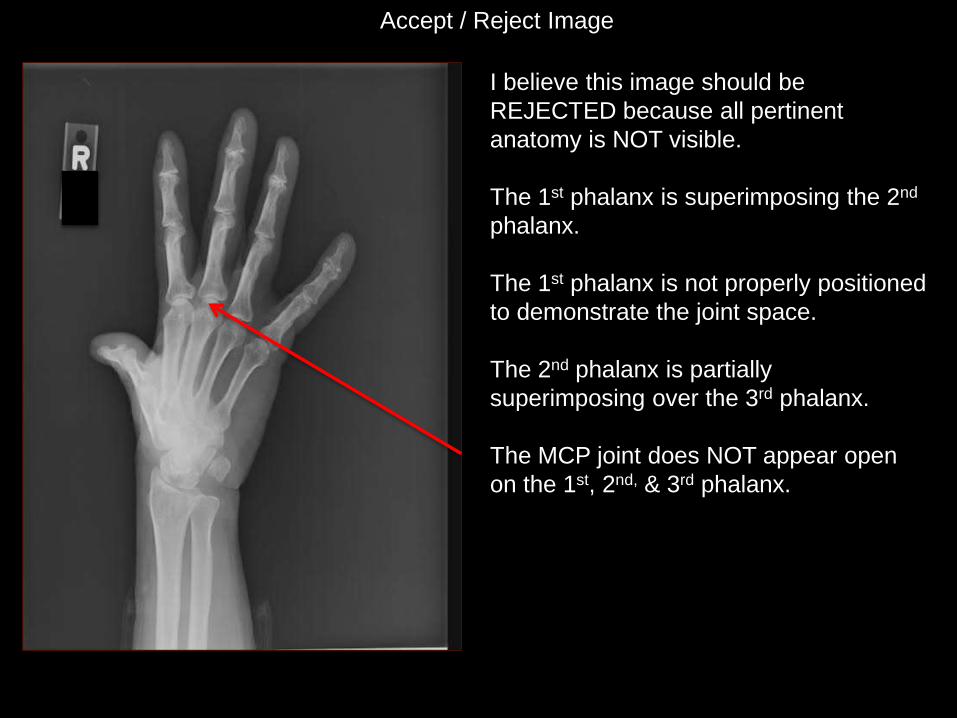
Accept / Reject Image
I believe this image should be
REJECTED because all pertinent
anatomy is NOT visible.
The 1st phalanx is superimposing the 2nd
phalanx.
The 1st phalanx is not properly positioned
to demonstrate the joint space.
The 2nd phalanx is partially
superimposing over the 3rd phalanx.
The MCP joint does NOT appear open
on the 1st, 2nd, & 3rd phalanx.

How to Correct for Errors if Repeated
The image needs to be repeated moving
the soft tissue, adding a compensating
filter and increasing MAS ≥50%
Doing this will demonstrate a more
uniform short scale contrast with CMC
joints & carpals clearly shown.
The CR needs to be centered to the base
of the 3rd metatarsal.
Increase collimation to (4) sides.
Correctly position the thumb to display the
CMC joint & also correct for
superimposition of the thumb over the 2nd
digit.

Original Radiograph
(62 kVp)
15% Rule
(50 kVp)

Works Cited
Frank, E. D., Long, B. W., Smith, B. J., Merrill, V., & Ballinger, P. W. (2007).
Merrill's atlas of radiographic positioning & procedures. St. Louis, MO:
Mosby/Elsevier.
McQuillen-Martensen, K. (2011). Radiographic image analysis (4th ed.). St.
Louis, MO: Saunders/Elsevier.
Image: Jeans Hospital