orthopedic conditions in the older adult tim barnett, pt, dpt, ocs leslie cheung, pt, dpt
TRANSCRIPT

Orthopedic Conditions in the Older Adult
Tim Barnett, PT, DPT, OCSLeslie Cheung, PT, DPT

Identify the “older adult” population Discuss…
Patient History and Presentation Clinical Prediction Rules Clinical Examination Treatment Outcomes
* …For Common Orthopedic Conditions
Course Objectives

The Older Adult Who are we addressing? (CDC)
“The State of Aging and Health in America 2013” How many?
Population of 65 and older to double in the next 25 years
By 2030 estimated to be 20% of population Health Care: “sick care” or “healthcare”
Mobility is critical to health outcomes Orthopedic conditions not in isolation Musculoskeletal health
Associated with depression, CV disease, cancer, injuries, and many other conditions
Introduction

Low Back Pain
Neck Pain
Hip Pain
Knee Pain
Shoulder Pain
Foot and Ankle Conditions
Common Orthopedic Conditions

Common Diagnoses: DDD, stenosis, lumbar strain, sciatica, lumbar radiculopathy, facet joint syndrome
History and Presentation Usually gradual onset Maybe central, unilateral, or bilateral May or may not include sciatica Specific questions (“Does this change your
symptoms”)
Low Back Pain in the Older Adult

Low Back Pain
Cluster to rule in/ out Malignancy (Henschke, 2007)
• Age >50• Hx. CA (+ LR 23.7)• Unexplained weight loss• Failure of conservative therapy
(4 signs present = 100% sensitivity for malignancy)(4 signs absent = -LR 0.00 "confidently rules out malignancy")

Low Back Pain
Rule in/ out Compression Fracture as cause of LBP
• Use of corticosteroids (+LR 12)
• < 50 years old (+LR 0.26)
• > 70 years old (+LR 5.5)
• History of trauma

Treatment-Based Classification System Manipulation/Mobilization Stabilization Directional Specific Exercise (flexion more
common for this group) Traction
Low Back Pain

Low Back Pain
Lumbar Spinal Manipulation CPR (Flynn et al. 2002)
• Less than 16 days duration (+LR 4.4)
• At least 1 hypomobile segment
• At least 1 hip with greater than 35 degrees of motion (+ LR 3.3)
• No symptoms distal to the knee
• FABQ < 19 points
(4 Positive Test: +LR 24)(2 or less Positive Tests: -LR 0.09)

Low Back Pain
Lumbar Spinal Stabilization CPR (Hicks, McGill et al. 2005)
• Age < 40
• SLR > 91 degrees
• (+) Prone instability test
• Aberrant motions with AROM
(3 tests need to be positive for positive inclusion in the clinical prediction rule)(3 Positive Tests: +LR 4.0)

Low Back PainSubjective findings for ruling in relevant Lumbar Spinal Stenosis (Sugioka 2008)
• Age >60 years old
• Onset of symptoms over 6 months
• Decreased symptoms with forward bending
• Increased symptoms with backward bending
• Increased symptoms in standing
• Signs of intermittent claudication
• Urinary incontinence

Clinical Examination Gait, Balance (single leg stance) AROM: flexion, extension, lateral flexion,
rotation, rotation with extension Hip ROM Dermatomes, Myotomes, DTRs Slump Sitting Straight Leg Raise Palpation
Low Back Pain

Treatment and Outcomes Rest Ice, heat Medications (pain relievers, muscle relaxants,
anti-inflammatory) Physical therapy (treatment based
classification system) OUTCOMES
Oswestry Disability Index (ODI), Global Rating of Change (GROC), pain rating
Low Back Pain

Common Diagnoses: DDD, cervical sprain/strain, cervical radiculopathy, cervical myelopathy, facet joint syndrome
History and Presentation Most often gradual onset (sub-acute or chronic) Local, referred, radicular May include headache Difficulty turning neck (i.e. driving) Aggravating: cervical rotation, prolonged static
positions Alleviating: often activity, position change
Neck Pain in the Older Adult

Neck Pain
Pre-test probability= 23%
(2 Positive Tests: Sensitivity .39, Specificity .56, +LR 0.88, -LR 1.09)
(3 Positive Tests: Sensitivity .39, Specificity .94, +LR 6.1, -LR 0.65)
(4 Positive Tests: Sensitivity .24, Specificity .99, +LR 30.3, -LR 0.77)
Cervical Radiculopathy Test Item Cluster (Wainner et al. 2003)
• Positive distraction test
• Less than 60 degress ipsilateral rotation
• Positive ULTT (A)
• Positive Spurling's test

Neck Pain
Cervical Myelopathy cluster (Cook et al, 2010)
Pre-test probability: 35%
• Gait deviation
• (+) Hoffman test
• Inverted supinator sign
• (+) Babinski test
• Age >45 years
(1 of 5 positive tests: +LR 1.4, -LR 0.18)(2 of 5 positive tests: +LR 3.3, -LR 0.63)(3 of 5 positive tests: +LR 30.9, -LR 0.81)(4 of 5 positive tests: +LR infinite, -LR 0.91)

Clinical Examination Posture and observation Balance Screen CROM Shoulder Screen: elevation (flexion, abduction,
ER hands behind head, IR hands up back) TMJ screen: open/close, protrusion, lateral
deviation Vision Cranial Nerve Screen
Neck Pain

Clinical Examination Ligamentous integrity testing (Sharpe-Purser,
transverse ligament, alar ligament) Compression, Distraction, Spurling Upper limb tension testing Clinical Prediction Rule
Cervical radiculopathy Cervical myelopathy
Neck Pain

Treatment and Outcomes Heat, ice, medications, general exercise Physical Therapy
Specific exercise and activity Postural and activity modification Manual therapy techniques to the cervical and
thoracic spine Traction, modalities
OUTCOMES Pain Rating, CROM, NDI, GROC
Neck Pain
Common Diagnoses: hip OA, DJD, bursitis, fracture
History and Presentation Usually gradual onset With trauma (i.e. a fall): rule out hip fracture Often anterior pain with weight-bearing Maybe lateral or posterior-lateral Complaints of pain and stiffness Aggravating: walking, stairs, movement after
prolonged static Alleviating: rest, medication
Hip Pain
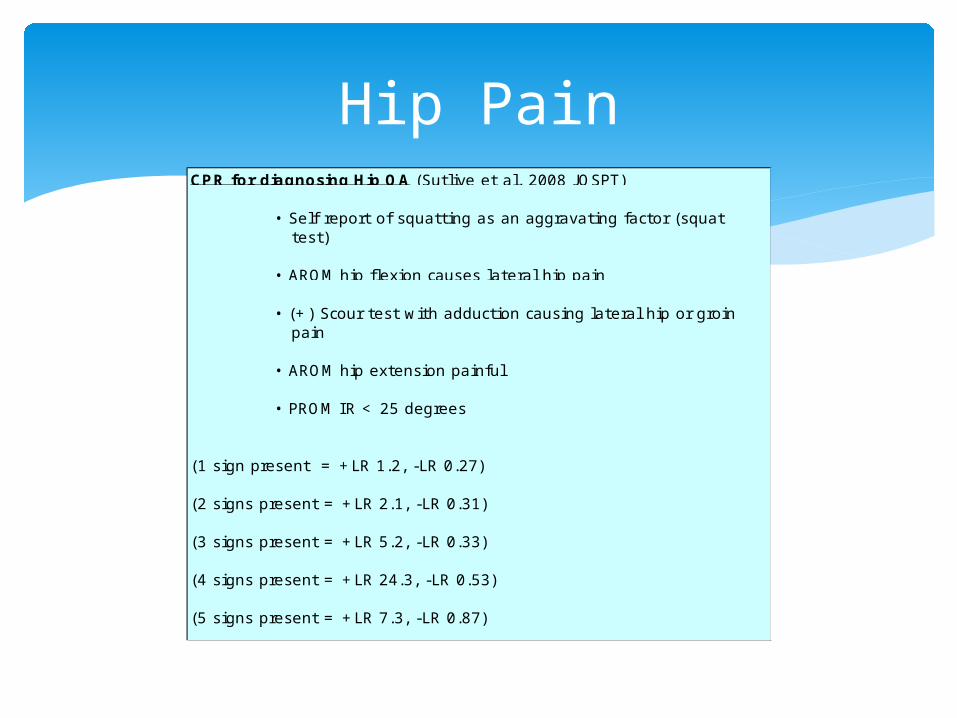
Hip PainCPR for diagnosing Hip OA (Sutlive et al. 2008 JOSPT)
• Self report of squatting as an aggravating factor (squat test)
• AROM hip flexion causes lateral hip pain
• (+) Scour test with adduction causing lateral hip or groin pain
• AROM hip extension painful
• PROM IR < 25 degrees
(1 sign present = +LR 1.2, -LR 0.27)
(2 signs present = +LR 2.1, -LR 0.31)
(3 signs present = +LR 5.2, -LR 0.33)
(4 signs present = +LR 24.3, -LR 0.53)
(5 signs present = +LR 7.3, -LR 0.87)

Clinical Examination Observation of gait Balance Screen of lumbar spine ROM (flexion and IR most restricted) FABER MMT Timed Up and Go (TUG)
Time to rise sit=>stand, walk 3 meters, turn, walk back and sit
Hip Pain

Treatment and Outcomes Medication Ice, heat Physical Therapy
Manual mobilization of the hip and lumbar spine Specific strengthening of the trunk, hips
(abductors and extensors), and legs Balance/Proprioceptive training
THA OUTCOMES
Pain Rating, LEFS, GROC, TUG
Hip Pain

Common Diagnoses: knee OA, knee DJD, knee sprain/strain, Baker’s cyst, pes anserine bursitis
History and Presentation Usually gradual onset Pain most often medial Stiffness, especially upon rising Edema may be evident Aggravating: walking, stairs, squatting,
sit<>stand
Knee Pain

Knee Pain
Altman's criteria for Knee OA
• (+) Radiographic osteophytosis
• Morning stiffness <30 minutes
• Crepitus
• >50 years old
• Tenderness of bony margins of the joint
• No palpable warmth of the synovium

Knee Pain
Ottawa Knee Rules: Radiographs required
• Age 55 or older
• Tenderness at fibular head
• I solated tenderness at patella
• Inability to flex to 90 degrees
• Inability to bear weight immediately and in E.R. (4 steps)

Clinical Examination Observation of gait Postural Observation (genu varus, valgus) Balance Knee ROM LE MMT Palpation TUG or other functional test
Knee Pain

Treatment and Outcomes Medication, heat, ice Topicals Bracing (i.e. sleeves, unloading brace) Physical Therapy
Mobilization of the lumbar spine, hip, knee, ankle Strengthening: hip abductors and extensors
(primary), quads and hamstrings Balance and proprioception enhancement Modalities TKA, debreidment
OUTCOMES Pain Rating, LEFS, TUG, ROM
Knee Pain

Common Diagnoses: DJD, RTC tear (full thickness vs partial), tendonitis, sub-acrominal bursitis
History and Presentation Sudden or gradual onset (e.g. from falls) Often pain at night Difficulty with dressing, bathing, reaching,
driving May have severe weakness Pain may be local only or referred to arm,
scapula
Shoulder Pain
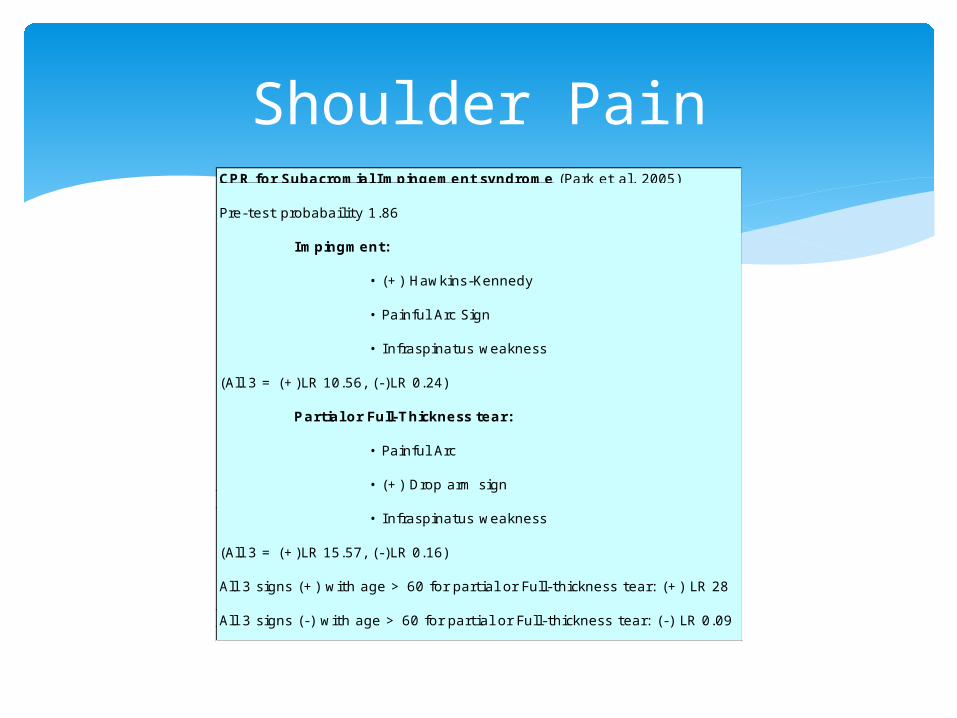
Shoulder PainCPR for Subacromial Impingement syndrome (Park et al. 2005)
Pre-test probabaility 1.86
Impingment:
• (+) Hawkins-Kennedy
• Painful Arc Sign
• Infraspinatus weakness
(All 3 = (+)LR 10.56, (-)LR 0.24)
Partial or Full-Thickness tear:
• Painful Arc
• (+) Drop arm sign
• Infraspinatus weakness
(All 3 = (+)LR 15.57, (-)LR 0.16)
All 3 signs (+) with age > 60 for partial or Full-thickness tear: (+) LR 28
All 3 signs (-) with age > 60 for partial or Full-thickness tear: (-) LR 0.09

Shoulder PainCriteria for Diagnosis of Adhesive Capsulitis (Zuckerman et al., JSES 2004)
• Insidious onet• Night pain• Painful restriction in both active and passive ROM:
• Elevation <100 degrees• ER to < half normal to other limb
• Normal radiographic appearance
Test Cluster for AC joint (Huijbregts 2006) • Active compression test• Cross-body adduction test• AC resisted extension • AC joint tenderness• Paxinos sign
(1 positive= +LR 0)(2 positive= +LR 7.4)(3 positive= +LR 8.3)

Clinical Examination Postural observation Cervical Screen (CROM and Spurling) ROM (general to detailed) MMT (often weakness with ER) Palpation Special Test
Drop Arm (r/o RTC tear) Empty Can, Hawkins-Kennedy (impingement,
tendonitis) Belly Press, Lift Off (subscapularis)
Shoulder Pain

Treatment and Outcomes Medications Injections Physical Therapy
Manual mobilization of the GHJ, scapula, thoracic spine, and cervical spine
Strength and stabilization for scapular mm. and RTC (should not worsen symptoms)
Postural education and activity modification Surgical: debriement, RTC repair, TSA, reverse
TSA, hemi-arthroplasty
Shoulder Pain

OUTCOMES Pain rating Shoulder ROM QuickDASH, SPADI
Shoulder Pain
Common Diagnoses: DJD, achilles tendonitis, posterior tibial tendonitis, plantar fasciitis
History and Presentation Usually gradual onset May complain of joint pain, stiffness, and/or
altered sensation Difficulty walking, standing
Foot and Ankle Conditions

Foot and Ankle ConditionsOttawa Ankle Rules: Radiographs required
Ankle: Pain in the malleolar zone + :
• Bone tenderness along the distal 6 cm of the posterior edge of the tibia or tip of the medial malleolus
• Bone tenderness along the distal 6 cm of the posterior edge of the fibula or tip of the lateral malleolus
• An inability to bear weight both immediately and in the emergency room for 4 steps
Foot: Pain in the midfoot zone + :
• Bone tenderness at the base of the fifth metatarsal
• Bone tenderness at the navicular bone
• An inability to bear weight both immediately and in the emergency room for 4 steps

Clinical Examination Observation of gait Balance Assessment of foot and ankle position Observation of deformities, skin inspection ROM and strength assessment
Foot and Ankle Conditions

Treatment and Outcomes Medication Orthotics and inserts Physical Therapy
Manual mobilization of the foot and ankle Soft tissue mobilization Proprioceptive and strengthening activities
OUTCOMES Pain Rating, gait pattern, need for assistive
device, LEFS
Foot and Ankle Conditions

Falls 1 out of 3 adults 65 and older fall each year 20-30% suffer moderate to sever injuries Hip fractures most common Average hospitalization cost $34,294 30 billion in medical cost (2010) Fear of falling may lead to reduced activity
Dizziness and Vestibular Dysfunction In the top 3 of most common complaints Positional vs. Velocity dependent vertigo Dizziness Handicap Index
Other Considerations

Growth of the older population Orthopedic conditions impact quality of life
and many other conditions related to health Early identification and intervention Use of Clinical Prediction Rules to assist The healthcare provider-patient interaction
as treatment Specific Language
Summary

Physical Activity Recommendations 2 hours and 30 minutes of moderate
intensity aerobic activity every week with 2 or more days of muscle strengthening activity
…or 75 minutes of vigorous intensity aerobic activity every week with 2 or more days of muscle strengthening
Summmary

Questions?
Thank you!
Orthopedic Conditions in the Older Adult