osu vascular medicine clinics and diagnostic vascular ... - pdf of slides.pdf · advances in...
TRANSCRIPT

1
Advances in Diagnosis and Management of PAD
Sanjay RajagopalanWolfe Professor of Medicine and Radiology
Director, Vascular MedicineThe Ohio State University School of Medicine
Quinn Capers IV, MD, FACCVascular Medicine, Cardiology and Endovascular Intervention Steven M Dean, DO, FBVM, FACPVascular Medicine and ImagingSanjay Rajagopalan, MD, FACC FBVMVascular Medicine, Cardiology and ImagingErnie Mazzaferri, MD FACCVascular Medicine, Cardiology and Endovascular InterventionKirsten Houck, BSVascular Medicine Program CoordinatorCarrie Morton, RNVascular Medicine Nurse
Vascular Medicine Program Staff
OSU Vascular Medicine Clinics and Diagnostic Vascular Laboratory(outpatient clinic/diagnostic testing)
3900 Stoneridge LaneDublin, Ohio 43017
Appointment scheduling: 614-889-5001, option 2 OR tollfree at 888-293-7677
Vascular CT and MR ImagingRichard M. Ross Heart Hospital
452 W. 10th AvenueColumbus, Ohio 43210
Appointment scheduling: 888-293-7677
Vascular Medicine Research and Administrative OfficesOSU Biomedical Research Tower
460 W. 12th AvenueColumbus, Ohio 43210
614-247-7760
Atherothrombosis in Contemporary Practice: The REACH REGISTRY
Steg et al. JAMA March 21, 2007; 927;1997-06.
14.4 15.2 14.5
21.1
5.3
12.81
2.61.53.83.12.92.8
0
5
10
15
20
25
14.4 15.2 14.5
21.1
5.3
12.81
2.61.53.83.12.92.8
0
5
10
15
20
25
Mor
talit
y/M
AC
E (%
ye
ar)
Mean age 69 yrs; >75% on statin, ACE/ARB and anti-platelet agents
Any CAD CVD PAD RF All
Revasc 5% 12.38%
MACEAll Cause Mortality
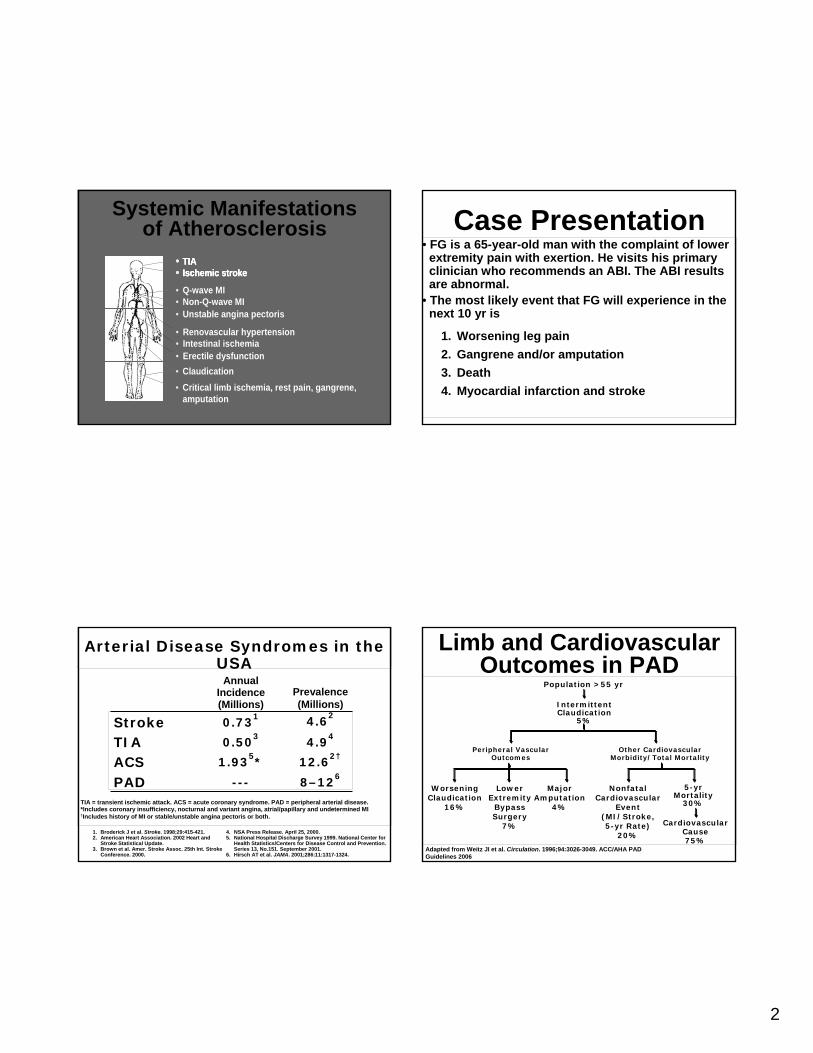
2
• TIA• Ischemic stroke
• Claudication• Critical limb ischemia, rest pain, gangrene,
amputation
• Renovascular hypertension• Intestinal ischemia• Erectile dysfunction
• TIA• Ischemic stroke• TIA• Ischemic stroke
• Q-wave MI• Non-Q-wave MI• Unstable angina pectoris
Systemic Manifestationsof Atherosclerosis
1. Broderick J et al. Stroke. 1998;29:415-421.2. American Heart Association. 2002 Heart and
Stroke Statistical Update.3. Brown et al. Amer. Stroke Assoc. 25th Int. Stroke
Conference. 2000.
4. NSA Press Release. April 25, 2000.5. National Hospital Discharge Survey 1999. National Center for
Health Statistics/Centers for Disease Control and Prevention. Series 13, No.151. September 2001.
6. Hirsch AT et al. JAMA. 2001;286:11:1317-1324.
TIA = transient ischemic attack. ACS = acute coronary syndrome. PAD = peripheral arterial disease.*Includes coronary insufficiency, nocturnal and variant angina, atrial/papillary and undetermined MI †Includes history of MI or stable/unstable angina pectoris or both.
PADACSTIAStroke
8–126
---
12.62†
1.935*
4.94
0.503
4.62
0.731
Prevalence(Millions)
AnnualIncidence(Millions)
Arterial Disease Syndromes in the USA
Case Presentation• FG is a 65-year-old man with the complaint of lower
extremity pain with exertion. He visits his primaryclinician who recommends an ABI. The ABI resultsare abnormal.
• The most likely event that FG will experience in thenext 10 yr is
1. Worsening leg pain2. Gangrene and/or amputation3. Death4. Myocardial infarction and stroke
Limb and Cardiovascular Outcomes in PAD
Adapted from Weitz JI et al. Circulation. 1996;94:3026-3049. ACC/AHA PAD Guidelines 2006
Population >55 yr
IntermittentClaudication
5%
Peripheral VascularOutcomes
Other CardiovascularMorbidity/Total Mortality
Lower Extremity
Bypass Surgery
7%
MajorAmputation
4%
WorseningClaudication
16%
NonfatalCardiovascular
Event(MI/Stroke, 5-yr Rate)
20%
5-yrMortality
30%
CardiovascularCause75%

3
Adapted from Ware JE. Ann Rev Pub Health. 1995;16:327-354
Quality of Life in PAD Is Comparable to Chronic Illnesses
30 34 38 40 50 55
Average Adult
Average Well Adult
Physical Component Summary (PCS)
36
IntermittentClaudication
# of
Peo
ple Congestive
Heart Failure
Chronic Lung
Disease
Critical Limb
Ischemia
Risk Factors for Developing PAD/Intermittent Claudication
Adapted from TASC Working Group. J Vasc Surg. 2000;31(1 suppl):S1-S296Ridker PM et al. Circulation 1998;97:425-428
Protective Harmful
-2 -1 0 1 2 3 4-2 -1 0 1 2 3 4
Male gender (vs female)
Age (per 10 yr)
Diabetes
SmokingHypertension
Hypercholesterolemia
CRP (>2)
Despite the relative risk associated with
male gender (which is age-dependent), the prevalence of PAD is gender-equal in the post-menopausal
years.
Assessment of Disease
• Vascular history• Physical examination • Noninvasive vascular laboratory tests
SymptomsSymptomsButtock, hip,Buttock, hip,thighthigh
Thigh, calfThigh, calf
Calf, ankle, footCalf, ankle, foot
Obstruction inObstruction inAorta orAorta oriliac arteryiliac artery
Femoral arteryFemoral arteryor branchesor branches
PoplitealPopliteal
TibioTibio--peronealperoneal(diabetic) (diabetic) Calf, ankle, footCalf, ankle, foot
Regardless of the location of PAD within the lower extremity vasculature, claudication is most frequently localized to the
muscles of the calf
PAD Anatomy: Sites of Claudication

4
12.65.5Classic Rose claudication
61.746.3Atypical leg symptoms
25.848.3No pain
Prior Diagnosis of PAD (%)
n=366
Newly Diagnosed PAD (%)n=457
Hirsch AT et al. JAMA. 2001;286:1317-1324
Data from PARTNERS study of primary care
practices
PAD: Classic Symptoms Are Rare, Contributing to Underdiagnosis
Determination of Ankle-Brachial Index (ABI)
• Measure ankle and brachial systolic pressures with handheld Doppler device• Use highest arm and each ankle pressure
• ABI is 95% sensitive, 99% specific for PAD• Lower ABI values are inversely related to
increased mortality and risk of limb loss
Ankle systolic pressureBrachial systolic pressure
ABI =
TASC Working Group. J Vasc Surg. 2000;31(1 suppl):S66-S67
Understanding the ABI
• The ABI does not correlate closely with limb symptoms or severity of claudication
• Request a Toe Brachial Index if vessels noncompressible
TASC Working Group. J Vasc Surg. 2000;31(1 suppl):S66-S67
Noncompressible vessels
>1.30
InterpretationABI
Severe≤0.40Moderate0.40–0.69Mild0.70–0.89Normal0.90–1.30
Other Noninvasive Diagnostic Tests
• Segmental blood pressure recording• Segmental pulse volume recording• Exercise Doppler (ABI) stress testing• Duplex ultrasound• Magnetic resonance angiography (MRA)• CT angiography
The tools of the noninvasive vascular laboratory provide additional details related to PAD diagnosis, including anatomic localization (to aid choice of revascularization options) and objective physiologic assessment of PAD severityAdapted from Manual of Vascular Diseases. Eds Rajagopalan, Mohler and Mukherjee 1rst Ed Lippincott Williams and Wilkins, Philadelphia.

Slide 13
ATH14 Title changedAlan T. Hirsch, M.D., 9/20/2003

5
EXERCISE ABI
H&P AND ABI
SEVEREMODERATE MILD
AORTO-ILIAC FEMORAL/INFRAPOP INCONSISTENT
INTERVENTION
CE MRA/CTA
SEGMENTAL PRESSURE AND WAVEFORMS
NO FURTHER W/U
ROUTINE SURVEILLANCE RE-INTERVENTION
Duplex MR/CT
Dellegrottaglie, Rajagopalan S. Nature Cardiovascular Reviews 2007.
Peripheral Arterial Disease:
Management
Reduction in Mortality and Morbidity
Is the Primary Goal!
Essentials of PAD Disease Management
Risk factor normalization• Smoking cessation
– Goal: complete cessation
• Lipid management
– Goal LDL <70* mg/dL
• Blood pressure control
– Goal <135/85 mm Hg
• Blood sugar control (diabetic patients)
– Goal: A1C <7%
Antiplatelet therapies
Clopidogrel, aspirin
Symptom-directed therapies
Supervised exercise rehab
Cilostazol
Selective use of revascularization (PTA, bypass)
Therapies to lower risk of MI, stroke, and death

6
If Your Patient Did This….
But they don’t!
Medications Proven to Improve Outcomes in Individuals with PADDrug Outcome
Aspirin 18% reduction MI/CVA/death
43% reduction in graft occlusion
Clopidogrel 24% reduction MI/CVA/deathvs aspirin
Ramipril 22% reduction MI/CVA/death
Simvastatin 24% reduction MI/CVA/death
Cilostazol Improvement in claudication symptoms and quality of life
CVA = cerebrovascular accident
Indications for Revascularization for
Intermittent Claudication
• Lifestyle-limiting symptoms• Continued disability despite appropriate
nonsurgical management• Technically feasible revascularization
options exist• Expectation of favorable risk/benefit ratio

7
Surgical Intervention Results
25ProsthFem-Distal50-75VeinFem-Distal33ProsthFem-Pop BK
47ProsthFem-Pop AK56-65VeinFem-Pop BK
66VeinFem-Pop AK
5 year (%)
TypeBypass
ACC/AHA Guidelines on Peripheral Arterial Disease. Circulation 2005.
Outcome depends on a number of factors including contextDiabetic status, state of the outflow vessels etc..
5-yrGRAFT
92%Aortic Endarterectomy
90%Aorto-Bifemoral
Aorto-Iliac Disease Surgical Results Morbidity/Mortality
>20Surgical Revision
0-24Early Graft Failure
1.9-3.4Myocardial infarction
1.3-6Mortality
10-30Wound infection
%COMPLICATION
TASC J Vasc Surg 2000
Systemic Atherosclerosis:An Interventionalist’s
Perspective
Quinn Capers, IV, MD, FACC, FSCAIAsst. Professor of Medicine
Division of Cardiovascular MedicineDirector, Peripheral Vascular Interventions, Ross Heart Hospital
Director, Cardiovascular Cath Lab, University Hospital East
The Ohio State University Medical Center
Systemic AtherosclerosisCurrent Treatments
2 therapeutic goals
Symptom Relief CV Event ReductionMechanical RevascularizationTherapeutic walking programAnti-claudication drugs
Mechanical revascularizationACE inhibitorsStatinsAspirin/Plavix

8
Systemic AtherosclerosisCurrent Treatment
• Symptom ReliefMechanical Revascularization• Surgical
–Endarterectomy–Bypass–Thrombectomy
• Percutaneous–PTA–Stent–Laser–Atherectomy–Thrombectomy
Trans-Atlantic Inter-Society Consensus Document (TASC)
• Document published in 2000 (updated 2007)
(radiology, surgical, cardiology, medical societies collaborated)
Evidence and experience-based guidelines for revascularization of LE atherosclerotic disease
Trans-Atlantic Inter-Society Consensus Document (TASC)
• “A”: Endovascular approach recommended
• “B”: Endovascular likely better than surgery
• “C”: Surgery likely better than endovascular
• “D”: Surgical approach recommended
Trans-Atlantic Inter-Society Consensus Document (TASC): Progress in
Endovascular Approaches• What happened from 2000 to 2007?
More aggressive approaches to endovascular mgmtNew technology• Atherectomy• Self-expanding stents• Cryoplasty• Laser• ? Medical approaches to retard progression
of atherosclerosis (statins, ACE inh)

9
Trans-Atlantic Inter-Society Consensus Document (TASC): Progress in
Endovascular Approaches• TASC (2000)• “A”: SFA stenosis <3 cm
• “B”: SFA stenosis up to 10 cm
• TASC II (2007)• “A”: SFA stenosis up to
10 cm/SFA occlusion up to 5 cm
• “B”: SFA stenosis or occlusion up to 15 cm
• “B”: popliteal stenosis
Stent vs PTA in SFA Disease
• 104 patients with Rutherford 3-5 PAD• SFA stenosis/occlusion >3 cm• Primary Endpoint
Restenosis >50% at 6-months as determined by CTA or DSA
• Secondary EndpointsDUS restenosis >50% at 3, 6, 12 months or finding of stent fractureClinical and Resting ABI
N Engl J Med 2006;354:1879-88
Stent vs PTA in SFA Disease
N Engl J Med 2006;354:1879-88
Duplex US Derived PatencyCT and DSA Patency
Case 1: Severe LLE Claudication

10
Case 1: Severe LLE Claudication
Case 1: Atherectomy of occluded L SFA
PRE
Total Occlusion
Widely
Patent
figure
POST
Excised plaque
In-stent restenotic lesionsIn SFA/popliteal
De novo atherosclerotic lesion
Case 2
PRE POST
Case 2•Multifocal lesions in diffusely diseased SFA/popliteal•Post atherectomy/balloon angioplasty•ABI=0.85

11
Case 2
PRE POSTDebris captured from distal protection device
• Multifocal lesions in diffusely diseased SFA/popliteal• Post laser atherectomy/balloon angioplasty• ABI=0.85
Focal in-stent restenosisInfrarenal aorta
Case 3• Severe bilateral LE claudication
Balloon angioplasty of In-stent lesion in aorta
Case 3• Severe bilateral LE claudication
Case 4
Angioseal collagenplug device in CFA

12
Case 4Step 1: Advancedistal protectiondevice
Step 2:“Vaporize”with laser
Step 3: Debulk withatherectomy catheter
• New, severe RLE ischemia, ABI 0.5 • 2 days after cardiac cath
Case 4
Preliminary results:Filling defect still visible.
• New, severe RLE ischemia, ABI 0.5 • 2 days after cardiac cath
Step 4: Prolonged balloonAngioplasty (4 min) required
• New, severe RLE ischemia, ABI 0.5 • 2 days after cardiac cath
Case 4
Fragments of collagen plug capturedin distal protection device
Case 4 • New, severe RLE ischemia, ABI 0.5 • 2 days after cardiac cath

13
Final result: ABI=0.9
Case 4• New, severe RLE ischemia, ABI 0.5 • 2 days after cardiac cath
Remember:When you see this . . .
Small AAAIliac artery aneurysms
. . . think of this!
Severe LMCA lesion
Go Bucks!!!
OSU Ross Heart Hospital