paolo marchetti oncologia medica ospedale sant’andrea & idi irccs roma higher drug costs and...
TRANSCRIPT
Paolo MarchettiOncologia MedicaOspedale Sant’Andrea&IDI IRCCSRoma
Higher drug costs and healthcare savings: a true conflict of interest
1
Oncology: New Drugs, New ProblemsRome, 2nd October 2009
Where are we moving?
• The medical humanism movement seeks to understand the patient as a person, focusing on individual values, goals, and preferences with respect to clinical decisions.
• A second movement is evidence-based practice, which aims to put medicine on a firm scientific footing; experts evaluate the best available data and develop clinical guidelines designed to standardize procedures and therapies.
2
• These two movements will now play out in the context of national health care reform, the goals of which are universal coverage and cost containment.
• Until now, the two trends have largely progressed in parallel, with mutual acknowledgment of the other's merits. But now, when it is most important for them to coalesce, they are poised to collide.
3
Conflicts of interest in medical practice
• Financial conflicts• Intellectual conflicts• Conflicts in regulatory duties• Conflicts with industry
4
Hormonal therapy in postmenopausal early breast cancer patients
How to interpret data and apply them to
clinical practice
5
6
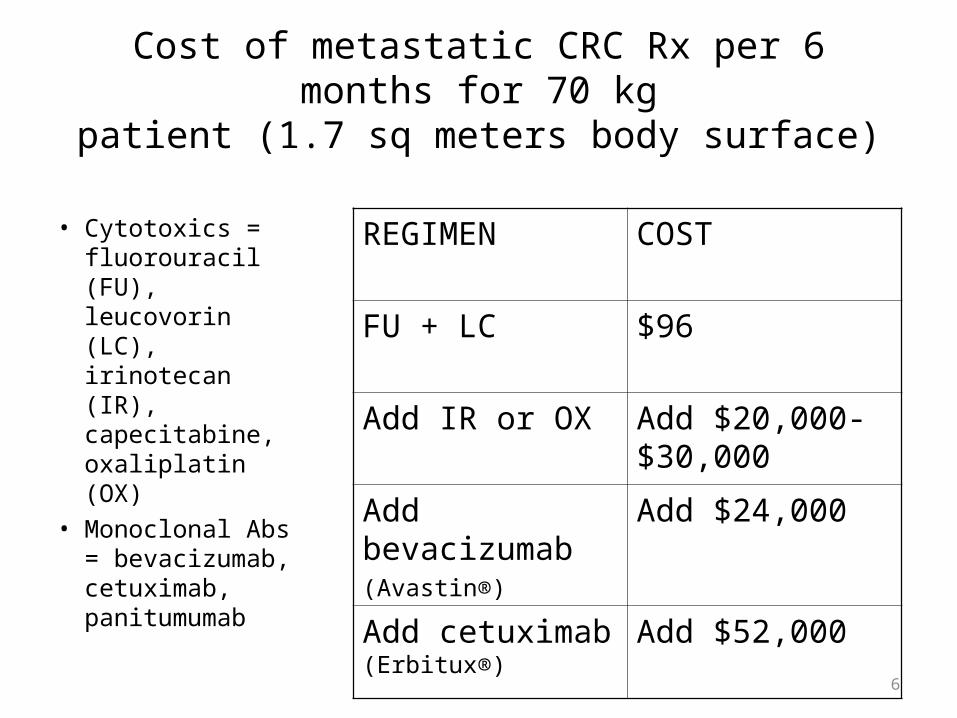
Cost of metastatic CRC Rx per 6 months for 70 kgpatient (1.7 sq meters body surface)
• Cytotoxics = fluorouracil (FU), leucovorin (LC), irinotecan (IR), capecitabine, oxaliplatin (OX)
• Monoclonal Abs = bevacizumab, cetuximab, panitumumab
REGIMEN COST
FU + LC $96
Add IR or OX Add $20,000-$30,000
Add bevacizumab(Avastin®)
Add $24,000
Add cetuximab (Erbitux®)
Add $52,000
7
The dilemma of balancing clinical relevance and costeffectiveness for new oncology products
How can it be resolved?
• Cancer is the second most important cause of death (after cardiovascular disease)
• It accounts for 16.7% of all DALYs lost in EU25, and 12.5% in US/Canada respectively
• In industrialized countries direct costs due to cancer amount to ~7% of the total health care costs.
• Cost for cancer drugs account for– 13% of all health care costs for cancer and– 5% of total drug costs
• Indirect cost accounts for more than two-thirds of the cost of cancer
*DALYs= disability-adjusted life yearsSource: Jönsson, Wilking Ann Onc 2007; 18: Suppl. 3
8
9
Which changes in clinical outcomes are
clinically relevant?• Whether a treatment result is of clinical relevance
is a value judgement and depends on the perspective
• A multitude of different stakeholders (oncologists, regulatory agencies, patients, payers, society, industry) might have different views
• Is a 20% increase in overall survival equally clinically relevant for all cancer, treatment lines, patient populations?
Britta Paschen, 2007
10
Factors determining clinical relevance
• The seriousness of the disease or condition• Intent of treatment (palliative, curative, preventive)• The availability and performance of other alternative therapies• The nature of the target population and whether it includes
vulnerable populations, such as children and the elderly• The choice of endpoints (response, progression-free survival,
overall survival, QoL)• Magnitude of clinical benefit
– related to the current QoL or remaining life expectancy• Risk-Benefit ratio• Individual patient characteristics (co-morbidities, age, other
prognostic factors)
Britta Paschen, 2007
11
Trends in total drug cost and survival in metastaticcolorectal cancer over the last decade
• Therapy improvements in oncology occur in small but tangible steps
• The value of these individual steps might not be reflected by cost-effectiveness results
• There is no single measure to resolve the misbalance• The use of cost-effectiveness analysis as currently
implemented has serious limitations• There is need to have a debate in society on
willingness to pay for treatment of life-threatening diseases
Britta Paschen, 2007
12
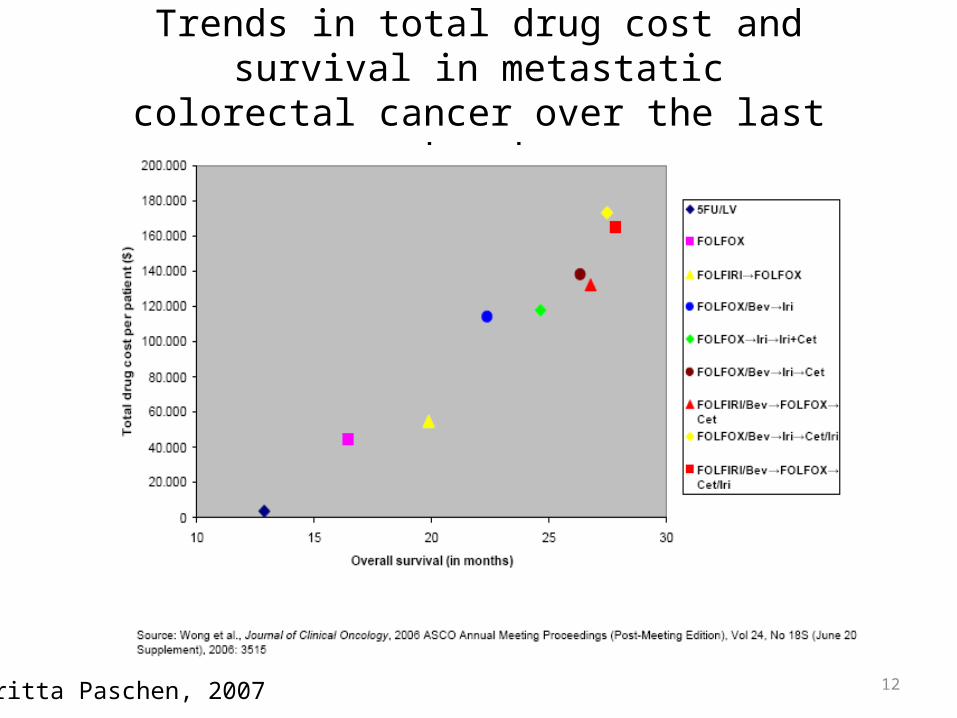
Trends in total drug cost and survival in metastaticcolorectal cancer over the last decade
Britta Paschen, 2007
Health Care Costs:the MD control
• Drugs!• …?
13