patient safety and health care associated infections infectious disease epidemiology workgroup jan....
TRANSCRIPT

Patient Safety and Health Care Associated Infections
Infectious Disease Epidemiology Workgroup
Jan. 4, 2008 Austin, Texas
Gary Heseltine MD MPH
Infectious Disease Control Unit
“When speculation has done its worst, two and two still make four.” Samuel Johnson, The Idler
Outline• Big picture – patient safety
– Harm unintentional or not, preventable or not– The many players
• Health care-associated infections (HAI)– Surgical care improvement project (SCIP)– The burden of morbidity and mortality– What the evidence says
• SB 288 Public Reporting of HAI– Where are we and where are we going in Texas?
• Changing practices – adopting protocols– Barriers and incentives– Direction for the future

Patient Safety• Hippocrates, Epidemics
"Declare the past, diagnose the present, foretell the future; practice these acts. As to diseases, make a habit of two things — to help, or at least to do no harm."
• The Joint Commission defines patient safety solutions:"Any system design or intervention that has demonstrated the ability to prevent or mitigate patient harm stemming from the processes of health care.“
• Institute for Healthcare Improvement defines medical harm:“Unintended physical injury resulting from or contributed to by medical care (including the
absence of indicated medical treatment), that requires additional monitoring, treatment or hospitalization, or that results in death.
Such injury is considered harm whether or not it is considered preventable, whether or not it resulted from a medical error, and whether or not it occurred within a hospital.”
• Safe - free from hurt, injury, danger or risk • Harm – injury; damage; hurt• Safety - state of being safe

Institute for Healthcare Improvement
37 Million AdmissionsX
40 Injuries per 100 Admissions=
15 Million Injuries per Year
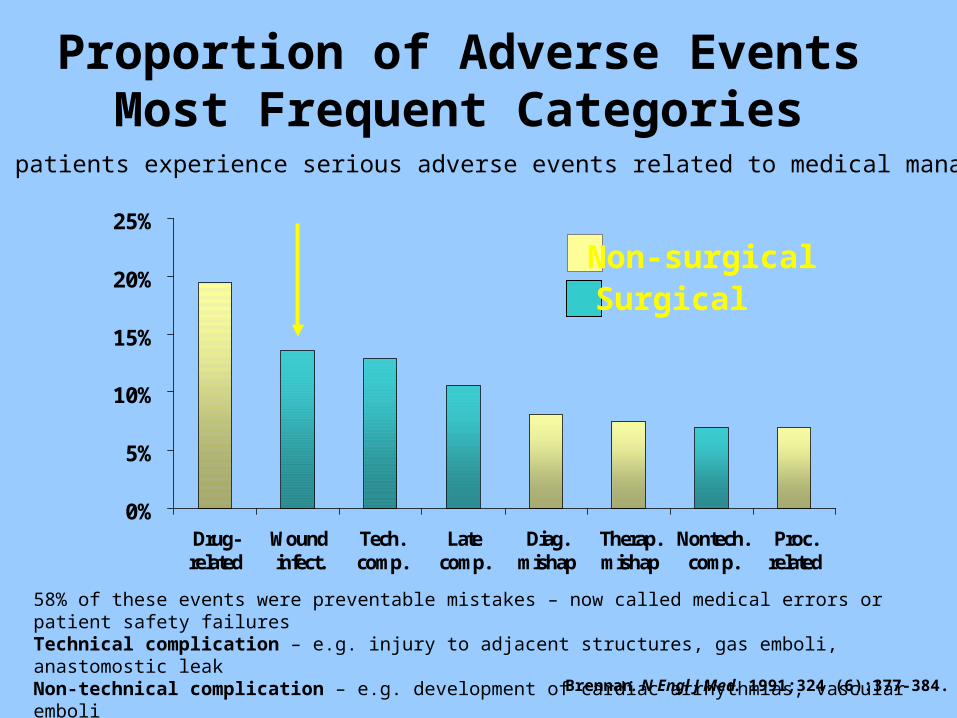
Proportion of Adverse EventsMost Frequent Categories
0%
5%
10%
15%
20%
25%
Drug-related
Woundinfect.
Tech.comp.
Latecomp.
Diag.mishap
Therap.mishap
Nontech.comp.
Proc.related
Brennan. N Engl J Med. 1991;324 (6):377-384.
Non-surgicalSurgical
3.7% of patients experience serious adverse events related to medical management.
58% of these events were preventable mistakes – now called medical errors or patient safety failuresTechnical complication – e.g. injury to adjacent structures, gas emboli, anastomostic leakNon-technical complication – e.g. development of cardiac arrhythmias, vascular emboli
Burden of Healthcare-Associated Infections in the United States, 2002
• 1.7 million infections in hospitals– Most (1.3 million) were outside of ICUs– 9.3 infections per 1,000 patient-days– 4.5 per 100 admissions
• 99,000 deaths associated with infections– 36,000 – pneumonia– 31,000 – bloodstream infections
Klevens, et al. Pub Health Rep 2007;122:160-6

Impact of Surgical Site Infections (SSI)
Infected Uninfected
Mortality (in-hospital)
7.8% 3.5%
ICU admission 29% 18%
Readmission 41% 7%
Median initial LOS 11d 6d
Median total LOS 18d 7d
Initial excess cost +$3,644 (median)
Total excess cost +$5,038 (median)
*Pairs matched for procedure, NNIS index, age*General inpatient surgical population; 22, 742 procedures included
Kirkland. Infect Control Hosp Epidemiol. 1999;20:725.
An estimated 40-60% of SSIs are preventable.
• Centers for Medicare & Medicaid Services (CMS)
• Centers for Disease Control and Prevention (CDC)
• Department of Veteran’s Affairs
• Institute for Healthcare Improvement (IHI)
• Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
• American College of Surgeons (ACS)
• American Hospital Association (AHA)
• American Society of Anesthesiologists (ASA)
• Association of peri- Operative Registered Nurses (AORN)
• Agency for Healthcare Research and Quality (AHRQ)
Surgical Care Improvement Project (SCIP)
2010 National GoalReduce preventable surgical morbidity and mortality by 25%
Surgical Infection Prevention (SIP): previous CMS initiative focusing appropriate selection, administration and discontinuation of surgical antibiotic prophylaxis.

SCIP Has Four Modules
Infection• 7 Infection Prevention Process Measures
Venous Thromboembolus (VTE)• 2 VTE Prevention Process Measures
Cardiac Prevention Module• 1 Cardiovascular Prevention Measure
Respiratory (Post-operative ventilator associated pneumonia)
• Delayed implementation to use these measures in expanding the ICU Core Measure Set

SCIP Infection Module• SCIP INF 1:
– Prophylactic antibiotic received within one hour prior to surgical incision
• SCIP INF 2:– Prophylactic antibiotic selection for surgical patients
• SCIP INF 3:– Prophylactic antibiotics discontinued within 24 hours after
surgery end time (48 hours for cardiac patients)• SCIP INF 4:
– Cardiac surgery patients with controlled 6 a.m. postoperative serum glucose
• SCIP INF 6:– Surgery patients with appropriate hair removal
• SCIP INF 7: – Colorectal surgery patients with immediate postoperative
normothermia
Effective with discharges beginning July 1, 2006

0
1
2
3
4
≤-3 -2 -1 0 1 2 3 4 ≥5
Classen. NEJM. 1992;328:281.
Prophylactic AntibioticsTiming Administration of Pre-op
DoseIn
fect
ion
s (%
)
Hours From IncisionNote: only 40% received antibiotics within two hours of incision
14/369
5/699
5/1009
2/180
1/81
1/411/47
15/441
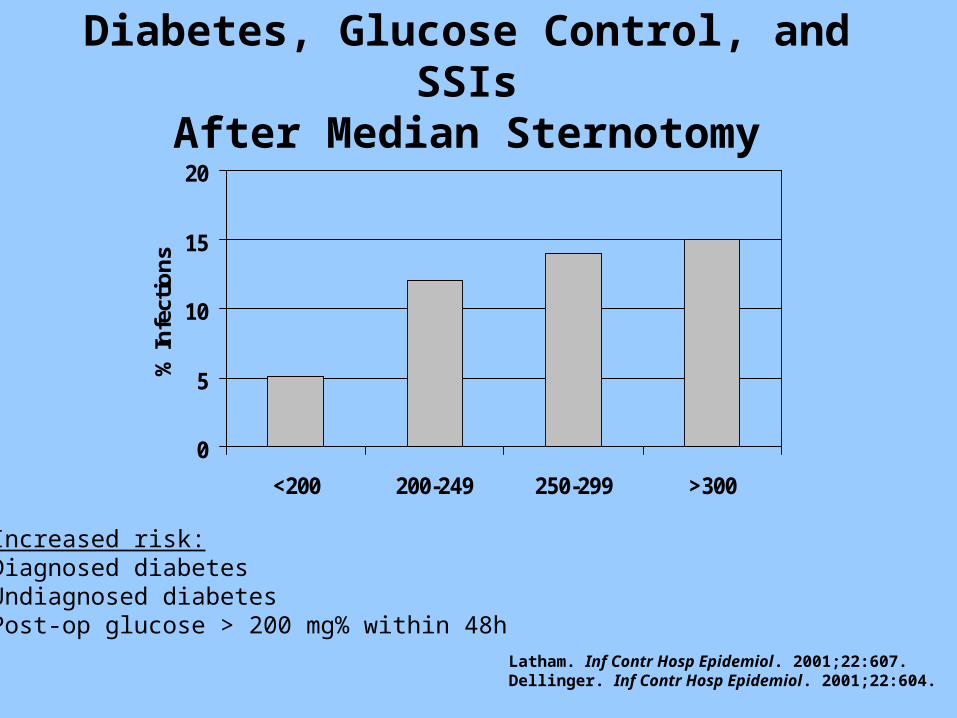
Diabetes, Glucose Control, and SSIsAfter Median Sternotomy
0
5
10
15
20
<200 200-249 250-299 >300
% In
fect
ion
s
Increased risk:Diagnosed diabetesUndiagnosed diabetesPost-op glucose > 200 mg% within 48h
Latham. Inf Contr Hosp Epidemiol. 2001;22:607.Dellinger. Inf Contr Hosp Epidemiol. 2001;22:604.
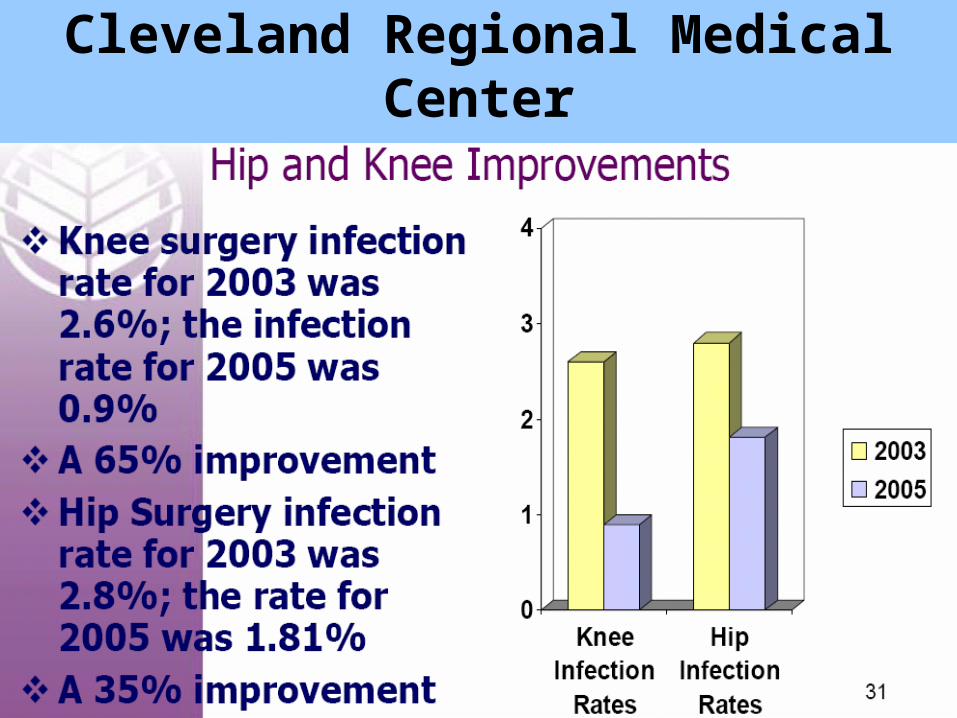
Cleveland Regional Medical Center
Central Line Infections:Incidence & Risk
• 48% of ICU patients have central venous catheters, accounting for 15 million central venous catheter-days per year in ICUs.
• The case fatality rate for catheter-related blood stream infections approaches 20%.
• Attributable mortality ranges from 12-25% but was 3% in one meta-analysis.
Mermel LA. Ann Int Med 2000;132: 391-402Soufir L et al. Infect Control Hosp Epidemiol 1999 Jun;20(6):396-401.
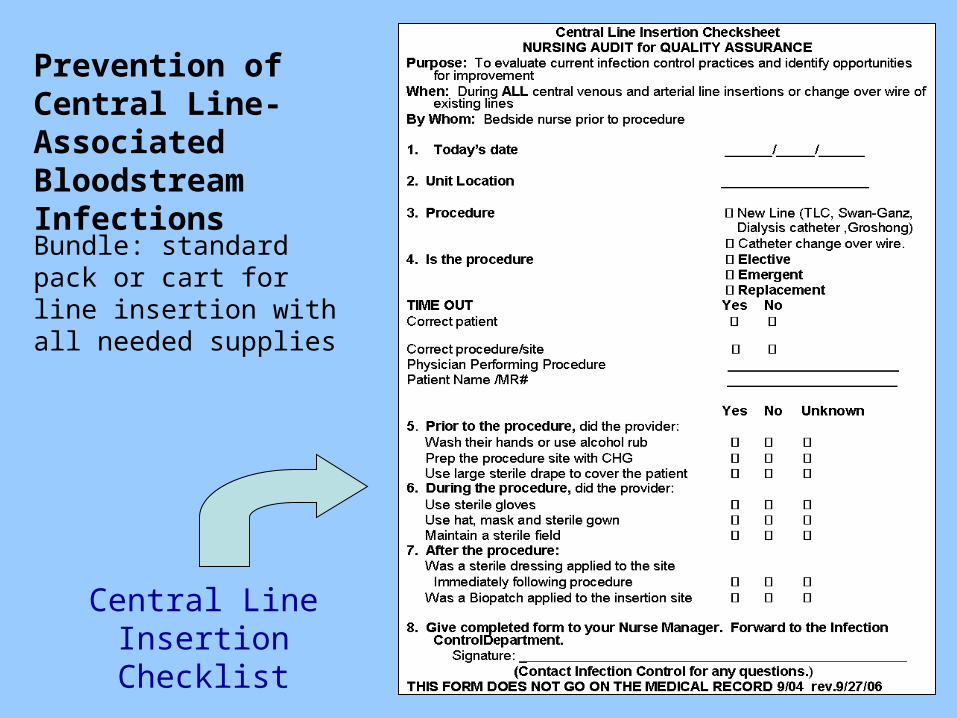
Central Line Insertion Checklist
Prevention of Central Line-Associated Bloodstream Infections
Bundle: standard pack or cart for line insertion with all needed supplies

Do Central Line Bundles Work?• 12 month Baseline average CA-BSI rate 2.84• 12 month Project Average CA-BSI rate .73 = 74% Reduction• 10 out of 12 months with zero CA-BSI
CA-BSI Process/ Outcome
0%
20%
40%
60%
80%
100%
Co
mp
lian
ce
0.002.004.006.008.0010.0012.0014.00
CA
-BS
I R
ate
CL Bundle Compliance 0% 0% 0% 0% 0% 0% 0% 0% 82% 67% 74% 70% 94% 91% 91% 94% 100 100 92% 86% 91%
CA-BSI Rate 0.00 0.00 0.00 4.00 11.8 3.13 3.47 3.46 0.00 0.00 0.00 5.68 3.02 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0
CA-BSI Cases 0 0 0 1 4 1 1 1 0 0 0 2 1 0 0 0 0 0 0 0 0
F-
04
M-
04
A-
04
M-
04
J-
04
J-
04
A-
04
S-
04
O-
04
N-
04
D-
04
J-
05
F-
05
M-
05
A-
05
M-
05
J-
05
J-
05
A-
05
S-
05
O-
05
Started PI
Spread to all providers
Overlake Hospital Medical Center - Seattle IHI Collaborative

IOM Report 2002
“Disparities in the health care delivered to racial and ethnic minorities are real and are associated with worse outcomes in many cases, which is unacceptable.”
Alan Nelson, committee chair
Unequal Treatment: Confronting Racial and Disparities in Health Care
Protocol driven interventions for HAIs are one step in addressing this larger issue.

SB 288 Mandatory Public Reporting of Healthcare-associated Infections
80th Regular Legislative Session 2007
• Hospitals, Ambulatory Surgical Centers (ASCs) to report specific HAIs to DSHS using CDC case definitions
• Must begin no later than 6/1/08• Minimum once per year, maximum each quarter• Must contain sufficient patient ID data
– avoid duplication– verify accuracy and completeness– allow for risk adjustment
• DSHS will review data for validity and “unusual data patterns or trends”

SB 288 Advisory Panel
• Two certified ICPs, one from a rural hospital• Two ICP certified and licensed nurses• Three MDs one with Pedi ID and Pedi epi, SHEA
members with expertise in IC• Two QA professionals-one ASC & one acute care• One officer of a general hospital• One officer of an ASC• Three nonvoting DSHS members• Two members representing the public as consumers
No lobbyists or healthcare trade association representatives Reimbursement is allowed
Sixteen member Advisory Panel– two year term

Adult Reportable SSI Infections• colon surgeries• hip and knee arthroplasties• abdominal and vaginal hysterectomies• CABG and vascular procedures
Pediatric Reportable SSI Infections
• Cardiac procedures excluding thoracic cardiac• VP shunt procedures• Spinal surgery with instrumentation• And (non-SSI) respiratory syncitial virus infection
Reportable Central Line InfectionsLab confirmed from a patient in any “special care setting
in the hospital”
Alternative Reporting
Report SSIs related to the 3 most frequently performed procedures from the National Healthcare Safety Network (NHSN) procedure list
For facilities with an average < 50 procedures/monthly
Reporting Mechanism• Plan A: Missouri Healthcare-Associated Infection
Reporting System- large IT project• Plan B: NHSN- complex and burdensome to ICP
– CDC proposal: vendors send HL7 messages to NHSN
• Plan C: Use Texas Hospital Discharge Data Network– Already reaches statewide except rural hospitals and will be
expanded to all ASCs under existing legislation– Claims file is called ANSI 837I, carries ICD9 claims data – ICP generated data attached to the ANSI 837
Common network carrying two data sets, claims and ICP-HAI.Both data sets can be used jointly to evaluate quality of care.
• Plan D – as needed• Option for public to report suspected SSIs to DSHS
– Poses significant challenges, particularly validation

HAI Report• Public summary for each reporting facility• Risk adjusted with a comparison of the risk- adjusted rates
for each reporting facility• Easy to read (consumer friendly)• Concise facility comments on report will be allowed• Posted on internet
Reporting Protections
• Confidential and privileged data• May not be used in a civil action to establish standard of
care• Enforcement- general hospital under Health and Safety
Code chapter 241, ASC under chapter 243
Potential Adverse Consequences of Reporting
• Diversion of resources from patient care to forms
• Creation of disincentives to treat higher risk patients• Misleading stakeholders through data manipulation

SB 288 Funding
• For FY 2008 DSHS requested $4.5M, 36 FTEs• LBB calculated $1.1M and 5 FTEs• FY 2009 DSHS requested $3.7M LBB calculated
$1.2M and 8 more FTEs• Other scenarios presented
Current status = not funded

• Safe, nurturing place
• Place of sanctuary
• Place of healing
Images of a Hospital
In one location• Lots of colonized and/or infected persons• Lots of vulnerable/susceptible persons• Lots of traffic between infected and vulnerable
persons Add in lots of antibiotic use
Reality of a Hospital
Design a system to facilitate the spread of infection. What would it look like?– A Hospital
Design a system to select for antimicrobial resistance.
What would it look like?– A Hospital
Reality of a Hospital

Adopting Change

Transformational Change
• Transformation (1) alters the culture of the institution by changing select underlying assumptions and institutional behaviors, processes and products; (2) is deep and pervasive, affecting the whole institution; (3) is intentional; and (4) occurs over time.
• Incremental improvement is not enough
• The pace of improvement is not fast enough
Resources
•Institute for Healthcare Improvement www.ihi.org•Texas legislature www.legis.state.tx.us•Association of Professionals in Infection Control
•www.apic.org•DSHS HAI website www.texasdisease.org