peri-implant complications complications.pdf · esthetics, it is anticipated that the oral...
TRANSCRIPT

Peri-Implant Complications
Anastasia Kelekis-CholakisReem AtoutNader HamdanIoannis John Tsourounakis
A Clinical Guide to Diagnosis and Treatment
123

Peri-Implant Complications
Anastasia Kelekis-Cholakis • Reem AtoutNader Hamdan • Ioannis Tsourounakis
Peri-Implant ComplicationsA Clinical Guide to Diagnosis and Treatment

Anastasia Kelekis-CholakisUniversity of Manitoba College of DentistryWinnipeg Manitoba Canada
Nader HamdanFaculty of DentistryDalhousie UniversityHalifaxNova Scotia Canada
Reem AtoutUniversity of Manitoba College of DentistryWinnipeg Manitoba Canada
Ioannis TsourounakisSouthwest Specialty GroupWinnipeg Manitoba Canada
ISBN 978-3-319-63717-4 ISBN 978-3-319-63719-8 (eBook)https://doi.org/10.1007/978-3-319-63719-8
Library of Congress Control Number: 2018935192
© Springer International Publishing AG, part of Springer Nature 2018This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recita-tion, broadcasting, reproduction on microfilms or in any other physical way, and transmission or infor-mation storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed.The use of general descriptive names, registered names, trademarks, service marks, etc. in this publica-tion does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use.The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Printed on acid-free paper
This Springer imprint is published by the registered company Springer International Publishing AG part of Springer NatureThe registered company address is: Gewerbestrasse 11, 6330 Cham, Switzerland

v
Preface
With the ever increasing use of dental implants aimed at restoring function and esthetics, it is anticipated that the oral healthcare team will encounter peri-implant diseases more frequently.
In addition, given the increasing life spans of treated populations and the parallel advances in biomaterials and implant designs, dental implants are expected to func-tion for longer periods of time. It is therefore incumbent on the oral healthcare team to diagnose, treat, and prevent peri-implant diseases.
This clinical guide has endeavored to address biologic soft and hard tissue com-plications that occur after loading of dental implants. The etiology, diagnosis, and treatment options for each condition are discussed in each chapter. Possible risk indicators for the development of these conditions are reviewed based on current scientific evidence.
This book is recommended for any member of the oral healthcare team that maintains dental implants.
It provides a comprehensive, yet simple, review of peri-implant diseases that will guide the practitioner in the long-term maintenance of dental implants.
Winnipeg, MB, Canada Anastasia Kelekis-CholakisWinnipeg, MB, Canada Reem AtoutHalifax, NS, Canada Nader HamdanWinnipeg, MB, Canada Ioannis John Tsourounakis

vii
Contents
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants: Similarities and Differences . . . . . . . . . . . . . . . . . . . . . . . . . 1 1.1 Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 1.2 Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 1.3 Classification of Peri-Implant Diseases . . . . . . . . . . . . . . . . . . . . . . . 2 1.4 Peri-Implant Mucositis vs. Peri-Implantitis . . . . . . . . . . . . . . . . . . . . 5
1.4.1 Peri-Implant Mucositis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 1.4.2 Peri-Implantitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.5 Teeth vs. Dental Implants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6 1.5.1 Soft Tissues around Implants and Teeth . . . . . . . . . . . . . . . . 6 1.5.2 Fiber Arrangement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 1.5.3 Periodontal Probing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 1.5.4 Inflammatory Response . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 1.5.5 Biofilm . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13 1.5.6 Microflora around Dental Implants . . . . . . . . . . . . . . . . . . . . 14 1.5.7 Healing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
1.6 Summary of Important Concepts . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
2 Peri-implant Soft Tissue Deficiencies . . . . . . . . . . . . . . . . . . . . . . . . . . 21 2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
2.1.1 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 2.2 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33 2.3 Management/Treatment Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
2.3.1 Improving Peri-implant Soft Tissue Volume . . . . . . . . . . . . . 43 2.3.2 Improving the Width of Keratinized Mucosa . . . . . . . . . . . . 48
2.4 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
3 Peri-implant Mucositis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59 3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59 3.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3.2.1 Risk Indicators . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59 3.3 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
3.3.1 Bleeding on Probing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61

viii
3.3.2 Probing Depths/Radiographic Evaluation . . . . . . . . . . . . . . . 61 3.3.3 Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
3.4 Management/Treatment Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62 3.4.1 Patient Education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64 3.4.2 Systemic and Local Factors . . . . . . . . . . . . . . . . . . . . . . . . . . 64 3.4.3 Patient-Administered Plaque Control . . . . . . . . . . . . . . . . . . 69 3.4.4 Mechanical Plaque Control . . . . . . . . . . . . . . . . . . . . . . . . . . 69 3.4.5 Chemical Plaque Control . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71 3.4.6 Professional Debridement . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
3.5 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
4 Hard Tissue Complications/ Peri-implantitis . . . . . . . . . . . . . . . . . . . . 79 4.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79 4.2 Etiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
4.2.1 History of Periodontal Disease . . . . . . . . . . . . . . . . . . . . . . . 81 4.2.2 Smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84 4.2.3 Poor Oral Hygiene/Lack of Maintenance . . . . . . . . . . . . . . . 84 4.2.4 Diabetes, Alcohol Consumption, and Genetic Factors IL-1
Polymorphisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 85 4.2.5 Dental Implant Surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86 4.2.6 Occlusal Overload . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86 4.2.7 Lack of Keratinized Tissue . . . . . . . . . . . . . . . . . . . . . . . . . . 88 4.2.8 Iatrogenic Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88
4.3 Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91 4.3.1 Bleeding on Probing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 91 4.3.2 Probing Depths and Radiographic Evaluation . . . . . . . . . . . . 92 4.3.3 Suppuration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92 4.3.4 Mobility . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94 4.3.5 Prevalence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94 4.3.6 Disease Progression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95
4.4 Management/Treatment Options . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95 4.4.1 Removal of Etiologic Factors. . . . . . . . . . . . . . . . . . . . . . . . . 96 4.4.2 Nonsurgical Treatment of Peri-implantitis . . . . . . . . . . . . . . . 96 4.4.3 Surgical Treatment of Peri-implantitis . . . . . . . . . . . . . . . . . . 96
4.5 Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114
Contents

1© Springer International Publishing AG, part of Springer Nature 2018A. Kelekis-Cholakis et al., Peri-Implant Complications, https://doi.org/10.1007/978-3-319-63719-8_1
1An Introduction to Understanding the Basics of Teeth vs. Dental Implants: Similarities and Differences
1.1 Definitions
Throughout the next sections of this book, the reader will encounter a host of terms. For purposes of clarity, this is a list of some important definitions taken from the American Academy of Periodontology (AAP) Glossary of Periodontal Terms [1]:
• Peri-implant mucositis: A disease in which the presence of inflammation is con-fined to the mucosa surrounding a dental implant with no signs of loss of sup-porting bone.
• Peri-implantitis: An inflammatory process around a dental implant which includes both soft tissue inflammation and loss of supporting bone.
• Biotype: The thickness or dimension of the soft and hard tissue surrounding natural teeth or dental implants.
• Osseointegration: A direct contact, on the light microscopic level, between living bone tissue and a dental implant.
• Fibro-osseous integration: The interposition of healthy dense collagenous tissue between a dental implant and bone. Also known as fibro-osteal integration.
• Implant, oral: Endosseous root-form implant – an implant placed into the alveo-lar process and/or basal bone that derives its support from a vertical length of bone and supports a prosthesis or other devices. Most commonly made of tita-nium, it can be cylindrical, tapered, etc.
• Implant fixture: A synonym for a dental implant, especially an endosseous implant.
• Implant abutment: That part of an implant system that connects the dental implant with a prosthesis or other devices.
• Overdenture: Complete or partial removable denture supported by soft tissue and retained roots or implants to provide support, retention, and stability and reduce ridge resorption.
• Recession: The migration of the marginal soft tissue to a point apical to the cementoenamel junction of a tooth or the platform of a dental implant.

2
• Biologic width: The dimension of soft tissue composed of a connective tissue and epithelial attachment extending from the crest of bone to the most apical extent of the pocket or sulcus.
• Occlusal trauma: Injury resulting in tissue changes within the attachment apparatus due to physiologic or parafunctional forces which may exceed its adaptive capacity.
• Piezoelectric surgery: A surgery performed using an instrument which generates micro-vibrating motion via the application of electromagnetic forces on a poly-crystal; the micro-vibration of the metallic tip results in ostectomy and osteo-plasty of the bone in contact with the tip.
1.2 Epidemiology
The prevalence of peri-implant diseases has been reported to range from 5 to 63.4% according to different reports [2]. This variability is due to various studies reporting different findings depending on the study design, the definitions (threshold of bone loss) adopted for peri-implant diseases, population size, and other factors.
A better understanding of peri-implant diseases and a consensus on the diagnos-tic criteria will eventually help in reducing some of this variability in the prevalence of peri-implant mucositis and peri-implantitis.
1.3 Classification of Peri-Implant Diseases
A classification system for peri-implant diseases is highly desirable. This will assist healthcare professionals in determining accurate prevalence estimates, providing clear diagnoses, and assigning prognoses. It will also improve the communication between health professionals and researchers, as well as the evaluation of treatment outcomes. However, to date, there is no consensus on a certain classification system as far as the authors know. This is consistent with the lack of clarity on established diagnostic criteria, as well as management protocols of peri-implant diseases.
In this section, two proposed classification systems will be provided as examples:
• The first was proposed by Froum and Rosen in [3]. This classification for peri- implantitis is based on the severity of the disease. A combination of bleeding on probing and/or suppuration, probing depth, and extent of radiographic bone loss around the dental implant is used to classify the severity of peri-implantitis into early, moderate, and advanced categories (Table 1.1, Figs. 1.1, 1.2 and 1.3).
• Peri-implant mucositis is a disease confined to the mucosa and is reversible.
• Peri-implantitis includes both soft tissue inflammation and loss of support-ing bone and is irreversible.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

3
Table 1.1 Classification of peri-implantitis as proposed by Froum and Rosen [3]
Staging DefinitionEarly PD ≥ 4 mm (bleeding and/or suppuration on probinga)
Bone loss <25% of the implant lengthb
Moderate PD ≥ 6 mm (bleeding and/or suppuration on probinga)Bone loss 25% to 50% of the implant lengthb
Advanced PD ≥ 8 mm (bleeding and/or suppuration on probinga)Bone loss >50% of the implant lengthb
aNoted on two or more aspects of the implantbMeasured on radiographs from time of definitive prosthesis loading to current radiograph. If not available, the earliest available radiograph following loading should be used
a b
Fig. 1.1 Early peri-implantitis as proposed by Froum and Rosen [3]. (a) (left) Clinical photograph of early peri-implantitis at an implant at the maxillary left lateral incisor position. Note the inflamed tissue and exudate. (Froum and Rosen [3]). (b) (right) Radiograph of maxillary left lateral incisor with bone loss <25% of the implant length, depicting early peri-implantitis (Froum and Rosen [3])
a b
Fig. 1.2 Moderate peri-implantitis as proposed by Froum and Rosen [3]. (a) (left) Clinical view of an implant in the mandibular left first molar site. Note the exudate (Froum and Rosen [3]). (b) (right) Radiograph depicting moderate peri-implantitis, with bone loss of 25–50% of the implant length on the mesial and distal aspects of the implant (Froum and Rosen [3])
1.3 Classification of Peri-Implant Diseases

4
• The second classification system was proposed by Ata-Ali et al. in [4]. In their article Ata-Ali et al. proposed a classification for peri-implant mucositis and peri-implantitis based on the severity of the disease, using a combination of peri- implant clinical and radiological parameters to classify severity into several stages (stage 0A and 0B = peri-implant mucositis and stage 1 to 4 = peri- implantitis) (Tables 1.2 and 1.3).
Currently, there is no consensus on a classification system for peri-implant diseases.
a b c
Fig. 1.3 Advanced peri-implantitis as proposed by Froum and Rosen [3]. (a) (left) Clinical prob-ing distal to the implant at the maxillary left canine site measured 8 mm (Froum and Rosen [3]). (b) (middle) Bleeding on probing was noted 15 seconds following removal of the probe (Froum and Rosen [3]). (c) (right) Radiograph depicting moderate peri-implantitis with bone loss <50% of the implant length (Froum and Rosen [3])
Table 1.2 Classification of peri-implant mucositis as proposed by Ata-Ali [4]
Staging DefinitionStage 0A PPD ≤ 4 mm and BoP and/or SUP, with no signs of loss of supporting bone
following initial bone remodeling during healingStage 0B PPD > 4 mm and BoP and/or SUP, with no signs of loss of supporting bone
following initial bone remodeling during healing
PPD probing pocket depth, BoP bleeding on probing, SUP suppuration
Table 1.3 Classification of peri-implantitis as proposed by Ata-Ali [4]
Staging DefinitionStage I BoP and/or SUP and bone loss ≤3 mm beyond biological bone remodelingStage II BoP and/or SUP and bone loss >3 mm and <5 mm beyond biological bone
remodelingStage III BoP and/or SUP and bone loss ≥5 mm beyond biological bone remodelingStage IV BoP and/or SUP and bone loss ≥50% of the implant lengtha beyond biological
bone remodeling
BoP bleeding on probing, SUP suppurationaDepending on implant length, if peri-implantitis can be classified as simultaneously correspond-ing to more than one stage, the most advanced stage should be chosen
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

5
1.4 Peri-Implant Mucositis vs. Peri-Implantitis
1.4.1 Peri-Implant Mucositis
• It has been proven that the disease process around dental implants is similar to that which occurs around teeth. Peri-implant mucositis around dental implants is seen as the equivalent of gingivitis around natural teeth. Peri-implant mucositis may or may not progress to peri-implantitis as gingivitis may or may not prog-ress to periodontitis [5, 6].
• Plaque accumulation on the titanium surface and the formation of a biofilm seem to be essential for the initiation and progression of peri-implant diseases in a way similar to that found around natural teeth [7–9].
• Peri-implant diseases are linked to similar gram-negative bacteria associated with severe chronic periodontitis [5, 6, 10, 11].
• When effectively treated, peri-implant mucositis can be reversed back to health [5, 6].
• The relatively weak epithelial seal around dental implants is similar in function to that around natural teeth [12].
• The structural difference between teeth and dental implants does not seem to influence the host response to the bacterial insult [13, 14].
1.4.2 Peri-Implantitis
• Peri-implantitis is seen as the equivalent of periodontitis around natural teeth and similarly occurs when the overwhelming bacterial insult leads to a destructive host immune response.
• Studies have shown that peri-implantitis and periodontitis lesions from human biopsies have many features in common [13, 15].
• Bacterial species associated with periodontitis and peri-implantitis are similar. Moreover, Staphylococcus aureus may also be an important pathogen in the ini-tiation of peri-implantitis [13, 16, 17].
• The connective tissue adjacent to the pocket epithelium is infiltrated by inflam-matory cells, with B-lymphocytes and plasma cells being the most dominant cell types. Similar markers are upregulated between peri-implantitis and periodonti-tis, including proinflammatory cytokines such as interleukin (IL)-1, IL-6, IL-8, IL-12, and tumor necrosis factor (TNF)-alpha [18, 19].
• Despite those many similarities between teeth and dental implants, the severity and rate of disease progression may differ significantly in peri-implantitis when compared to periodontitis. Experiments that allowed undisturbed dental plaque
The removal of the biofilm from the dental implant surface is the primary objective when treating peri-implant mucositis and will lead to the reversal of disease to a state of health the majority of the time if adequately performed.
1.4 Peri-Implant Mucositis vs. Peri-Implantitis

6
formation on dental implants and teeth in humans and in dogs demonstrated a more advanced inflammatory cell infiltrate in the peri-implant mucosa. Features of experimentally created peri-implantitis and periodontitis have also been com-pared. The results suggested that clinical and radiographic signs of tissue destruc-tion were more pronounced in peri-implantitis cases. Furthermore, the size of the inflammatory cell infiltrate in the connective tissue was larger, approaching the crestal bone around implants [13, 20–23]. This could be attributed to the differ-ences in the orientation and insertion of collagen fibers around teeth compared to those around dental implants [22].
• All implants appear to be susceptible to peri-implantitis [24, 25].
1.5 Teeth vs. Dental Implants
There are many differences between dental implants and teeth at both the micro-scopic and the macroscopic level. Some of those differences are best summarized in Table 1.4 and Fig. 1.4.
Many articles and book chapters have reported on the similarities and differences that exist between tissues around teeth and those around dental implants. The reader is encouraged to consult the published literature on this topic including a recent review entitled “Peri-Implant and Periodontal Tissues: A Review of Differences and Similarities” [26]. Part of this section was adapted from this publication.
1.5.1 Soft Tissues around Implants and Teeth
• The anatomy and histology of soft tissues surrounding dental implants and teeth is structurally similar. Those are made up of keratinized oral epithelium, non- keratinized sulcular epithelium, and the underlying connective tissue.
Similar to teeth, the junctional epithelium connects to the dental implant/abutment surface via hemidesmosomes and basal lamina [27]. The combined height of the
Early diagnosis and intervention by the elimination of the bacterial biofilm and correction of other possible contributory factors is the most effective way in preventing peri-implant diseases.
Despite the similarities in both the bacterial etiology and the immune host response components between periodontitis and peri-implantitis, peri- implantitis progresses at a faster rate with more pronounced bone loss. This could be attributed to the differences in orientation and insertion of collagen fibers around teeth compared to those around dental implants.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

7
junctional epithelium and connective tissue attachment is usually referred to as the “biologic width.” Early work by Gargiulo et al. [28] estimated this to be about 2.04 mm around teeth. However, a recent systematic review concluded that there is no universal dimension for biologic width around teeth with large intra- and interin-dividual variances (subject sample range, 0.2–6.73 mm) [87].
• In a human histologic study, the length of the peri- implant seal was found to be about 4–4.5 mm [88]. When compared to the “biologic width” around teeth, the same attachment around dental implants was longer nearly by the factor of 1.5 mm [89].
• This protective distance that exists between the alveolar crest of bone and the base of the gingival pocket should always be kept constant and respected in order to avoid bone loss around teeth. If for any reason, e.g., deeply placed restorative margin, this biologic distance is not maintained, then bone around the affected tooth will resorb in what seems like an adaptive mechanism, to mitigate the
Table 1.4 Teeth are different from dental implants on both the micro- and the macroscopic levels
Teeth Dental ImplantsPeriodontal fibers Insert into cementum on the root
surfaces of natural teeth13 groups
Extend parallel to the surface of the implant and/or abutment2 groups
Connection Periodontal ligaments OsseointegrationConnective tissue Lower percentage of collagen fibers
Higher percentage of cellsMore vascular
Higher percentage of collagen fibersLower percentage of fibroblasts. Looks very similar to a scar tissueLess vascular
Blood supply to surrounding gingivae
Three different sources (the periodontal ligament space, the interdental bone, and the supraperiosteal region)
Two different sources (the supraperiosteal vessels and a few vessels from the bone)
Periodontal ligament space
Present Absent
Resistance to mechanical and microbiological insults
More resistant Less resistant
Biological width (BW) JE: 0.97–1.14 mmCT: 0.77–1.07 mmBW: 2.04–2.91 mm
JE: 1.88 mmCT: 1.05 mmBW: 3.08 mm
Sulcus depth ≤ 3 mm when healthy Could be >3 mm depending on multiple factors
Proprioception Periodontal mechanoreceptors OsseoperceptionTactile sensitivity High LowAxial mobility 25–100 μm 3–5 μmFulcrum when lateral force applied
Apical third of the root Crestal bone
Possible relief Pressure absorption, distribution Pressure concentration on the crestal bone
Adapted from different sources, mainly Tokmakidis et al. [85] and Ramoglu et al. [86].
1.5 Teeth vs. Dental Implants

8
effects of those noxious stimuli. A similar principle applies to dental implants where changes in the soft tissue to bone relationship may be one of the reasons for the early crestal bone loss seen around dental implants [29].
• Upon dental implant placement, the fast-moving epithelial cells will migrate api-cally until they reach the dental implant surface where they attach themselves rapidly through the basal lamina and the hemidesmosomes [30]. Another possi-ble attachment modality hypothesized is an indirect epithelium-to-implant con-tact [31]. This is very similar to what happens around teeth following soft tissue flap reflection and healing.
• Human studies have demonstrated that epithelium surrounding dental implants possess similar patterns of differentiation and function to gingival tissues [32]. However, what stops the epithelium from migrating further api-cally on the implant surface? The presence of granulation tissue adhering to the surface of the transmucosal components is considered the principal factor
Enamel
Sulcus
Sulcular(crevicular)epithelium
Junctionalepithelium
Connectivetissue
Cementum
Bone
Sulcularepithelium
Junctionalepithelium
Connectivetissue
Titanium implant
Bone
a b
Fig. 1.4 Schematic illustration of hard and soft tissue around a tooth and an implant. (a) Hard and soft tissue anatomy around a natural tooth demonstrates bone support with a periodontal ligament, a connective tissue zone above the crest of bone with connective tissue fibers (Sharpey’s) inserting into dentin, a long junctional epithelial attachment, a gingival sulcus lined with sulcular epithe-lium, and oral gingival epithelium (outer surface of gingiva). (b) Hard and soft tissue anatomy around an implant demonstrates some similarities and some distinct differences. There is support-ing bone in direct approximation to the implant surface without any intervening soft tissues (i.e., no periodontal ligament). A connective tissue zone is present above the level of bone with fibers running parallel to the implant surface and no inserting fibers. There is a long junctional epithelial attachment, a gingival or mucosal sulcus lined with sulcular epithelium, and oral gingival or muco-sal epithelium (outer surface of soft tissue) (From Rose LF, Mealey BL: Periodontics: Medicine, surgery, and implants, St. Louis, 2004, Mosby)
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

9
that prevents the apical migration of epithelium [33]. Berglundh speculated that this most likely occurs due to the interaction of the titanium surface with the soft tissue [34].
• The following sequence of events occur once an dental implant is inserted into bone: – Formation and adhesion of the fibrin clot to the dental implant surface – Adsorption of the fibrin clot to the dental implant surface and adsorption of
the extracellular matrix (ECM) proteins and connective tissue cells to the den-tal implant surface
– Transformation of the clot into granulation tissue and migration of epithelial cells on top of the fibrin clot/granulation tissue [35]
• The connective tissue zone next to the dental implant surface is primarily divided into two segments. – The first part is a 50 μm inner zone that is rich in fibers, resembling scar tissue
and containing several scattered fibroblasts in close contact with the titanium surface. This zone maintains the seal between the peri-implant bone and the oral environment [36, 37].
– The remaining part of the connective tissue is comprised of fibers running in different directions, along with cellular elements and blood vessels [37]. Connective tissue cells and collagen fiber bundles are separated from the TiO2 surface with a 20-nm-wide proteoglycan layer [38].
1.5.2 Fiber Arrangement
• In natural teeth, the non-keratinized junctional epithelium attaches to the enamel surface via the internal basal lamina and hemidesmosomes along the entire length of the junctional epithelium. In contrast, the attachment of the peri-implant epithelium to the implant surface is confined to the coronal region only.
• In human subjects, fibers have been described as running a parallel course to the dental implant surface [39]. Several other authors, however, have found fibers oriented in different directions. A perpendicular direction was also found with dental implants harboring porous surfaces [40, 41]. The orientation of fibers seems to be dependent on the quality of the mucosa: fibers tend to be parallel in alveolar mucosa and perpendicular in keratinized mucosa. In teeth, fibers insert perpendicularly into the cementum.
• Apart from the orientation of the fibers, there exists a significant difference between the connective tissue around the tooth and abutment. The dentogingival collagen fibers are firmly inserted into the cementum and the bone, in a
The “biologic width” should always be respected and maintained around the dental implant to decrease early bone loss.
1.5 Teeth vs. Dental Implants

10
perpendicular or oblique direction, thus serving as a barrier to the epithelial migration and the impending bacterial invasion [42]. The connective tissue adhe-sion with dental implants has poor mechanical resistance when compared to the one on natural teeth [43]. This in part explains the higher rate of disease progres-sion around dental implants compared to the more resistant cell-rich environ-ment that typically exists around natural teeth.
• Due to the reduced vascularization and parallel orientation of the collagen fibers, peri-implant tissues are more susceptible to inflammatory disease than periodontal tissues. This phenomenon can be verified immunohistochemically through increased formation of inflammatory infiltrate, nitric oxide 1/3, VEGF, lymphocytes, leukocytes, and Ki-67 [44]. Besides, in analogy to peri-odontitis, the level of matrix metalloproteinases (MMP), such as MMP-8, is increased up to 97.1% in peri-implant lesions. The latter can be used for diag-nostic purposes [45–47].
• There appears to be a resilient connection between bone, periodontal ligament, and cementum around a tooth. However, a rigid connection appears in the form of functional ankylosis/osseointegration, due to the lack of periodontal ligament, around the dental implant. Absence of resiliency somewhat leads to the direct transmission of the loads to the bone-implant interface, and no compensatory tooth movements can accommodate the occlusal disharmony.
• The lack of periodontal ligament also precludes the use of dental implants in growing individuals.
• The adaptive capacity of the periodontal ligament allows orthodontic tooth movements; however, such movements cannot be undertaken with dental implants.
• The highly sensitive receptors present within the periodontal ligament are responsible for the proprioceptive and tactile sensitivity around the tooth. Absence of the periodontal ligament leads to reduced tactile sensation and reflex function around dental implants [48].
1.5.3 Periodontal Probing
• Periodontal probing is one of the basic diagnostic tools used to measure clinical attachment level (CAL), pocket depth, and width of the attached gingiva [1].
• The probing depth is the distance between the gingival margin and the depth of the probe tip penetration into the pocket [49].
• Increased probing depth with concurrent loss of clinical attachment is pathogno-monic of periodontal disease [50].
Due to the reduced vascularization and parallel orientation of the collagen fibers, peri-implant tissues are more susceptible for inflammatory disease than periodontal tissues.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants
11
• Peri-implant probing provides an assessment of different parameters such as bleeding on probing, suppuration, and exudation from the sulcus and peri- implant tissues [40].
• Studies have shown that, when used, probe pressure of 0.5 N penetrates an aver-age of 0.7 mm deeper at implant sites [51]. Clinical probing depth is greater around dental implants versus teeth, as the probe tip ends apically to the junc-tional epithelium into the connective tissue close to the bone crest [52]. This explains why bleeding on probing is a more reliable sign of inflammation around a tooth but is less reliable around dental implants.
1.5.4 Inflammatory Response
• Diagnostic criteria for detection of peri-implant health and for monitoring the progression of disease are similar to that of periodontal disease. The gingival/mucosal tissues constitute the primary defense mechanism against microbial infections. The conversion of the junctional epithelium to the pocket epithelium is considered to be the key to the progression of gingivitis/peri-implant mucositis to periodontitis/peri-implantitis.
• When performing visual inspection of peri-implant soft tissues signs of disease include color alteration, swelling, thickness, and bleeding on probing, all clinical indices used for the evaluation of gingival disease. Inflammatory lesions may be present in the absence of visual signs of inflammation.
• The peri-implant crevice is surgically created and is not developed as it is for natural teeth. Pocket depth is determined by many factors such as abutment height, depth of fixture countersinking at stage 1 surgery, and the amount of tis-sue thinning during stage 2 surgery [37]. Structural differences between the peri- implant and periodontal tissues, dictate the probing pattern around dental implants as well.
• As stated previously, the parallel disposition of the collagen fibers to the implant surface and the absence of the connective tissue insertion cause the probe to go beyond the epithelial seal, which results in injury to the underlying connective tissue [53].
• Sulcular exudate from gingiva is called gingival crevicular fluid (GCF), and that from dental implants is known as peri-implant sulcular (crevicular) fluid (PISF/PICF). Gingival crevicular fluid is a healthy serum transudate in a healthy free gingiva, and during inflammation GCF is converted into an inflammatory exudate originating from the vessels of the gingival plexus. GCF is recognized as a part of the gingival defense system. GCF is rich in leucocytes, especially polymorphonuclear leukocytes (PMN), and is attracted
Gentle probing around dental implants during routine clinical examinations is necessary to diagnose early peri-implant disease.
1.5 Teeth vs. Dental Implants

12
by a chemotactic gradient of bacterial or host origin. It is also rich in host-derived molecules from blood, as well as substances from microorganisms of dental plaque. The GCF flow requires permeability- induced initiators of inflammation. About 65 different infection- induced enzymes and their inhibi-tors and regulators have been found [26].
• PISF is an inflammatory exudate originating from the vessels of the gingival plexus and is similar to GCF. It contains the host-derived enzymes and their inhibitors, host response modifiers, and tissue breakdown products. PISF vol-ume, along with increased enzymatic activity, has been suggested to be elevated during inflammation, which confirms the diagnostic potential of PISF in peri-implant inflammation.
• GCF functions to continuously flush the dentogingival crevice and release anti-microbial components of serum such as antibodies and complement enzymes. In disease, the crevicular fluid flow increases 30 times more than in health.
• The biologic inflammatory response of the tissues around teeth and dental implants depends largely on their histologic framework. Dental implants are surrounded by a dense network of collagen fibers that originate from the alveo-lar bone crest, and extend to the peri-implant mucosal margin in a parallel fashion, in contrast to teeth, where collagen fibers are perpendicular to the root surface. The fibers in peri-implant tissues appear very large and follow a circu-lar arrangement around the dental implant neck. Fiber-to-metal surface contact has generally not been observed. There are studies, however, that have observed direct fibrous attachment to the titanium surface [43]. The length of the supra-alveolar connective tissue in dental implants is also significantly larger than that of teeth. Teeth have multiple collagen bundle fibers that run in various directions to various adjacent structures. Studies based on the response of teeth and dental implants to experimental breakdown, have revealed the differences in the nature of tissue loss. Ligature-induced periodontal and peri-implant lesions, in beagle dogs, revealed more pronounced tissue destruction around dental implants than around teeth. Furthermore, the size of the soft tissue lesion was found to be larger around dental implants and extended into the bone mar-row [21]. Another study described the host response results of long-standing plaque and gingivitis. This study revealed an inflammatory cell infiltrate that extended more apical into the peri-implant mucosa (~ 1.5 mm) than the gingi-val tissues (~ 0.9 mm) [55].
• Histomorphometric studies have revealed that dental implants and teeth have a comparable ratio of collagen, vessels, and plasma cells, whereas peri-implant tissues have lower proportions of lymphocytes, macrophages, and PMNs. Hence, peri-implant tissues form a weaker biologic barrier to the api-cal migration of inflammatory cell infiltrate [20]. Another study measured the levels of myeloperoxidase (MPO) and nitrite as 2 molecular measures of inflammation between teeth and dental implants. Although MPO was found to be stable in healthy and diseased sites, in both GCF and PISF, nitrite levels were found to be significantly elevated in the PISF of diseased sites compared to healthy sites [56].
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

13
1.5.5 Biofilm
• When exposed in the oral cavity the transmucosal abutment of an osseointegrated dental implant provides a favorable surface for bacterial colonization. This further leads to the selective adsorption of salivary proteins, peptides, etc., and the rapid formation of pellicle [55]. Biofilm formation around dental implants is similar to that formed around teeth [57]. The composition of the pellicle around dental implants lacks the low molecular mucins commonly found on the enamel in natu-ral teeth. This may explain the qualitative and quantitative differences of plaque formation around dental implants, when compared to natural teeth [58]. However, these differences do not seem to influence the bacterial composition of the early biofilms formed on the dental implant surface. Biofilm formation on dental implants is influenced by the properties of the surface to be colonized, including chemical composition, surface roughness, and surface free energy [59].
• Many studies have pointed out the comparative rates and the composition of the microbiota associated with health and disease in teeth and dental implants [5, 60, 61]. Classic differences in the microbial profile of the peri-implant flora in cer-tain in vitro studies reveal an affinity of Staphylococcus aureus for the titanium surface; however, it is not commony found in the microflora around teeth [62]. This bacterium has, according to the results of Salvi et al. a high positive (80%) and negative (90%) predictive value for the development of peri-implantitis [63]. A host response to the bacterial challenge is known to develop irrespective of the dental implant system [64], while the initial host response to the bacterial chal-lenge in the peri-implant mucosa is similar to that found in gingiva. However, the long-standing inflammation does have a more pronounced response in the peri- implant tissues than in gingival tissues. This leads to the significant apical exten-sion of the inflammatory infiltrate in the peri-implant mucosa and the increased size of the lesion as compared to the gingival tissues [57].
• Histopathologic data of human case series have described the dominance of B cells and plasma cells in the inflammatory lesion, suggesting that peri-implantitis and periodontitis lesions are similar [65, 66]. Despite the fact that peri- implantitis and periodontitis develop similarly, the dynamics of this process could be differ-ent. Because the periodontitis lesion is walled off by the intact supracrestal con-nective tissue fiber compartment, the penetration of the infiltrate into the bone marrow is generally not evident. However, because of the absence of the supra-crestal connective tissue fibers, the peri-implantitis lesion often progresses rap-idly into the bone marrow [56, 67].
• Periodontitis and peri-implantitis share common risk factors, such as poor oral hygiene, tobacco consumption, and diabetes mellitus. Cross-sectional analyses have evaluated the risk indicators for peri-implantitis to be poor oral hygiene, history of periodontal disease tobacco consumption, diabetes mellitus, alcohol consumption, and genetic traits [68].
Periodontitis and peri-implantitis share common risk factors.
1.5 Teeth vs. Dental Implants

14
1.5.6 Microflora around Dental Implants
• The microbiota on dental implants in edentulous and partially edentulous patients and in patients with a history of periodontal disease varies. Studies have stated that the microbiota obtained from colonizing clinically healthy dental implant fixtures in fully edentulous subjects are similar to the microbiota associated with healthy periodontal sites in periodontally healthy subjects [69]. It was suggested that extraction of all teeth results in elimination of the Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans from the oral microbiota [70].
• In partially edentulous subjects the developing microbiota around dental implants is similar to that of natural teeth [71]. This microflora – 85% of which is identi-fied as gram-positive cocci—colonize the dental implant surface, immediately after the installation of the fixture. Microbial colonization and the ensuing inflammatory reaction in the peri-implant tissues might be analogous to the key events in the pathogenesis of periodontitis. The literature comparing the micro-biota around dental implants in fully edentulous and partially edentulous mouths, reports a higher percentage and frequency of black-pigmented bacteroides, fewer coccoids and motile rods, and a higher frequency of the P. gingivalis and P. inter-media on implant surfaces in partially edentulous subjects [72, 73]. The micro-biota of the remaining teeth serve as the primary source of the putative pathogens. This reveals that the microbial state of the remaining teeth influences the fate of the newly incorporated dental implants [74]. The microbiota on dental implants in subjects with a history of periodontal disease is similar in nature to those found in the periodontal pockets around teeth [75]. It would seem likely that susceptibility to periodontitis may translate to higher risk for peri-implantitis. Several reviews have reported a history of treated periodontitis as a risk indicator for implant outcomes with statistically significant results [17, 76, 77]. Zitzmann et al. quantified the incidence of the development of peri-implantitis in patients with a history of periodontitis almost six times higher than in patients with no history of periodontal inflammation [2].
1.5.7 Healing
• The healing response of tissues around dental implants varies from that of natu-ral teeth [78]. Dental implants exhibit a poor vascular supply compared to teeth. Following dental implant insertion, tissue repair requires development of the vasculature at the site of injury. The delivery of oxygen and nutrients, as well as the removal of cell debris is essential for a complete healing process [79].
Active periodontal disease should be controlled before placement of dental implants.Microbial biofilms on dental implants, in subjects with a history of periodon-tal disease, are similar to those found in periodontal pockets around teeth.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

15
• Berglundh reported that dental implants placed following flap elevation resulted in poor vascular supply between the junctional epithelium and marginal bone [34]. Ericcson explained that the poor vascular supply in the peri-implant mucosa may be the reason for the extensive progression of plaque-associated inflammation [55].
• In the presence of teeth, blood supply to the bone comes from 3 different sources: the periodontal ligament space, the connective tissue above the periosteum, and from within the bone. However, when a tooth is lost, periodontal ligament blood supply is also lost. Cortical bone by nature is poorly vascularized and has very few blood vessels running through it, in contrast to marrow bone. So, when soft tissue flaps are reflected for implant placement, the third and last source of blood supply from the soft tissue to the bone (supraperiosteal blood supply) is removed leaving poorly vascularized cortical bone with minimal or no vascular supply, thus prompting bone resorption during the initial healing phase [54, 80, 82]. With a flapless approach, the periosteum and blood vessels remain intact with clinically insignificant crestal bone loss for up to 4 years [90]. In an experimental study in pigs, Vlahović et al. concluded that when compared to conventional flap proce-dures, flapless techniques minimized postoperative bone inflammatory reactions [91]. Furthermore, flapless implant placement results in the reduction of surgery duration, pain intensity, related analgesic consumption and most other complica-tions typical in the postimplant surgery period, accelerating the postsurgical heal-ing as the amount of tissue injury is known to influence the speed and quality of healing [81, 92, 93]. In spite of these evident advantages, the major drawback of flapless approach is that it is a “blind” surgical technique. Nevertheless, the devel-opment of three-dimensional imaging technology and computer-guided implanto-logy and its recent widespread adoption in the field of dental implantology have improved the accuracy in the preparation of dental implant sites [91, 94–96]
• Due to similar etiologies of periodontal and peri-implant infections, the thera-peutic approaches also appear to be similar – i.e., anti-infective. Evidence sug-gests that the long-term results of periodontal treatment are promising [83]. Since existing periodontal lesions can become a reservoir of pathogens to colo-nize the dental implant surface, it is imperative to successfully treat and control periodontal disease prior to dental implant placement. Periodontal treatment involves the debridement of the contaminated root surfaces, whereas the treat-ment of peri- implantitis focuses on the decontamination of the dental implant surface. Despite the surface roughness and configuration, decontamination of the titanium surface poses inherent problems and can likely not be achieved by debridement alone. Animal studies have concluded that no method of dental implant surface decontamination is superior to another [84].
Despite the surface roughness and configuration, decontamination of the tita-nium surface poses inherent problems and can likely not be achieved by debridement alone. Animal studies have concluded that no method of dental implant surface decontamination is superior to another.
1.5 Teeth vs. Dental Implants
16
1.6 Summary of Important Concepts
• Peri-implant mucositis is a disease confined to the mucosa and is reversible.• Peri-implantitis includes both soft tissue inflammation and loss of supporting
bone and is irreversible.• Currently, there is no consensus on a classification system for peri-implant
diseases.• The removal of the biofilm from the implant surface is the primary objective in
the treatment peri-implant mucositis and will lead to the reversal of disease, in most cases, if properly performed.
• Despite the similarities in both the bacterial etiology and the immune host response, between periodontitis and peri-implantitis, peri-implantitis progresses at a faster rate with more pronounced bone loss. This can be attributed to the differences in orientation and insertion of collagen fibers around teeth vs. dental implants.
• Early diagnosis and intervention, by eliminating the bacterial biofilm and con-trolling other possible contributing factors, is the most effective way in prevent-ing peri-implant diseases.
• The “biologic width” should always be respected and maintained around dental implants to avoid early bone loss.
• Due to the reduced vascularization and parallel orientation of the collagen fibers, peri-implant tissues are more prone to inflammatory breakdown than periodontal tissues.
• Gentle probing around dental implants during routine clinical examinations is necessary to diagnose early peri-implant disease.
• Periodontitis and peri-implantitis share common risk factors.• Active periodontal disease should be controlled before placement of dental implants.• Microbiota on dental implants in subjects with a history of periodontal disease
are similar in nature to those found in the periodontal pockets around teeth.• Despite the surface roughness and configuration, decontamination of the tita-
nium surface poses inherent problems and can likely not be achieved by debride-ment alone. Animal studies have concluded that no method of dental implant surface decontamination is superior to another.
References
1. Periodontology AAo. Glossary of periodontal terms: American Academy of Periodontology; 2001.
2. Smeets R, Henningsen A, Jung O, Heiland M, Hammächer C, Stein JM. Definition, etiology, prevention and treatment of peri-implantitis—a review. Head Face Med. 2014;10:1.
3. Froum SJ, Rosen PS. A proposed classification for peri-implantitis. Int J Periodontics and Restorative Dentistry. 2012;32:533.
4. Ata-Ali J, Ata-Ali F, Bagan L. A classification proposal for peri-implant mucositis and peri- implantitis: a critical update. The Open Dentistry J 2015;9.
5. Pontoriero R, Tonelli M, Carnevale G, Mombelli A, Nyman S, Lang N. Experimentally induced peri-implant mucositis. A clinical study in humans. Clin Oral Implants Res 1994;5:254–9.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

17
6. Salvi GE, Aglietta M, Eick S, Sculean A, Lang NP, Ramseier CA. Reversibility of experi-mental peri-implant mucositis compared with experimental gingivitis in humans. Clin Oral Implants Res. 2012;23:182–90.
7. Berglundh T, Lindhe J, Marinell C, Ericsson I, Liljenberg B. Soft tissue reaction to de novo plaque formation on implants and teeth. An experimental study in the dog. Clin Oral Implants Res. 1992;3:1–8.
8. Quirynen M, Vogels R, Peeters W, Steenberghe D, Naert I, Haffajee A. Dynamics of ini-tial subgingival colonization of ‘pristine’peri-implant pockets. Clin Oral Implants Res. 2006;17:25–37.
9. Augthun M, Conrads G. Microbial findings of deep peri-implant bone defects. Int J Oral Maxillofacial Implants 1997;12.
10. Leonhardt Å, Berglundh T, Ericsson I, Dahlén G. Putative periodontal and teeth in pathogens on titanium implants and teeth in experimental gingivitis and periodontitis in beagle dogs. Clin Oral Implants Res. 1992;3:112–9.
11. Mombelli A, Lang NP. The diagnosis and treatment of peri-implantitis. Periodontology. 1998;17:63–76.
12. Gould T, Westbury L, Brunette D. Ultrastructural study of the attachment of human gingiva to titanium in vivo. J Prosthet Dent. 1984;52:418–20.
13. Rosen P, Clem D, Cochran D, et al. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84:436–43.
14. Zitzmann N, Berglundh T, Marinello C, Lindhe J. Experimental peri-implant mucositis in man. J Clin Periodontol. 2001;28:517–23.
15. Konttinen YT, Ma J, Lappalainen R, et al. Immunohistochemical evaluation of inflammatory mediators in failing implants. Int J Periodontics Restorat Dentistry. 2006;26.
16. Heitz-Mayfield LJ, Lang NP. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontology. 2010;53:167–81.
17. Leonhardt Å, Renvert S, Dahlén G. Microbial findings at failing implants. Clin Oral Implants Res. 1999;10:339–45.
18. Duarte PM, De Mendonça AC, Máximo MBB, Santos VR, Bastos MF, Nociti Júnior FH. Differential cytokine expressions affect the severity of peri-implant disease. Clin Oral Implants Res. 2009;20:514–20.
19. Javed F, Al-Hezaimi K, Salameh Z, Almas K, Romanos GE. Proinflammatory cytokines in the crevicular fluid of patients with peri-implantitis. Cytokine. 2011;53:8–12.
20. Ericsson I, Berglundh T, Marinello C, Liljenberg B, Lindhe J. Long-standing plaque and gin-givitis at implants and teeth in the dog. Clin Oral Implants Res. 1992;3:99–103.
21. Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res. 1992;3:9–16.
22. Schou S, Holmstrup P, Reibel J, Juhl M, Hjørting-Hansen E, Kornman KS. Ligature-induced marginal inflammation around osseointegrated implants and ankylosed teeth: stereologic and histologic observations in cynomolgus monkeys (Macaca Fascicularis). J Periodontol. 1993;64:529–37.
23. Zitzmann N, Berglundh T, Ericsson I, Lindhe J. Spontaneous progression of experimentally induced periimplantitis. J Clin Periodontol. 2004;31:845–9.
24. Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of peri- implantitis at different types of implants. An experimental study in dogs. I: clinical and radio-graphic observations. Clin Oral Implants Res. 2008;19:997–1002.
25. Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of ligatured induced peri-implantitis at implants with different surface characteristics. An experimental study in dogs II: histological observations. Clin Oral Implants Res. 2009;20:366–71.
26. Sangeeta Dhir B, Lanka Mahesh B, Gregori MK, Vandana K. Peri-implant and periodontal tissues: a review of differences and similarities. Compendium. 2013;34.
27. James RA, Schultz R. Hemidesmosomes and the adhesion of junctional epithelial cells to metal implants—a preliminary report. Oral Implantol. 1974;4:294.
28. Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of the dentogingival junction in humans. J Periodontol. 1961;32:261–7.
References

18
29. Oh T-J, Yoon J, Misch CE, Wang H-L. The causes of early implant bone loss: myth or science? J Periodontol. 2002;73:322–33.
30. Listgarten M, Lai C. Ultrastructure of the intact interface between an endosseous epoxy resin dental implant and the host tissues. J Biol Buccale. 1975;3:13.
31. Kawahara H, Kawahara D, Mimura Y, Takashima Y, Ong JL. Morphologic studies on the bio-logic seal of titanium dental implants. Report II. In vivo study on the defending mechanism of epithelial adhesion/attachment against invasive factors. Int J Oral Maxillofac Implants. 1998;13:465–73.
32. Liljenberg B, Gualini F, Berglundh T, Tonetti M, Lindhe J. Some characteristics of the ridge mucosa before and after implant installation a prospective study in humans. J Clin Periodontol. 1996;23:1008–13.
33. Listgarten MA. Soft and hard tissue response to endosseous dental implants. Anat Rec. 1996;245:410–25.
34. Berglundh T, Lindhe J, Ericsson I, Marinello C, Liljenberg B, Thornsen P. The soft tissue bar-rier at implants and teeth. Clin Oral Implants Res. 1991;2:81–90.
35. Meyle J. Cell adhesion and spreading on different implant surfaces. In: Proceedings of the 3rd European Workshop on Periodontology: ISBN 3–87652–306-0 Quintessenz Verlags-GmbH, Berlin, Germany, 1999:55–72.
36. Abrahamsson I, Berglundh T, Wennström J, Lindhe J. The peri-implant hard and soft tis-sues at different implant systems. A comparative study in the dog. Clin Oral Implants Res. 1996;7:212–9.
37. Buser D, Weber HP, Donath K, Fiorellini JP, Paquette DW, Williams RC. Soft tissue reac-tions to non-submerged unloaded titanium implants in beagle dogs. J Periodontol. 1992;63: 225–35.
38. Hansson H, Albrektsson T, Branemark P. Structural aspects of the interface between tissue and titanium implants. Plast Reconstr Surg. 1985;76:494.
39. Ericsson I, Lindhe J. Probing depth at implants and teeth. J Clin Periodontol. 1993;20:623–7. 40. Akagawa Y, Takata T, Matsumoto T, Nikai H, Tsuru H. Correlation between clinical and histo-
logical evaluations of the peri-implant gingiva around the single-crystal sapphire endosseous implant. J Oral Rehabil. 1989;16:581–7.
41. Schroeder A, van der Zypen E, Stich H, Sutter F. The reactions of bone, connective tissue, and epithelium to endosteal implants with titanium-sprayed surfaces. J Maxillofac Surg. 1981;9:15–25.
42. Stern IB. Current concepts of the dentogingival junction: the epithelial and connective tissue attachments to the tooth. J Periodontol. 1981;52:465–76.
43. Hermann JS, Cochran DL, Buser D, Schenk RK, Schoolfield JD. Biologic width around one- and two-piece titanium implants. Clin Oral Implants Res. 2001;12:559–71.
44. Degidi M, Artese L, Piattelli A, et al. Histological and immunohistochemical evaluation of the peri-implant soft tissues around machined and acid-etched titanium healing abutments: a prospective randomised study. Clin Oral Investig. 2012;16:857–66.
45. Sorsa T, Hernández M, Leppilahti J, Munjal S, Netuschil L, Mäntylä P. Detection of gingi-val crevicular fluid MMP-8 levels with different laboratory and chair-side methods. Oral Dis. 2010;16:39–45.
46. Sorsa T, Tervahartiala T, Leppilahti J, et al. Collagenase-2 (MMP-8) as a point-of-care bio-marker in periodontitis and cardiovascular diseases. Therapeutic response to non- antimicrobial properties of tetracyclines. Pharmacol Res. 2011;63:108–13.
47. Xu L, Yu Z, Lee H-M, et al. Characteristics of collagenase-2 from gingival crevicular fluid and peri-implant sulcular fluid in periodontitis and peri-implantitis patients: pilot study. Acta Odontol Scand. 2008;66:219–24.
48. Jacobs R, Dv S. Role of periodontal ligament receptors in the tactile function of teeth: a review. J Periodontal Res. 1994;29:153–67.
49. Hermann F, Lerner H, Palti A. Factors influencing the preservation of the periimplant marginal bone. Implant Dent. 2007;16:165–75.
50. Chow YC, Wang H-L. Factors and techniques influencing peri-implant papillae. Implant Dent. 2010;19:208–19.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

19
51. Armitage GC, Svanberc GK, Löe H. Microscopic evaluation of clinical measurements of con-nective tissue attachment levels. J Clin Periodontol. 1977;4:173–90.
52. Mombelli A, Lang NP. Clinical parameters for the evaluation of dental implants. Periodontology. 1994;4:81–6.
53. Ikeda H, Yamaza T, Yoshinari M, et al. Ultrastructural and immunoelectron microscopic stud-ies of the peri-implant epithelium-implant (Ti-6Al-4V) interface of rat maxilla. J Periodontol. 2000;71:961–73.
54. Fickl S, Zuhr O, Wachtel H, Bolz WG, Huerzeler M. Tissue alterations after tooth extraction with and without surgical trauma: a volumetric study in the beagle dog. J Clin Periodontol. 2008;35:356–63.
55. Kohavi D, Klinger A, Steinberg D, Sela MN. Adsorption of salivary proteins onto prosthetic titanium components. J Prosthet Dent. 1995;74:531–4.
56. Tözüm, Tolga F, et al. Analysis of the inflammatory process around endosseous dental implants and natural teeth: myeloperoxidase level and nitric oxide metabolism. Int J Oral Maxillofac Implants. 2007;22(6):969–79. Web.
57. Shibli JA, Melo L, Ferrari DS, Figueiredo LC, Faveri M, Feres M. Composition of supra-and subgingival biofilm of subjects with healthy and diseased implants. Clin Oral Implants Res. 2008;19:975–82.
58. Steinberg D, Klinger A, Kohavi D, Sela MN. Adsorption of human salivary proteins to tita-nium powder. I. Adsorption of human salivary albumin. Biomaterials. 1995;16:1339–43.
59. Teughels W, Van Assche N, Sliepen I, Quirynen M. Effect of material characteristics and/or surface topography on biofilm development. Clin Oral Implants Res. 2006;17:68–81.
60. Agerbaek MR, Lang NP, Persson GR. Comparisons of bacterial patterns present at implant and tooth sites in subjects on supportive periodontal therapy. Clin Oral Implants Res. 2006;17:18–24.
61. Quiryen M, Listgarten M. The distribution of bacterial morphotypes around natural teeth and titanium implants ad modum Brånemark. Clin Oral Implants Res. 1990;1:8–12.
62. Renvert S, Lindahl C, Renvert H, Persson GR. Clinical and microbiological analysis of sub-jects treated with Brånemark or AstraTech implants: a 7-year follow-up study. Clin Oral Implants Res. 2008;19:342–7.
63. Salvi GE, Fürst MM, Lang NP, Persson GR. One-year bacterial colonization patterns of Staphylococcus Aureus and other bacteria at implants and adjacent teeth. Clin Oral Implants Res. 2008;19:242–8.
64. Abrahamsson L, Berglundh T, Lindhe J. Soft tissue response to plaque formation at different implant systems. A comparative study in the dog. Clin Oral Implants Res. 1998;9:73–9.
65. Berglundh T, Gislason Ö, Lekholm U, Sennerby L, Lindhe J. Histopathological observations of human periimplantitis lesions. J Clin Periodontol. 2004;31:341–7.
66. Gualini F, Berglundh T. Immunohistochemical characteristics of inflammatory lesions at implants. J Clin Periodontol. 2003;30:14–8.
67. Seymour GJ, Powell R, Davies W. The immunopathogenesis of progressive chronic inflamma-tory periodontal disease. J Oral Pathol Med. 1979;8:249–65.
68. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. 2008;35:292–304.
69. Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontology. 2005;38:135–87. 70. Danser MM, van Winkelhoff AJ, Uvd V. Periodontal bacteria colonizing oral mucous mem-
branes in edentulous patients wearing dental implants. J Periodontol. 1997;68:209–16. 71. Mombelli A, Buser D, Lang N. Colonization of osseointegrated titanium implants in edentu-
lous patients. Early results. Oral Microbiol Immunol. 1988;3:113–20. 72. Hultin M, Boström L, Gustafsson A. Neutrophil response and microbiological findings around
teeth and dental implants. J Periodontol. 1998;69:1413–8. 73. Kalykakis G, Mojon P, Nisengard R, Spiekermann H, Zafiropoulos G. Clinical and microbial
findings on osseo-integrated implants; comparisons between partially dentate and edentulous subjects. Eur J Prosthodont Restor Dent. 1998;6:155–9.
74. Apse P, Ellen R, Overall C, Zarb G. Microbiota and crevicular fluid collagenase activity in the osseointegrated dental implant sulcus: a comparison of sites in edentulous and partially edentulous patients. J Periodontal Res. 1989;24:96–105.
References

20
75. Mombelli A, Marxer M, Gaberthüel T, Grander U, Lang NP. The microbiota of osseointegrated implants in patients with a history of periodontal disease. J Clin Periodontol. 1995;22:124–30.
76. Karoussis IK, Kotsovilis S, Fourmousis I. A comprehensive and critical review of dental implant prognosis in periodontally compromised partially edentulous patients. Clin Oral Implants Res. 2007;18:669–79.
77. Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Nine-to fourteen-year follow-up of implant treatment. Part III: factors associated with peri-implant lesions. J Clin Periodontol. 2006;33:296–301.
78. Etter TH, Håkanson I, Lang NP, Trejo PM, Caffesse RG. Healing after standardized clinical probing of the perlimplant soft tissue seal. Clin Oral Implants Res. 2002;13:571–80.
79. Arnold F, West DC. Angiogenesis in wound healing. Pharmacol Ther. 1991;52:407–22. 80. Wilderman MN, Pennel BM, King K, Barron JM. Histogenesis of repair following osseous
surgery. J Periodontol. 1970;41:551–65. 81. Sabiston DC. The biological basis of modern surgical practice. The Textbook of Surgery, 15th
edn, WB Saunders Company, Philadelphia. 1997;1484. 82. Campelo LD, Camara JRD. Flapless implant surgery: a 10-year clinical retrospective analysis.
Int J Oral Maxillofac Implants. 2002;17:271–6. 83. Lindhe J, Nyman S. Long-term maintenance of patients treated for advanced periodontal dis-
ease. J Clin Periodontol. 1984;11:504–14. 84. Schou S, Holmstrup P, Jørgensen T, et al. Implant surface preparation in the surgical treatment
of experimental peri-implantitis with autogenous bone graft and ePTFE membrane in cyno-molgus monkeys. Clin Oral Implants Res. 2003;14:412–22.
85. Tokmakidis K, Wessing B, Papoulia K, Spiekermann H. Load distribution and loading con-cepts on teeth and implants. Original study-ZZI 2009;1.
86. Ramoglu S, Tasar S, Gunsoy S, Ozan O, Meric G. Tooth-implant connection: a review. ISRN Biomaterials. 2012;2013:921645.
87. Schmidt JC, Sahrmann P, Weiger R, Schmidlin PR, Walter C. Biologic width dimensions—a systematic review. J Clin Periodontol. 2013;40:493–504. https://doi.org/10.1111/jcpe.12078.
88. Glauser R, Schüpbach P, Gottlow J, Hämmerle CHF. Periimplant soft tissue barrier at experi-mental one-piece mini-implants with different surface topography in humans: a light-micro-scopic overview and histometric analysis. Clin Implant Dent Relat Res. 2005;7:s44–51. https://doi.org/10.1111/j.1708-8208.2005.tb00074.x.
89. Linkevicius T. Biologic width around implants. An evidence-based. Stomatologija. 2008;10(1):27.
90. Becker W, Goldstein M, Becker BE, Sennerby L, Kois D, Hujoel P. Minimally invasive flapless implant placement: follow-up results from a multicenter study. J Periodontol. 2009;80:347–52.
91. Vlahović Z, Marković A, Lazić Z, Šćepanović M, Đinić A, Kalanović M. Histopathological comparative analysis of periimplant bone inflammatory response after dental implant insertion using flap and flapless surgical technique. An experimental study in pigs. Clin Oral Implants Res. 2017;28:1067–73. https://doi.org/10.1111/clr.12919.
92. Nkenke E, Eitner S, Radespiel-Troger M, Vairaktaris E, Neukam FW, Fenner M. Patient-centred outcomes comparing transmucosal implant placement with an open approach in the maxilla: a prospective, non-randomized pilot study. Clin Oral Implants Res. 2007;18:197–203.
93. Arisan V, Karabuda CZ, Ozdemir T. Implant surgery using bone- and mucosa-supported ste-reolithographic guides in totally edentulous jaws: surgical and post-operative outcomes of computer-aided vs. Standard techniques. Clin Oral Implants Res. 2010;21:980–8.
94. Azari A, Nikzad S. Flapless implant surgery: review of the literature and report of 2 cases with computer-guided surgical approach. J Oral Maxillofac Surg. 2008;66:1015–21.
95. Verhamme LM, Meijer GJ, Boumans T, Schutyser F, Berge SJ, Maal TJJ. A clinically rel-evant validation method for implant placement after virtual planning. Clin Oral Implants Res. 2013;24:1265–72.
96. Vercruyssen M, Hultin M, Van Assche N, Svensson K, Naert I, Quirynen M. Guided surgery: accuracy and efficacy. Periodontology. 2014;66:228–46.
1 An Introduction to Understanding the Basics of Teeth vs. Dental Implants

21© Springer International Publishing AG, part of Springer Nature 2018A. Kelekis-Cholakis et al., Peri-Implant Complications, https://doi.org/10.1007/978-3-319-63719-8_2
2Peri-implant Soft Tissue Deficiencies
2.1 Introduction
The definition of a “successful implant” has evolved over the years to include, beyond functional utility, high esthetic outcomes. Nowadays, a definition of a suc-cessful dental implant includes, among others, the patient’s and clinician’s esthetic satisfaction, which is achieved by a restoration that is in harmony with the surround-ing teeth and tissues [1]. The final restoration should match the size, form, and color of the adjacent teeth and be framed by soft tissues consistent in color, shape, and texture [2] (Fig. 2.1).
The harmonization of peri-implant structures may depend on several clinical parameters such as bone and soft tissue volume, precise implant placement, and the quality of the prosthetic restoration. Appropriate diagnosis and treatment planning is imperative to achieve a successful outcome.
Lack of keratinized mucosa, inadequate soft tissue volume, and peri-implant tis-sue recession may all result from inappropriate treatment planning and execution. Peri-implant soft tissue plastic surgery has been used to prevent and correct such tissue deficiencies. In this chapter both preventive and treatment strategies will be reviewed.
2.1.1 Etiology
Multiple factors may predispose to peri-implant soft tissue deficiencies. These fac-tors may have a synergistic effect on dental implant esthetics, stability of the peri- implant tissues, and peri-implant tissue health [3] (Table 2.1).
2.1.1.1 Inadequate Keratinized TissueThe need for keratinized mucosa around dental implants has been controversial. While some systematic reviews have shown no significant difference in long-term

22
peri-implant health and stability, others have disputed this conclusion. Wennström et al. examined the importance of keratinized tissue in maintaining peri-implant health and tissue stability. They concluded that there was limited evidence that keratinized tissue was necessary if plaque control was adequate. Appropriate width of keratinized tissue was defined as >2 mm [4]. However, recent evidence has shown a stronger correlation between the lack of keratinized tissue around dental implants and worse peri-implant parameters, including more pronounced gingival recession [5] (Fig. 2.2). Despite the controversy existing in the literature, on the need for keratinized tissue around dental implants, soft tissue augmentation may be advantageous for the maintenance of peri-implant soft tissue health [6]. Furthermore, an increased width of keratinized tissue may facilitate more effec-tive oral hygiene and improve peri-implant soft tissue health, as well as long-term soft tissue stability [7].
2.1.1.2 Soft Tissue Volume/Mucosal ThicknessThere is no general consensus on the amount of soft tissue needed around dental implants in order to maintain soft tissue architecture. Zigdon and Machtei found that thin mucosa (<1 mm) was associated with two times greater recession than thick (>1 mm) [8]. In addition, a narrow mucosal band (<1 mm) was associated with three times greater mucosal recession and more peri-implant attachment loss.
Fig. 2.1 Excellent hard and soft tissue outcome with a dental implant present in the maxillary right central incisor position
Table 2.1 Factors predis-posing to peri-implant recession
Inadequate keratinized mucosaSoft tissue volumePeriodontal biotypeDental implant positionPeri-implant bone volumePersistent inflammationTiming of implant placementProsthesis design and contour
Adapted from Jia-Hui Fu et al. “Esthetic soft tissue management for teeth and implants”. J Evid Based Dent Pract. 2012;12 (3 Suppl): 129–42
2 Peri-implant Soft Tissue Deficiencies

23
It has been recommended that the optimal thickness of the peri-implant tissue be around 2 mm [9, 10]. Evidence suggests that when the tissue volume is less than 2 mm, the restorative material may affect the esthetic outcome [11, 12]. Thus, all ceramic abutments/restorations should be used in order to achieve optimal esthetics. On the other hand, when the soft tissue volume is more than 2 mm, more options for the restorative materials are available, as the esthetic outcome does not seem to be compromised [13, 14] (Fig. 2.3).
There is evidence that soft tissue volume may facilitate hard tissue stability. A prospective controlled clinical trial found that significantly less bone loss occurred around bone-level implants placed in naturally thick buccal mucosa when compared to ones surrounded by thin soft tissue [15]. However, at this point in time, Akcali et al., in a systematic review, found that there is insufficient evidence that soft tissue thickness impacts crestal bone loss [16]. Unfortunately, a critical soft tissue dimen-sion that would offer long-term peri-implant soft tissue stability has not yet been universally accepted [17].
Fig. 2.2 Thin keratinized mucosa with high frenulum attachment on the mandibular first premolar implant, resulting in peri-implant tissue recession
Fig. 2.3 Sub-optimal soft tissue volume allowing the titanium abutment to show through the tissue creating a gray shadow, at the maxillary right first premolar implant
2.1 Introduction

24
2.1.1.3 Periodontal BiotypePeriodontal biotype plays a critical role in the predictability of the outcome and long-term stability of peri-implant soft tissues. Multiple studies have subdivided periodontal tissues into thin, scalloped, and thick, flat periodontium [18, 19]. Each periodontal biotype responds differently and has its own characteristics that may affect the final surgical outcome [20, 21] (Table 2.2). One of the difficulties in evaluating the data that attempts to link peri-implant biotype to mucosal reces-sion is that current studies have limited sample size and lack of consensus as to what is considered a thin or thick biotype. In some studies thin biotype is defined as “probe seen through the labial tissue,” while in others 1mm or less soft tissue thickness is used as a criterion. There are, however, some studies that have shown an increased risk of mucosal recession around dental implants, in patients with thin soft tissue biotype [22–24]. In general, periodontal biotype should be taken into consideration during treatment planning, keeping in mind that a thick peri-odontal biotype is typically more predictable in preserving the gingival architec-ture when compared to a thin biotype. In patients with a thin biotype, a more sophisticated treatment protocol should be selected in order to achieve the desired outcome (Figs. 2.4 and 2.5).
2.1.1.4 Dental Implant PositionImplant position in relation to the buccolingual, apico-coronal, and mesiodistal dimensions of the alveolar ridge is a factor that influences the degree of bone
Table 2.2 Characteristics of tissue biotypes, their association to tooth morphology, and the reac-tion of each biotype to inflammation, surgery, and tooth extraction
Periodontal biotypes Thin, scalloped biotype Thick, flat biotypeAnatomy and anatomical variations
Scalloped gingiva Flat soft tissueScalloped bone Flat bony architecturePointed papillae Short papillaeThin buccal plate Thick buccal plateIncreased prevalence of fenestration and dehiscence defects
Dehiscence and fenestration defects are rare
Tooth morphology Narrow teeth (tapered)Tooth proportions of 50–60%
Wide teeth (square)Tooth proportions of 80–90%
Inflammation Responds to inflammation by recession and loss of the thin alveolar bone
Responds to insult by pocket formation, and infra-bony defects
Surgery Delicate tissues, unpredictable healing (recession, tissue dehiscence)
Predictable hard and soft tissue healing
Tooth extraction Extensive ridge resorption Minimal ridge resorption
Sourced from: Olsson M and Lindhe J: Periodontal characteristics in individuals with varying form of the upper central incisors. J Clin Periodontol 1991; 18: 78-82, Becker W, Ochsenbein C, Tibbetts L, Becker BE. Alveolar bone anatomic profiles as measured from dry skulls. J Clin Periodontol 24:727-731,1997 Kao, R. T., Fagan, M. C. & Conte, G. J. (2008) Thick vs. thin gingival biotypes: a key determinant in treatment planning for dental implants. Journal of the California Dental Association 36, 193–198. De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J. The gingival biotype revisited: transparency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J Clin Periodontol 2009; 36: 428–433
2 Peri-implant Soft Tissue Deficiencies

25
remodeling following implant placement [25]. Bone remodeling may have a nega-tive impact on the soft tissue position around dental implants and could lead to unfavorable esthetic outcomes.
BuccolingualA recent systematic review identified buccal implant positioning as one of the fac-tors that can lead to resorption of the buccal plate and mucosal recession [26]. This finding was supported by another systematic review that reported that immediately placed implants that were buccally malpositioned in extraction sockets had a three times greater chance of recession when compared to more palatally placed implants [27] (Fig. 2.6).
Apico-coronalSome clinical guidelines have been proposed regarding the ideal dental implant positioning. Funato et al. described the ideal position as a restoration-driven 3D implant placement [28]. The author also suggested that the platform of the implant should be placed 2–4 mm below the mid-buccal aspect of the future gingival mar-gin. Buser described the concept of “comfort zone and danger zone,” when dental implants are placed in the esthetic zone, where the position of the dental implant
Fig. 2.4 Thick biotype, short papillae, flat tissue architecture
Fig. 2.5 Thin biotype, pointed papilla, scalloped gingiva
2.1 Introduction

26
shoulder should be at the ideal point of emergence [29]. He also suggested that the implant shoulder should be placed as shallow as possible and as deep as necessary, as a compromise between biological principles and esthetics.
MesiodistalThe distance between an implant and a tooth or among two implants can affect pap-illary height.
When considering implant placement adjacent to a tooth, the papilla fill depends mostly on the clinical attachment level of the adjacent tooth and more specifically on the apico-coronal distance from the alveolar bone crest to the contact point. Choquet et al. reported that when the distance from the alveolar crest to the contact point is 5 mm or less, the papilla was present in almost 100% of the cases, whereas when the distance increased to 6 mm or more, the papilla was present in only 50% or less of the cases [30]. The greater the distance from the bone crest to the contact point, the higher the risk for incomplete papilla fill. There is no current agreement in the literature on an absolute number that will result in a predictable papilla fill [9].
Buser et al. suggested that the mesiodistal distance between a tooth and an implant should not be less than 1.5 mm and between two implants should be 3 mm or more [29]. Therefore if this distance is not respected, there is a risk of bone loss resulting in loss of interproximal papilla.
When two implants are placed adjacent to each other, there appears to be an addi-tive osseous remodeling effect. A study with adjacent implants found that when implants were placed within 3 mm from each other, they developed 1.04 mm of interproximal bone loss compared to implants placed at a greater than 3.0 mm dis-tance, which lost only 0.45 mm of bone [31]. However a recent systematic review concluded that based on the current level of evidence, it is not possible to determine an absolute number for an optimal inter-implant distance. However, a tendency existed for incomplete papilla fill when adjacent implants were placed closer than 3 mm [32] (Fig. 2.7).
2.1.1.5 Peri-implant Bone VolumeA critical component of treatment planning in dental implant therapy is the amount of available bone. It has been postulated that to maintain stable peri-implant soft
Fig. 2.6 Peri-implant mucosal recession is obvious at the right maxillary central incisor due to the buccal position of the dental implant
2 Peri-implant Soft Tissue Deficiencies

27
tissue levels on the buccal aspect of dental implants, a minimum amount of 1–2 mm of buccal bone needs to be present [33, 34]. While some studies support the con-cept that a thick buccal plate will support peri-implant soft tissues and prevent recession, others have disputed this claim [35]. Given the fact that no consensus currently exists in the literature, it would seem prudent for the clinician to aim at obtaining a buccal plate thickness of 1–2 mm. This can be accomplished by various ridge augmentation methods. Buser et al. in a 10-year follow-up of 41 implant cases placed in conjunction with GBR found that this technique achieved good dimensional stability over several years [36]. This has been supported by a recent consensus report that stated that “lateral bone augmentation procedures are associ-ated with peri- implant soft tissue stability based on bleeding on probing (BOP), probing depth (PD), and marginal bone levels (mBI) ranging from 1- to 10-year follow-up” [37].
2.1.1.6 Persistent InflammationPeri-implant diseases are defined as inflammatory lesions of the surrounding peri- implant tissues and include peri-implant mucositis and peri-implantitis. Both of these peri-implant diseases are infectious in nature and are caused by bacterial bio-films [38].
2.1.1.7 Timing of Implant PlacementTiming of implant placement may critically influence the final esthetic outcome [9]. The timing of dental implant placement is dependent on specific hard and soft tissue characteristics of the extraction socket. Hammerle et al. introduced a classification for implant placement in extraction sites outlining the advantages and disadvantages of each [39]. Chen and Buser amended this classification and used the terms imme-diate, early, and late implant placement [22] (Table 2.3).
2.1.1.8 Immediate Implant PlacementEven though the survival rate of immediately placed dental implants is comparable to early or late placements, the risk of mucosal recession is also elevated [40].
Fig. 2.7 Loss of inter-implant soft tissue due to inadequate inter-implant distance
2.1 Introduction

28
In a long-term follow-up study, the placement of immediate dental implants resulted in an average buccal mucosal recession of 1.13 mm [41]. This might be related to the dimensional changes of the alveolar bone and soft tissue following tooth extraction. Immediate implant placement does not reduce bone remodeling [42]. A history of periodontal disease, trauma, or pathology may also result in hard and soft tissue loss. In a recent systematic review, it was shown that immediate implant placement is associated with greater variability in outcomes and a higher frequency of recession of >1 mm of the mid-buccal mucosa in 9–41% of sites, 1–3 years postoperatively. In comparison, early implant placement exhibited no sites with recession >1 mm [27] (Fig. 2.8). Immediate implant placement is a surgically demanding procedure and requires an experienced skill set. Proper case selection is crucial to achieve the desired outcome.
Selection criteria to increase outcome predictability include:
1. Gingival levels of the failing tooth are at the same level as the adjacent and/or contralateral teeth.
2. The extraction socket has a fully intact buccal plate. 3. There is a thick gingival biotype. 4. The sagittal root position is favorable. 5. There is sufficient bone volume apical and palatal to the extraction socket to
allow for ideal three-dimensional implant placement with adequate primary sta-bility [40, 43].
In a review by Chen and Buser, it was noted that the majority of studies pub-lished after 2008 involving immediate implant placement imposed inclusion criteria that included a thick biotype and an intact buccal plate in an effort to reduce muco-sal recession [27]. Multiple treatment modalities have been utilized to minimize soft and hard tissue changes following immediate implant placement. Those include flapless surgery, simultaneous placement of connective tissue grafts, the use of bone grafts in the residual socket gap, and immediate provisionalization.
Another recent study demonstrated that the least amount of soft tissue changes occurred when a bone graft was placed in the residual socket gap after immediate implant placement followed by either a custom healing abutment or a provisional restoration [44]. In the same study, sites that received no bone graft or a stock heal-ing abutment showed significant tissue collapse.
Table 2.3 Timing of dental implant placement, following tooth extraction
Immediate implant placement Early implant placement
Late implant placement
Same day as extraction
Soft tissue healing4–8 weeks following tooth extraction
Partial bone healing12–16 weeks following tooth extraction
Complete bone healingMore than 16 weeks
Adopted from Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontology 2000. 2017;73(1):84–102
2 Peri-implant Soft Tissue Deficiencies
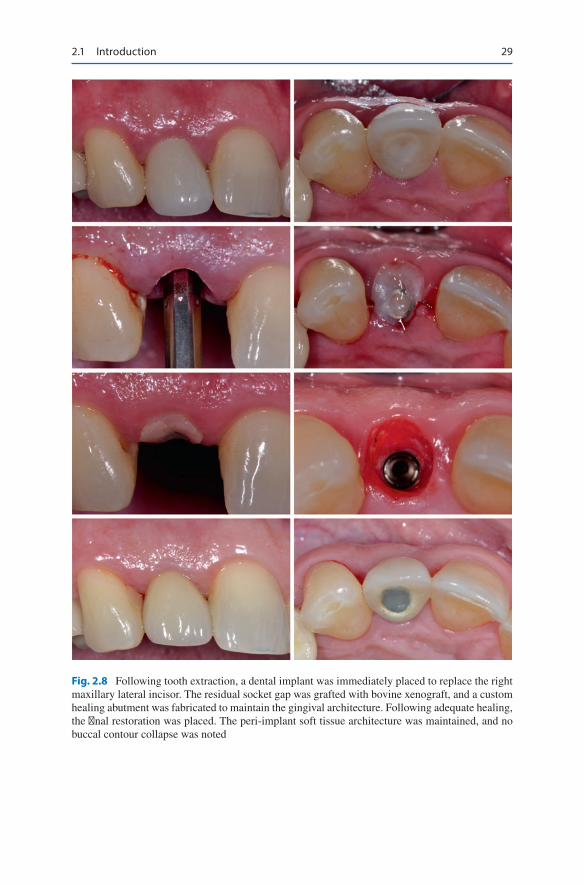
29
Fig. 2.8 Following tooth extraction, a dental implant was immediately placed to replace the right maxillary lateral incisor. The residual socket gap was grafted with bovine xenograft, and a custom healing abutment was fabricated to maintain the gingival architecture. Following adequate healing, the final restoration was placed. The peri-implant soft tissue architecture was maintained, and no buccal contour collapse was noted
2.1 Introduction

30
2.1.1.9 Early Implant PlacementThe concept of a 4–8-week healing period post extraction, to allow for soft tissue healing, is utilized in cases where additional height and thickness of soft tissue are required (Fig. 2.9). In a 3D analysis of alveolar bone changes at 8 weeks post extrac-tion, Chappuis et al. found that most osseous remodeling occurred in the center of
Fig. 2.9 The maxillary left central incisor was diagnosed with a root fracture and was deemed hopeless. Due to the buccal recession, the early implant placement protocol was selected to restore the edentulous site. Following 6 weeks of healing, a dental implant was placed at a favorable three-dimensional position. Contour augmentation was done with freeze-dried bone allograft and bovine xenograft. The graft was covered with an absorbable collagen membrane, which was secured with absorbable periodontal sutures. The implant was exposed, 6 months following placement. Significant buccal bone width was noted. An autogenous, vascularized, pedicle connective tissue graft was used to increase the soft tissue thickness. The peri-implant soft tissue was further devel-oped with a temporary implant-supported crown, to create satisfactory buccal tissue contour, mucosal margin level, and interproximal papillae
2 Peri-implant Soft Tissue Deficiencies

31
the facial plate with minimal changes in the proximal areas [45]. Consequently a two-wall morphology was present at 8 weeks post extraction facilitating osseous grafting and implant placement. Low risk for mucosal recession, good esthetic out-comes, and adequate facial bone thickness have been reported [43].
Early implant placement with partial bone healing is another dental implant placement protocol in the esthetic zone. This placement protocol has been advo-cated when a periapical bone lesion is present and hard tissue healing is desired to assist in appropriate implant position and primary stability [43].
2.1.1.10 Late Implant PlacementLate implant placement is advocated more than 16 weeks following osseous heal-ing. A randomized clinical trial compared soft tissue stability following immediate and delayed dental implant placement at 3 and 6 months. This study found no
Fig. 2.9 (continued)
2.1 Introduction

32
Fig. 2.10 The maxillary right central incisor was deemed hopeless due to severe loss of attach-ment. Following tooth extraction the site was developed through guided bone regeneration. After 6 months of healing, adequate ridge volume was noted. A dental implant was placed and, subse-quently, restored with a screw-retained prosthesis
significant differences in the soft tissue changes. Authors agree that both immediate and delayed implant placement approaches are appropriate and that the preferred treatment approach should be based on other factors such as bone dimension, dehis-cence, and fenestrations [46]. In another multicenter randomized controlled clinical trial, the esthetic outcome for both immediately and delayed single implants in the anterior maxilla was compared 1-year postoperatively. The authors reported that patients of both groups were equally satisfied at 4 months and 1 year after loading [47] (Fig. 2.10).
2 Peri-implant Soft Tissue Deficiencies

33
2.1.1.11 Prosthesis Design and ContourIn order to enhance the esthetic outcomes and healing around dental implants placed in an ideal position, it is critical to have a proper emergence profile of the restoration. A transition from the circumferential design of the dental implant plat-form to the correct cervical tooth anatomy is required for an appropriate restoration contour. The facial contour of the dental implant restorations could be flat, con-cave, or convex. Each contour has a different effect on the facial soft tissue healing and stability [48].
A recent study attempted to determine the effect of abutment contour on the peri- implant soft tissue around restored dental implants. This paper identified two dis-tinct zones within the implant abutment and crown, defined as critical and subcritical contours. The critical contour is located immediately apical to the mucosal margin (1.5 mm); it could be on the crown, abutment, or both, whereas the subcritical con-tour is the area located apical to the critical contour from the dental implant neck to the gingival margin [48]. Changes in the critical contour have a major influence on the stability of the mucosal margin around dental implants, while alterations in the subcritical contour have a minor effect. The concave or flat contour is often pre-ferred in order to avoid pressure on the buccal tissue, while over-contoured restora-tions may cause contraction of the buccal tissue and recession [48] (Fig. 2.11).
The type of abutment used could also influence the stability of the mucosal mar-gin around dental implants. In a 2-year prospective multicenter cohort study, 72 patients with single dental implants in the anterior area were examined [49]. In this study the authors concluded that zirconia and titanium cad-cam abutments had bet-ter mucosal margin stability when compared to the stock counterparts.
2.2 Diagnosis
Peri-implant tissue deficiencies may have an impact on the esthetic appearance of implant-supported restorations, as well as on the health status of the peri-implant tissues. Such deficiencies may refer to lack of keratinized tissue, and/or insufficient tissue volume, which includes thin peri-implant tissue and/or peri-implant tissue recession (Figs. 2.12, 2.13). To date, widely accepted definitions on peri-implant tissue deficiencies do not exist. No threshold has been defined, in regard to the lack of peri-implant keratinized tissue. Most studies, though, have identified that a band of peri-implant keratinized tissue of 1.5–2.0 mm may be advantageous for the maintenance of peri-implant health and stability of the peri-implant tissues. Furthermore, the term peri-implant tissue recession is unclear and confusing. Based on the glossary of periodontal terms, peri-implant tissue recession is the migration of the peri- implant mucosa, apical to the implant plat-form [50]. Although this definition may address the lack of tissue quantity, it does not address the presence or absence of keratinized tissue or the esthetic appearance of the implant restoration.
Multiple indices have been proposed in the literature for the objective assessment of the peri-implant tissues, surrounding implant-supported restorations. In 1997,
2.2 Diagnosis

34
Fig. 2.12 Lack of keratin-ized tissue, in conjunction with inadequate peri-implant tissue volume, may predis-pose to peri-implant tissue recession
Fig. 2.11 Gradual modification of the prosthesis contour and shape may alter the peri-implant soft tissue architecture. The temporary restoration of the implant at the left maxillary central inci-sor was modified to achieve favorable tissue architecture that would create symmetry and harmony, of the implant-supported crowns and the peri-implant tissues, with the adjacent teeth. (Courtesy of Dr. Jose D. Viquez)
2 Peri-implant Soft Tissue Deficiencies

35
Fig. 2.13 Peri-implant tissue enhancement is often needed before the delivery of the final restora-tion. The lack of attached and or keratinized peri-implant mucosa may hinder adequate oral hygiene and jeopardize the long-term outcomes
Table 2.4 Proximal contour papilla index
0 1 2 3 4Papilla fill
No papilla is present, and there is no indication of a curvature of the soft tissue contour adjacent to the single-implant restoration
Less than half of the height of the papilla is present. A convex curvature of the soft tissue contour adjacent to the single-implant crown and the adjacent tooth is observed
At least half of the height of the papilla is present, but not all the way up to the contact point between the teeth. The papilla is not completely in harmony with the adjacent papillae between the permanent teeth. Acceptable soft tissue contour is in harmony with adjacent teeth
The papilla fills up the entire proximal space and is in good harmony with the adjacent papillae. There is optimal soft tissue contour
The papillae are hyperplasic and cover too much of the single- implant restoration and/or the adjacent tooth. The soft tissue contour is more or less irregular
Sourced from Jemt T. Regeneration of Gingival Papillae After Single-Implant Treatment Int. J Periodont Rest Dent 1997:17:327-33
T. Jemt developed the “proximal contour papilla index” [51]. This index objectively measures the amount of interproximal tissue present, between a tooth and a dental implant (Table 2.4). The “papilla height classification system” [52] (Table 2.5) and the “modified Jemt papilla index” [53] (Table 2.6) are other indices that have been used for the evaluation of the interproximal peri-implant tissues as well.
More recently, a pilot study attempted to validate another index for the objective esthetic assessment of implant-supported restorations, the implant crown esthetic index [54]. This index takes into consideration nine parameters, which assess the color, form, and surface characteristics of the restoration and the peri-implant tis-sues. The clinician assigns penalty points, on a 5-point or a 3-point rating scale (depending on the parameter examined). The points are assigned based on the amount of mismatch or discrepancy that any of those nine parameters may have,
2.2 Diagnosis

36
with the adjacent and contralateral teeth and tissues (Table 2.7). Based on the num-ber of points accumulated, the esthetic result is deemed “excellent” (0 penalty points) or “poor” (5 points or more). However, if any major discrepancy or mis-match is noted, the esthetic result is automatically deemed poor. This study con-cluded that the implant crown esthetic index is a useful tool to objectively rate the esthetics of implant-supported single crowns. Nevertheless, its practical use needs to be determined with larger-scale clinical trials.
The “pink esthetic score” (PES) is another index that was developed, to objec-tively assess the peri-implant soft tissues, compared to the contralateral tooth [55]. This index evaluates seven variables: mesial papilla, distal papilla, soft tissue level, soft tissue contour, alveolar process deficiency, soft tissue color, and texture. Each variable is assessed with a score from 0 to 2, with 2 being the best and 0 the poorest score that can be achieved (Table 2.8). Hence, the highest score that can be achieved with PES is 14. This index showed a high level of reproducibility, in regard to the evaluation of the peri-implant soft tissues, of single-implant-supported restorations.
A cross-sectional, retrospective study attempted to objectively evaluate the esthetics of implants placed in the anterior maxilla, using the early implant place-ment protocol [56]. This study developed a new index to comprehensively assess outcome parameters, using objective esthetic criteria. This new index included the existing PES index, further simplified, and complemented by the “white esthetic score” (WES) index. The PES/WES index includes five parameters to assess the
Table 2.5 Papilla height classification system
Normal Class I Class II Class IIIPapilla level
Interdental papilla fills embrasure space to the apical extent of the interdental contact point/area
The tip of the interdental papilla lies between the interdental contact point and the most coronal extent of the interproximal CEJ (space present, but interproximal CEJ is not visible)
The tip of the interdental papilla lies at or apical to the interproximal CEJ, but coronal to the apical extent of the facial CEJ (interproximal CEJ visible)
The tip of the interdental papilla lies level with or apical to the facial CEJ
Sourced from Nordland & Tarnow. A Classification System for Loss of Papillary Height. J Periodontol 1998; 69:1124–1126
Table 2.6 Modified Jemt papilla index
0 1 2 3Papilla fill
No papilla or a negative papilla
Less than half of the height of the proximal area occupied by soft tissue
At least half of the height of the proximal area occupied by soft tissue
Interproximal area completely occupied by soft tissue
Sourced from Schropp & Isidor. Clinical outcome and patient satisfaction following full-flap ele-vation for early and delayed placement of single-tooth implants: A 5-year randomized study. Int J Oral Maxillofac Implants 2008;23:733–743
2 Peri-implant Soft Tissue Deficiencies

37
peri-implant soft tissues and five parameters for the implant-supported restoration (Table 2.9). These parameters are scored at a scale from 0 to 2 based on their har-mony and symmetry with the adjacent and contralateral teeth. The maximum score that can be attained with the PES/WES index is 20.
Table 2.7 Implant crown esthetic index
5 1 0 1 5Crown penalty points Mesiodistal
dimensionGrossly undercontoured
Slightly undercontoured
No mismatch
Slightly overcontoured
Grossly overcontoured
Position of incisal edge
Grossly undercontoured
Slightly undercontoured
No mismatch
Slightly overcontoured
Grossly overcontoured
Labial convexity
Grossly undercontoured
Slightly undercontoured
No mismatch
Slightly overcontoured
Grossly overcontoured
Color and translucency
Gross mismatch Slight mismatch
No mismatch
Surface Gross mismatch Slight mismatch
No mismatch
Mucosa penalty points Position of
labial margin of peri-implant mucosa
Deviation of ≥ 1.5 mm
Deviation of < 1.5 mm
No deviation
Position of mucosa in the approximal embrasures
Deviation of ≥ 1.5 mm
Deviation of < 1.5 mm
No deviation
Contour of the labial surface of the mucosa
Grossly undercontoured
Slightly undercontoured
No deviation
Slightly overcontoured
Grossly overcontoured
Color and surface of the labial mucosa
Gross mismatch Slight mismatch
No deviation
Total penalty points
Penalty points are assigned to each of the above items if not matching to the desired situation: one penalty point for minor (slight) deviations and five penalty points for major (gross) deviations. The total score leads to a final esthetic score:0 penalty points: excellent esthetics1 or 2 points: satisfactory esthetics3 or 4 points: moderate esthetics5 or more points: poor estheticsA major deviation automatically leads to a poor esthetic result and can never be accepted as moder-ate or satisfactorySourced from Meijer et al. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues – the Implant Crown Aesthetic Index. A pilot study on validation of a new index. Clin. Oral Impl. Res. 16, 2005; 645–649
2.2 Diagnosis

38
Table 2.9 PES/WES index
Pink esthetic scoreParameter Absent Incomplete Complete Mesial papilla 0 1 2 Distal papilla 0 1 2
Major discrepancy
Minor discrepancy
No discrepancy
Curvature of facial mucosa 0 1 2 Level of facial mucosa 0 1 2 Root convexity/soft tissue color and
texture0 1 2
Maximum total PES scoreWhite esthetic score (WES)Parameter Major
discrepancyMinor discrepancy
No discrepancy
Tooth form 0 1 2 Tooth volume/outline 0 1 2 Color (hue/value) 0 1 2 Surface texture 0 1 2 Translucency 0 1 2Maximum total WES score 10
Adopted from Belser et al. Outcome Evaluation of Early Placed Maxillary Anterior Single-Tooth Implants Using Objective Esthetic Criteria: A Cross-Sectional, Retrospective Study in 45 Patients With a 2- to 4-Year Follow-Up Using Pink and White Esthetic Scores. J Periodontol 2009;80:140-151
Table 2.8 The pink esthetic score
Variables 0 1 2Mesial papilla Shape vs reference
toothAbsent Incomplete Complete
Distal papilla Shape vs reference tooth
Absent Incomplete Complete
Level of tissue margin
Level vs reference tooth
Major discrepancy > 2 mm
Minor discrepancy 1–2 mm
No discrepancy < 1 mm
Soft tissue contour
Natural, matching reference tooth
Unnatural Fairly natural Natural
Alveolar process
Alveolar process deficiency
Obvious Slight None
Soft tissue color
Color vs reverence tooth
Obvious difference
Moderate difference
No difference
Soft tissue texture
Texture vs reference tooth
Obvious difference
Moderate difference
No difference
Adopted from Furhauser et al. Evaluation of soft tissue around single-tooth implant crowns: the pink esthetic score. Clin. Oral Impl. Res. 16, 2005; 639–644
The complex esthetic index (CEI) was proposed as a tool to rate the esthetics of anterior single-tooth implant-supported restorations [57]. The CEI consists of three different components. It includes a soft tissue index (S) and an implant-supported restoration index (R), for the evaluation of the peri-implant soft tissues and implant restorations. Additionally, the CEI includes a third component, the predictive index
2 Peri-implant Soft Tissue Deficiencies

39
(P). This component evaluates the mesial and distal bone height, the tissue biotype, the apico-coronal position of the implant, and the horizontal ridge contour. Each component of this index assesses five different characteristics that relate to the esthetic appearance of the peri-implant tissues and the implant-supported restora-tion. Each characteristic is rated as adequate (20%), compromised (10%), or inad-equate (0%) (Table 2.10). Each component is rated separately, and the combination of the three comprises the final CEI score. When all components are deemed ade-quate, then the CEI has a rating of 100%. If one of the components is compromised (60%–90%), then the CEI would render a compromised but clinically acceptable result. A <50% CEI rating is deemed esthetically unacceptable.
Those indices that have been reported in the literature show promising results in regard to their applicability and reproducibility. However, the present indices are lacking information that would propose any intervention to enhance peri-implant soft tissues, to improve esthetics or peri-implant tissue health, based on the index evaluation outcome. More recently, a classification system was proposed, evaluat-ing peri-implant tissue deficiencies around loaded dental implants [58]. This system
Table 2.10 Complex esthetic index (CEI)
Index and parameters
Rating and evaluation grades of parameter variationsAdequate (20%)
Compromised (10%)
Deficient (0%)
S: Soft tissue index 1. Soft tissue contour variations No <2 mm ≥ 2 mm 2. Soft tissue vertical deficiency No 1–2 mm ≥2 mm 3. Soft tissue color and texture
variationsNo Moderate Obvious
4. Mesial papillae appearance Complete fill Partial fill None 5. Distal papillae appearance Complete fill Partial fill NoneGeneral rating and evaluation grade 100% 60–90% <50%P: Predictive index
1. Mesial interproximal bone height <5 mm 5–7 mm >7 mm2. Distal interproximal bone height <5 mm 5–7 mm >7 mm3. Gingival tissue biotype >2 mm 1–2 mm <1 mm4. Implant pico-coronal position 1.5–3 mm >3-5 mm >5 mm5. Horizontal contour deficiency No 1–3 mm >3 mm
General rating and evaluation grade 100% 60–90% <50%R: Implant-supported restoration index
1. Color and translucency No Moderate Obvious2. Labial convexity in the abutment/
implant junctionNo <1 mm <2 mm
3. Implant/crown-incised edge position No ±1 mm ±2 mm4. Crown width/length ratio <0.85 0.85–1.0 >1.05. Surface roughness and ridges No Moderate Obvious
General rating and evaluation grade 100% 60–90% <50%
Each component is rated separately, and all evaluated parameters are graded as adequate (rating 20%), compromised (rating 10%), or deficient (rating 0%)Adopted from Juodzbalys & Wang. Esthetic Index for Anterior Maxillary Implant-Supported Restorations. J Periodontol 2010;81:34–42
2.2 Diagnosis

40
focuses on the enhancement of peri-implant tissues to improve peri-implant health. According to this classification, there are four distinct clinical scenarios:
• The width of keratinized tissue at the buccal aspect of the implant measures ≥2 mm.
• The width of keratinized tissue at the buccal aspect of the implant measures <2 mm (presence or absence of a frenulum, low inserting).
• The width of keratinized tissue at the buccal aspect of the implant measures <2 mm, and a soft tissue recession can be distinguished (i.e., the rough implant surface is visible). The peri-implant mucosa is thin, and no frenulum pull is visible.
• No or minimal width of keratinized tissue at the lingual aspect of the implant in the mandible.
This classification system proposes a treatment modality for peri-implant tissue enhancement, based on the type of deficiency.
Due to the great variety of methods, parameters, and measures used, there is still no commonly accepted index for the evaluation of dental implant restorations and peri-implant soft tissues. A recent systematic review concluded that “there is a strong need for a consensus on objective and well-defined parameters to assess aes-thetics in implant dentistry” [59]. Furthermore, a consensus for the diagnosis of peri-implant tissue deficiencies is also required, focusing on the need for peri- implant tissue enhancement, to improve and maintain peri-implant tissue health.
2.3 Management/Treatment Options
Mucogingival procedures come with a great variety of techniques and materials that offer treatment flexibility, improved esthetic outcomes [8], and better maintenance [60]. The esthetic outcome variables usually examined are recession coverage, soft tissue volume of the peri-implant tissue, gain of keratinized tissue, and interproxi-mal papillary fill. Recent evidence supports peri-implant tissue enhancement, as thicker peri-implant soft tissue will result in more favorable peri-implant parameters and long-term stability of the outcome. Evidence from earlier studies, however, is controversial on the need for soft tissue augmentation around dental implants.
A recent literature review [58] suggested that the timing of peri-implant mucosal augmentation is critical to reach the desired outcome. Evidence from this review indicated that attempting to enhance peri-implant soft tissues, after the delivery of a restoration, decreases significantly the predictability of the outcome. The authors advocated soft tissue enhancement during site development (pre-implant surgery) (Fig. 2.14), implant placement (Fig. 2.15), and/or at second-stage surgery (implant exposure) (Fig. 2.16), as the predictability of tissue augmentation increases, when compared to interventions after loading. However, in another systematic review, it
2 Peri-implant Soft Tissue Deficiencies

41
Fig. 2.14 Adequate site development is important to optimize the final outcome. Following tooth extraction, freeze-dried bone allograft was used to preserve the ridge dimensions. An autogenous, pedicle connective tissue graft was also utilized to minimize the volumetric alterations after tooth extraction and further improve the ridge volume
was shown that similar outcomes of peri-implant soft tissue augmentation could be achieved regardless of the timing of intervention [61] (Fig. 2.17).
The appropriate treatment modality is selected based on the diagnosis that takes into consideration all predisposing factors. Bassetti et al. proposed a treatment decision tree, based on the pre-existing tissue quality/quantity [58] (Table 2.11). A coronally advanced flap with a subepithelial connective tissue graft (SCTG) is
2.3 Management/Treatment Options

42
Fig. 2.15 Ridge augmentation was performed to replace this congenitally missing lateral incisor. Although hard tissue volume increased significantly, a ridge deficiency is evident. An autogenous subepithelial connective tissue graft was utilized to increase the tissue volume at the time of implant placement. Following the delivery of the final restoration, adequate peri-implant tissue volume and keratinized tissue were noted, contributing to a pleasing esthetic outcome
proposed for type I deficiencies and a combination of vestibuloplasty with a free gingival graft (FGG) for type II deficiencies. Type III deficiencies would require a more extensive intervention as the authors advocated a combination of both the aforementioned treatment modalities. The same treatment modalities, also, apply for type IV deficiencies, which may, additionally, require apical repositioning of the floor of the mouth. Multiple treatment modalities have been advocated with two common outcomes: the gain of keratinized mucosa and the increase of peri-implant tissue volume.
2 Peri-implant Soft Tissue Deficiencies

43
Fig. 2.16 Two dental implants were placed in this severely resorbed alveolar ridge, following ridge augmentation. The implant sites lack soft tissue volume and keratinized mucosa. At the time of stage 2 surgery, vestibuloplasty was performed in conjunction with a split-thickness, apically positioned flap. Two, partially epithelialized, free soft tissue grafts were placed at the buccal aspect of each dental implants. After 4 weeks of healing, there is a significant increase in peri-implant tissue volume and keratinized mucosa
2.3.1 Improving Peri-implant Soft Tissue Volume
Subepithelial connective tissue grafts have been advocated for the treatment of mucosal recession and the increase of peri-implant tissue volume (Fig. 2.18). In a 6-month prospective study, ten patients were treated with a coronally advanced flap, in conjunction with a free connective tissue graft around restored dental implants. The flap was advanced to overcompensate the mucosal recession with an average of
2.3 Management/Treatment Options

44
Fig. 2.17 Significant peri-implant mucosal recession was noted at the maxillary right central inci-sor implant. Prior to flap elevation, the buccal contour of the existing crown was altered, to obtain a more concave abutment surface. A lateral sliding flap in conjunction with a connective tissue graft was performed to correct the mucosal recession. Significant resolution of the mucosal defect was observed, after 1 year. Further improvement was noted after 5 years, with a significant increase in peri-implant soft tissue volume
0.5 mm (0.2–1.2 mm). These patients had a mean mucosal recession defect of 3 mm, and 99.6% of recession coverage was obtained immediately following the procedure. Significant shrinkage of the tissue was noted after 1 month, giving a mean coverage of 75%. Further recession occurred after 6 months, for an average peri-implant recession coverage of 66% [62]. In a 1-year prospective study, 16 patients with non-submerged dental implants, with a mean buccal recession of 2 mm, were treated with a coronally advanced flap combined with a SCTG,
2 Peri-implant Soft Tissue Deficiencies

45
harvested from the maxillary tuberosity. After 1 year the recession defects were decreased to a mean of 0.3 mm resulting in 89.6% of mean coverage and 56.3% of complete defect resolution. Furthermore the esthetic evaluation through a visual analog scale (0–10) improved from 3.5 to 8.5 [63]. Zucchelli et al. evaluated the efficacy of peri-implant mucosal augmentation, through a surgical-prosthetic approach, around restored, single dental implants with buccal dehiscences [64]. In this study the implant crown was removed, and the abutment contour was altered. Each site was then grafted with a split-thickness, coronally advanced flap in con-junction with a SCTG. Following adequate healing, a new final restoration was placed. After 1 year, the mean soft tissue dehiscence coverage was 96.3%, and com-plete coverage was achieved in 75% of the treated sites.
Soft tissue substitutes have been suggested as an alternative to autogenous tissue grafts for the treatment of soft tissue defects around teeth and implants (Fig. 2.19). The abundance of tissue material, the lack of a second surgical site, as well as the reduced morbidity following the surgical procedure have made soft tissue allografts an attractive alternative [65].
Acellular dermal matrices (ADM) are the most studied soft tissue substitutes, as an alternative to autogenous tissue grafts, for the treatment of recession defects, around teeth. Although soft tissue allografts seem to have many advantages, SCTGs still remain the “gold standard.” A systematic review, by Cairo et al., demonstrated that a combination of a coronally advanced flap with ADM did not improve the clinical results, compared to the coronally advanced flap alone, when used to treat gingival recession defects [66]. Furthermore, in the same review, it was shown that
Table 2.11 Proposed intervention around loaded dental implants, based on the pre-existing peri- implant tissue condition
Soft tissue deficiency Proposed treatmentType I (buccal)Width of KM ≥2 mm
Subepithelial connective tissue graft + Coronally advanced flap
Type II (buccal)Width of KM < 2 mm (presence or absence of a frenulum low inserting)
Vestibuloplasty + Free gingival graft
Type III (buccal)Width of KM <2 mm in combination with a soft tissue dehiscence
Subepithelial connective tissue graft + Coronally advanced flap + Vestibuloplasty + Free gingival graft
Type IV (lingual)Minimal width or lack of keratinized mucosa at the lingual aspect
Vestibuloplasty + Free gingival graft
• Adequate vertical distance between the floor of the mouth and the alveolar ridge
Tunneling technique + Subepithelial connective tissue graft
Type IV (lingual)Minimal width or lack of keratinized mucosa at the lingual aspect • Floor of the mouth is elevated in relation to the alveolar ridge
Lowering of the floor of the mouth + Free gingival graft (split-skin graft)
Adapted from Bassetti et al. Soft tissue grafting to improve the attached mucosa at dental implants: A review of the literature and proposal of a decision tree. Quintessence Int 2015;46:499–510
2.3 Management/Treatment Options

46
a SCTG offered superior results, compared to ADM, when both grafts were com-bined with a coronally advanced flap. When it comes to dental implants, a system-atic review (Thoma et al.) concluded that the addition of various soft tissue allografts offers no benefit, in regard to the increase of keratinized mucosa and soft tissue volume, around dental implants, when compared with autogenous soft tissue grafts [67].
Fig. 2.18 Progressive recession was noted at this implant during the first 2 years in function. The peri-implant tissue is lacking keratinization and volume, and peri-implant tissue recession is evi-dent. Following the preparation of a split-thickness flap, a partially epithelialized connective tissue graft was used. The epithelialized part was placed toward the coronal aspect of the implant. The flap was advanced to cover only the de-epithelialized part of the tissue graft. Following 3 months of healing, complete coverage of the exposed rough surface is noted, along with a significant increase in peri-implant tissue volume and keratinized mucosa
2 Peri-implant Soft Tissue Deficiencies

47
Fig. 2.19 The maxillary left central incisor was lost due to trauma. Following extraction, 6 weeks were allowed for soft tissue healing. A dental implant was placed with the early implant placement protocol. Following implant placement, contour augmentation was performed using freeze-dried bone allograft, layered with a bovine xenograft and covered with an absorbable collagen mem-brane. A soft tissue allograft was used to increase the peri-implant soft tissue volume. Increased ridge volume is noted after 3 months of healing. Two weeks after the second-stage exposure, there is a significant increase in peri-implant tissue volume and presence of adequate keratinized tissue
2.3 Management/Treatment Options

48
2.3.2 Improving the Width of Keratinized Mucosa
A wider zone of keratinized tissue is proven to improve periodontal parameters and promote gingival health [5, 68]. The treatments described for the increase of kera-tinized mucosa include vestibuloplasty, apically positioned flap/vestibuloplasty (APF/V) in combination with autogenous tissue grafts (FGG or SCTG) (Fig. 2.20), or soft tissue substitutes (ADM or collagen matrices). The use of FGGs is a predict-able choice for the augmentation of the keratinized case around dental implants [69]. In a prospective study, vestibuloplasty alone was performed around 131 dental implants, placed at sites with a mean of 2.23 mm of keratinized mucosa [70]. The vestibuloplasty procedure was performed at the time of implant placement. This technique allowed for a mean of 5 mm increase in keratinized mucosa, compared to baseline. Furthermore, the result of this study indicated that the gain in keratinized tissue remained stable for a period of 4 years.
In a randomized controlled trial, vestibuloplasty alone was compared to vestibu-loplasty combined with FGG, in regard to the increase of keratinized tissue around dental implants [71]. The increase in keratinized tissue was significantly greater in the FGG group compared to vestibuloplasty alone (2.36 vs 1.15 mm). A similarly designed study compared APF/V in conjunction with ADM or FGG, in regard to the increase of peri-implant keratinized tissue [72]. This study demonstrated that the autogenous FGG was superior to ADM, with an increase in keratinized tissue of
Fig. 2.19 (continued)
2 Peri-implant Soft Tissue Deficiencies
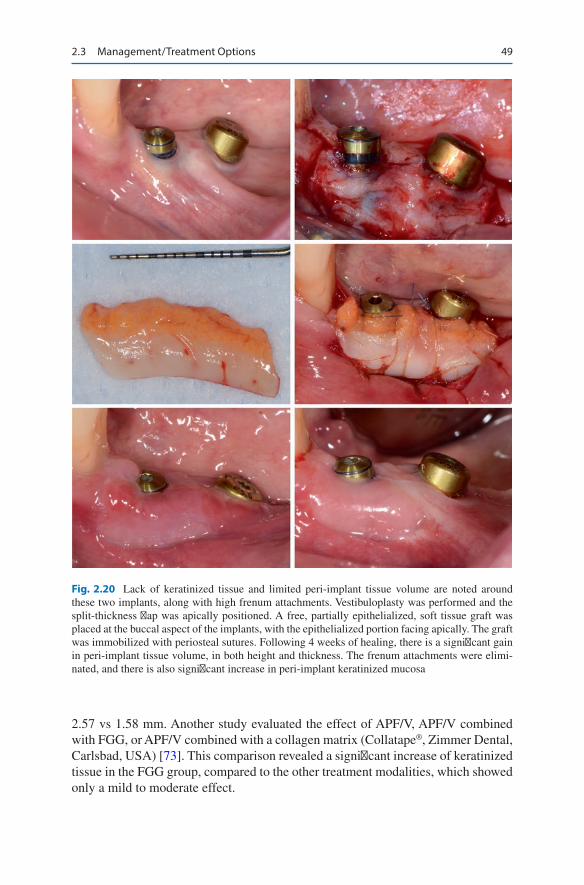
49
2.57 vs 1.58 mm. Another study evaluated the effect of APF/V, APF/V combined with FGG, or APF/V combined with a collagen matrix (Collatape®, Zimmer Dental, Carlsbad, USA) [73]. This comparison revealed a significant increase of keratinized tissue in the FGG group, compared to the other treatment modalities, which showed only a mild to moderate effect.
Fig. 2.20 Lack of keratinized tissue and limited peri-implant tissue volume are noted around these two implants, along with high frenum attachments. Vestibuloplasty was performed and the split-thickness flap was apically positioned. A free, partially epithelialized, soft tissue graft was placed at the buccal aspect of the implants, with the epithelialized portion facing apically. The graft was immobilized with periosteal sutures. Following 4 weeks of healing, there is a significant gain in peri-implant tissue volume, in both height and thickness. The frenum attachments were elimi-nated, and there is also significant increase in peri-implant keratinized mucosa
2.3 Management/Treatment Options

50
Recently, a porcine-derived collagen matrix (Mucograft®) has been introduced for the increase of keratinized tissue around teeth and implants (Fig. 2.21). In an experimental study, a prototype, porcine-derived collagen matrix (CM), was com-pared to SCTGs for large volume, soft tissue, ridge augmentations [74]. A volumet-ric analysis of digitized master casts revealed no significant differences between the two groups. This study concluded that this substitute may be a good alternative of SCTGs, for the augmentation of localized soft tissue ridge deficiencies. The efficacy
Fig. 2.21 Lack of keratinized tissue noted at the posterior maxillary right. Ridge augmentation was performed due to a severe ridge deficiency, which resulted in displacement of the mucogingi-val junction. Eight weeks following implant placement, vestibuloplasty was performed and the split-thickness flap was apically positioned. A soft tissue substitute was placed at the recipient bed and immobilized with periosteal sutures. After delivery of the final restoration, an increase of 2–3mm in keratinized tissue was noted
2 Peri-implant Soft Tissue Deficiencies

51
of this new CM has been assessed in multiple studies. In a randomized controlled trial, teeth or implant abutments of partial fixed restorations, with ≤1 mm of keratin-ized tissue, were treated with either SCTG or CM [75]. A significant increase in keratinized tissue, of 2.5 and 2.6 mm, was noted for the test and control groups, respectively. No significant differences were noted between groups, in terms of keratinized tissue gain. In a similarly designed study, the same collagen matrix was compared to SCTGs, regarding the increase of keratinized tissue around dental implants, only [76]. This study demonstrated a significant increase in keratinized tissue for both groups, with no significant difference between test and control (2.75 vs. 2.8 mm). Both of the abovementioned studies concluded that this CM is a suit-able substitute to SCTG, for increase of keratinized tissue around teeth and implants. Furthermore, both studies reported significantly lower patient morbidity and less surgical time, for the test group.
A Cochrane systematic review attempted to answer the question “what is the best approach to manage soft tissue recession around dental implants” [77]. The authors concluded that there is insufficient reliable evidence to provide a recom-mendation on which is the most effective soft tissue augmentation technique around dental implants. Another systematic review analyzed the efficacy of soft tissue grafting around dental implants in partially edentulous patients, in regard to the gain of keratinized tissue and the increase of peri-implant tissue volume [67]. This review concluded that better outcomes were observed, in terms of peri-implant tissue volume, when a coronally positioned flap combined with a SCTG was used, compared to a coronally advanced flap alone. Vestibuloplasty combined with a free gingival graft offered superior results in terms of increase in keratinized tissue compared to vestibuloplasty alone or no treatment. Soft tissue allografts (ADM) demonstrated very high shrinkage rates, with a histological picture that resembled scar tissue. The increase in keratinized tissue was similar for autogenous grafts (2.2–2.5 mm) and CMs (1.8–2.3 mm). However, CMs demonstrated better esthet-ics and less patient morbidity.
More recently, another systematic review assessed the influence of peri-implant tissue augmentation, on peri-implant health or disease, in partially or fully eden-tulous patients [78]. This review evaluated the increase of keratinized tissue width or increase in mucosal thickness, on various peri-implant parameters related to peri-implant disease (Fig. 2.22). The increase of keratinized tissue did not signifi-cantly affect BOP, when comparing augmented and non-augmented sites. However, there was a tendency for decreased BOP in augmented sites when com-pared to maintenance with mucosa alone. On the other hand, gingival index (GI) scores were significantly better for the augmented sites, compared to controls that had <2 mm width of keratinized tissue. Furthermore, augmented sites demon-strated significantly lower plaque scores (PI), compared to controls. Peri-implant probing depths (PD) and marginal bone levels were also superior to sites aug-mented with autogenous grafts, compared to all control treatments, with a statisti-cally significant difference. This meta-analysis favored APF combined with autogenous gingival grafts, over any other treatment modality, for the increase of peri-implant keratinized tissue.
2.3 Management/Treatment Options

52
Augmentation procedures for the increase of peri-implant mucosal thickness were predominantly recommended to improve implant esthetics. Only recent stud-ies have attempted to investigate the effect of mucosal thickness on peri-implant health [78]. Due to the lack of clinical data, this systematic review did not detect any influence of increased mucosal thickness on BOP, GI, or PI. Although limited data were also available regarding the effect of mucosal thickness on PDs and marginal
Fig. 2.22 These two implants are part of a full-arch, implant supported prosthesis, that was never completed. There is poor oral hygiene, lack of keratinized and attached mucosa, and mucosal recession. Vestibuloplasty and an apically positioned flap were performed, in conjunction with an autogenous free gingival graft. The graft was stabilized with periosteal and sling sutures. Following adequate healing, there is a significant increase in keratinized tissue and soft tissue volume. Oral hygiene has dramatically improved, however, the exposed rough dental implant surface will always be susceptible to plaque accumulation
2 Peri-implant Soft Tissue Deficiencies

53
bone levels, this data favored augmented sites, with increased mucosal thickness, compared to controls.
2.4 Summary
Peri-implant tissue deficiencies may compromise dental implant esthetics as well as peri-implant health. Inadequate peri-implant tissue volume and lack of keratinized tissue are the most common peri-implant tissue deficiencies that may predispose to peri-implant tissue recession. Tissue biotype, implant malposition, and poor pros-thesis design are also a few other factors that may contribute to peri-implant tissue recession. Unfortunately, to date, no uniform criteria exist for the diagnosis of peri- implant soft tissue deficiencies, and consequently no specific treatment modalities can be recommended for their management. Peri-implant soft tissue augmentation procedures may compensate for ridge volume deficiencies and improve peri-implant esthetics. Multiple techniques and materials have been described for the enhance-ment of peri-implant keratinized tissue and soft tissue volume. Based on the avail-able evidence, autogenous tissue grafts are the treatment of choice, and collagen matrices may be a good alternative. Peri-implant tissue augmentation with autoge-nous tissue grafts improved peri-implant parameters (BOP, GI, PI, PD) and demon-strated more stable marginal bone levels. Thus, improvements in quality and quantity of peri-implant soft tissues may play a critical role in the long-term survival and success of dental implants.
References
1. Myshin HL, Wiens JP. Factors affecting soft tissue around dental implants: a review of the literature. J Prosthet Dent. 2005;94(5):440–4.
2. Palacci P, Nowzari H. Soft tissue enhancement around dental implants. Periodontology. 2008;47(1):113–32.
3. Fu J-H, Su C-Y, Wang H-L. Esthetic soft tissue management for teeth and implants. J Evid Based Dent Pract. 2012;12(3):129–42.
4. Wennström JL, Derks J. Is there a need for keratinized mucosa around implants to maintain health and tissue stability? Clin Oral Implants Res. 2012;23:136–46.
5. Brito C, Tenenbaum HC, Wong BK, Schmitt C, Nogueira-Filho G. Is keratinized mucosa indispensable to maintain peri-implant health? A systematic review of the literature. J Biomed Mater Res B Appl Biomater. 2014;102(3):643–50.
6. Greenstein G, Cavallaro J. The clinical significance of keratinized gingiva around dental implants. Compend Contin Educ Dent. 2011;32(8):24–31.
7. Thoma DS, Mühlemann S, Jung RE. Critical soft-tissue dimensions with dental implants and treatment concepts. Periodontology. 2014;66(1):106–18.
8. Zigdon H, Machtei EE. The dimensions of keratinized mucosa around implants affect clinical and immunological parameters. Clin Oral Implants Res. 2008;19(4):387–92.
9. Jung RE, Heitz-Mayfield L, Schwarz F, Meeting GotnOFC. Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 3—Aesthetics of peri-implant soft tissues. Clin Oral Implants Res. 2018;29:14–7.
10. van Brakel R, Noordmans HJ, Frenken J, de Roode R, de Wit GC, Cune MS. The effect of zirconia and titanium implant abutments on light reflection of the supporting soft tissues. Clin Oral Implants Res. 2011;22(10):1172–8.
References

54
11. Sailer I, Zembic A, Jung RE, Siegenthaler D, Holderegger C, Hämmerle CHF. Randomized controlled clinical trial of customized zirconia and titanium implant abutments for canine and posterior single-tooth implant reconstructions: preliminary results at 1 year of function. Clin Oral Implants Res. 2009;20(3):219–25.
12. Zembic A, Sailer I, Jung RE, Hämmerle CHF. Randomized-controlled clinical trial of custom-ized zirconia and titanium implant abutments for single-tooth implants in canine and posterior regions: 3-year results. Clin Oral Implants Res. 2009;20(8):802–8.
13. Jung RE, Sailer I, Hammerle C, Attin T, Schmidlin P. In vitro color changes of soft tissues caused by restorative materials. Int J Periodontics Restorative Dent. 2007;27(3):251.
14. Jung RE, Holderegger C, Sailer I, Khraisat A, Suter A, Hämmerle CH. The effect of all- ceramic and porcelain-fused-to-metal restorations on marginal peri-implant soft tis-sue color: a randomized controlled clinical trial. Int J Periodontics Restorative Dent. 2008;28(4):357–65.
15. Puisys A, Linkevicius T. The influence of mucosal tissue thickening on crestal bone stability around bone-level implants. A prospective controlled clinical trial. Clin Oral Implants Res. 2015;26(2):123–9.
16. Akcalı A, Trullenque-Eriksson A, Sun C, Petrie A, Nibali L, Donos N. What is the effect of soft tissue thickness on crestal bone loss around dental implants? A systematic review. Clin Oral Implants Res. 2017;28(9):1046–53.
17. Schneider D, Grunder U, Ender A, Hämmerle CH, Jung RE. Volume gain and stability of peri- implant tissue following bone and soft tissue augmentation: 1-year results from a prospective cohort study. Clin Oral Implants Res. 2011;22(1):28–37.
18. Olsson M, Lindhe J. Periodontal characteristics in individuals with varying form of the upper central incisors. J Clin Periodontol. 1991;18(1):78–82.
19. De Rouck T, Eghbali R, Collys K, De Bruyn H, Cosyn J. The gingival biotype revisited: trans-parency of the periodontal probe through the gingival margin as a method to discriminate thin from thick gingiva. J Clin Periodontol. 2009;36(5):428–33.
20. Becker W, Ochsenbein C, Tibbetts L, Becker BE. Alveolar bone anatomic profiles as measured from dry skulls. J Clin Periodontol. 1997;24(10):727–31.
21. Kao RT, Fagan MC, Conte GJ. Thick vs. thin gingival biotypes: a key determinant in treatment planning for dental implants. J Calif Dent Assoc. 2008;36(3):193–8.
22. Chen ST, Buser D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int J Oral Maxillofac Implants. 2009;24(Suppl):186–217.
23. Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. Clin Oral Implants Res. 2007;18(5):552–62.
24. Kan JY, Rungcharassaeng K, Umezu K, Kois JC. Dimensions of peri-implant mucosa: an evaluation of maxillary anterior single implants in humans. J Periodontol. 2003;74(4):557–62.
25. Cardaropoli G, Lekholm U, Wennström JL. Tissue alterations at implant-supported single-tooth replacements: a 1-year prospective clinical study. Clin Oral Implants Res. 2006;17(2):165–71.
26. Lin G-H, Chan H-L, Wang H-L. Effects of currently available surgical and restorative interven-tions on reducing midfacial mucosal recession of immediately placed single-tooth implants: a systematic review. J Periodontol. 2014;85(1):92–102.
27. Chen ST, Buser D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 2014;29.(Suppl):186–215.
28. Funato A, Salama MA, Ishikawa T, Garber DA, Salama H. Timing, positioning, and sequen-tial staging in esthetic implant therapy: a four-dimensional perspective. Int J Periodontics Restorative Dent. 2007;27(4):313–23.
29. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior max-illa: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004;19(7):43–61.
30. Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retro-spective study in the maxillary anterior region. J Periodontol. 2001;72(10):1364–71.
31. Tarnow D, Cho S, Wallace S. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546–9.
2 Peri-implant Soft Tissue Deficiencies

55
32. Ramanauskaite A, Roccuzzo A, Schwarz F. A systematic review on the influence of the hori-zontal distance between two adjacent implants inserted in the anterior maxilla on the inter- implant mucosa fill. Clin Oral Implants Res. 2018;29:62–70.
33. Lang NP, Lindhe J. Clinical periodontology and implant dentistry, 2 Volume set. West Sussex, UK: Wiley; 2015.
34. Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: stage 1 placement through stage 2 uncovering. Ann Periodontol. 2000;5(1):119–28.
35. Merheb J, Vercruyssen M, Coucke W, Beckers L, Teughels W, Quirynen M. The fate of buccal bone around dental implants. A 12-month postloading follow-up study. Clin Oral Implants Res. 2017;28(1):103–8.
36. Buser D, Chappuis V, Kuchler U, Bornstein M, Wittneben J, Buser R, et al. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013;92(12_suppl):176S–82S.
37. Schwarz F, Giannobile W, Jung RE. Groups of the 2nd Osteology Foundation Consensus Meeting Evidence-based knowledge on the aesthetics and maintenance of peri-implant soft tissues: Osteology Foundation Consensus Report Part 2—Effects of hard tissue augmenta-tion procedures on the maintenance of peri-implant tissues. Clin Oral Implants Res 2018; Mar(29):11-13.
38. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84(4):436–43.
39. Hammerle C, Chen ST, Wilson TGJ. Consensus statements and recommended clinical pro-cedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004;19.(Suppl):26–8.
40. Kan JYK, Rungcharassaeng K, Deflorian M, Weinstein T, Wang HL, Testori T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontology. 2018;2000
41. Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G. Facial gingival tissue stability fol-lowing immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. Int J Oral Maxillofac Implants. 2011;26(1):179–87.
42. Cardaropoli G, Araujo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. J Clin Periodontol. 2003;30(9):809–18.
43. Buser D, Chappuis V, Belser UC, Chen S. Implant placement post extraction in esthetic single tooth sites: when immediate, when early, when late? Periodontology. 2017;73(1):84–102.
44. Tarnow DP, Chu SJ, Salama MA, Stappert J, Christian F, Salama H, et al. Flapless postextrac-tion socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent. 2014;34(3):323–31.
45. Chappuis V, Engel O, Reyes M, Shahim K, Nolte L-P, Buser D. Ridge alterations post- extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res. 2013;92(12_suppl):195S–201S.
46. van Kesteren CJ, Schoolfield J, West J, Oates T. A prospective randomized clinical study of changes in soft tissue position following immediate and delayed implant placement. Int J Oral Maxillofac Implants. 2010;25(3):562–70.
47. Esposito M, Barausse C, Pistilli R, Jacotti M, Grandi G, Tuco L, et al. Immediate loading of post-extractive versus delayed placed single implants in the anterior maxilla: outcome of a pragmatic multicenter randomised controlled trial 1-year after loading. Eur J Oral Implantol. 2015;8(4):347–58.
48. Su H, González-Martín O, Weisgold A, Lee E. Considerations of implant abutment and crown contour: critical contour and subcritical contour. Int J Periodontics Restorative Dent. 2010;30(4):335–43.
49. Lops D, Bressan E, Parpaiola A, Sbricoli L, Cecchinato D, Romeo E. Soft tissues stability of cad-cam and stock abutments in anterior regions: 2-year prospective multicentric cohort study. Clin Oral Implants Res. 2015;26(12):1436–42.
50. The American Academy of Periodontology. Glossary of periodontal terms. Illinois, CA: American Academy of Periodontology; 2001.
51. Jemt T. Regeneration of gingival papillae after single-implant treatment. Int J Periodontics Restorative Dent. 1997;17(4):326–33.
References

56
52. Nordland WP, Tarnow DP. A classification system for loss of papillary height. J Periodontol. 1998;69(10):1124–6.
53. Schropp L, Isidor F. Clinical outcome and patient satisfaction following full-flap elevation for early and delayed placement of single-tooth implants: a 5-year randomized study. Int J Oral Maxillofac Implants. 2008;23(4):733–43.
54. Meijer HJ, Stellingsma K, Meijndert L, Raghoebar GM. A new index for rating aesthetics of implant-supported single crowns and adjacent soft tissues–the Implant Crown Aesthetic Index. Clin Oral Implants Res. 2005;16(6):645–9.
55. Fürhauser R, Florescu D, Benesch T, Haas R, Mailath G, Watzek G. Evaluation of soft tis-sue around single-tooth implant crowns: the pink esthetic score. Clin Oral Implants Res. 2005;16(6):639–44.
56. Belser UC, Grütter L, Vailati F, Bornstein MM, Weber H-P, Buser D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: a cross- sectional, retrospective study in 45 patients with a 2-to 4-year follow-up using pink and white esthetic scores. J Periodontol. 2009;80(1):140–51.
57. Juodzbalys G, Wang HL. Esthetic Index for Anterior Maxillary Implant-Supported Restorations. J Periodontol. 2010;81(1):34–42.
58. Bassetti M, Kaufmann R, Salvi GE, Sculean A, Bassetti R. Soft tissue grafting to improve the attached mucosa at dental implants: A review of the literature and proposal of a decision tree. Quintessence Int. 2015;46(6):499–510.
59. Benic GI, Wolleb K, Sancho-Puchades M, Hämmerle CH. Systematic review of parameters and methods for the professional assessment of aesthetics in dental implant research. J Clin Periodontol. 2012;39(s12):160–92.
60. Prato GPP, Cairo F, Tinti C, Cortellini P, Muzzi L, Mancini EA. Prevention of alveolar ridge deformities and reconstruction of lost anatomy: a review of surgical approaches. Int J Periodontics Restorative Dent. 2004;24(5):434–45.
61. Poskevicius L, Sidlauskas A, Galindo-Moreno P, Juodzbalys G. Dimensional soft tissue changes following soft tissue grafting in conjunction with implant placement or around pres-ent dental implants: a systematic review. Clin Oral Implants Res. 2017;28(1):1–8.
62. Burkhardt R, Joss A, Lang NP. Soft tissue dehiscence coverage around endosseous implants: a prospective cohort study. Clin Oral Implants Res. 2008;19(5):451–7.
63. Roccuzzo M, Gaudioso L, Bunino M, Dalmasso P. Surgical treatment of buccal soft tissue recessions around single implants: 1-year results from a prospective pilot study. Clin Oral Implants Res. 2014;25(6):641–6.
64. Zucchelli G, Mazzotti C, Mounssif I, Mele M, Stefanini M, Montebugnoli L. A novel surgi-cal–prosthetic approach for soft tissue dehiscence coverage around single implant. Clin Oral Implants Res. 2013;24(9):957–62.
65. Zuhr O, Bäumer D, Hürzeler M. The addition of soft tissue replacement grafts in plastic peri-odontal and implant surgery: critical elements in design and execution. J Clin Periodontol. 2014;41(s15):123–42.
66. Cairo F, Pagliaro U, Nieri M. Treatment of gingival recession with coronally advanced flap procedures: a systematic review. J Clin Periodontol. 2008;35(s8):136–62.
67. Thoma DS, Buranawat B, Hämmerle CH, Held U, Jung RE. Efficacy of soft tissue augmen-tation around dental implants and in partially edentulous areas: a systematic review. J Clin Periodontol. 2014;(s15):41, S77–S91.
68. Chung DM, Oh T-J, Shotwell JL, Misch CE, Wang H-L. Significance of keratin-ized mucosa in maintenance of dental implants with different surfaces. J Periodontol. 2006;77(8):1410–20.
69. Ten Bruggenkate C, Krekeler G, Van Der Kwast W, Oosterbeek H. Palatal mucosa grafts for oral implant devices. Oral Surg Oral Med Oral Pathol. 1991;72(2):154–8.
70. Bruschi GB, Crespi R, Capparé P, Gherlone E. Clinical study of flap design to increase the keratinized gingiva around implants: 4-year follow-up. J Oral Implantol. 2014;40(4):459–64.
71. Başeğmez C, Ersanlı S, Demirel K, Bölükbaşı N, Yalcin S. The comparison of two tech-niques to increase the amount of peri-implant attached mucosa: free gingival grafts versus
2 Peri-implant Soft Tissue Deficiencies

57
vestibuloplasty. One-year results from a randomised controlled trial. Eur J Oral Implantol. 2012;5(2):139–45.
72. Basegmez C, Karabuda ZC, Demirel K, Yalcin S. The comparison of acellular dermal matrix allografts with free gingival grafts in the augmentation of peri-implant attached mucosa: a randomised controlled trial. Eur J Oral Implantol. 2013;6(2):145–52.
73. Lee K-H, Kim B-O, Jang H-S. Clinical evaluation of a collagen matrix to enhance the width of keratinized gingiva around dental implants. J Periodontal Implant Sci. 2010;40(2):96–101.
74. Thoma DS, Jung RE, Schneider D, Cochran DL, Ender A, Jones AA, et al. Soft tissue volume augmentation by the use of collagen-based matrices: a volumetric analysis. J Clin Periodontol. 2010;37(7):659–66.
75. Sanz M, Lorenzo R, Aranda JJ, Martin C, Orsini M. Clinical evaluation of a new collagen matrix (Mucograft® prototype) to enhance the width of keratinized tissue in patients with fixed prosthetic restorations: a randomized prospective clinical trial. J Clin Periodontol. 2009;36(10):868–76.
76. Lorenzo R, García V, Orsini M, Martin C, Sanz M. Clinical efficacy of a xenogeneic collagen matrix in augmenting keratinized mucosa around implants: a randomized controlled prospec-tive clinical trial. Clin Oral Implants Res. 2012;23(3):316–24.
77. Esposito M, Maghaireh H, Grusovin MG, Ziounas I, Worthington HV. Soft tissue management for dental implants: what are the most effective techniques? A Cochrane systematic review. Eur J Oral Implantol. 2012;5(3):221–38.
78. Thoma DS, Naenni N, Figuero E, Hämmerle CH, Schwarz F, Jung RE, et al. Effects of soft tissue augmentation procedures on peri-implant health or disease: A systematic review and meta-analysis. Clin Oral Implants Res. 2018;29:32–49.
References

59© Springer International Publishing AG, part of Springer Nature 2018A. Kelekis-Cholakis et al., Peri-Implant Complications, https://doi.org/10.1007/978-3-319-63719-8_3
3Peri-implant Mucositis
3.1 Introduction
The definition of peri-implant mucositis has been revised over the years. It was originally described as “a reversible inflammatory change of the peri-implant soft tissue without bone loss” [1] and eventually was included in a collective term of “peri-implant diseases,” which were deemed to be infectious in nature [2]. According to the Glossary of Terms of the American Academy of Periodontology [3], peri- implant mucositis is “a disease in which the presence of inflammation is confined to the mucosa surrounding a dental implant with no signs of loss of supporting bone.”
3.2 Etiology
The primary etiology of peri-implant mucositis is microbial biofilm accumulation on the implant fixture [4, 5]. Shortly after placement, bacterial plaque colonizes dental implant surfaces [6, 7]. This biofilm is similar to the one identified around the natural dentition, and the inflammatory process seems to mimic that of gingivitis around natural teeth [8]. In an animal study Ericsson et al. [9] demonstrated that prolonged plaque accumulation on implant abutments resulted in inflammation of the peri-implant mucosa due to the establishment of an inflammatory cell infiltrate. This finding was supported by further human studies where it was demonstrated that the accumulation of plaque initiates peri-implant inflammation [8, 10, 11].
3.2.1 Risk Indicators
There are several risk indicators that may contribute to the development of peri- implant inflammation. To date there is some evidence to support the following as risk indicators for the development of peri-implant mucositis: poor oral hygiene, smoking, radiation therapy, and residual cement [12].
60
3.2.1.1 Poor Oral HygieneA clinical study performed by Pontoriero et al. [13] proved that there was a cause and effect relationship between the absence of oral hygiene and plaque accumulation and the development of peri-implant mucositis. Furthermore experimental peri- implant mucosi-tis was reversed when oral hygiene measures were instituted [14]. A recent cross-sec-tional study supported the importance of good oral hygiene by multilevel analysis which determined that a high plaque score was a risk indicator for peri-implant mucositis [15].
3.2.1.2 Smoking and Radiation TherapyKarbach et al. [16] examined 100 patients with a 1–19-year follow-up and showed that smoking was a significant risk indicator for the development of peri-implant mucositis. Similarly Roos Janseker et al. [17] and Rinke et al. [18] determined that smoking was a possible indicator for peri-implant mucositis.
In the same study that assessed smoking as a risk indicator for peri-implant mucositis, Karbach et al. [18] indicated that radiation therapy was also an “explana-tory variable” for the presence of peri-implant inflammation.
3.2.1.3 Residual Cement and Poor Restoration DesignThere is increasing evidence that the presence of residual cement in the subgingival tissues contributes to peri-implant tissue inflammation [19]. In a prospective study evaluating the influence of the restorative margin position and the amount of unde-tected cement, Linkevicius et al. concluded that the more apical the restorative margin, the greater the probability of undetected cement being present. The greatest amount of cement was detected when the restorative margin was placed 2–3 mm subgingivally. Furthermore if an undercut >2 mm is present on the implant restoration, the chance of residual cement increases significantly even if the restorative margin is shallow [20].
A current literature review investigated the role of cement as a risk indicator in peri-implant diseases. It concluded that there is an association with a tendency to higher disease prevalence with cemented, compared to screw-retained, implant res-torations [21]. The authors advocated the collection of baseline data 2 weeks follow-ing the placement of the implant prosthesis with regular follow-up intervals for early detection of peri-implant mucositis and cement excess. A retrospective case analysis compared screw-retained restorations to cement-retained restorations in patients with and without a history of chronic periodontitis. This study demonstrated, that patients with a history of chronic periodontitis and residual cement tended to develop peri-implant diseases more rapidly (23.4 months compared to 40.8 months). Patients with a history of periodontal disease and screw-retained prostheses had a lower incidence of peri-implant disease. It was therefore recommended to consider screw-retained restorations in patients with a history of periodontal disease [22].
3.2.1.4 Potential Emerging Risk IndicatorsThere is weak evidence for diabetes, abutment surface characteristics, absence of keratinized tissue, genetics, gender, time function, alcohol consumption, and rheu-matoid arthritis as risk indicators for peri-implant mucositis [12, 23]. However, these factors should always be considered when developing a treatment plan for future implant patients, or an individualized maintenance protocol for patient with existing implants.
3 Peri-implant Mucositis

61
3.3 Diagnosis
There is heterogeneity in the diagnostic criteria used in studies to define peri-implant mucositis [24]. In one study, peri-implant mucositis was defined as bleeding on probing around implants with no bone loss [25]. In another study, however, the case definition was identified as plaque, probing depth ≤ 5 mm, and evidence of inflam-mation by modified bleeding index [26]. More recently Felo et al. defined peri-implant mucositis [27] as bleeding on probing, modified gingival index >1.5, modified plaque index >1.5, and probing depth ≤ 3 mm.
Out of all the diagnostic parameters, bleeding upon probing has been consis-tently used in all studies as a tool for the diagnosis of peri-implant mucositis.
3.3.1 Bleeding on Probing
The clinical tool in the diagnosis of peri-implant mucositis is bleeding on gentle probing (<0.25 N) [28]. In an experimental animal study, healthy peri-implant sites showed an absence of bleeding on probing, while peri-implant mucositis sites showed an increase of bleeding on probing [29].
The presence of inflammatory signs such as edema, redness, and hyperplasia as well as bleeding upon probing is pathognomonic of peri-implant mucositis (see Figs. 3.1 and 3.2a–c).
3.3.2 Probing Depths/Radiographic Evaluation
Periodontal probing using a light force (0.2–0.3 N) has been deemed a reliable tool for diagnosing peri-implant diseases [30].
To confirm the diagnosis of peri-implant mucositis, stable probing depths, recorded from the time of prosthetic component connection, are of importance in conjunction with the establishment of baseline radiographs [31].
Fig. 3.1 Localized inflammation of the lingual mucosa of peri-implant tissues
3.3 Diagnosis

62
3.3.3 Prevalence
There are significant limitations in the present literature as to the prevalence of peri- implant diseases. Those relate more to issues of study design such as small sample sizes, randomization bias, cross-sectional nature, and short follow-up. Moreover, the variations applied to thresholds for bone loss also affect the disease classifica-tion and perceived prevalence. In a recent systematic review, the subject level preva-lence of peri-implant mucositis was reported to range from 19 to 65% [32]. Further meta-analyses estimated the weighted mean prevalence of peri-implant mucositis to be 43% (CI: 32–54%) [33].
3.4 Management/Treatment Options
Removal of plaque from the abutment/implant surface is the main goal of treatment of peri-implant mucositis. This goal can be achieved with patient education, oral hygiene instruction, professional debridement, and ensuring that there is adequate access to the area in question.
There is currently evidence in the literature to support that peri-implant mucosi-tis is reversible, similarly to gingivitis, when treated effectively with recommended therapeutic modalities [13, 14]. One study however did report that full resolution of experimentally induced peri-implant mucositis in humans was not fully reversed at 3 weeks when oral hygiene measures were reinstituted [14]. Another more recent
a b
c
Fig. 3.2 (a) Visual signs of redness of marginal peri-implant tissues; (b) clinical probing depth less than 4 mm; (c) bleeding upon probing
3 Peri-implant Mucositis

63
study countered these results by observing that in an elderly population, reinstituted oral hygiene measures resulted in complete resolution of peri-implant mucositis [34]. It is important to note, however, that a return to baseline of inflammatory cre-vicular fluid biomarkers was noted in both studies (Figs. 3.3 and 3.4).
a b
c
Fig. 3.3 (a–c) 3–5 mm clinical probing depths with bleeding on probing
a b c
Fig. 3.4 (a) Baseline radiograph, (b) radiograph 1-year post-implant loading, (c) radiograph 6 years later exhibiting no evidence of bone loss beyond physiologic remodeling
3.4 Management/Treatment Options

64
Treatment of peri-implant mucositis is essential, as there appears to be evi-dence that the lack of periodic supportive peri-implant maintenance may result, for some patients, in the development of peri-implantitis. After 5 years of regular peri-implant maintenance, 18% of patients developed peri-implant disease as opposed to those with no maintenance where 43.9% developed peri- implantitis [35].
The primary goal of treatment of peri-implant mucositis is to prevent plaque accumulation. This is achieved by eliminating biofilms at the mucosal abutment interface and around implant-supported restorations. Challenges in achieving this goal for both the patient and the treating clinician are the design and surface tex-ture of the implant abutment, the design of the prosthesis or superstructure, and the patient’s ability and compliance to perform adequate oral hygiene.
Upon initial diagnosis of peri-implant mucositis, the clinician will use a two- pronged approach for treatment (Table 3.1).
The first approach aims at controlling or modifying local or systemic etiological factors such as smoking cessation counseling, prosthesis design modification, patient education, and oral hygiene instruction.
The second approach aims at maintaining peri-implant tissue health such as the establishment of a professional, patient-centered peri-implant debridement proto-col, and a maintenance plan.
3.4.1 Patient Education
Prior to initiation of implant treatment, it is crucial to educate each patient on the importance of adequate plaque control and the need for appropriate maintenance of the implant prosthesis. This is of particular necessity in patients with a past history of chronic or aggressive periodontitis and associated tooth loss as a result of these diseases.
3.4.2 Systemic and Local Factors
3.4.2.1 Systemic Factors
SmokingA discussion with the patient about the impact of smoking on peri-implant tissue health is very important. In a recent microbiological study, smoking seemed to
Table 3.1 Peri-implant mucositis management
Patient education
Systemic factors Local factorsPeri-implant debridement Maintenance
Smoking Prosthesis design (poor access for oral hygiene)
Patient administered Individualized protocol
Inability to perform oral hygiene
Cement Professionally administered
3 Peri-implant Mucositis

65
affect the peri-implant microbiome, creating a high-risk bacterial community for peri-implant disease [36]. Smoking has now been identified in the literature as an independent risk indicator for peri-implant mucositis [37].
Systemic Factors Influencing the Ability to Perform Adequate Oral HygieneInability to perform oral hygiene can be due to systemic factors, such as the devel-opment of conditions that affect the cognitive or physical abilities of an individual to perform adequate oral hygiene. Conditions such as Alzheimer’s, senile demen-tia, or Parkinson’s may place the onus of oral hygiene delivery on loved ones or healthcare staff. A thorough individualized assessment is paramount. Possible con-version of a fixed restoration to a removable prosthesis may be needed, in patient with full-arch implant supported restorations to assist in daily homecare maintenance.
3.4.2.2 Local Factors
Prosthesis ModificationAn assessment will be made of the area to be treated, and an evaluation of the prosthesis will be performed, to ensure adequate access for plaque control. Adjusting restorations to allow for appropriate access to the peri-implant tissues as well as patient education is of paramount importance in the long-term mainte-nance of dental implants (Figs. 3.5 and 3.6).
Ridge lap restorations, closed embrasure spaces, and flanges on fixed implant- supported prostheses are all examples of prosthetic barriers to adequate oral hygiene. A study demonstrated that 48% of implants that presented with peri-implantitis had no accessibility/capability for proper oral hygiene. Furthermore, the authors stated that inadequate plaque control was found in around 74% of implants studied [38].
It is important to note, however, that it may not be advisable to simply adjust the prosthesis or superstructure but it may be necessary to fabricate a new prosthesis altogether after obtaining adequate tissue health (Figs. 3.7 and 3.8). Such may be the case of pink porcelain restorations with buccal flanges (Fig. 3.9).
CementThe diagnosis of residual cement as a contributing factor to peri-implant mucositis is not easy to establish, as a certain percentage of peri-implant mucositis cases do not respond to conventional treatment [25]. In addition many times cement is not radiographically detectable and has been found around implant restorations and peri-implant tissues despite concentrated attempts at removal [20] (Figs. 3.10 and 3.11).
Removal of cement remnants should be attempted initially nonsurgically, with careful monitoring of soft and hard tissues, for resolution of the peri-implant inflam-mation. If persistence of the inflammation is noted and/or signs of peri-implant bone loss develop, removal of the superstructure or elevation of the peri-implant tissues to gain better access is recommended.
3.4 Management/Treatment Options

66
a b
c d
Fig. 3.5 (a) Closed embrasure space. (b) Radiographic evidence of poorly seated restorations and presence of cement. (c) Radiographic evidence of stable bone levels over a 5-year period. (d) Opening of embrasure space
3 Peri-implant Mucositis

67
a b
c d
Fig. 3.6 (a) Over-contoured buccal restoration due to nonideal (palatal and coronal) implant placement. (b) Recontouring of restoration and placement of a soft tissue graft. (c) Suturing of soft tissue graft in place. (d) 5-year follow-up of healthy peri-implant tissues
Fig. 3.7 Before and after prosthesis flange adjustment to facilitate oral hygiene measures. Disclosing paste on the intaglio aspect of the prosthesis assists in ensuring appropriate contours for the performance of adequate oral hygiene (Courtesy of Dr. J. Viquez)
3.4 Management/Treatment Options

68
Fig. 3.9 Pink porcelain ridge lap flanges making plaque removal very difficult for the patient and healthcare provider
Fig. 3.10 Presence of cement not detectable on radiograph
Fig. 3.8 Prosthesis adjustment, oral hygiene instructions, and patient compliance result in a sig-nificant decrease in peri-implant inflammation (Courtesy of Dr. J. Viquez)
3 Peri-implant Mucositis

69
3.4.3 Patient-Administered Plaque Control
3.4.3.1 Oral Hygiene InstructionsOral hygiene instructions given to patients with dental implants are modeled after those given to patients with periodontal diseases. An individualized protocol should be established, and the clinician should evaluate the patient’s ability to perform adequate plaque control. A plaque index is recommended as a guide on proper oral hygiene maintenance [39] (Renvert S and Giovannoli JL 2012 textbook).
One challenge when faced with reviewing current literature on patient- administered plaque control is that there are, frequently, no definitions provided of peri-implant mucositis at baseline and often resolution outcomes are not reported [40]. Thus, the delivery of oral hygiene instructions is often performed on an empir-ical basis.
3.4.4 Mechanical Plaque Control
3.4.4.1 Electric vs. Manual ToothbrushesBoth manual and electric toothbrushes can be used in a self-administered oral hygiene program. Four comparative studies were conducted on the outcomes of patient-administered plaque control with manual or powered toothbrushes. No dif-ference between powered versus manual toothbrushes was evident [40].
Fig. 3.11 Persistent inflammation and purulence that went untreated resulted in the loss of this implant fixture due to the presence of cement on the implant threads
3.4 Management/Treatment Options

70
In a Cochrane systematic review, there appeared to be superior patient preference and ease of maintenance with electric toothbrushes; however the correlation was weak [41].
3.4.4.2 Flossing vs. Interdental BrushesThe use of toothbrushing alone has been shown to be ineffective at removing all inter-proximal plaque around teeth [42]. Various tools have been used in the performance of interdental cleaning such as dental floss, interdental brushes, and toothpicks.
A recent randomized clinical trial compared the efficacy of dental floss to inter-dental brushes in controlling bleeding on probing and reducing implant plaque scores [43]. No significant differences in plaque or bleeding indices were noted in the 6-month follow-up (Fig. 3.12).
When a qualitative pain questionnaire, was given to the same cohort, patients expressed a slight preference in terms of the ease of use of interdental brushes (Fig. 3.13).
Recently there has been a case report on the presence of floss remnants subgin-givally around dental implants with exposed rough surfaces [44]. Another case series pointed to a potential allergic response of certain individuals to coated or flavored dental floss [45]. Consequently in this instance as well, clinicians should
BO
P_a
vera
ge L
S-M
ean
0.6
0.4
0.2
0 months 3 months
TIME
Group 0 1
LS-Means for Group*TIMEwith 95% confidence Limits
Fig. 3.12 Comparison of mean peri-implant bleeding on probing in patients using floss (blue) vs. interdental brushes (red) at 6 months showed no statistical differences
3 Peri-implant Mucositis

71
Fig. 3.13 In a recent clinical trial, patients found interdental brushes easier to use than dental floss
take into account individual patient needs and circumstances when recommending oral hygiene aids.
3.4.5 Chemical Plaque Control
3.4.5.1 ToothpastesTwo studies have compared the efficacy of a triclosan-containing toothpaste to a sodium fluoride toothpaste when using a manual toothbrush [46, 47]. Both studies reported greater reduction of the triclosan group on bleeding on probing at 6 months, when compared to the sodium fluoride group. This finding can be explained by tak-ing into account the anti-inflammatory effect of triclosan as reported in Trombelli and Farina [48]. However, these results should be interpreted with caution, as nei-ther study reported on the number of patients with resolution of peri- implant muco-sitis [40].
3.4.5.2 GelIn a double-blind randomized clinical trial, the use of a 0.5% chlorhexidine gel in conjunction with manual toothbrushing was compared to the use of a placebo gel. All patients received professionally administered mechanical debridement. Both groups experienced a reduction in the mean number of probing depths and bleed-ing on probing, but there were no statistically significant differences between groups [25].
3.4.5.3 MouthwashesThe use of various antiseptic mouthwashes has been proposed as an adjunct to patient-administered mechanical therapy. Essential oil and chlorhexidine mouth-washes have been used in clinical trials.
3.4 Management/Treatment Options

72
Different methods of delivery have been investigated, namely, rinsing and self-irrigation.
RinsingCiancio et al. [49] demonstrated a beneficial effect of rinsing with an essential oil mouthwash (Listerine®) in patients that had not received mechanical professional therapy. A reduction in plaque and gingival inflammation was observed in the con-trol group when compared to the placebo group. In another study comparing rinsing with 0.2% chlorhexidine to self-administration of 1% chlorhexidine gel, De Siena et al. [50] reported a reduction in bleeding scores at the 3-month examination period when compared to baseline. Both methods were equivalent in their effect, but due to the lack of a control group, the efficacy of the chlorhexidine products alone could not be evaluated.
Self-IrrigationIn a study comparing self-irrigation of 0.06% chlorhexidine to rinsing with a 0.12% chlorhexidine solution, self-irrigation was shown to be more effective in reducing peri-implant mucositis than rinsing alone. There was less staining and calculus for-mation in the self-irrigation group [27].
3.4.6 Professional Debridement
Even though professional debridement is paramount to successful peri-implant therapy, it is insufficient by itself in the long term. Adequate patient- administered plaque control is also crucial, in maintaining peri-implant health [51].
3.4.6.1 Curettes, Ultrasonic, and Sonic InstrumentationA recent randomized controlled clinical trial compared the outcomes of hand instru-mentation with unfilled resin-tipped curettes (Hu–Friedy Implacare II) to a piezo ultrasonic scaler (Tigon W&H), in a group of peri-implant maintenance patients. After 1 year of follow-up, no differences in bleeding indices, plaque, or probing depths were noted. Cytokine testing did not reveal any differences between the treatment modalities, neither did patient preference [52]. In a multicenter study comparing the effect of sonic scalers with plastic tips, rubber cup with polishing paste, titanium curettes, and airflow with glycine powder, all treatment modalities were effective in reducing peri-implant mucositis, with no statistically significant differences between the two methods [53].
3.4.6.2 Air PolishingGlycine powder seems to be the instrument of choice in air polishing devices, as it appears to be less abrasive to titanium surfaces than sodium bicarbonate [54]. Two randomized controlled clinical trials have failed to show a greater decrease in bleed-ing on probing or a resolution of peri-implant mucositis with the use of an air pol-ishing device as compared to mechanical debridement [55, 56]. A recent systematic
3 Peri-implant Mucositis

73
review and meta-analysis concluded that “glycine air powder polishing is as effec-tive as the control treatments at mucositis sites” [57].
3.4.6.3 Adjunctive Local AntibacterialsProfessionally administered 0.12% chlorhexidine irrigation and chlorhexidine gel application did not show any superior benefits to mechanical debridement alone [26]. These results were supported by a more recent clinical trial that compared 0.12% sub-gingival chlorhexidine irrigation, home rinsing, and mechanical therapy, to mechanical therapy with placebo solutions. While both treatment modalities were effective in reducing inflammation and peri-implant mucositis, the authors noted that complete resolution of inflammation was not achieved in all sites with either modality [58].
The use of a full mouth decontamination protocol used to treat peri-implant mucositis patients was investigated by Thone-Muhling et al. [59] The bacterial reduction after full mouth decontamination was noted to be temporary with a ten-dency towards recolonization.
In a double-blind randomized clinical trial, patients were instructed to brush daily with a manual toothbrush with either 0.5% chlorhexidine or placebo gel. While, in both groups, there were statistically significant reductions in the mean number of sites with bleeding on probing and a decrease in the mean probing depths between 1 and 3 months, no differences were noted between test and control groups [25].
3.4.6.4 Adjunctive Local and Systemic AntibioticsA study by Renvert et al. [60] compared minocycline to chlorhexidine gel application following mechanical debridement. At the 1-year follow-up, no differences were observed between the two groups in terms of clinical probing depths and plaque levels (Fig. 3.14). A similar outcome was noted when tetracycline fibers were used in the treatment of peri-implant mucositis and hyperplasia. This was also true when sys-temic antibiotics were studied. Another clinical trial compared the use of systemic azithromycin and mechanical debridement vs. debridement alone in the treatment of
Fig. 3.14 Administration of local antibiotic
3.4 Management/Treatment Options

74
peri-implant mucositis. This study did not report any difference on bacterial counts between the two groups [61].
3.5 Summary
The primary approach for treating peri-implant mucositis is patient education and patient-administered plaque control. Appropriate design of implant restorations and the provision of adequate oral hygiene aids as well as demonstration of their use are of paramount importance. The provision of peri-implant professional evaluation and therapy is a cornerstone of implant treatment.
Although clinical improvements of peri-implant mucositis lesions with profes-sional debridement and adequate oral hygiene are well documented, it is important to note that not all lesions are responsive to the above treatments. Consequently, adjunctive methods of therapy such as patient- or professionally administered chemical plaque control may have some additional benefits. It is up to the treating clinician to select and prescribe appropriate treatment combinations based on indi-vidual patient needs.
Fig. 3.15 Healthy peri-implant tissue in an area that is difficult to reach due to patient’s excellent oral hygiene efforts and good professional support
Recommendations for Dental Professionals [37] (Adapted from Jepsen et al.)
• An individual risk assessment should be performed prior to implant ther-apy; factors such as presence of periodontal disease, poor oral hygiene practices, or smoking should be addressed prior to initiation of implant therapy.
• Patients should be informed prior to initiation of treatment of the risks of biological complications and the need for appropriate oral hygiene mea-sures and peri- implant maintenance.
• Professional, individualized, supportive peri-implant maintenance should be established, based on baseline clinical and radiographic records (Fig. 3.15).
3 Peri-implant Mucositis

75
References
1. Albrektsson T, Isidor F. Criteria for success and failure of an implant system. Consensus report. In: Proceedings of the 1st European workshop on Periodontology. Chicago, IL: Quintessence; 1994. pp 243–244.
2. Lindhe J, Meyle J. Peri-implant diseases: consensus report of the sixth European Workshop on Periodontology. J Clin Periodontol. 2008;35(8):282–5.
3. The American Academy of Periodontology. Glossary of periodontal terms. Illinois, CA: American Academy of Periodontology; 2001.
4. Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesions different from periodonti-tis lesions? J Clin Periodontol. 2011;38(s11):188–202.
5. Tonetti MS, Chapple IL, Jepsen S, Sanz M. Primary and secondary prevention of periodontal and peri-implant diseases. J Clin Periodontol. 2015;42(S16):S1–4.
6. van Winkelhoff AJ, Goené RJ, Benschop C, Folmer T. Early colonization of dental implants by putative periodontal pathogens in partially edentulous patients. Clin Oral Implants Res. 2000;11(6):511–20.
7. Fürst MM, Salvi GE, Lang NP, Persson GR. Bacterial colonization immediately after installa-tion on oral titanium implants. Clin Oral Implants Res. 2007;18(4):501–8.
8. Leonhardt Å, Berglundh T, Ericsson I, Dahlén G. Putative periodontal and teeth in pathogens on titanium implants and teeth in experimental gingivitis and periodontitis in beagle dogs. Clin Oral Implants Res. 1992;3(3):112–9.
9. Ericsson I, Berglundh T, Marinello C, Liljenberg B, Lindhe J. Long-standing plaque and gin-givitis at implants and teeth in the dog. Clin Oral Implants Res. 1992;3(3):99–103.
10. Quirynen M, Vogels R, Peeters W, Steenberghe D, Naert I, Haffajee A. Dynamics of initial subgin-gival colonization of ‘pristine’ peri-implant pockets. Clin Oral Implants res. 2006;17(1):25–37.
11. Zitzmann NU, Berglundh T, Marinello CP, Lindhe J. Experimental peri-implant mucositis in man. J Clin Periodontol. 2001;28(6):517–23.
12. Renvert S, Polyzois I. Risk indicators for peri-implant mucositis: a systematic literature review. J Clin Periodontol. 2015;42(S16):S172–86.
13. Pontoriero R, Tonelli MP, Carnevale G, Mombelli A, Nyman SR, Lang NP. Experimentally induced peri-implant mucositis. A clinical study in humans. Clin Oral Implants Res. 1994;5(4):254–9.
14. Salvi GE, Aglietta M, Eick S, Sculean A, Lang NP, Ramseier CA. Reversibility of experi-mental peri-implant mucositis compared with experimental gingivitis in humans. Clin Oral Implants Res. 2012;23(2):182–90.
15. Konstantinidis IK, Kotsakis GA, Gerdes S, Walter MH. Cross-sectional study on the preva-lence and risk indicators of peri-implant diseases. Eur J Oral Implantol. 2015;8(1):75–88.
16. Karbach J, Callaway A, Kwon YD, d’Hoedt B, Al-Nawas B. Comparison of five parameters as risk factors for peri-mucositis. Int J Oral Maxillofac Implants. 2009;24(3):491–6.
17. Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Nine-to fourteen-year follow-up of implant treatment. Part III: factors associated with peri-implant lesions. J Clin Periodontol. 2006;33(4):296–301.
18. Rinke S, Ohl S, Ziebolz D, Lange K, Eickholz P. Prevalence of periimplant disease in par-tially edentulous patients: a practice-based cross-sectional study. Clin Oral Implants Res. 2011;22(8):826–33.
19. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80(9):1388–92.
20. Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res. 2013;24(1):71–6.
21. Staubli N, Walter C, Schmidt JC, Weiger R, Zitzmann NU. Excess cement and the risk of peri-implant disease—a systematic review. Clin Oral Implants Res. 2017;28(10):1278–90.
22. Linkevicius T, Puisys A, Vindasiute E, Linkeviciene L, Apse P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin Oral Implants Res. 2013;24(11):1179–84.
References

76
23. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84(4):436–43.
24. Figuero E, Graziani F, Sanz I, Herrera D, Sanz M. Management of peri-implant mucositis and peri-implantitis. Periodontol 2000. 2014;66(1):255–73.
25. Heitz-Mayfield LJ, Salvi GE, Botticelli D, Mombelli A, Faddy M, Lang NP. Anti-infective treatment of peri-implant mucositis: a randomised controlled clinical trial. Clin Oral Implants Res. 2011;22(3):237–41.
26. Porras R, Anderson GB, Caffesse R, Narendran S, Trejo PM. Clinical response to 2 different therapeutic regimens to treat peri-implant mucositis. J Periodontol. 2002;73(10):1118–25.
27. Felo A, Shibly O, Ciancio SG, Lauciello FR, Ho A. Effects of subgingival chlorhexidine irriga-tion on peri-implant maintenance. Am J Dent. 1997;10(2):107–10.
28. Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. J Clin Periodontol. 2008;35(s8):286–91.
29. Lang NP, Wetzel AC, Stich H, Caffesse RG. Histologic probe penetration in healthy and inflamed peri-implant tissues. Clin Oral Implants Res. 1994;5(4):191–201.
30. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. 2008;35(s8):292–304.
31. Todescan S, Lavigne S, Kelekis-Cholakis A. Guidance for the maintenance care of dental implants: clinical review. J Can Dent Assoc. 2012;78:c107.
32. Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiol-ogy. J Clin Periodontol. 2015;42(S16):S158–71.
33. Papathanasiou E, Finkelman M, Hanley J, Parashis AO. Prevalence, etiology and treatment of peri-implant mucositis and peri-implantitis: a survey of periodontists in the United States. J Periodontol. 2016;87(5):493–501.
34. Meyer S, Giannopoulou C, Courvoisier D, Schimmel M, Müller F, Mombelli A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin Oral Implants Res. 2017;28(8):1005–12.
35. Costa FO, Takenaka-Martinez S, Cota LO, Ferreira SD, Silva GL, Costa JE. Peri-implant disease in subjects with and without preventive maintenance: a 5-year follow-up. J Clin Periodontol. 2012;39(2):173–81.
36. Tsigarida AA, Dabdoub SM, Nagaraja HN, Kumar PS. The influence of smoking on the peri-implant microbiome. J Dent Res. 2015;94(9):1202–17.
37. Jepsen S, Berglundh T, Genco R, Aass AM, Demirel K, Derks J, Figuero E, Giovannoli JL, Goldstein M, Lambert F, Ortiz-Vigon A. Primary prevention of peri-implantitis: Managing peri-implant mucositis. J Clin Periodontol. 2015;42(S16):S152–7.
38. Serino G, Ström C. Peri-implantitis in partially edentulous patients: association with inad-equate plaque control. Clin Oral Implants Res. 2009;20(2):169–74.
39. Renvert S, Giovannoli J-L. Peri-implantitis. Hanover Park, IL: Quintessence International; 2012.
40. Salvi GE, Ramseier CA. Efficacy of patient-administered mechanical and/or chemical plaque control protocols in the management of peri-implant mucositis. A systematic review. J Clin Periodontol. 2015;42(S16):S187–201.
41. Grusovin MG, Coulthard P, Worthington HV, George P, Esposito M. Interventions for replac-ing missing teeth: maintaining and recovering soft tissue health around dental implants. Cochrane Database Syst Rev. 2010;8:CD003069.
42. Salvi GE, Chiesa AD, Kianpur P, Attström R, Schmidlin K, Zwahlen M, Lang NP. Clinical effects of interdental cleansing on supragingival biofilm formation and development of experi-mental gingivitis. Oral health & preventive dentistry. 2009;7(4):383–91.
43. Nwachukwu OG, Dick M, Atout R, et al. A comparison of the efficacy of two different inter-dental protocols around dental implants in maintenance patients: A randomized controlled trial. (Submitted for publication).
44. van Velzen FJ, Lang NP, Schulten EA, Ten Bruggenkate CM. Dental floss as a possible risk for the development of peri-implant disease: an observational study of 10 cases. Clin Oral Implants Res. 2016;27(5):618–21.
3 Peri-implant Mucositis

77
45. Kelekis-Cholakis A, Perry JB, Pfeffer L, Millete A. Successful treatment of generalized refrac-tory chronic periodontitis through discontinuation of waxed or coated dental floss use: A report of 4 cases. Am Dent Assoc. 2016;147(12):974–8.
46. Ramberg P, Lindhe J, Botticelli D, Botticelli A. The effect of a triclosan dentifrice on mucositis in subjects with dental implants: a six-month clinical study. J Clin Dent. 2009;20(3):103.
47. Prasad KV, Sreenivasan PK, Rajesh G, Ramya K, Rao CB, DeVizio W. The efficacy of den-tifrices on extrinsic tooth stains among com-munity dwelling adults in India—a randomised controlled trial. Community Dent Health. 2011;28:201–5.
48. Trombelli L, Farina R. Efficacy of triclosan-based toothpastes in the prevention and treatment of plaque-induced periodontal and peri-implant diseases. Minerva Stomatol. 2013;62(3):71–88.
49. Ciancio SG, Lauciello F, Shibly O, Vitello M, Mather M. The effect of an antiseptic mouth-rinse on implant maintenance: plaque and peri-implant gingival tissues. J Periodontol. 1995;66(11):962–5.
50. Siena F, Francetti L, Corbella S, Taschieri S, Fabbro M. Topical application of 1% chlorhexi-dine gel versus 0.2% mouthwash in the treatment of peri-implant mucositis. An observational study. Int J Dent Hyg. 2013;11(1):41–7.
51. Tonetti MS, Eickholz P, Loos BG, Papapanou P, Velden U, Armitage G, Bouchard P, Deinzer R, Dietrich T, Hughes F, Kocher T. Principles in prevention of periodontal diseases. J Clin Periodontol. 2015;42(S16):S5–11.
52. Castro M, Dick M, Atout R, et al. A 12-month comparison of piezo ultrasonic scaler and hand instrumentation in the maintenance of peri-implant tissues: A randomized clinical trial. (Submitted for publication).
53. Blasi A, Iorio-Siciliano V, Pacenza C, Pomingi F, Matarasso S, Rasperini G. Biofilm removal from implants supported restoration using different instruments: a 6-month comparative mul-ticenter clinical study. Clin Oral Implants Res. 2014;27(2):e68–73.
54. Schwarz F, Ferrari D, Popovski K, Hartig B, Becker J. Influence of different air-abrasive pow-ders on cell viability at biologically contaminated titanium dental implants surfaces. J Biomed Mater Res B Appl Biomater. 2009;88(1):83–91.
55. Riben-Grundstrom C, Norderyd O, André U, Renvert S. Treatment of peri-implant mucositis using a glycine powder air-polishing or ultrasonic device: a randomized clinical trial. J Clin Periodontol. 2015;42(5):462–9.
56. Ji YJ, Tang ZH, Wang R, Cao J, Cao CF, Jin LJ. Effect of glycine powder air-polishing as an adjunct in the treatment of peri-implant mucositis: a pilot clinical trial. Clin Oral Implants Res. 2014;25(6):683–9.
57. Schwarz F, Becker K, Renvert S. Efficacy of air polishing for the non-surgical treatment of peri-implant diseases: a systematic review. Journal of clinical periodontology. 2015;42(10):951–9.
58. Menezes KM, Fernandes-Costa AN, Neto RD, Calderon PS, Gurgel BC. Efficacy of 0.12% chlorhexidine gluconate for non-surgical treatment of peri-implant mucositis. J Periodontol. 2016;87(11):1305–13.
59. Thöne-Mühling M, Swierkot K, Nonnenmacher C, Mutters R, Flores-de-Jacoby L, Mengel R. Comparison of two full-mouth approaches in the treatment of peri-implant mucositis: a pilot study. Clin Oral Implants Res. 2010;21(5):504–12.
60. Renvert S, Lessem J, Dahlén G, Lindahl C, Svensson M. Topical minocycline microspheres versus topical chlorhexidine gel as an adjunct to mechanical debridement of incipient peri-implant infections: a randomized clinical trial. J Clin Periodontol. 2006;33(5):362–9.
61. Hallström H, Persson GR, Lindgren S, Olofsson M, Renvert S. Systemic antibiotics and debridement of peri-implant mucositis. A randomized clinical trial. J Clin Periodontol. 2012;39(6):574–81.
62. Korsch M, Robra BP, Walther W. Cement-associated signs of inflammation: retrospective anal-ysis of the effect of excess cement on peri-implant tissue. Int J Prosthodont. 2015;28(1):11–8.
References
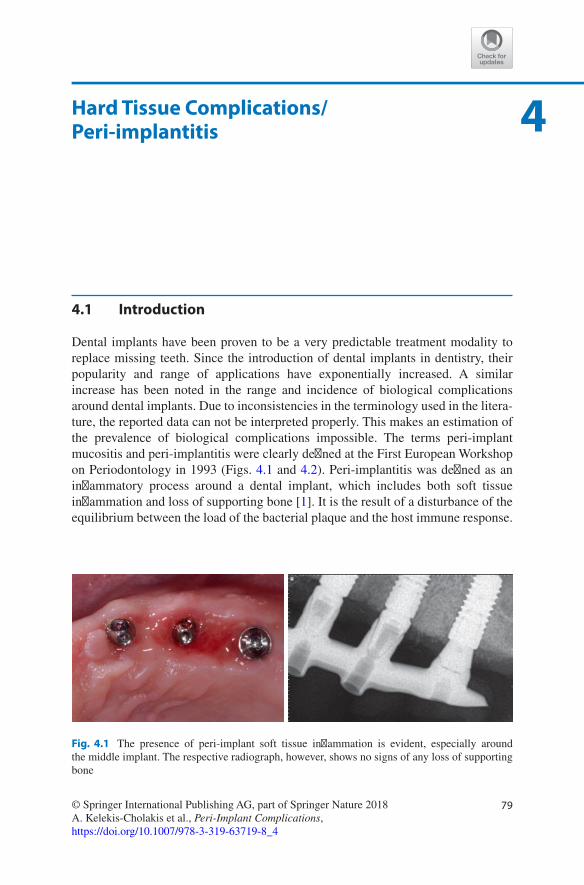
79© Springer International Publishing AG, part of Springer Nature 2018A. Kelekis-Cholakis et al., Peri-Implant Complications, https://doi.org/10.1007/978-3-319-63719-8_4
4Hard Tissue Complications/ Peri- implantitis
4.1 Introduction
Dental implants have been proven to be a very predictable treatment modality to replace missing teeth. Since the introduction of dental implants in dentistry, their popularity and range of applications have exponentially increased. A similar increase has been noted in the range and incidence of biological complications around dental implants. Due to inconsistencies in the terminology used in the litera-ture, the reported data can not be interpreted properly. This makes an estimation of the prevalence of biological complications impossible. The terms peri-implant mucositis and peri-implantitis were clearly defined at the First European Workshop on Periodontology in 1993 (Figs. 4.1 and 4.2). Peri-implantitis was defined as an inflammatory process around a dental implant, which includes both soft tissue inflammation and loss of supporting bone [1]. It is the result of a disturbance of the equilibrium between the load of the bacterial plaque and the host immune response.
Fig. 4.1 The presence of peri-implant soft tissue inflammation is evident, especially around the middle implant. The respective radiograph, however, shows no signs of any loss of supporting bone

80
The clinical signs of peri-implantitis are characterized by soft tissue inflammation, manifesting as redness, swelling and bleeding on probing, which may be accompa-nied by suppuration. However, progressive radiographic bone loss is the main diag-nostic parameter. Peri-implantitis is a very common entity among biologic complications that occur around dental implants.
4.2 Etiology
Bacterial biofilms have been proven to be the primary etiological factor for the ini-tiation of the inflammatory lesion of the periodontal tissues. Several animal studies have demonstrated the mechanisms of the development of the inflammatory lesion around dental implants [2, 3]. Evidence supports that the initiation and progression of peri-implantitis follows the same series of events as periodontal disease.
The response of the peri-implant tissues to the bacterial insult (biofilm forma-tion) follows a similar pattern to the one noted around natural teeth, both in magni-tude and intensity. This will ultimately lead to complete loss of osseointegration and implant failure (Fig. 4.3a, b). A similar response was also noted, to established bio-films in both implants and teeth, with an increase in the inflammatory infiltrate and substantial loss of collagen. The peri-implant lesion was considerably larger and with greater apical extension for peri-implant mucosa than teeth [4].
Multiple other variables can influence the progression of peri-implant disease (Table 4.1). A variable can be characterized as a true risk factor, for the progression of peri-implant disease, once it has been studied in longitudinal studies and its nega-tive impact has been established. Variables with an impact on the progression of peri-implant disease, that have been identified in retrospective and cross-sectional studies, can only be identified as risk indicators.
Fig. 4.2 The deep probing depth, along with the bleeding and suppuration upon probing, rendered the diagnosis of peri-implantitis. Significant bone loss was seen radiographically, and a circumfer-ential, infra-bony defect was identified clinically, upon flap reflection
4 Hard Tissue Complications/Peri-implantitis

81
4.2.1 History of Periodontal Disease
The progression of periodontal disease may ultimately lead to tooth loss, and reha-bilitation of the lost dentition with dental implants (Fig. 4.4). As defined by Heitz-Mayfield and Huynh-Ba [5], implant survival refers to the presence of an integrated implant with or without complications and implant success to the presence of an implant without any complications. A multitude of studies have been conducted to determine the effect of the history of periodontal disease on the survival and suc-cess of dental implants [7–15]. Evidence suggests that patients with a history of periodontal disease are more susceptible to peri-implant bone loss, compared to healthy controls [6].
In a systematic review by Van der Weijden [7], it was concluded that implant survival rates and peri-implant bone loss, of dental implants placed in individuals with a history of treated periodontal disease, might be different from those in peri-odontally healthy individuals, in the long-term. In another meta-analysis [8], it was also concluded that dental implants placed in patients with a history of treated peri-odontitis exhibited a higher incidence of peri-implantitis and marginal peri- implant bone loss.
Fig. 4.3 Significant plaque and calculus deposits are noted around the body of this implant. The implant was entirely encapsulated in soft tissue and was removed as it presented with significant mobility. Established biofilm formations are noted on the rough surface of a failed dental implant
Table 4.1 Etiological factors associated with the prevalence and progression of peri-implantitis
History of periodontal diseaseHistory of smokingPoor oral hygieneDiabetesGenetic factors—IL-1 polymorphismAlcohol consumptionImplant surfaceOcclusal overloadPresence of keratinized tissueIatrogenic factors
Adapted from Heitz-Mayfield LJA. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol 2008; 35 (Suppl. 8): 292–304
4.2 Etiology

82
Karoussis et al. [9] evaluated the short- (<5 years) and long-term (>5 years) survival and success rates of dental implants placed in patients with a history of periodontitis. This review demonstrated that implants placed in patients with pre-viously treated periodontal disease have similar survival rates with implants placed in periodontally healthy patients. However, individuals with a history of periodontal disease experienced a significantly higher incidence of peri-implanti-tis, deeper probing depths, and increased peri-implant bone loss. Late implant loss and peri-implant bone loss was also demonstrated in another systematic review by Quirynen et al. [10]. This was true, especially for implants with a very rough sur-face, and for patients that were not on a regular maintenance schedule. The rate of late implant loss was three times higher for subjects that did not receive regular maintenance therapy.
Klokkevold and Han [11] concluded that there is no significant difference on survival rates of implants placed in patients with a history of treated periodontitis
Fig. 4.4 A patient with a failing dentition, as a result of chronic periodontitis, received full mouth reconstruction with implant-supported prostheses. Compliance with a strict maintenance schedule was established prior to implant treatment. Peri-implant tissues appear healthy, and radiographic bone levels appear stable, 1 year following treatment
4 Hard Tissue Complications/Peri-implantitis

83
(95%) compared to patients with no previous history of periodontal disease (97.1%). However, this study indicated that patients with a history of treated periodontal disease experienced significantly lower implant success rates (11.05% better for periodontally healthy patients), as defined by adverse outcomes of peri-implant tissues.
More recently two systematic reviews assessed the survival and success of implants placed in patients with a history of periodontal disease. Zangrando et al. [12] analyzed, the long-term (>5 years) survival and success rates of dental implants placed in patients with a history of periodontal disease. The authors concluded that dental implant therapy can be successful in patients with a history of periodontal disease, as long as the periodontal disease had been properly treated, and the patients were enrolled in a regular maintenance program. The study demonstrated an implant survival rate of 92.1% after 10 years of follow-up. However, increased prevalence of bleeding on probing and residual pocket depths were directly associated with occurrence of peri-implantitis. Furthermore, non- compliance with periodontal maintenance and tobacco smoking had a negative influence on implant outcomes. Another systematic review, reported that implants placed in patients with a history of treated periodontitis had a higher incidence of biological complications and implant loss [13]. Moreover, smoking and lack of periodontal maintenance nega-tively affected the success of dental implants. Evidence from this review suggested that patients with sites of persistent periodontitis were four times more likely to develop biological complications compared to successfully treated individuals. Moreover, when aggressive periodontitis subjects are treated with implants, a trend for lower implant survival and success rates was noted, when compared to chronic periodontitis individuals or healthy individuals.
A recent study systematically assessed the literature to identify the effect of a history of aggressive periodontitis on implant therapy [14]. The results of this review indicated that the effect of aggressive periodontitis depends on the “end outcome” reported. No significant difference was found when “implant survival” was used as the end outcome, for patients with aggressive periodontitis com-pared to healthy or chronic periodontitis patients. However, when “implant fail-ure” was considered as the end outcome, a risk ratio for implant loss of 4.00 and 3.97 was identified, when comparing the aggressive periodontitis group with the healthy and the chronic periodontitis groups, respectively. The authors con-cluded that due to the small sample of failed implants in aggressive periodontitis patients, these numbers should be interpreted with great caution. This review also demonstrated that implants in patients with a history of aggressive peri-odontitis experienced more marginal bone loss, compared to implants in patients with a history of chronic periodontitis (0.28 mm vs. 0.43 mm). The authors advised caution in the interpretation of this fact, as it might not be clinically significant.
The survival rates of supra-structures and implants are high in individuals with a history of periodontitis-associated tooth loss. However, the higher incidence of peri- implantitis may jeopardize the longevity of the implant treatment. Therefore, implant treatment in periodontitis-susceptible patients is not contraindicated,
4.2 Etiology

84
provided that there is adequate plaque control and that an individualized mainte-nance program is implemented [15].
4.2.2 Smoking
Cigarette smoking should be considered a risk factor for the long-term survival and maintenance of dental implants. In a systematic review and meta-analysis [16], it was shown that smoking may significantly affect the survival of dental implants, with an implant-related and patient-related OR of 2.25 and 2.69, respectively, when smokers were compared to non-smokers. Previously augmented implant sites showed a significantly higher risk for implant failure when smokers (OR 3.61) were compared to non-smokers (OR 2.15). Furthermore, biological complications, such as peri-implant tissue inflammation and marginal peri-implant bone loss, were found to occur with higher frequency in smoking compared to non-smoking individuals.
In contrast, studies reporting on implants with recently introduced micro- roughened surfaces show a significantly lower risk of implant failure in smokers with an OR of 1.49 [17, 18]. Thus, implant surface treatment may play a role in the survival of implant fixtures in smokers. Smoking was found to have a negative influ-ence on the occurrence of biologic complications on machined, Titanium Plasma Sprayed (TPS) and Hydroxy-apatite (HA) coated implants [19]. However, when comparing implants with particle-blasted and acid-etched (SLA), anodized (TiUnite) and dual acid-etched (Osseotite) surfaces no significant influence of smoking on marginal bone loss was noted around those implants [20].
Patients undergoing implant treatment should be thoroughly informed regarding the potentially negative influence of cigarette smoking on dental implants and their overall health. The positive influence of the newer micro-roughened surfaces on implant survival and peri-implant marginal bone levels should be further investi-gated, with more studies, and further reinforced with more adequately powered, long- term evidence in large sample sizes.
4.2.3 Poor Oral Hygiene/Lack of Maintenance
There is substantial evidence that poor oral hygiene is associated with an increase in peri-implant marginal bone loss (Fig. 4.5). In an epidemiologic study of Brazilian subjects, individuals with high plaque scores (>2) were 14.3 times more likely to experience peri-implant marginal bone loss when compared to individuals with low plaque scores [21]. In another prospective study, it was noted that 48% of implants referred for treatment of peri-implantitis, had restorations that did not allow enough access for adequate oral hygiene [22].
Lack of regular peri-implant maintenance care has also been associated with an increased incidence of marginal peri-implant bone loss.
4 Hard Tissue Complications/Peri-implantitis

85
4.2.4 Diabetes, Alcohol Consumption, and Genetic Factors IL-1 Polymorphisms
There is limited evidence to suggest that diabetes, alcohol consumption, or gene polymorphisms can negatively affect peri-implant tissue health and lead to
Fig. 4.5 Poor oral hygiene, due to limited access, and complete lack of maintenance, resulted in severe peri-implant inflammation and loss of peri-implant soft and hard tissues. Upon peri-implant therapy, two of the implants were replaced, and the fixed prosthesis was converted to a removable one in order to facilitate maximum access for proper oral hygiene and implant maintenance
4.2 Etiology

86
peri- implant bone loss. Although diabetic subjects may be at increased risk for den-tal implant failure [23], only one study has shown that patients with poor metabolic control may be at increased risk of peri-implantitis [21]. Similarly, there is only one study indicating that individuals consuming >10 g of alcohol daily, may be at increased risk of peri-implant bone loss.
A systematic review by Huyhn-Ba et al. [24] could not reach a conclusion on whether or not IL-1 genotype status is associated with peri-implantitis. The identi-fication of IL-1 gene polymorphisms as risk factors for peri-implant disease cannot be justified at this time.
4.2.5 Dental Implant Surface
The dental implant surface quality may determine the tissue reactions to the implant fixture [25]. Dental implant surface characteristics, such as roughness and chemical treatment, have been shown to play a role in the progression of peri-implant bone loss. The initial Branemark implant carried a machined surface with a roughness (Sa) of 0.5–1.0 μm, and is the most widely researched implant. Rough-surface implants (Sa >2.0 μm TPS and HA coated) were shown to have a favorable bone response which led to faster osseointegration. However, rough-surface implants demonstrated a higher incidence of peri-implantitis and a more rapid progression of marginal bone loss. On the other hand, moderately rough-surface implants (Sa 1.0–2.0 μm most of the implants used today, TiO Blast, SLA, TiUnite, Frialit-2) have shown no increase in the incidence of peri-implantitis and maintenance of the mar-ginal bone levels for a follow-up of 5 years [26]. Nevertheless, in an animal study by Berglundh et al. [27], it was shown that the progression of peri-implantitis, in moderately rough- surface implants (SLA surface), was more pronounced than in smooth-surface implants, if left untreated. In another comparative animal study, it was shown that progression of experimentally induced peri-implantitis occurred in implants with different geometry and surface treatment [28]. Peri-implant marginal bone loss was more pronounced on implants with an anodized surface (TiUnite). In a randomized controlled clinical trial by Wenstromm et al. [29], patients were treated with implant-supported fixed partial dentures and followed up for a period of 5 years. This study demonstrated that implants with a moderately rough surface (TiO Blast Sa 1,5 μ) had similar marginal bone levels with machined surface implants after 5 years in function. In the same study, moderately rough-surface implants demonstrated a similar response to peri-implant bone loss, when compared to implants with a machined surface.
4.2.6 Occlusal Overload
The effect of occlusal overload on peri-implant bone loss is reported in the literature with great controversy. Early reports on animal models, by Isidor [30, 31], showed that loss of osseointegration and implant mobility could be observed 4.5–15.5 months
4 Hard Tissue Complications/Peri-implantitis

87
following implant placement, when excessive load was applied (Fig. 4.6). Implants in the control group, which were allowed to accumulate plaque, showed a mean marginal bone loss of 1.8 mm. However, the models of occlusal overload applied in these studies do not reflect real clinical scenarios.
More recent histological observations though, demonstrated that occlusal over-load does not affect the peri-implant bone levels or bone to implant contact of
Fig. 4.6 This implant lost bone integration completely, 3 months following the installation of the final restoration. The implant was placed in a grafted site (ridge preservation, first radiograph, top left), 5 months following graft placement. Four months following implant placement (second radiograph, top right), the implant appeared stable at a torque of 35 N/cm, and the bone levels appeared normal at the stage 2 appointment. Three months following the placement of the restora-tion, the implant became mobile and was removed. A radiograph at his time showed significant bone loss and a peripheral radiolucency
4.2 Etiology

88
osseointegrated dental implants, in the absence of peri-implant inflammation [32]. In this study the occlusal overload model applied was more relevant to clinical prac-tice, utilizing implant-supported crowns in supraocclusion in order to create over-load of the dental implants (Table 4.2). However, occlusal overload can be detrimental on the peri-implant marginal bone levels, when applied to dental implants surrounded by inflamed peri- implant tissues. In another dog study, utiliz-ing the same model of occlusal overload, it was demonstrated that overloading may aggravate the peri-implant bone resorption, only in the presence of peri-implant inflammation [33]. Peri-implant bone loss is noted when a load in excess of 3000 micro strain is applied. According to the third EAO concensus conference, none of the studies conducted to evaluate the effect of overload on peri-implant bone, have measured the amount of micro strain on the bone-implant interface [34].
4.2.7 Lack of Keratinized Tissue
The amount of keratinized mucosa (KM) around dental implants has been discussed in the literature with great controversy. Evidence suggests that KM may not be nec-essary to maintain peri-implant health [35] and may not be associated with peri-implant bone loss [36]. However, despite its presence, peri-implantitis may still occur [37]. Earlier studies had failed to show any correlation between keratinized and attached mucosal width, and increased implant success [35]. Soft tissue grafting increased the width of keratinized tissue: however, no improvement in implant suc-cess rates was noted [38].
Recent studies suggest otherwise (Fig. 4.7). Wider KM will better preserve hard and soft tissue [39] and may be more favorable for the long-term maintenance of implants [40]. Furthermore, lack of KM may result in greater soft tissue recession and inadequate plaque control [41]. This resulted in a clinical recommendation of 2 mm of KM around implants [42].
4.2.8 Iatrogenic Factors
Hard tissue changes around dental implants may also be provoked by non-bacterial causes. Traumatic surgical techniques, implant design, implant malposition, loose prosthesis, or abutment are only a few of the parameters that can lead to peri-implant bone loss [43]. The most widely researched iatrogenic factor contributing to
Table 4.2 Effect of occlusal overload on peri-implant parameters
48 implants Probing depths (mm)Bone lossShoulder crest (mm) Bone to implant contact (%)
Not loaded 2.5 ± 0.3 3.6 ± 0.4 73Overloaded 2.6 ± 0.3 3.7 ± 0.2 75
Adapted from Heitz-Mayfield LJ, Schmid B, Weigel C, Gerber S, Bosshardt DD, Jönsson J, Lang NP, Jönsson J. Clin Oral Implants Res. 2004 Jun;15 [3]:259–68.
4 Hard Tissue Complications/Peri-implantitis

89
peri- implant bone loss is the residual cement that remains in the peri-implant tissue, following delivery of the final restoration (Fig. 4.8). The positive relationship between residual cement and peri-implant disease was demonstrated in a prospec-tive study with the use of an endoscope [44]. This study showed that 81% of cases with peri-implant disease were associated with residual cement, as detected with the use of an endoscope. Furthermore, 74% of these cases showed no signs of
Fig. 4.7 Deep peri-implant probing depth was noted on the buccal aspect of this implant, along with a lack of keratinized tissue. Upon flap reflection, significant bone loss was noted. Open flap debridement with implantoplasty and guided bone regeneration of the infra-bony components of the defect was done. Following adequate healing time, soft tissue augmentation was performed, to increase the quantity (volume) and improve the quality (keratinized mucosa) of the peri-implant tissue
4.2 Etiology

90
peri- implant disease 30 days following the removal of the cement remnants. The high prevalence of residual cement in cases of peri-implantitis may be explained by the fact that most of the commercially available cements are non-detectable by radiographic means [45]. Another study confirmed the capacity of residual cement to elicit peri-implant inflammation, leading to peri-implant bone loss [46]. This inflammatory response can be exaggerated in patients with a previous history of periodontal disease. Furthermore, the amount of residual cement is directly
Fig. 4.8 Significant plaque accumulation was noted around these two implants in the posterior mandible, upon prosthesis removal. The implants were placed at a supra-crestal position leaving the rough surface exposed. This along with an unhygienic prosthesis design provoked significant plaque accumulation and hindered optimal oral hygiene. Upon flap reflection significant bone loss was noted around both implants. The implants were removed along with the adjacent first premo-lar, which was deemed hopeless. Excess cement was noted along the open margin of the tooth supported crown as well as on the rough surface of the dental implants
4 Hard Tissue Complications/Peri-implantitis

91
proportional to the depth of the margin of the restoration [47]. Thus, restorations with subgingival margins are more likely to retain cement material following the final delivery of the restoration. Different methods of crown cementation have been proposed in order to reduce the prevalence of residual cement during delivery of the final restoration. Alternatively, screw-retained restorations may be selected.
4.3 Diagnosis
Peri-implantitis is defined as an inflammatory process around a dental implant, which includes both soft tissue inflammation and loss of supporting bone [48, 49]. Due to the similarities, in the pathogenesis, of periodontitis with peri-implantitis, similar criteria have to be used in order to diagnose peri-implantitis [50].
4.3.1 Bleeding on Probing
The absence of bleeding on probing (BOP) is considered an excellent predictor of health and periodontal stability [51]. The presence of BOP has shown limited posi-tive predictive value, and it is considered a weak marker for future periodontal dis-ease progression. BOP around dental implants (Fig. 4.9), however, has shown a significantly higher positive predictive value compared to teeth. In a study by Luterbacher et al. [52], it was demonstrated that implants with a positive BOP in ≥50% of the recall appointments showed 100% chance for disease progression. Disease progression was defined as a 2.5 mm of attachment loss or −3.7 in Computer Assisted Densitometric Image Analysis (CADIA) values, over a period of 5 years. These values were further reinforced when paired with microbiological tests that showed the presence of certain pathogenic bacteria [52]. Hence, the presence of BOP around dental implants may be a valuable diagnostic parameter to monitor the stability of peri-implant tissue health.
Fig. 4.9 Deep clinical probing depths were noted around this implant. Shortly after the probe was removed, bleeding was noted across the mucosal margin around the implant-supported restoration
4.3 Diagnosis

92
4.3.2 Probing Depths and Radiographic Evaluation
Clinical assessment of peri-implant tissue health is imperative in order to establish the long-term success of implant treatment. Probing of the peri-implant tissue (25 N probing force) is a safe diagnostic means to identify any deviation from peri- implant tissue health. Any disruption of the soft tissue attachment with the implant surface, by a periodontal probe, will be restored fully by 5 days [53]. Lang et al. [54] have demonstrated that the peri-implant mucosa has the capacity to provide the underly-ing bone with an excellent seal in the presence of peri-implant mucosal health and peri-implant mucositis. In the presence of peri-implantitis, however, the probe tip will penetrate further to the underlying bone. Hence, probing around dental implants is a valuable tool to monitor peri-implant tissue health and diagnose peri-implant diseases.
Multiple studies have suggested a specific probing depth threshold that can be associated with peri-implant tissue health. However, it is important to note that a sub-crestal position of the implant may often be necessary in order to achieve an optimal outcome, especially in the esthetic zone. This will ultimately result in deeper probing depths, which alone are not considered a sign of peri-implant dis-ease. Thus, it is important to establish a health-related baseline at the time of the connection of the prosthetic components. Comparison of future measurements to baseline is essential to identify the presence of health or pathology [43].
Establishing a baseline is also critical for the radiographic records in order to detect any future bone loss around the implant fixture. Baseline radiographs should be taken at implant placement and after the connection of the restorative component [43], as bone loss prior to this time point may be due to iatrogenic factors or normal bone turnover during the healing phase. Every effort should be made to standardize these radiographs by taking them perpendicular to the implant body, with a clear demarcation of the restorative platform and the implant threads. The implant threads will serve as points of reference to diagnose peri-implant bone loss in future radiographs.
Anytime there is bleeding on probing with increasing probing depths; a new radiograph is recommended, in order to confirm the progression of further bone loss, if any, in comparison to baseline measurements (Figs. 4.10 and 4.11).
4.3.3 Suppuration
Suppuration with or without probing represents a pathognomonic sign of peri- implant disease (Fig. 4.12). The presence of suppuration denotes the presence of active infection and pathological changes. Therefore, further evaluation and treat-ment is indicated.
4 Hard Tissue Complications/Peri-implantitis

93
Fig. 4.10 Deep clinical probing depths with profuse bleeding upon probing were noted around these implants. Significant bone loss is noted on the corresponding radiograph, along with a radiopaque finding at the mesial of implant #13. Upon flap reflection the clinical and radiographic findings were confirmed. Significant bone loss can be seen in the intraoperative picture. Circumferential bone loss is noted around both implants, along with an infra-bony defect around the most distal implant
Fig. 4.11 This patient received two dental implants to replace his central incisors. The implants pre-sented with mobility, severe inflammation of the peri-implant soft tissues, and spontaneous suppuration
4.3 Diagnosis

94
4.3.4 Mobility
The ultimate result of untreated peri-implantitis is the loss of supporting bone around the dental implant fixture. As this infection develops due to plaque accumu-lation around the gingival margin of the implant restoration, bone loss occurs at the coronal aspect and progressively extends apically. Therefore, mobility of the implant denotes complete loss of integration and ultimately implant failure.
4.3.5 Prevalence
It is widely accepted that all of the abovementioned diagnostic parameters are use-ful for the diagnosis of peri-implant diseases. However, there is inconsistent evi-dence when reporting prevalence rates. These differences can be explained by the lack of uniform guidelines in the diagnosis of peri-implantitis and the wide range of threshold values of diagnostic measurements. Furthermore, the level of data report-ing (patient level vs. implant level) contributes to that variation. In an epidemiologic study, Koldsland et al. [55] demonstrated that different diagnostic thresholds would yield different rates of prevalence of peri-implant diseases. The most significant parameter affecting the prevalence of peri-impant disease, is the threshold of pathol-ogy as it relates to probing depths. The most significant change in prevalence occurs when the probing depth threshold increases from ≥4 mm to ≥6 mm.
In a systematic review by Tomasi et al. [56], the authors agreed that the preva-lence of peri-implant diseases depends on the diagnostic threshold and that no set criteria for diagnosis exist. In a meta-analysis of five studies, it was cautiously esti-mated that the prevalence of peri-implant diseases is approximately 10% when reported on the patient level and 20% when reported on the implant level [57]. However, the lack of uniform diagnostic criteria was also pointed out in this meta-analysis.
Fig. 4.12 Progressive bone loss can be seen around these three implants. The bone loss follows a different pattern around each implant, with a non-linear progression in time
2008 2011 2012
4 Hard Tissue Complications/Peri-implantitis

95
In an effort to create consistency in the diagnosis of peri-implantitis, different classification systems have been proposed, [58] classifying peri- implantitis, based on the severity of the defect (See Sect. 1.3).
Unfortunately, to date, no uniform diagnostic criteria are widely accepted for the diagnosis of peri-implantitis. The potential intervention depends on the stability of the case over the long-term based on the clinical and radiographic measurements taken at baseline.
4.3.6 Disease Progression
The progression of peri-implant disease has been extensively researched. Most studies have implemented the model of ligature-induced peri-implantitis [3], in order to induce peri-implant bone loss. The most distinct difference between the periodontal lesion and the peri-implantitis lesion is that the first has a self-limit-ing capacity due to the configuration of the gingival collagen fibers around the teeth, a characteristic that is not found in the latter [59]. Furthermore, following ligature removal, there was spontaneous bone loss around the implant fixtures. Different studies have assessed the progression of bone loss (Fig. 4.12), on dif-ferent implant surfaces during a period of plaque accumulation, following a period of ligature- induced peri-implantitis [27, 60, 61]. In general, all studies are in agreement that peri-implantitis progresses in a faster rate on rough implant surfaces, compared to smooth-surface implants. When different rough surfaces were compared [60], no statistically significant differences were found between the different rough implant surfaces. However, in the analysis there was a consis-tent finding that indicated a more pronounced severity of peri-implantitis on anodized surface implants.
The pattern on peri-implant bone loss was reported in a cohort study of 487 peri- implantitis- affected implants [62]. The peri-implant bone loss showed a nonlinear pattern and the rate of bone loss increased over time. In this study the pattern of peri-implantitis-associated bone loss showed a variation among individuals and a similar pattern of progression within the same subject.
4.4 Management/Treatment Options
As there are many common features on the pathogeneses and the diagnoses of peri-odontal and peri-implant diseases, similar strategies and treatment modalities are applied toward their treatment [63]. The ultimate goal of peri-implantitis treatment is to establish inflammation-free peri-implant soft tissues, eliminate all plaque retentive factors, prevent any further bone loss [64]. Furthermore, treatment aims to allow adequate access for proper oral hygiene for long-term peri-implant tissue health.
4.4 Management/Treatment Options

96
4.4.1 Removal of Etiologic Factors
Once the diagnosis of peri-implantitis has been rendered, a thorough assessment of the peri-implant tissues, as well as the corresponding prostheses, should be per-formed in order to identify all local causative factors. Systemic and environmental factors that may provoke the occurrence and progression of peri-implantitis should, also, be identified. The control and/or elimination of these factors is crucial for the success of the treatment and the maintenance of the desired outcome.
4.4.2 Nonsurgical Treatment of Peri-implantitis
Although nonsurgical debridement has been proven effective for the treatment of peri-implant mucositis, it shows limited efficacy when used alone for the treatment of peri-implantitis. It has been demonstrated that the addition of local antimicrobi-als to mechanical debridement offers marginal improvement of peri-implant tissue parameters [65]. A recent systematic review evaluated the success of treatment pro-tocols on inflammation resolution in patients with peri-implantitis- affected implants [64]. Although most protocols showed improvement on peri- implant tissue param-eters, 18–89% of implants still bled on probing following nonsurgical therapy of peri-implantitis. This type of treatment may be more suitable for esthetic areas where a surgical approach would result in implant thread exposure and compro-mised esthetics [66]. Laser treatment or photodynamic therapy were proven effec-tive in reducing inflammation for a period of at least 6 months. Their effect though on probing depths and attachment levels was negligible [67]. Once the nonsurgical treatment has been completed, a close follow-up of 1–2 months is necessary in order to re-evaluate peri-implant parameters [68].
4.4.3 Surgical Treatment of Peri-implantitis
4.4.3.1 Surface DecontaminationSince the nonsurgical treatment modalities have limited efficacy, surgical interven-tion is usually needed. The surgical treatment of peri-implantitis aims on the arrest of peri-implant bone loss and often times on the regeneration of the resorbed bone.
The main determinant of success of surgical intervention is the decontamination of the exposed implant surface. This task is carried out through mechanical debride-ment, often combined with chemical disinfection and implant surface modification (Fig. 4.13). A systematic review of the literature revealed that no specific chemical agent (Table 4.3) was superior for implant surface decontamination [69]. Another systematic review addressed the effect of various instruments on roughness altera-tions of the surface of dental implants, as well as their prosthetic components [70] (Table 4.4). According to this analysis, smooth-surface implants and implant pros-thetic components should be treated with nonmetal instruments (nonmetal curettes and nonmetal power-driven tips), as it was shown that these leave smooth surfaces
4 Hard Tissue Complications/Peri-implantitis

97
Fig. 4.13 (a) Peri-implant inflammation and radiographic bone loss are evident around this implant. Upon flap reflection significant peri-implant bone loss was noted, and the implant was planned for removal. A titanium micro-brush was used to clean the distal half of the exposed implant surface. Upon removal the implant was submitted for microscopic examination. (b) The microscopic examination revealed established bacterial biofilms on the contaminated implant sur-face. The area of the implant treated with the titanium micro-brush presents with a clean rough surface, free of bacterial biofilms
a
b
unaltered or may produce the least increase in surface roughness. On the other hand, treatment of the exposed rough surface of dental implants with metal instruments (power-driven and curettes) showed a decrease in roughness. This occured by either tearing or scrapping off parts of the TPS surface, or decreasing the height of eleva-tions of the SLA surface.
4.4 Management/Treatment Options

98
A recent review analyzed the literature for different implant surface decontami-nation protocols and their correlation with the treatment outcome [71]. Due to the heterogeneity of the data, no method was proven to be superior. Interestingly the factors that mainly influenced the surgical outcome were: adequate access for proper decontamination, defect configuration, the use of a bone replacement graft, as well as the use of a membrane.
Laser therapy has also been used as an aid for the decontamination of the exposed implant surface and the regeneration of the peri-implant bone. Multiple laser devices, with various wavelengths, have been used, with the Er:YAG laser being the one most extensively researched. A recent systematic review of the literature indi-cated that the improvements noted from the use of lasers in the treatment of peri- implantitis are not substantial in order to indicate a major change in the peri-implantitis treatment protocols [72]. Another systematic review and meta- analysis concluded that due to limited data, the use of lasers in the treatment of peri-implantitis, was not found superior when compared to conventional treatment modalities [67]. Existing evidence is in agreement, that more well designed clinical trials, with longer follow-up periods, are necessary to validate the use of lasers for the treatment of peri-implant diseases.
Table 4.3 Agents used for implant surface decontamination
Abrasive pumiceAir powder (sodium bicarbonate, glycine, etc.)ChlorhexidineCitric acidDelmopinolEDTAHydrogen peroxideLaser therapyPhotosensitizationSaline
Adapted from Claffey N, Clarke E, Polyzois I, Renvert S: Surgical treatment of peri- implantitis. J Clin Periodontol 2008; 35 (Suppl. 8): 316–332
Table 4.4 Instruments used for mechanical debridement of the implant surface
Nonmetal instruments Metal instrumentsCurettes/ultra-sonic • Plastic • Carbon • Resin reinforced, • Non-resin reinforced
Curettes/ultra-sonic • Stainless steel • Titanium • Gold coated
Air abrasion Burs: carbide/diamondRubber cup with/without abrasive paste Diamond polishers
Adapted from Louropoulou A, Slot DE, Van der Weijden F. Titanium surface alterations following the use of different mechanical instruments: a systematic review. Clin. Oral Impl. Res. 23, 2012; 643–658
4 Hard Tissue Complications/Peri-implantitis

99
4.4.3.2 Surgical Intervention ModalitiesMultiple surgical procedures have been advocated for the surgical treatment of peri- implantitis, and the choice of intervention may greatly depend on the configuration of the peri-implant defect [73, 74] (Table 4.5).
The main goal of surgical intervention is to gain access to the contaminated den-tal implant surface (Fig. 4.14). Access flap surgery, however, has shown limited efficacy on the treatment of peri-implantitis. In a prospective study, dental implants diagnosed with peri-implantitis were treated with access flap surgery and bone recontouring. After a 2-year follow-up period, 50% of the implants appeared dis-ease-free. However, 42% of the implants in this study showed signs of peri-implant disease despite treatment, with seven implants removed due to excessive bone loss [75]. In a different study, implants presenting with peri- implantitis were treated with access flap surgery, bone recontouring, and implantoplasty. Although implanto-plasty appears to be a more radical method of implant surface decontamination, it is likely to have a positive effect on the final outcome [76, 77].
A recent meta-analysis assessed the efficacy of surgical interventions on the treatment of peri-implantitis [78]. The results of this review indicated that surgical intervention would yield an average probing depth reduction of 2–3 mm. The addi-tion of implantoplasty seemed to yield superior results, compared to access surgery alone (Fig. 4.15). A mean radiographic bone fill of approximately 2 mm was noted for defects treated with bone grafts or guided bone regeneration (Fig. 4.16). This review concluded that the best results in the literature are reported in studies with very sophisticated implant surface decontamination protocols and those that used a combination of bone replacement grafts with bone morphogenetic proteins. The use of barrier membranes, however, may not offer significant advantages, as the risk of membrane exposure is substantial and may compromise the final result.
Table 4.5 Armamentarium of surgical procedures
Diagnosis Surgical interventionMucogingival defect with bony fenestration or dehiscence
Mucogingival therapy (see Chap. 2)
Horizontal bone loss mild/moderate Apically positioned flap with osseous respective surgery with or without implantoplasty
Vertical bone lossContained infra-bony defect, funnel- shaped three-wallNon-contained one- to two-wall defect
Bone grafts with or without resorbable membraneGuided bone regeneration (non-resorbable membrane and autogenous bone)
Combined vertical and horizontal bone loss
Guided bone regeneration (non-resorbable membrane and autogenous bone)
Loss of osseointegration or bone loss >50% of the implant
Explantation, regeneration, and implant restoration
Adopted from Parma-Benfenati S, Roncati M, Tinti C. Int. J Periodontics Restorative Dent 2013;33:627–633
4.4 Management/Treatment Options

100
Fig. 4.14 The implant at site 4.6 presented with deep probing depths, bleeding on probing, and suppuration. The screw-retained restoration was removed, and significantly inflamed peri-implant tissues were noted. Upon flap reflection a circumferential bone defect was identified. Osteoplasty and implantoplasty were performed. The modified implant surface was disinfected with the use of clindamycin slurry, followed by a hydrogen peroxide rinse. A healing abutment was placed, and the flaps were apically repositioned. Following a healing period of 4 months, clinical probing depths of 2 and 4 mm were noted at the buccal/lingual and mesial/distal aspects, respectively. Inflammation-free peri-implant soft tissues were noted after removing the healing abutment. The initial screw-retained restoration was replaced. Slight mucosal recession was noted at the time of restoration replacement. At 1-year follow-up (last two pictures), a probing depth of 3 mm, abscense of mucosal recession, and inflammation free tissues were noted
4 Hard Tissue Complications/Peri-implantitis
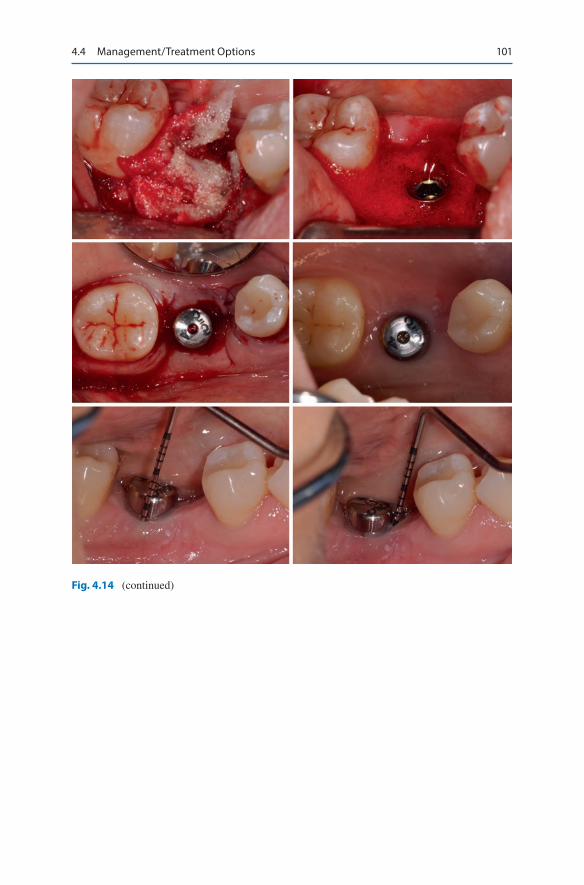
101
Fig. 4.14 (continued)
4.4 Management/Treatment Options

102
Fig. 4.14 (continued)
4 Hard Tissue Complications/Peri-implantitis

103
Fig. 4.15 This implant presented with pain and significant tissue edema around the restoration. Upon removal of the restoration, severe inflammation was evident at the peri-implant soft tissue, with clinical probing depths of 9–10 mm. Plaque and calculus deposits were noted on the implant restoration. Upon flap elevation, significant amounts of granulation tissue were noted, around the implant. Following removal of granulation tissue, bone loss of about 4 mm was noted around the implant, as well as at the proximal surfaces of the adjacent teeth. Implantoplasty, and osteoplasty were performed, and the implant surface was decontaminated with hydrogen peroxide. A stock healing abutment was placed, and the flaps were repositioned apically. After a healing period of 4 months, the healing abutment was removed, and the peri-implant soft tissues were re-evaluated. The peri-implant soft tissues appeared healthy, with no bleeding upon probing. Clinical probing depths of 3 mm were noted at all aspects of the dental implant. A new implant-supported restora-tion was installed, following sufficient healing time. At the 1-year follow-up, the peri-implant tis-sues appear healthy with no bleeding upon probing and normal probing depths. The radiographic examination revealed stable bone levels over the healing period
4.4 Management/Treatment Options

104
Fig. 4.15 (continued)
4 Hard Tissue Complications/Peri-implantitis

105
Fig. 4.15 (continued)
4.4 Management/Treatment Options

106
In a recent systematic review, it was noted that most studies, reporting on the surgical treatment of peri-implantitis, were considered at high risk of bias [64]. Even though, favorable outcomes were reported in the majority of clinical trials, 13–53% of dental implants still bled on probing following surgical intervention. Successful treatment outcomes need to be more consistently defined. Thus, a com-posite criterion of PD <5 mm with no concomitant BOP, and no progressing bone loss, was proposed as the threshold for the need of further treatment [64].
To date, existing evidence on the prevention and treatment of peri-implant dis-eases is subject to a high level of bias, inadequate quality of reporting, and outcome measures [79]. Both clinical and preclinical studies provide inadequate or missing information [79, 80]. Surrogate outcomes, such as probing depths, attachment lev-els, and recession, are often adopted as endpoints, as they have been extensively researched in periodontal disease. However, these endpoints may not represent out-comes appropriate for treatment comparisons. Literature on quality reporting is in agreement that future research must adhere to more strict guidelines.
The choice of surgical treatment modality is largely dependent on defect configu-ration, as well as local and systemic factors. The amount of the remaining bone sup-port will dictate whether treatment should be rendered or the dental implant needs to be removed. Dental implant removal should be considered for those fixtures that have lost more than 2/3 of their total bone support (Fig. 4.17). Furthermore, when signifi-cant peri-implant bone loss is noted prior to the connection of the implant restoration, implant removal should also be considered. Reconstruction of the deficient site is necessary prior to proceeding with dental implant replacement (Fig. 4.18).
Fig. 4.15 (continued)
4 Hard Tissue Complications/Peri-implantitis

107
Fig. 4.16 This implant presented with evidence of peri-implantitis. Clinical and radiographic data confirmed peri-implant bone loss. Upon flap elevation the granulation tissue was removed, and the exposed rough implant surface was mechanically debrided with a titanium micro brush. Following defect debridement and implant surface decontamination, a circumferential bone defect was noted. The infra-bony defect was grafted with a combination of autogenous bone chips with freeze-dried bone allograft. The flaps were repositioned and sutured firmly around the implant restoration
4.4 Management/Treatment Options

108
Fig. 4.17 Significant radiographic bone loss along with deep probing depths were noted around this implant prior to the initiation of the restorative phase. Following flap reflection significant bone loss was identified around the dental implant, accounting for more than 50% of its total length. Thus, dental implant removal was planned, with subsequent site development for future implant replacement. An dental implant removal tool was used, and the implant was reversed torqued and removed. Upon implant removal, a significant bone defect was noted, with total anni-hilation of the palatal wall. Significant bone loss was observed at the adjacent lateral incisor due to the peri-implant infection. Peri-implant bone loss may often affect the prognosis of the adjacent teeth, if it is not dealt within a timely manner. Enamel matrix derivative (Emdogain Straumann®) was used on the denuded root surface, and the residual ridge defect was reconstructed with freeze-dried bone allograft (MTF Dentsply) and a non-absorbable Ti-reinforced d-PTFE membrane (Cytoplast®). After 8 weeks the membrane was removed and the site healed uneventfully. Following healing, adequate ridge width was observed clinically and radiographically. The defect at the mesial aspect of the lateral incisor was fully healed. A regular platform implant (Straumann 4.1 × 10 mm) was placed and was subsequently loaded with a provisional restoration to develop the soft tissue profile. The final restoration was delivered 4 months following implant placement
4 Hard Tissue Complications/Peri-implantitis

109
Fig. 4.17 (continued)
4.4 Management/Treatment Options

110
Fig. 4.17 (continued)
4 Hard Tissue Complications/Peri-implantitis

111
Fig. 4.17 (continued)
4.4 Management/Treatment Options

112
Fig. 4.18 Significant inflammation was noted around these implants, with deep probing depths and bleeding upon probing. A peri-apical radiograph revealed significant bone loss around implants at sites 1.1 and 1.3. Upon flap elevation a significant amount of granulation tissue was noted. The defect was thoroughly debrided, and the exposed rough implant surface was decontaminated via mechanical (diamond burs) and chemical (tetracycline slurry and hydrogen peroxide) means. The defect was grafted with freeze-dried bone allograft, following implant surface decontamination. A collagen membrane was used to contain the bone graft, and the flap was repositioned and sutured around the implant restorations. Significant reduction of the inflammation was noted during the initial healing period. Healthy peri-implant tissues were noted at the 5-year follow-up
4 Hard Tissue Complications/Peri-implantitis

113
Fig. 4.18 (continued)
4.5 Summary
The incidence of peri-implant complications will continue to increase as the use of dental implants, as a treatment modality, becomes more popular. All patients receiv-ing dental implants should be informed of the possibility of peri-implant complica-tions. Good oral hygiene is of paramount importance as it is the main limiting factor for most complications. A radiograph should be taken when an increasing
4.5 Summary

114
peri- implant probing depth is identified. When a diagnosis of peri-implantitis has been rendered, all etiological factors should be controlled or eliminated, when pos-sible. The choice of the surgical treatment modality should depend on the amount of peri-implant bone loss, as well as the configuration of the peri-implant bony defect. Optimal oral hygiene is very important to maintain peri-implant tissue health, fol-lowing the surgical intervention. A personalized maintenance recall protocol should be implemented until all peri-implant parameters are stable and compatible with health.
References
1. Albrektsson T, editor. Consensus report of session IV. Proceeding of the 1st European Workshop on Periodontology. Quintessence Publishing Co.; 1985.
2. Berglundh T, Lindhe J, Marinell C, Ericsson I, Liljenberg B. Soft tissue reaction to de novo plaque formation on implants and teeth. An experimental study in the dog. Clin Oral Implants Res. 1992;3(1):1–8.
3. Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res. 1992;3(1):9–16.
4. Ericsson I, Berglundh T, Marinello C, Liljenberg B, Lindhe J. Long-standing plaque and gin-givitis at implants and teeth in the dog. Clin Oral Implants Res. 1992;3(3):99–103.
5. Heitz-Mayfield LJ, Huynh-Ba G. History of treated periodontitis and smoking as risks for implant therapy. Int J Oral Maxillofac Implants. 2009;24:39–68.
6. Heitz-Mayfield LJ. Peri-implant diseases: diagnosis and risk indicators. J Clin Periodontol. 2008;35(8 Suppl):292–304.
7. Van der Weijden G, Van Bemmel K, Renvert S. Implant therapy in partially edentulous, peri-odontally compromised patients: a review. J Clin Periodontol. 2005;32(5):506–11.
8. Schou S, Holmstrup P, Worthington HV, Esposito M. Outcome of implant therapy in patients with previous tooth loss due to periodontitis. Clin Oral Implants Res. 2006;17(S2):104–23.
9. Karoussis IK, Kotsovilis S, Fourmousis I. A comprehensive and critical review of dental implant prognosis in periodontally compromised partially edentulous patients. Clin Oral Implants Res. 2007;18(6):669–79.
10. Quirynen M, Abarca M, Van Assche N, Nevins M, Van Steenberghe D. Impact of supportive periodontal therapy and implant surface roughness on implant outcome in patients with a his-tory of periodontitis. J Clin Periodontol. 2007;34(9):805–15.
11. Klokkevold PR, Han TJ. How do smoking, diabetes, and periodontitis affect outcomes of implant treatment? Int J Oral Maxillofac Implants. 2007;22(7):173–202.
12. Zangrando MS, Damante CA, Sant’Ana AC, Rubo de Rezende ML, Greghi SL, Chambrone L. Long-term evaluation of periodontal parameters and implant outcomes in periodontally compromised patients: a systematic review. J Periodontol. 2015;86(2):201–21.
13. Sousa V, Mardas N, Farias B, Petrie A, Needleman I, Spratt D, et al. A systematic review of implant outcomes in treated periodontitis patients. Clin Oral Implants Res. 2016;27(7):787–844.
14. Monje A, Alcoforado G, Padial-Molina M, Suarez F, Lin G-H, Wang H-L. Generalized aggres-sive periodontitis as a risk factor for dental implant failure: a systematic review and meta- analysis. J Periodontol. 2014;85(10):1398–407.
15. Atieh MA, Alsabeeha NH, Faggion CM Jr, Duncan WJ. The frequency of peri-implant dis-eases: a systematic review and meta-analysis. J Periodontol. 2013;84(11):1586–98.
16. Strietzel FP, Reichart PA, Kale A, Kulkarni M, Wegner B, Küchler I. Smoking interferes with the prognosis of dental implant treatment: a systematic review and meta-analysis. J Clin Periodontol. 2007;34(6):523–44.
4 Hard Tissue Complications/Peri-implantitis

115
17. Grunder U, Gaberthuel T, Boitel N, Imoberdorf M, Meyenberg K, Andreoni C, et al. Evaluating the clinical performance of the Osseotite implant: defining prosthetic predictability. Compend Contin Educ Dent. 1999;20(7):628–33, 36, 38–40
18. Kumar A, Jaffin RA, Berman C. The effect of smoking on achieving osseointegration of surface- modified implants: a clinical report. Int J Oral Maxillofac Implants. 2002;17(6):816–9.
19. Peñarrocha M, Palomar M, Sanchis JM, Guarinos J, Balaguer J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location, and morphology. Int J Oral Maxillofac Implants. 2004;19(6):861–7.
20. Aalam A-A, Nowzari H. Clinical evaluation of dental implants with surfaces roughened by anodic oxidation, dual acid-etched implants, and machined implants. Int J Oral Maxillofac Implants. 2005;20(5):793–8.
21. Ferreira S, Silva G, Cortelli J, Costa J, Costa F. Prevalence and risk variables for peri-implant disease in Brazilian subjects. J Clin Periodontol. 2006;33(12):929–35.
22. Serino G, Ström C. Peri-implantitis in partially edentulous patients: association with inad-equate plaque control. Clin Oral Implants Res. 2009;20(2):169–74.
23. Balshi TJ, Wolfinger GJ. Dental implants in the diabetic patient: a retrospective study. Implant Dent. 1999;8(4):355–9.
24. Huynh-Ba G, Lang NP, Tonetti M, Zwahlen M, Salvi G. Association of the composite IL-1 geno-type with peri-implantitis: a systematic review. Clin Oral Implants Res. 2008;19(11):1154–62.
25. Albrektsson T, Wennerberg A. Oral implant surfaces: part 1—review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int J Prosthodont. 2004;17(5):536–43.
26. Albrektsson T, Wennerberg A. Oral implant surfaces: part 2—review focusing on clinical knowledge of different surfaces. Int J Prosthodont. 2004;17(5):544–64.
27. Berglundh T, Gotfredsen K, Zitzmann N, Lang NP, Lindhe J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: an experimental study in dogs. Clin Oral Implants Res. 2007;18(5):655–61.
28. Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of peri- implantitis at different types of implants. An experimental study in dogs. I: clinical and radio-graphic observations. Clin Oral Implants Res. 2008;19(10):997–1002.
29. Wennström JL, Ekestubbe A, Gröndahl K, Karlsson S, Lindhe J. Oral rehabilitation with implant-supported fixed partial dentures in periodontitis-susceptible subjects. J Clin Periodontol. 2004;31(9):713–24.
30. Isidor F. Loss of osseointegration caused by occlusal load of oral implants. A clinical and radiographic study in monkeys. Clin Oral Implants Res. 1996;7(2):143–52.
31. Isidor F. Histological evaluation of peri-implant bone at implants subjected to occlusal over-load or plaque accumulation. Clin Oral Implants Res. 1997;8(1):1–9.
32. Heitz-Mayfield LJ, Schmid B, Weigel C, Gerber S, Bosshardt DD, Jonsson J, et al. Does excessive occlusal load affect osseointegration? An experimental study in the dog. Clin Oral Implants Res. 2004;15(3):259–68.
33. Kozlovsky A, Tal H, Laufer BZ, Leshem R, Rohrer MD, Weinreb M, et al. Impact of implant overloading on the peri-implant bone in inflamed and non-inflamed peri-implant mucosa. Clin Oral Implants Res. 2007;18(5):601–10.
34. Klinge B, Meyle J. Peri-implant tissue destruction. The third EAO consensus conference 2012. Clin Oral Implants Res. 2012;23(s6):108–10.
35. Wennström J, Bengazi F, Lekholm U. The influence of the masticatory mucosa on the peri- implant soft tissue condition. Clin Oral Implants Res. 1994;5(1):1–8.
36. Chung DM, Oh T-J, Shotwell JL, Misch CE, Wang H-L. Significance of keratinized mucosa in maintenance of dental implants with different surfaces. J Periodontol. 2006;77(8):1410–20.
37. Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Nine-to fourteen-year follow-up of implant treatment. Part III: factors associated with peri-implant lesions. J Clin Periodontol. 2006;33(4):296–301.
38. Strub J, Gaberthüel T, Grunder U. The role of attached gingiva in the health of peri-implant tissue in dogs. 1. Clinical findings. Int J Periodontics Restorative Dent. 1991;11(4):317–33.
References

116
39. Bouri A Jr, Bissada N, Al-Zahrani MS, Faddoul F, Nouneh I. Width of keratinized gingiva and the health status of the supporting tissues around dental implants. Int J Oral Maxillofac Implants. 2008;23(2):323–6.
40. Kim B-S, Kim Y-K, Yun P-Y, Yi Y-J, Lee H-J, Kim S-G, et al. Evaluation of peri-implant tissue response according to the presence of keratinized mucosa. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107(3):e24–8.
41. Schrott AR, Jimenez M, Hwang JW, Fiorellini J, Weber HP. Five-year evaluation of the influ-ence of keratinized mucosa on peri-implant soft-tissue health and stability around implants sup-porting full-arch mandibular fixed prostheses. Clin Oral Implants Res. 2009;20(10):1170–7.
42. Adibrad M, Shahabuei M, Sahabi M. Significance of the width of keratinized mucosa on the health status of the supporting tissue around implants supporting overdentures. J Oral Implantol. 2009;35(5):232–7.
43. Peri-implant mucositis and peri-implantitis: a current understanding of their diagnoses and clinical implications. J Periodontol. 2013;84(4):436–43.
44. Wilson TG Jr. The positive relationship between excess cement and peri-implant disease: a prospective clinical endoscopic study. J Periodontol. 2009;80(9):1388–92.
45. Wadhwani C, Hess T, Faber T, Piñeyro A, Chen CS. A descriptive study of the radiographic density of implant restorative cements. J Prosthet Dent. 2010;103(5):295–302.
46. Linkevicius T, Puisys A, Vindasiute E, Linkeviciene L, Apse P. Does residual cement around implant-supported restorations cause peri-implant disease? A retrospective case analysis. Clin Oral Implants Res. 2013;24(11):1179–84.
47. Linkevicius T, Vindasiute E, Puisys A, Linkeviciene L, Maslova N, Puriene A. The influence of the cementation margin position on the amount of undetected cement. A prospective clinical study. Clin Oral Implants Res. 2013;24(1):71–6.
48. Periodontology AAo. Glossary of periodontal terms. Chicago, IL: American Academy of Periodontology; 2001.
49. Zitzmann NU, Berglundh T. Definition and prevalence of peri-implant diseases. J Clin Periodontol. 2008;35(s8):286–91.
50. Heitz-Mayfield LJ, Lang NP. Comparative biology of chronic and aggressive periodontitis vs. peri-implantitis. Periodontol 2000. 2010;53:167–81.
51. Lang N, Nyman S, Senn C, Joss A. Bleeding on probing as it relates to probing pressure and gingival health. J Clin Periodontol. 1991;18(4):257–61.
52. Luterbacher S, Mayfield L, Brägger U, Lang NP. Diagnostic characteristics of clinical and microbiological tests for monitoring periodontal and peri-implant mucosal tissue conditions during supportive periodontal therapy (SPT). Clin Oral Implants Res. 2000;11(6):521–9.
53. Etter TH, Håkanson I, Lang NP, Trejo PM, Caffesse RG. Healing after standardized clinical probing of the periimplant soft tissue seal. Clin Oral Implants Res. 2002;13(6):571–80.
54. Lang N, Wetzel A, Stich H, Caffesse R. Histologic probe penetration in healthy and inflamed peri-implant tissues. Clin Oral Implants Res. 1994;5(4):191–201.
55. Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010;81(2):231–8.
56. Tomasi C, Derks J. Clinical research of peri-implant diseases–quality of reporting, case defini-tions and methods to study incidence, prevalence and risk factors of peri-implant diseases. J Clin Periodontol. 2012;39(s12):207–23.
57. Mombelli A, Müller N, Cionca N. The epidemiology of peri-implantitis. Clin Oral Implants Res. 2012;23(s6):67–76.
58. Froum SJ, Rosen PS. A proposed classification for peri-implantitis. Int J Periodontics Restorative Dent. 2012;32(5):533.
59. Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesions different from periodonti-tis lesions? J Clin Periodontol. 2011;38(s11):188–202.
60. Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of ligatured induced peri-implantitis at implants with different surface characteristics. An experimental study in dogs II: histological observations. Clin Oral Implants Res. 2009;20(4):366–71.
4 Hard Tissue Complications/Peri-implantitis

117
61. Albouy JP, Abrahamsson I, Berglundh T. Spontaneous progression of experimental peri- implantitis at implants with different surface characteristics: an experimental study in dogs. J Clin Periodontol. 2012;39(2):182–7.
62. Fransson C, Tomasi C, Pikner SS, Gröndahl K, Wennström JL, Leyland AH, et al. Severity and pattern of peri-implantitis-associated bone loss. J Clin Periodontol. 2010;37(5):442–8.
63. Heitz-Mayfield LJ. Diagnosis and management of peri-implant diseases. Aust Dent J. 2008;53(Suppl 1):S43–8.
64. Heitz-Mayfield LJ, Mombelli A. The therapy of peri-implantitis: a systematic review. Int J Oral Maxillofac Implants. 2014;29(Suppl):325–45.
65. Esposito M, Grusovin MG, Worthington HV. Interventions for replacing missing teeth: treat-ment of peri-implantitis. Cochrane Libr Syst Rev. 2012;(1):CD004970.
66. Renvert S, Polyzois IN. Clinical approaches to treat peri-implant mucositis and peri- implantitis. Periodontol 2000. 2015;68(1):369–404.
67. Kotsakis GA, Konstantinidis I, Karoussis IK, Ma X, Chu H. Systematic review and meta- analysis of the effect of various laser wavelengths in the treatment of peri-implantitis. J Periodontol. 2014;85(9):1203–13.
68. Heitz-Mayfield L, Needleman I, Salvi G, Pjetursson B. Consensus statements and clinical recommendations for prevention and management of biologic and technical implant complica-tions. Int J Oral Maxillofac Implants. 2014;29:346.
69. Claffey N, Clarke E, Polyzois I, Renvert S. Surgical treatment of peri-implantitis. J Clin Periodontol. 2008;35(s8):316–32.
70. Louropoulou A, Slot DE, Van der Weijden FA. Titanium surface alterations following the use of different mechanical instruments: a systematic review. Clin Oral Implants Res. 2012;23(6):643–58.
71. Froum SJ, Dagba AS, Shi Y, Perez-Asenjo A, Rosen PS, Wang WC. Successful surgical pro-tocols in the treatment of peri-implantitis: a narrative review of the literature. Implant Dent. 2016;25(3):416–26.
72. Natto ZS, Aladmawy M, Levi PA Jr, Wang H-L. Comparison of the efficacy of different types of lasers for the treatment of peri-implantitis: a systematic review. Int J Oral Maxillofac Implants. 2015;30(2):338.
73. Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol. 2010;37(5):449–55.
74. Parma-Benfenati S, Roncati M, Tinti C. Treatment of peri-implantitis: surgical thera-peutic approaches based on peri-implantitis defects. Int J Periodontics Restorative Dent. 2013;33(5):627.
75. Serino G, Turri A. Outcome of surgical treatment of peri-implantitis: results from a 2-year prospective clinical study in humans. Clin Oral Implants Res. 2011;22(11):1214–20.
76. Romeo E, Ghisolfi M, Murgolo N, Chiapasco M, Lops D, Vogel G. Therapy of peri-implantitis with resective surgery. Clin Oral Implants Res. 2005;16(1):9–18.
77. Romeo E, Lops D, Chiapasco M, Ghisolfi M, Vogel G. Therapy of peri-implantitis with resec-tive surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part II: radiographic outcome. Clin Oral Implants Res. 2007;18(2):179–87.
78. Chan H-L, Lin G-H, Suarez F, MacEachern M, Wang H-L. Surgical management of peri- implantitis: a systematic review and meta-analysis of treatment outcomes. J Periodontol. 2014;85(8):1027–41.
79. Graziani F, Figuero E, Herrera D. Systematic review of quality of reporting, outcome measure-ments and methods to study efficacy of preventive and therapeutic approaches to peri-implant diseases. J Clin Periodontol. 2012;39(s12):224–44.
80. Schwarz F, Iglhaut G, Becker J. Quality assessment of reporting of animal studies on patho-genesis and treatment of peri-implant mucositis and peri-implantitis. A systematic review using the ARRIVE guidelines. J Clin Periodontol. 2012;39(s12):63–72.
References