perineal repair - nursescholars.files.wordpress.com€¦ · web viewremove the intravaginal swab,...
TRANSCRIPT
Perineal repair
Assessment:- Is the woman in a stabile condition to perform the procedure?- Is the newborn baby in a safe place, and cared for?- Is an assistant available?- Review the technique of repairing a perineal tear- Are all the required items available?
Perineal tear degrees:1st degree: vaginal mucosa and connective tissue2nd degree: vaginal mucosa, connective tissue and muscles3rd degree: complete transection of the anal sphincter4th degree: rectal mucosa also involved
Equipment:- screen- apron- sterile gloves- sharps box- good light source(torch)- sterile suture pack, which should contain gallipot with gauze, needle holder, tissue forceps
(non toothed), scissors, kidney dish, 2 sterile towels- sterile gallipot with sterile maternity cottom wool (big) - sterile sutures (absorbable) 2-0; 3-0 chromic catgut- lignocaine with sterile syringe and 2 needles (10 ml of 0.5% or 1% Lignocaine)- kidney dish- antiseptic solution- trolley or table to prepare the sterile field
Intervention:- screen the bed- inform the woman and obtain informed consent- provide throughout the procedure reassurance- prepare the equipment- let the woman lie on her back on the delivery bed, legs apart, position her towards the lower end of
the bed, keep her covered- ensure good light, directing onto the woman`s perineum and put a stool for you near by, the repair
might take same time and it might be more comfortable to sit while suturing- put on the apron and wash hands- prepare the sterile field on a table ( either open the pack and use the inner layer as the surface for the
sterile field or use a sterile towel to put on the table as the surface for the sterile field, drop all the required item on it, retain the sterility)
- put on sterile gloves and arrange the items on the field- ask the assistant to pour anit-septic solution in the gallipot- ask the assistant to hold the ampoule with the Lidocaine and draw up with aseptic technique 10mls
of Lignocaine into the syringe- ask the assistant to remove the woman`s sheet - cleanse the vulva, using the sponge forceps and in anti-septic solution soaked swabs, working from
top to bottom, using each swab only once ( if you use the gloved hands for cleansing, change the sterile gloves once you finished the cleansing)
- establish a sterile field beneath the woman`s buttocks, over her legs and abdomen, using steril towels- re-examine the genital tract to establish the extent of the trauma - if the tear is extented to the sphincter (3rd and 4th degree) the repair has to be done in theatre by a
doctor- infiltrate the perineum and give time for anaesthesia to be achieved (at least 2minutes)
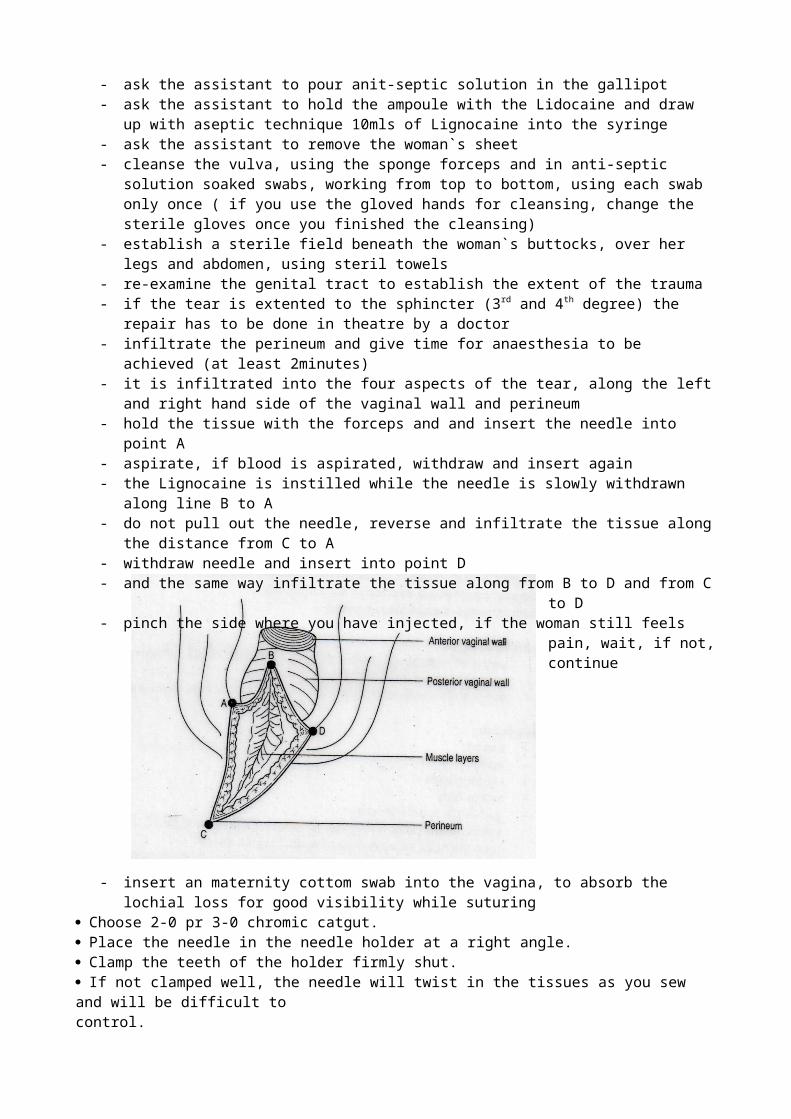
- it is infiltrated into the four aspects of the tear, along the left and right hand side of the vaginal wall and perineum
- hold the tissue with the forceps and and insert the needle into point A- aspirate, if blood is aspirated, withdraw and insert again - the Lignocaine is instilled while the needle is slowly withdrawn along line B to A- do not pull out the needle, reverse and infiltrate the tissue along the distance from C to A- withdraw needle and insert into point D- and the same way infiltrate the tissue along from B to D and from C to D- pinch the side where you have injected, if the woman still feels pain, wait, if not, continue
- insert an maternity cottom swab into the vagina, to absorb the lochial loss for good visibility while suturing
Cho ose 2-0 pr 3-0 chromic catgut.Plac e the needle in the needle holder at a right angle.Clamp the teeth of the holder firmly shut.If not clamped well, the needle will twist in the tissues as you sew and will be difficult tocontrol.
------------------- Run your finger through the whole wound (cut) see clearly where the top of the wound is.- locate the apex(top) of the vaginal tear, insert the first suture 1cm above the apex and anchor with a
knotHold the non-toothed dissecting forceps in your other hand.Use the dissecting (thumb) forceps to pull the needle through the tissue.Never use your fingers, using your finger to feel for the needle is dangerous.Tie the suture off with a square knot and trim off the short thread to about 1cm.
- continue the continuous locked/non-locked suture to the level of the vaginal opening, at the vaginal opening bring together the cut edges and secure the suture with a buried knot at the fourchette
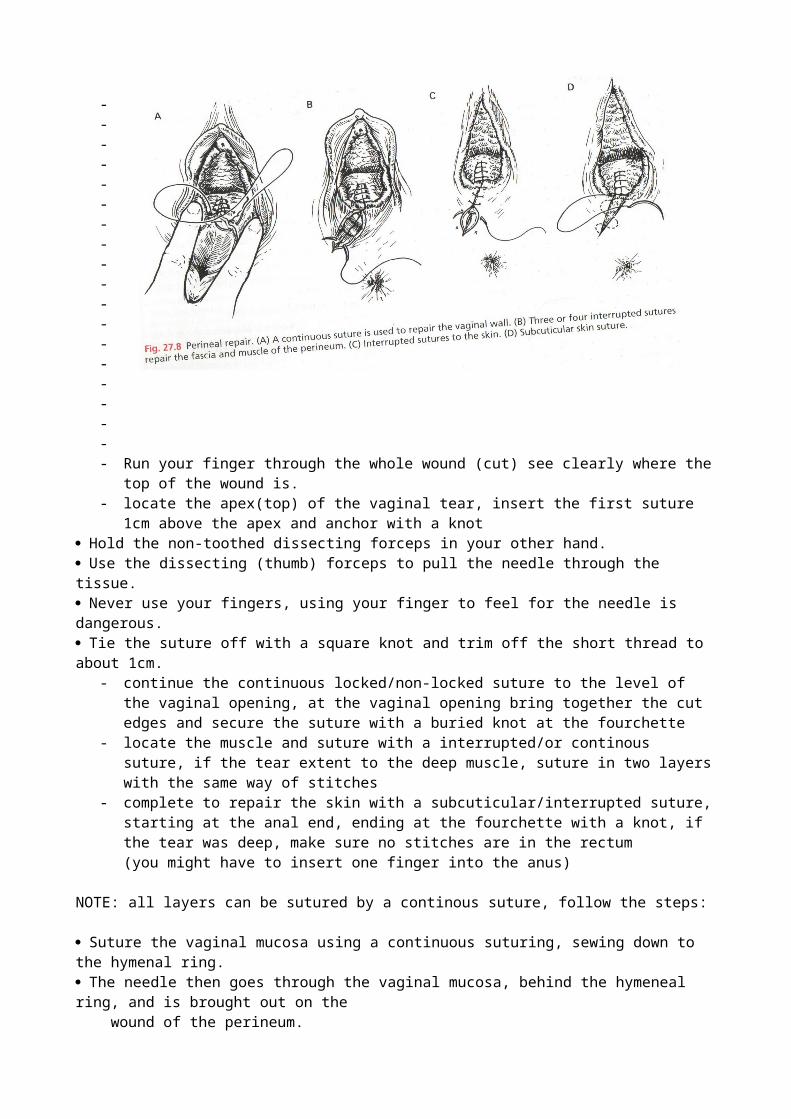
- locate the muscle and suture with a interrupted/or continous suture, if the tear extent to the deep muscle, suture in two layers with the same way of stitches
- complete to repair the skin with a subcuticular/interrupted suture, starting at the anal end, ending at the fourchette with a knot, if the tear was deep, make sure no stitches are in the rectum (you might have to insert one finger into the anus)
NOTE: all layers can be sutured by a continous suture, follow the steps:
Suture the vaginal mucosa using a continuous suturing, sewing down to the hymenal ring.The needle then goes through the vaginal mucosa, behind the hymeneal ring, and is brought out on the wound of the perineum.Notice how close the needle is to the top of the wound.Use continuous suturing as you suture the muscle layer.LOOK inside the cut for the muscle layer; normally, it looks a little red in colour and feels firm to touch.It is important to sew muscle to muscle.FEEL the bottom of the cut; the suture should come though just above the bottom of the cut.When you reach the end of the wound, you have closed the deep muscle layer.Once you have reached the very tip of the wound turn your needle over and start to sew up towards the vagina, using continuous stitches to close the subcuticular tissue.Look for the subcuticular layer just immediately under the skin.This tissue is soft touch and has the same colour as the vaginal mucosa.You are now making a second layer of stitches; this second layer of suture will leave the wound about 0.5 cm. open.This will close well by itself as healing occurs.Now move the suture again from the perineal part of the wound back into the vagina behind the hymenal ring to be secured, tied off, and cut.Tie off the suture with a square knot.To make the knot very secure, make one and a half square knots.Cut the two ends of suture off, leaving about 1 cm.If you cut the end too short, the stitch may pull apart, if this happens, the whole episiotomy/tear becomes loose or pulls apart.
- examine the vagina, that the tissue is in good appostion and the bleeding has stopped- remove the intravaginal swab, examine again the repair gently- wash perineal area with anti-septic, pat dry, and place a sterile sanitary pad over the vulva and
perineum- remove your instruments, make sure the sharp items are disposed directly into the sharps box- clean the woman and help her in a comfortable position- give health talk to her about ongoing care for the repaired perineal tear- dispose the equipment correctly, decontaminate instruments by placing in a plastic container filled
with 0.5% chlorine solution for 10 minutes. and wash hands- offer the woman regular analgesic/anti inflammatory for 48hrs: Diclofenac 50mg TID or
Paracetamol 1g 6 hrly- document: date and time of the procedure, nature and extent of the tear, amount of Lignocaine used,
suture material used, suture techniques used, post-procedure examination results, signature- make her an appointment for review after 1 week