post fall investigations - khca
TRANSCRIPT
10/15/2018
1
Post Fall Investigations
Peg Wessel, RN-BC, DON
Helpful advice from an acting DON
on how to efficiently and accurately
investigate falls in your community

10/15/2018
2
This presentation includes:• Tools for completing a post-fall investigation to
uncover root cause• Training tips for the interdisciplinary team to
assist you with gathering information about the fall
• Guidelines on how to write a clear and concise self-report to submit to KDADs
“How to get the team to “paint the picture” for you”
- How to write a good witness statement- Storyboard education- Associate competencies/education- Do they know what is in the care plan?- Do you share information to ALL associates when a fall
has occurred?

10/15/2018
3
The face of the DON after reviewing witness statements and it states “I was on break when the fall happened”!
FallsWhat to include on a witness statement
- Where was the resident found and in what position? (near the bed, near the bathroom door, face down, on his back or right or left side, legs bent? straight?)
- Equipment? Bed in lowest position, walker nearby? Walker tipped over? Wheelchair nearby? Brakes locked? Call light in reach?
- Fall summary: found on floor, lowered to floor (this is STILL a fall), resident self reported a fall.
- Fall location: resident room, activity room, resident bathroom, dining room, shower/tub room, hallway
- What was resident doing prior to fall? In bed sleeping, eating, sitting in wheelchair, reaching for something, slid out of bed, sitting on toilet (be sure to ASK the resident what they were doing).
- What did the resident say? Write down exactly what they said.
- Footwear at time of fall? Barefoot, slipper socks, shoes, regular socks
- Time resident last toileted or resident last ate?
- Was there anything unusual about the resident during the shift prior to the fall (not eating, lethargic, stated they didn’t feel good)?
****** The primary CNA who observed and/or assisted the resident during the 3 hours prior to the fall will need to write a description to recreate the life of the resident before the fall.
10/15/2018
4
1
COMPLAINT INVESTIGATION WITNESS STATEMENT OF FACTS BEFORE THE KANSAS DEPARTMENT FOR AGING AND DISABILITY SERVICES
THIS FORM MUST BE SIGNED IN THE PRESENCE OF A NOTARY PUBLIC
State of Kansas, County of ______________________________________ Case # __________________________
In the Matter of: _______________________________________________________________________________ (Alleged Perpetrator’s Name)
WITNESS INFORMATION I was employed as _______________________________ at ____________________________________________________ Job Title Name of Facility in __________________________________, Kansas. On or about ________________________ in the year 20_____, I was investigated/witnessed the following incident (describe below) involving
____________________________________________
_____________________________________________________________________________________________________
Resident(s) Involved)
EVENT: In your own words, describe what happened: 1) as accurately as possible; 2) telling when it happened, how it happened and what happened; 3) describing any injury or harm done to the resident(s) and 4) listing the names and titles of other witnesses (if any).
1
I, ________________________________________________ of lawful age, being first duly sworn upon my oath,
hereby state as follows: I have read the above and foregoing statements (or have had the same read to me); have
personal knowledge as to the contents thereof; and that the statements made herein are true and correct.
_________________________________________________________ Signature of Witness, Title __________________________________________________________ ________________________________ Address Phone Number SUBSCRIBED AND SWORN TO before me, the undersigned authority, of this _____ day of ____________________________, 20_____. _________________________________________________________ Notary Public My appointment expires: __________________
10/15/2018
5
“Guidelines for Charge Nurses”
- Do they know your community policy on Incidents/Accidents, specifically Falls?
- Fall Guideline Checklist tool

10/15/2018
6
Apparent Injury No Apparent Injury
-Assess for injury/perform ROM -Assess for injury/perform ROM-Treat Initial Injury/take VS/first aid administered?
-Take vital signs-Did resident hit head?If resident hit head or fall was unwitnessed -Did resident hit head?you MUST initiate neurochecks! If resident hit head OR fall was unwitnessed
you MUST initiate neurochecks!-Notify family/DPOA-Notify physician of fall/ARNP -Notify physician of fall/ARNP-Notify DON
-Notify family/DPOA-Hospital packet: Print medication l ist andpertinent labs or x-rays -Notify DON
-Nurse's note: time of event, where incident -Bed in low positionoccurred, who found resident, where was the -Call light within reachresident found, Dr notified, family notified, -Nonskid shoes or slippers when resident intervention put in place if noninjury fall , any is upfurther orders obtained from the physician. -Night lightIf injury, who transported resident where? -Referral to therapy/restorative program
-System assessment and laboratory-Continue 72 hour neurochecks (q15x4, q30x2 evaluation1 hour x2, then q shift for duration of 72 hrs) -Ensure safe environment
-Toileting program as appropriate-F/U fall charting for 72 hours -Bedside commode
-Medication regimen review-Complete incident report (thoroughly) -Increase activity participation
-Appropriate positioning-Gather witness statements from all (includes CNA, -Evaluation of sensory stimuliCMA, ancillary staff) involved in resident's care -Assess staffing (family, 1:1)Witness statements need to include - What -Light snack or fluids offeredoccurred prior to fal l? When was resident toileted? -Rearrange furniture if needed and lessHad resident complained of pain? When had resident restrictivelast had food or drink? When was resident lastvisually checked? (very important ALL of these
issues are addressed)
What to Chart! Post-fall Interventions
Fall Guidelines ChecklistFollow up Care
10/15/2018
7
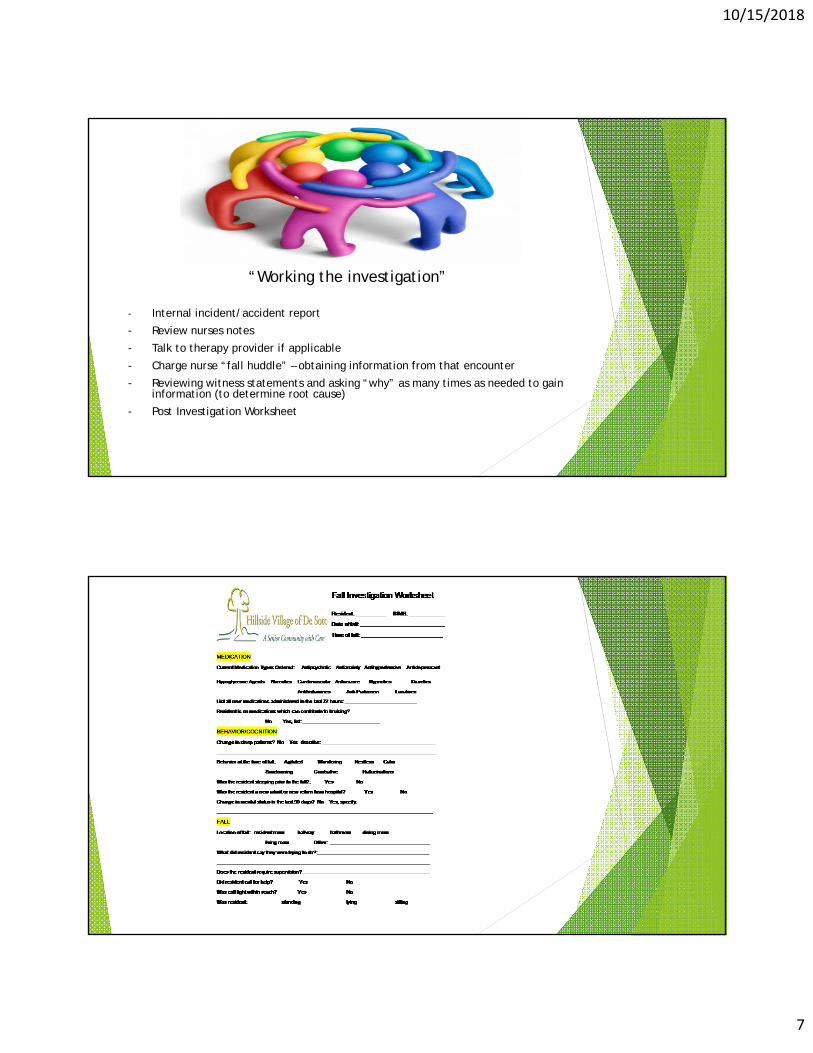
“Working the investigation”
- Internal incident/accident report
- Review nurses notes
- Talk to therapy provider if applicable
- Charge nurse “fall huddle” – obtaining information from that encounter
- Reviewing witness statements and asking “why” as many times as needed to gain information (to determine root cause)
- Post Investigation Worksheet

10/15/2018
8
Was resident using an assistive device? Yes No
Walker Rolling Walker Cane Wheelchair Other: _____________________
What was resident doing prior to fall? ___________________________________________________
When was the last time the resident was toileted? _______________________________________
Incontinent? Bladder Bowel Both
Did resident report the need to be toileted? _____________________________________________
Was resident injured? No injury Injury, describe: _______________________
# of falls in the last 30 days? _______ # of falls in last 31-180 days: _________________
Was this fall: Unwitnessed Witnessed
If unwitnessed fall, were neurochecks initiated? Yes No
CLINICAL CONSIDERATIONS
Recent change in medical condition: No Yes, describe: _______________________
__________________________________________________________________________________
Diagnoses: _______________________________________________________________________
Contributing clinical factors: postural hypotension Parkinson’s disease
Hemiplegia/Hemiparesis impaired hearing impaired vision
Dizziness/Vertigo Fatigue/Weakness Pain Cognitive impairment
Vitals taken at time of fall: B/P ________ P________R________T______O2%__________
ENVIRONMENTAL
Rugs or carpet on floor Floor surface wet Bedspread or Blanket
Furniture Clothing/Shoes Cords (telephone/bed) Other: __________________
Interventions in place at time of fall: ___________________________________________________
ROOT CAUSE OF FALL
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
RECOMMENDATIONS/INTERVENTIONS
_____________________________________________________________________________________
_____________________________________________________________________________________
Care Plan updated (date)____________________________________________
Signature of Investigator: ______________________ Date: _______________
“Sharing the results of the investigation”
- Updating Care Plan/Kardex
- Communicating to all staff about falls (we use PCC Communications portal)
- QAPI – all FALLS are to be discussed at QA meeting (trending and tracking is important)!!
- PIP (Performance Improvement Plan)? Is one needed?
- Fall Committee “meeting of the minds”

10/15/2018
9
“Helping our survey team partners”
- Self-report form filled out completely/detailed**** DON’T FORGET CP NUMBER****
- Pertinent information to assist them in understanding what happened, why it happened and what you did to prevent it from happening again
- Only send part of the care plan and MDS pertaining to the fall (this may include medication care plan)
- If law enforcement involved, ensure you submit complete information or at least a case #
- If Alleged Perpetrator Information Form necessary, fill out all areas completely and accurately
- At the end of the Incident Information section, give a detailed list of what you have provided to the Regional Manager.
10/15/2018
10
Example
Exhibit A: witness statements from Sally Smith, CNA, Joe Jones, RN charge nurse, etc
Exhibit B: nurses progress notes
Exhibit C: pertinent labs or medication order changes or diagnostic tests (x-rays)
Exhibit D: Section C and G of MDS
Exhibit E: Care Plan sections pertaining to ambulation, risk for falls, medications (whatever is pertinent to this report)
And so on…… Regional Managers reviewing these reports are busy too…..
1
KANSAS DEPT FOR AGING & DISABILITY SERVICES CP Number:
REPORTING FACILITY Name: Phone No.: Address: E-mail Address:
(Street/PO Box) (City/State) (Zip code)
REPORTING PARTY Name:
Address:
Work Tele
(Last) (First) (Title/Position)
(Street/PO Box) (City/State)
phone: Work E-mail: (Zip code)
INCIDENT INFORMATION Date of Incident (on or about):
Name of resident(s) involved Cognitive status of resident(s) Description of injury, if any Information upon which this report is being made is as follows: (Please include a specific description of the incident, who was involved, what happened, when it happened, where it happened and how it happened)

10/15/2018
11
1
Corrective Actions taken in response to this incident: For licensed nurse(s), was report made to the Ks State Board of Nursing? _Yes No Plan for monitoring the on-going effectiveness of the corrective action plan through QAA program or other:
Quality Assurance & Assessment guidance resource: S & C Letter 06-11 at http://www.cms.gov/SurveyCertificationGenInfo/PMSR/list.asp
For reporting suspected crime in a LTC facility in accordance with the Affordable Care Act (Certified facilities only): Date and time report made to Law Enforcement LE case number: List of covered individuals who were present or had knowledge of the incident:
Attachments:
Facility Investigative Report & supportive documentation. Please include MDS, care plan, nursing notes pertinent to the incident. For state licensed only ACH such as ALF, RHCF, Home Plus, etc. submit copies of the FCS, NSA and Health Care Plans as appropriate.
Nurse Aide Registry verification if the alleged perpetrator is a CNA and/or CMA and copy of certificate Copy of license if the alleged perpetrator is a licensed nurse List of witnesses and original Notarized witness statements from those individuals regarding abuse, neglect or exploitation
alleged to have been committed by a facility staff member. Completed Alleged Perpetrator Information form (if applicable)
Attestation Statement: I certify that all the information given is true and correct.
Signature of person completing the investigation Printed name Title Date
Please send completed investigation and attachments within 5 working days to:
Regional Manager review/comments/recommendations:
RM Signature Date
1
Case Number: ALLEGED PERPETRATOR INFORMATION FORM
Facility: City:
ALLEGED PERPETRATOR INFORMATION:
Name: (Last) (First) (MI) (Alias)
Address: (Street/PO Box) (City/State) (Zip code)
Telephone:
Please ensure the following information is attached or provided with this form.
EVIDENCE OF PRE-EMPLOYMENT SCREENING & TRAINING ON ANE FOR THIS EMPLOYEE
COPY OF CERTIFICATE OR LICENSE
ALLEGED PERPETRATOR’S NOTARIZED STATEMENT
Date of Hire:
Was the AP Suspended? If suspended, date(s) of suspension
Was the AP Terminated? If terminated, date of termination:
CREDENTIALING/LICENSURE INFORMATION:
Certificate or License No.
Type if Certification (check all that apply)
NAT CNA CMA HHA AD SSD Other
NAT = Nurse Aide Trainee I or II HHA = Home Health Aide
CNA = Certified Nurse Aide AD = Activity Director
CMA = Certified Medication Aide SSD = Social Service Designee
Type of License (check all that apply)
ACHA RN LPN RPT OT LMHT Licensed SW
ACHA = Adult Care Home Administrator RPT = Registered Physical Therapist Licensed SW = Licensed Social Worker
RN = Registered Nurse OT = Occupational Therapist
LPN = Licensed Practical Nurse LMHT = Licensed Mental Health Tech
10/15/2018
12
How Regional Managers look when they receive self-report investigations that are incomplete, inaccurate….and are 200 pages in length……..
10/15/2018
13
For the good work you do every day and bringing quality to the care of our elders!
Peg Wessel, RN-BC, DON