pour.flomax mans 5.29.14
TRANSCRIPT
5/7/13
Does Flomax Reduce Rates of Post-op Urinary Retention in NSX
Patients?
Azam Basheer MD
Mohammed Alsaidi MDMuwaffak Abdulhak MD
Mokbel Chedid MDDonald Seyfried MD
Department of NeurosurgeryHenry Ford Hosital
Detroit, MI
Post Operative Urinary Retention Definition:
inability to empty bladder completely
Sequelae: Pain/anxiety Bladder distention and damage Longer hospital stay Renal failure
Standard treatment: Straight catheterization strictures, trauma, infection & delirium Foley re-insertion
Incidence
5 to 75% of all surgical procedures
Highest in urologic, colorectal and certain orthopedics procedures (hip sx)
POUR in Neurosurgery
Has not been extensively studied
Boulis et al. 39.1% in 503 spine patients McLain et al. 23% in 200 L-spine patients Jellish et al. 22.9% in 61 L-spine patients


Study Design
137 patients prospectively followed for the development of POUR
Definition: Post void residual (PVR) >250 ml 6 hours after the removal of the indwelling urinary catheter (IUC)
For patients with PVR >250 ml on the third check, IUCs were re-inserted, and kept for 5-7 days.

Results
The overall incidence of clinical POUR was 39.4%
Statistical significance (p< 0.05) for high PVR1 was noted in Males Patients older than 60 years of age Spine surgery

PVR1 information by patient characteristics:
0100200300400500
Male Female
Gender (p<0.001)
Me
an
PV
R1
(S
E)
0100200300400500
<60 years 60+ years
Age (p=0.043)
Me
an
PV
R1
(S
E)
0100200300400500
<=200 min >200 min
Surgery Time (p=0.08)
Me
an
PV
R1
(S
E)
0100200300400500
Cranial C/T Lumbar
Surgery location (p=0.012)
Me
an
PV
R1
(S
E)
5/7/13
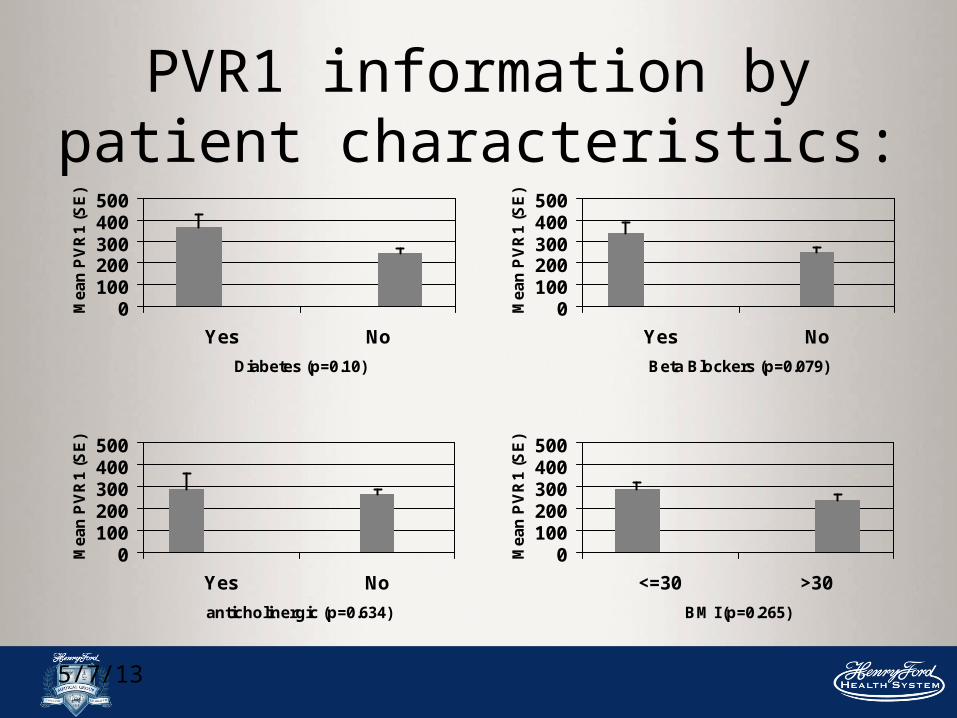
PVR1 information by patient characteristics:
0100200300400500
Yes No
Diabetes (p=0.10)
Me
an
PV
R1
(S
E)
0100200300400500
Yes No
Beta Blockers (p=0.079)
Me
an
PV
R1
(S
E)
0100200300400500
Yes No
anticholinergic (p=0.634)
Me
an
PV
R1
(S
E)
0100200300400500
<=30 >30
BM I (p=0.265)
Me
an
PV
R1
(S
E)
Results cont.
24 (18%) pts had IUCs re-inserted
The association of IUC re-insertion with male gender was significant
5/7/13
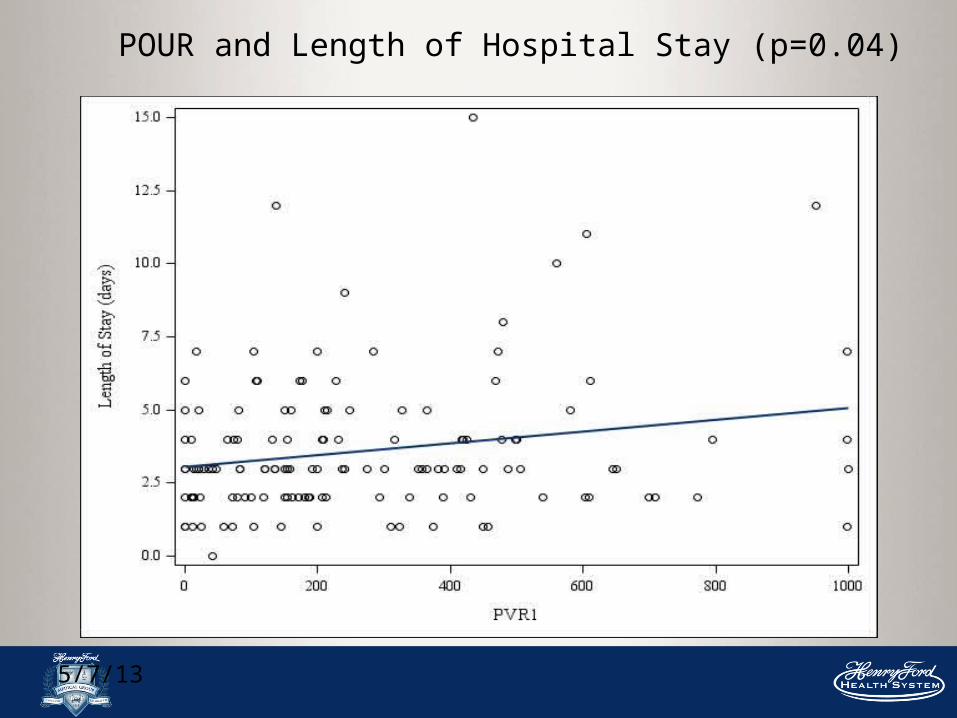
POUR and Length of Hospital Stay (p=0.04)
Conclusion
POUR is prevalent among NSX patients, especially in males, older than 60 years of age, and those with spinal pathologies.
It leads to higher rates of infection and longer hospital stay.
Preventive effect of tamsulosin on postoperative urinary retention in
neurosurgical patients

Flomax
Well-tolerated Effective in people
with BPH Commonly prescribed
by the consulting urology department when NSX patients develop POUR
Potential Benefits
Reduction in morbidity related to treatment of urinary retention
Shortened hospital stays Decreased healthcare costs

5/7/13
Urology Literature
Effectiveness of tamsulosin in prevention of post-operative urinary retention: a randomized double-blind placebo-controlled study. 2/2014
Scrotal surgery. 232 patients Flomax reduced POUR (5.9% vs. 21.1%)
Prophylactic tamsulosin (Flomax) in patients undergoing prostate brachytherapy for prostate carcinoma: final report of a double-blind placebo-controlled randomized study. 5/2005
Prostate surgery. 126 patients. No difference, but positive impact on urinary symptoms at Week 5
Preventive effect of tamsulosin on postoperative urinary retention 6/2012
inguinal herniorrhaphy. Double-blinded. 80 patients. Flomax reduced POUR (2.5% vs 15%)
Methods
A double blinded, two-armed randomized controlled trial
95 male neurosurgical patients undergoing spine surgery
were enrolled and followed up for the development of POUR
Participants were randomized to receive 0.4 mg/day Flomax vs Placebo from 2 days prior to the operation until foley removal post-op
Inclusion criteria
All male patients that undergoing spine surgery, age 18 to 80
Exclusion criteria1. Being on Flomax within the last one month.2. Patients with history of moderate to severe orthostatic hypotension3. Patients who make less than 200 ml/day of urine preoperatively (i.e. end stage renal disease, renal failure) 4. Patients with allergies to Tamsulosin or sulfonamides hypersensitivity5. Patients who have chronic urinary catheterization6. Patients with alterative voiding pathways, such as suprapubic catheters7. Patients who will be admitted to the intensive care unit.8. Patients with history of symptomatic hypotension. Patients will be excluded in clinic if they have a systolic blood pressure < 90.9. History of severe heart failure or major cardiovascular event within the previous 6 months.10. Patients with current ALT or AST > 1000, or Crt > 2.5 during their clinic visits.11. Patients who are actively taken medication that may interact with Flomax( See Clinic Exclusion Medication list)
5/7/13
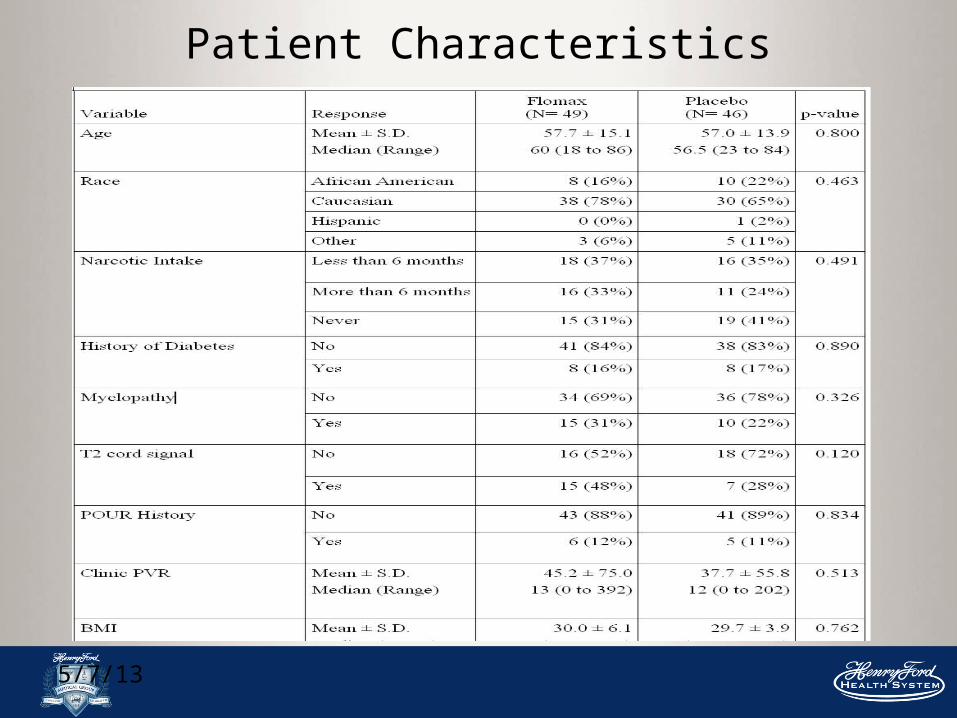
Patient Characteristics
5/7/13
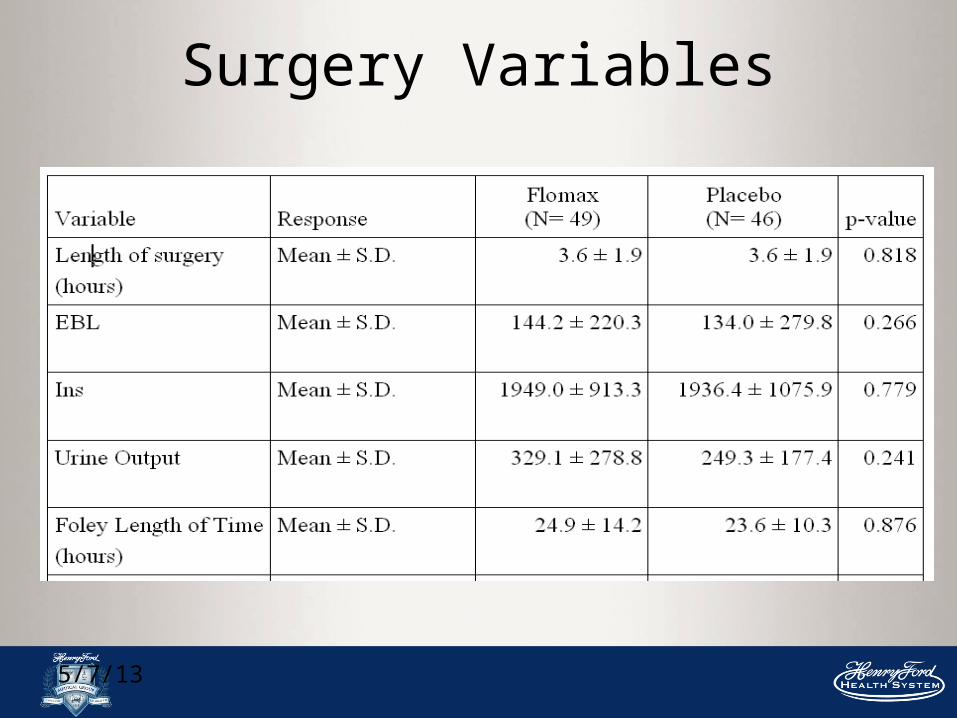
Surgery Variables
5/7/13
POUR
Overall, the rate of developing POUR was similar in the control and treatment groups
16 pts (36%) who were given Tamsulosin developed POUR compared to 13 pts (28%) from the placebo group (P = 0.455)

5/7/13
PVR
0
50
100
150
200
250
300
350
Flomax Placebo
PVR 1
PVR 2
PVR 3
5/7/13
Foley Re-insertion
Of the control group, 5 pts (11%) had foley catheters re-inserted postoperatively
While 7 (14%) pts in the tamsulosin group had the foley re-inserted (p = 0.616)
5/7/13
Conclusion
Tamsulosin peri-operatively showed no real benefit in decreasing the incidence of POUR
Reasons for this?
Placebo effect Multi-factorial cause for POUR Sample size Long term follow up Pain medication use
References1) Gabriele Baldini, M.D.,* Hema Bagry, M.D., F.R.C.A., F.R.C.P.C.,* Armen Aprikian, M.D., F.R.C.S.C.,† Franco Carli, M.D., M.Phil., F.R.C.A., F.R.C.P.C.‡, Postoperative Urinary Retention Anesthetic and Perioperative Considerations. Anesthesiology 2009; 110:1139–57
2) Petros JG, Rimm EB, Robillard RJ. Factors influencing urinary tract retention after elective open cholecystectomy. Surg Gynecol Obstet 1992;174(6): 497–500.
3 ) Williams MP, Wallhagen M, Dowling G. Urinary retention in hospitalized elderly women. J Gerontol Nurs 1993;19(2):7–14.
4 ) Getliffe K. Care of urinary catheters. Nurs Stand. 1996;11(11):47–50.
5.) Schaeffer AJ. Catheter-associated bacteriuria. Urol Clin North Am 1986;13(4): 735–47.
6 ). Smith NK, Albazzaz MK. A prospective study of urinary retention and risk of death after proximal femoral fracture. Age Ageing 1996;25(2):150–4.
7) Darrah DM MD, Griebling TL, MD, MPHb,c, Silverstein JH, MDd,e, Postoperative Urinary Retention. Anesthesiology Clin. 27 2009; 465–484
8) Wu AK, M.D.a,*, Auerbach AD, M.D.a, Aaronson DS, M.D.a,b National incidence and outcomes of postoperative urinary retention in the Surgical Care Improvement Project. Amer Jor of Surgery 2012 Aug;204(2):167-71.
5/7/13
References cont.
9) Keita H, MD, PhD, Diouf E, MD, Tubach F, MD, Brouwer T, MD, Dahmani S, MD, Mantz J, MD, PhD, and Desmonts J, MD. Predictive Factors of Early Postoperative Urinary Retention in the Postanesthesia Care Unit. Anesth Analg. 2005;101:592–6
10) Boulis NM, Mian FS, Rodriguez D, et al. Urinary retention following routine neurosurgical spine procedures. Surg Neurol 2001;55(1):23–7
11) Mclain RF, M.D., Kalfas I, M.D., Bell GR, M.D., Tetzlaff JE, M.D., Yoon HJ M.D., And Rana M, M.D. Comparison of spinal and general anesthesia in lumbar laminectomy surgery: a case-controlled analysis of 400 patients. J Neurosurg Spine 2:17–22, 2005
12) Jellish WS, MD, PhD*, Thalji Z, MD+, Stevenson K, MD*, and Shea J, MDt, A Prospective Randomized Study Comparing Short- and Intermediate-Term Perioperative Outcome Variables After Spinal or General Anesthesia for lumbar Disk and Laminectomy Surgery. Anesth Analg 1996;83:559-64
13) Ali M, Hamiderza A, Ghoamerza M, Samaneh E. Effectiveness of tamsulosin in prevention of post-operative urinary retention: a randomized double-blind placebo-controlled study. Int Braz J Urol. 2014 Jan-Feb;40(1):30-6.
14) Mohamaddi M, Hamedanchi S, Tayyebi A. Preventive effect of tamsulosin on postoperative urinary retention. Korean J Urol. 2012 Jun;53(6):419-23.
15) Elshaikh MA, Ulchaker JC, Reddy CA, Ciezki JP. Prophylactic tamsulosin (Flomax) in patients undergoing prostate 125I brachytherapy for prostate carcinoma: final report of a double-blind placebo-controlled randomized study. Inr J Radiat Oncol Biol Phy. 2005 May 1; 62(1):164-9.