presentation for skin traction
TRANSCRIPT

SKIN TRACTIONPrepared by: Jacqueline Bacayo; RN
Jayson Teruel; RN
Definition
• Traction - Is the application of a pulling force to a part of the body with counter traction a pull in the opposite direction. More specifically, orthopaedic traction occurs when “ A pulling force is exerted on a part or parts of the body”(Davis, 1996).
Purpose of traction
• To reduce a fracture and realign bone fragments by overcoming muscle spasms.
• To maintain skeletal length and alignment.
• To reduce and treat dislocations.
• To immobilize and to prevent further tissue damage.
Purpose of Traction
• To relieve muscle spasms that occur as a reaction to musculoskeletal trauma in the absence of a fracture such as cervical sprain or low back pain.
• To lesson deformities, such as with arthritis.
• To rest a diseased joint.

SKIN TRACTION
Skin Traction
Is attached directly to the patient’s skin to immobilize a body part continuously or intermittently over a short or extended period. The direct application of a pulling force to the patients skin and soft tissues may be accomplished by using adhesive or non adhesive traction tape or other skin traction devices such as a cast, a boot, a belt or a halter. - (Schoen 2000)
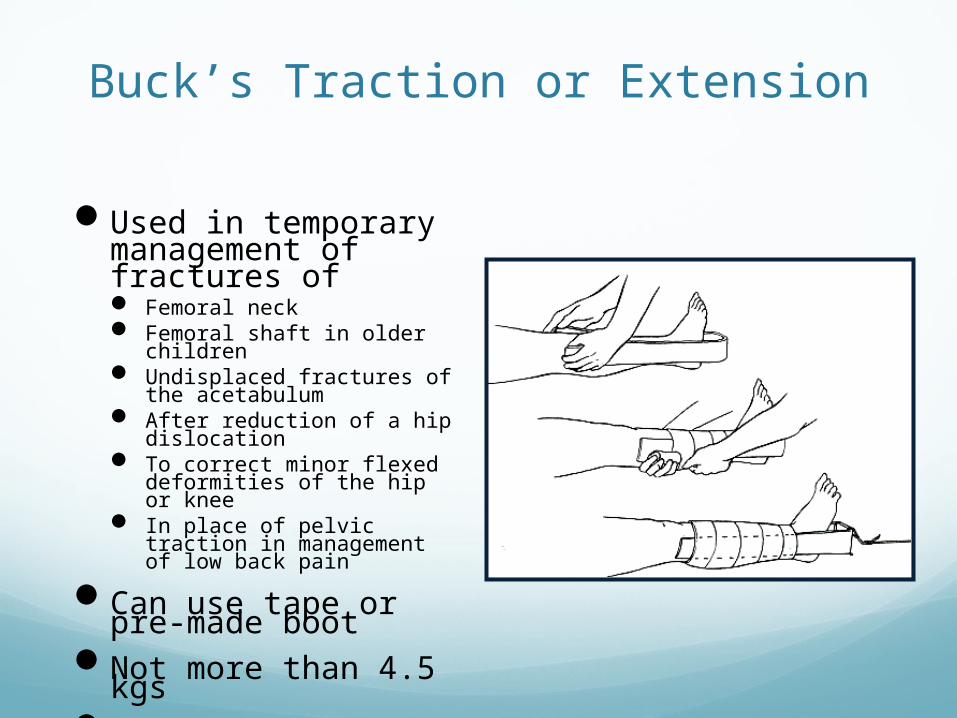
Buck’s Traction or Extension
Used in temporary management of fractures of Femoral neck Femoral shaft in older
children Undisplaced fractures of the
acetabulum After reduction of a hip
dislocation To correct minor flexed
deformities of the hip or knee
In place of pelvic traction in management of low back pain
Can use tape or pre-made boot
Not more than 4.5 kgs
Not used to obtain or hold reduction

Hamilton Russell TractionBuck’s with sling
May be used in more distal femur fracture in children
Can be modified to hip and knee exerciser

Bryant’s Traction
Useful for treatment of femoral shaft fracture in infant or small child
Combines gallows traction and Buck’s traction
Raise mattress for counter traction
Rarely used currently
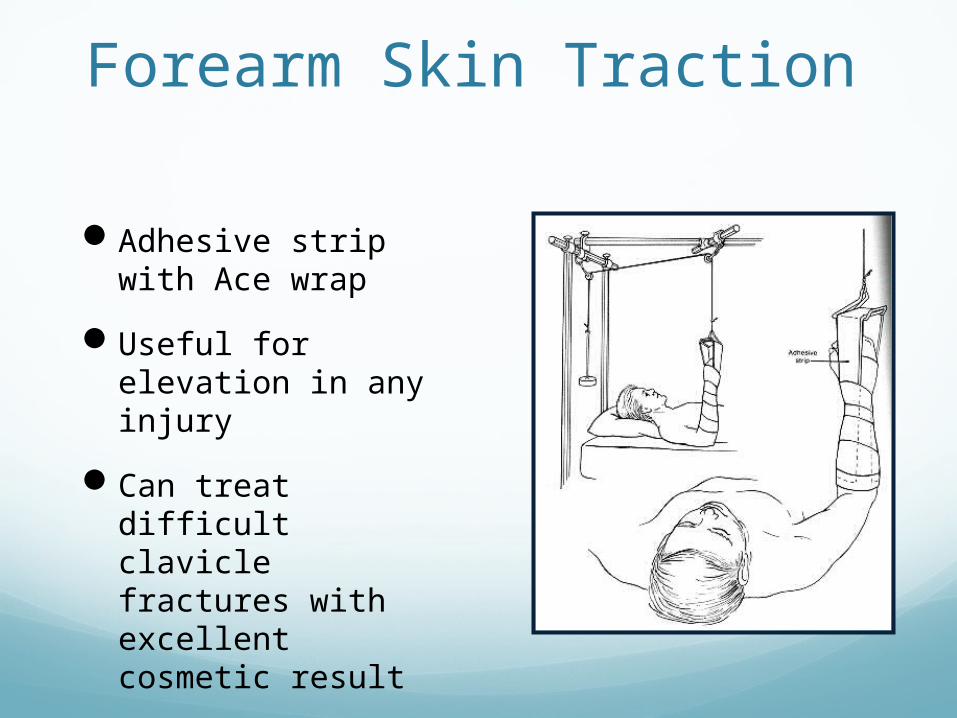
Forearm Skin Traction
Adhesive strip with Ace wrap
Useful for elevation in any injury
Can treat difficult clavicle fractures with excellent cosmetic result
Risk is skin loss
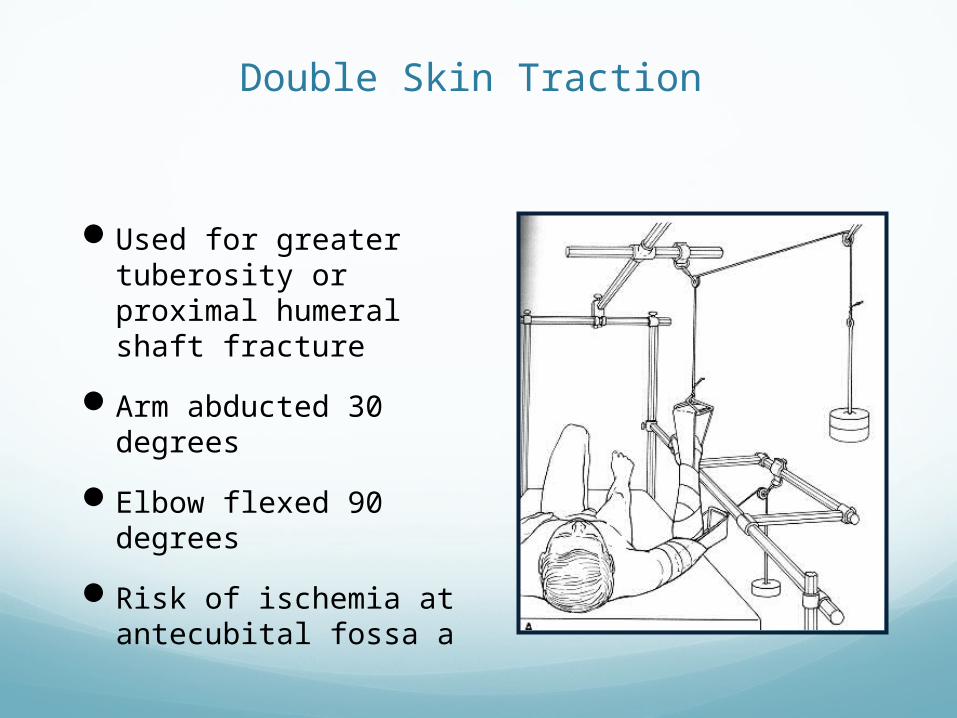
Double Skin Traction
Used for greater tuberosity or proximal humeral shaft fracture
Arm abducted 30 degrees
Elbow flexed 90 degrees
Risk of ischemia at antecubital fossa a

Dunlop’s Traction
Used for supracondylar and transcondylar fractures in children
Used when closed reduction difficult or traumatic
Forearm skin traction with weight on upper arm
Elbow flexed at 45 degrees
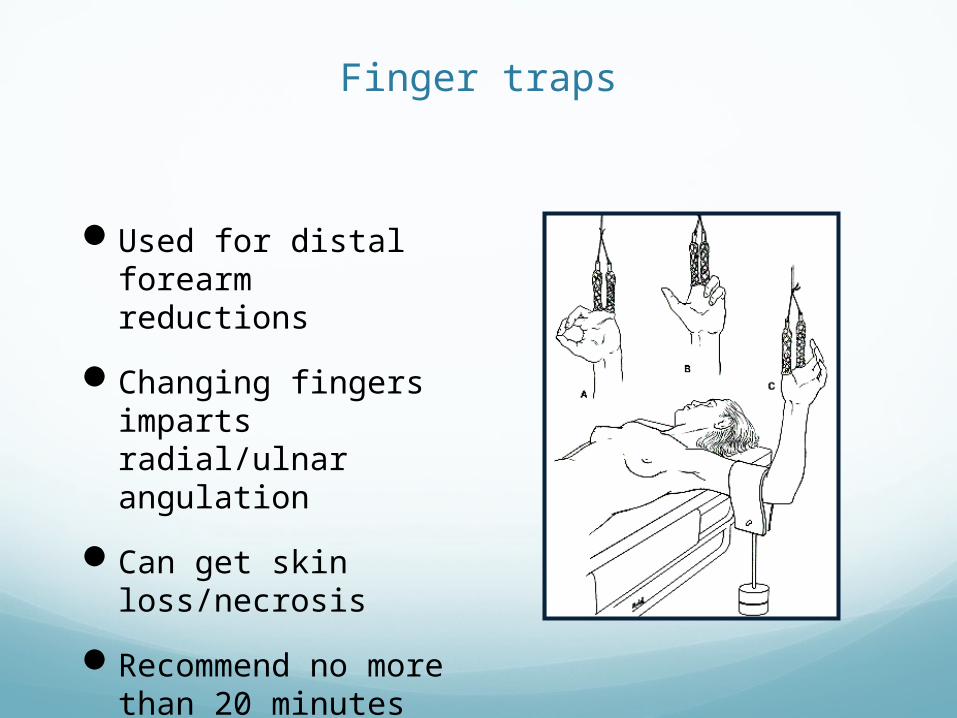
Finger traps
Used for distal forearm reductions
Changing fingers imparts radial/ulnar angulation
Can get skin loss/necrosis
Recommend no more than 20 minutes

Head Halter traction
Simple type cervical traction
Management of neck pain
Weight should not exceed 2.3 kg
Can only be used a few hours at a time
Contraindications Abrasions and lacerations of skin in the area to
which traction is to be applied
Impairment of circulation - Varicose veins, impending gangrene
Dermatitis
When there is marked shortening of the bony fragments, the traction weight required will be more then 6.7 kg which cannot be applied through the skin
ComplicationsAllergic reactions to adhesive
Excortication of skin
Pressure sores around the malleoli and over the tendo calcaneus
Common peroneal nerve palsy
Action/ResponsibilityActionKnowledge Deficit.
Explain the purpose of tractionrelated to injury and healingprocess. Explain the tractionapparatus. For skeletal tractionexplain pin insertion and removalprocedures and care of pin-sites.Maintaining activities of daily livingwhile in traction.
Pain Management.
Assess the patient’s level ofpain and administer analgesiaas prescribed.
Explain that tractiondecreases muscle spasms andwill gradually help lessen pain.
Rationale.
· Providing information helpsalleviate anxiety and enables thepatient to retain furtherinformation and instructions.
· To monitor the effectiveness ofthe prescribed analgesia
· Patient’s treated in traction havepain due to soft tissue and boneTrauma.
Eliminate additional sourcesof pain by providing comfortmeasures.
Assess for correct positioningof traction and alignment ofaffected extremity.
Risk for Impaired Skin Integrity
The patient’s Waterlow Score is assessed. Assess skin over bony prominences (sacrum, trochanters, scapulae, elbows, heels, inner and outer malleolus, inner and outer knees and back of head). Areaswhere skin is stretched tautly over bony prominences are at a greater risk for breakdown because the possibility of ischeamia to skin is high due to compression of skin capillaries between a hard surface(mattress, chair,) and the bone.
-Diversionary activities (books, games, television etc), heat or cold treatments and position changes.
-Incorrect positioning andmalalignment can be sources ofpain.
· Frequent repositioning isrequired to alleviate pressurepain and discomfort. A thoroughskin assessment should becarried out each time thepatient is repositioned.

The decision to nurse thepatient on a pressure-relievingmattress depends on thenurse’s clinical judgment.
Maintain correct padding foraffected extremity in traction,keep bed-linen wrinkle free anddry.
Assess for fecal or urinaryincontinence, clean and dry skindaily.
-These measures help tominimize the risk ofcomplications of skinbreakdown.
· Pressure areas and skin irritationcan develop under or at the edgeof traction device.
· The urea in urine turns into ammonia within minutes, and iscaustic to the skin. Feces maycontain enzymes that cause skinbreakdown.
Impaired Physical Mobility.
Instruct in the use of assistance devices i.e. Monkey pole.
Teach strengthening exercisesto affected limb and other limbsas appropriate.
Encourage activities of selfcare and the use of the trapezeif the patient’s arms will allow.
-To promote independence.
-Exercises should be active toprevent muscle atrophy and jointstiffness, which occur quickly inthe situation of reduced mobility.
· To promote independence.
High risk of injury.
Traction Device:
-Keep weights hanging freely, tighten all traction equipment and secure all knots.
-Cords should be checked daily for fraying, particularly where they pass over pulleys.
-Monitor the patient for signs and symptoms of neurovascular compromise, comparing findings to the unaffected limb.
a) Check for diminished or absentpedal pulses.
b) Check for capillary refill time >3seconds.
The traction system should be checked thoroughly at least daily and always after interventions such as physiotherapy and x-ray.
· To maintain a safe environment.
- Careful monitoring enables early detection. The traction equipment may through increased pressure on nerves and blood vessels cause temporary or permanent damage.
-Surgical trauma causes swellingand oedema, which can compromise circulation and compress nerves.
- Prolonged capillary refill timepoints to diminished capillaryperfusion.
c) Observe for pallor, blanching,cyanosis and coolness ofextremity.
d) Check for complaints ofabnormal sensations, e.g.tingling and numbness.
e) Observe for increased pain notcontrolled by medication.
Assess the affected extremityfor signs and symptoms of alteredperfusion of compartmentsyndrome. (See guideline onCompartment Syndrome.)
- These signs may indicatecompromised circulation.
- These symptoms may resultfrom nerve compression.
- Tissue and nerve ischemia produces a deep, throbbing unrelenting pain.
Compartment syndrome resultsfrom severe tissue swelling thatdecreases blood flow, causesischemia and may causepermanent motor/sensorydamage.
Risk for Deep venous thrombosis/Pulmonary embolus.
- Ensure anti-embolic stockings are fitted on both limbs.
- Continuously assess the patient for signs and symptoms Of: Deep Venous Thrombosis
* Positive Homan’s Sign ( Forced dorsiflexion of the foot causing discomfort in the upper calf.)• Swelling of leg,• Tenderness in calf.
Pulmonary Embolus.Dyspnea, Chest pain, Tachycardia, Hemoptysis,Cyanosis, Anxiety, Pyrexia of unknown origin.
Give anti-coagulanti.e.Clexane s/c Daily
Elastic stockings have beenshown to reduce the risk ofD.V.T. by about 25%(Todd&Sitzman 1998).
Compression stockings must beused correctly, otherwise theymay become a cause rather thana deterrent of D.V.T. (Evans,1991).
· Early detection and treatment.
-To prevent complications of deepvenous thrombosis or pulmonaryembolus.
References
Apley, A.G., Solomon, L. (1993) Apley’s System of Orthopaedics and Fractures. 7th Edition.Butterworth Heinemann.
Black, Matassarin, Jacobs (1993). An Introduction to OrthopaedicNursing 2nd Edition. Naon ProductionsDavis, P.S. (1996) Nursing the Orthopaedic Patient. ChurchillLivingstone.
Evans A. (1991) Sensible Stockings. Nursing Times 87 (51) 40-41.
Todd B.,Sitzman M.D. (1998) Prevention of Perioperative Deep VeinThrombosis and Pulmonary Embolism.
Schoen D.C. (2000). Adult Orthopaedic Nursing.1st PublicationPhiladelphia Lippincott.

THANK YOUand
HAVE A NICE DAY