proceedings ofthe society of british
TRANSCRIPT

Journal of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 1277-1287
Proceedings of theSociety of British Neurological Surgeons
The 86th Meeting of the Society of British Neurological Surgeons was held at the NationalHospital, Queen Square, and the Hospital for Sick Children, London, on 2 and 3 May 1974.
SURGERY OF SUPRATENTORIAL MENINGIOMAS:A MODERN SERIES
VALENTINE LOGUE (London) emphasized that post-operative neurological defects, persistence of pre-operative epilepsy, and the appearance of postopera-tive epilepsy were due to brain retraction anddistortion, damage to arteries, or interruption ofveins. A series of 350 cases was presented. Essentialfeatures of the operative technique were circum-ferential incision of dura mater close to the tumour,exenteration of the tumour with diathermy loop,sucker, or rongeur, division of vessels betweentumour capsule and brain, excision of exposed duramater, and removal of the bone flap, which was thenfrozen in antibiotic solution in preparation forreplacement at a later date. Where possible, involvedsinus was removed.
There were 16 operative deaths, giving a totalmortality rate of 4-57%. For convexity tumours therate was 3-2%y and for basal tumours 6-7%. Venousinfarction was a more frequent cause of death thanarterial. Three patients were admitted in coma.Of the 350 cases, 287 returned to work, 15 were
left dependent, and 48 died before being gainfullyemployed or settled. Thirty-seven of those who wentback to work did so in a higher grade, 220 returned inthe same grade, and 30 went back at a lower grade.Two hundred and nine (60%) of the patients had
preoperative epilepsy. Of these 130 were completelyfree of fits after operation. Postoperative epilepsyoccurred in 8 (5-7%4) of the 141 patients without pre-operative seizures.
Epilepsy was thus relieved in 62 2%4. The numberof recurrences among 296 survivors to 1971 was 33(1 1 1%).INTRACRANIAL VOLUME/PRESSURE RELATIONSHIPS-
CLINICAL AND EXPERIMENTAL ASPECTS
hypertension. Increase in ICP was thought to be dueto failure of compensation for the increased volumeof intracranial mass lesions. During continuous ICPmonitoring it was not possible to measure the amountof compensatory reserve when the ICP was stillnormal.
Experiments were made with humans and baboons,introducing fluid into a lateral ventricle and measur-ing the volume/pressure response (VPR). In humansa significant positive correlation was found betweenresting ICP and VPR induced by a 1 ml increase inventricular fluid volume. In baboons there was acorrelation between VPR and increase in size of anextradural balloon. When ICP approached arterialpressure, cerebral blood flow decreased, and VPRfell. With normal ranges of ICP, changes of arterialpressure did not affect the low VPR. When ICP wasincreased, VPR rose with arterial hypertension.Mannitol produced 20%4 reduction in ICP for 30minutes and 50°4 reduction in VPR for 45 minutes.Hyperventilation to an arterial PCO2 of 25 mmHgproduced a reduction in ICP (30%O) which returnedto the control level at 45 minutes. The effect on theVPR was similar. Clinical studies on humans withbrain injuries demonstrated a closer correlationbetween angiographic shift and VPR than betweenresting ICP and VPR.The value of VPR measurement in patients with
mass lesions was less when hydrocephalus is present.In humans mannitol produced a fall in ICP but agreater reduction in VPR over a 45 minute periodBeta-methasone (4 mg/6 hourly) reduced ICP by18%. and VPR by 71%Y over 24 hours.VPR was a measure of periventricular elastance
which was largely a property of cerebral bloodvessels. The aim of treatment was not only to reduceICP but give the brain the ability to compensatefurther and this property was measured by VPR.
J. D. MILLER, P. J. LEECH, and J. D. PICKARD (Glasgow)pointed out that sudden unpredictable increases in PREFERRED ROUTE TO THE PITUITARY-intracranial pressure (ICP) might occur in a variety TRANSETHMOIDAL SURGERYof conditions such as trauma, tumour, vascular dis- HUW GRIFFITH and RASHID AHMAD (Bristol) describedorders, cerebral hypoxia, and benign intracranial their experience of 136 transethmoidal pituitary
1277
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from
Proceedings of the Society of British Neurological Surgeons
operations, and showed a film of the procedure.After packing the nose with gauze soaked in cocaine,adrenaline, and chlorhexidine, the surgeon made aright ethmoidal incision which was deepened as faras the anterior ethmoidal artery, a landmark for thelevel of the cribriform plate. The operating micro-scope was brought to bear and the approach con-tinued through the ethmoidal cells, the perpendicularplate of the ethmoid, and the sphenoidal air sinus.A chisel and a 2 mm bite punch were used to enterthe sella. The dura mater was opened with dia-thermy and special bayonet microscissors. Whenendocrine surgery was being performed the pituitarystalk was divided before removal of the gland. Incases where gland and fossa were large, removal ofsome of the gland might be necessary before accessto the stalk was obtained. Complete removal ofchromophobe adenomas was seldom possible. Thefossa was sealed with muscle and fascia lata, a gauzepack was led down the right nostril, and the skin wasclosed in two layers. Results are tabulated below.
No. Mortality
Carcinoma of breastAcromegalyCushing's syndromeNelson's syndromeVisual pathway compression
Totals
1001771
11
136
61
One patient had a central scotoma due to ahaemorrhage in the retracted eye, one developed acentral field defect thought to be due to use of uni-polar diathermy near the right optic nerve, one had a6th nerve palsy which recovered, nine had cerebro-spinal fluid leaks (cured by fascial grafts), three hadmeningitis, and one had a tear in the right internalcarotid artery due to the use of too large a bonepunch.
This operation was advocated for all cases ofpituitary disease requiring surgery.
VARIABILITY STUDY OF HUMAN BRAIN-STEM
STRUCTURES
F. AFSHAR (London) had investigated the positionand variability of the trigeminal nucleus and tractand of related brain-stem structures, including thespinothalamic tract, because of interest in techniquesof percutaneous tractotomy. Measurements hadbeen made in 30 hemibrain-stems obtained fromnecropsies on patients without central neurologicaldisorder.At the obex level the coordinates of the centre of
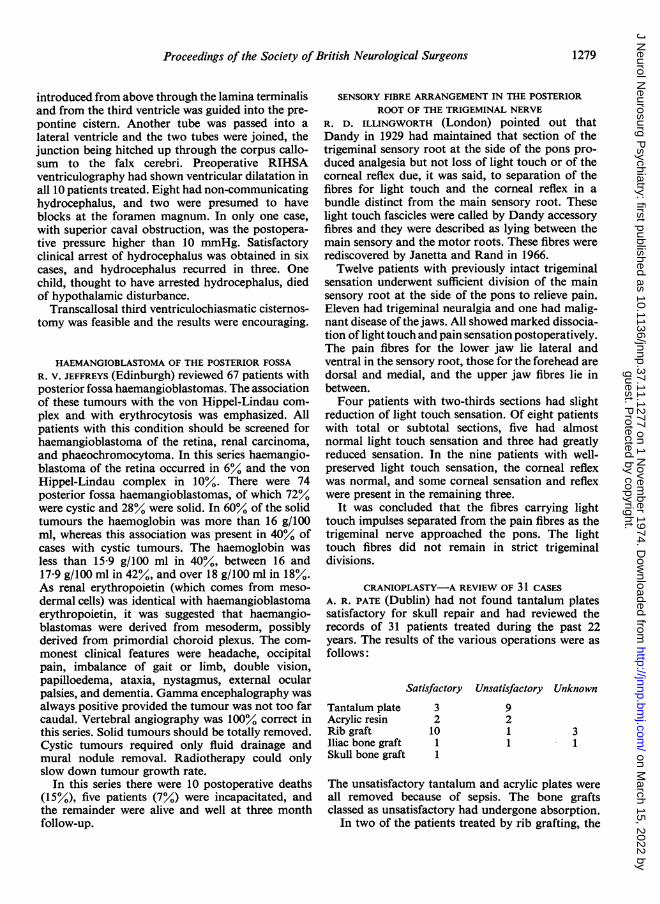
the trigeminal tract were 6-5 mm from the midlineand 4 5 mm from the posterior surface of the brain-stem. The mean measurements and variability were:
At obex level-22 mm caudal to fastigiumMean(mm)
MedialLateralAnteriorPosterior
SD± SEM
5-46 064 0-146-97 0-72 0-165-67 1.11 0-253-41 0-92 0-21
At the Cl level in the spinal cord the coordinateswere 3-0 mm from the posterior cord surface and5 25 mm from the midline. The mean measurementsand variability were:
Level 31 mm caudal to fastigium
MedialLateralAnteriorPosterior
Mean(mm)4*285-463.932-03
SD± SEM
0-70 0-17064 0161.09 0-270-60 0-15
At 5 mm below the fastigial level (approximatelythe site for tractotomy) the centre of the structurewas 6-0 mm from the 4th ventricular floor and 5 75mm from the midsagittal plane. In view of the closeproximity of important nuclei and tracts here, it wassuggested that tractotomy would be better carriedout 8 to 9 mm more caudally in the medulla.
FORAMEN OF MAGENDIE
GORDON BROCKLEHURST (Hull) read a paper based onhis 1973 Sir Hugh Cairns Memorial Fund prizeessay. Some primitive animals had no anatomicalpathway through the roof of the fourth ventricle,most mammals had laterally placed fourth ventricleforamina, and man, in common with Old Worldmonkeys and anthropoids, had a median foramen.In the 20 mm human embryo, the metapore was in aprocess of active development. Evidence showed thephylogenetic and physiological independence of theinternal and external cerebrospinal fluid compart-ments. In the treatment of hydrocephalus the limitedsuccess of the Torkildsen operation was probablydue to obliteration of the ambient cistern, whilefailure of the Stookey-Scarff procedure might be dueto surgical destruction of the chiasmatic and inter-peduncular cisterns. To overcome these problems theoperation of transcallosal third ventriculochiasmaticcisternostomy had been devised. A silastic tube
1278
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from
Proceedings of the Society of British Neurological Surgeons
introduced from above through the lamina terminalisand from the third ventricle was guided into the pre-pontine cistern. Another tube was passed into alateral ventricle and the two tubes were joined, thejunction being hitched up through the corpus callo-sum to the falx cerebri. Preoperative RIHSAventriculography had shown ventricular dilatation inall 10 patients treated. Eight had non-communicatinghydrocephalus, and two were presumed to haveblocks at the foramen magnum. In only one case,with superior caval obstruction, was the postopera-tive pressure higher than 10 mmHg. Satisfactoryclinical arrest of hydrocephalus was obtained in sixcases, and hydrocephalus recurred in three. Onechild, thought to have arrested hydrocephalus, diedof hypothalamic disturbance.
Transcallosal third ventriculochiasmatic cisternos-tomy was feasible and the results were encouraging.
HAEMANGIOBLASTOMA OF THE POSTERIOR FOSSAR. V. JEFFREYS (Edinburgh) reviewed 67 patients withposterior fossa haemangioblastomas. The associationof these tumours with the von Hippel-Lindau com-plex and with erythrocytosis was emphasized. Allpatients with this condition should be screened forhaemangioblastoma of the retina, renal carcinoma,and phaeochromocytoma. In this series haemangio-blastoma of the retina occurred in 6% and the vonHippel-Lindau complex in 10%. There were 74posterior fossa haemangioblastomas, of which 72%were cystic and 28% were solid. In 60% of the solidtumours the haemoglobin was more than 16 g/100ml, whereas this association was present in 40% ofcases with cystic tumours. The haemoglobin wasless than 15-9 g/100 ml in 40%, between 16 and17-9 g/100 ml in 42%, and over 18 g/100 ml in 18%.As renal erythropoietin (which comes from meso-dermal cells) was identical with haemangioblastomaerythropoietin, it was suggested that haemangio-blastomas were derived from mesoderm, possiblyderived from primordial choroid plexus. The com-monest clinical features were headache, occipitalpain, imbalance of gait or limb, double vision,papilloedema, ataxia, nystagmus, external ocularpalsies, and dementia. Gamma encephalography wasalways positive provided the tumour was not too farcaudal. Vertebral angiography was 100% correct inthis series. Solid tumours should be totally removed.Cystic tumours required only fluid drainage andmural nodule removal. Radiotherapy could onlyslow down tumour growth rate.
In this series there were 10 postoperative deaths(15%), five patients (7%.) were incapacitated, andthe remainder were alive and well at three monthfollow-up.
SENSORY FIBRE ARRANGEMENT IN THE POSTERIORROOT OF THE TRIGEMINAL NERVE
R. D. ILLINGWORTH (London) pointed out thatDandy in 1929 had maintained that section of thetrigeminal sensory root at the side of the pons pro-duced analgesia but not loss of light touch or of thecorneal reflex due, it was said, to separation of thefibres for light touch and the corneal reflex in abundle distinct from the main sensory root. Theselight touch fascicles were called by Dandy accessoryfibres and they were described as lying between themain sensory and the motor roots. These fibres wererediscovered by Janetta and Rand in 1966.
Twelve patients with previously intact trigeminalsensation underwent sufficient division of the mainsensory root at the side of the pons to relieve pain.Eleven had trigeminal neuralgia and one had malig-nant disease of the jaws. All showed marked dissocia-tion of light touch and pain sensation postoperatively.The pain fibres for the lower jaw lie lateral andventral in the sensory root, those for the forehead aredorsal and medial, and the upper jaw fibres lie inbetween.Four patients with two-thirds sections had slight
reduction of light touch sensation. Of eight patientswith total or subtotal sections, five had almostnormal light touch sensation and three had greatlyreduced sensation. In the nine patients with well-preserved light touch sensation, the corneal reflexwas normal, and some corneal sensation and reflexwere present in the remaining three.
It was concluded that the fibres carrying lighttouch impulses separated from the pain fibres as thetrigeminal nerve approached the pons. The lighttouch fibres did not remain in strict trigeminaldivisions.
CRANIOPLASTY-A REVIEW OF 31 CASESA. R. PATE (Dublin) had not found tantalum platessatisfactory for skull repair and had reviewed therecords of 31 patients treated during the past 22years. The results of the various operations were asfollows:
Satisfactory Unsatisfactory Unknown
Tantalum plateAcrylic resinRib graftIliac bone graftSkull bone graft
321011
9211
31
The unsatisfactory tantalum and acrylic plates wereall removed because of sepsis. The bone graftsclassed as unsatisfactory had undergone absorption.
In two of the patients treated by rib grafting, the
1279
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
pleura was opened and atelectasis occurred inanother.Rib grafting was recommended as a simple and
effective method of skull repair, although thecosmetic results were inferior to those obtained byuse of plates.
SOME PARTICULAR FEATURES IN THE MANAGEMENTOF EXTRA-INTRACRANIAL ANASTOMOSIS
J. LECUIRE, R. DERUTY, J. P. DECHAUME, and PH. BRET(Lyons, France) had performed 15 extra-intracranialarterial anastomoses. The extracranial vessel usedwas the superficial temporal artery in 12 cases, andthe occipital artery in three. In 10 cases anastomosiswas made with the anterior temporal branch of themiddle cerebral artery, and in five cases with theposterior temporal or angular artery. Scovilleclamps were placed on the cortical vessel in the earlycases but, because these clamps seemed to causevasospasm, microtourniquets are now preferred.
Postoperative angiograms showed patency in ninecases and obstruction in six. One patient died ofcardiovascular disease six months after operationand was found at necropsy to have a patent anasto-mosis. The six patients with obliterated anastomoseswere no worse clinically after operation. Of the ninepatients with patent anastomoses, one remainedunaltered, two improved neurologically, and six hadno more ischaemic attacks.
STUDIES OF LOCAL BLOOD FLOW AND CORTICALACTIVITY IN THE EXPERIMENTAL PRIMATE
LINDSAY SYMON, NEIL M. BRANSTON, H. ALANCROCKARD, and JOHAN JUHASZ (London) had em-ployed a technique of hydrogen polarography usingmultiple platinum electrodes in cortex and deepnuclei to study the distribution of reduced bloodflow after middle cerebral artery occlusion in experi-mental animals. The focal nature of hydrogenrecording enabled local blood flow to be related tonervous tissue function.The study showed no significant differences
between CO2 reactivity obtained from cortex,putamen, or white matter, which were in the regionof 2-3 5% per Torr increase in flow, although the datasuggested a somewhat greater reactivity for whitematter than for grey. Excellent autoregulation toaltered perfusion pressure induced either by haemor-rhage or by raised intracranial pressure was found,and autoregulatory curves to changes in perfusionpressure obtained by either method seemed identical.Pressure measurements during establishment of anextradural space occupying lesion indicated passivepressure perfusion of the compressed hemispherefirst, followed by general autoregulation failureassociated with subfalcine herniation.
After middle cerebral artery occlusion, reductionof blood flow was present over the entire lateralaspect of the cerebral hemisphere, being maximal inthe frontoparietal and temporal opercula and in thedeep nuclei. Reactivity to carbon dioxide wascorrespondingly reduced and intracerebral steal wasfound in the most densely ischaemic opercular zone.In no area was tissue blood flow increased. With theestablishment of an acute ischaemic lesion failure ofa somatosensory evoked response occurred whichwas critically dependent on a final blood flow afterocclusion of < 16 ml/100 g (two minutes' clearance).
PROXIMAL OCCLUSION OF THE ANTERIOR CEREBRALARTERY FOR ANTERIOR COMMUNICATING ANEURYSM
A. HOCKLEY (Cambridge) reported 10 years' experi-ence in the treatment of anterior communicatinganeurysms in a centre where proximal anteriorcerebral artery occlusion had been the operation ofchoice. Out of a total number of 372 patients withhaemorrhage from aneurysms, 124 had anteriorcommunicating aneurysms. When the aneurysmfilled mainly from one side, and the cross-flow wasadequate, occlusion of the main supplying anteriorcerebral artery was the preferred treatment.
In this series 68 patients were treated by anteriorcerebral artery occlusion, 15 by direct surgery, one byevacuation of subdural haematoma only, one bydecompression, and 39 conservatively. The reasonsfor this last line of treatment were poor clinicalcondition, vasospasm, multiplicity of aneurysms,myocardial infarction, pulmonary embolus, andrefusal of operation. In the 15 patients undergoingdirect surgery, the aneurysm was clipped in six,wrapped with muslin and muscle in six, and bothclipped and wrapped in three.The mortality rates were 10-3% for anterior
cerebral artery clipping, 13% for direct surgery,and 69% for conservative management. Afterproximal occlusion, the causes of death were infarc-tion (five), pulmonary embolus (one), and rebleedingdue to lack of obliteration of the clipped vessel (one).In the five deaths from infarction there had beenvasospasm in three cases and very poor cross-flow inone. One patient had internal carotid artery thrombo-sis at postmortem examination. Death after directsurgery was due to infarction and in the conserva-tively managed group was most commonly caused byrecurrent haemorrhage. Of the 61 survivors afterproximal anterior cerebral artery occlusion, 51returned to their usual work and seven to lighterwork, two had a major deficit, and one died later ofpneumonia in an institution. One patient died sevenmonths and one four years later of haemorrhage,although angiography had demonstrated adequateclip closure.
1280
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
ANATOMICAL VARIATIONS IN THE ORIGIN OF THE total of 105 aneurysms, the majority being doublets.POSTERIOR CEREBRAL ARTERY DEMONSTRATED BY Bilateral carotid angiography was carried out in allCAROTID ANGIOGRAPHY, AND THEIR SIGNIFICANCE IN cases but vertebral angiography was not a routineTHE DIRECT SURGICAL TREATMENT OF POSTERIOR investigation. Forty-one operations were carried out
COMMUNICATING ANEURYSMS in 38 patients (operability rate 85%). Seven un-R. P. SENGUPTA (Newcastle upon Tyne) emphasized operated cases died (mortality 27%), and there werethe risk of ischaemic complications after treatment of five deaths in the operated series (mortality 13%).posterior communicating aneurysms either by direct In 15 cases there was doubt about the site of bleeding.surgery or by carotid ligation. It was suggested that The criteria of localization were vessel displacement,some common basic factor underlay these complica- local arterial attenuation, and the relative size of thetions. Thirty patients had been treated by direct aneurysm.clipping of aneurysms and the size of the posterior It was concluded that localization of the site ofcommunicating artery was studied retrospectively on haemorrhage was usually possible, and that if thethe preoperative angiograms. The postoperative fate aneurysms were suitably situated a curative one-of the artery was also examined by angiography. stage or two-stage operation was possible. ThreeAge of the patient, preoperative status, and time of patients had more than one operation and a cure rateoperation after haemorrhage were all studied. The of 24% was achieved. The other survivors wererelation of size of the posterior communicating being observed and occasionally submitted toartery to outcome was as follows: angiography for a check on the size of remaining
aneurysms.
Result In the group of 15 patients where there was diffi-culty in deciding which aneurysm had bled, there
Good Fair Poor Died Total were two deaths (one postoperative), and sevenLarge artery 7 2 2 1 12 radical cures.Small artery 15 1 1 1 18 In the management of these cases it was recom-
mended that clearly defined ruptured lesions shouldbe made safe, that neighbouring unruptured aneur-
The fate of the posterior communicating artery is ysms should be operated upon if appropriate, thatshown below: more than one aneurysm should be excised at a
single operation if the site of bleeding were in doubt,Outcome that more than one operation might be necessary,
and that long term detailed review might be required.ArteryIntactOccludedSevere spasmNot known
Good4
12
Fair
11
Poor
2
Died Total43
1 32
The significantly high rate of poor results withlarge posterior communicating arteries indicatedthat the size of this artery was an important factor inthe production of ischaemic effects. A large posteriorcommunicating artery seen on the angiogram wasregarded as the posterior cerebral artery on that side.
PROBLEMS IN THE MANAGEMENT OF MULTIPLEINTRACRANIAL ANEURYSMS
R. A. C. JONES (Salford) thought that multipleaneurysm cases differed from single aneurysm
patients because of difficulty in locating the site ofhaemorrhage and doubts concerning progress afterincomplete operations. In a series of 205 aneurysm
cases 45 (22%) had more than one aneurysm.
Forty-three of these presented with haemorrhageand two with 3rd nerve palsy. The 45 patients had a
AFFINITY OF CERTAIN STREPTOCOCCI FORTHE CENTRAL NERVOUS SYSTEM
JOHN DE LOUVOIS, PETER GORTVAI, and ROSALINDEHURLEY (London) pointed out that certain strepto-cocci, notably S. pneumoniae, had an affinity for thecentral nervous system. Three recent cases of brainabscess had been found to be due to streptococci andin two the organism was S. milleri. In 374 patientswith serious streptococcal disease it had been foundthat the majority of isolates of S. agalactiae wereassociated with meningitis, and that S. milleri wasassociated with meningitis and brain abscess.Streptococci were shown in a series of controlledexperiments in mice to differ markedly in virulenceaccording to the site of injection. S. agalactiaeinoculated intravenously and intraperitoneally athigh dosage killed all animals by 72 hours. Wheninoculated intracerebrally it killed by 48 hours. S.milleri showed a similar affinity for the centralnervous system when inoculated intracerebrally athigh dosage. S. mutans was lethal at high doses if itwas injected intraperitoneally or intracerebrally. Inlow dosage S. agalactiae still killed all animals
1281
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
within 48 hours after injection into the brain. S.mutans and S. milleri in low dosage killed none.There was therefore a difference both in virulenceand in target affinity in these three streptococcalspecies.
Differentiation of streptococci to group or specieslevel might help the neurosurgeon by enablingpredictions of likely response to antibiotics. Further,if the natural history of brain abscess could beestablished by laboratory studies, the surgeon mightbe able to hazard an informed guess as to the natureof the infecting microbe before culture.
EFFECTS OF AN EXPERIMENTAL WATER SOLUBLE
CONTRAST MEDIUM IN THE POSTERIOR FOSSAOF THE BABOON
I. G. VVYLIE, F. AFSHAR, and T. H. KOEZE (London)emphasized the need for a radiological techniquewhich would demonstrate clearly the fastigium, thefloor of the fourth ventricle, and the dorsal surface ofcervical cord and medulla for the purpose of stereo-taxic surgery. Myodil, emulsified Pantopaque, andConray all had disadvantages. Investigations werecarried out on four anaesthetized baboons usingmetrizamide (Amipaque). In each injection theneedle lay in line with the foramen of Magendie. Theforamen lay vertically below the needle tip, and theviscosity of the medium was at or above a concentra-tion of 300 mg I/ml. Excellent radiographs showingthe necessary detail were obtained. During andimmediately after injection there were no alterationsin EEG, ECG, pulse rate, respiration rate, bloodpressure, or rectal temperature. The duration ofanaesthetic action was prolonged. EEG abnormali-ties and grand mal seizures occurred in three animalsfour to six hours after injection. One of these died,and one had a transient hemiplegia. These baboonshad been anaesthetized with Nembutal, Droperidol,and Fentanyl. A fourth animal anaesthetized withhalothane and nitrous oxide behaved in exactly thesame way as the first three.
It seemed that injections of metrizamine in highconcentration into the fourth ventricle might not befeasible clinically, so, in a fifth baboon anaesthetizedwith halothane, nitrous oxide and intraperitonealbarbiturate, 1 ml of the contrast medium at a con-centration of 300 mg I/ml was injected into alateral ventricle. Good visualization only as far asthe foramen of Magendie was obtained. This animaldid not have seizures. The investigation was pro-ceeding.
COMPUTERIZED AXIAL TOMOGRAPHY WITH THEEMI SCANNER-EARLY AND FRUITFUL EXPERIENCE
IN PAEDIATRIC NEUROSURGERYKENNETH TILL (London) had found computerized
axial tomography especially valuable in childrenbecause of absence of need for general anaesthesia,short duration (41 to 20 minutes), ease of repetition,no necessity for injections, possibility of outpatientinvestigation, and very low exposure to irradiation.Examples of cases in which it had been possible tomake important decisions with a minimum of dis-turbance to the child were given. The desirability ofavoiding disturbing and hazardous investigationbefore a decision not to operate was stressed. Thefollowing illustrations of EMI scan diagnosis weregiven:
1. A boy with a left hypotonic hemiparesis and calci-fication in the left internal capsule and thalamus wasdiagnosed as having an inoperable pineal teratoma.
2. A girl with a craniopharyngioma was shown to havea very large solid tumour with no ventricular enlargementand it was decided to treat with radiotherapy.
3. The son of parents who suffered from migrainepresented with episodes of hemiparesis, and headache.The parents' opposition to angiography was countered bythe demonstration of a frontotemporal mass.
4. Three years after operation and radiotherapy forcerebellar ependymoma a boy developed mild upper limbataxia. The necessity of reoperation was shown by thedemonstration of a cerebellar mass.
5. In two cases cerebellar tumours were so clearlydemonstrated that operation was performed without anyother investigations. One child had a cerebellar hemi-sphere astrocytoma, and the other had a vermis medullo-blastoma.
6. A boy of 13 who had been treated in infancy forhydrocephalus with a ventriculocardiac shunt developedmild headache. There was no sign of raised intracranialpressure but the scan showed grossly enlarged ventriclesindicating that shunt revision was necessary.
7. Excision of an optic nerve tumour from a girl withan enlarged optic foramen was carried out because thescan showed that the tumour had not extended to thechiasm.
AQUEDUCT STENOSIS IS A RESULTOF HYDROCEPHALUS1
BERNARD WILLIAMS (Birmingham) said that aqueductstenosis could cause hydrocephalus but it was pos-sible that aqueductal closure or narrowing mightoccur as a result of hydrocephalus. In some cases inthe past aqueduct stenosis might have been wronglyblamed as the cause of hydrocephalus to which itcontributed only in the final stages. From the secondmonth of fetal life until birth the aqueduct was com-
pressed from outside by the cerebral hemispheres. Ifthe ventricles were distended, excessive aqueductalnarrowing might follow.The facts about nontumoural stenosis of the
aqueduct could be explained on the basis that
1 This paper needs to be read in full for the authors' argu-ment to be understood and appreciated.
1282
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from
Proceedings of the Society of British Neurological Surgeons
hydrocephalus from any cause distal to the aqueductacting in early life might cause the lateral ventriclesto enlarge and displace the tentorium and the hind-brain downwards. Thereafter, compression of themidbrain between the hemispheres might occur,aggravating the normal tendency of the aqueduct tobecome narrowed during intrauterine life. If thehydrocephalus was not too severe, and becamecompensated, so enabling the fetus to live, thensubsequent decompensation might occur after birth,in infancy, childhood, or adult life, by blockagewhich appeared to be at the aqueduct alone.
BRAIN ANTIGEN RELEASE INTO THE PERIPHERAL
BLOOD OF PATIENTS WITH HEAD INJURIES
D. G. T. THOMAS (Glasgow) considered the difficultyof early prognosis in severe head injuries. In experi-mentally induced brain injuries, synaptic vesicleantigens had been found in the cerebrospinal fluid,and pulmonary embolism by fragments of braintissue had been recorded. Brain antigens had beenfound in the sera of patients with neurologicaldisease. It seemed worthwhile to investigate thepossible existence of brain antigens in peripheralblood after head injury. Antisera were produced byinjection of grey and white cerebral tissue fromcraniotomies into mice. Patients' sera were tested forbrain antigen using absorbed antisera by Ouchter-lony's double diffusion method.
Brain antigen was found in the serum of 22 of 36patients (63%) with severe blunt head injuries. It waspresent in two out of 15 patients (13%) with otherbrain damage and in none of 24 healthy medicalstudents who formed a control group.Of the 22 head injured patients with antigen in the
serum, 10 died, and only one made a good recovery.Of the 14 patients with no brain antigen in the serum,eight made a good recovery, two were disabled at onemonth, and four died, but only two of these deathswere directly attributable to brain injury. Applica-tion of Fishers' Exact Test showed significant corre-lation between presence of brain antigens in serumand death or persisting brain damage.
EPENDYMOMAS IN CHILDHOODR. A. COULON and NORMAN GRANT (London) reviewed43 cases of intracranial ependymoma. These repre-sented 6% of the total number of intracranialtumours treated over an 18 year period. Thirteenwere supratentorial and 30 in the posterior fossa.The average age for benign lesions was 7 years andfor malignant lesions 3 5 years. The duration of thehistory averaged nine to 10 months in the benigncases and three to four months in the malignantones. Vomiting and headaches were common.
Personality changes were frequent. In the veryyoung, retardation or developmental regressionoccurred. Unsteadiness of gait was common withposterior fossa lesions. Signs were papilloedema in67%, increase in head circumference above the 90thpercentile in 37%/, abnormal skull percussion notein 51%, stiff neck in 23%o, ataxia in 350, hemi-paresis in 19%, and marked meningeal signs in onecase. Skull radiographs were abnormal (suturediastasis, sellar changes, pathological calcification)in 7400. Tumour cells were found in cerebrospinalfluid from five cases.Of the 13 supratentorial lesions, three had burr-
hole biopsy only, and 10 had craniotomies. One ofthe burrhole biopsy cases and one craniotomy died inhospital. The surviving craniotomy cases and onebiopsy case had radiotherapy.Of the 30 infratentorial tumours, one died before
operation and 29 had attempted maximal removal,the aim being at least to unblock the 4th ventricle.Seven of these children died in hospital, and oneshortly after discharge. The 21 survivors had radio-therapy.Of 13 supratentorial operation cases, two died in
hospital (operative mortality 150%). Three year sur-vival was 3000 (three out of 10). No child had yetlived five years, but four might do so. Three yearsurvival in the radiotherapy series was 4300 (threeout of seven).Of 30 infratentorial tumours, seven were operative
deaths (23%). Three year survival was five out of 26(190%), and five year survival was 12%. Three yearsurvival after radiotherapy was five out of 17 (29%4),and five year survival three out of 16 (19%)0No child with a malignant lesion had survived
beyond the second year after operation.
SIR BERNARD KATZ, FRS (Department of Biophysics,University College, London) gave a lecture on 'TheMolecular Effect of the Neuromuscular Trans-mitter'.
CONTINUOUS MEASUREMENT OF DIFFERENTIAL CSF
PRESSURES ACROSS THE TENTORIUMS. R. SONI (Swansea) described a method for continu-ous and simultaneous comparison of ventricularfluid pressure and the difference between ventricularand cisterna magna pressure by means of two radio-telemetric transducers. Raised intracranial pressurewas likely to be of immediate serious consequenceonly if differential pressures in various compartmentsled to brain shifts. There was an impression thatconing results if the ventricular pressure exceededthat in the cisterna magna by 100 mm water.
Differential pressure measurements were made on13 occasions in 12 patients with raised intracranial
1283
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from
Proceedings of the Society of British Neurological Surgeons
pressure. Continuous recordings were made forbetween two and 18 hours.
Despite large recorded differences between ven-tricular and cisternal pressure, only one patient hadtentorial herniation. High differential pressure couldbe reduced to zero by ventricular aspiration.Mannitol reduced pressure, especially in the supra-tentorial compartment. Differential wave formswere seen in some cases.
This investigation was the first in which a differen-tial transducer had been used and showed that adifference of 165 mm water pressure across thetentorium was compatible with life and did notindicate that tentorial herniation had occurred.
Further work was necessary to determine theplace of differential measurements in clinicalpractice.
FRONTAL LOBE LESIONS FOR DEPRESSIVE ILLNESSRAYMOND NEWCOMBE (London) had found that indepressive illness the lower medial quadrants of thefrontal lobes were the usual target areas for leucot-omy. These involved the amygdalothalamic-orbitalcircuits of the limbic systems and regions of con-vergence of the somatosensory cortical activity onthe visceral brain. Experience of orbital undercutsafter previous rostral procedures had indicated thebeneficial effects of the deeper parts of these lesions.A stereotaxic tractotomy operation was employed.The target position for introduction of yttrium seedswas determined in the lateral radiograph by refer-ence to the plane passing through the orbital rooflaterally and the tuberculum sellae, and the planeperpendicular to the latter. Six seeds were insertedon each side. From the average brain outline it wasseen that the lesions usually lay anteroventral to thestriatum. These conclusions received support frompostmortem studies in seven patients who died fromintercurrent disease. Small lesions in the ventral partof the head of the caudate nucleus caused temporaryconfusion or lethargy. It was concluded that smallplanar lesions of about 1 ml volume anteroventral tothe striatum might relieve intractable depression.These lesions need not extensively involve the pro-jection from the dorsomedial nucleus of the thalamus,neither need they extend posteriorly to isolate theagranular orbital cortex or enter the substantiainnominata of Reichert.
CLINICAL SIGNIFICANCE OF MESIAL TEMPORAL(AMMON'S HORN) SCLEROSIS IN EPILEPSY
MURRAY A. FALCONER (London) drew attention tothe involvement of the amygdala, hippocampalgyrus, and uncus in Ammon's horn sclerosis. Thelesion usually resulted from a severe febrile convul-sion in infancy. Surgery for epilepsy gave its best
results when mesial temporal sclerosis was found.Suitable patients for operation were those with drug-resistant temporal lobe epilepsy, with exclusion byneuroradiology of space-occupying lesions, and withEEG evidence of focal spike discharges confined toor, if bilateral, predominant on the side chosen forresection. Three hundred patients had undergoneoperation with two deaths, one in the first case of theseries, and one due to pulmonary embolism. Halfthe patients had mesial temporal sclerosis, a fifth hadhamartomas, a tenth had scars and infarcts, and theremainder had no definite neuronal pathology.Fifty to 60% of cases of mesial temporal sclerosiscould be rendered fit-free. An olfactory or gustatoryaura usually pointed to a diagnosis of tumour orhamartoma. In 30 to 40%/a of patients with mesialtemporal sclerosis a history of a febrile convulsionlasting at least half an hour could be obtained. Afamily history of epilepsy was also frequent. Almostall the patients had a remembered aura or psycho-motor seizures. Some had also had grand mal orabsence types of seizure. Dysphasia was of greatlocalizing value, and intracarotid sodium amylo-barbitone tests were less and less frequently used.Radiologically there might be relative smallness ofthe middle fossa on the affected side, and a collateraleminence might be visible in the temporal horn.Spike discharges on the EEG were usual. Lack ofbarbiturate induced fast activity usually pointed tomesial temporal sclerosis but sometimes to hamar-toma. If depth electrodes in the hippocampus andamygdala showed EEG silence or uncal activityonly, mesial temporal sclerosis was the likelypathology. Injury potentials or spike dischargespointed to other types of lesion.The importance in prophylaxis of prompt and
vigorous treatment of febrile convulsions in infancywas emphasized. In Copenhagen a reduced incidenceof habitual epilepsy was believed to be following adetermined effort to treat infantile convulsions earlyand effectively.
CONTROL OF INCONTINENCE DUE TO THEUNINHIBITED BLADDER BY SELECTIVE SACRAL
NEURECTOMYMICHAEL J. TORRENS and HUW B. GRIFFITH (Bristol)studied 304 incontinent patients in 48% of whomthere were uninhibited bladder contractions. Physio-logical assessments of the effects of sacral rootblocks and selective sacral root sections on bladderand sphincter functions had been made. Seventeenpatients underwent bilateral selective nerve blocks ofthe S2-S4 roots. After assessment by cystometry,pressure flow analysis, and urethral pressure record-ing, nine were selected for sacral neurectomy.Blocking the S3 nerve root seemed effective in
1284
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
increasing bladder capacity and reducing uninhibitedactivity. S4 blocking resulted in an increase inresting sphincter pressure. Operation consisted ofnerve root exposure by means of limited sacrallaminectomy. Intraoperative nerve root stimulationproduced sustained tonic bladder contraction. Thelevel for neurectomy was selected by combining theinformation from preoperative nerve blocks andintraoperative nerve stimulation. The S3 roots werecut in eight cases and the S4 roots in one. Cysto-metrogram capacity was increased in six patients.Average volume voided became greater in fourcases. Maximum volume voided was significantlyincreased. Uninhibited bladder activity became lessin eight patients. Resting urethral sphincter tonewas insignificantly increased. Urinary flow rate rosein most cases. Enuresis was cured in two cases,substantially improved in four, and unchanged inthree. Urinary frequency tended to improve.Urge incontinence was cured in six patients. None
of the four male patients had changed sexual potency.There was no significant disturbance of bowelfunction.
It seemed that the best results followed bilateralsacral neurectomy at one level, usually S3. Suitablepatients for operation were those with urge inconti-nence, reflex incontinence, or enuresis where con-servative treatment had failed. Urodynamic assess-ment should confirm uninhibited bladder activity,absence of sphincter weakness and outflow obstruc-tion, and show intact sensation. A potential func-tional capacity of 400 ml should be demonstrated.
OPERATION FOR REINNERVATION OF URINARYSPHINCTERS IN CONGENITAL OR POST-TRAUMATIC
PARAPLEGICSH. A. MASLOWSKI (Manchester) had operated on fourinfants with paraplegia due to meningomyeloceles.S3-S4 nerve roots were detached from the neuralplates and joined to nerve roots to the lesion, eitherdirectly or by using sacrificed nerve roots to closegaps. It was thought that unilateral operation shouldbe sufficient. The first anastomosis was performedfour years ago using silk sutures and sleeves, but theoperation was difficult and unsuccessful, so in theother three cases a spot-glue technique using L-ethyl-cyanoacrylate had been employed. The outcome wasexpected to be satisfactory in the last two cases.The operation should be suitable for adults with
post-traumatic paraplegia where the lesion wasbetween the midthoracic level and the conus. Ahemilaminectomy at one or two levels should besufficient. One or two sacrificed cauda equina nerveroots could be used to bridge the gaps between theS3-S4 nerve roots (sectioned close to the cord) androots just above the level of the lesion. Alternatively,
freeze dried and irradiated cadaver allografts couldbe employed in combination with immunosuppres-sive therapy.
C. A. Carlsson and T. Sudin had had a satisfactoryfunctional result after anastomosing the S1-S2 rootsto the TIO-Tl roots in a four year old girl withmeningomyelocele and paraplegia.
SPASMODIC TORTICOLLISL. S. WALSH (London) had treated 25 men and 21women with spasmodic torticollis over a period of 17years. Pain was usually due to cervical spondylosis.Three patients developed myelopathy. Only twopatients had spontaneous remissions. Thirty-threehad torticollis, five had retrocollis, and six hadtorticollis associated with other involuntary move-ments. It was thought that the condition was organic-ally determined. In five patients significant headinjury had preceded the onset of the disorder, onehad a parietal lobe abscess four years previously,one had Sydenham's chorea in childhood, and onehad choreoathetosis 30 years before the onset oftorticollis. Another had an influenza-like illnessimmediately beforehand, and one patient laterdeveloped Huntington's chorea.
Six patients were treated by section of the acces-sory nerve in the neck, and two of these showed someimprovement.Three underwent bilateral stereotaxic operations.
All developed dysarthria, and abnormal movementsreturned to some extent in one.
Six unilateral thalamotomies were performed. Inonly one case was there benefit from the procedure.
Thirty-three patients had been treated by cervicalrhizotomy, including three who had previously hadunsuccessful thalamotomies. The operation con-sisted of division of the upper four cervical motorroots on the side to which the head moved and of theupper three roots on the other side. On both sidesthe spinal accessory nerve was cut intrathecally atthe Cl level and connections between the nerves andthe first cervical roots were divided. On the side ofsternomastoid spasm the accessory nerve was cut inthe neck, sparing the fibres to the trapezius muscleif possible, whenever the intrathecal operation hadnot stopped the sternomastoid contractions. In 26cases the results had been satisfactory. Of the re-maining seven, one died of pulmonary embolism,one died of myocardial infarction, one was relievedof torticollis but had a deformed neck due to muscleweakness, one was disabled by Huntington's choreawhile being cured of torticollis, and three had norelief. The 26 patients who were improved had noinvoluntary movements but had some stiffness of theneck. Ten had some dysphagia. Some had ache in
1285
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
the neck and a few had difficulty in raising one orboth arms at the shoulder.
DORSAL COLUMN STIMULATION:AN INITIAL EXPERIENCE
G. CORKILL, 0. W. ALBRAND, and J. R. YOUMANS(Davis, California) pointed out that chronic benignpain did not always respond to the classical painoperation. The 'gate theory' of pain perceptioncalled for modulation in the dorsal horn area of theamount of centrally transmitted pain signals.Inhibition of the transmitter cell by the substantiagelatinosa was the anatomical basis. Alpha and betafibre activity enhanced the inhibition. Gamma anddelta fibre activity decreased the inhibitory effect ofthe substantia gelatinosa and allowed more painimpulses to reach consciousness after passing throughthe transmitter (or T) cell gate. Stimulation of thebeta fibres in the posterior columns had beenemployed by several investigators in the manage-ment of pain.Nine patients with intractable pain had undergone
12 operations. A foot plate was implanted on thedorsal columns in the subarachnoid space and con-nected by a subcutaneous wire to a radio receiverimplanted beneath the skin in the right mid-clavicularline. The patient applied a radiofrequency trans-mitter to the skin over the receiver when necessary.
All the patients were relieved of pain. Onedeveloped paraplegia six hours after surgery, and atreoperation was found to have a swollen cord.
It was concluded that all patients needed extensivescreening before operation, that the foot plate shouldnot be inserted between the T4 and T8 levels wherethe canal was narrow, that arachnoiditis contra-indicated operation, that steroids should be em-ployed, that intensive postoperative care was neces-sary, and that the patient should be flat for three daysafter operation to minimize the risk ofCSF leakage.
Further research into technical improvements wasproceeding.
ASSESSING AND RECORDING 'CONSCIOUS LEVEL'G. M. TEASDALE, R. KNILL-JONES, and w. B. JENNETT(Glasgow) had found little consistency betweenvarious systems of describing patients with impairedconsciousness. Unstructured observations result inambiguities and misunderstandings, when it comesto exchanging information about patients. A systembased on best motor response, verbal response, andeye opening, was devised.The best motor response varied for obeying com-
mands (best response possible), through localizingresponse, flexion responses, and extensor posturing.Verbal responses were graded from orientation downthrough confused conversation, and inappropriate
verbal responses, to incomprehensible sounds. Eyeopening was recorded as provoked spontaneously onapproach of the observer, in response to speech, orafter the application of a painful stimulus.
Observer consistency was investigated and anaverage rate of disagreement of one in 10 was foundin a group of nurses, neurosurgeons, and generalsurgical trainees.The need for defining consciousness and coma in
absolute terms was avoided. The system had themerit of simplicity, making it appropriate for use byrelatively inexperienced staff.
CONGENITAL ATRESIA OF THE FORAMINA OF LUSCHKAAND MAGENDIE, WITH ABSENCE OF THE CEREBELLAR
VERMIS AND CORPUS CALLOSUM IN AN ADULTR. E. RAMIREZ (Haywards Heath) described the caseof a 29 year old woman with a short history of head-ache, nausea, vomiting, and dizziness. Physical signswere bilateral papilloedema, gross horizontal jerknystagmus, left hypotonia, and slight incoordinationof left arm movements. Radiologically there wasthinning of the skull vault and of the dorsum sellae.The electroencephalogram was moderately abnormalwith dominant beta activity accentuated by hyper-ventilation. Slow activity was not attenuated by eyeopening. A brain scan showed a high position of thetorcular. Left carotid angiography revealed evi-dence of a posterior fossa space occupying lesionwith forward displacement of the deep cerebral veinsand of the occipital lobes. A vertebral angiogramshowed an avascular mass displacing the cerebellumforwards.
Posterior fossa exploration revealed a distendedfourth ventricle, and absence of the cerebellarvermis. A ventriculoatrial shunt was established laterbecause of persistently high posterior fossa pressure,but the patient died two months after the first opera-tion.At necropsy the brain was found to be hydro-
cephalic, with a cyst between the cerebellar hemi-spheres and having the floor of the fourth ventricleas its base. The cerebellar vermis, corpus callosumand septum lucidum were absent.
This case was considered to be an example of mal-development of midline structures, with involvementof both cerebrum and cerebellum.
CERVICAL SPINAL INTERBODY FUSIONWITH KIEL BONE
P. S. RAMANI, R. M. KALBAG, and R. P. SENGUPTA(Newcastle upon Tune) had used iliac crest auto-grafts for spinal fusion by the Cloward technique, buthad abandoned the technique in 1968 because ofcomplaints of pain at donor sites, and had turned toprocessed animal bone from calves for grafts.
1286
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from

Proceedings of the Society of British Neurological Surgeons
Traction had been applied during operation andpatients had been discharged to their homes on thefifth postoperative day unless they had required pro-longed treatment for paraparesis.
Complications noted were anterior protrusion ofgraft (17 cases), partial absorption of dowel (fourcases), retropharyngeal abscess (one case), partialresorption of vertebral bodies (three cases), fractureof adjacent vertebral bodies (two cases).
Fifty-five cases out of the 65 submitted to surgeryshowed satisfactory alignment of the spine withoutabnormal mobility in flexion or extension. In no casecould it be said with confidence that bony fusion hadoccurred. Only six cases were considered to be fail-ures despite the seemingly long list of complications.
OPTIC NERVE COMPRESSION BY THE OPHTHALMICARTERIES IN CASES OF PITUITARY ADENOMA
P. R. R. CLARKE (Middlesbrough) described twocases of chromophobe pituitary adenoma with visualfailure in which local pressure effects exerted by theophthalmic arteries had been noted.A 53 year old man with hypopituitarism and a pituitary
tumour presented with recent visual deterioration in theright eye only, a visual acuity on the right of 6160, a
central temporal field defect, and a filling impairmentbelow the right optic nerve as seen on pneumoencephalo-graphy. At operation a considerable quantity of the aden-oma was removed, and it was noted that the right opticnerve was elevated over the ophthalmic artery whichpassed under it from the lateral to the medial side. Theprocessus falciformis, which was tightly applied to theupper surface of the nerve, was divided. After operationthe visual acuity improved to 6/18.A 46 year old man, who had multiple sclerosis, de-
veloped a chromophobe pituitary adenoma, centraltemporal visual field defects, and deterioration in vision to6/36 in each eye. Pneumoencephalography showed thatthere was a considerable suprasellar extension of tumour.At right frontal craniotomy it was seen that the rightophthalmic artery ran from lateral to medial under thenerve and was splitting the nerve at its centre so that theartery was visible in the middle of the optic nerve. Theprocessus falciformis was divided, and as much aspossible of the adenoma was removed. Postoperativelyvisual acuity did not improve.
It was pointed out that the ophthalmic artery didsometimes run medially beneath the optic nervebefore entering the optic canal, and that the pro-cessus falciformis might produce pressure on thenerve from above.
1287
guest. Protected by copyright.
on March 15, 2022 by
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.37.11.1277 on 1 Novem
ber 1974. Dow
nloaded from