radiographic evaluation of arthritis:...
TRANSCRIPT

Radiographic Evaluation ofArthritis: Inflammatory Conditions1
Jon A. Jacobson, MDGandikota Girish, MDYebin Jiang, MD, PhDDonald Resnick, MD
In the presence of joint space narrowing, it is important todifferentiate inflammatory from degenerative conditions.Joint inflammation is characterized by bone erosions, os-teopenia, soft-tissue swelling, and uniform joint space loss.Inflammation of a single joint should raise concern forinfection. Multiple joint inflammation in a proximal distri-bution in the hands or feet without bone proliferationsuggests rheumatoid arthritis. Multiple joint inflammationin a distal distribution in the hands or feet with boneproliferation suggests a seronegative spondyloarthropa-thy, such as psoriatic arthritis, reactive arthritis, or anky-losing spondylitis.
� RSNA, 2008
1 From the Department of Radiology, University of Michi-gan Medical Center, 1500 E Medical Center Dr, TC-2910L, Ann Arbor, MI 48109-0326 (J.A.J., G.G., Y.J.); andDepartment of Radiology, University of California SanDiego VA Hospital, La Jolla, Calif (D.R.). Received Decem-ber 11, 2006; revision requested February 7, 2007; revi-sion received July 25; accepted August 20; final versionaccepted November 1; final review by J.A.J. Addresscorrespondence to J.A.J. (e-mail: [email protected] ).
� RSNA, 2008
REVI
EWS
AND
COM
MEN
TARY
�RE
VIEW
FOR
RESI
DENT
S
378 Radiology: Volume 248: Number 2—August 2008
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.

Radiography is typically the firstimaging study in evaluation for ar-thritis. On radiographs, one criti-
cal assessment is differentiating inflam-matory arthritis from a degenerativeprocess, because the treatment optionsare quite different. Identification of aninflammatory joint due to infection oftenrequires diagnostic aspiration followedby administration of antibiotics and pos-sible surgical drainage and lavage. Withregard to systemic arthritides, withearly diagnosis there are several typesof medications used to control joint in-flammation and even prevent or reducesubsequent joint destruction. The treat-ment options for a degenerative processinclude medication, joint injection, and,later, joint replacement.
The objective of this review is topresent a simplified approach to radio-graphic evaluation of arthritis (Fig 1).This is presented as an algorithm thatuses joint space narrowing of the distalextremities as a starting point. While itis acknowledged that it is nearly impos-sible to include all types of arthritis inone simple algorithm, and that there arealways exceptions and variations, thisapproach will encompass the most com-mon features of the frequently seen ar-thritides and can be viewed as a frame-work for radiographic evaluation. This
algorithm does not include substantialdetail of each topic but rather focuseson radiographic findings that, with theuse of this algorithm, lead to a final andusually correct diagnosis. The first criti-cal step in the algorithm is to determineif joint space narrowing detected withradiography is related to an inflamma-tory or a degenerative condition.
Inflammatory versus DegenerativeJoint Disease
There exist essential radiographic find-ings that are common to inflammatoryarthritis due to any cause. The hallmarkof joint inflammation is erosion of bone.This will initially appear as a focal dis-continuity of the thin, white, subchon-dral bone plate (Fig 2). Normally, thissubchondral bone plate can be seeneven in cases of severe osteopenia,whereas its discontinuity indicates ero-sion. Although it is true that periarticu-lar osteopenia and focal subchondral os-teopenia can appear prior to a truebone erosion, it is the presence of boneerosion that indicates definite joint in-flammation. As the bone erosion en-larges, osseous destruction extends intothe trabeculae within the medullaryspace.
One important feature of inflamma-tory arthritis relates to the concept of amarginal bone erosion. This term isgiven to bone erosion that is located atthe margins of an inflamed synovialjoint. This specific location representsthat portion of the joint that is intraar-ticular but not covered by hyaline carti-lage; therefore, early joint inflammationwill produce marginal erosions prior toerosions of the subchondral bone platebeneath the articular surface (Fig 3).When looking for bone erosions, multi-ple views of a joint are essential to pro-file the various bone surfaces.
A second important characteristicof an inflammatory joint process is uni-form joint space narrowing. This occursbecause destruction of the articular car-tilage is uniform throughout the intraar-ticular space. A third finding of inflam-matory joint disease is soft-tissue swell-ing.
There are essential radiographic
features of a degenerative joint, as well.In addition to lack of the findings de-scribed for inflammatory joint disease,degenerative findings include osteo-phyte formation and bone sclerosis(Fig 4). Although underlying cartilagedamage is presumed, joint space nar-rowing does not involve the joint uni-formly, as is seen with inflammatoryjoint disease, and osteophytes are typi-cally present. As the joint space nar-rows, the osteophytes become larger,sclerosis increases, and subchondralcysts—or geodes—may be seen. If de-generative joint disease involves a syno-vial articulation, the term osteoarthro-sis or osteoarthritis is appropriate.
Inflammatory Arthritis
Septic ArthritisOnce joint space narrowing and fea-tures of inflammatory arthritis are iden-tified, the next step in the algorithm is todetermine how many joints are in-volved. Multiple joints may be involvedin as many as 20% of cases (1). If jointinflammation is limited to a single joint,infection must first be carefully ex-cluded (Fig 1). The cause of septic ar-thritis is usually related to hematoge-nous seeding owing to staphylococcal orstreptococcal microorganisms.
The radiographic features of a sep-tic joint encompass those of any inflam-matory arthritis—namely, periarticularosteopenia, uniform joint space narrow-ing, soft-tissue swelling, and bone ero-sions (Fig 5). Not all findings may bepresent simultaneously, and, acutely,bone erosions may not be evident. Fur-thermore, the joint space may be ini-tially widened owing to the effusion.Joint space widening may also be seenwith more indolent and atypical infec-tions, such as those related to tubercu-losis and fungal agents; but, again, otherinflammatory changes are typically present
Published online10.1148/radiol.2482062110
Radiology 2008; 248:378–389
Authors stated no financial relationship to disclose.
Essentials
� It is important to differentiate in-flammatory from degenerativecauses of joint space narrowing.
� Inflammatory arthritis is charac-terized by bone erosions, osteope-nia, soft-tissue swelling, and uni-form joint space narrowing.
� With monoarticular joint inflam-mation, it is important to excludeinfection.
� Inflammation that involves multi-ple joints in a proximal distribu-tion of the hands or feet withoutbone proliferation suggests rheu-matoid arthritis.
� Inflammation that involves multi-ples joints in a distal distributionof the hands or feet with boneproliferation suggests a seronega-tive spondyloarthropathy.
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 379

(Fig 6). The Phemister triad describesthese findings classically seen in tuber-culous arthritis: juxtaarticular osteope-nia, peripheral bone erosions, and grad-ual narrowing of the joint space (2).
Rheumatoid ArthritisIf joint space narrowing and other ra-diographic findings of inflammatory ar-thritis involve multiple joints, a systemicarthritis must be considered. The nextstep in the algorithm is evaluation of thehands and feet. Proximal distribution atthese sites and lack of bone prolifera-tion suggest the diagnosis of rheumatoidarthritis. Rheumatoid arthritis is mostcommon in women aged 30–60 years.Serologic markers such as rheumatoidfactor and antibodies to cyclic citrulli-nated peptide are important indicatorsof rheumatoid arthritis (3,4).
The radiographic features of rheu-matoid arthritis are those of joint in-flammation and include periarticularosteopenia, uniform joint space loss,bone erosions, and soft-tissue swelling(Fig 7). Because of the chronic nature ofthe inflammation, additional findingssuch as joint subluxation and subchon-dral cysts may also be evident. Althoughthe radiographic findings are not spe-cific for one condition, the proximal dis-tribution of joint involvement in thehands and feet and the lack of boneproliferation suggest rheumatoid arthri-tis.
In the hands, target sites of rheu-matoid arthritis include the metacar-pophalangeal, proximal interphalan-geal, midcarpal, radiocarpal, and dis-tal radioulnar joints, with predilectionfor the ulnar styloid process (Figs 7,8). Involvement is usually bilateral andfairly symmetric, although isolatedcarpal joint involvement may occur.Ulnar deviation occurs at the metacar-pophalangeal joints. Hyperextensionat the proximal interphalangeal jointswith flexion at the distal interphalan-geal joints results in a swan neck de-formity, while flexion at the proximalinterphalangeal joint and hyperexten-sion at the distal interphalangeal jointresults in a boutonniere deformity. Itis important to profile the bone corti-ces with multiple radiographic views
to identify cortical discontinuity. If around subchondral lucency does notinterrupt the bone surface, possibili-ties include a subchondral cyst or anerosion viewed en face.
In the feet, target sites of rheuma-toid arthritis include the metatarsopha-langeal, proximal interphalangeal (in-cluding the first interphalangeal), andintertarsal joints, and such involvement
Figure 1
Figure 1: Flow chart shows approach to radiographic evaluation of arthritis. Algorithm begins with jointspace narrowing and initially uses differentiation between inflammatory and degenerative findings to reach thefinal diagnosis.
Figure 2
Figure 2: (a, b) Posteroanterior wrist radiographs show discontinuity of bone cortex representing erosion(arrow) with development of osteopenia. Note progression of disease from a to b.
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
380 Radiology: Volume 248: Number 2—August 2008

is commonly bilateral and nearly sym-metric in distribution (Fig 9). It is im-portant to closely evaluate the lateralaspect of the fifth metatarsal head, be-cause this is often the first site of a boneerosion in the foot and, at times, suchinvolvement occurs prior to hand orwrist involvement (Fig 10). Becauserheumatoid arthritis is a disease thataffects synovium diffusely, other sites ofinvolvement include tendon sheaths and
bursae such as the retrocalcaneal bursa.Loss of the normal radiolucent trianglebetween the posterosuperior margin ofthe calcaneus and the adjacent Achillestendon suggests the presence of bursalfluid, with subjacent calcaneal erosionsindicating inflammation (Fig 11).
Other peripheral joints may also beinvolved in rheumatoid arthritis, withsimilar findings. Joint involvement in-cludes the knees (Fig 12), the hips
(Fig 13), and the sacroiliac and glenohu-meral joints, with involvement of thelast of these often associated with ahigh-riding humeral head related to alarge rotator cuff tear. Spinal involve-ment is also possible. At the C1-C2 ar-ticulation, the odontoid process may beeroded, and the anterior atlantodens in-terval may be abnormally widened (�3mm in adults), especially with neck flex-ion (Fig 14) (5).
Figure 3
Figure 3: (a) Illustration of synovial joint shows joint fluid (f) and articular cartilage (c). (b) Illustration and (c) radiograph show inflammatory arthritis, synovitis, andpannus (P) causing cartilage destruction. Marginal erosions (arrows) are seen where subchondral bone plate is exposed to intraarticular synovitis. f � Fluid.
Figure 4
Figure 4: Osteoarthritis. Posteroanterior radio-graph shows interphalangeal joint space narrow-ing, subchondral sclerosis, and osteophyte forma-tion (arrows).
Figure 5
Figure 5: Septic arthritis.(a) Posteroanterior and(b) oblique radiographs show jointspace narrowing (arrows), os-teopenia, soft-tissue swelling, anda bone erosion (arrowhead).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 381
Seronegative SpondyloarthropathiesReturning to the proposed algorithm, if oneobserves joint space narrowing, signs of in-flammation,multiple joint involvement, anddistal involvement in the hands and feetwith added features of bone proliferation, aseronegative spondyloarthropathy is sug-gested. This category includes psoriatic ar-thritis, reactive arthritis, and ankylosing
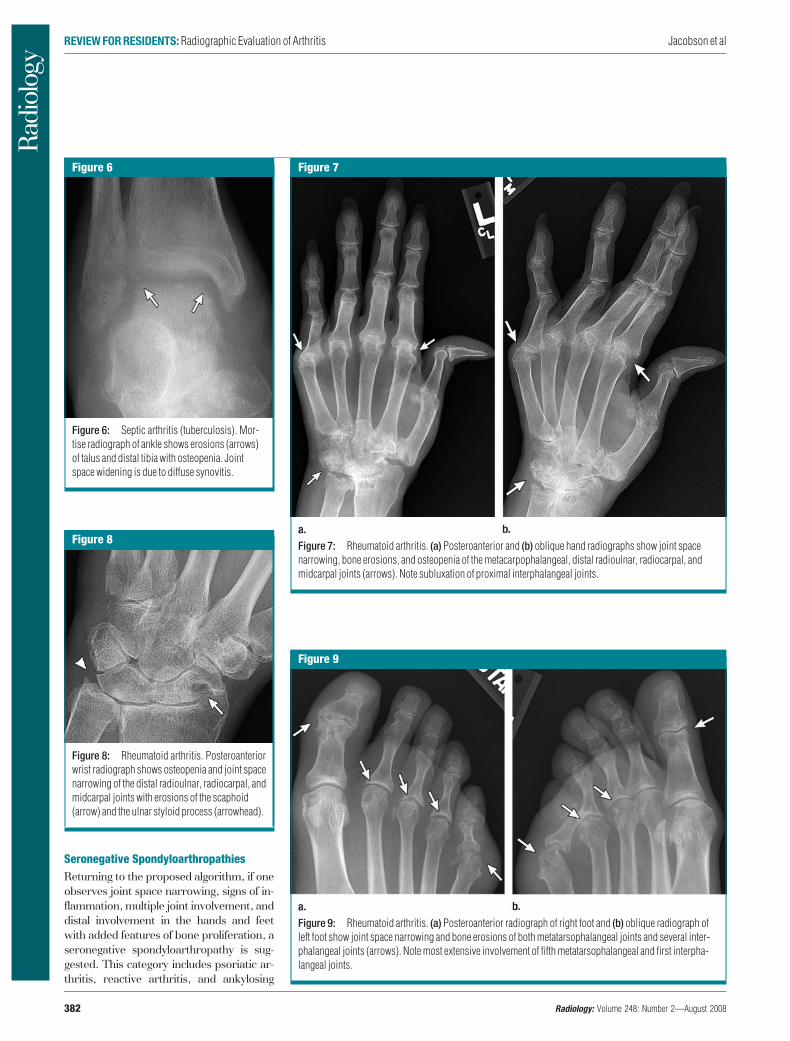
Figure 6
Figure 6: Septic arthritis (tuberculosis). Mor-tise radiograph of ankle shows erosions (arrows)of talus and distal tibia with osteopenia. Jointspace widening is due to diffuse synovitis.
Figure 7
Figure 7: Rheumatoid arthritis. (a) Posteroanterior and (b) oblique hand radiographs show joint spacenarrowing, bone erosions, and osteopenia of the metacarpophalangeal, distal radioulnar, radiocarpal, andmidcarpal joints (arrows). Note subluxation of proximal interphalangeal joints.
Figure 8
Figure 8: Rheumatoid arthritis. Posteroanteriorwrist radiograph shows osteopenia and joint spacenarrowing of the distal radioulnar, radiocarpal, andmidcarpal joints with erosions of the scaphoid(arrow) and the ulnar styloid process (arrowhead).
Figure 9
Figure 9: Rheumatoid arthritis. (a) Posteroanterior radiograph of right foot and (b) oblique radiograph ofleft foot show joint space narrowing and bone erosions of both metatarsophalangeal joints and several inter-phalangeal joints (arrows). Note most extensive involvement of fifth metatarsophalangeal and first interpha-langeal joints.
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
382 Radiology: Volume 248: Number 2—August 2008

spondylitis. Differentiation among thesedisorders largely relies on the distributionof radiographic abnormalities and clinicalinformation. In addition, other findings thathelp differentiate the seronegative spondy-loarthropathies from rheumatoid arthritisare that cartilaginous joints and enthesesare involved to a greater extent, the latterrepresenting the osseous attachment sitesof ligaments and tendons. Entheseal in-volvement leads to increased density andirregular bone proliferation.
Psoriatic arthritis.—The cause ofpsoriatic arthritis is considered to be a com-
bination of environmental and hereditaryfactors, with as many as to 60% of patientsbeing HLA-B27 positive (6). Approximately10%–15% of patients with skin manifesta-tions of psoriasis will develop psoriatic ar-thritis (6). Usually such manifestations willprecede the development of arthritis. Thehallmarks of psoriatic arthritis, similar to
those of the other seronegative spondyloar-thropathies, are signs of inflammatory ar-thritis combined with bone proliferation,periostitis, enthesitis, and a distal joint dis-tribution in the extremities (Fig 15).
In the hands, wrists, and feet, a dis-tal distribution is characteristic. Find-ings may be bilateral or unilateral and
Figure 10
Figure 10: Rheumatoid arthri-tis. (a, b) Posteroanterior radio-graphs in two patients show smallbone erosion about the fifth meta-carpophalangeal joint with os-teopenia in a (arrow) and moreextensive involvement in b (ar-rows) with alterations of the fifthmetatarsal head and proximalphalanx.
Figure 11
Figure 11: Rheumatoid arthritis. Lateral radio-graph of calcaneus shows bone erosion (arrow)related to inflammation of the retrocalcaneal bursa.
Figure 12
Figure 12: Rheumatoid arthritis. Anteroposte-rior knee radiograph shows diffuse and uniformjoint space loss (arrows) with osteopenia.
Figure 13
Figure 13: Rheumatoid arthritis. Anteroposterior pelvis radiograph shows bilateral involvement of hips,with uniform diffuse joint space narrowing, bone erosions, osteopenia, and acetabular protrusion (arrows).Note bone sclerosis related to involvement of sacroiliac joints (arrowheads).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 383

symmetric or asymmetric. Involvementof several joints in a single digit, withsoft-tissue swelling, produces what ap-pears clinically as a “sausage digit” (Fig16). The bone proliferation produces anirregular and indistinct appearance tothe marginal bone about the involved
joint, characterized as a “fuzzy” appear-ance or “whiskering” (Fig 17).
Periostitis may take several forms:It may appear as a thin periosteal layerof new bone adjacent to the cortex, athick irregular layer, or irregular thick-ening of the cortex itself (Fig 17). It may
be difficult to define where periostitisends and bone erosion begins, as bothmay produce marked irregularity of the
Figure 14
Figure 14: Rheumatoid arthritis. (a) Lateral cervical spine radiograph shows erosions of dens (straightarrows) with narrowing of facet joints (curved arrow). (b) Lateral flexion radiograph shows widening of atlan-todens interval (arrowheads).
Figure 15
Figure 15: Psoriatic arthritis. Posteroanteriorfinger radiograph shows marginal bone erosionswith adjacent irregular bone proliferation (arrows).
Figure 16
Figure 16: Psoriatic arthritis. Posteroanteriorfinger radiograph shows narrowing of distal inter-phalangeal joint. Note bone proliferation and peri-ostitis throughout phalanges (arrows), whichappear thicker than in Figure 15, with partial incor-poration of new bone into the cortex. There is soft-tissue swelling of entire digit.
Figure 17
Figure 17: Psoriatic arthritis. (a) Oblique wrist radiograph shows irregular bone proliferation and periosti-tis about radial and ulnar aspects of the wrist (arrows), with erosion of the ulnar styloid process. (b) Contralat-eral wrist radiograph shows bone erosion and irregular periostitis of the scaphoid, with more distal periostitisinvolving the metacarpal base (arrows).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
384 Radiology: Volume 248: Number 2—August 2008

osseous surface (Fig 18). It is importantto note that periostitis may occur in anarea without bone erosions; one suchsite is the radial aspect of the wrist ex-tending into the first metacarpal bone.Because of the degree of bone destruc-tion, an involved joint may take the ap-pearance of a “pencil and cup,” with one
end of the joint forming a cup and theother a pencil that projects into this cup(Fig 19). This appearance is not specificfor psoriatic arthritis or any of the sero-negative spondyloarthropathies, but itis most commonly seen in these condi-tions. One characteristic feature of pso-riatic arthritis in the foot is the “ivory
phalanx,” which classically involves thedistal phalanges (especially in the firstdigit) with sclerosis, enthesitis, periosti-tis, and soft-tissue swelling (Fig 20).Joint subluxation may also be present.
Psoriatic arthritis may also involvethe axial skeleton, a finding that occursin 20%–40% of persons with peripheral
Figure 18
Figure 18: Psoriatic arthritis. Lateral kneeradiograph shows irregular thick bone prolifera-tion and periostitis of posterior aspect of the tibia(arrows).
Figure 19
Figure 19: Psoriatic arthritis. Anteroposteriorfoot radiograph shows inflammatory and destruc-tive changes of fifth metatarsophalangeal andseveral interphalangeal joints (straight arrows).Note pencil-and-cup deformity (arrowhead) andinterphalangeal joint fusion (curved arrow).
Figure 20
Figure 20: Psoriatic arthritis. Anteroposteriorradiograph shows increased density and boneproliferation of distal phalanx (ivory phalanx) ofthe first digit (arrows), with soft-tissue swelling.
Figure 21
Figure 21: Psoriatic arthritis. (a) Anteroposterior sacrum radiograph shows bone erosions and narrowing of sacroiliac joints with partial fusion (arrows). (b) Antero-posterior lumbar spine radiograph shows comma-shaped paravertebral ossifications (arrows).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 385

articular disease (6). The sacroiliac jointswill show signs of inflammation, with anindistinct subchondral bone plate or os-seous erosions, joint space irregularityand mild widening, and eventual jointspace narrowing and intraarticular
bone ankylosis (Fig 21a). Sacroiliacjoint involvement in psoriatic arthritis isusually bilateral, either symmetric orasymmetric in distribution. The thora-columbar spine may show large comma-shaped paravertebral ossifications (Fig21b); spondylitis is uncommon in theabsence of sacroiliitis, however (6). Thefacet joints are relatively spared, andthere is absence of vertebral body“squaring.”
Other sites of joint involvement inpsoriatic arthritis include the knees (Fig18), elbows, ankles, and joints aboutthe shoulders.
Reactive arthritis.—Reactive ar-thritis (also called Reiter syndrome,which is currently being used less fre-
quently) is a sterile inflammatory ar-thritis that follows an infection at adifferent site, commonly enteric orurogenital (6,7). An association withurethritis and conjunctivitis, as well asseropositivity for the HLA-B27 anti-gen, has been described (6). Reactivearthritis is most common in youngmen aged 25–35 years. The radio-graphic features of reactive arthritisare similar to those of psoriatic arthri-tis and include joint inflammation,bone proliferation, periostitis, and en-thesitis. The features allowing differ-entiation between reactive arthritisand psoriatic arthritis relate to clinicalhistory, patient sex and age, and dis-tribution of joint involvement.
Similar to psoriatic arthritis, the ra-diographic features seen in the hands,wrists, and feet in reactive arthritis in-clude joint inflammation, bone prolifer-ation, periostitis, and enthesitis, with adistribution that is unilateral or bilateraland symmetric or asymmetric (Fig 22);lower-extremity involvement is morecommon than upper-extremity involve-ment (6). Sausage digit and pencil-and-cup deformities may also occur (Fig 23).In the feet, an ivory phalanx may beseen (Fig 24).
Axial involvement may also occur,leading to bilateral symmetric or asym-metric sacroiliitis. Large, comma-shaped, paravertebral ossification mayalso be seen. Other peripheral joints areless commonly involved.
Ankylosing spondylitis.—Ankylos-ing spondylitis is an idiopathic inflam-matory arthritis, although a geneticcontribution is noted as 96% of pa-tients are HLA-B27 positive (8). Menare affected three times more fre-quently than women, with the age ofonset typically between 20 and 40years (8). This is a disease that morecommonly involves the axial skeleton,although peripheral joints may also beaffected. Spine involvement is charac-terized by osteitis, syndesmophyteformation, facet inflammation, andeventual facet joint and vertebral bodyfusion. Sacroiliac joint disease is bilat-eral and symmetric. Other peripheraljoints, such as the hips and glenohu-meral joints, may be involved. The ra-
Figure 22
Figure 22: Reactive arthritis. Lateral radio-graph of calcaneus shows bone sclerosis andirregular inflammatory enthesopathy (arrow).
Figure 23
Figure 23: Reactive arthritis. Posteroanteriorfinger radiograph shows involvement of multiplejoints with joint space narrowing, bone erosions,and bone proliferation (arrows).
Figure 24
Figure 24: Reactive arthritis. Anteroposteriorradiograph of great toe shows bone sclerosis,marginal bone erosions, and bone proliferation(arrows) about interphalangeal joint and distalphalanx, with soft-tissue swelling.
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
386 Radiology: Volume 248: Number 2—August 2008

diographic appearance of spine andsacroiliac abnormalities in ankylosingspondylitis is identical to that foundwith inflammatory bowel diseasessuch as ulcerative colitis and Crohndisease.
Sacroiliac involvement is typicallybilateral and symmetric, and it usuallyprecedes spinal involvement. Initially,there is indistinctness and discontinu-ity of the thin white subchondral boneplate about the sacroiliac joints. Thesechanges can progress to gross boneerosions (Fig 25). Early erosions ofthe subchondral bone are often bestseen in the inferior aspect of the jointsbecause they are in profile in this re-gion on an anteroposterior pelvis ra-diograph. Along with the bone ero-sions, the adjacent bone is often scle-rotic and joint space narrowing andbone fusion eventually occur (Fig 26).Because the sacroiliac joints may bedifficult to interpret on radiographs,magnetic resonance imaging can beuseful in the diagnosis of sacroiliitis byshowing joint fluid and marrow edemawhen radiographs are normal orequivocal. When radiographs are ab-normal, computed tomography maybe used to differentiate bone erosionsfrom osteophytes. The differential di-agnosis of bilateral sacroiliac jointerosions includes inflammatory boweldisease (Fig 27) and hyperparathy-roidism (Fig 28); however, in hyper-parathyroidism, sacroiliac joint spacewidening is more dramatic, and typi-cally there are other clinical and radio-graphic features of hyperparathyroid-ism.
Spine involvement in ankylosingspondylitis is often centered at thethoracolumbar or lumbosacral junc-tion, and coned-down lateral radio-graphs at these sites optimally depictsubtle and early abnormalities. Earlyradiographic findings are erosions atthe anterior margins of the vertebralbody at the discovertebral junction.These focal areas of osteitis becomeincreasingly sclerotic, a finding termedthe “shiny corner sign” (Fig 29). Moreextensive discovertebral erosions mayalso occur. Associated bone prolifera-tion leads to a “squared” appearance
of the vertebral body. Thin and slen-der syndesmophytes are generally ev-ident, representing ossification of theouter layer of the annulus fibrosis
(Fig 30). The differential diagnosis forbone production at the vertebral mar-gins includes diffuse idiopathic ske-letal hyperostosis, or DISH, although
Figure 25
Figure 25: Ankylosing spon-dylitis. Anteroposterior pelvisradiograph shows bilateral sym-metric bone erosions, sclerosis,and widening of sacroiliac joints(arrows).
Figure 26
Figure 26: Ankylosing spon-dylitis. Anteroposterior radio-graph of sacrum shows fusion ofsacroiliac joints (arrows).
Figure 27
Figure 27: Inflammatory boweldisease. Anteroposterior radio-graph of sacrum shows bilateraland symmetric bone erosions,bone sclerosis, and widening ofsacroiliac joints (arrows).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 387

this latter condition more commonlyreveals a flowing and undulating ap-pearance.
As the syndesmophytes thicken andbecome continuous, the term bamboospine is used to describe the appearance
on anteroposterior lumbar spine radio-graphs (Fig 31). Facet joint inflammationleads to indistinctness and narrowing ofthe involved joint, and bone fusion of thejoints appears later (Fig 30). Ossificationof the posterior interspinous ligaments
produces a dense radiopaque line, desig-nated the “dagger sign,” on anteroposte-rior radiographs of the lumbar spine(Fig 32). The combination of the fusedfacets and ossification of the interspi-nous ligaments produces the “trolley-track sign” (Fig 33). Disk calcificationmay also occur, possibly due to relativeimmobilization of the vertebral column.
Other peripheral joints can be in-volved in ankylosing spondylitis. Hip in-volvement is usually bilateral in distri-bution (Fig 34). Uniform joint space lossin these joints is combined with acetab-ular protrusion, subchondral cysts, anda rim of osteophytes about the femoralneck. Bone erosions and remodeling inthe lateral proximal aspect of the hu-merus produce a “hatchet” appearance.
Conclusion
Once joint space narrowing is recog-nized, the presence of bone erosionssuggests an inflammatory arthritis,while osteophytes indicate a degenera-tive arthritis. The joint distribution and
Figure 29
Figure 29: Ankylosing spondylitis. Laterallumbar spine radiograph shows sclerosis at ante-rior aspect of the end plate (shiny corner sign)(arrow), with squaring of anterior margin of verte-bral body.
Figure 30
Figure 30: Ankylosing spondylitis. Laterallumbar spine radiograph shows anterior bridgingsyndesmophytes (arrows) and facet joint fusion(arrowheads).
Figure 31
Figure 31: Ankylosing spondylitis. Anteropos-terior lumbar spine radiograph shows bridgingsyndesmophytes (bamboo spine) (arrows).
Figure 28
Figure 28: Hyperparathyroidism. Anteroposterior radiograph of sacrum shows bilateral and symmetricbone sclerosis and irregularity of sacroiliac joints (arrow). Note marked widening of sacroiliac joints and renaldialysis catheter.
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
388 Radiology: Volume 248: Number 2—August 2008

the presence of bone proliferation allowdistinction between septic arthritis, rheu-matoid arthritis, and the seronegativespondyloarthropathies. If inflammationinvolves a single joint, one must care-fully exclude infection. If inflammatoryarthritis is diffuse and involves the prox-imal joints of the hands and feet withoutbone proliferation, rheumatoid arthritisis most likely. Distal joint involvementwith bone proliferation suggests thepresence of one of the seronegativespondyloarthropathies.
References1. Learch TJ. Imaging of infectious arthritis. Se-
min Musculoskelet Radiol 2003;7:137–142.
2. Rutten MJ, van den Berg JC, van den HoogenFH, Lemmens JA. Nontuberculous mycobac-terial bursitis and arthritis of the shoulder.Skeletal Radiol 1998;27:33–35.
3. Machold KP, Nell V, Stamm T, Aletaha D,Smolen JS. Early rheumatoid arthritis. CurrOpin Rheumatol 2006;18:282–288.
4. Tehranzadeh J, Ashikyan O, Dascalos J. Mag-netic resonance imaging in early detection ofrheumatoid arthritis. Semin MusculoskeletRadiol 2003;7:79–94.
5. Monsey RD. Rheumatoid arthritis of the cer-vical spine. J Am Acad Orthop Surg 1997;5:240–248.
6. Klecker RJ, Weissman BN. Imaging featuresof psoriatic arthritis and Reiter’s syndrome.Semin Musculoskelet Radiol 2003;7:115–126.
7. Lu DW, Katz KA. Declining use of the eponym“Reiter’s syndrome” in the medical literature,1998–2003. J Am Acad Dermatol 2005;53:720–723.
8. Vinson EN, Major NM. MR imaging of anky-losing spondylitis. Semin Musculoskelet Ra-diol 2003;7:103–113.
Figure 32
Figure 32: Ankylosing spondylitis. Anteropos-terior lumbar spine radiograph shows ossificationof the interspinous ligament (dagger sign)(arrows).
Figure 33
Figure 33: Ankylosing spondylitis. Anteropos-terior lumbar spine radiograph shows ossificationof interspinous ligament and facet joint fusion(trolley-track sign) (arrows).
Figure 34
Figure 34: Ankylosing spon-dylitis. Anteroposterior pelvisradiograph shows bilateral diffusejoint space narrowing and boneerosions of each hip joint (arrow-heads), with sacroiliac joint fusion(arrows).
REVIEW FOR RESIDENTS: Radiographic Evaluation of Arthritis Jacobson et al
Radiology: Volume 248: Number 2—August 2008 389