radiologic evaluation of petrous apex...
TRANSCRIPT
Radiologic Evaluation of Petrous Apex MassesPavan Kavali, MS-IVMorehouse School of MedicineNovember 16, 2009

Roadmap
Petrous Apex AnatomyPatient D.S.: Clinical PresentationDifferential diagnosis of masses in the petrous apex of temporal bonePatient CourseAcknowledgementsReferences

Petrous Apex Anatomy
• Petrous portion of the temporal bone is pyramidal and is wedged in at the base of the skull between the sphenoid and occipital
• Consists of a base, apex, anterior, inferior and posterior surfaces.
• Apex: angular interval between the posterior border of the great wing of the sphenoid and the basilar part of the occipital
http://en.wikipedia.org/wiki/File:Gray193.png

Axial CT Anatomy
http://www.urmc.rochester.edu/smd/Rad/neuroanatomy/headCT_anatomy.htm

Our Patient AI: Clinical History
D.S. is a 44 year old man with a four day history of left facial droopNoted difficulty in whistling and drinking from a cupSeen at the Winchester ER where a CT scan was performed which revealed a 3-4 cm posterior fossa mass that extends into the bone and the cerebellum He denies any headache, visual changes, loss of coordination, or other sensory or motor deficits.
• Past Medical HistoryMeniere’s Disease with total deafness of left earHypertensionDepression/Anxiety

Our Patient AI: Initial Imaging Findings
Heterogeneous erosive mass centered within the posterior left temporal bone, eroding into the middle ear cavity, jugular foramen and carotid canal.
Axial CT, patient AIImage Source: BIDMC (PACS)

Our Patient AI: CT and CT-A Findings
• Axial CT showing heterogeneous mass extending into the posterior left temporal bone
• CT-Angiogram confirming the findings of the reference head CT from Winchester ER.

Our Patient AI: Differential Diagnosis
• Primary ConsiderationsEndolymphatic Sac TumorCholesterol Granuloma of Petrous ApexLipomaChondrosarcomaParagangliomaAcoustic SchwannomaInternal Carotid Artery AneurysmCholesteatoma of Petrous Apex

Endolymphatic Sac Tumors (ELST)
• The endolymphatic sac is located at the end of endolymphatic duct– lies within dura of the posterior fossa
• Slow growing tumor that arises from cells lining endolymphatic sac– Most sporadic– Mutations and allelic deletions of von Hippel-Lindau (VHL) tumor
suppressor gene plays a role– If bilateral, VHL disease is present– Histologically benign
• Clinical Presentation– Most Common Signs/Symptoms
• Sensorineural hearing loss – 100%• Facial Nerve Palsy – 60%• Pulsatile Tinnitus – 50%• Vertigo – 20%
• Average Age at Surgical Resection – 36 years

Endolymphatic Sac Tumor
• MR Imaging Findings– Peripheral rim of increased signal intensity is strongly
indicative of early endolymphatic sac tumor– Hyperintense foci within tumor matrix on T1 (80%)
• Along tumor margin when tumor < 3 cm• Within tumor matrix when tumor > 3 cm
– Flow voids (focal low signal areas on T1) when tumors > 2 cm
– T2 Weighted Images• Common to see inhomogeneous signal• Bone fragments show low signal
– T1 with Contrast• Heterogeneous enhancement
• CT Imaging Findings– Intramural bone spicules – “moth-eaten” appearance noted
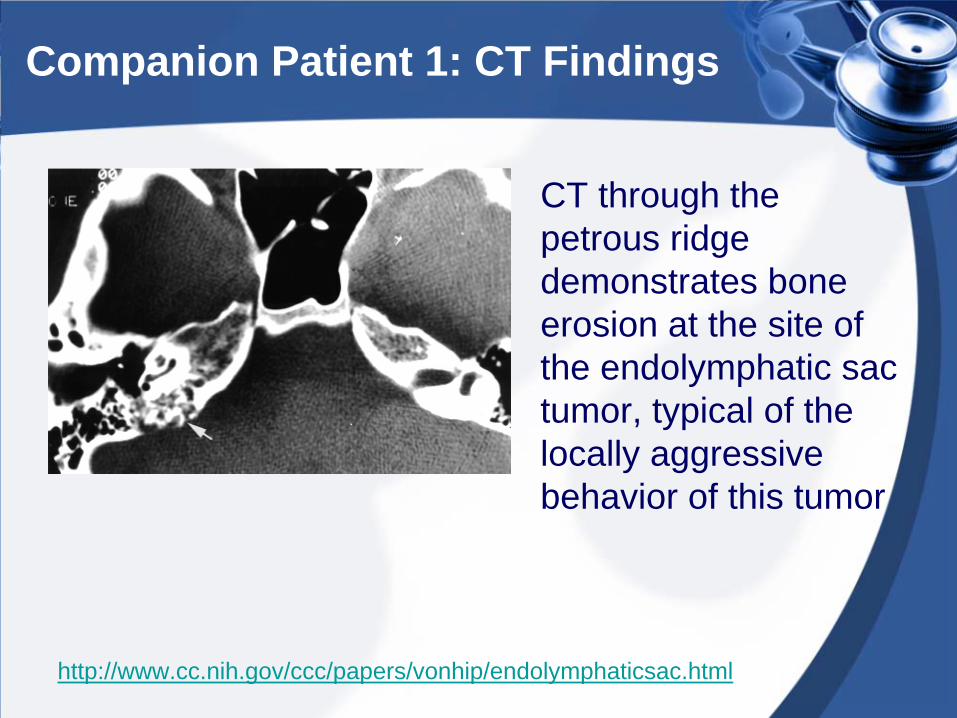
Companion Patient 1: CT Findings
CT through the petrous ridge demonstrates bone erosion at the site of the endolymphatic sac tumor, typical of the locally aggressive behavior of this tumor
http://www.cc.nih.gov/ccc/papers/vonhip/endolymphaticsac.html

Companion Patient 1: MR Images
• T1 MRI demonstrates high signal intensity
• Post-contrast T1 image demonstrates intense enhancement within the tumor focus
http://www.cc.nih.gov/ccc/papers/vonhip/endolymphaticsac.html

Cholesterol Granuloma of Petrous Apex (CGPA)
• Most common lesion of the petrous apex. • Reaction to a foreign body (typically to
cholesterol deposits)– Due to occlusion of the mastoid air cells and
degradation of accumulated hemosiderin to cholesterol
– Leads to an inflammatory reaction and progressive granuloma formation
• Clinical Presentation– Hearing loss most common– Vestibular dysfunction– Headache, tinnitus, facial spasms and diplopia
also seen

CGPA Imaging Findings
• MRI– T1: High Internal Signal
• Hemorrhage, break-down products, cholesterol crystals– T2: High Internal Signal
• Peripheral dark hemosiderin ring– FLAIR: High Internal Signal without attenuation– T1 + Contrast: No internal enhancement
• CT– Well-defined, smoothly expansile mass– Lesions show focal bony dehiscence– Can also evaluate adjacent carotid canal and otic
capsule• MR more sensitive than CT to evaluate
recurrence

Companion Patient 2: CT Images
Courtesy of Dr. Rafael Rojas
• Axial CT demonstrates a smoothly expansile mass lesion through the left temporal bone
• Coronal CT scan confirms the findings of a smoothly expansile mass in the left temporal bone.

Companion Patient 2: MR T1 and T2 Weighted Images
Courtesy of Dr. Rafael Rojas
Bright signal observed on T1 and T2 weighted images in the tumor matrix.

Lipoma of CPA-IAC
• Congenital fatty lesion that is benign• Current hypothesis for development of lipomas:
– Maldevelopment of meningeal precursor tissue– Maldifferentiation of mesoderm into lipocytes as opposed to
arachnoidal cells– Hyperplasia of fat cells within the pia
• Clinical Presentation– Young adult that typically presents with progressive unilateral
sensorineural hearing loss– With compression of CN VIII, tinnitus (40%) and vertigo (45%) is
also seen in patients– With compression of CN VII, facial nerve weakness/spasms are
also seen– Trigeminal neuralgia is seen in about 15% of patients with nerve
root entry zone compression

Lipoma Imaging Findings
• MRI– T1: High signal mass in the cerebellopontine
angle– T2: Intermediate fat-intensity lesion– FLAIR: High signal mass continues to be seen– T1 + Contrast: No enhancement seen if fat-
saturated T1 + C sequences are seen.
• CT– Non-enhancing, well-circumscribed lesion seen– Use Hounsfield units to determine nature of the
mass

Companion Patient 3: MR Images
Courtesy of Dr. Rafael Rojas
CT shows a hypointense lesion in the CPA
MRI – T1WI: Seen again is an avidly enhancing, well- circumscribed lesion at the CPA

Chondrosarcoma of Petrous Apex
• Malignant tumor of cartilaginous origin – Tumor matrix is entirely chondroid– Severity is based on histological grading– Typically occurs near the petrous apex if it occurs in the
skull base
• Clinical presentation similar to other petrous apex lesions
• CT scan used to evaluate extent of bony destruction
• MR scan typically shows enhancement on T1- and T2-weighted images.

Companion Patient 4: CT Images
Courtesy of Dr. Rojas
Axial CT showing a chondrosarcoma showing an isodense mass and bony dehisence at the petrous apex of the left temporal bone.
Coronal CT showing a large mass that is isodense

Companion Patient 4: MR Images
T1W1 image shows a peripherally enhancing mass at the petrous apex as well as encroaching the cerebello- pontine angle.
T2W1 image shows a heterogeneously enhancing mass
Courtesy of Dr. Rojas

Back to Our Patient
• Patient was sent from Winchester ER to BIDMC for definitive care
• He continued to exhibit the same symptoms while at BIDMC as well
• Further characterization of the mass was needed using an MRI with and without contrast.

Our Patient AI: Axial MRI Findings
• Heterogeneous 4.5 x 2.0 x 3.4 cm mass centered within and growing out of the left temporal bone
• Striking T1 hyperintensity seen
MR T1 Axial Image
Image Source: BIDMC (PACS)

Our Patient AI: MR Findings
• Continued to be seen is a heterogeneous, T2 hyperintense mass along the petrous apex
• Mass extends into and expands the internal auditory canal on the left.
• The cochlea and semicircular canals are poorly defined on the left side.
MR T2 Axial Image
Image Source: BIDMC (PACS)

Our Patient AI: MR Findings
MR Axial FLAIR Image
• The FLAIR image exhibits avidly enhancing mass in the petrous apex also causing mass effect on the left cerebellum.
Image Source: BIDMC (PACS)

Our Patient AI: Sagittal MR
• Sagittal MR T1WI showing a hyperintense, heterogeneous mass
Image Source: BIDMC (PACS)

Our Patient AI: Initial MR @ BIDMC – Final Report
• Impression: Heterogeneous mass centered within the left temporal bone with osseous erosion and mild mass effect. It is difficult to appreciate any significant enhancement given the intrinsic T1 hyperintensity, with probable intra-lesional hemorrhage. There is a broad differential including an endolymphatic sac tumor or cholesterol granuloma. Less likely considerations would include metastatic disease, a primary osseous lesion or an unusual aggessive nerve sheath tumor.

Our Patient AI: Hospital Course
• As mentioned earlier, patient’s history of prior severe anxiety attacks contributed to his initial discharge from the hospital without any further neurosurgical workup.
• Since the patient was in stable condition and surgery was non-emergent, patient was counseled extensively to come back for a definitive procedure to remove the mass.
• Patient came back a week later and underwent resection of the mass.

Our Patient AI: Final Diagnosis
• Final Path Report– Papillary neoplasm consistent with
endolymphatic sac tumor

Our Patient AI: Post-Surgical Result
• Partial resection of the previously identified hyperintense and partially enhancing lesion in the left temporal bone
• Resection of the mass seen more medially but the left hyperintense area persists
MR Axial T1 Image
Image Source: BIDMC (PACS)

Acknowledgements
• Dr. Rafael Rojas, BIDMC Radiology• Dr. Brian Livingston, BIDMC Radiology• Dr. Gillian Lieberman, BIDMC
Radiology• Maria Levantakis, BIDMC Radiology

References
• Kim HC et al. Petrous apex cholesterol granuloma presenting as endolymphatic hydrops: a case report. Clin Exp Otorhinolaryngol. 2(3):151-4. Epub 2009
• Mendenhall, et al. “Management of Acoustic Neuroma” American Journal of Otolaryngology. 2004; 25: 38-47
• Cohen JE et al. Endolymphatic sac tumor: staged endovascular-neurosurgical approach. Neurol Res. 25(3): 237-40, 2003
• Richards PS, Clifton AG. Endolymphatic sac tumors. J Laryngol Otol. 117(8):666-9, 2003
• Choyke PL et al. Von Hippel Lindau Disease: Genetic, Clinical and Imaging Features. Radiology 146:629-642,1995
• http://www.cc.nih.gov/ccc/papers/vonhip/endolymphaticsac.h tml