%rdug 5hylhz &rxuvh 8sgdwh 4xhvwlrq %orfn 6hoi …
TRANSCRIPT
Saturday, July 17, 2021
2:55 - 3:25 p.m. EDT
WITH ANSWERS
Question Block #2:Self-Directed Case Breakouts
Board Review Course & Update
Case 1 Background• HPI: A 72-year-old woman presents with nausea, anorexia, and increasing fatigue/weakness,
prompting an ED visit. Increased serum Cr is noted on blood draw in ED.
• PMH: T2 DM, HTN, GERD, osteoarthritis, osteoporosis, and constipation
• Medications: Enalapril, amlodipine, metformin, canagliflozin, lansoprazole, calcium-vitamin Dtablets, docusate and occasional polyethylene glycol, occasional tramadol and naproxen (forhip pain); no OTC or herbal products
• Allergies: None
• Examination: BP: 138/86, P: 88, T: 99.1• Head and Neck: Pale conjunctiva, normal JVP• Lungs: Clear, petechial rash on chest• Heart: S1S2; no S3 or rub• Abdomen: Benign with normal BS; no flank tenderness• Extremities: 1+ ankle edema; no rash
Case 1 BackgroundLabs:
• Electrolytes: Na+ = 137 mEq/L, K+ = 5.3 mEq/L, HCO3- = 16 mEq/L,
Cl- = 102 mEq/L, AG = 19
• BUN = 55 mg/dl Cr = 4.1 mg/dl
• Glucose = 145 mg/dl Alb = 3.5 g/dl
• Hb = 10.5 mg/dl Plt = 235 × 1000/uL
• WBCs = 14,000 per mm3, Eosinophils = 2%
• Urinalysis: SG-1.014, pH-6.0, Protein-1+, Blood-1+, Glucose-2+,
Leukocyte esterase-2+
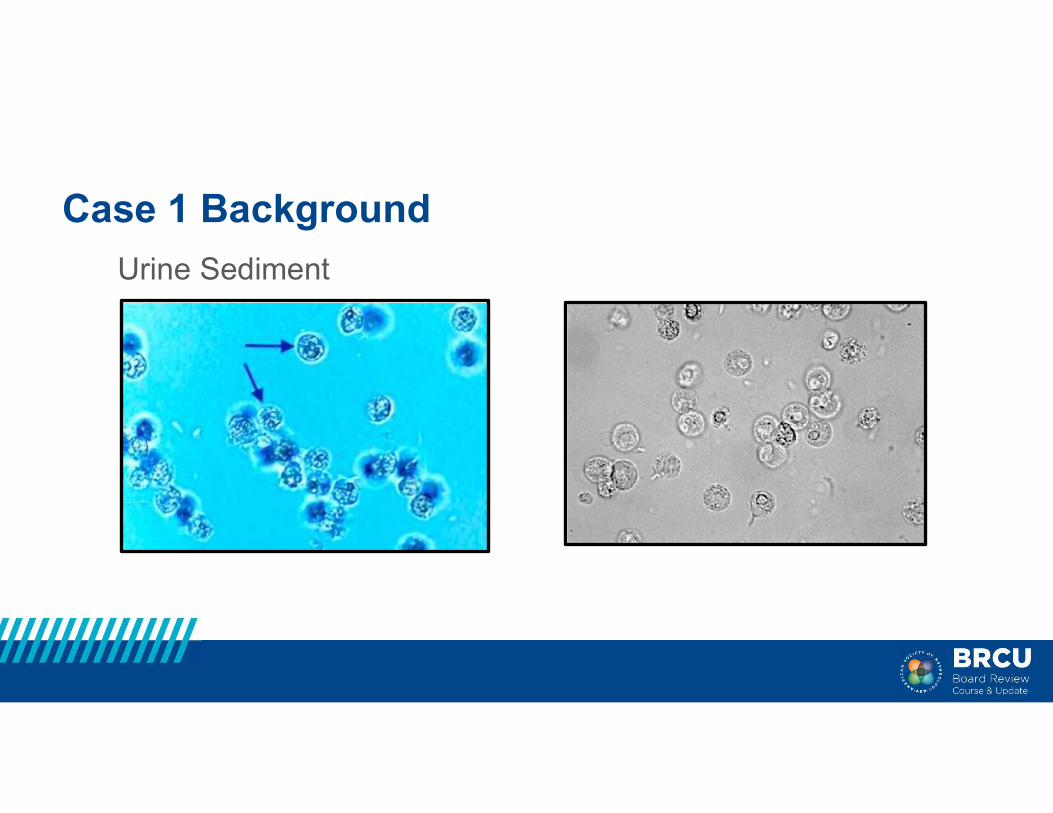
Case 1 Background
Urine Sediment

Case 1 Question
What is present on urine microscopy?
A. Renal tubular epithelial cells
B. White blood cells
C. Isomorphic RBCs
D. Transitional epithelial cells
E. Squamous epithelial cells
For the explanation, review "Cases: Urinalysis..." by Mark Perazella.
Case 2 Background• HPI: A 58-year-old obese woman presents with malaise, weakness, and
frequent “oily” stools (8/day) for the past several months.• PMH: HTN, T2-DM, arthritis, CKD (baseline serum Cr=2.1 mg/dl), GERD,
asthma, gout, s/p gastric bypass 6 months ago• Medications: Diltiazem, montelukast sodium, furosemide, pantoprazole,
allopurinol, colchicine prn, Bactrim for URI for past 7 days; no herbal productsor NSAIDs
• Examination: BP: 130/80, P: 82, Afebrile• Head and Neck: Mild conjunctival pallor, elevated JVP• Lungs: Clear• Heart: S1S2, 1/6 SM; no rub• Abdomen: Obese; no flank pain• Extremities: Trace edema of ankles
Case 2 Background
Labs:
• Electrolytes: Na+ = 136 mEq/L, K+ = 4.8 mEq/L, HCO3- = 26 mEq/L,Cl- = 99 mEq/L
• BUN = 52 mg/dl Cr = 3.8 mg/dl 5.8
• Hb = 10.2 mg/dl Plt = 286 × 1000/uL
• WBCs = 9 per mm3, Eosinophils = 4%, Hb = 11 g/dl
• Uric acid = 10.6 mg/dl Ca++ = 8.7 mg/dl PO4 = 8.5 mg/dl
Case 2 Background
Urinalysis:
• SG = 1.018, pH = 6.0, Protein-negative, Blood-trace,
Glucose-negative, Leukocyte esterase-trace
Ultrasound of Kidneys:
• 10.4 cm and 10.7 cm kidneys
• Increased cortical echogenicity

Case 2 Background
Urine Sediment

Case 2 Question
What crystals are present on urine microscopy?
A. Sulfonamide crystals
B. Calcium phosphate crystals
C. Calcium oxalate crystals
D. Uric acid crystals
E. Hippurate crystals
For the explanation, review "Cases: Urinalysis..." by Mark Perazella.
Question 3 (no case)
Which is the MOST common cause of AIN?
A. Sarcoidosis
B. Tubulointerstitial nephritis with uveitis (TINU)
C. Medications
D. Infectious agents
E. Sjogren syndrome
F. IgG4 disease
For the explanation, review "Acute and Chronic Interstitial Nephritis" by Mark Perazella.
Case 3 Background
A 49-year-old obese woman with HTN, OA, and T2 DM presents
feeling poorly over past 4-6 weeks and is noted to sCr 3.2 mg/dl.
Medications include glipizide, losartan/HCTZ, naproxen, and a
health store weight loss regimen (past 2 years). Exam is
unremarkable. U/A: 1+ pro, 1+ glu, trace LE and blood. Urine
microscopy: 2-5 WBCs and 1-3 RBCs/HPF, 1-2 waxy casts/LPF.
Biopsy is obtained.

Case 3 Background
M. Perazella
Case 3 Question
Which is the MOST likely diagnosis?
A. Weight loss regimen (aristolochic acid) nephropathy
B. Obesity-related nephropathy
C. NSAID-induced acute interstitial nephritis
D. Diabetic nephropathy
E. HCTZ-induced acute interstitial nephritis
For the explanation, review "Acute and Chronic Interstitial Nephritis" by Mark Perazella.
Question 4 (no case)
In a patient with AKI from biopsy-proven AIN, which is associated with an increased likelihood that kidney function will improve following a course of corticosteroid therapy?
A. Peak serum creatinine concentration less than 6 mg/dl
B. Corticosteroid therapy initiated within 1 week of diagnosis
C. Preserved kidney size on ultrasonography
D. Baseline GFR greater than 60 ml/min/1.73m2
E. Proteinuria less than 1 gram per day
For the explanation, review "Acute and Chronic Interstitial Nephritis" by Mark Perazella.
Case 4 Background
• 59-year-old woman with history of osteoporosis (on oral calciumand cholecalciferol) and cystic breast disease developsprogressive nausea and confusion over the past 2 weeksprompting her family to bring him the emergency department.
• In the ED, she is found to be hypotensive, orthostatic, and with thefollowing notable labs:
• Sodium 148 meq/L HCO3 18 meq/L• Calcium 15.6 mg/dL• Creatinine 2.1 mg/dL
Case 4 Question
Which would be your first therapeutic step?
A. Pamidronate 30 mg IV over 6 hours
B. IV normal saline 1 L bolus followed by infusion at 150 ml/hour
C. Furosemide 40 mg IV
D. Denosumab infusion
E. Calcitonin nasal spray
For the explanation, review "Cases: Onco-Nephrology" by Mark Perazella and Mitchell Rosner.
Case 5 Background
A 63-year-old man is admitted for refractory hypokalemia and metabolic alkalosis. The patient had a 1-year history of small cell lung carcinoma that was treated with paclitaxel, carboplatin, and gemcitabine. Two weeks before admission, he noticed increasing weakness.
On physical examination, his BP was 182/95 mmHg, and he had 2+ ankle edema. Cardiovascular and chest examinations were unremarkable. Abdominal examination showed no central obesity nor striae. Neurologic examination showed proximal muscle weakness. His laboratory values were as follows: BUN, 12 mg/dl; creatinine, 1.1 mg/dl; sodium, 137 mEq/L; K, 2.8 mEq/L; Cl, 85 mEq/L; and HCO3, 35 mEq/L. Glucose was 165 mg/dl.
Case 5 Question
At this point, which laboratory test would cause his metabolic abnormalities?
A. Plasma aldosterone
B. Plasma cortisol
C. Plasma ACTH
D. Plasma thyroid stimulating hormone
E. Plasma glucagon
For the explanation, review "Cases: Onco-Nephrology" by Mark Perazella and Mitchell Rosner.