renal trauma nurse teaching jan 2017
TRANSCRIPT

RENAL TRAUMAAMBER Z JAFFERIEMERGENCY DEPARTMENTSIH
BACKGROUND 1-5% of all traumasMale to female ratio 3:1Mechanism is classified as blunt or penetratingBlunt trauma accounts 90-95%Traffic accidents accounts half of blunt renal injuriesRenal lacerations and renal vascular injuries make up only 10-15% of blunt renal injuries

BACKGROUND
Renal artery occlusion is associated with a rapid deceleration injuriesRate of nephrectomy in recent wars is relatively high (25-33%)

INJURY CALSSIFICATION
A total of 26 classifications have been presented in the literature in the past 50 years
These are oriented to different criteria such as : 1. The pathogenesis ( blunt or penetrating )2. The morphological findings ( type and degree of
lacerations )3. The clinical course ( nature and time of
symptoms )



AAST RENAL INJURY GRADING SCALEGradeDescription of injury
1Contusion or non-expanding subcapsular hematoma No laceration
2Non-expanding perirenal hematoma Cortical laceration < 1 cm deep without extravasation
3Cortical laceration > 1cm without urinary extravasation
4Laceration : through corticomedullary junction in to collecting systemOr Vascular : segmental renal artery or vein injury with contained hematoma
5Laceration: shatered kidneyOrVascular : renal pedicle injury or avulsion

INITIAL EMERGENCY ASSESSMENT Securing of the airwayControlling any of the external bleedingResuscitation of shockPhysical examination is carried out during stabilization
HISTORY AND PHYSICAL EXAMINATION
Direct history is obtained from conscious patientsWitness and emergency personnel can provide information regarding unconscious patients

POSSIBLE INDICATORS OF MAJOR RENAL INJURY

The following findings on physical examination may indicate possible renal involvement :
1. Hematuria2. Flank pain3. Flank ecchymosis4. Flank abraisions5. Fractured ribs6. Abdominal distension7. Abdominal mass8. Abdominal tenderness

GUIDELINES ON LABORATORY EVALUATION
Urine from a patient with suspected renal injury should be inspected grossly and then by dipstick analysisSerial hematocrit measurement indicates blood loss ( renal or associated injuries ? )Creatinine measurement reflects renal function preior to the injury
GUIDELINES ON RADIOGRAPHIC ASSESSMENT
Blunt trauma patients with macroscopic or microscopic hematuria ( at least 5 rbc/hpf ) with hypotension (systolic blood pressure < 90 mmHg ) should undergo radiographic evaluation Radiographic evaluation is also recommended for all patients with a history of rapid deceleration injury and /or significant associated injuryAll patients with any degree of hematuria after penetrating abdominal or thoracic injury require urgent renal imagingUltrasonography can be informaive during the primary evaluation of polytrauma patients and for the follow-up of the recuperating patients

GUIDELINES ON RADIOGRAPHIC ASSESSMENT
A CT scan with enhancement of intravenous contrast material is the best imaging study for diagnosis and staging renal injuries in hemodynamically stable patientsUnstable patients who require emergency surgical exploration should undergo a one-shot IVP with bolus intravenous injection of 2ml/kg contrast Formal IVP , MRI , and radiographic scintigraphy are reliable alternative methods of imaging renal trauma when CT is not availableAngiography can be used for diagnosis and simultaneous selective embolization of bleeding vessels

COMPUTED TOMOGRAPHY SCAN OF RIGHT KIDNEY FOLLOWING STAB WOUND LACERATION WITH URINE EXTRAVASATION , LARGE RIGHT RETROPERITONEAL
HEMATOMA

TREATMENT Non-operative management is the treatment of choice for the majority of renal injuries The overall exploration rate for blunt trauma is less than 10%The overall rate of patients who have a nephrectomy during exploration is around 13%

GUIDELINES ON MANAGEMENT OF RENAL TRAUMA
Stable patients following grade 1-4 blunt renal trauma , should be managed conservatively : Bed-rest , hydration and antibiotics , and continuous monitoring of vita signs until hematuria resolvesStable patients , following grade 1-3 stab and low velocity-gunshot wounds after complete staging , should be selected for expectant management

GUIDELINES ON MANAGEMENT OF RENAL TRAUMAIndications for surgical management include : 1. Haemodynamic instability2. Exploration for associated injuries3. Expanding or pulsatile perirenal hematoma identified
during laparotomy4. A grade V injury5. Incidental finding of pre-existing renal pathology
requiring surgical therapy
Renal reconstruction should be attempted in cases where the primary goal of controlling hemorrhage is achieved and sufficient amount of renal parenchyma is viable

GUIDELINES ON POST-OPERATIVE MANAGEMENT AND FOLLOW-UPRepeat imaging is recommended for all hospitalized patients within
2-4 days following renal traumaNuclear scintigraphy before discharge from the hospital is useful
for documenting functional recoveryWithin 3 months of major renal trauma , patients follow-up should
involve :1. Physical examination2. Urinalysis3. Individualized radiological investigation4. Serial blood pressure measurement5. Serum determination of renal functionLong-term follow-up should be decided on a case-by-case basis





COMPLICATIONS Early complications : Bleeding , infection , perinephric abscess , sepsis , urinary fistula , hypertension , urinary extravasation and urinoma Delayed complications : Bleeding , hydronephrosis , calculus formation , chronic pyelonephritis , hypertension , arteriovenous fistula , and psuedoaneurism

GUIDELINES ON MANAGEMENT OF COMPLICATIONS
Complication following renal trauma require a thorough radiographic evaluationMedical management and minimal invasive techniques should be the first choice for the management of complicationsRenal salvage should be the aim of surgeon for patients in whom surgical intervention is necessary


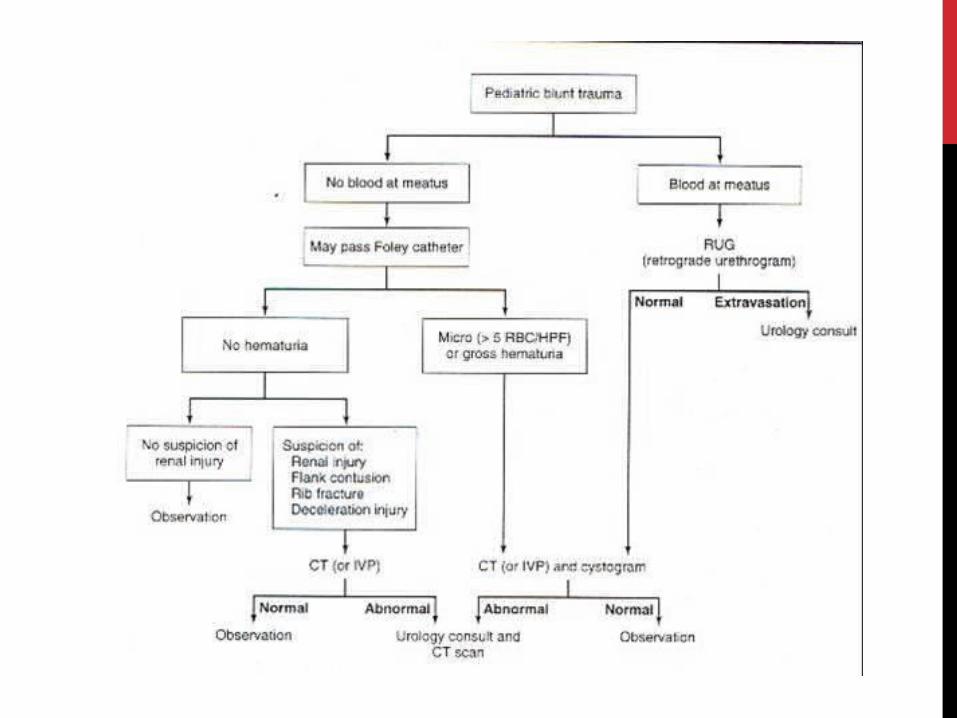
GUIDELINES ON MANAGEMENT OF PAEDIATRIC TRAUMA
Indications for radiographic evaluation of children suspected for renal trauma include :
1. Blunt and penetrating trauma patients with any level of hematuria
2. Patients with associated abdominal injuries regardless of the urinalysis findings
3. Patients with normal urinalysis who sustained a rapid deceleration events , direct flank trauma , or fall from height
Ultrasonography is considered a reliable method of screening and following blunt renal injuries
CTscans is the imaging study of choice for staging renal injury Haemodynamic instability and a diagnosed grade V injury are
absolute indications for surgical exploration

GUIDELINES ON MANAGEMENT OF POLYTRAUMA PATIENTS WITH ASSOCIATED RENAL INJURY
Polytrauma patients with associated renal injuries should be evaluated on the basis of the most threatening injuryIn cases where the decision for surgical intervention is made , all associated injuries should be evaluated simultaneouslyThe decision for conservative management should regard all injuries independently