research article engaging stakeholders to design a ... · patterns of beliefs, interactions,...
TRANSCRIPT

17J. Comp. Eff. Res. (2016) 5(1), 17–30 ISSN 2042-6305
part of
Research Article
10.2217/cer.15.52 © 2016 Future Medicine Ltd
J. Comp. Eff. Res.
Research Article 2016/01/305
1
2016
Aim: To present the methods and outcomes of stakeholder engagement in the development of interventions for children presenting to the emergency department (ED) for uncontrolled asthma. Methods: We engaged stakeholders (caregivers, physicians, nurses, administrators) from six EDs in a three-phase process to: define design requirements; prototype and refine; and evaluate. Results: Interviews among 28 stakeholders yielded themes regarding in-home asthma management practices and ED discharge experiences. Quantitative and qualitative evaluation showed strong preference for the new discharge tool over current tools. Conclusion: Engaging end-users in contextual inquiry resulted in CAPE (CHICAGO Action Plan after ED discharge), a new stakeholder-balanced discharge tool, which is being tested in a multicenter comparative effectiveness trial.
First draft submitted: 14 July 2015; Accepted for publication: 4 October 2015; Published online: 21 December 2015
Keywords: asthma • health communication • patient discharge • pediatrics • stakeholder engagement • written action plan
Comparative effectiveness research is intended to address the expressed needs of patients, care-givers and other decision-makers in health-care [1]. Such engagement is considered critical to evaluating interventions relevant to end-users and that are feasible for use in real world clinical settings. National and international asthma guidelines recommend the use of writ-ten instructions to promote appropriate use of medications, avoidance of environmental trig-gers and advice about when to seek additional medical attention [2,3]. However, systematic reviews indicate that the content, format and benefits of such written instructions (usually called action plans) are highly variable, with relatively low rates of use because most action plans are designed by teams of medical experts with relatively little input from patients, caregivers and clinicians [4,5].
The CHICAGO study is a multicenter comparative effectiveness trial funded by the Patient-Centered Outcomes Research Insti-
tute (PCORI) to test strategies to improve the care and outcomes of African–Ameri-can and Latino children with uncontrolled asthma presenting to the emergency depart-ment (ED) in Chicago [6]. In Chicago, African–American and Latino children aged 5–11 years bear a disproportionate share of the burden from asthma [7]. Among the most visible of these disparities is the five- to seven-fold higher rate of visits to the ED for uncontrolled asthma in communities with a high proportion of African–American and Latino children compared with other com-munities [Department of Public Health, Chicago,
Pers. Comm.] . As part of the PCORI-funded CHICAGO study, we employed user-cen-tered design methods to engage caregivers, clinicians and administrators in the develop-ment and evaluation of an asthma discharge tool for African–American and Latino chil-dren who present to the ED for uncontrolled asthma [8]. To our knowledge, this is the first
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma
Kim Erwin*,1, Molly A Martin2, Tara Flippin1, Sarah Norell1, Ariana Shadlyn1, Jie Yang1, Paula Falco1, Jaime Rivera1, Stacy Ignoffo3, Rajesh Kumar4, Helen Margellos-Anast5, Michael McDermott6, Kate McMahon7, Giselle Mosnaim8, Sharmilee M Nyenhuis2, Valerie G Press9, Jessica E Ramsay5, Kenneth Soyemi10, Trevonne M Thompson2 & Jerry A Krishnan2,11
1IIT Institute of Design, 350 N LaSalle,
Chicago, IL 60654, USA 2University of Illinois at Chicago, 1200 W
Harrison St Chicago, IL 60607, USA 3Chicago Asthma Consortium,
PO Box 31757, Chicago, IL 60631, USA 4Ann & Robert H Lurie Children’s
Hospital of Chicago, 225 E Chicago Ave.,
Chicago, IL 60611, USA 5Sinai Health System, California Avenue,
15th Street, Chicago, IL 60608, USA 6Illinois Emergency Department Asthma
Surveillance Project (IEDASP) 7Respiratory Health Association, 1440 W
Washington Blvd, Chicago, IL 60607,
USA 8Rush University Medical Center, 1653 W
Congress Pkwy, Chicago, IL 60612, USA 9University of Chicago, 5801 S Ellis Ave.,
Chicago, IL 60637, USA 10John H Stroger Jr Hospital of Cook
County, 1901 W Harrison St Chicago,
IL 60612, USA 11University of Illinois Hospital & Health
Sciences System, 1740 W Taylor St
Chicago, IL 60612, USA
*Author for correspondence:
For reprint orders, please contact: [email protected]
18 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
report of methods and outcomes of end-user engage-ment to develop an asthma discharge tool tailored to high-risk children for a comparative effectiveness trial. We are now testing the effectiveness of the asthma dis-charge tool on implementation and clinical outcomes in the multicenter CHICAGO pragmatic clinical trial (ClinicalTrials.gov NCT02319967) [9].
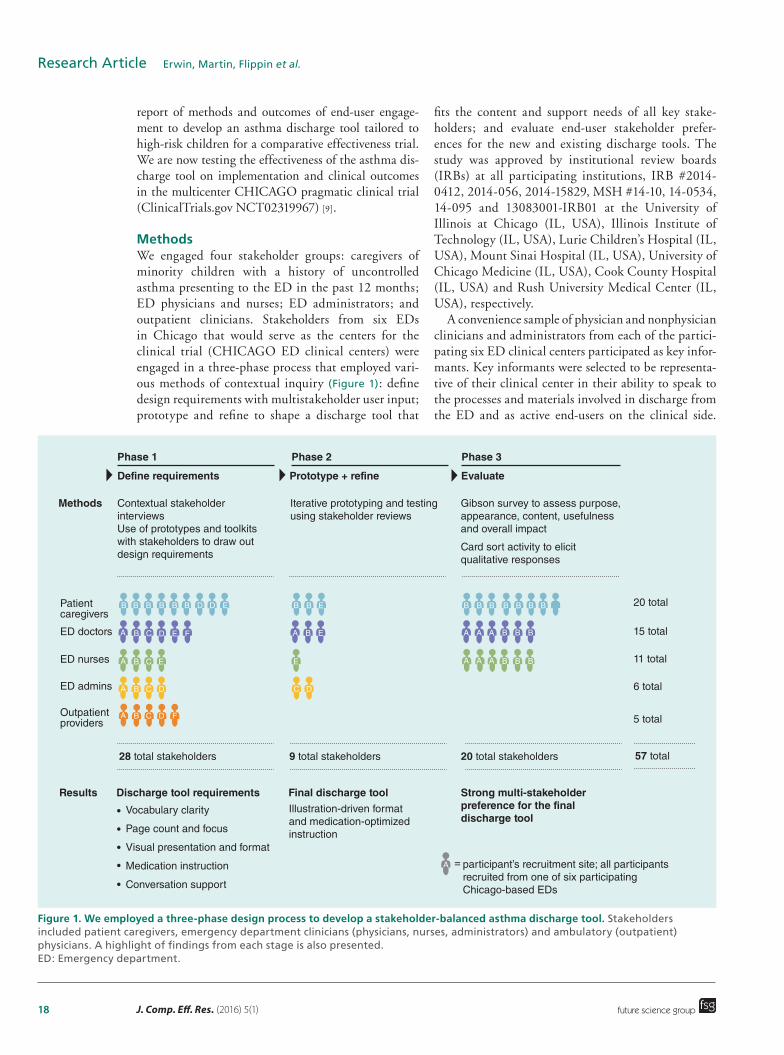
MethodsWe engaged four stakeholder groups: caregivers of minority children with a history of uncontrolled asthma presenting to the ED in the past 12 months; ED physicians and nurses; ED administrators; and outpatient clinicians. Stakeholders from six EDs in Chicago that would serve as the centers for the clinical trial (CHICAGO ED clinical centers) were engaged in a three-phase process that employed vari-ous methods of contextual inquiry (Figure 1): define design requirements with multistakeholder user input; prototype and refine to shape a discharge tool that
fits the content and support needs of all key stake-holders; and evaluate end-user stakeholder prefer-ences for the new and existing discharge tools. The study was approved by institutional review boards (IRBs) at all participating institutions, IRB #2014-0412, 2014-056, 2014-15829, MSH #14-10, 14-0534, 14-095 and 13083001-IRB01 at the University of Illinois at Chicago (IL, USA), Illinois Institute of Technology (IL, USA), Lurie Children’s Hospital (IL, USA), Mount Sinai Hospital (IL, USA), University of Chicago Medicine (IL, USA), Cook County Hospital (IL, USA) and Rush University Medical Center (IL, USA), respectively.
A convenience sample of physician and nonphysician clinicians and administrators from each of the partici-pating six ED clinical centers participated as key infor-mants. Key informants were selected to be representa-tive of their clinical center in their ability to speak to the processes and materials involved in discharge from the ED and as active end-users on the clinical side.
Figure 1. We employed a three-phase design process to develop a stakeholder-balanced asthma discharge tool. Stakeholders included patient caregivers, emergency department clinicians (physicians, nurses, administrators) and ambulatory (outpatient) physicians. A highlight of findings from each stage is also presented. ED: Emergency department.
Contextual stakeholderinterviewsUse of prototypes and toolkitswith stakeholders to draw outdesign requirements
28 total stakeholders
Results Discharge tool requirements Final discharge tool Strong multi-stakeholderpreference for the finaldischarge tool
9 total stakeholders
Illustration-driven formatand medication-optimizedinstruction
Vocabulary clarity
Page count and focus
Visual presentation and format
Medication instruction
Conversation support
participant’s recruitment site; all participantsrecruited from one of six participatingChicago-based EDs
=
20 total stakeholders 57 total
20 total
15 total
11 total
6 total
5 total
Iterative prototyping and testingusing stakeholder reviews
Patientcaregivers
ED doctors
ED nurses
ED admins
Outpatientproviders
Gibson survey to assess purpose,appearance, content, usefulnessand overall impact
Card sort activity to elicitqualitative responses
Methods
Phase 1 Phase 2 Phase 3
Define requirements Prototype + refine Evaluate
B
A
A
B
B C
A B C D
A B C D F
E
C D E F
BB B B B B
A B E
E
C D
B B
A
A A A
A A A
B B B
B B B
B B B
B B BED D E

www.futuremedicine.com 19
Figure 2. Sample projectives used with stakeholders in Phase I (from left to right): a caregiver-drawn asthma journey map; a physician-annotated prototype discharge tool; three sample discharge tools built by outpatient providers from a toolkit of preprinted sticky notes.
future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research Article
Similarly, a convenience sample of caregivers of black or Hispanic/Latino children who had visited at least one of the six ED clinical centers in the past 12 months participated in focus groups, user-centered home observations or both. Previous studies have established the critical role of triggers in the home environment and inadequate asthma controller use as risk factors for asthma exacerbations and emergency department visits in children with asthma. Thus, the asthma discharge tool included a focus on both environmental control and appropriate use of asthma medications [10–14].
Phase I: define design requirementsData collection in Phase I employed a user-centered design approach that combines field interviews con-ducted onsite in a user’s home or workplace with direct observation of users engaged in relevant tasks. These methods come from the field of design, which are not typically used in qualitative health research. The pri-mary difference is that design employs a contextual approach that focuses on context of use – not just a tool or its content – and conducts the inquiry using user-centered observations. [15]. Central to contextual inquiry is the belief that human actions can only prop-erly be understood in context, and that all activity is informed by immediate circumstances and therefore is best observed ‘in the wild’ rather than in a lab or through recounting past events with others in focus groups [16]. We, therefore, conducted all inquiry in clinical settings in the ED and ambulatory sites, and in the homes of caregivers. We also employed projectives, which in this study were prototype discharge docu-ments, toolkits from which physicians could construct their own discharge document and probes consisting of stakeholder-drawn visualizations of relevant past and present experiences of asthma management and ED experiences (Figure 2).
We conducted 19 key informant stakeholder interviews with physicians, nurses and administrators from the ED,
and outpatient clinicians. All interviews were conducted in the ED or ambulatory setting for 60–80 min. Two interviewers were present, and interviews were audio-recorded and photographed. The key informant protocol covered three domains: ED patient discharge experience using open-ended questions, discharge simulations and role play to target challenges and barriers in preparing a patient/caregiver for discharge; asthma treatment rec-ommendations on ED discharge, including barriers to implementing these components in their ED or practice; and prototype discharge tool review to elicit feedback about preferred discharge instructions.
We also conducted interviews with caregivers of African–American and Latino children with a his-tory of an ED visit for uncontrolled asthma in the past 12 months in one or more of the CHICAGO ED clinical centers. Eight of the caregivers were Afri-can–American and one was Latino, seven were single mothers, seven had other children and seven had other family members diagnosed with asthma. All interviews were conducted in the home and ranged from 2 to 3 h. They were audio-recorded and transcribed. A digital camera was used to document the home environment and location of relevant artifacts, such as storage of medications and discharge documents. Interviews tar-geted baseline asthma knowledge, self-management practices and recent ED discharge experience across four touchpoints – waiting, triage, treatment and dis-charge. The approach consisted of open-ended ques-tions, review of a prototype discharge document and use of multiple probes and activities to help caregivers express asthma care experiences.
All interview data were coded and analyzed using principles of Grounded Theory to identify recurring patterns of beliefs, interactions, behaviors and needs across stakeholder groups and clustered into design requirements and opportunity areas for concept devel-opment [17,18]. Analysts worked in pairs to ensure intercoder reliability (S Norell, J Rivera and T Flippin).

20 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
Phase II: prototype & refineA total of 9 caregivers, ED clinicians (physicians and nurses) and ED administrators were engaged in two iterations of assessment and refinement to converge on a single discharge tool that incorporated health literacy and information design principles (maximum Flesch–Kincaid 6th reading grade level; reduced word count, sentence length, text blocks and medical jargon; consistent use of typographic hierarchy and underlying grid; and key information presented in illustration and callouts) [19–24]. We also evaluated the Flesch–Kincaid reading level of existing discharge documents at the CHICAGO ED clinical centers. The CHICAGO investigators (clinicians, social scientists, community health workers and supervisors) then collaborated in providing feedback to the design team to finalize an asthma discharge tool for use in children presenting to the ED with uncontrolled asthma.
Phase III: evaluate stakeholder preferencesWe then assessed preferences among caregivers and ED clinicians by comparing the documents currently in use in two different CHICAGO ED clinical centers with the newly developed tool. We employed a published quantitative assessment tool (Gibson survey) that evalu-ates five domains (purpose, appearance, usefulness, overall impact and for clinicians, content) developed for patients/caregivers (15 items) and clinicians (30 items) [25]. Participants were asked to respond using a five-point Likert scale (strongly disagree to strongly agree); possible scores are 1–5, with higher scores indi-cating greater preference. To understand the rationale for preferences among caregivers and clinicians, we also employed qualitative methods using a card sorting activ-ity. Card sorting works to surface mental models and evaluate participant agreement by providing a stack of cards containing phrases or words and asking each par-ticipant to sort the cards into categories, as makes sense to them [26,27]. A total of 11 cards were presented to cli-nicians, with another 11 to caregivers. All cards were crafted with first-person statements, such as “I think this document provides more guidance for my patients after discharge” and were structured to capture both partici-pant behaviors and attitudes. Responses were tabulated and assessed for patterns across and within stakeholder segments using data visualization software Nineteen [28].
ResultsPhase I: define design requirementsWe conducted 28 on-site stakeholder interviews with nine caregivers, six ED physicians, four ED nurses, four ED administrators and five outpatient clinicians (Figure 1). Analysis of contextual research data pro-duced eight themes for in-home asthma management
practices and three themes related to ED discharge experiences (Table 1).
Tools to share information, coordinate careCaregivers expressed the need for a discharge tool that facilitates communication, education and coordina-tion of care with others (babysitters, extended family, school, daycare and camp personnel) who share in the care of their children.
Discharge information stored out of sightCurrent discharge documents are often stored in bags, drawers and with stacks of bills, so are not easily available for reference if needed. No caregiv-ers had asthma-related information on display in the home.
Learning through trial & error causes gaps in understanding even in experienced caregiversThe sheer number of contributing factors can make the logic of asthma exacerbations hard to piece together. While our caregivers reported prioritiz-ing their children’s health – by moving, leaving their jobs, delaying promotions to be more available to care for their children, vigorous cleaning or keeping kids inside – interviews suggested their management strat-egies are often based on an incomplete understanding of asthma. The resulting failure of proactive efforts can promote reactive behavior (i.e., ED visits).
Medication workaroundsMedication adherence is tough even for informed care-givers. Inhalers run out, causing families to share or to substitute reliever medicine. Because childcare usually occurs outside the home, shared inhalers must travel to multiple sites and return home without getting lost.
Medication confusionMany caregivers and outpatient clinicians reported confusion between reliever and controller inhalers. Caregivers also expressed distrust of continuous steroid use and potential side effects on their growing child, affecting their commitment to prescribed regimens.
Patient education positioned at the weakest momentDischarge protocols position patient education at the moment when patient caregivers are least prepared to take advantage of it – in the last 20 min of a typically 3–6 h (or longer) ED visit. Several nurses expressed frustration with caregivers’ unwillingness or inability to focus on patient education at discharge. Caregiv-ers also reported frustration related to lengthy dis-charge processes, repetition of information they say

www.futuremedicine.com 21future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research ArticleTa
ble
1. T
hem
es f
rom
co
nte
xtu
al r
esea
rch
in t
he
ho
me
and
em
erg
ency
dep
artm
ent
site
s.
Them
esD
etai
lsQ
uo
tes
1. T
oo
ls t
o s
har
e in
form
atio
n, c
oo
rdin
ate
care
Nee
d t
o e
du
cate
oth
ers
Nee
d t
o s
har
e in
form
atio
n“(
Yo
u n
eed
to
) n
ot
on
ly e
du
cate
yo
urs
elf,
bu
t to
ed
uca
te o
ther
s th
at y
ou
will
leav
e yo
ur
child
w
ith
fo
r lo
ng
per
iod
s –
bab
ysit
ters
, car
egiv
ers,
tea
cher
s” –
Car
egiv
er
“May
be
(we
cou
ld h
ave
) a
web
site
to
get
th
is a
ctio
n c
are
pla
n t
o p
rin
t o
ut
and
giv
e to
th
e sc
ho
ol
or
care
take
r? S
om
eth
ing
th
at y
ou
can
ed
uca
te s
om
ebo
dy
wit
h in
2 m
in?”
– C
areg
iver
2. D
isch
arg
e in
form
atio
n s
tore
d o
ut
of
sig
ht
Nee
d f
or
sim
plifi
ed in
stru
ctio
n
Sto
red
, no
t d
isp
laye
d
Rep
etit
ive
info
rmat
ion
ign
ore
d
“I k
eep
th
em in
a b
in w
her
e I k
eep
all
my
mai
l an
d s
tuff
. Th
en a
fter
a y
ear
or
two
, I g
o t
hro
ug
h
it, a
nd
wh
at e
ver
nee
ds
to b
e th
row
n o
ut,
I th
row
ou
t” –
Car
egiv
er
“It
is p
rett
y m
uch
du
plic
ates
of
wh
at w
e h
ave.
So
I h
ave
it p
iled
up
. I h
ave
a to
n o
f st
uff
to
sh
red
n
ow
” –
Car
egiv
er
3. L
earn
ing
th
rou
gh
tr
ial a
nd
err
or
cau
ses
gap
s in
un
der
stan
din
g
in e
ven
exp
erie
nce
d
care
giv
ers
Men
tal m
od
el o
f as
thm
a p
iece
d
tog
eth
er t
hro
ug
h t
rial
an
d e
rro
r,
per
son
al e
xper
ien
ce
Log
ic o
f as
thm
a h
ard
to
see
, pla
n
for
Wel
l-in
ten
ded
act
ion
s o
ften
in
effe
ctiv
e
“I h
op
e sh
e d
oes
no
t ca
tch
(an
ast
hm
a at
tack
) to
day
bec
ause
it is
rai
nin
g a
t o
ne
po
int,
th
en it
is
ho
t at
an
oth
er p
oin
t” –
Car
egiv
er
“Eve
ry t
ime
he
has
had
an
ast
hm
a at
tack
, it
has
bee
n d
iffe
ren
t si
tuat
ion
s. S
o w
e d
o n
ot
real
ly
kno
w w
hat
his
tri
gg
er is
. Th
e in
itia
l tim
e it
was
fre
sh c
ut
gra
ss t
hat
set
him
off
. It
has
bee
n a
ch
ang
e o
f te
mp
erat
ure
, it
has
bee
n if
yo
u s
pra
y so
met
hin
g, i
f h
e h
as b
een
aro
un
d s
om
ebo
dy
wit
h a
co
ld. A
nd
so
it is
ver
y h
ard
to
say
, oka
y, w
hat
tri
gg
ered
it t
his
tim
e?”
– C
areg
iver
“G
erm
s ar
e a
trig
ger
… s
o I
clea
n. I
ble
ach
. I a
m a
ble
ach
fan
atic
” –
Car
egiv
er
4. M
edic
atio
n
wo
rkar
ou
nd
s
Inh
aler
s d
o n
ot
last
as
lon
g a
s th
ey
sho
uld
Fa
mili
es s
har
e in
hal
ers
Sub
stit
ute
wit
h ‘r
escu
e’ m
edic
ine
inh
aler
s n
eed
to
tra
vel
“If
my
son
use
s u
p t
he
inh
aler
wit
hin
2 o
r 3
wee
ks,
wh
at a
m I
sup
po
sed
to
do
fo
r th
e o
ther
w
eek?
Bec
ause
yo
u h
ave
4 w
eek
s in
th
e m
on
th”
– C
areg
iver
“M
y m
om
is a
n a
sth
mat
ic, s
o w
e w
ill g
o t
o h
er h
ou
se a
nd
get
so
me
asth
ma
spra
y (w
hen
ou
rs
run
s o
ut)
” –
Car
egiv
er
“If
we
are
ou
t, I
hav
e n
o c
ho
ice
bu
t to
use
th
e re
scu
e in
hal
er”
– C
areg
iver
“I
hav
e vi
sits
wh
ere
…th
ey a
re b
rin
gin
g t
he
bab
ysit
ter
and
th
e g
ran
dm
a an
d t
he
dad
an
d t
he
mo
m. A
nd
th
ey a
re t
ryin
g t
o fi
gu
re o
ut
ho
w t
hey
are
go
ing
to
tra
nsf
er t
he
kid
s’ m
edic
atio
ns
bet
wee
n a
ll th
ese
site
s”–
Ou
tpat
ien
t p
rovi
der
5. M
edic
atio
n c
on
fusi
on
In
hal
er m
ix-u
ps
Med
icat
ion
nam
es s
ou
nd
alik
e ‘B
ette
r =
cu
red
’
“Fas
t ac
tin
g o
r re
scu
e m
edic
atio
n?
Ho
nes
tly?
I n
ever
kn
ew w
hat
th
e co
ntr
olle
r m
edic
ine
was
to
w
hat
is a
res
cue
med
icin
e” –
Car
egiv
er
“Th
is P
rove
nti
l so
un
ds
like
pre
ven
tati
ve. S
o I
mig
ht
hav
e sa
id t
ake
Flo
ven
t, t
he
ora
ng
e p
um
p…
and
th
e p
atie
nt
com
es b
ack
wit
h a
yel
low
an
d o
ran
ge
Pro
ven
til p
um
p a
nd
say
s ye
ah, t
his
is t
he
pre
ven
t o
ne.
I ta
ke t
wo
pu
ffs
ever
y m
orn
ing
an
d t
wo
pu
ffs
ever
y n
igh
t. I
am li
ke n
o!
I can
no
t ev
en t
ell y
ou
ho
w m
any
tim
es t
hat
has
hap
pen
ed”
– O
utp
atie
nt
pro
vid
er
“W
hen
th
ey fi
rst
sen
t h
im h
om
e w
ith
th
e m
edic
atio
n I
was
like
I am
no
t g
ivin
g h
im a
ll th
at
med
icat
ion
all
the
tim
e, h
e d
oes
no
t n
eed
it”
– C
areg
iver
6. P
atie
nt
edu
cati
on
p
osi
tio
ned
at
the
wea
kest
mo
men
t in
d
isch
arg
e
Car
egiv
er f
atig
ue
Rep
etit
ive
info
rmat
ion
N
egle
ctin
g o
ther
fam
ily
“Par
ents
do
no
t w
ant
to s
it h
ere
and
list
en t
o t
his
stu
ff w
hen
th
eir
rid
e is
wai
tin
g o
uts
ide
and
th
ey h
ave
alre
ady
bee
n h
ere
for
4–6
h, a
nd
th
ey a
re t
ired
an
d h
un
gry
an
d m
iser
able
an
d t
hei
r ki
d is
scr
eam
ing
”– E
D p
hys
icia
n
“Up
on
dis
char
ge,
th
ey g
ive
you
th
e w
ho
le w
ork
-up
– d
isch
arg
e in
stru
ctio
ns,
a n
um
ber
to
cal
l fo
r em
erg
enci
es, f
ollo
w-u
p a
pp
oin
tmen
ts, i
nfo
rmat
ion
on
ast
hm
a. T
hey
do
it e
very
tim
e. E
ven
if w
e ar
e so
use
d t
o t
he
info
rmat
ion
we
do
no
t n
eed
it a
ny
mo
re”
– C
areg
iver
“4
h is
th
e m
ost
we
hav
e st
ayed
th
ere.
I am
just
rea
dy
to g
o, b
ecau
se o
f th
e o
ther
th
ree
(kid
s) I
hav
e at
ho
me”
– C
areg
iver
ED: Emergency department.

22 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
they already know, and the need to manage work, other children and household obligations reduces receptivity to education at discharge.
Fragmented discharge experienceOperational realities can produce an ED discharge experience that is executed piecemeal and by multiple staff members. For example, sometimes the attending physician delivers medication instruction, a resident attempts patient education and a nurse prints and delivers paperwork. This workflow may change based on the number of patients waiting to be seen or acuity of illness among patients in the ED – the pressure to ‘treat and street’ was noted as a driver of practice vari-ation. Clinical staff reported that continuity and pre-dictability in discharge is difficult to provide using hand-offs, especially in EDs where poor site lines can limit communication between staff.
Clinician/caregiver conversations not well-supported by existing toolsCaregivers often receive large amounts of information at an ED visit. Clinic staff across sites reported numer-ous challenges in communicating that information to caregivers in the ED. Many staff said they do not review discharge documents with patients, as time is tight and documents are long, complicated and hard to use with caregivers.
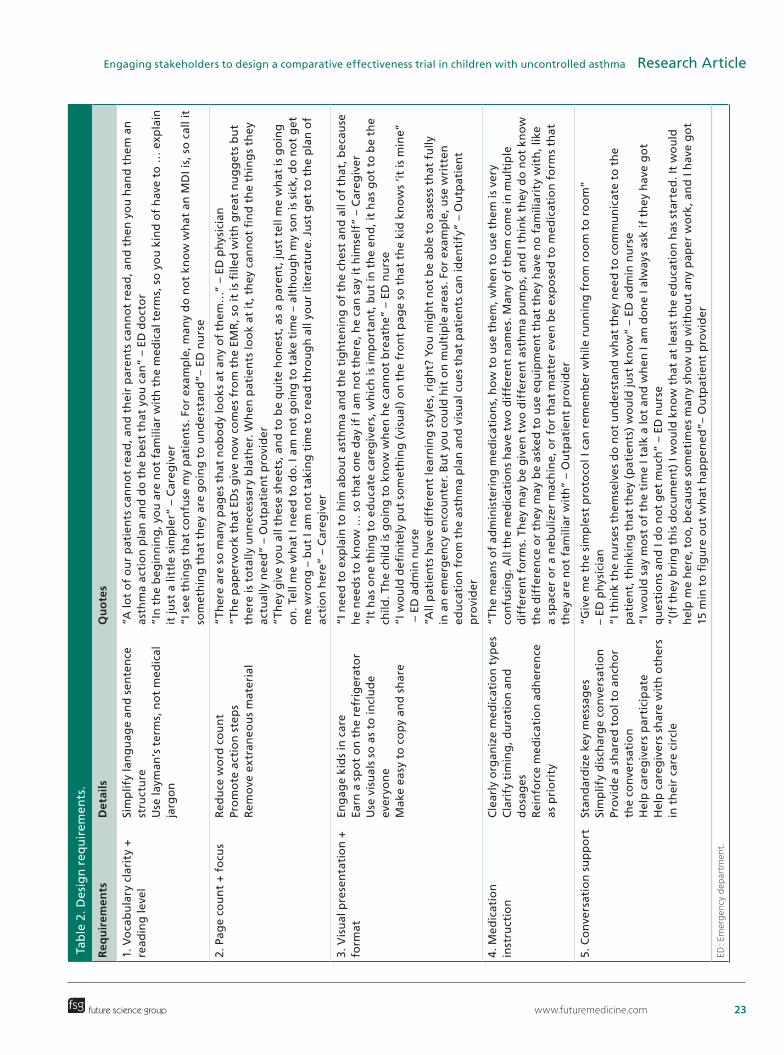
Stakeholder input regarding the design of the dis-charge tool identified several design priorities for the discharge tool (Table 2).
Vocabulary clarity + reading levelReduce complexity and simplify language to include children, more caregivers and others outside the family.
Page count & focusRemove extraneous content and streamline to focus on caregiver action steps.
Visual presentation & formatUse illustrations and layout to make key ideas acces-sible and inclusive, while retaining a professional and serious appearance.
Medication instructionOrganize, clarify and detail all medication-related instruction so as to create a plan that caregivers can understand and follow.
Conversation supportSimplify and structure the protocol for clinicians, support discussion of sensitive topics and make a tool caregivers can use with others.Th
emes
Det
ails
Qu
ote
s
7. F
rag
men
ted
dis
char
ge
pro
cess
‘T
reat
an
d s
tree
t’
Dis
char
ge
dis
trib
ute
d a
cro
ss s
taff
St
aff
han
d-o
ff a
llow
s in
form
atio
n
to s
lip t
hro
ug
h t
he
crac
ks
“No
rmal
ly, t
he
nu
rse
will
co
me
bac
k…w
ith
th
e p
resc
rip
tio
ns
and
fu
rth
er in
stru
ctio
ns.
Fir
st t
he
do
cto
r al
way
s co
mes
in a
nd
say
s w
hat
ever
, th
en t
he
nu
rse
is t
he
on
e w
ho
co
mes
bac
k an
d g
ives
yo
u y
ou
r d
isch
arg
e” –
Car
egiv
er
”Mu
ltip
le p
rofe
ssio
nal
s co
uld
be
resp
on
sib
le f
or
(dis
char
ge
), y
ou
kn
ow
, so
wh
en m
ult
iple
peo
ple
co
uld
be
invo
lved
, if
each
of
tho
se p
eop
le is
med
iocr
e, y
ou
co
uld
get
dis
char
ged
wit
h p
aper
wo
rk
that
say
s n
oth
ing
” –
ED n
urs
e
8. C
linic
ian
, car
egiv
er
con
vers
atio
ns
no
t w
ell-
sup
po
rted
by
too
ls
Too
ls a
re d
ense
, tex
t-h
eavy
, har
d
to u
se
Co
nve
rsat
ion
is t
he
edu
cati
on
al
tou
chp
oin
t
“Mo
st o
f th
e ti
me
I do
no
t p
ay v
ery
mu
ch a
tten
tio
n t
o t
he
dis
char
ge
pap
er b
ecau
se it
off
ers
me
no
thin
g. I
can
no
t im
agin
e th
at it
off
ers
mu
ch t
o t
he
pat
ien
t” –
ED
nu
rse
”It
get
s to
be
15 p
ages
…yo
u h
and
th
is t
o t
hem
an
d t
hey
are
like
, ‘W
hat
is a
ll th
is s
tuff
?’ I
f th
ere
is s
om
eth
ing
imp
ort
ant,
I tr
y to
cir
cle
it”
– ED
ph
ysic
ian
”W
e d
o n
ot
hav
e g
oo
d e
du
cati
on
to
ols
, an
d e
very
thin
g f
alls
bac
k to
th
e n
urs
e at
th
e en
d o
f th
e lin
e” –
ED
nu
rse
”Th
e va
lue
in a
dis
char
ge
do
cum
ent…
is t
he
teac
hin
g t
hat
hap
pen
s w
hen
yo
u a
re g
ivin
g t
he
do
cum
ent.
Th
e d
ocu
men
t sh
ou
ld b
e a
teac
hin
g t
oo
l, n
ot
on
ly ‘
the
thin
g y
ou
rec
eive
” –
Ou
tpat
ien
t p
rovi
der
ED: Emergency department.
Tab
le 1
. Th
emes
fro
m c
on
text
ual
res
earc
h in
th
e h
om
e an
d e
mer
gen
cy d
epar
tmen
t si
tes
(co
nt.
).
www.futuremedicine.com 23future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research ArticleTa
ble
2. D
esig
n r
equ
irem
ents
.
Req
uir
emen
tsD
etai
lsQ
uo
tes
1. V
oca
bu
lary
cla
rity
+
read
ing
leve
l Si
mp
lify
lan
gu
age
and
sen
ten
ce
stru
ctu
re
Use
laym
an’s
ter
ms,
no
t m
edic
al
jarg
on
“A lo
t o
f o
ur
pat
ien
ts c
ann
ot
read
, an
d t
hei
r p
aren
ts c
ann
ot
read
, an
d t
hen
yo
u h
and
th
em a
n
asth
ma
acti
on
pla
n a
nd
do
th
e b
est
that
yo
u c
an”
– ED
do
cto
r ”I
n t
he
beg
inn
ing
, yo
u a
re n
ot
fam
iliar
wit
h t
he
med
ical
ter
ms,
so
yo
u k
ind
of
hav
e to
… e
xpla
in
it ju
st a
litt
le s
imp
ler”
– C
areg
iver
”I
see
th
ing
s th
at c
on
fuse
my
pat
ien
ts. F
or
exam
ple
, man
y d
o n
ot
kno
w w
hat
an
MD
I is,
so
cal
l it
som
eth
ing
th
at t
hey
are
go
ing
to
un
der
stan
d”–
ED
nu
rse
2. P
age
cou
nt
+ f
ocu
s
Red
uce
wo
rd c
ou
nt
Pro
mo
te a
ctio
n s
tep
s R
emo
ve e
xtra
neo
us
mat
eria
l
“Th
ere
are
so m
any
pag
es t
hat
no
bo
dy
loo
ks
at a
ny
of
them
…”
– ED
ph
ysic
ian
”T
he
pap
erw
ork
th
at E
Ds
giv
e n
ow
co
mes
fro
m t
he
EMR
, so
it is
fille
d w
ith
gre
at n
ug
get
s b
ut
ther
e is
to
tally
un
nec
essa
ry b
lath
er. W
hen
pat
ien
ts lo
ok
at it
, th
ey c
ann
ot
fin
d t
he
thin
gs
they
ac
tual
ly n
eed
” –
Ou
tpat
ien
t p
rovi
der
”T
hey
giv
e yo
u a
ll th
ese
shee
ts, a
nd
to
be
qu
ite
ho
nes
t, a
s a
par
ent,
just
tel
l me
wh
at is
go
ing
o
n. T
ell m
e w
hat
I n
eed
to
do
. I a
m n
ot
go
ing
to
tak
e ti
me
– al
tho
ug
h m
y so
n is
sic
k, d
o n
ot
get
m
e w
ron
g –
bu
t I a
m n
ot
taki
ng
tim
e to
rea
d t
hro
ug
h a
ll yo
ur
liter
atu
re. J
ust
get
to
th
e p
lan
of
acti
on
her
e” –
Car
egiv
er
3. V
isu
al p
rese
nta
tio
n +
fo
rmat
En
gag
e ki
ds
in c
are
Earn
a s
po
t o
n t
he
refr
iger
ato
r U
se v
isu
als
so a
s to
incl
ud
e ev
eryo
ne
Mak
e ea
sy t
o c
op
y an
d s
har
e
“I n
eed
to
exp
lain
to
him
ab
ou
t as
thm
a an
d t
he
tig
hte
nin
g o
f th
e ch
est
and
all
of
that
, bec
ause
h
e n
eed
s to
kn
ow
… s
o t
hat
on
e d
ay if
I am
no
t th
ere,
he
can
say
it h
imse
lf”
– C
areg
iver
”I
t h
as o
ne
thin
g t
o e
du
cate
car
egiv
ers,
wh
ich
is im
po
rtan
t, b
ut
in t
he
end
, it
has
go
t to
be
the
child
. Th
e ch
ild is
go
ing
to
kn
ow
wh
en h
e ca
nn
ot
bre
ath
e” –
ED
nu
rse
”I w
ou
ld d
efin
itel
y p
ut
som
eth
ing
(vi
sual
) o
n t
he
fro
nt
pag
e so
th
at t
he
kid
kn
ow
s ‘it
is m
ine”
–
ED
ad
min
nu
rse
”All
pat
ien
ts h
ave
dif
fere
nt
lear
nin
g s
tyle
s, r
igh
t? Y
ou
mig
ht
no
t b
e ab
le t
o a
sses
s th
at f
ully
in
an
em
erg
ency
en
cou
nte
r. B
ut
you
co
uld
hit
on
mu
ltip
le a
reas
. Fo
r ex
amp
le, u
se w
ritt
en
edu
cati
on
fro
m t
he
asth
ma
pla
n a
nd
vis
ual
cu
es t
hat
pat
ien
ts c
an id
enti
fy”
– O
utp
atie
nt
pro
vid
er
4. M
edic
atio
n
inst
ruct
ion
C
lear
ly o
rgan
ize
med
icat
ion
typ
es
Cla
rify
tim
ing
, du
rati
on
an
d
do
sag
es
Rei
nfo
rce
med
icat
ion
ad
her
ence
as
pri
ori
ty
“Th
e m
ean
s o
f ad
min
iste
rin
g m
edic
atio
ns,
ho
w t
o u
se t
hem
, wh
en t
o u
se t
hem
is v
ery
con
fusi
ng
. All
the
med
icat
ion
s h
ave
two
dif
fere
nt
nam
es. M
any
of
them
co
me
in m
ult
iple
d
iffe
ren
t fo
rms.
Th
ey m
ay b
e g
iven
tw
o d
iffe
ren
t as
thm
a p
um
ps,
an
d I
thin
k th
ey d
o n
ot
kno
w
the
dif
fere
nce
or
they
may
be
aske
d t
o u
se e
qu
ipm
ent
that
th
ey h
ave
no
fam
iliar
ity
wit
h, l
ike
a sp
acer
or
a n
ebu
lizer
mac
hin
e, o
r fo
r th
at m
atte
r ev
en b
e ex
po
sed
to
med
icat
ion
fo
rms
that
th
ey a
re n
ot
fam
iliar
wit
h”
– O
utp
atie
nt
pro
vid
er
5. C
on
vers
atio
n s
up
po
rt
Stan
dar
diz
e ke
y m
essa
ges
Si
mp
lify
dis
char
ge
con
vers
atio
n
Pro
vid
e a
shar
ed t
oo
l to
an
cho
r th
e co
nve
rsat
ion
H
elp
car
egiv
ers
par
tici
pat
e H
elp
car
egiv
ers
shar
e w
ith
oth
ers
in t
hei
r ca
re c
ircl
e
“Giv
e m
e th
e si
mp
lest
pro
toco
l I c
an r
emem
ber
wh
ile r
un
nin
g f
rom
ro
om
to
ro
om
”
– ED
ph
ysic
ian
”I
th
ink
the
nu
rses
th
emse
lves
do
no
t u
nd
erst
and
wh
at t
hey
nee
d t
o c
om
mu
nic
ate
to t
he
pat
ien
t, t
hin
kin
g t
hat
th
ey (
pat
ien
ts)
wo
uld
just
kn
ow
” –
ED a
dm
in n
urs
e
“I w
ou
ld s
ay m
ost
of
the
tim
e I t
alk
a lo
t an
d w
hen
I am
do
ne
I alw
ays
ask
if t
hey
hav
e g
ot
qu
esti
on
s an
d I
do
no
t g
et m
uch
” –
ED n
urs
e ”(
If t
hey
bri
ng
th
is d
ocu
men
t) I
wo
uld
kn
ow
th
at a
t le
ast
the
edu
cati
on
has
sta
rted
. It
wo
uld
h
elp
me
her
e, t
oo
, bec
ause
so
met
imes
man
y sh
ow
up
wit
ho
ut
any
pap
er w
ork
, an
d I
hav
e g
ot
15 m
in t
o fi
gu
re o
ut
wh
at h
app
ened
”– O
utp
atie
nt
pro
vid
er
ED: Emergency department.

24 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
Phase II: prototype & refineNine stakeholders participated in prototype reviews (three caregivers; three ED physicians; one ED nurse and two ED administrators, Figure 1). In these reviews, stakeholders were presented with three potential dis-charge tool concepts based on Phase I results and were asked to engage in two cycles of review and collabora-tive editing (Figures 2 & 3). Across stakeholder groups, highly-illustrated visual learning concepts earned the strongest favorable responses for its simplicity, clarity, visual appeal and ease of use. Literacy levels of patients and caregivers were a recurring topic in the formative research. Many ED physicians asked for solutions that used visual strategies to offset the complexity of text. ED nurses sought tools that could engage children directly in self-management. Caregivers also expressed confusion and impatience with materials that were hard to read, apply and share. In response, we custom-ized illustrations to explain key vocabulary and self-management concepts and employed the traffic light construct of green/yellow/red zones to aid caregiver assessment. The final CHICAGO asthma discharge tool, called the CAPE (CHICAGO Action Plan after ED discharge) (Figure 4), has a Flesch–Kincaid read-ing level of 4.7 (compared with existing documents in use across the CHICAGO ED clinical centers that had reading levels of 5.5–7.8). The final discharge tool is also designed to support simplified reading strategies by using multiple principles of information design, such as typographic hierarchy to create prior-ity and aid browsing, use of an underlying grid and white space to reduce visual complexity, reduced line length and text blocks to increase readability and the
option for printing or copying in black and white for low-cost distribution.
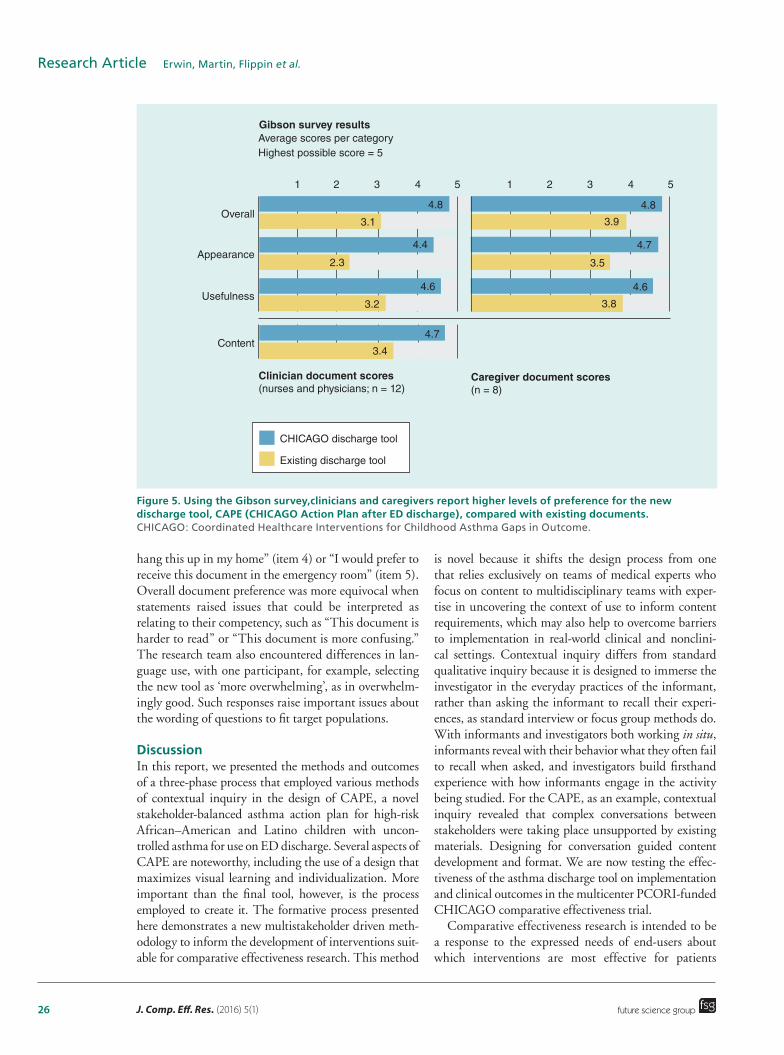
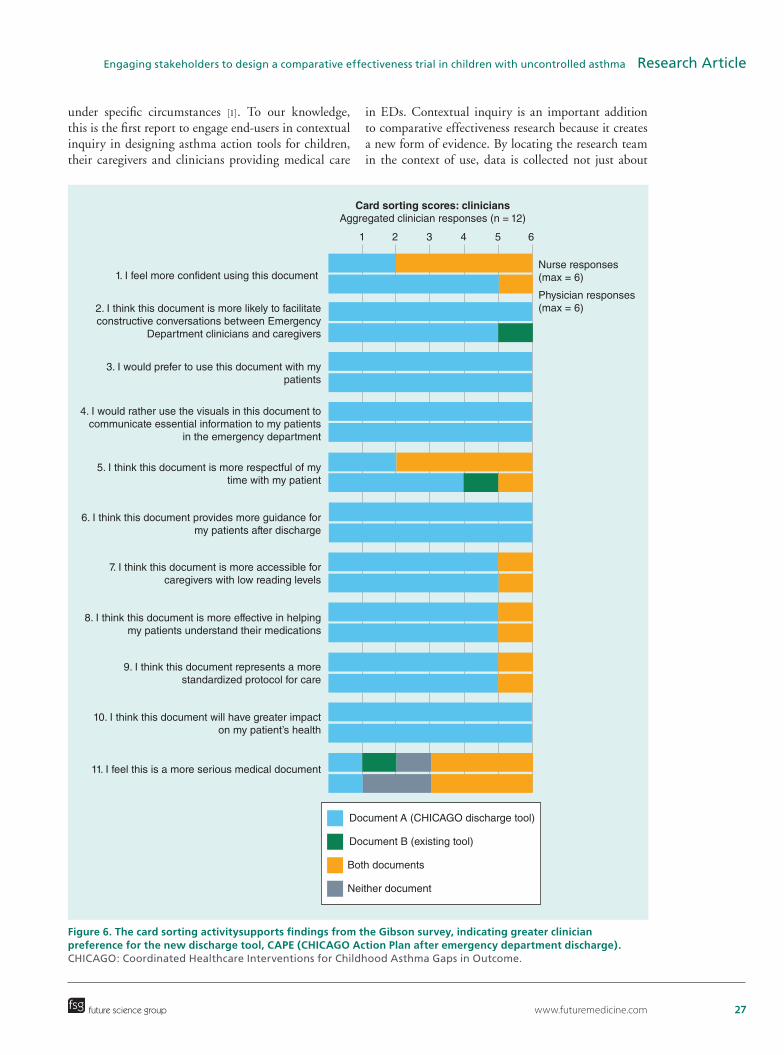
Phase III: evaluate stakeholder preferencesResults of the Gibson survey suggested caregiver and clinician preference for the new discharge tool across all categories (Figure 5). Qualitative assessments using the card sorting activity also demonstrated a preference for the new discharge tool (Figure 6). Among clinicians, the card sorting activity elicited strong emotional responses as they shared their frustrations over their current asthma action plans. There was full consen-sus for the new tool for four of eleven questions (items 3, 4, 6 and 10). Clinicians reported that they favored the new tool in part because of its clarity; one physi-cian observed that “for our patient population, this is awesome…it is not too dense, and it is not word over-loaded. This is very succinct. It is easy to understand.” Clinicians also indicated that the new tool could serve as a support for conversations and for teaching self-management. One clinician noted that the new tool was ‘more interactive, so as you go through it people will have a visual and can ask questions’, whereas when using the existing document ‘there is not as much to go through, step-wise, so its less likely that you are going to be able to point and continue a dialog based on what is in the document’.
Caregiver responses also demonstrated a preference for the new discharge tool (Figure 7). However, caregiver responses were strongest for the new tool when queried about behavioral items, such as “This document is more clear about which actions I should take after the Emer-gency Department” (item 3) or “I am more likely to
Figure 3. In Phase II, an early prototype was refined through iterative stakeholder input to develop a new discharge tool, CAPE (CHICAGO Action Plan after emergency department discharge). CHICAGO: Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcome; QR: Quick response.
An early-stage prototype...
1. Digital resource focused A stakeholder balanced solution
Includes QR codes that linkto online asthma content tobetter accommodate differinglevels of caregiver expertise
Structured around four action steps
Illustration-driven format fromprototype 3 with supporting textat a reading grade level of 4.7(Flesch–Kincaid)
Also integrates stakeholderpreferred medication instructionfrom prototype 2 and a digitallink from prototype 1
Dedicates an entire page toclarifying inhaler types andmedication regimen
Uses illustration to representkey vocabulary and self-management conceptsto address low-literacypopulations and children
2. Medication optimized
3. Visual learning focused
Drafted collaboratively byCHICAGO Plan investigators;
Organizes content into four clearaction steps:
1. Take medication2. Follow-up with provider3. Recognize symptoms4. Stay on top of asthma (self-management instruction)
...informs three new prototypes ...refined into a finaldischarge tool
www.futuremedicine.com 25future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research Article
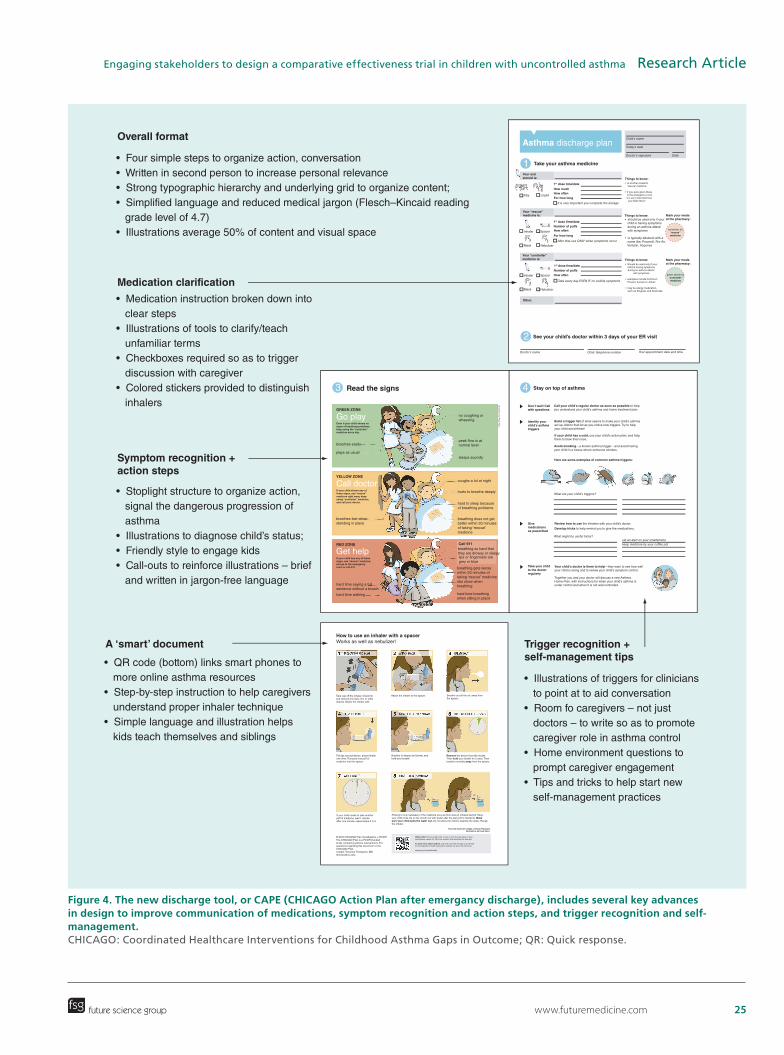
Figure 4. The new discharge tool, or CAPE (CHICAGO Action Plan after emergancy discharge), includes several key advances in design to improve communication of medications, symptom recognition and action steps, and trigger recognition and self-management. CHICAGO: Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcome; QR: Quick response.
Overall format
Medication clarification
Trigger recognition +self-management tips
A ‘smart’ document
Symptom recognition +action steps
• Four simple steps to organize action, conversation• Written in second person to increase personal relevance• Strong typographic hierarchy and underlying grid to organize content;• Simplified language and reduced medical jargon (Flesch–Kincaid reading grade level of 4.7) • Illustrations average 50% of content and visual space
• Medication instruction broken down into clear steps• Illustrations of tools to clarify/teach unfamiliar terms• Checkboxes required so as to trigger discussion with caregiver• Colored stickers provided to distinguish inhalers
• Stoplight structure to organize action, signal the dangerous progression of asthma• Illustrations to diagnose child’s status;• Friendly style to engage kids• Call-outs to reinforce illustrations – brief and written in jargon-free language
• QR code (bottom) links smart phones to more online asthma resources• Step-by-step instruction to help caregivers understand proper inhaler technique• Simple language and illustration helps kids teach themselves and siblings
• Illustrations of triggers for clinicians to point at to aid conversation• Room fo caregivers – not just doctors – to write so as to promote caregiver role in asthma control• Home environment questions to prompt caregiver engagement• Tips and tricks to help start new self-management practices
2
GREEN ZONE
YELLOW ZONE
Call 911RED ZONE
How to use an inhaler with a spacerWorks as well as nebulizer!
Even if your child shows nosigns of breathing problems,keep using the “controller”medicine every day.
breathes easily
plays as usual
breathes fast whenstanding in place
Go play
Call doctor
Get help
If your child shows any ofthese signs, use “rescue”medicine right away, keepusing “controller” medicine,and call your doctor.
If your child has any of thesesigns, use “rescue” medicine,and go to the emergencyroom or call 911.
hard time saying a fullsentence without a breath
hard time walking
no coughing orwheezing
peak flow is atnormal level
sleeps soundly
coughs a lot at night
hurts to breathe deeply
hard to sleep becauseof breathing problems
breathing does not getbetter within 20 minutesof taking “rescue”medicine
breathing so hard thatthey are drowsy or sleepylips or fingernails aregrey or blue
breathing gets worsewithin 20 minutes oftaking “rescue” medicineribs show whenbreathing
hard time breathingwhen sitting in place
Take cap off the inhaler. Check forand remove any dust, lint, or otherobjects. Shake the inhaler well.
Put lips around device, press inhalerone time. This puts one puff of medicine into the spacer.
If your child needs to take anotherpuff of medicine, wait 1 minute. After one minute, repeat steps 3 to 6.
© 2015 CHICAGO Plan investigators + PCOR1The CHICAGO Plan is a PCOR1-fundedstudy comparing asthma interventions. Forquestions regarding this document or theCHICAGO Plan.contact: Trevonne Thompson, [email protected]
Breathe in deeply and slowly, andhold your breath.
Attach the inhaler to the spacer. Breathe out all the air, away fromthe spacer.
Remove the device from the mouth. Then hold your breath for 5 secs. Thenbreathe normally away from the spacer.
Rinsing is only necessary if the medicine you just took was an inhaled steroid. Haveyour child rinse his or her mouth out with water after the last puff of medicine. Makesure your child spits the water out. Do not allow the child to swallow the water. Recapthe inhaler.
See your child’s doctor within 3 days of your ER visit
From the American College of Chest PhysiciansIllustrations by Paula Falco
1st dose time/date
1st dose time/date
How often
How often
For how long
It is very important you complete the dosage
After that, use ONLY when symptoms occur
Take every day EVEN IF no visibile symptoms
Number of puffs
Number of puffs
Things to know:
Things to know:
Things to know:
Mark your medsat the pharmacy:
Mark your medsat the pharmacy:
• is another powerful “rescue” medicine
• if you were given these in the emergency room, it is very important that
you finish them!
Doctor’s name
What are your child’s triggers?
What might be useful tricks?set an alert on your smartphonekeep medicine by your coffee pot
Clinic telephone number Your appointment date and time
Call your child’s regular doctor as soon as possible to helpyou understand your child’s asthma and home treatment plan.
Build a trigger list of what seems to make your child’s asthmaact up. Add to that list as you notice new triggers. Try to helpyour child avoid these!
If your child has a cold, use your child’s action plan; and helpthem to blow their nose.
Avoid smoking—a known asthma trigger—and avoid havingyour child in a house where someone smokes.
Here are some examples of common asthma triggers:
Review how to use the inhalers with your child’s doctor.
Develop tricks to help remind you to give the medications.
Your child’s doctor is there to help—they want to see how wellyour child is doing and to review your child’s symptom control.
Together you and your doctor will discuss a new AsthmaHome Plan, with instructions for when your child’s asthma isunder control and when it is not well-controlled.
• should be used only if your child is having symptoms during an asthma attack/ with symptoms
• is typically albuterol with a name like: Proventil, Pro-Air, Ventolin, Xopenex
Child’s name
Today’s date
Doctor’s signature Date
Other:
Your “controller”medicine is:
Your “rescue”medicine is:
red sticker for“rescue”medicine
green sticker for“controller”medicine
What is this? This is a QR code. To use it, go to the app store on yoursmartphone, search for ‘QR code readers’ and download the free app.
To learn more about asthma, scan this code with the app to go directlyto the Respiratory Health Association website. Or go to the link below:
www.tinyurl.com/asthmalib
Inhaler Spacer
Mask Nebulizer
3 Read the signs 4 Stay on top of asthma
1 Take your asthma medicine
Pills Liquid
1st dose time/date
How muchHow often
For how long
Your oralsteroid is:
Asthma discharge plan
Don’t wait! Callwith questions
Identify yourchild’s asthmatriggers
Givemedicationsas prescribed
Take your childto the doctorregularly
Inhaler Spacer
Mask Nebulizer
Illustrations by P
aula Falco
• Should be used only if yourchild is having symptomsduring an asthma attack/
with symptoms
• examples include Pulmicort, Flovent, Azmacort, Advair
• may be allergy medication, such as Singulair and Associate
26 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
hang this up in my home” (item 4) or “I would prefer to receive this document in the emergency room” (item 5). Overall document preference was more equivocal when statements raised issues that could be interpreted as relating to their competency, such as “This document is harder to read” or “This document is more confusing.” The research team also encountered differences in lan-guage use, with one participant, for example, selecting the new tool as ‘more overwhelming’, as in overwhelm-ingly good. Such responses raise important issues about the wording of questions to fit target populations.
DiscussionIn this report, we presented the methods and outcomes of a three-phase process that employed various methods of contextual inquiry in the design of CAPE, a novel stakeholder-balanced asthma action plan for high-risk African–American and Latino children with uncon-trolled asthma for use on ED discharge. Several aspects of CAPE are noteworthy, including the use of a design that maximizes visual learning and individualization. More important than the final tool, however, is the process employed to create it. The formative process presented here demonstrates a new multistakeholder driven meth-odology to inform the development of interventions suit-able for comparative effectiveness research. This method
is novel because it shifts the design process from one that relies exclusively on teams of medical experts who focus on content to multidisciplinary teams with exper-tise in uncovering the context of use to inform content requirements, which may also help to overcome barriers to implementation in real-world clinical and nonclini-cal settings. Contextual inquiry differs from standard qualitative inquiry because it is designed to immerse the investigator in the everyday practices of the informant, rather than asking the informant to recall their experi-ences, as standard interview or focus group methods do. With informants and investigators both working in situ, informants reveal with their behavior what they often fail to recall when asked, and investigators build firsthand experience with how informants engage in the activity being studied. For the CAPE, as an example, contextual inquiry revealed that complex conversations between stakeholders were taking place unsupported by existing materials. Designing for conversation guided content development and format. We are now testing the effec-tiveness of the asthma discharge tool on implementation and clinical outcomes in the multicenter PCORI-funded CHICAGO comparative effectiveness trial.
Comparative effectiveness research is intended to be a response to the expressed needs of end-users about which interventions are most effective for patients
Figure 5. Using the Gibson survey,clinicians and caregivers report higher levels of preference for the new discharge tool, CAPE (CHICAGO Action Plan after ED discharge), compared with existing documents. CHICAGO: Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcome.
Gibson survey results
Overall
1
4.8
3.1
2.3
4.4
3.2
4.6
4.7
3.4
2 3 4 5 1 2 3
3.9
4
4.8
4.7
4.6
3.5
3.8
5
Appearance
Usefulness
Content
Clinician document scores(nurses and physicians; n = 12)
Caregiver document scores(n = 8)
Average scores per categoryHighest possible score = 5
CHICAGO discharge tool
Existing discharge tool
www.futuremedicine.com 27future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research Article
under specific circumstances [1]. To our knowledge, this is the first report to engage end-users in contextual inquiry in designing asthma action tools for children, their caregivers and clinicians providing medical care
in EDs. Contextual inquiry is an important addition to comparative effectiveness research because it creates a new form of evidence. By locating the research team in the context of use, data is collected not just about
Figure 6. The card sorting activitysupports findings from the Gibson survey, indicating greater clinician preference for the new discharge tool, CAPE (CHICAGO Action Plan after emergency department discharge). CHICAGO: Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcome.
1. I feel more confident using this document
Physician responses(max = 6)2. I think this document is more likely to facilitate
constructive conversations between EmergencyDepartment clinicians and caregivers
3. I would prefer to use this document with mypatients
4. I would rather use the visuals in this document tocommunicate essential information to my patients
in the emergency department
5. I think this document is more respectful of mytime with my patient
6. I think this document provides more guidance formy patients after discharge
7. I think this document is more accessible forcaregivers with low reading levels
8. I think this document is more effective in helpingmy patients understand their medications
9. I think this document represents a morestandardized protocol for care
10. I think this document will have greater impacton my patient’s health
11. I feel this is a more serious medical document
1 2 3 4 5 6
Nurse responses(max = 6)
Card sorting scores: cliniciansAggregated clinician responses (n = 12)
Document A (CHICAGO discharge tool)
Document B (existing tool)
Both documents
Neither document

28 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
patient practices, but how those practices are shaped by interactions with others, how practices become embed-ded (or not) in everyday activities and responsibilities and how practices are negotiated against the inevitable disruptors of everyday life that compete for patients’ time and attention. This evidence is especially produc-tive when seeking to tailor interventions to populations and circumstances for better uptake and adherence. Additionally, contextual inquiry is equally productive when applied to ED clinical staff, who report struggling
with tools and protocols that do not seem designed to fit the complex operational realities of the ED and its many users. Indeed, results of quantitative and qualita-tive assessments suggest substantial preference among clinical staff for the new tool’s ease of use and fit with desired caregiver conversations, compared with existing tools used in the ED.
By design, our new discharge tool shifts the commu-nication paradigm in the ED from delivery of informa-tion (from expert to novice) to supporting collaborative
Figure 7. The card sorting activitysupports findings from the Gibson survey,indicating greater caregiver preference for the new discharge tool. CHICAGO: Coordinated Healthcare Interventions for Childhood Asthma Gaps in Outcome
1. I think that with this document, my family wouldvisit the emergency department less
2. This document is easier to read
3. This document is more clear about which action Ishould take first after the emergency department
Negative assessmentstatements; lowerscores are better
Card sorting scores: caregiversAggregated caregiver responses (n = 8)
Responses
Positive assessmentstatements; higherscores are better
4. I am more likely to hang this document up inmy home
5. If I was in the emergency room with my child,I would prefer to receive this document
6. This document is more approachable
7. This document is more organized
8. This document is more worthy of my time
9. This document is better for my family
10. This document is more overwhelming
11. This document is more confusing
Document A (CHICAGO discharge tool)
Document B (existing tool)
Both documents
Neither document
1 2 3 4 5 6 7 8

www.futuremedicine.com 29future science group
Engaging stakeholders to design a comparative effectiveness trial in children with uncontrolled asthma Research Article
conversation (between equally engaged stakeholders). This is an important shift because it institutional-izes what some clinicians in this study have already acknowledged: that communication is more effective when built with caregivers through an exchange of information in the moment than ‘delivered’ to them in a monologue or handout. The new discharge tool was noted by clinical staff as a tool that ‘at least starts the conversation’, ‘opens up the conversation better’ and ‘is more interactive as you go through it with people’. Shifting to a collaborative model in the ED also creates new conditions that encourage caregivers to see them-selves as partners in asthma control. Current ED expe-riences contribute to caregiver belief that an asthma attack is an event best fixed by a doctor in an ED; a collaborative approach can stress asthma as a chronic condition best managed by caregivers at home.
While our project offers multiple strengths, our approach to engagement was limited to address-ing the needs of elementary school-age high-risk African–American and Latino children with uncon-trolled asthma presenting to the ED. This focus was deliberately given the goals of our PCORI-funded CHICAGO comparative effectiveness trial. However, the discharge tool may not be sufficiently optimized for other populations (e.g., preschoolers, adolescents, adults). While we did include physicians and nurses, our engagement process did not include other clini-cians who provide care to children with uncontrolled asthma (e.g., respiratory therapists, social work-ers, pharmacists). Moreover, most of our children and their caregivers were low income and African–American. The methods employed in this project offer a template for future work that could address the needs of other end-user populations, including those with other conditions (e.g., diabetes, hypertension, sickle cell disease).
ConclusionWe present the application of contextual inquiry of end-user stakeholders to design a novel ED-based asthma action plan (CAPE) for a comparative effectiveness trial
in asthma. We speculate that engaging multiple stake-holders in the design of a discharge tool ‘fit for purpose’ offers a promising approach for improving asthma self-management skills and improving asthma outcomes in African–American and Latino children presenting to the ED for uncontrolled asthma. Our on-going PCORI-funded CHICAGO comparative effectiveness trial will evaluate the effects of employing CAPE (vs usual care) in the ED on implementation and clinical outcomes.
AcknowledgementsThe authors gratefully acknowledge the help of T MacTav-
ish, IIT Institute of Design; JT Senko, JH Stroger, Jr Hospital of
Cook County; CJ Lohff, Chicago Department of Public Health;
ZE Pittsenbarger, Ann and Robert H Lurie Children’s Hospital
of Chicago; J E Kramer, Rush University Medical Center; H
Margellos-Anast, LS Zun, Mount Sinai Hospital; SM Paik and
J Solway, University of Chicago; ML Berbaum, N Bracken, and
HA Gussin, for their role in the development of the CHICAGO
comparative effectiveness trial. The authors thank L Sanker for
her help in the development and conduct of focus groups. The
authors also thank the families and the staff in the CHICAGO
ED clinical centers and partner organizations who contributed
their time to make this study possible.
Financial & competing interests disclosureThe study was sponsored by the Patient-Centered Outcomes
Research Institute (contract #AS-1307-05420). The authors
have no other relevant affiliations or financial involvement
with any organization or entity with a financial interest in or fi-
nancial conflict with the subject matter or materials discussed
in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this
manuscript.
Ethical conduct of researchThe authors state that they have obtained appropriate institu-
tional review board approval or have followed the principles
outlined in the Declaration of Helsinki for all human or animal
experimental investigations. In addition, for investigations in-
volving human subjects, informed consent has been obtained
from the participants involved.
Executive summary
Designing interventions to improve communication in comparative effectiveness research• Multistakeholder driven design methods of contextual inquiry can be successfully employed to inform the
development of interventions for comparative effectiveness research.• Our approach shifted the design process from one that relies exclusively on teams of medical experts who
focus on content to multidisciplinary teams with expertise in uncovering the context of use to inform content requirements, which may also help to overcome barriers to implementation in real-world clinical and nonclinical settings.
• The new discharge tool or CAPE (CHICAGO Action Plan after emergency department discharge) shifts the communicationparadigm in the emergency department from delivery of information (from expert to novice) to supporting collaborative conversation (between equally-engaged stakeholders).

30 J. Comp. Eff. Res. (2016) 5(1) future science group
Research Article Erwin, Martin, Flippin et al.
References1 Comparative Effectiveness Research: National Institutes of
Health. PCAST Session on Health Reform and CER (2009). www.whitehouse.gov
2 National Institutes of Health/National Heart, Lung, and Blood Institute. Expert Panel Report 3: guidelines on asthma. www.nhlbi.nih.gov/health-pro
3 Global Initiative for Asthma (GINA). www.ginasthma.org/
4 Gupta S, Wan FT, Ducharme FM, Chignell MH, Lougheed MD, Straus SE. Asthma action plans are highly variable and do not conform to best visual design practices. Ann. Allergy Asthma Immunol. 108(4), 260–265 (2012).
5 Ring N, Jepson R, Hoskins G, et al. Understanding what helps or hinders asthma action plan use: a systematic review and synthesis of the qualitative literature. Patient Educ. Couns. 85(2), e131–e143 (2011).
6 Patient-Centered Outcomes Research Institute. www.pcori.org/research-results/2013
7 Gupta RS, Zhang X, Sharp LK, Shannon JJ, Weiss KB. Geographic variability in childhood asthma prevalence in Chicago. J. Allergy Clin. Immunol. 121(3), 639–645 (2008).
8 Martin B, Hanington B. Universal Methods of Design: 100 Ways to Research Complex Problems, Develop Innovative Ideas and Design Effective Solutions. Rockport Publishers, MA, USA (2012).
9 Proctor E, Silmere H, Raghavan R et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm. Policy Ment. Health. 38(2), 65–76 (2011).
10 Eggleston PA, Diette G, Lipsett M et al. Lessons learned for the study of childhood asthma from the Centers for Children’s Environmental Health and Disease Prevention Research. Environ Health Perspect. 113(10), 1430–1436 (2005).
11 Swartz LJ, Callahan KA, Butz AM et al. Methods and issues in conducting a community-based environmental randomized trial. Environ. Res. 95(2), 156–165 (2004).
12 Eggleston PA, Butz A, Rand C et al. Home environmental intervention in inner-city asthma: a randomized controlled clinical trial. Ann. Allergy Asthma Immunol. 95(6), 518–524 (2005).
13 Al-Muhsen S, Horanieh N, Dulgom S et al. Poor asthma education and medication compliance are associated with increased emergency department visits by asthmatic children. Ann Thorac Med. 10(2), 123–131 (2015).
14 Adams RJ, Fuhlbrigge A, Finkelstein JA et al. Impact of inhaled anti-inflammatory therapy on hospitalization and
emergency department visits for children with asthma. Pediatrics 107(4), 706–711 (2001).
15 Beyer H, Holtzblatt K. Contextual design. Interactions 6 (1), 32–42 (1999).
16 Suchman L. Plans and Situated Actions: The Problem of Human-Machine Communication. Cambridge University Press, Cambridge, UK (1987).
17 Glaser B, Strauss A. The discovery of grounded theory: strategies for qualitative research. Aldine de Gruyter, NY, USA (1967).
18 Corbin J, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual. Sociol. 13(1), 3–21 (1990).
19 Seligman HK, Wallace AS, DeWalt DA et al. Facilitating behavior change with low-literacy patient education materials. Am. J. Health Behav. 31(0 1), S69–S78 (2007).
20 Doak CC, Doak LG, Root JH. Teaching Patients with Low Literacy Skills (Second Edition). J.B. Lippincott Company, PA, USA (1996).
21 Doak CC, Doak LG, Friedell GH, Meade CD. Improving comprehension for cancer patients with low literacy skills: strategies for clinicians. CA. Cancer J. Clin. 48(3), 151–162 (1998).
22 Oates D J, Paasche Orlow MK. Health literacy: communication strategies to improve patient comprehension of cardiovascular health. Circulation 119(7), 1049–1051 (2009).
23 Osborn CY, Cavanaugh K, Kripalani S. Strategies to address low health literacy and numeracy in diabetes. Clin. Diabetes 28(4), 171–175 (2010).
24 U.S. Department of Health and Human Services. Plain language: a promising strategy for clearly communicating health information and improving health literacy. www.health.gov/communication/literacy
25 Gibson PA, Ruby C, Craig MD. A health/patient education database for family practice. Bull. Med. Libr. Assoc. 79(4), 357–369 (1991).
26 Cataldo EF, Johnson RM, Kellstedt LA, Milbrath LW. Card sorting as a technique for survey interviewing. Pub. Opin. Quart. 34(2), 202–215 (1970).
27 Nawaz A. A comparison of card sorting analysis methods. Presented at: The 10th Asia Pacific Conference on Computer Human Interaction (Apchi 2012). Matsue-city, Shimane, Japan, 28–31 August 2012.
28 Erwin K, Pollari T. Small packages for big (qualitative) data. In: EPIC: The Ethnographic Practice In Industry Conference. John Wiley & Sons, Hoboken, NJ, USA, 44–61 (2013).