respiratory distress beyond the neonate -...
TRANSCRIPT

Respiratory Distress beyond the Respiratory Distress beyond the NeonateNeonate
Tina M. Slusher, MD FAAPTina M. Slusher, MD FAAPUniversity of MinnesotaUniversity of Minnesota
[email protected]@umn.edu

What is the biggest killer of What is the biggest killer of children>1mo & under 5yo worldchildren>1mo & under 5yo world--wide?wide?
Diar
rhea
Res
piratory
Illnes
ses
HIV/A
IDS
Mea
sles
25% 25%25%25%
1.1. DiarrheaDiarrhea2.2. Respiratory Respiratory
IllnessesIllnesses3.3. HIV/AIDSHIV/AIDS4.4. MeaslesMeasles


Pediatric Cardiopulmonary ArrestsPediatric Cardiopulmonary Pediatric Cardiopulmonary ArrestsArrests
1° Respiratory
Shock
1° Cardiac
1° Respiratory
Shock
1° Cardiac
10% 10%
80%80%

Acute Respiratory EmergenciesAcute Respiratory Emergencies
•• Common in infants/childrenCommon in infants/children•• If not properly treated can have significant M&MIf not properly treated can have significant M&M•• Practitioner MUST appreciate unique anatomic & Practitioner MUST appreciate unique anatomic &
physiologic characteristics of growing infant/childphysiologic characteristics of growing infant/child•• Ability to accurately access child in respiratory Ability to accurately access child in respiratory
distress CRITICAL!distress CRITICAL!


Airway positioning children <2yrsAirway positioning children <2yrs

Airway Airway PositioningPositioning≥≥2yo2yo
““Sniffing PositionSniffing Position””In the child older than 2 yearsIn the child older than 2 years
Towel is placed under the headTowel is placed under the head

Nasopharyngeal AirwayNasopharyngeal Airway
Contraindications:Contraindications:Basilar skull Basilar skull fracturefractureCSF leakCSF leakCoagulopathyCoagulopathy
Length: Nostril to TragusLength: Nostril to TragusLength: Nostril to Tragus
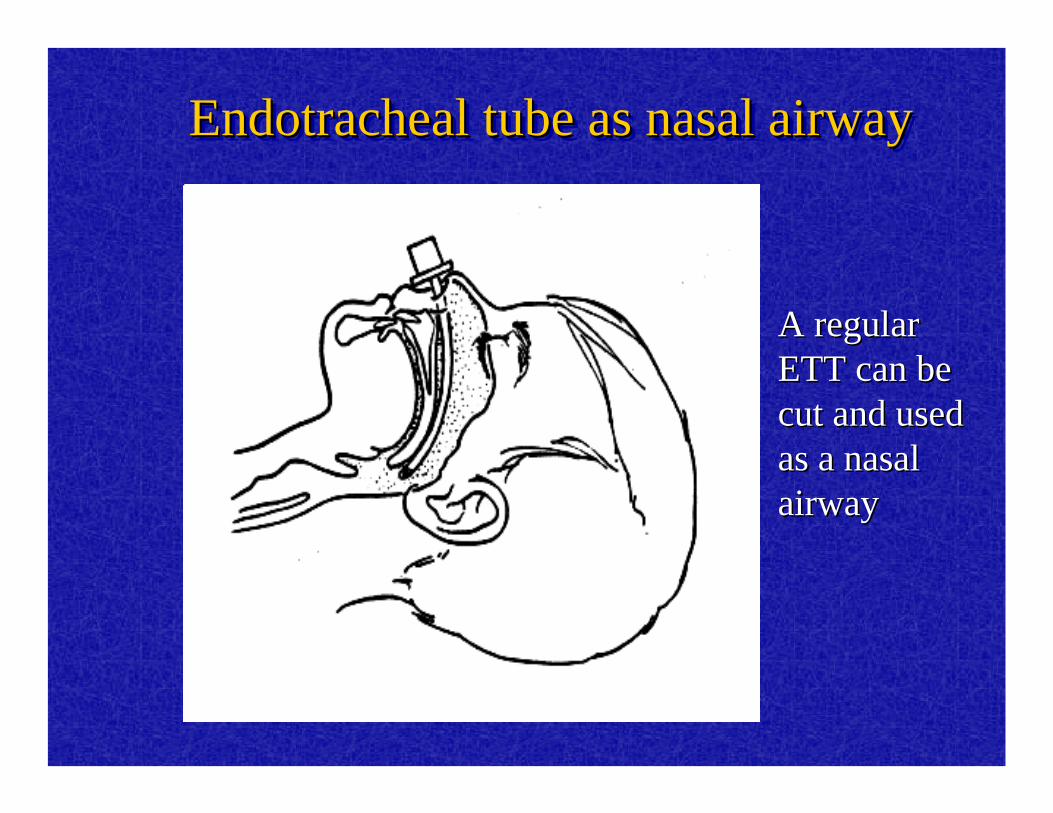
Endotracheal tube as nasal airwayEndotracheal tube as nasal airwayEndotracheal tube as nasal airway
A regular A regular ETT can be ETT can be cut and used cut and used as a nasal as a nasal airway airway

Adjuncts: Oral AirwaysAdjuncts: Oral Airways

Always evaluate for signs of Always evaluate for signs of respiratory distressrespiratory distress
•• TachypneaTachypnea--often 1often 1stst sign esp. in infantssign esp. in infants•• Seesawing or abdominal breathingSeesawing or abdominal breathing•• Head bobbingHead bobbing•• ↑↑respiratory effortrespiratory effort--retractions, flaringretractions, flaring
–– Retraction w/stridor or snoring Retraction w/stridor or snoring ≈≈ upper airway upper airway obstructionobstruction
–– Retractions w/expiratory wheezing Retractions w/expiratory wheezing ≈≈ lower lower airwayairway
–– Retractions w/grunting & Retractions w/grunting & ↑↑RR RR ≈≈ lung tissue lung tissue diseasedisease

First sign of respiratory distress in First sign of respiratory distress in most childrenmost children
Retr
actio
ns Tac
hypnea
Oxy
gen re
quire
ment
Tachyc
ardia
25% 25%25%25%1.1. RetractionsRetractions2.2. TachypneaTachypnea3.3. Oxygen Oxygen
requirementrequirement4.4. TachycardiaTachycardia

TachypneaTachypnea
•• Most common response of child to Most common response of child to ↑↑respiratory needsrespiratory needs
•• Most common due to hypoxia & Most common due to hypoxia & hypercarbiahypercarbia
•• May also be due to metabolic acidosis, May also be due to metabolic acidosis, pain, anxiety, or CNS insultpain, anxiety, or CNS insult

Normal Resting Respiratory RatesNormal Resting Respiratory Rates(infants/children(infants/children))
1212--1616>12 yrs.>12 yrs.1616--202066--12 yrs.12 yrs.2020--252544--6 yrs.6 yrs.2020--303011--4 yrs.4 yrs.2424--4646Infant (6Infant (6--12mo)12mo)3030--5050Infant (1Infant (1--6mo)6mo)3030--6060NewbornNewbornRATES (breathes/min)RATES (breathes/min)AGEAGE

•• Adept at Adept at recruitmentrecruitment of accessory of accessory musclesmuscles--manifest by retractions & nasal manifest by retractions & nasal flaringflaring
•• GruntingGrunting--closure of glottis at end closure of glottis at end expiration generating PEEP=sign of lower expiration generating PEEP=sign of lower airway airway dsds & an ominous sign& an ominous sign

Allow position of comfort!!!Allow position of comfort!!!
•• Position of comfortPosition of comfort--most adequate anatomic most adequate anatomic compensation relative to disease statecompensation relative to disease state
•• Sniffing positionSniffing position--upright, lean forward, generate upright, lean forward, generate their own jaw thrust to open upper airway their own jaw thrust to open upper airway (epiglottitis)(epiglottitis)
•• Tripoding positionTripoding position--upright, lean forward, support upright, lean forward, support upper thorax by use of extended arms (asthma upper thorax by use of extended arms (asthma & lower airway & lower airway dsds))
•• Open mouthOpen mouth--suggests dysphagia in presence of suggests dysphagia in presence of air hungerair hunger
Provide oxygen whenever possibleProvide oxygen whenever possible
•• CyanosisCyanosis–– OminousOminous-- represent eitherrepresent either
•• Inadequate oxygenation w/in pulmonary bed ORInadequate oxygenation w/in pulmonary bed OR•• Inadequate oxygen delivery by CV systemInadequate oxygen delivery by CV system
•• Signs of Signs of cyanosis cyanosis –– Infant=Infant=agitation, irritability, and failure to agitation, irritability, and failure to
feed feed –– Child=Child=somnolence somnolence esp. if hypercarbia as wellesp. if hypercarbia as well
What % oxygen does a premature What % oxygen does a premature neonate get from 1L per nasal canulaneonate get from 1L per nasal canula
30%
25%
50%
>60%
25% 25%25%25%
1.1. 30%30%2.2. 25%25%3.3. 50%50%4.4. >60%>60%

Oxygen TherapyOxygen Therapy
•• Oxygen Oxygen concentrators work concentrators work best with nasal best with nasal cannulacannula’’s.s.
66%66%1L1L60%60%¾¾LL44%44%½½LL34%34%¼¼LL
≅≅ FI02FI02Flow Flow raterate
Nasal(neonate)Nasal(neonate)Cannula Cannula Conversion Conversion ((GomellaGomella--Lange)Lange)
In an adult 1L flow ≅ 24% FIO2↑FIO2 by 4% for every 1L flow
up to 6 L flow (2L ≅28%)

Oxygen Delivery Techniques cont.Oxygen Delivery Techniques cont.
9090--95951010--1212Nonrebreather Nonrebreather maskmask
8080--90901010--1515OxyhoodOxyhood
5050--60601010--1212Partial Partial rebreathing maskrebreathing mask
2525--606044--1010Venturi maskVenturi mask3535--40401010--1515Face tentFace tent3535--606066--1010Simple face maskSimple face mask
% Oxygen% OxygenFlow (L/min)Flow (L/min)DeviceDevice

Impending Respiratory FailureImpending Respiratory Failure
•• Reduced air entryReduced air entry•• Severe workSevere work•• Cyanosis despite OCyanosis despite O22
•• Irregular breathing / apneaIrregular breathing / apnea•• Altered ConsciousnessAltered Consciousness•• DiaphoresisDiaphoresis
Teach PPV well before considering teaching intubationIF considering intubation have a plan of what to do
If no ventilator available



Trouble Shooting Ineffective Ventilation: IF chest Trouble Shooting Ineffective Ventilation: IF chest not rising and/or patient still blue/cyanoticnot rising and/or patient still blue/cyanotic
•• Reposition airwayReposition airway•• Verify appropriate mask size & ensure Verify appropriate mask size & ensure
tight seal on face avoiding eyestight seal on face avoiding eyes•• Suction if neededSuction if needed•• Check oxygen Check oxygen soucesouce•• Check bag & maskCheck bag & mask•• Insert Insert ngtngt or suction stomach if gastric or suction stomach if gastric
distentiondistention

Acute Upper Airway ObstructionAcute Upper Airway Obstruction•• Main causes include; viral croup, allergic Main causes include; viral croup, allergic
(recurrent croup), foreign body, retropharyngeal (recurrent croup), foreign body, retropharyngeal abscess, epiglottitisabscess, epiglottitis
•• Main features of AUAO is stridorMain features of AUAO is stridor•• Diagnosis based on the history and specific Diagnosis based on the history and specific
feature of each causefeature of each cause•• Treatment is specific for each cause including Treatment is specific for each cause including
antibiotics, steroids, intubation, tracheostomy antibiotics, steroids, intubation, tracheostomy and surgery and surgery
•• Supportive care include oxygen, airway Supportive care include oxygen, airway positioning and humidificationpositioning and humidification
Airway and Respiratory Distress from CCM Pediatric Airway ManagementBy Margaret Winkler UAB & APLS course edited by
Tina Slusher

*Croup Treatment*Croup Treatment
•• Racemic Epi: Racemic Epi: ≤≤4yo=4yo=0.05ml/kg up to max of 0.05ml/kg up to max of 0.5ml Q10.5ml Q1--2 hours>4yo 0.5ml q32 hours>4yo 0.5ml q3--4 hours4 hours
•• Epinephrine: 0.5ml/kg of 1:1000 solution Epinephrine: 0.5ml/kg of 1:1000 solution diluted in 3ml of NSS (max dose diluted in 3ml of NSS (max dose ≤≤4yo=2.5ml/dose; max dose 4yo=2.5ml/dose; max dose >4yo=5ml/dose)>4yo=5ml/dose)

Bacterial Pneumonia/Respiratory InfectionBacterial Pneumonia/Respiratory Infection
Cephalosporin + antiCephalosporin + anti--Staph if indicated or Staph if indicated or pertussis coveragepertussis coverage
S. pneumonia, H. S. pneumonia, H. influinflu, , Staph aureus, Staph aureus, GrpGrp A A Strep, pertussisStrep, pertussis
3mo3mo-- 5 5 yrs.yrs.
PCN OR Amp OR PCN OR Amp OR Cephalosporin + antiCephalosporin + anti--Staph if indicated or Staph if indicated or pertussis coveragepertussis coverage
S. pneumonia, H. S. pneumonia, H. influinflu, , GrpGrp A StrepA Strep
>5yo>5yo
Amp + Amp + CefotaxCefotaxH. H. influinflu, S. pneumonia, , S. pneumonia, GrpGrp A or B strep, A or B strep, pertussispertussis
11--3mo3mo
Amp + Aminoglycoside Amp + Aminoglycoside OR Amp + CefotaximeOR Amp + Cefotaxime
Group B strep, E. Coli, Group B strep, E. Coli, Klebsiella, Klebsiella, Pseudomonas, ListeriaPseudomonas, Listeria
<1mo<1mo
Empiric TherapyEmpiric TherapyBacterial PathogenBacterial PathogenAgeAge

Musts to Diagnosis PneumoniaMusts to Diagnosis Pneumonia
CXR
Stetho
scope
Res
piratory
Rate Fev
er, co
ugh
3 & 4
All o
f the a
bove
17% 17% 17%17%17%17%1.1. CXRCXR2.2. StethoscopeStethoscope3.3. Respiratory RateRespiratory Rate4.4. Fever, coughFever, cough5.5. 3 & 43 & 46.6. All of the aboveAll of the above

•• Studies have shown doctors, labs, and XStudies have shown doctors, labs, and X--rayray’’s are not required to drastically reduce s are not required to drastically reduce mortality due to pneumonia. mortality due to pneumonia.
•• Many lives have been saved by training Many lives have been saved by training village health workers to:village health workers to:
-- Count respiratory rates.Count respiratory rates.-- To administer oral antibiotics for To administer oral antibiotics for children whose fevers and coughs w/ children whose fevers and coughs w/ tachypneatachypnea..

BronchiolitisBronchiolitis•• Cough, URICough, URI•• Low grade feverLow grade fever•• Apnea in neonateApnea in neonate•• CracklesCrackles•• Air trappingAir trapping•• Appropriate to trial bronchodilators but Appropriate to trial bronchodilators but
only continue if helpsonly continue if helps•• Antibiotics NOT indicated or helpful!!Antibiotics NOT indicated or helpful!!
••AsthmaAsthma is primarily an is primarily an inflammatory diseaseinflammatory disease
Mucous pluggingMucous plugging
Smooth muscle Smooth muscle spasmspasm Airway edemaAirway edema
Asthma: CCM courseHendrick WernerUKMC- edited by Tina Slusher UL
Needed to Treat AsthmaNeeded to Treat Asthma
Steroid
s Spac
er for
MDI
1 & 3
All o
f the a
bove
20% 20% 20%20%20%1.1. SteroidsSteroids2.2. Spacer for MDI Spacer for MDI
3.3. ββ2 agonist2 agonist4.4. 1 & 31 & 35.5. All of the aboveAll of the above

Lung MechanicsLung Mechanics
•• HyperinflationHyperinflation–– Obstructed small airways cause premature Obstructed small airways cause premature
airway closure, leading to air trapping and airway closure, leading to air trapping and hyperinflationhyperinflation
•• HypoxemiaHypoxemia–– Inhomogeneous distribution of affected areas Inhomogeneous distribution of affected areas
results in V/Q mismatch, mostly shuntresults in V/Q mismatch, mostly shunt

AssessmentAssessment•• Findings consistent with impending Findings consistent with impending
respiratory failure:respiratory failure:–– Altered level of consciousnessAltered level of consciousness–– Inability to speakInability to speak–– Absent breath soundsAbsent breath sounds–– Central cyanosisCentral cyanosis–– DiaphoresisDiaphoresis–– Inability to lie downInability to lie down–– Marked pulsus paradoxusMarked pulsus paradoxus

OxygenOxygen
•• Deliver high flow oxygen, as severe Deliver high flow oxygen, as severe asthma causes V/Q mismatch (shunt)asthma causes V/Q mismatch (shunt)
•• Oxygen will not suppress respiratory drive Oxygen will not suppress respiratory drive in children with asthmain children with asthma
•• Schiff M. Schiff M. ClinClin Chest Med 1980;1(1):85Chest Med 1980;1(1):85--99
FluidFluid•• Judicious use of IV fluid necessaryJudicious use of IV fluid necessary
–– Most asthmatics are dehydrated on Most asthmatics are dehydrated on presentations presentations -- rehydrate torehydrate to eueuvolemiavolemia
–– OverOverhydration may lead to pulmonary hydration may lead to pulmonary edemaedema
–– SIADH may be common in severe SIADH may be common in severe asthmaasthma
•• Baker JW. Mayo Baker JW. Mayo ClinClin Proc 1976;51(1):31Proc 1976;51(1):31--44

ßß--AgonistsAgonists
Relatively selective Relatively selective ββ2 effects2 effects
Albuterol/SalbutamolAlbuterol/Salbutamol
TerbutalineTerbutaline
Significant Significant ββ1 1 cardiovascular effectscardiovascular effects
EpinephrineEpinephrine
ßß--receptor agonists stimulate receptor agonists stimulate ßß22--receptors on bronchial smooth muscle receptors on bronchial smooth muscle and mediate muscle relaxationand mediate muscle relaxation

Metered Dose Inhalers (Metered Dose Inhalers (MDIMDI’’ss))•• In pts w/ coordinated handIn pts w/ coordinated hand--
breathing motion albuterol breathing motion albuterol delivered by MDI delivered by MDI with with spacerspacer 44--8 8 puffs every 20 minutes for 3 doses puffs every 20 minutes for 3 doses compares favorably w/ nebs 2.5compares favorably w/ nebs 2.5--5mg q 20 minutes 5mg q 20 minutes
•• --In pts w/more severe asthma MDI In pts w/more severe asthma MDI dosing can be increased to 1 puff q dosing can be increased to 1 puff q 3030--60 seconds60 secondsBouletBoulet LP Canadian Asthma Consensus Group. CMAJ 1999;161(11suppl):S53LP Canadian Asthma Consensus Group. CMAJ 1999;161(11suppl):S53--Ackerman AD. Continuous nebsAckerman AD. Continuous nebs……CritCrit Care Med 1993;21:1422Care Med 1993;21:1422--44

HomeHome--made spacer for bronchodilator therapy in made spacer for bronchodilator therapy in children with acute asthma: randomized trialchildren with acute asthma: randomized trial””ZarZar et al Lancet 1999;354:979et al Lancet 1999;354:979--8282
•• InterpretationInterpretation–– Conventional spacer and sealed 500 ml plastic bottle Conventional spacer and sealed 500 ml plastic bottle
produced similar bronchodilationproduced similar bronchodilation–– Unsealed bottle gave intermediate improvementUnsealed bottle gave intermediate improvement–– Polystyrene cup was least effective as a spacerPolystyrene cup was least effective as a spacer
•• Use of bottle spacers should be incorporated into Use of bottle spacers should be incorporated into guidelines for asthma management in developing guidelines for asthma management in developing countries. countries.
Sealed spacersSealed spacersTake 500 ml plastic cold drink bottlesTake 500 ml plastic cold drink bottlesCut hole in base to fit size and shape of Cut hole in base to fit size and shape of MDIMDISeal bottleSeal bottle--MDI perimeter w/ glueMDI perimeter w/ glueUse opposite end as mouthpieceUse opposite end as mouthpiece

Other routes of Other routes of ββ agonistagonist•• TerbutalineTerbutaline can be given can be given subQsubQ in doses of in doses of
0.0050.005--0.01mg/kg (maximum 0.4mg/kg/dose) 0.01mg/kg (maximum 0.4mg/kg/dose) every 20 minutes X 3 dose (0.01ml/kg of every 20 minutes X 3 dose (0.01ml/kg of 1mg/cc drug)1mg/cc drug)
•• Werner Werner HA.StatusHA.Status asthmaticus in children: a review. Chest 2001;119:1913asthmaticus in children: a review. Chest 2001;119:1913--29.29.
•• EpinephrineEpinephrine SQ may help avoid need for SQ may help avoid need for mechanical ventilation in pts w/status mechanical ventilation in pts w/status asthmaticus. asthmaticus. –– SQ dose is 0.01cc/kg 1/1000 up to a maximum of SQ dose is 0.01cc/kg 1/1000 up to a maximum of
0.5cc every 150.5cc every 15--20 minutes x 320 minutes x 3--4 doses or Q4hrs 4 doses or Q4hrs prnprn(max in adults is 0.3cc)(max in adults is 0.3cc)

SteroidsSteroids•• Asthma is an Asthma is an
inflammatory inflammatory diseasedisease
•• Steroids are a Steroids are a mandatory mandatory element of first element of first line therapy line therapy regimen (few regimen (few exceptions only)exceptions only)
-20
0
20
40
60
80
100
120
140
-5 0 6 12 18 24
Hours
FEV
1% SteroidsPlacebo
Effect of Effect of i.vi.v. hydrocortisone vs placebo. hydrocortisone vs placebo
Fanta CH: Am J Med 1983;74:845Fanta CH: Am J Med 1983;74:845

AnticholinergicsAnticholinergics
•• Change in FEVChange in FEV11 is significantly greater is significantly greater when ipratropium was added to when ipratropium was added to ßß--agonists agonists (199 adults)(199 adults)
•• Rebuck AS: Am J Med 1987;82:59Rebuck AS: Am J Med 1987;82:59
•• Highly significant improvement in Highly significant improvement in pulmonary function when ipratropium was pulmonary function when ipratropium was added to albuterol (128 children). Sickest added to albuterol (128 children). Sickest asthmatics experienced greatest asthmatics experienced greatest improvementimprovement
•• SchuhSchuh S. J S. J PediatrPediatr 1995;126(4):6391995;126(4):639--4545

IpratropiumIpratropium•• Nebulize 250 Nebulize 250 -- 500 500 μμg every 6 hoursg every 6 hours
AtropineAtropine••Alternative to Ipratropium bromide Alternative to Ipratropium bromide ••Dose: 0.03Dose: 0.03--0.05mg/kg/dose 0.05mg/kg/dose
••(max 2.5mg/dose q 6(max 2.5mg/dose q 6--8 hours)8 hours)••Atropine comes in many different Atropine comes in many different strengths so strengths so yoursyours

TheophyllineTheophylline
•• Role in children with severe asthma Role in children with severe asthma remains controversialremains controversial
•• Narrow therapeutic rangeNarrow therapeutic range•• High risk of serious adverse effectsHigh risk of serious adverse effects•• Mechanism of effect in asthma remains Mechanism of effect in asthma remains
unclearunclear

•• May have a role in selected, critically May have a role in selected, critically ill children with asthma unresponsive ill children with asthma unresponsive to conventional therapy:to conventional therapy:–– Randomized, placeboRandomized, placebo--controlled, blinded controlled, blinded
trial (n=163) in children with severe trial (n=163) in children with severe status asthmaticusstatus asthmaticus
–– Theophylline group had greater Theophylline group had greater improvement in PFTs and Oimprovement in PFTs and O22 saturationsaturation
–– No difference in length of PICU stayNo difference in length of PICU stay–– Theophylline group had significantly Theophylline group had significantly
more N/Vmore N/V
–– Yung M. Arch Dis Child 1998;79(5):405Yung M. Arch Dis Child 1998;79(5):405--1010
0
10
20
30
40
50
60
Prior 6 hr 12 hr 24 hr
FEV 1 (%)
PlaceboTheophylline

Theophylline another point of viewTheophylline another point of view……..
•• Theophylline when added to continuous Theophylline when added to continuous nebulized albuterol therapy and IV nebulized albuterol therapy and IV corticosteroids, is as effective as terbutaline in corticosteroids, is as effective as terbutaline in treating critically ill childrentreating critically ill children……More cost More cost effectiveeffective……theophylline should be considered theophylline should be considered early in the management of critically ill early in the management of critically ill asthmatic childrenasthmatic children””–– Wheeler et al Wheeler et al PediatrPediatr CritCrit Care Med. 2005 Care Med. 2005
Mar;6(2):142Mar;6(2):142--7. 7.

MagnesiumMagnesium
•• SmoothSmooth--muscle relaxation by inhibition of calcium muscle relaxation by inhibition of calcium uptake (=bronchodilator)uptake (=bronchodilator)
•• Dosage recommendation: 25 Dosage recommendation: 25 -- 75 mg/kg 75 mg/kg i.vi.v. over 20 . over 20 minutes (May use drip of 25 mg/kg/hour and titrate minutes (May use drip of 25 mg/kg/hour and titrate attempting to maintain magnesium levels of 4attempting to maintain magnesium levels of 4--6 6 mg/dL mg/dL or if in the developing world maintaining knee or if in the developing world maintaining knee jerksjerks——if knee jerk present should not have toxic if knee jerk present should not have toxic magnesium levels)magnesium levels)
•• May be particularly beneficial in pts who are prone to May be particularly beneficial in pts who are prone to ↓↓Mg because of prolonged heavy use of Beta 2 Mg because of prolonged heavy use of Beta 2 agonistsagonists

ALL Wheezing NOT AsthmaALL Wheezing NOT Asthma•• Think other Think other dxdx when treatment failswhen treatment fails•• Bronchiolitis or other infectionBronchiolitis or other infection•• ForeignForeign--body aspirationbody aspiration•• TracheomalaciaTracheomalacia•• Congenital heart or lung diseaseCongenital heart or lung disease•• Pulmonary embolismPulmonary embolism•• CHFCHF•• Vocal cord dysfunctionVocal cord dysfunction•• Other forms of extraOther forms of extra--thoracic airway obstruction thoracic airway obstruction
(such as vascular ring or (such as vascular ring or papilomapapiloma))•• Higgins J. Am Higgins J. Am FamFam Physician..2003 Mar 1;67(5):997Physician..2003 Mar 1;67(5):997--1004. Review. 1004. Review.
